Embed Size (px)
Citation preview
Contributors: Michael Power, PhD, Emily Kahn, PhD, Jennifer
Williams, MSN, MPH, Denise Jamieson, MD, MPH, Kitty MacFarlane, CNM, MPH,
Jay Schulkin, PhD, Yujia Zhang, PhD, and William Callaghan, MD, MPH
Attitudes and Practices of Obstetrician-Gynecologists
Regarding Influenza Vaccination in Pregnancy
National Center for Chronic Disease Prevention and Health Promotion
Division of Reproductive Health
Dmitry Kissin, MD, MPHDivision of Reproductive Health, CDC
Disclaimer
The findings and conclusions in this presentation have not been formally disseminated by the Centers for Disease Control and Prevention and should not be construed to represent any agency determination or policy
Background Pregnant women are at high risk for influenza-
related complications, including severe disease
Neonates are at high risk for morbidity and mortality from respiratory infections, but active immunization for influenza is not successful in newborns or infants <6 months of age
Use of influenza vaccine in pregnancy can benefit both the woman and her infant
Inactivated influenza vaccine is recommended for all women who will be pregnant during influenza season
Vaccination can occur in any trimester of pregnancy
Study Objectives
Assess knowledge, attitudes and practices of U.S. obstetrician-gynecologists regarding influenza vaccination during pregnancy
Assess barriers and facilitators to influenza vaccination during pregnancy among U.S. obstetrician-gynecologists
Study Methods Study population and sampling:
Random sample of U.S. obstetrician-gynecologists ACOG fellows or junior fellows in ACOG database Only ob-gyns currently involved in obstetric patient care
Survey: Self-administered mail survey (cover letter and pre-paid
envelope) Questions about basic demographics, experience with ILI in
their practice, attitudes and practices re: influenza vaccinations
No incentives were offered
Timeline: Initial mailing in February 2010, right after the peak of
H1N1 pandemic Follow-up survey to non-respondents at 4- to 5-week
intervals
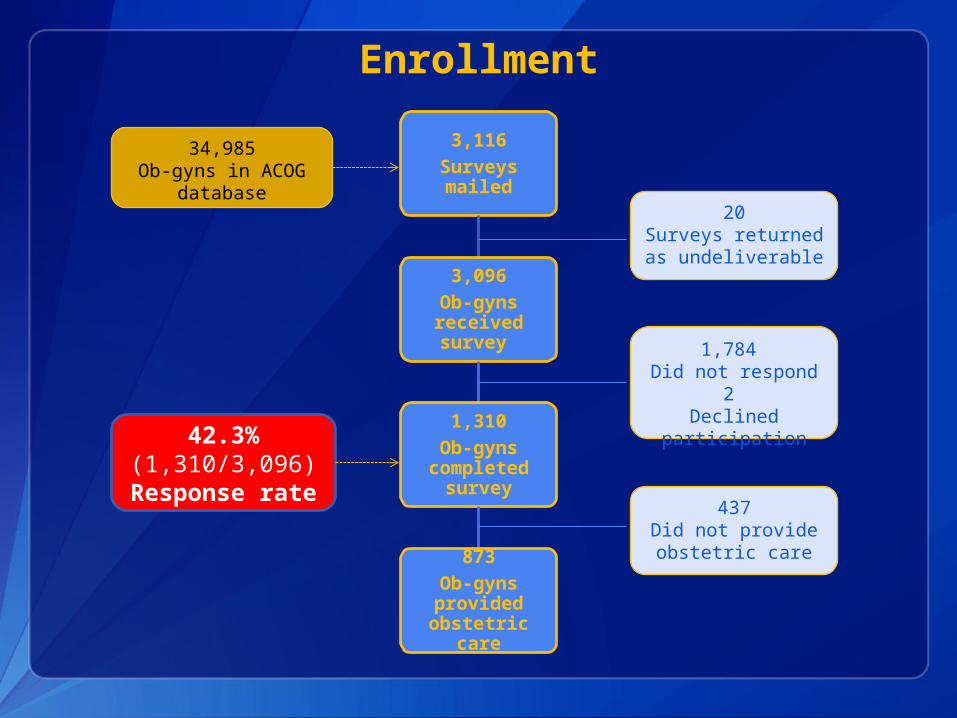
3,116Surveys mailed
3,096Ob-gyns received survey
1,310Ob-gyns
completed survey
873Ob-gyns provided obstetric
care
20Surveys returned as undeliverable
1,784 Did not respond
2 Declined
participation
34,985Ob-gyns in ACOG
database
437Did not provide obstetric care
42.3%(1,310/3,096)
Response rate
Enrollment
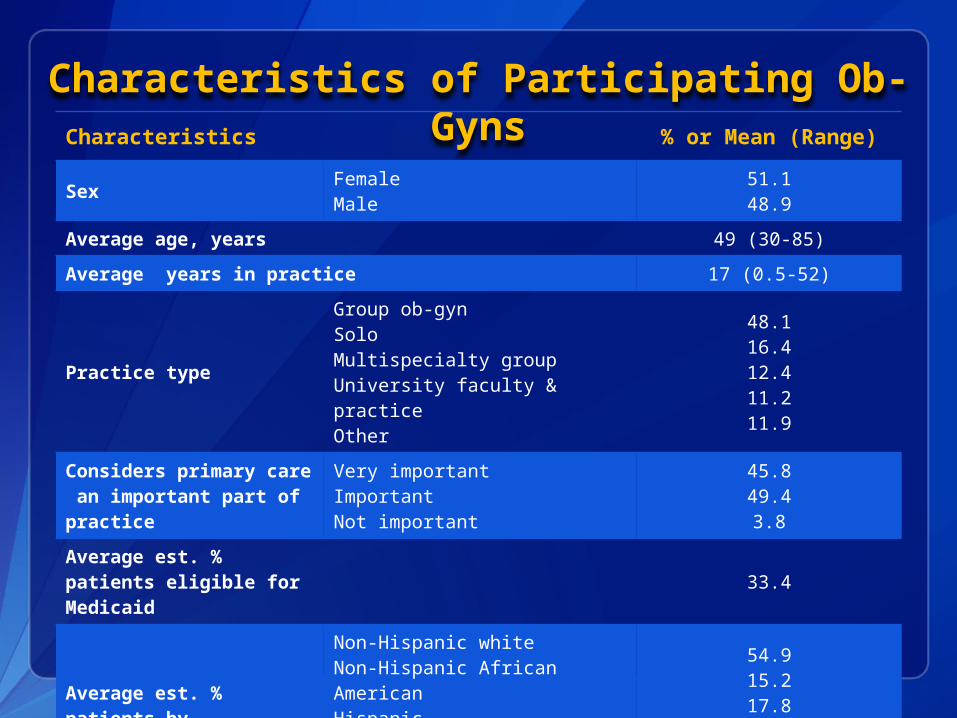
Characteristics of Participating Ob-GynsCharacteristics % or Mean (Range)
SexFemaleMale
51.148.9
Average age, years 49 (30-85)
Average years in practice 17 (0.5-52)
