Embed Size (px)
Citation preview

Pergamon
0021-9630(95)00176-X
J. Child Psyehol Psyehiat. Vol. 37. No. 6, pp. 737-746,1996£> 1996 Association for Oiikl Psychology and Psychtatry
Published by Elsevier Science LtdPrinted in Great Britain. Al) rights reserved
0021-%3O/% $13.00 -f 0.00
Controlled Trial of a Brief Cognitive-Behavioural Intervention inAdolescent Patients with Depressive Disorders
Alison Wood, Richard Harrington and Anne MooreRoyal Manchester Children's Hospital, U.K.
Fifty-three child and adolescent psychiatric patients with depressive disorders wererandomly allocated to brief cognitive-behaviour therapy (CBT) or to a control treatment,relaxation training. Forty-eight patients completed the treatment phase of the trial, whichcomprised 5-8 treatment sessions. Post-treatment assessments showed a clear advantageof CBT over relaxation on measures of both depression and overall outcome. However,there were no significant differences between the treatments on comorbid anxiety andconduct symptoms. At follow-up, the differences between the groups were reduced, partlybecause of a high relapse rate in the DTP group and partly because subjects in therelaxation group continued to recover.
Copyright © 1996 Association for Child Psychology and Psychiatry.
Keywords: Depression, disorder, child, treatment
Abbreviations: ABS, Antisocial Behaviour Scale; CBT, Cognitive behaviour therapy;CGI, Clinical Global Improvement scale; DTP, Depression Treatment Programme; GAS,Global Assessment Scale; K-SADS, Kiddie — Schedule for Affective Disorders andSchizophrenia; MDD, Major depressive disorder; MFQ, Mood and Feelings Ques-tionnaire; RCI, Reliable change index; RCMAS, Revised Children's Manifest AnxietyScale; RT, Relaxation training; SAICA, Social Adjustment Inventory for Children andAdolescents; WJS, Warr and Jackson Self Esteem Scale
Clinical trials with adults have shown that cognitive-behavioural techniques are effective in reducing depres-sive symptoms (see reviews by Haaga and Beck (1992)and by HoUon, Shelton and Davis (1993)). Thesetechniques have also been evaluated in many studies ofgroup-administered treatment programmes in non-clin-ical samples of depr ssed children and adolescents, withgood results (Butler, xMeizitis, Friedman & Cole, 1980;Clarke et al., 1995; Hops & Lewinsohn, 1995; Jaycox,Reivich, Gillham & Seligman, 1994; Kahn, Kehle,Jenson & Clarke, 1990; Lewinsohn, Clarke, Hops &Andrews, 1990; Reynolds & Coats, 1986; Stark, 1990;Stark, Reynolds & Kaslow, 1987). However, it is notknown whether these positive findings apply to indivi-dual treatment given to patients with depressivedisorders in clinical samples.
The present study was therefore designed to test theprimary hypothesis that within a clinical sample ofadolescents with depressive disorders, a cognitive-behavioural depression treatment programme (DTP)would lead to a greater reduction in depression than a
Requests for reprints to Professor Harrington, Department ofChild and Adolescent Psychiatry, Royal Manchester Chil-dren's Hospital, Manchester Road, Pendlebury, ManchesterM27 4HA, U.K.
control intervention. The study also considered thesecondary questions: (1) do the benefits of the DTPpersist at follow-up?; and (2) is the DTP more effectivethan the control intervention on comorbid symptoms?
Subjects and Methods
OverviewInformed consent was obtained from the child and the
parent and cases were then randomly allocated to treatmentcondition (DTP or relaxation training), stratified by therapist(AW, RH). Measures of depression and other psychopathologywere obtained without knowledge of treatment condition by aresearch worker (AM) immediately after treatment ("post-treatment"), and at follow-up three months and six monthsafter the end of treatment.
Subjects
The study was based on 109 consecutive outpatient referralsto a clinic that specializes in the treatment of depression.
Inclusion criteria were: age 9 through 17 years, DSM-III-Rmajor depressive disorder (MDD) or RDC minor depression,and a Mood and Feelings Questionnaire (MFQ) (Angold,Costello, Pickles & Winder, 1987) score of 15 or niore.
Exclusion criteria were: psychotic disorder, inpatients,taking or likely to require antidepressants, unable to complete
737

738 A. WOOD et al.
the questionnaires, autism, attending a special school becauseof leaming problems, major physical illness or epilepsy.
Seventy-two cases met the inclusion criteria. Of these, 10needed other forms of treatment (usually medication) or werealready having that treatment, 6 refused the trial, 3 did notenter for other reasons and 53 entered the trial.
Rationale and Description of the Depression Treat-ment Programme (DTP)
The DTP was designed to tackle three areas of difficultythat have often been documented in children with depressivedisorders:
(i) Negative styles of thinking, which include low selfesteem, negative attributions and negative cognitions(Gotlib, Lewinsohn, Seeley, Rohde & Redner, 1993;Hammen, Adrian & Hiroto, 1988; Kempton, Hasselt,Bukstein & Null, 1994; Kendall, 1991; Lewinsohn,Rohde & Seeley, 1993; McCauley, Mitchell, Burke &Moss, 1988; Robins & Hinkley, 1989; Rohde,Lewinsohn & Seeley, 1990; Vostanis & Harrington,1994).
(ii) Difficulties with social relationships (Goodyer, Ger-many, Gowmsankur & Altham, 1991; Puig-Antich etal., 1993, 1985a, b).
(iii) Symptoms of depression, such as poor sleep andinactivity (Kolvin et al., 1991; Mitchell, McCauley,Burke & Moss, 1988; Ryan et al., 1987).
The programme therefore contains three main components:
(i) A "cognitive" component, the central elements ofwhich were drawn from traditional cognitive therapy(Beck, 1967).
(ii) A social problem solving component, which teacheschildren to set clear goals, generate altematives foraction, test them and measure the results.
(iii) A component designed to help with symptoms ofdepression, such as sleep hygiene measures andactivity scheduling.
