-
7/28/2019 Control 3 Linfedema
1/9
Annals of Oncology18: 639646, 2007
doi:10.1093/annonc/mdl182
Published online 3 October 2006review
A systematic review of common conservative therapies
for arm lymphoedema secondary to breast cancer
treatmentA. L. Moseley1*, C. J. Carati2 & N. B. Piller3
1School of Nursing & Midwifery, University of South
Australia, Adelaide; 2Department of Anatomy, School of Medicine,
Flinders University, Adelaide; 3Department of
Surgery & Lymphoedema Assessment Clinic, Flinders University
& Medical Centre, Adelaide, Australia
Received 10 April 2006; revised 13 June 2006; accepted 23 June
2006
Secondary arm lymphoedema is a chronic and distressing condition
which affects a significant number of
women who undergo breast cancer treatment. A number of health
professional and patient instigated
conservative therapies have been developed to help with this
condition, but their comparative benefits are not
clearly known. This systematic review undertook a broad
investigation of commonly instigated conservative
therapies for secondary arm lymphoedema including; complex
physical therapy, manual lymphatic drainage,
pneumatic pumps, oral pharmaceuticals, low level laser therapy,
compression bandaging and garments,
limb exercises and limb elevation. It was found that the more
intensive and health professional based therapies,
such as complex physical therapy, manual lymphatic drainage,
pneumatic pump and laser therapy generally
yielded the greater volume reductions, whilst self instigated
therapies such as compression garment wear,
exercises and limb elevation yielded smaller reductions. All
conservative therapies produced improvements in
subjective arm symptoms and quality of life issues, where these
were measured. Despite the identified benefits,
there is still the need for large scale, high level clinical
trials in this area.
Key words: breast cancer, conservative therapies,
lymphoedema
introduction
Currently, secondary arm lymphoedema affects approximately30% of
those who undergo breast cancer treatment [1] andresults in excess
fluid accumulation in the interstitial space,detrimental tissue
changes, limb swelling and quality of lifeissues. As this condition
will generally worsen over time [2],a number of health
professionals based and patient instigatedconservative therapies
that aim to decrease the limb swelling andits associated problems
have been developed. Two systematicreviews have investigated some
of these therapies in upper andlower limb lymphoedema, including
manual lymphaticdrainage, compression bandaging and garments [3]
andbenzopyrones [4], with both studies finding it difficult to
makedefinitive therapy recommendations. Due to the chronicity
of
secondary arm lymphoedema there is still a need to determinethe
comparative benefits of the different conservative therapiesfor
this condition. Therefore this review aimed to undertakea broad
investigation of commonly instigated conservativetherapies for this
population, including; complex physicaltherapy, manual lymphatic
drainage, pneumatic pumps, oral
pharmaceuticals, low level laser therapy, compressionbandaging
and garments, limb exercises and limb elevation.
inclusion and exclusion criteria
All study participants had to have a formal diagnosis
ofsecondary arm lymphoedema subsequent to breast cancersurgery
(total or partial mastectomy) radiotherapychemotherapy. Studies
which included participants withrecurrent cancer and/or primary
lymphoedema were excluded.
conservative therapies
This systematic review focused on therapies that are
commonly
administered to or undertaken by secondary arm
lymphoedemapatients, and included the following:Complex physical
therapy (CPT) involves 24 weeks of daily
manual lymphatic drainage (described below) followed
bycompression bandaging (administered by a health professional)and
skincare plus prescribed limb exercises undertaken by thepatient
[5]. The patient is then fitted with a compressiongarment.
Manual lymphatic drainage (MLD) uses various light
massagetechniques to encourage the removal of excess interstitial
fluid,increase lymphatic transport and soften fibrotic
induration
*Correspondence to: Ms A. L. Moseley, Institute of Womens
Health, Department of
Gynaecological Oncology, University College London, London,
UK;
E-mail: [email protected]
2006 European Society for Medical Oncology
-
7/28/2019 Control 3 Linfedema
2/9
[68]. All methods start by clearing the areas distance
oradjacent to the affected limb before moving to the limb rootthen
to its most distal section and then back to the limb rootagain.
Self/partner massage: Health professionals often teach
patients(or their significant other) a simplified version of
manuallymphatic drainage which includes clearing of the adjacent
areaand limb root followed by sweeping strokes over the limb
itself [9].Pneumatic pumps: These are single or multiple
chambered
pumps that envelop the limb and inflate and deflate at
differentcycles and pressures to encourage fluid drainage from the
distalto the proximal end of the limb [12].
Oral pharmaceuticals encompass the alpha (a) Benzopyronessuch as
the Coumarin derivatives and the gamma (c)Benzopyrones such as the
flavones and flavonols [16].Benzopyrones may help lymphoedema by
reducing vascularpermeability, protein and extracellular fluid
accumulation[16, 17], stimulating lymph contractility and flow [16,
18] andreducing protein concentration and fibrotic induration in
thetissues by stimulating proteolysis [19].
Low level laser therapyuses low intensity wave lengthsbetween
6501000 nm, either in a scanning or spot laser form.Research
suggests that laser therapy increases the rate of lymphvessel
pumping and promotes lymph vessel regeneration [13],reduces pain
[14] and softens both fibrous tissue and surgicalscarring [15].
Compression bandaging consists of a gauze sleeve whichprotects
the skin, soft cotton wrap or high density foam and23 layers of
short-stretch bandaging. Compression helps todecrease the amount of
interstitial fluid formation, preventlymph back flow and enhance
the muscle pump by providinga relatively inelastic barrier for the
muscle to work against [10].
Compression garments have a similar mode of action ascompression
bandaging and are designed to be graduated, with
the greatest compression being at the distal end of the limb
andthe least amount being at the proximal end.