Practice type
Group ob-gynSoloMultispecialty groupUniversity faculty & practiceOther
48.116.412.411.211.9
Considers primary care an important part of practice
Very importantImportantNot important
45.849.43.8
Average est. % patients eligible for Medicaid
33.4
Average est. % patients by race/ethnicity
Non-Hispanic whiteNon-Hispanic African AmericanHispanicAsian or Pacific IslanderNative AmericanMultiracialOther
54.915.217.85.31.32.61.0
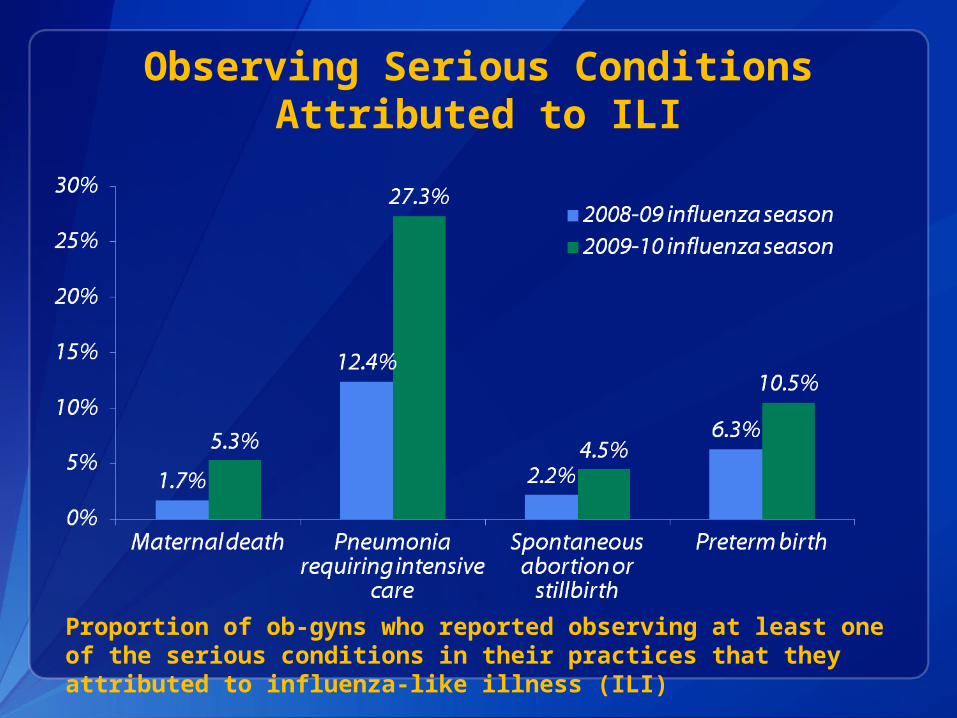
Observing Serious Conditions Attributed to ILI
Proportion of ob-gyns who reported observing at least one of the serious conditions in their practices that they attributed to influenza-like illness (ILI)
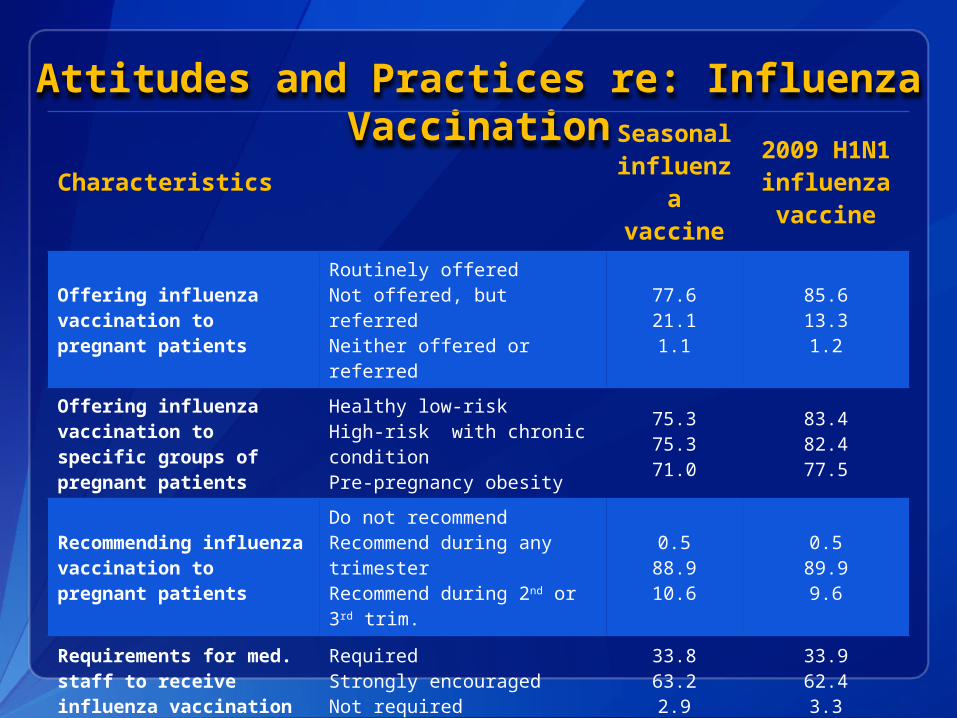
Attitudes and Practices re: Influenza Vaccination
Characteristics
Seasonal
influenza
vaccine
2009 H1N1 influenza vaccine
Offering influenza vaccination to pregnant patients
Routinely offeredNot offered, but referredNeither offered or referred
77.621.11.1
85.613.31.2
Offering influenza vaccination to specific groups of pregnant patients
Healthy low-riskHigh-risk with chronic conditionPre-pregnancy obesity
75.375.371.0
83.482.477.5
Recommending influenza vaccination to pregnant patients
Do not recommendRecommend during any trimesterRecommend during 2nd or 3rd trim.