This programme is similar to the group-based forms ofpsychological treatment that have been used in non-clinicalsamples (Butler et al., 1980; Jaycox et al., 1994; Kahn et al.,1990; Lewinsohn et al., 1990; Reynolds et al., 1986; Stark,1990; Stark et al., 1987). The main reason for using individual-based rather than group-based treatment was that even in ourspecialized clinic we seldom have enough depressed patientsat a time to run a group.
The programme was tested and standardized during threeyears' pilot work. An early version (Vostanis & Harrington,1994), which was based on treatment programmes used for thegroup treatment of depression in non-clinical samples(Reynolds et al., 1986; Stark, 1990), was further revised foruse with individual clinical cases of depressive disorder. Theassessment procedures and the treatment components havebeen specified in a manual.
Rationale and Description of Relaxation Training(RT)
A high proportion of depressed patients eventually recoverfrom the acute episode (Harrington & Vostanis, 1995) and inclinical samples no treatments have thus far been shownsignificantly to enhance the rate of recovery. Therefore, thekey question for the present study was whether or not the DTPwas better than no treatment. It was not, however, practical toput clinically referred depressed cases on a waiting list since
they often present urgently. Moreover control conditions suchas clinical monitoring are difficult to standardize and oftenhave a substantial therapeutic effect (Elkin et al., 1989).Rather, a comparison treatment was required that was credible;could be standardized; allowed monitoring of the patient;controlled for therapist contact and attention; and would havelittle effect on the core symptoms of depression.
There were three main reasons for thinking that relaxationtraining would meet these requirements. First, comorbiditywith nondepressive symptoms, which is usually seen as aproblem in the design of treatment trials in this age group(Kendall & Morris, 1991), could be used to produce a crediblecontrol treatment. Thus, since around 80% of depressed youngpatients suffer from anxiety symptoms such as somaticcomplaints or anxiety (Ryan et al., 1987), there is a logicalrationale for using relaxation to treat these symptoms. Thiswas intended to result in comparable patient expectancy andinterest. Second, although relaxation has been shown to havesome benefits for nonclinical depressed cases (Reynolds &Coats, 1986), it was not expected to be an active treatment foradolescent patients with depressive disorders because it mainlytargets symptoms that are not part of the DSM criteria forMDD. Indeed, research with adult depressed patients hasshown that relaxation is less effective than CBT (McLean &Hakstian, 1979). Third, one of the therapists had muchprevious experience with relaxation training in a researchcontext (Wieck, Harrington, Marks & Marsden, 1988), and itwas therefore expected that RT could be implemented withtherapist skill and effort that was similar to that of the DTP.
Relaxation training was specified in a manual and wasbased on the procedures described by Bemstein & Borkovec(1973).
Therapists
The two therapists (AW and RH) trained on at least fivecases before the trial and received supervision from apsychologist experienced in the use of CBT with adolescents.Both therapists had a minimum of three years experience inchild psychiatry. They met weekly throughout the trial insupervision.
Adherence of the therapists to the treatments was examinedby an independent assessor, who rated four audiotaped therapysessions in each modality and was asked to say which therapyhad been given. Seven out of eight assignments were correct.
Measures at Baseline
Psychiatric diagnoses were made using the Schedule forAffective Disorders and Schizophrenia Child Version (K-SADS) (Puig-Antich & Chambers, 1978), best estimate ofchild and parental accounts (Wood, Kroll, Moore & Harring-ton, 1995). Descriptive data on the severity of the child'sdisorder, developmental stage and psychosocial context werecollected using the following measures:
(i) The Social Adjustment Inventory for Children andAdolescents (SAICA) (John, Gammon, Pmsoff &Wamer, 1987) consists of 18 scales covering mostdomains of functioning. In the present study a meanscore was obtained by summing the scores on theapplicable scales and dividing by the number of thesescales. This score ranges from " 1 " ("no problems")to " 4 " ("severe problems").
(ii) Scores on the Global Assessment Scale (GAS)(Shaffer et al., 1983) can range from " 0 " ("needsconstant supervision") to "100" ("no symptoms"),with a score of "50" being defined as "any serious

TREATMENT OF DEPRESSIVE DISORDER IN ADOLESCENTS 739
symptomatology or impairment of functioning thatmost clinicians would think obviously requirestreatment".
(iii) A questionnaire measure of puberty (Petersen,Crockett, Richards & Boxer, 1988).
(iv) A semi-standardized assessment of the 39 abnormalpsychosocial stressor sub-categories of ICD-10 (vanGoor-Lambo, Orley, Poustka &. Rutter, 1990), withscores ranging from 0 (no stressors) to 78 (allstressors definitely present).
Cases entering the trial completed the following scales,which were chosen to measure the outcome of depression, therelated constmct of low self-esteem and comorbid problemssuch as anxiety. Identical versions of the first four scales hadbeen used in a large general population study (Harrington etal., 1995), thus enabling us to estimate the clinical significanceof changes using predefined criteria (Jacobson & Truax, 1991).
(i) A depression scale, the Mood and Feelings Ques-tionnaire (MFQ) (Angold et al., 1987). This is a 32item scale, with a total score that can range from 0 to64.
(ii) The Revised Children's Manifest Anxiety Scale{RCMAS) (Reynolds & Richmond, 1978) contains28 items (with the lie items removed), with a totalscore that can range from 0 to 28.
(iii) The self-esteem scale of Warr and Jackson (1985)(WJS), which contains eight items, with a total scorethat can range from 0 (high self esteem) to 32 (verylow self esteem).
(iv) Conduct problems over the past three months wererated on the Antisocial Behaviour Scale (ABS)(Olweus, 1989). This scale contains 32 items, with atotal score ranging from 0 to 32.
(v) A questionnaire measure of expectancy of treatment(a 0-8 Likert scale from Marks (1981), with 0 = "willnot help at all", 4 = "will definitely help", 8 = "willhelp greatly").
Parallel versions of these scales were completed by parentsabout the child.
Measures at Follow-Up
The questionnaire measures, plus a measure of satisfactionwith treatment (a 0-8 Likert scale, the '"satisfaction scale"(Marks, 1981), with 0 = "no help", 4 = "definitely helped", 8= "helped greatly") were repeated at the post-treatment andfollow-up assessments. In addition, the depression section ofthe K-SADS, the Clinical Global Improvement scale (CGI) (a0-7 scale, with 1 = "very much improved", 4 = "no change",7 = "much worse") and the GAS were completed by theassessor.