Limb exercises can be progressive, resistive or sequential
innature and are recommended as a way of varying total
tissuepressure to encourage lymphatic drainage and for
improvinglimb range of movement and strength [11].
Limb elevation reduces capillary exudation in to the tissuesand
promotes lymphatic return. It is considered most useful inthe
earlier (fluid) stage of lymphoedema [5].
literature search
The literature search was limited to English, with the
followingdatabases searched; Cumulative Index to Nursing &
AlliedHealth Literature (Cinahl), Medline, Academic
ResearchPeriodicals, PubMed Clinical Queries
(includingComplementary Medicine), CANCERLIT, EBM Reviews Cochrane
Central Register of Controlled Trials, CochraneDatabase of
Systematic Reviews (CDSR), American Collegeof Physicians (ACP)
Journal Club, Database of Abstracts ofReviews of Effects (DARE),
PREMEDLINE, Australian MedicalIndex, Physiotherapy Evidence
Database (PEDro) and theNational Guidelines Clearing House.
The general terms used for all these search engines were
asfollows:
Secondary lymphoedema/lymphedema Arm swelling/oedema/edema
These were then combined with the following terms:
Complex/complete, physical/decongestive therapy Manual lymphatic
drainage/lymphatic massage/lymphatic
drainage Support hosiery Compression garment/sleeve Compression
bandaging/bandage Pneumatic/compression/intermittent pump therapy
Exercise/physical therapy Elevation Laser/low level laser/laser
therapy
In addition, health institution websites and online
lymphaticsocieties were also searched. The biennial congress
proceedingsof The International Society of Lymphology (19772004)
andthe Australian Lymphoedema Association (20002004) were
searched by hand. Primary authors were contacted
whenpublications were difficult to source. The reference section
ofeach article was also checked for relevant articles.
data extraction and quality assessment
Endnote 7 was used as the data extraction tool. Once thedata had
been extracted and recorded, the quality of eachstudy was assessed
and given a rating. The Quality ScaleAssessment tools used in this
review were based upon a tooldeveloped by Mulrow and Oxman (1996)
[20], with one toolbeing developed and used for the review of
randomised trials(scored out of 10) and the other for
non-randomised trials
(scored out of eight). The data extraction and rating
wasundertaken by A. Moseley, with the process checked byN. Piller
and C. Carati. The quality rating and level ofevidence [21] for
each reviewed study is presented in Table 1.
analysis
This review included studies performed in the
randomizedcontrolled, parallel and cross-over format plus case
control andcohort studies. Case studies and anecdotal evidence were
notreviewed. Due to treatment and data heterogeneity, a
meta-analysis could not be performed. Therefore, only a narrative
ofthe different conservative therapies for secondary arm
lymphedema is presented. For ease of comparison, anapproximate
oedema reduction (%) has been calculated ineach case where the limb
volume reduction is presented inmilliliters (ml).
results
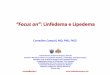
The average percentage volume change at end of trial achievedby
each reviewed conservative therapy is displayed in Figure 1.This
demonstrates the magnitude of the reduction (average)that can be
achieved by the different conservative therapies.
review Annals of Oncology
640 | Moseley et al. Volume 18 | No. 4 |April 2007
-
7/28/2019 Control 3 Linfedema
3/9
complex physical therapy (CPT)
Five studies reviewed investigated standard CPT over a
varyingtreatment period of 8 days to 3 months [9, 2225].
Participantnumbers ranged from 1678, with some studies having no
statedexclusion criteria [22, 23] and others having a poorly
statedcriterion [24, 25]. The reductions achieved from the
fivestudies varied from 298652 ml (18.766%), with three
studiesdemonstrating additional volume reductions over 612
months
follow up [9, 22, 25]. Two studies measured subjectivesymptoms,
with one showing a reduction in pain [24] and theother in
tightness, heaviness, pins and needles, cramps andtension [9].
One study investigated standard CPT (n = 13) in comparisonwith
CPT plus 30 min of intermittent pump (50 mmHg)therapy (n = 14)
[26]. After 10 days CPT alone yielded a3.1% mean volume reduction
whilst the CPT + pneumaticgroup had a statistically greater
reduction of 7.9%. Althougha reduction in symptoms was reported, it
was not stated whatsymptoms were actually measured. The
follow-upmeasurements over one and two months demonstrated
acontinuing decrease in percentage volume in both treatment
groups (3.6% and 9.6% at 2 months). Two studies investigatedCPT
in combination with intermittent pump therapy. Thefirst study [27]
involved 1 hour of intermittent pump(4070 mmHg) therapy
incorporated into the CPT regime(n = 188), with this regime
yielding statistically significantpercentage reductions in all
grades of lymphoedemas (gradeIIII, 43.419.3 %) after 5 weeks of
treatment. The second studyinvolved a regime of CPT with a pump
of
-
7/28/2019 Control 3 Linfedema
4/9
treatments incorporated into the CPT regime, includingmechanical
plus manual massage, hand grip exercises, thewearing of a
compression garment and the addition of hotcompresses during one
treatment phase [29]. All treatmentcombinations yielded similar
actual oedema reductions in therange of 8.513%.
All the reviewed studies demonstrated that a reduction inlimb
volume and/or percentage oedema can be achieved with
standard CPT, CPT plus pump therapy and a combination
oftherapies, with five studies [9, 22, 25, 26, 28] demonstratinga
continued volume reduction at follow up (range 112months). The
three studies [9, 24, 26] which measuredsubjective symptoms
demonstrated that these improved afterthe CPT regime, unfortunately
none of these studies reportwhether these improvements were
sustained at the follow upperiods. The study by Piller et al.