0.588.910.6
0.589.99.6
Requirements for med. staff to receive influenza vaccination
RequiredStrongly encouragedNot required
33.863.22.9
33.962.43.3
Received influenza vaccination themselves
YesNo
91.78.3
89.810.2
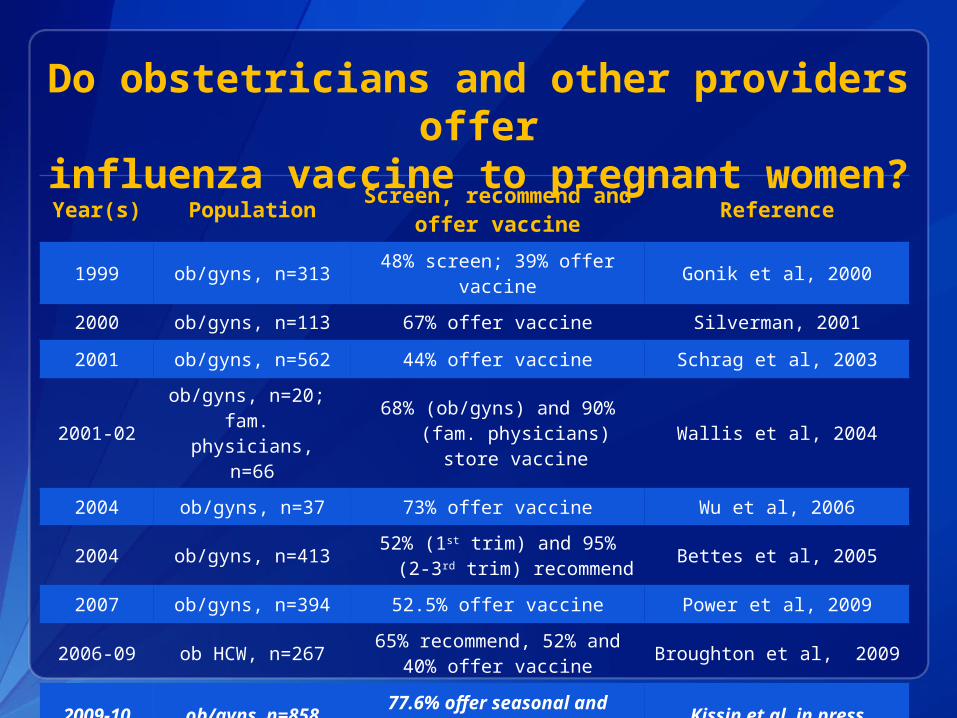
Year(s) Population Screen, recommend and offer vaccine Reference
1999 ob/gyns, n=31348% screen; 39% offer
vaccineGonik et al, 2000
2000 ob/gyns, n=113 67% offer vaccine Silverman, 2001
2001 ob/gyns, n=562 44% offer vaccine Schrag et al, 2003
2001-02ob/gyns, n=20; fam. physicians,
n=66
68% (ob/gyns) and 90% (fam. physicians) store
vaccineWallis et al, 2004
2004 ob/gyns, n=37 73% offer vaccine Wu et al, 2006
2004 ob/gyns, n=41352% (1st trim) and 95% (2-3rd
trim) recommendBettes et al, 2005
2007 ob/gyns, n=394 52.5% offer vaccine Power et al, 2009
2006-09 ob HCW, n=26765% recommend, 52% and
40% offer vaccineBroughton et al, 2009
2009-10 ob/gyns, n=85877.6% offer seasonal and 85.6% offer H1N1 vaccine
Kissin et al, in press
Do obstetricians and other providers offer
influenza vaccine to pregnant women?
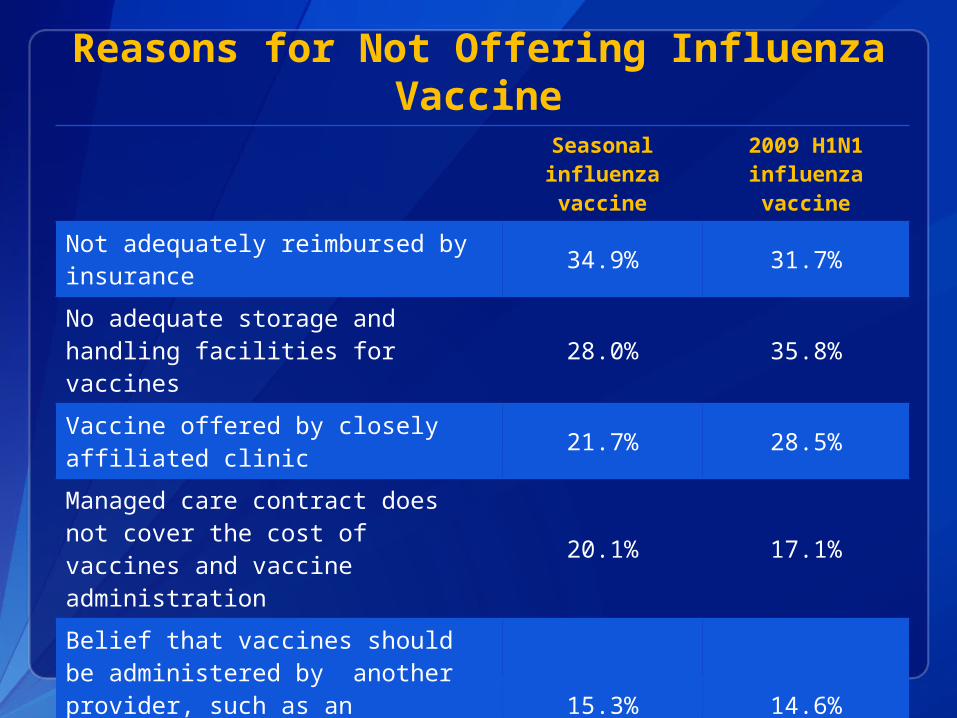
Reasons for Not Offering Influenza Vaccine
Seasonal influenza vaccine
2009 H1N1 influenza vaccine
Not adequately reimbursed by insurance 34.9% 31.7%