To ensure that the assessor did not have knowledge oftreatment condition subjects were asked at the end of therapynot to tell the assessor about the treatment. However, in threecases the assessor was told which treatment had been given.Removal of these cases from the analyses made no differenceto the results.
It was not possible to withold other interventions during thefollow-up. However, the assessor kept a record of the othertreatments that were given during the follow-up period, such associal work involvement and special education.
Psychometric Properties of the Main OutcomeMeasures and the Assessment of Clinical Significance
The MFQ-C, which was the main outcome measure, was
found to have good test-retest reliability and internalconsistency in this sample, and was also a sensitive andspecific measure of change in clinical depressive disorder(Wood et al., 1995). The MFQ-C was a good principaloutcome measure for our study because much MFQ data havebeen collected from general population samples in the U.K.(Cooper & Goodyer, 1993; Harrington et al., 1995; Thapar &McGuffin, 1994). Therefore, if it was assumed that clinicallysignificant change had something to do with a retum to normalfunctioning, a common supposition in psychotherapy outcomeresearch with both children and adults (Kazdin, Bass, Siegel &Thomas, 1989; Ogles, Lambert & Sawyer, 1995), then ajudgement could be made about the clinical significance ofsymptom levels after therapy. There were various ways ofachieving this, but in a study like ours in which the scores ofthe clinical population and the general population overlapped,the most conservative approach according to Jacobson andTruax (1991) was to designate scores that were less than apoint half-way between the general population mean and theclinical population mean as "clinically significant improve-ment". To do this, we used the data from the study ofHarrington and colleagues (1995), in which MFQ self-reportdata were collected on a sample of 1664 boys and girls agedbetween 11 and 18 years from three mainstream secondaryschools in London. In this age group, depression questionnairescores showed large sex differences and some age trends, andso we stratified both samples by age (13 years or younger or 14years or older) before calculating a separate MFQ-C cutoff forboys and girls within each age group. For boys these pointswere 24 and 19 respectively, and for girls they were 29 and 28.
Our second approach to measuring clinical significance withthe MFQ-C was also obtained from the work of Jacobson andTmax (1991) and involved estimating how much change hadoccurred for each subject. This was achieved by calculating areliable change index (RCI), which is a measure of thedifference between scores before and after treatment that takesinto account the reliability of the measuring instrument. Tocalculate the RCI we used reliability data from the presentstudy (Wood et al., 1995). An RCI of greater than 1.96suggests that the change in scores is unlikely to be the result offluctuations caused by an imprecise measuring instrument.
Our third approach to measuring clinical significance wasthe method that has been used in many clinical trials oftreatment of depressed people, such as the Treatment ofDepression Collaborative Research Programme (Elkin et al.,1989). This method involves determining the number ofpatients who meet predefined criteria for clinical remission, asassessed by a standardized clinical interview. In the presentstudy we used the criteria of Puig-Antich and his colleagues(1987), which are derived from ratings on the K-SADSdepression scale. These criteria define clinical remission asscores in both depressed mood and anhedonia of " 2 "("slight") or less. Inter-rater reliability for the depressionscale, tested by rating audiotapes, was good {N = 10, intraclasscorrelation = .93, F = 27.5, p < .001).
Determination of Sample Size
As indicated above, it was anticipated that relaxationtraining would be a credible yet inactive treatment for clinicalcases of MDD, somewhat analogous to giving a placebo inpharmacological research. If this tumed out to be the case, thenan effect size of more than 1.0 could be expected, which with aone-sided test would mean that a sample size of just 20 or socases would have been sufficient. On the other hand, ifrelaxation training was found to be an active treatment forclinical depression, or if the DTP was less effective than weexpected, then the effect size would be comparable to thatfound in clinical studies comparing two active treatments

740 A. WOOD et al.
Table 1Demographic and Clinical Characteristics of Subjects who Completed the Treatment Phase
DTP Relaxation (RT)Statistic
Sex, female N {%)Mean age, years {SD)Pubescent/postpubertaP, N (%)Duration of present episode (weeks), median (range)Major depression, N (%)RDC endogenous**, N (%)Conduct disorder, N (%)Overanxious disorder, N (%)ICD-10 psychosocial stressor score, mean (SD)Total SAICA score, mean (SD)Child expectancy, mean (SD)Parent expectancy, mean {SD)
16 (67%)13.8 (1.7)19 (79%)42 (3 to 156)21 (87%)6 (25%)4 (17%)
13 (54%)11.6 (5.2)2.4 (0.6)4.1 (3.1)4.2 (2.3)
17 (71%)14.6 (1.6)21 (87%)34 (4 to 250)23 (96%)7 (29%)7 (29%)
14 (58%)8.6 (4.7)2.5 (0.7)3.4 (2.3)4.9 (2.2)
z ' = 0.1, df 1f=1.7, rf/46
X^ = 0.6, df 1U=250,p=:.4
X^^ 1.1, dflxl = o.i,dfiX^ = l.l,dflX^ = 0.1,dfl
t = 2.1, df 46*t = 0.4, df 46t = 0.7, df 30t = 1.0, df 35
Note. DTP = depression treatment programme; RT = relaxation training; RDC = Research Diagnostic Criteria; ICD = Intema-tional Classification of Diseases; SAICA = Social Adjustment Inventory for Children and Adolescents.
^Tanner staging, as assessed with the Petersen questionnaire.''Six or more endogenous symptoms from the K-SADS.*p = .04.
(Fine, Forth, Gilbert & Haley, 1991), at around 0.6. With atwo-sided test, power calculations for this effect size gave arelatively large sample size, of 44 cases in each group.
From a statistical point of view, the most conservativestrategy would have been to opt for the larger sample and tocontinue the study until this sample size was achieved.However, if relaxation tumed out to be much inferior to theDTP, which was expected, then there would have been anethical problem. More than 40 children, most of whom weresuicidal as well as depressed (Wood, Moore, Harrington &Jay son, 1995 in press), would have been at risk of allocation toa treatment that was known to be ineffective. Alternatively, ifthe DTP was found to be no different from relaxation at themid-point, then the chances of a significant result being foundby completing the study could have been calculated (Puig-Antich et al., 1987) and the study could have been terminatedif these calculations showed that the probability of such aresult was very low.