(1996) also demonstrated thatvolume and subjective symptom
reductions could be achievedwhen patients and their partners were
taught how to applya regime of lymphatic massage and compression
bandagingthemselves [9]. The optimal treatment period for
CPTappears to be 1 month, however, two studies [22, 29]
achieved
a volume reduction at the end of 78 days of treatment.
manual lymphatic drainage (MLD)
Two studies investigated the effect of MLD alone. These
twostudies [30, 31] involved 1217 participants who received MLDand
who experienced a volume reduction of 104156 ml(810%), with one
study reporting that the volume reductionwas maintained at 6-months
follow up [31]. The other studyreported reductions in heaviness and
tension, but did not statethe inclusion/exclusion criteria or the
length and frequency ofMLD [30]. Two studies investigated MLD in
comparison toanother treatment modality. The first of these studies
useda cross-over design to investigated a phase of MLD and self
massage (n = 27), each over a 3-week period [32]. Resultsshowed
that MLD produced a statistically significant reductionof 71 ml and
improvements in subjective heaviness, fullness andbursting whilst
the self massage resulted in a non significantreduction of 30 mls.
The second randomized study investigatedMLD (n = 20) in comparison
to a control group whoundertook education, wearing a compression
sleeve and limbexercises (n = 20) [33]. After 2 weeks the control
group actuallyhad a greater percentage reduction in absolute oedema
(60%) incomparison to the MLD group (48%). Both groups
equallyexperienced a reduction in the symptoms of heaviness
andtightness, whilst the control group also had a reduction
inreported discomfort. The reduction in absolute oedema (66%)
was maintained at 12-months follow up (pooled data).Four studies
investigated the effect of MLD in combination
with compression (bandaging or garment). All four studies hada
clearly stated inclusion/exclusion criterion, with the first
twostudies investigating MLD plus compression bandaging. Thesetwo
studies [34, 35] involved 1824 women who received MLDplus
compression bandaging over 1 week to 1 month. After 1week there was
a significant volume reduction of 47 ml (11% inoedema) [34], whilst
over 1 month the reduction was 260 ml(46.1%), with significant
improvements in tension, heavinessand pain [35]. The third study
investigated the effect of
a compression (3040 mmHg) sleeve worn for 2 weeks followedby 2
weeks of additional MLD (n = 12) [36]. Wearing the sleevealone
resulted in a significant volume reduction of 49 ml (7%),with the
addition of MLD resulting in a significant reduction of75 ml (15%).
Both phases also significantly improved armtension and heaviness.
The last study investigated MLD incombination with a compression
garment or bandaging oncea week for 12 weeks [37]. Both treatment
groups experienced
significant reductions in oedema of 84% and 78% respectively.One
study compared MLD and pneumatic pump therapy
[38], with one group receiving 1 hour of MLD over 43 sessions(n
= 27) and the other receiving 0.5 h of pump therapy(40 mmHg)
followed by 0.5 h of MLD over 25 sessions (n = 62).Results showed
that the MLD alone and when combinedwith pneumatic pump therapy
yielded similar reductions inoedema volume (40% and 45%
respectively), however, therewere no accompanying statistical
values so significance is notknown. The follow up period in this
study (1424 months)demonstrated an oedema volume increase of 33% in
those whounderwent no further treatment, whilst those who
underwentregular treatment (type not stated) experienced a
slight
reduction (1%) in oedema volume.The volume reductions achieved
by MLD alone varied from104156 ml, with the greatest percentage
reduction being 48%[33]. Larger reductions were achieved from MLD
incombination with compression, which varied from 47260 ml(784%),
with these studies demonstrating that either form ofcompression
(garment or bandaging) could be effectively usedin combination with
MLD. MLD in combination withpneumatic pump therapy was also shown
to be effective [38].The majority of volume reductions were
achieved after a 4 weektreatment period, although volume reductions
were also seento occur over 2 weeks of treatment [31, 33, 36]. Only
threeof the reviewed studies included a follow up period
whichdemonstrated that the initial volume reductions were
maintained [31, 33, 38]. The overall lack of follow up in
thesestudies makes it difficult to formulate strong conclusions on
thelong term benefits of MLD ( bandaging).
pneumatic pump therapy
Five studies were reviewed which investigated the effect
ofpneumatic pump therapy. The first was a poorly reported
studywhich involved a group that received a combination of MLD(0.5
h) and pump therapy (0.5 h) over 25 sessions (n = 62) andanother
that received 6 hours of sequential (40 mmHg) pumptherapy (only)
over 5 days (n = 14) [38]. Both groupsexperienced identical oedema
volume reductions (45%), with
this reduction being achieved over a shorter treatment
duration(5 days) in the pump only group. However, considering
thisgroup had a sample size of 14, it is hard to determine
whetherthis volume reduction is a true reflection of what can
beachieved with this form of sequential (40 mmHg) pump. Szubaet al.
(2002) performed two randomised studies whichinvestigated the use
of a four-chambered, sequential pump as anadjunct therapy [39]. The
first study compared 10 days ofcomplex physical therapy (CPT) alone
(n = 11) and incombination with 30 min of 3040 mmHg pump therapy(n
= 12). Results showed that the CPT plus pump therapy
review Annals of Oncology
642 | Moseley et al. Volume 18 | No. 4 |April 2007
-
7/28/2019 Control 3 Linfedema
5/9
resulted in a greater and significant limb volume reduction
incomparison to CPT alone (45.3% versus 26%
respectively).Interestingly, the CPT plus pump therapy reduction
was notmaintained at 1 month follow up (increase of 15%), whilst
theCPT alone reduction was maintained. The second studyinvestigated
a 1 month phase of arm self maintenance includingself massage and
compression garment wear, followed by aphase of applying 1 hour of
pump therapy for a further 1 month
period (n = 25). The self maintenance phase resulted in anarm
volume increase of 32.7 ml (3.3%), with the addition ofthe 1 h of
pump therapy resulting in a statistically significantreduction of
89.5 ml (9.0%). Some participants continuedusing the pump an
average of four times a week for 6 months,with 19 participants
having an additional reduction in limbvolume of 29.1 ml (3.0%) and
five having an increase of 35 ml(3.5%). Why this sub-group of
participants had a worseningin limb volume was not explored.