No adequate storage and handling facilities for vaccines 28.0% 35.8%
Vaccine offered by closely affiliated clinic 21.7% 28.5%
Managed care contract does not cover the cost of vaccines and vaccine administration
20.1% 17.1%
Belief that vaccines should be administered by another provider, such as an internist or family practitioner
15.3% 14.6%
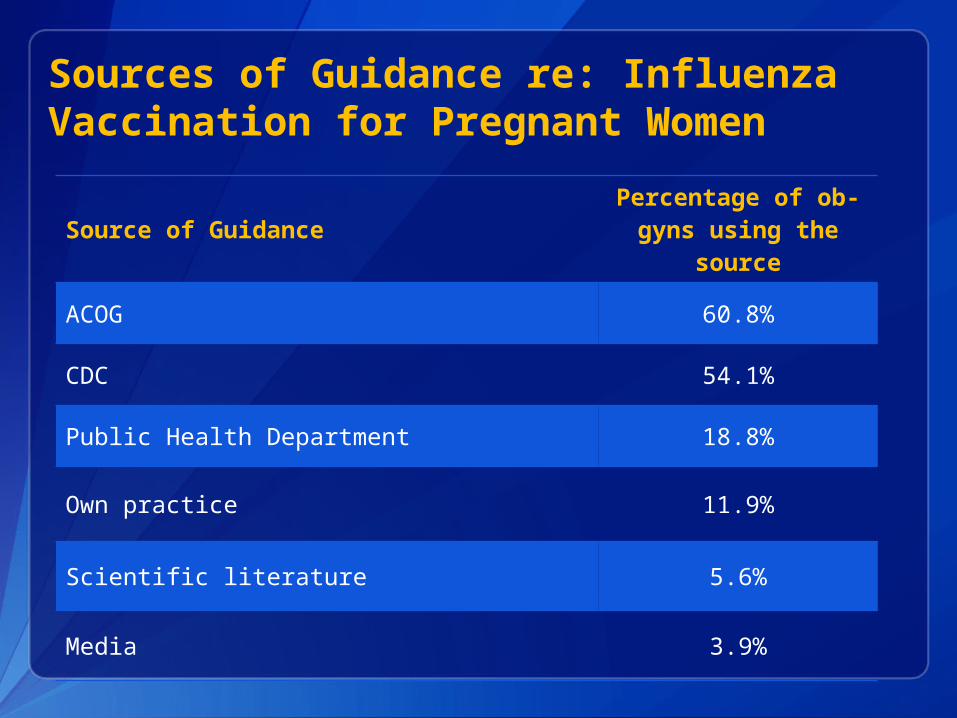
Sources of Guidance re: Influenza Vaccination for Pregnant Women
Source of GuidancePercentage of ob-
gyns using the source
ACOG 60.8%
CDC 54.1%
Public Health Department 18.8%
Own practice 11.9%
Scientific literature 5.6%
Media 3.9%
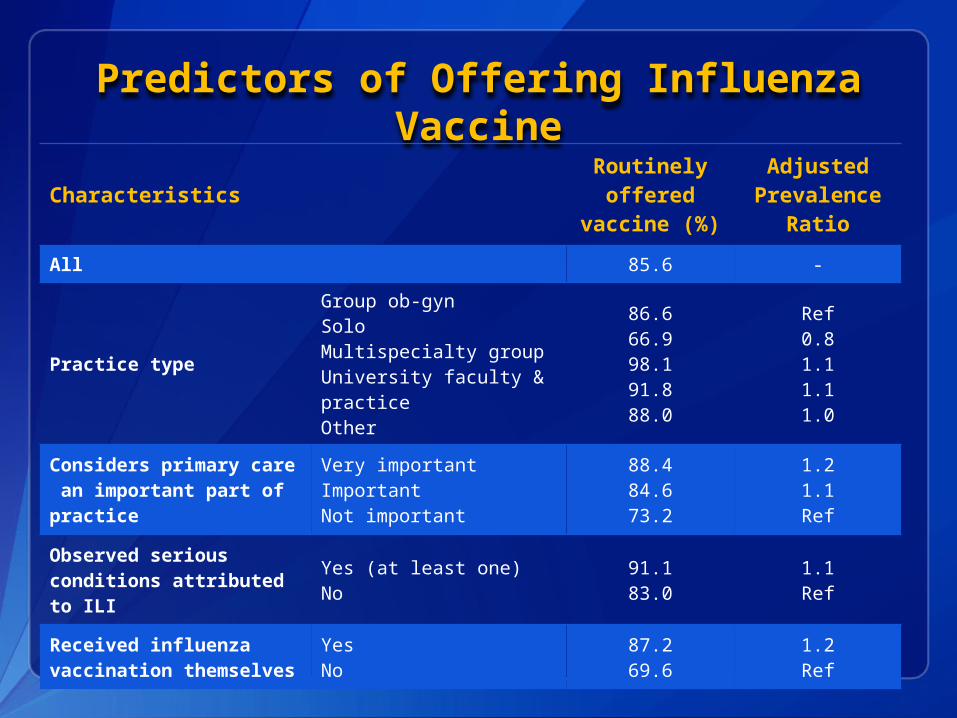
Predictors of Offering Influenza Vaccine
CharacteristicsRoutinely offered
vaccine (%)
Adjusted Prevalence
Ratio
All 85.6 -
Practice type
Group ob-gynSoloMultispecialty groupUniversity faculty & practiceOther
86.666.998.191.888.0
Ref0.81.11.11.0
Considers primary care an important part of practice
Very importantImportantNot important
88.484.673.2
1.21.1Ref
Observed serious conditions attributed to ILI
Yes (at least one)No
91.183.0
1.1Ref
Received influenza vaccination themselves
YesNo
87.269.6
1.2Ref
Summary Most ob-gyns routinely offered influenza
vaccinations to their patients
A considerable proportion of ob-gyns did not offer vaccination or did not recommend vaccination in the first trimester of pregnancy
Barriers to recommending and administering influenza vaccination among ob-gyns included financial and logistical concerns (inadequate reimbursement, absence of storage and handling facilities)
Solo practice providers were less likely to offer influenza vaccination, but more likely to consider primary care a very important part of their practice
Recommendations
Utilize available approaches to increase vaccination during pregnancy: Engage in educational and promotion activities for
obstetric providers Collaborate with professional organizations on provider
education Promote standing orders for influenza vaccinations Address financial (insurance coverage and
reimbursement), administrative and logistical concerns (especially among solo practice providers)
Encourage providers to be vaccinated themselves
Design, implement and evaluate interventions to improve vaccination coverage among pregnant women
For more information please contact Centers for Disease Control and Prevention1600 Clifton Road NE, Atlanta, GA 30333Telephone, 1-800-CDC-INFO (232-4636)/TTY: 1-888-232-6348E-mail: [email protected] Web: www.cdc.gov
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Thank You!