Therefore, we opted for a compromise solution in which thestudy was designed to last for three years and recmit around 40cases in each group, but which included an interim analysishalf way through. TTiere are well established stoppage mles forsuch mid-point analyses (Pocock, 1983), which have been
conducted in several of the pharmacological trials withdepressed young people (Geller, Cooper, Graham, Marsteller& Bryant, 1990; Puig-Antich et al, 1987). Following theserules one interim analysis was conducted after 22 patients hadcompleted each type of treatment. This analysis was conductedon the main criterion outcome variable (MFQ-C), and a morestringent nominal significance level were chosen (p < .01).
Statistical Analysis
The comparability of the groups on baseline measures wastested using the appropriate parametric or nonparametric tests.Differences between the groups at the post-treatment assess-ment were tested by analysis of covariance (with the baselinevalue as the covariate). Maintenance of treatment effects wasstudied in independent group (DTP vs RT) x time (post vs 3-month vs 6-month) MANOVAs.
Results
Completion Rate
Subjects were regarded as "dropping out" of treat-
Table 2Parental Questionnaires
Parent MFQ
Parent RCMAS
Parent WJS
Parent ABS
MeanSD
MeanSD
MeanSD
MeanSD
Baseline
DTP
25.89.8
15.74.4
16.55.72.92.5
RT
28.711.616.97.3
16.45.53.83.2
Post-treatment
DTP
14.910.411.75.2
11.86.82.02.1
RT
19.813.313.97.3
12.86.61.92.0
Three monthfollow-up
DTP
18.917.211.36.9
10.87.41.61.7
RT
17.911.912.77.2
13.76.72.32.2
Six monthfollow-up
DTP
13.413.18.56.38.96.91.93.5
RT
15.212.99.97.39.77.02.22.5
Note. MFQ = Mood and Feelings Questionnaire; RCMAS = Revised Children's Manifest Anxiety Scale; WJS = Warr andJackson self-esteem scale; ABS = Antisocial Behaviour Scale.
None of the differences reached statistical significance atp < .05.

TREATMENT OF DEPRESSIVE DISORDER IN ADOLESCENTS 741
Table 3Clinical Outcome Measures for Subjects Who Completed the Treatment Phase
Clinical globalimprovement (CGI)
Clinically remitted^
MFQ-C score reachesclinical significance^
Reliable change indexscore (MFQ-C) >1.96^
Child satisfaction.
Parent satisfaction.
MeanSDN
{%)N
(%)A'
(%)MeanSD
MeanSD
Post-treatment
DTP
2.20.9^
13/24(54%)18/24(75%)12/24(50%)
4.52.7^5.6,2.3
RT
3.1,1.1
5/24,(21%)8/24,(33%)5/24,(21%)
2.8,2.44.43.0^
Three monthfollow-up
DTP
10/22,(45%)15/22^(68%)14/22^(64%)
3.92.9^5.02.6^
RT
—5/22,(25%)7/21,(33%)7/21,(33%)
2.5^4.42.0^
Six monthfollow-up
DTP_
12/22(54%)14/21,(67%)11/21(52%f
3.8,d
3.04.72.7^
RT
8/21,(38%)16/22,(73%)11/22,(50%)
3.3,2.9'4.62'l '
Note. DTP = depression treatment programme; RT = relaxation training.^Clinical remission was based on the K-SADS interview and the criteria of Puig-Antich and his colleagues (1987).^Clinical significance represents the no. of individuals whose MFQ-C score was less than a cutpoint half-way between the mean
for the clinical population and the mean for the general population.^Reliable change index >1.96 represents the no. of individuals who reliably improved when compared with the pretreatment
MFQ-C rating.Pairs of means or proportions in the same column with the same subscript are not significantly different aip < .05 in a f-test or a
Chi-square test, as appropriate, of the differences between the DTP and RT.
ment if they missed four or more treatment sessions. Themean number of sessions, including the assessmentsession, did not differ significantly between the DTP andRT groups (6.4 and 6.2, respectively), and neither didmean duration of treatment (64.5 days and 58.8 days,respectively).
Of the 53 patients who entered the trial {N = 26 DTP,N=27 RT) 48 completed treatment (A = 24 DTP, A = 24RT). Four cases dropped out {N = 1 DTP, A = 3 RT) andone was excluded during treatment (DTP) because thepsychiatrist who was jointly responsible for care, whowas not a member of the research team, felt that aworsening in clinical state required medication. At thepost-treatment assessment, MFQ-child (MFQ-C) datawere obtained on all 53 cases who had entered the trial.These data were obtained on 48 subjects at both thethree- and six-months follow-ups. K-SADS data wereobtained on 53 subjects at post-treatment, 47 subjects atthree months and 48 subjects at six months.
Sample Characteristics at Baseline
Table 1 shows the demographic and clinical char-acteristics of the 48 cases who completed treatment. Asthe table indicates, the treatment groups were wellmatched on most variables, though the group who hadthe DTP had a significantly higher level of psychosocialstressors at the pretreatment assessment.
There were no significant differences between thegroups on any of the baseline measures of psychopathol-ogy (Figs. 1-5). The groups did not differ in theirexpectancies of treatment (Table 1). In line with manyprevious studies, parental ratings of depressive symp-toms in their child were significantly lower than childratings (paired t test, t = 4.2, df = 46, p < .001).
Post-Treatment Assessment
Tables 2 and 3 and the figures, summarize the resultsof the post-treatment assessments. The mean level ofdepressive symptoms (MFQ-C) was significantly lowerin the DTP group than in the relaxation group(ANCOVA, N = 4S, with baseline MFQ-C score as thecovariate, main effect of treatment condition, df 1,F = 8.0, p < .01), as were child reports of negative selfimage on the WJS (ANCOVA, A^=43, main effectF=13.1,p< .001).