One study investigated 2 h of pump therapy (4060 mmHg)5 days a
week for 2 weeks [36]. After this time there wasa non significant
reduction in arm volume (28 ml; 7%) andreported tension and
heaviness. One study investigated the
wearing of a compression (3040 mmHg) garment for 6 monthsthen 6
h of pump therapy (3560 mmHg) over 10 sessionsfollowed by the
continued wear of the compression garment(n = 54) [40]. Results
showed a significant 8% reduction afterwearing the compression
garment and an additional 9%significant reduction after the pump
therapy (with theassumption that the total edema reduction at this
time pointwas 17%). A 6-month follow up demonstrated a
19.8%reduction in those who continued to wear the
compressiongarment. The last study investigated 23 h of
sequential(100150 mmHg) pump therapy, three times a day for 3
days(n = 25) [41]. After 3 days the percentage reduction rangedfrom
1244% (statistical values not stated). After trial cessation,2 h of
maintenance therapy was applied onefour times a week
over the following 6 months. Follow up at this time showed
thatthe initial treatment reductions had been maintained.
However,it was not reported whether the maintenance of limb
volumewas the result of one or four sessions of treatment per
week.
Two studies [38, 41] demonstrated that volume reductionscould be
achieved from pump therapy alone, although the highpressures
(100150 mmHg) used by Zelikovski et al. (1980) [41]are above the 60
mmHg of pressure normally recommended forthe treatment of
lymphoedematous limbs [42]. Three of thereviewed studies [36, 38,
40] demonstrated that better results involume reduction were
achieved when the pneumatic pump wascombined with other therapies,
including; manual lymphaticdrainage, compression garments and self
massage. Three studies
[38, 40, 41] also demonstrated that continuing the pumptherapy
or wearing a compression garment were beneficial inmaintaining the
initial volume reductions.
oral pharmaceuticals
Five studies were reviewed that investigated the effect of
oralpharmaceuticals. Two studies investigated Coumarin [43,
44],with the first study investigating two dosages; 90 mg (n =
23)and 135 mg (n = 30) over 12 months [43]. At trial end,
bothgroups experienced a similar reduction in percentage limb
volume (14.9% and 13.2% respectively) and reductions
inheaviness, pain and cramps. The second study used a cross
overdesign to investigate a 6-month phase of Coumarin (400 mg)and a
6 month phase of a placebo (n = 138) [44]. Resultsdemonstrated a
volume increase (and therefore worsening) of58 ml (6%) in the
treatment phase and 21 ml (2.1%) in theplacebo phase. Despite this,
participants reportedimprovements in arm swelling, pressure,
tightness, heaviness
and mobility. The third study investigated Daflon (Diosminplus
Hesperidin 1g, n = 46) or placebo (n = 48) over 6 months[45]. After
this period the treatment group experienced a 7%volume reduction
whilst the placebo group experienceda volume increase of 10%. Both
groups experienced a significantreduction in reported discomfort,
with the treatment group alsohaving a significant reduction in
heaviness.
The fourth study investigated three capsules of
Cyclo-Fort(Ruscus Aculeatus and Hesperidin Methyl Chalcone)
threetimes a day (n = 27) compared to placebo (n = 30) over
3months, with the addition of MLD (2 week) in the first monthof the
trial [46]. After the first month both the treatment andplacebo
groups experienced volume reductions of 1.2% and
0.5% respectively. By 3 months the treatment (Cyclo-Fort)group
had an overall volume reduction of 12.9% whilst theplacebo group
had an increase of 2.5%. Both groupsexperienced improvements in
heaviness and limb mobility, withthese being significant in the
Cyclo-Fort group. The last studyused a cross over design to
investigate a 6 month phase of 56Benzo-a-pyrone (200 mg) and
placebo (n = 31) [47]. Resultsdemonstrated a volume reduction of
840 ml (35.6%) in thetreatment phase, with this reduction being
significant incomparison to the control phase in which the limb
increased involume by 490 ml (41.6%). A 1-month follow up
demonstratedan additional decrease of 3.3% in oedema (treatment
phase) andan additional increase of 1.2% (placebo phase).
The two studies which investigated Coumarin had
conflicting results, with one showing a decrease in armvolume
(dosage 90 mg, 135 mg) [43] and the other showingan increase in
volume (dosage 400 mg) [44]. As neither studyhad a follow up period
it is not known whether the initialvolume reduction or increase
would have continued. The otherreviewed studies [4547] demonstrated
that varying volumereductions and subjective improvements could be
obtainedfrom oral pharmaceuticals such as Daflon (1000 mg)
andCyclo-fort, with the greatest limb reduction (840 ml,
35.6%)being obtained from the 56 Benzo-a-pyrone (200 mg) [47].It is
also important to note that two studies [43, 47]
reportedgastrointestinal upsets in 13.7% and 22.6% of
participants.