Division of Reproductive Health
National Center for Chronic Disease Prevention and Health Promotion
Additional Slides
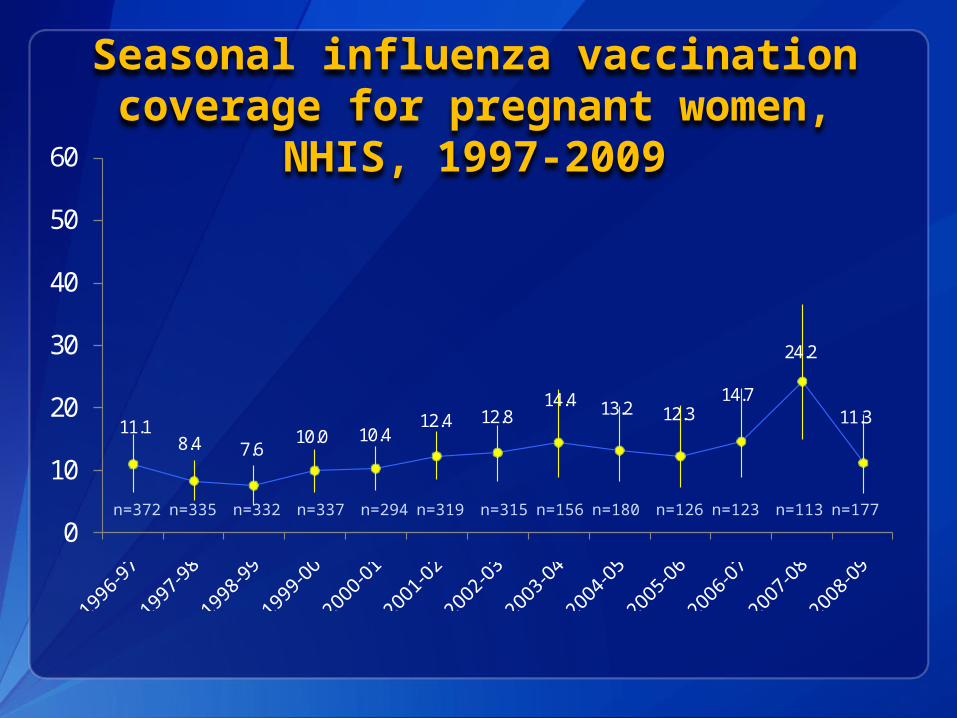
Seasonal influenza vaccination coverage for pregnant women,
NHIS, 1997-2009
11.18.4 7.6
10.0 10.412.4 12.8
14.4 13.2 12.314.7
24.2
11.3
0
10
20
30
40
50
60
n=372
n=335
n=332
n=337
n=294
n=319
n=315
n=156
n=180
n=126
n=123
n=113
n=177
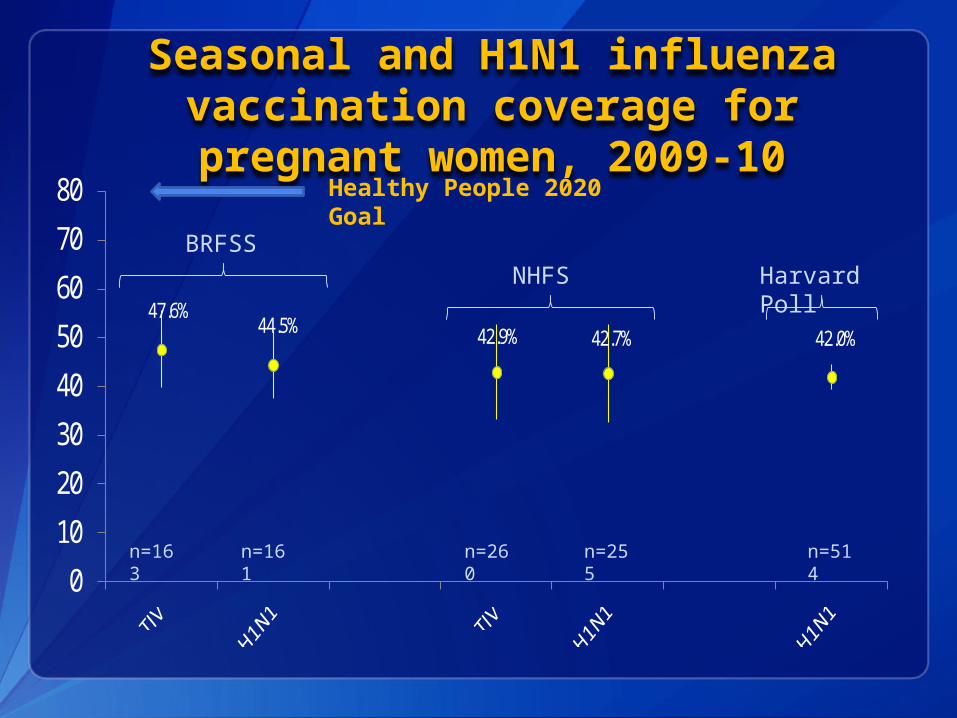
Seasonal and H1N1 influenza vaccination coverage for
pregnant women, 2009-10
47.6%44.5% 42.9% 42.7% 42.0%
0
10
20
30
40
50
60
70
80
BRFSSNHFS Harvard
Poll
n=163
n=161
n=260
n=255
n=514
Healthy People 2020 Goal
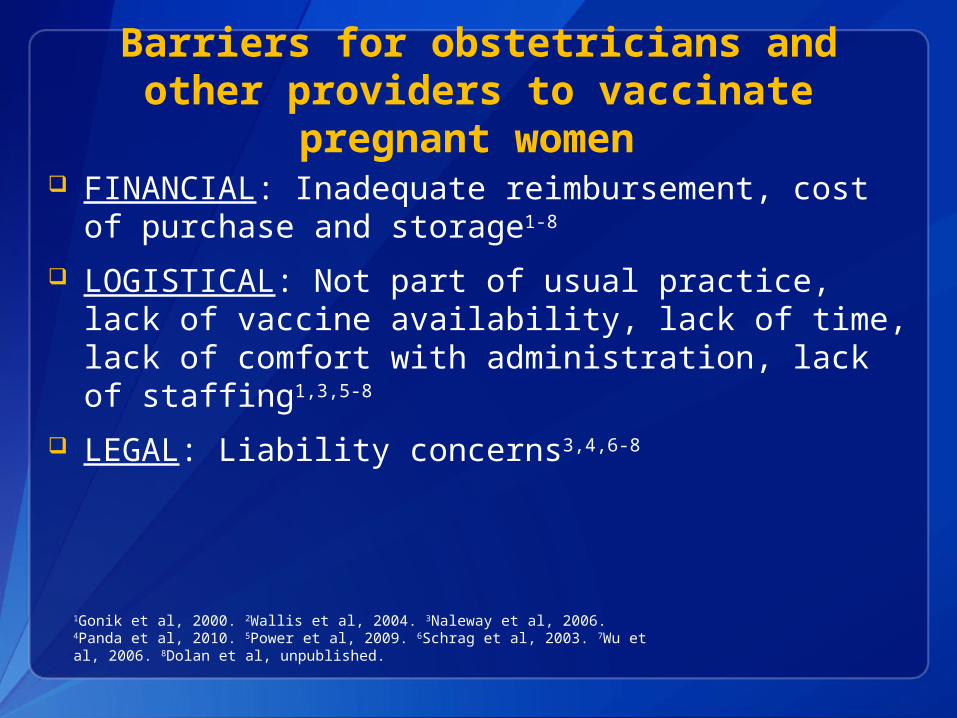
Barriers for obstetricians and other providers to vaccinate pregnant
women FINANCIAL: Inadequate reimbursement, cost of
purchase and storage1-8
LOGISTICAL: Not part of usual practice, lack of vaccine availability, lack of time, lack of comfort with administration, lack of staffing1,3,5-8
LEGAL: Liability concerns3,4,6-8
1Gonik et al, 2000. 2Wallis et al, 2004. 3Naleway et al, 2006. 4Panda et al, 2010. 5Power et al, 2009. 6Schrag et al, 2003. 7Wu et al, 2006. 8Dolan et al, unpublished.
Barriers for obstetricians and other providers to vaccinate pregnant
women - continued KNOWLEDGE: Uncertainty about
recommendations, lack of knowledge about increased morbidity of pregnant women from influenza, lack of knowledge about conferring passive immunity to infant, lack of data on effectiveness1-5