40 1
ouC/)
cea0)
30-
20-
10-
0
DTPRT
Baseline Post 3 months 6 monthsTreatment
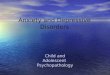
Figure 1. Mean MFQ-child scores for the DTP (dark circles)and relaxation (clear circles) groups at different time points.Error bars show standard errors.

742 A. WOOD et al.
201
15-ou(A
OCCc
10-
5- DTPRT
Baseline Post 3 months 6 monthstreatment
oo
m
c(0a>
6 i
5-
4-
2-
1 - DTPRT
Baseline Post 3 months 6 monthstreatment
Figure 2. Mean RCMAS-child scores for the DTP (darkcircles) and relaxation (clear circles) groups at different timepoints. Error bars show standard errors.
Figure 4. Mean ABS-child scores for the DTP (dark circles)and relaxation (clear circles) groups at different time points.Error bars show standard errors.
The DTP group was significantly more likely to beimproved than the RT group on both of the measures ofclinical significance that were derived from the MFQ-C(Table 3). Patients who had the DTP were also morelikely to be rated by the assessor with the K-SADS ashaving clinically remitted from their depressive disorderthan patients who had relaxation {x^ = 5.7, df=l,p = .02). In addition, they had significantly lower (ie,more improved) Clinical Global Improvement scores{t = 3.0, df= 46, p < .01). For example, 22 out of the 24cases who had the DTP were rated by the assessor ashaving "improved" (CGI score of 1, 2, or 3) at the post-treatment assessment, compared with 15 out of 24relaxation cases {x^ = 5.8, df=l,p = .02). Moreover, in
20 n
1 5 -0)
ou
cn
Cre
10-
5-DTPRT
Baseline 3 months 6 monthstreatment
Figure 3. Mean WJS-child scores for the DTP (dark circles)and relaxation (clear circles) groups at different time points.Error bars show standard errors.
comparison with children who had relaxation, childrenwho had the DTP were significantly more satisfied withtreatment {t = 2.2, df 40, p < .05) and had significantlyhigher (i.e. less impaired) GAS scores (ANCOVA, withpretreatment GAS as the covariate, n = 48, main effect oftype of treatment df= 1, F = 5.5, p < .05).
On the other hand, there were no significantdifferences between the groups on anxiety (RCMAS)and conduct (ABS) symptoms. Anxiety decreasedsignificantly between baseline and the post-treatmentassessment (paired t-test, t = 3.4, df= 42, p < .01) butconduct symptoms did not (paired Mest, t - 1.5, df= 39,
80-1
60-
cn<O
cra0)
40-
20-
0
DTPRT
Baseline Post 3 months 6 monthstreatment
Figure 5. Mean GAS-child scores for the DTP (dark circles)and relaxation (clear circles) groups at different time points.Error bars show standard errors.

TREATMENT OF DEPRESSIVE DISORDER IN ADOLESCENTS 743
None of the differences between the groups onparental reports reached statistical significance (Table2).
Although the groups were well matched on mostvariables the DTP cases had higher levels of adversepsychosocial situations at baseline. However, remissionfrom depression tended to be associated with reducedlevels of adversity. So, when ICD psychosocial scorewas entered into a regression model with treatmentgroup as the other predictor and MFQ-C score post-treatment as the criterion, the effect of group wasincreased.
Intent to Treat Analyses
Another problem that could exaggerate differencesbetween treatments would be if drop-outs differed fromthose who completed treatment. This issue can betackled by analyzing the results on an "intent to treatbasis", including everyone who entered the trial. All theanalyses were therefore repeated on the total sample of53 cases. The DTP was still superior to relaxation(ANCOVA, main effect of type of treatment on MFQself-report, N = 53,dfl,F = 6.2, p = .02).
Follow-Up Analyses
As the figures indicate, the differences between theDTP and relaxation groups were reduced at follow-up.MANOVA of the MFQ-child data (AT = 39) showedsignificant time {F - 3.3, p = .04) and group x timeinteractions (F = 4.6, p = .01). Planned univariate F-tests(with dfl, 37) showed that, at post-treatment, significantgroup differences existed in favour of the DTP on theMFQ-child (F = 7.9, p < .01). However, at neither thethree month nor the six month follow-up was there asignificant difference between the treatments on theMFQ-child score (F=1.9, p = .2; and F=.2 , p = .6,respectively).
Some differences between the groups did persist to thethree months follow-up. For example, on the twomeasures of clinical significance that were derived fromthe MFQ-C the DTP was still superior to relaxation(Table 3). Univariate F-tests showed significant differ-ences ip < .05) between the DTP and relaxation on self-reports of anxiety (F (1,34) = 4.2) and low self-esteem F[1,36) = 4.6]. However, on most other measures the twogroups did not differ at the three month follow-up, andby six months the groups were very similar.
The reduction in the difference between the twogroups was partly because the relaxation group con-tinued to improve, with a significant decline between thepost-treatment MFQ-C score and the six-month follow-up score (paired f-test, t = 3.6, df= 21, p < .01). How-ever, the lack of difference between the groups at follow-up was also due to relapses in the DTP group. Thus, ofthe 14 cases in the DTP group who had remitted fromdepression either by the post-treatment assessment(A = 13) or by the three-month assessment (N = 1), 6(or 43%) had another episode of depression (5 majordepression, 1 minor depression) during the follow-upperiod.
The mean MFQ-C score of the group who relapsed
climbed from 12.4 (SD = 6.4) at post-treatment to 31.2(SD = 10.6) by the 3-month follow-up. By contrast, themean MFQ-C score of the group who had remitted aftertreatment continued to decline, from a mean of 14.3(SD = 16.3) at post-treatment to a mean of 6.8 (SD = 6.8)at three months (Wilcoxon test, z=1.5, /7 = .13). Itseems, then, that the apparent stability of MFQ-C scoresafter the DTP (Fig. 1) masked at least three subgroups:(a) a group who never remitted; (b) a group who remittedand then relapsed; and (c) a group who remitted and thencontinued to improve.