low level laser therapy
Three studies were reviewed which investigated concentrated
orscanning laser therapy. The first study was a
double-blinded,randomised controlled trial involving one group
which receivedtwo cycles of active laser to the axilla three times
a week for 3weeks (n = 37) and another group who received one cycle
ofplacebo laser and one cycle of active laser (n = 27) over the
sametime periods [48]. At trial end there were volume reductions
inall phases: placebo; 35 ml (3.5%), one cycle; 15 ml (1.5%),two
cycles; 25 ml (2.5%). A 3-month follow up demonstrated
Annals of Oncology review
Volume 18 | No. 4 | April 2007 doi:10.1093/annonc/mdl182 |
643
-
7/28/2019 Control 3 Linfedema
6/9
a volume increase of 30 ml (3.0%) in those who receivedplacebo
and volume reductions in the one cycle (10 ml 1.0%)and two cycle
(90 ml 9.0%) phases. The two cycle phase alsoresulted in a
significant reduction in the mean perceptual scoreand improvements
in quality of life parameters. The secondstudy investigated 30 min
of scanning laser, twice a week for6 weeks and then once a week for
a further 4 weeks (n = 10)[49]. This resulted in a volume reduction
of 19.3% and
progressive improvements in subjective symptoms. A followup
study of these participants (n = 8) [50] demonstratedthat there
were continued volume reductions of 397 ml(40%) at 6 months and 288
ml (29%) at 36 months,with subjective symptoms returning to
pre-treatment levelsby the 36-month mark.
These three studies demonstrate that benefits includingvolume
reduction, improved subjective symptoms and qualityof life can be
derived from either concentrated or scanning lasertherapy. The best
results in the Carati et al. (2003) study [48]were seen at 3 months
post treatment, which suggests that theremaybe ongoing benefits
from laser therapy. This is supportedby the Piller and Thelander
(1998) study [50] (albeit with
a much smaller sample size), which found that there
werecontinued reductions in arm volume and reported armtightness 6
months after treatment cessation.
compression
Four studies investigated the effect of compression (garment
orbandaging) alone. Two studies [30, 35] which involved
3555participants investigated compression bandaging. Thesestudies
demonstrated a volume reduction of 38 ml (7%) [30]and 20 ml (4%
oedema) [35] respectively and significantimprovements in arm
heaviness and tension. Two studiesinvestigated the effect of a 3040
mmHg compression garment.
The first study involved 12 participants who wore the
garmentover a 2-week period [36], after which time there wasa
significant volume reduction of 49 ml (5.0%) andimprovements in
tension and heaviness. The second studyinvolved participants (n =
26) wearing the compressiongarment over a 6-month period [40].
Results showed an 8%reduction in actual oedema, however, at the
6-month pointonly 12 women remained in the study. Two studies
investigatedthe effect of wearing a compression garment in
combinationwith other activities. One study [33] demonstrated that
after3 months of limb exercise and compression wear (n = 22)there
was a 60% reduction in absolute oedema, with the otherstudy showing
a 243 ml (24.4%) volume reduction after
4 weeks of self massage combined with compression wear
[51].Neither study reported statistical values, so the significance
ofthese volume reductions are not known.
Four of the reviewed studies [30, 35, 36, 40] demonstratedthat
modest volume reductions of 2049 ml (48%) andsignificant
improvements in heaviness and tension could beachieved when wearing
compression (bandaging or garment)alone. However, none of these
studies included a follow upperiod, so the ongoing effects of
compression cannot bedetermined. Two studies [33, 51] demonstrated
that greatervolume reductions of 243 ml (24.4%) and 60% could
be
achieved when the wearing of a compression garment wascombined
with limb exercise or self massage.
exercise
Five studies were reviewed which investigated a variety
ofexercise regimes. The first study investigated a 10-minute
armexercise and deep breathing regime (n = 38) [52] which
resulted
in an arm volume reduction of 52 ml (5.8%) and improvementsin
heaviness and tension, with some reductions maintained over24 h and
1 week follow up. After 1 month of performing thisregime (n = 24)
there was a volume reduction of 101 ml (9%)and significant
improvements in heaviness and perceived limbsize. Two studies
investigated the effects of 4045 min ofhydrotherapy [11, 53], with
neither study stating the exclusioncriteria. The first was a
randomised study which involveda control group (n = 8) and a
hydrotherapy exercise group (n =8) [53]. After 4 weeks there was a
volume reduction of 48 ml(4.8%) in the hydrotherapy group, with
continued reductionsat 3 and 6 weeks follow up (30 ml 2.9% and 86
ml 8.6%respectively). This in comparison to the control group,
which
increased in limb volume. The exercise group also hadreductions
in reported aching, heaviness, tightness, limbswelling, stiffness
and heat intolerance. The second studyinvestigated hydrotherapy
performed by seven participants intwo different pool temperatures
(28 C; 82 F and 34 C; 93 F)[11]. After the first session (28 C)
there was a decrease in armvolume of 32 ml (12% oedema change),
whilst after the secondsession (34 C) there was a slight increase
in volume of 2 ml(0.7% change). Subjective symptoms remained
unchanged afterboth pool sessions. One study investigated a 30 min
regime ofinstructed deep breathing, self massage and sequential
limbexercises (n = 7) [54]. Directly after performing the regime
therewas a slight increase in arm volume (12 ml, P= n.s.), with a
netdecrease (12 ml, P= n.s.) experienced 20 minutes post
regime.
Despite the minimal volume reduction, the group
reportedimprovements in arm range of movement, subjective
limbtemperature difference, heaviness and tightness.