ATTITUDES/PRACTICES: patient demand low or patient unwillingness, not being vaccinated themselves2-6
SAFETY: Concerns about safety for pregnant women and fetus, concern about preservatives, concerns about vaccination during the first trimester2-7
1Gonik et al, 2000. 2Naleway et al, 2006. 3Power et al, 2009. 4Schrag et al 2003. 5Wu et al, 2006. 6Panda et al, 2010. 7Dolan et al, unpublished.
Provider/system- based and access-enhancing interventions to
increase vaccination during pregnancy Provider reminder systems: chart prompts, printing
vac. record Provider assessment and feedback: monitoring and
reporting vaccination rates Standing orders: vaccination by healthcare personnel
without direct physician involvement, encouraged by ACIP Provider education: active education, promotion
activities, vaccination training, communication with ob providers through letters and calls from ACOG, AMA leadership*
Enhancing access to vaccinations: providing vaccine directly to ob providers (2009-10), vaccination clinics for pregnant women and their partners*
Sources: CDC, MMWR 2000. Naleway et al, 2006. Ndiaye et al, 2005. Mouzoon et al, 2010. Ogburn et al, 2007. Panda et al, 2010. Wallis et al, 2006. Mills, Maine Dept of Health, personal communication, 2010. Koelemay, Seattle King County Health Dept, personal communication, 2010.*Interventions not formally evaluated





