Finally, it should be noted that the DTP group hadsignificantly fewer other treatments during the follow-upthan the relaxation group (42% versus 71% respectively,^ 4df
Discussion
DTP versus Relaxation Training
The findings support our main hypothesis that at thepost-treatment assessment the DTP leads to a greaterreduction in depressive symptoms than a controlpsychological intervention. The size of the effect ofthe DTP on MFQ scores (0.73) was "moderately" large(Kazdin & Bass, 1989) and the benefits of activetreatment over the control condition were found across arange of other measures, including self-esteem, patientsatisfaction, clinical measures of remission, and globalfunctioning. We can conclude that the beneficial effectsof the DTP stem at least in part from factors specific tothis therapy and are not just the result of non-specificfactors such as therapist attention.
However, these differences between the DTP andrelaxation training were found mainly on child ratings ofpsychopathology. Parental ratings, though in the samegeneral direction, did not reach statistical significance.Of course, the main outcome of this study wasdepression, and parents will often be unaware of evensevere depression or suicidal attempts in their offspring(Harrington, 1993). The same seems to have occurred inour study, in which parental ratings of depression werelower than child ratings. Nevertheless, the finding thatparental assessments did not distinguish the groups isimportant.
It must also be noted that the two treatments did notdiffer greatly in their effects on nondepressive sympto-matology. Anxiety symptoms were reduced in bothforms of treatment, whereas conduct symptoms re-mained unchanged.
Generalization of the Findings
In interpreting the positive results of this trial, itshould be emphasized that although nearly all our caseshad MDD, it cannot be assumed that the results wouldapply to the more severe cases of MDD who have beenadmitted to drug trials. The cases included in our studywere relatively mild compared to these cases, as judgedby the findings that (a) their GAS scores were higher(Geller et al., 1992, 1990); (b) a smaller proportion hadendogenous subtype (Geller et al., 1992, 1990; Puig-

744 A. WOOD et al.
Antich et al., 1987); (c) they were outpatients, whereasdrug trials have also included inpatients.
Nevertheless, the kinds of cases recruited into thisstudy accounted for about two thirds of all referrals toour clinic. About 50% responded to the DTP, which islikely then to be an appropriate treatment for manydepressed outpatients.
Clinical Significance
Several of our findings suggest that the DTP leads toclinically important short-term improvements in de-pressed young people. First, there were significantbetween group differences on many of the clinicalmeasures (Table 3), including patient satisfaction and allthe measures of "clinical significance". Second, by theend of treatment around two thirds of the cases had MFQscores that were closer to the mean of the generalpopulation than to that of the clinical population. Thisimprovement persisted to the 6-month follow-up.
On the other hand, the significance of our results forroutine clinical practice is limited by the finding that theDTP did not appear to have any specific benefits forcomorbid problems such as anxiety and conductsymptoms. This is important because comorbidity isvery common among depressed adolescents. It suggeststhat in routine practice the DTP should be combinedwith other forms of treatment.
Follow-Up Findings
In interpreting the follow-up findings, we should firstemphasize that our study was not designed to detectlarge differences between the groups at follow-up, butrather to test hypotheses about short-term treatmenteffects. Some of the differences between the groups atthe three-month follow-up would probably have reachedsignificance with a larger sample. However, by the 6-month follow-up these differences were trivial in astatistical sense, and therefore it seems reasonable toconclude that specific treatment effects, as measured bycase-control differences, genuinely did not persist.
At first sight, this seems disappointing. However,since patients who had the DTP were less likely to begiven other forms of treatment during the follow-upperiod than the RT group, it may be that the size of thetreatment effect was spuriously reduced. Moreover, theDTP was relatively brief, lasting just five to eightsessions and was not designed to produce long-lastingeffects. Indeed, research with depressed adults hasshown that there is a high relapse rate when psycholo-gical or pharmacological treatments for the acuteepisode are stopped (Kupfer, 1992; Prien, 1992).Adolescent depressive disorders have many features incommon with adult-onset forms of the condition(Harrington & Wood, 1995), and seem to be as difficultto treat (Ryan, 1990). There is therefore no a priorireason for thinking that beneficial effects of treatmentwill be any more persistent in adolescents than in adults.
Conclusions
We can conclude, then, that although CBT appears to
be a promising treatment for the acute phase ofdepressive disorder in adolescent outpatients, moreresearch is needed on the value of longer term formsof the therapy. It will be particularly important to studyits ability to prevent relapse.
Acknowledgements—^This research was supported by agrant from the Mental Health Foundation. Special thanks aredue to all those consultants who referred cases to our clinic.We also want to thank Christine Verduyn for clinicalsupervision during the trial and Sally HoUis for her help withstatistical analysis.
References
Angold, A., Costello, E. J., Pickles, A. & Winder, F. (1987).The development of a questionnaire for use in epidemiolo-gical studies of depression in children and adolescents.London: Medical Research Council Child Psychiatry Unit.
Beck, A. T. (1967). Depression: clinical, experimental andtheoretical aspects. New York: Harper and Row.
Bernstein, A. D. & Borkovec, T. D. (1973). Progressiverelaxation training. Champaign, IL: Research Press.
Butler, L., Meizitis, S., Friedman, R. & Cole, E. (1980). Theeffect of two school-based intervention programs ondepressive symptoms in pre-adolescents. American Educa-tion Research Journal, 17, 111-119.
Clarke, G. N., Hawkins, W., Murphy, M., Sheeber, L. B.,Lewinsohn, P. M. & Seeley, J. R. (1995). Targetedprevention of unipolar depressive disorder in an at-risksample of high school adolescents: a randomized trial of agroup cognitive intervention. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 34, 312-321.
Cooper, P. J. & Goodyer, I. (1993). A community study ofdepression in adolescent girls: I—estimates of symptom andsyndrome prevalence. British Journal of Psychiatry, 163,369-374.
Elkin, I., Shea, T., Watkins, J. T., Imber, S. D., Sotsky, S. M.,Collins, J. F., Glass, D. R., Pilkonis, P. A., Leber, W. R.,Docherty, J. P., Fiester, S. J. & Parloff, M. B. (1989).National Institute of Mental Health treatment of depressioncollaborative research program. General effectiveness oftreatments. Archives of General Psychiatry, 46, 971-982.
Fine, S., Forth, A., Gilbert, M. & Haley, G. (1991). Grouptherapy for adolescent depressive disorder: a comparison ofsocial skills and therapeutic support. Journal of theAmerican Academy of Child Psychiatry, 30, 75-79.