Two studies investigated the effect of resistive arm
exercises.The first of these studies involved a regime of shoulder
flexionand abduction and elbow extension and flexion using 0.5
kghand weights, performed firstly with no compression garmentand
secondly when wearing a compression garment (n = 23)[11]. Results
showed an initial increase in arm volume afterperforming the
regime, plus or minus garment wear (12 ml,0.5% and 10 ml, 0.3%
respectively). However, at the 24 h followup the volume increases
had been reversed, with both phasesdemonstrating a volume reduction
of 15 ml (0.71.0%) at this
time point. Reported tension and heaviness remainedunchanged in
both phases, however, when the regime wasperformed without a
compression garment there wasa significant increase in reported
physical exertion. The secondstudy investigated latissimus dorsi,
bicep and tricep exerciseswith weights and the wearing of a
compression garmentundertaken three times a week for 8 weeks (n =
7) [55]. Thisresulted in a limb volume reduction of 2% plus
significantimprovements in physical functioning, general health and
vitality.
The five studies reviewed demonstrated that exercise regimescan
have a varying impact upon limb volume, ranging from
review Annals of Oncology
644 | Moseley et al. Volume 18 | No. 4 |April 2007
-
7/28/2019 Control 3 Linfedema
7/9
12101 ml (0.49%), with three studies demonstratingimprovements
in subjective symptoms [5254]. Sustainedvolume reductions were also
seen to occur 24 h to 6 weeks afterexercise program cessation [11,
52, 53]. The hydrotherapy study[11] suggests that this form of
exercise is best undertaken ina pool temperature of 28 C (82
F).
elevation
Only one study was reviewed that investigated the effects oflimb
elevation [56]. It involved 33 women who elevated theirarm at 80
angle over a 5-h period. At the end of this time therewas a
significant 3.1% reduction in arm volume. Subjectivesymptoms and
adverse effects were not recorded, so it is notknown how well this
regime was tolerated.
discussion
In recent times, sentinel lymph node biopsy (SLNB) has becomea
more common procedure in breast cancer surgery, resulting inless
arm morbidity [57], including lymphoedema [58].
However, there is still the possibility of developing
armlymphoedema after SLNB, especially if the sentinel node
islocated at the level of the axillary vein and lymphatic
collectors[59] and if SLNB is combined with axillary radiotherapy
[60].Although the number of women developing arm lymphoedemamaybe
reduced as a consequence of SLNB, it is still important toknow the
benefits of conservative therapies for the proportion ofwomen who
do go on to develop this condition after breastcancer
treatment.
The current review investigated conservative therapies forarm
lymphoedema that can essentially be divided into
intensivetreatments administered by trained health professionals
andlimb maintenance therapies undertaken by the patient.
Asdemonstrated by Figure 1, treatments that are predominantly
administered by health professionals, such as complex
physicaltherapy, manual lymphatic drainage (with and
withoutcompression), laser therapy and pneumatic pump
therapygenerally yielded the larger percentage volume
reductions.Maintenance therapies (normally undertaken by the
patient),such as wearing a compression garment, limb
exercises,elevation and self massage generally yielded smaller
percentagereductions. There is some research to suggest that
undertakingtherapies such as arm rehabilitation and exercise may
preventthe onset of lymphoedema [61], but further research is
requiredto determine the true benefits of such programs.
Although those therapies which would be categorised as
selfmaintenance yielded smaller volume reductions, this review
has
demonstrated that they are more beneficial than doing nothingat
all for the lymphoedematous limb. This indicates that suchtherapies
maybe useful when health professional based therapiesare not
accessible or economically viable for the patient. Thereview also
demonstrated the positive impact upon subjectivelimb complaints and
quality of life issues, indicating that theseconservative therapies
can be initiated by the health professionalor patient with the
anticipation of some benefit. Follow upperiods (when incorporated)
indicated that some form ofcontinuing therapy (intensive or patient
based) needed to beundertaken to maintain the initial volume
reductions, which
demonstrates the chronic nature of this condition. Despitethe
range of positive outcomes identified in this review, theevidence
to support them is, in some instances, poor. Therefore,there is
still a need for large scale, high level clinical trials inthis
area.
references
1. Williams A, Franks PJ, Moffatt CJ. Lymphoedema: estimating
the size of the
problem. Pall Med 2005; 19 (4): 300313.
2. Casley-Smith JR, Casley-Smith JR. Volume alterations in
lymphoedema;
untreated, and after complex therapy (C.P.T), benzo-pyrones, or
both.
Lymphology 1994; 27 (suppl): 627631.
3. Badger C, Preston N, Seers K, Mortimer P. Physical therapies
for reducing and
controlling lymphoedema of the limbs. The Cochrane Database of
Systematic
Reviews 2004; Issue 4.
4. Badger C, Preston N, Seers K, Mortimer P. Benzo-pyrones for
reducing and
controlling lymphoedema of the limbs. The Cochrane Database of
Systematic
Reviews 2003; Issue 4.
5. Bernas MJ, Witte CL, Witte MH. The diagnosis and treatment of
peripheral
lymphedema. Draft revision of the 1995 Consensus Document of
the
International Society of Lymphology Executive Committee for
Discussion at the
September 3 76, 2001, XVIII International Congress of Lymphology
in Genoa,
Italy. Lymphology 2001; 34: 8491.
6. Casley-Smith JR, Casley-Smith JR. Modern Treatment for
Lymphoedema
(5th Edn), Australia: Terrace Printing, 1997, 138139.
7. Kasseroller RG. The Vodder School. The Vodder Method. Cancer
1998; 83
(suppl): 28402842.
8. Foldi M, Foldi E, Kubrik S. Textbook of Lymphology for
Physicians and
Lymphedema Therapists, Germany: Elsevier, 2003, pp 496497.
9. Piller NB, Packer R, Coffee J, Swagemakers S. Accepting
responsibility for health
management: Partner training as an effective means of managing
chronic
lymphoedema. Progress in Lymphology XV, 1996; 266269.
10. Yasuhara H, Shigematsu H, Muto T. A study of the advantages
of elastic
stockings for leg lymphoedema. Int Angiology 1996; 15:
272277.
11. Johansson K, Tibe K, Kanne L, Skantz H. Controlled physical
training for arm
lymphedma patients. Lymphology 2004; 37 (suppl): 3739.
12. Brenan MJ, Miller LT. Overview of treatment options and
review of the currentrole and use of compression, intermittent
pumps and exercise in the
management of lymphedema. Cancer 1998; 83 (suppl 12B):
28212827.
13. Lievens P. The effect of a combined HeNe and I.R. laser
treatment on the
regeneration of the lymphatic system during the process of wound
healing.
Lasers Med Sci 1991; 6(193): 193199.
14. Nakaji S, Shiroto C, Yodono M et al. Retrospective study of
adjunctive diode laser
therapy for pain attenuation in 662 patients: detailed analysis
by questionnaire.
Photomedicine, Laser Surg 2005; 23(1): 6065.
15. Nouri K, Jimenez G, Harrison-Balestra C, Elgert G. 545-nm
pulsed dye laser in
the treatment of surgical scarring starting on the suture
removal day. Dermatol
Surg 2003; 29: 6573.
16. Ramlett AA. Pharmacologic aspects of phlebotropic drug in
CVI-associated
edema. Angiology 2000; 51(1): 1923.
17. Roztocil K, Pretovsky I, Olivia I. The effects of
hydroethylrutosides on capillary
filtration rate in the lower limbs of man. Eur J Clin Pharm
1993; 11: 435438.18. Clement DL. Management of venous edema:
Insights from an international task
force. Angiology 2000; 51(1): 1317.
19. Knight KR, Khazanchi RK, Pederson WC et al. Coumarin and
7-hydroxycoumarin
treatment of canine obstructive lymphoedema. Clinic Sci (London)
1989; 77(1):
6976.
20. Mulrow C, Oxman A. How to Conduct a Cochrane Systematic
Review (3rd Edn),
UK: BMJ Publishing Group, 1996.
21. NHMRC. Levels of Evidence. 2000.
22. Szuba A, Cooke JP, Yousuf S, Rockson SG. Decongestive
lymphatic therapy for
patients with cancer-related or primary lymphedema. Amer J Med
2000; 109 (4):
296300.
Annals of Oncology review
Volume 18 | No. 4 | April 2007 doi:10.1093/annonc/mdl182 |
645
-
7/28/2019 Control 3 Linfedema
8/9
23. Boris M, Weindorf S, Lasinski B. Lymphedema reduction by
noninvasive complex
lymphedema therapy. Oncology 1994; 8 (9): 95106.
24. Carroll D, Rose K. Treatment leads to significant
improvement. Effect of
conservative treatment on pain in lymphoedema. Prof Nurse
1992;
8 (1): 3236.
25. Casley-Smith JR, Casley-Smith JR. Modern treatment of
lymphoedema I.
Complex physical therapy: the first 200 Australian limbs.
Austral J Derm 1992;
33: 6168.
26. Szolnoky G, Lakatos B, Keskeny T, Dobozy A. Advantage of
combined
decongestive lymphatic therapy over manual lymph drainage: A
pilot study.Lymphology 2002; 35 (suppl 1): 277282.
27. Wozniewski M, Jasinski R, Pilch U, Dabrowska G. Complex
physical therapy for
lymphoedema of the limbs. Physiotherapy 2001; 87(5): 252256.
28. Bunce IH, Mirolo BR, Hennessy JM, Ward LC, Jones LC.
Post-mastectomy
lymphoedema treatment and measurement. Med J Aus 1994; 161:
125127.
29. Swedborg I. Effectiveness of combined methods of
physiotherapy for post-
mastectomy lymphoedema. Scand J Rehab Med 1980; 12: 7785.
30. Korpon MI, Vacariu G, Schneider B, Fialka Moser V. Effects
of compression
therapy in patients with lymphedema after breast cancer surgery.
Annual
Congresses of the American College of Phlebology August 2003;
San Diego,
California.
31. Piller NB, Swedborg I, Wilking N, Jensen G. Short-term
manual lymph drainage
treatment and maintenance therapy for post-mastectomy
lymphoedema.
Lymphology 1994; 27 (suppl): 589592.
32. Williams AF, Vadgama A, Franks PJ, Mortimer PS. A randomized
controlled
cross-over study of manual lymphatic drainage therapy in women
with breast
cancer-related lymphedema. Eur J Cancer Care 2002; 11(5):
254263.
33. Andersen L, Hojris I, Erlandsen, M, Andersen J. Treatment of
breast-cancer-
related lymphedema with or without manual lymphatic drainage. A
randomized
study. Acta Oncologica 2000; 39 (3): 399405.
34. McNeely ML, Magee DL, Lees AL et al. The addition of manual
lymphatic
drainage to compression therapy for breast cancer related
lymphedema: A
randomized controlled trial. Breast Cancer Treat Res 2004; 86
(2): 96105.
35. Johansson K, Albertsson M, Ingvar C, Ekdahl C. Effects of
compression
bandaging with or without manual lymph drainage treatment in
patients with
postoperative arm lymphedema. Lymphology 1999; 32: 103110.
36. Johansson K, Lie E, Ekdahl C, Lindfeldt J. A randomized
study comparing manual
lymph drainage with sequential pneumatic compression for
treatment of
postoperative arm lymphedema. Lymphology 1998; 31: 5664.37. Ang
N, Saraswathi N, Chan H. Outcome study on the effectiveness of
two
different modified lymphoedema management protocols for
post-mastectomy
patients: A pilot study. IVth Australasian Lymphology
Association Conference
Proceedings 2003; 717.