Geller, B., Cooper, T. B., Graham, D. L., Fetner, H. H.,Marsteller, F. A. & Wells, J. M. (1992). Pharmacokineti-cally designed double-blind placebo-controlled study ofnortriptyline in 6- to 12-year-olds with major depressivedisorder. Journal of the American Academy of ChildPsychiatry, 31, 34-44.
Geller, B., Cooper, T. B., Graham, D. L., Marsteller, F. A. &Bryant, D. M. (1990). Double-blind placebo-controlledstudy of nortriptyline in depressed adolescents using a"fixed plasma level" design. Psychopharmacoloey Bulletin,26,85-90.
Goodyer, I. M., Germany, E., Gowmsankur, J. & Altham, P.(1991). Social influences on the course of anxious anddepressive disorders in school-age children. British Journalof Psychiatry, 158, 676-684.
Gotlib, I. H., Lewinsohn, P. M., Seeley, J. R., Rohde, P. &Redner, J. E. (1993). Negative cognitions and attributionalstyle in depressed adolescents: An examination of stabilityand specificity. Journal of Abnormal Psychology, 102, 607-
Haaga, D. A. F. & Beck, A. T. (1992). Cognitive therapy. In E.

TREATMENT OF DEPRESSIVE DISORDER IN ADOLESCENTS 745
S. Paykel (Ed.), Handbook of affective disorders (2nd Ed.)(pp. 511-523). Edinburgh: Churchill Livingstone.
Hammen, C, Adrian, C. & Hiroto, D. (1988). A longitudinaltest of the attributional vulnerability model in children atrisk for depression. British Journal of Clinical Psychology,27, 37-46.
Harrington, R. C. (1993). Depressive disorder in childhoodand adolescence. Chichester: John Wiley.
Harrington, R. C, Rutter, M., Pickles, A., Fudge, H.,Groothues, C. and Bredenkamp, D. (1995). Age trends indepressive symptomatology during early adolescence:comparison with other psychological symptoms. In pre-paration.
Harrington, R. C. & Vostanis, P. (1995). Longitudinalperspectives and affective disorder in children and adoles-cents. In I. M. Goodyer (Ed.), The depressed child andadolescent. Developmental and clinical perspectives (pp.311-341). Cambridge: Cambridge University Press.
Harrington, R. C. & Wood, A. J. (1995). Validity andclassification of child and adolescent depressive disorders.Review of the field circa 1995. In G. Forrest (Ed.),Childhood depression. ACPP Occasional paper No. 11(pp. 3-22). London: ACPP.
HoUon, S. D., Shelton, R. C. & Davis, D. D. (1993). Cognitivetherapy for depression: conceptual issues and clinicalefficacy. Journal of Consulting and Clinical Psychology,61, 270-275.
Hops, H. & Lewinsohn, P. M. (1995). A course for thetreatment of depression among adolescents. In K. D. Craigand K. S. Dobson (Eds), Anxiety and depression in adultsand children (pp. 230-245). Thousand Oaks, CA: SagePublications.
Jacobson, N. S. & Truax, P. (1991). Clinical significance: astatistical approach to defining meaningful change inpsychotherapy research. Journal of Consulting and ClinicalPsychology, 59, 12-19.
Jaycox, L. H., Reivich, K. J., Gillham, J. & Seligman, M. E. P.(1994). Prevention of depressive symptoms in schoolchildren. Behaviour Research and Therapy, 32, 801-816.
John, K., Gammon, G., Pnisoff, B. & Warner, V. (1987). TheSocial Adjustment Schedule for Children and Adolescents(SAICA). Testing of a new semi-structured interview.Journal of the American Academy of Child Psychiatry, 26,898-911.
Kahn, J. S., Kehle, T. J., Jenson, W. R. & Clarke, E. (1990).Comparison of cognitive-behavioral, relaxation, and self-modelling interventions for depression among middle-school students. School Psychology Review, 19, 195-210.
Kazdin, A. E. & Bass, D. (1989). Power to detect differencesbetween alternative treatments in comparative psychother-apy outcome research. Journal of Conulting and ClinicalPsychology, 57, 138-147.
Kazdin, A. E., Bass, D., Siegel, T. & Thomas, C. (1989).Cognitive-behavioural therapy in the treatment of childrenreferred for antisocial behaviour. Journal of Consulting andClinical Psychology, 57, 522-535.
Kempton, T., Hasselt, V. B. V., Bukstein, O. G. & Null, J. A.(1994). Cognitive distortions and psychiatric diagnosis indually diagnosed adolescents. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 33, 217-222.
Kendall, P. C. (Ed.) (1991). Child and adolescent therapy.Cognitive-behavioural procedures. New York: GuilfordPress.
Kendall, P. C. & Morris, R. J. (1991). Child therapy: issuesand recommendations. Journal of Consulting and ClinicalPsychology, 59, 777-784.
Kolvin, I., Barrett, M. L., Bhate, S. R., Bemey, T. P.,Famuyiwa, O. O., Fundudis, T. & Tyrer, S. (1991). TheNewcastle Child Depression Project: diagnosis and classi-
fication of depression. British Journal of Psychiatry,i59(suppl 11), 9-21.
Kupfer, D. (1992). Maintenance treatment in recurrentdepression: cunent and future directions. British Journalof Psychiatry, 161, 309-316.
Lewinsohn, P. M., Clarke, G. N., Hops, H. & Andrews, J.(1990). Cognitive-behavioural treatment for depressedadolescents. Behavior Therapy, 21, 385^01.
Lewinsohn, P. M., Rohde, P. & Seeley, J. R. (1993).Psychosocial characteristics of adolescents with a historyof suicide attempt. Journal of the American Academy ofChild and Adolescent Psychiatry, 32, 60-68.
Marks, I. (1981). Cure and care ctf neuroses. New York: JohnWiley.
McCauley, E., Mitchell, J. R., Burke, P. & Moss, S. (1988).Cognitive attributes of depression in children andadolescents. Journal of Consulting and ClinicalPsychology, 56, 903-908.
McLean, P. D. & Hakstian, A. R. (1979). Clinical depression:comparative efficacy of outpatient treatments. Journal ofConsulting and Clinical Psychology, 47, 818-836.