38. Dubois F. Comparison between applying manual lymphatic
drainage only,
applying sequential pressotherapy by Lympha-Press itself, and
the combination
of using both applications. 2004;
http://www.lympha-press.com/pdf/
phystreatment.pdf.
39. Szuba A, Achalu R, Rockson SG. Decongestive lymphatic
therapy for patients
with breast carcinoma-associated lymphedema. A randomized,
prospective study
of a role for adjunctive intermittent pneumatic compression.
Cancer Dec 2002;
95(11): 22602267.
40. Swedborg I. Effects of treatment with an elastic sleeve and
intermittent
pneumatic compression in post-mastectomy patients with
lymphoedema of the
arm. Scand J Rehab Med 1984; 16: 3541.
41. Zelikovski A, Melamed I, Kott I et al. The Lymphapress A new
pneumatic
device for the treatment of lymphedema: Clinical trial and
results. Folia
Angiologica 1980; XXVVIII: 165169.
42. Eliska O, Eliskova M. Are peripheral lymphatics damaged by
high pressure
manual massage? Lymphology 1995; 29(1): 2130.
43. Burgos A, Alcaide A, Alcoba C et al. Comparative study of
the clinical efficacy of
two different coumarin dosages in the management of arm
lymphedema after
treatment for breast cancer. Lymphology 1999; 32: 310.
44. Loprinzi CL, Kugler JW, Sloan JA et al. Lack of effect of
Coumarin in women with
lymphedema after treatment for breast cancer. New Eng J Med
1999; 340 (5):346350.
45. Pecking AP, Fevrier B, Wargon C, Pillion G. Efficacy of
Daflon 500 mg in the
treatment of lymphedema (Secondary to conventional therapy of
breast cancer).
Angiology 1997; 48 (1): 9398.
46. Cluzan RV, Alliot F, Ghabboun S, Pascot M. Treatment of
secondary lymphedema
of the upper limb with Cyclo 3 Fort. Lymphology 1996; 29:
2935.
47. Casley-Smith JR, Morgan RG, Piller NB. Treatment of
lymphedema of the arms and
legs with 5,6-BENZO-[a]-PYRONE. New Eng J Med 1993; 329 (16):
11581163.
48. Carati CJ, Anderson SN, Gannon BJ, Piller NB. Treatment of
postmastectomy
lymphedema with low-level laser therapy. Cancer 2003; 98 (6):
11141122.
49. Piller NB, Thelander A. Low level laser therapy: A cost
effective treatment to
reduce post mastectomy lymphoedema. Lymphology 1996; 29 (suppl
1):
297300.
50. Piller NB, Thelander A. Treatment of chronic postmastectomy
lymphedema with
low level laser therapy: a 2.5 year follow-up. Lymphology 1998;
31 (2): 7486.
51. Hornsby R. The use of compression to treat lymphoedema. Prof
Nurse 1995; 11
(2): 127128.
52. Moseley A, Piller N, Carati C. The effect of gentle arm
exercise and deep
breathing on secondary arm lymphoedema. Lympholoy 2005; 38 (3):
136145.
53. Box R, Marnes T, Robertson V. Aquatic physiotherapy and
breast cancer related
lymphoedema. 5th Australasian Lymphology Association Conference
Proceedings
2004; 4749.
54. Buckley G, Piller N, Moseley A. Can exercise improve
lympatic flow? A pilot
trial of the objective measurement of fluid movement in subjects
with mild
secondary lymphoedema. 5th Australasian Lymphology Association
Conference
Proceedings 2004; 3742.
55. McKenzie DC, Kalda AL. Effect of upper extremity exercise on
secondary
lymphedema in breast cancer patients: A pilot study. J Clin
Oncol 2003; 21 (3):
463466.56. Swedborg I, Norrefalk J, Piller NB, Asard C.
Lymphoedema post-mastectomy:
is elevation alone an effective treatment? Scand J Rehab Med
1993; 25: 7982.
57. Purushotham AD, Upponi S, Klevesath MB et al. Morbidity
after sentinel lymph
node biopsy in primary breast cancer: results from a randomized
controlled trial.
J Clin Oncol 2005; 23 (19): 43124321.
58. Schulze T, Mucke J, Markwardt J et al. Long-term morbidity
of patients with early
breast cancer after sentinel lymph node biopsy compared to
axillary lymph node
dissection. J Surg Oncol 2006; 93 (2): 109119.
59. Petrek JA, Pressman PI, Smith RA. Lymphedema: current issues
in research and
management. CA: Cancer J Clinic 2000; 50 (5): 292307.
60. Erickson VS, Pearson ML, Ganz PA et al. Arm edema in breast
cancer patients.
J Natl Cancer Inst 2001; 93 (2): 96111.
61. Box RC, Reul-Hirche HM, Bullock-Saxton JE, Furnival CM.
Physiotherapy after
breast cancer surgery: results of a randomised controlled study
to minimise
lymphoedema. Breast Canc Res Treat 2002; 75 (1): 5164.
review Annals of Oncology
646 | Moseley et al. Volume 18 | No. 4 |April 2007
http://www.lympha-press.com/pdf/phystreatment.pdfhttp://www.lympha-press.com/pdf/phystreatment.pdfhttp://www.lympha-press.com/pdf/phystreatment.pdfhttp://www.lympha-press.com/pdf/phystreatment.pdf
-
7/28/2019 Control 3 Linfedema
9/9
Reproducedwithpermissionof thecopyrightowner. Further
reproductionprohibitedwithoutpermission.