Mitchell, J., McCauley, E., Burke, P. M. & Moss, S. J. (1988).Phenomenology of depression in children and adolescents.Journal of the American Academy of Child Psychiatry, 27,12-20.
Ogles, B., Lambert, M. J. & Sawyer, J. D. (1995). Clinicalsignificance of the National Institute of Mental HealthTreatment of Depression Collaborative Research Programdata. Journal of Consulting and Clinical Psychology, 63,321-326.
Olweus, D. (1989). Prevalence and incidence in the study ofantisocial behaviour: definitions and measurement. In M.W. Klein (Ed.), Cross-national research in self-reportedcrime and delinquency (pp. 187-201). Dordrecht, theNetherlands: Kluwer.
Petersen, A. C, Crockett, L., Richards, M. & Boxer, A. (1988).A self-report measure of pubertal status: reliability, validity,and initial norms. Journal of Youth and Adolescence, 17,117-133.
Pocock, S. J. (1983). Clinical trials: a practical approach.Chichester: John Wiley.
Prien, R. F. (1992). Maintenance treatment. In E. S. Paykel(Ed.), Handbook of affective disorders (2nd Ed.) (pp. 419-435). Edinburgh: Churchill Livingstone.
Puig-Antich, J. & Chambers, W. (1978). The schedule foraffective disorders and schizophrenia for school-agedchildren. New York State Psychiatric Institute: Unpublishedinterview schedule.
Puig-Antich, J., Kaufman, J., Ryan, N. D., Williamson, D. E.,Dahl, R. E., Lukens, E., Todak, G., Ambrosini, P.,Rabinovich, H. & Nelson, B. (1993). The psychosocialfunctioning and family environment of depressedadolescents. Journal of the American Academy of Childand Adolescent Psychiatry, 32, 244-253.
Puig-Antich, J., Lukens, E., Davies, M., Goetz, D., Brennan-Quattrock, J. & Todak, G. Psychosocial functioning inprepubertal major depressive disorders. II. Interpersonalrelationships after sustained recovery from affectiveepisode. Archives of General Psychiatry, 42, 511-517.
Puig-Antich, J., Lukens, E., Davies, M., Goetz, D., Brennan-Quattrock, J. & Todak, G. Psychosocial functioning inprepubertal major depressive disorders. I. Interpersonalrelationships during the depressive episode. Archives ofGeneral Psychiatry, 42, 500-507.
Puig-Antich, J., Perel, J. M., Lupatkin, W., Chambers, W. J.,Tabrizi, M. A., King, J., Goetz, R., Davies, M. & Stiller, R.L. (1987). Imipramine in prepubertal major depressivedisorders. Archives of General Psychiatry, 44, 81-89.
Reynolds, C. R. & Richmond, B. O. (1978). What I think and

746 A. WOOD et al.
feel: a revised version of the children's manifest anxiety.Journal of Abnormal Child Psychology, 6, 271-280.
Reynolds, W. M. & Coats, K. I. (1986). A comparison ofcognitive-behavioural therapy and relaxation training for thetreatment of depression in adolescents. Journal of Consult-ing and Clinical Psychology, 54, 653-^60.
Robins, C. J. & Hinkley, K. (1989). Social-cognitiveprocessing and depressive symptoms in children: a compar-ison of measures. Journal of Abnormal Child Psychology,17, 29-36.
Rohde, P., Lewinsohn, P. M. & Seeley, J. R. (1990). Arepeople changed by the experience of having an episode ofdepression? A further test of the scar hypothesis. Journal ofAbnormal Psychology, 99, 264-271.
Ryan, N. D. (1990). Pharmacotherapy of adolescent majordepression. Beyond TCAs. Psychopharmacology Bulletin,26, 75-79.
Ryan, N. D., Puig-Antich, J., Ambrosini, P., Rabinovich, H.,Robinson, D., Nelson, B., Iyengar, S. & Twomey, J. (1987).The clinical picture of major depression in children andadolescents. Archives of General Psychiatry, 44, 854-861.
Shaffer, D., Gould, M. S., Brasic, J., Ambrosini, P., Fisher, P.,Bird, H. & Aluwahlia, S. (1983). A children's GlobalAssessment Scale (C-GAS). Archives of GeneralPsychiatry, 40, 1228-1231.
Stark, K. D. (1990). Childhood depression: school-basedintervention. New York: Guilford Press.
Stark, K. D., Reynolds, W. M. & Kaslow, N. (1987). Acomparison of the relative efficacy of self-control therapyand a behavioral problem-solving therapy for depression in
children. Journal of Abnormal Child Psychology, 15, 9 1 -113.
Thapar, A. & McGuffm, P. (1994). A twin study of depressivesymptoms in childhood. British Journal of Psychiatry, 165,259-265.
van Goor-Lambo, G., Orley, J., Poustka, F. & Rutter, M.(1990). Classification of abnormal psychosocial situations:preliminary report of a revision of a WHO scheme. Journalof Child Psychology and Psychiatry, 31, 229-241.
Vostanis, P. & Harrington, R. C. (1994). Cognitive-behaviour-al treatment of depressive disorder in child psychiatricpatients—^rationale and description of a treatment package.European Child and Adolescent Psychiatry, 3, 111-123.
Warr, P. B. & Jackson, P. R. (1985). Factors influencing thepsychological impact of prolonged unemployment and ofreployment. Psychological Medicine, 15, 795-807.
Wieck, A., Harrington, R. C , Marks, I. M. & Marsden, C. D.(1988). Writer's cramp: a controlled trial of habit reversaltreatment. British Journal of Psychiatry, 153, 111-115.
Wood, A., Kroll, L., Moore, A. & Harrington, R. C. (1995).Properties of the Mood and Feelings Questionnaire inadolescent psychiatric outpatients: a research note. Journalof Child Psychology and Psychiatry, 36, 327-334.
Wood, A , Moore, A., Harrington, R. C. & Jayson, D. (inpress). Clinical validity of major depression-endogenoussubtype in adolescent patients. European Child andAdolescent Psychiatry.
Accepted manuscript received 4 December 1995