Embed Size (px)
Citation preview

P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S E S 5 6 ( 2 0 1 4 ) 4 3 4 – 4 4 0
Ava i l ab l e on l i ne a t www.sc i enced i rec t . com
ScienceDirect
www.on l i nepcd .com
Contribution of Cardiorespiratory Fitness to theObesity Paradox
Paul A. McAuleya,⁎, Kristen M. Beaversb
aDepartment of Human Performance and Sport Sciences, Winston-Salem State University, Winston-Salem, NC, USAbSticht Center on Aging, Wake Forest School of Medicine, Winston-Salem, NC, USA
A R T I C L E I N F O
Statement of Conflict of Interest: see page⁎ Address reprint requests to Paul A. McAu
University, 601 S Martin Luther King Jr. DriveE-mail address: [email protected] (P.A
0033-0620/$ – see front matter © 2014 Elseviehttp://dx.doi.org/10.1016/j.pcad.2013.09.006
A B S T R A C T
Keywords:
Until recently, cardiorespiratory fitness (CRF) has been overlooked as a potential modifier ofthe inverse association between obesity and mortality (the so-called obesity paradox),observed in patients with known or suspected cardiovascular (CV) disease. Evidence fromfive observational cohort studies of 30,104 patients (87% male) with CV disease indicatesthat CRF significantly alters the obesity paradox. There is general agreement across studiesthat the obesity paradox persists among patients with low CRF, regardless of whetheradiposity is assessed by body mass index, waist circumference, or percentage body fat.However, among patients with high CRF, risk of all-cause mortality is lowest for theoverweight category in some, but not all, studies, suggesting that higher levels of fitnessmay modify the relationship between body fatness and survival in patients manifesting anobesity paradox. Further study is needed to better characterize the joint contribution of CRFand obesity on mortality in diverse populations.© 2014 Elsevier Inc. All rights reserved.
Cardiorespiratory fitnessObesity paradoxCoronary heart disease
Controversy exists as to whether exercise or weight exerts agreater influence on risk of death. In their 1999 landmarkreport of over 25,000 men from the Aerobic Center Longitudi-nal Study (ACLS), Wei and colleagues1 found that men with abody mass index (BMI) ≥30 kg/m2 (i.e. obese) who also hadhigh levels of cardiorespiratory fitness (CRF; i.e. fit) were nomore likely to die from cardiovascular (CV) disease or all-causes than normal-weight (i.e. BMI 18.5–24.9 kg/m2) and fitmen. A similar ACLS study published that same year foundthat measures accounting for body fat mass and distributionproduced results similar to BMI.2 Together, these seminalpapers formed the basis of the “fat and fit” hypothesis whichsuggests that higher CRF attenuates the increased mortalityrisk associated with excess adiposity in the general popula-tion. Numerous studies in both men and women from the
439.ley, PhD, Department of H, Anderson 141B, Winsto. McAuley).
r Inc. All rights reserved.
ACLS3 and from other large observational datasets4 havesince replicated these findings.
In not all populations, however, is a direct associationobserved between obesity and mortality. About a decade ago,an unexpected finding that overweight and obese patientsundergoing percutaneous coronary interventions had re-duced mortality when compared to their lean counterpartswas first reported by Gruberg et al.5 who coined the term“obesity paradox.” This inverse association between obesityand mortality has been repeatedly observed in patients withestablished CV disease.6 Despite its prevalence, however, fullyaccounting for this observation remains elusive.
Since most studies reporting an obesity paradox have usedBMI to assess adiposity,7 critics have argued that thisphenomenon is simply an artifact of the limitation of BMI to
uman Performance and Sport Sciences, Winston-Salem Staten-Salem, NC 27110.

Abbreviations and Acronyms
ACLS = Aerobics Center Longitu-dinal Study
BMI = body mass index
%BF = body fat
CHD = coronary heart disease
CRF = cardiorespiratory fitness
CV = cardiovascular
HF = heart failure
HR = hazard ratio
MET = metabolic equivalent
VETS = Veterans Exercise TestingStudy
WC = waist circumference
WHR = waist-to-hip ratio
435P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S E S 5 6 ( 2 0 1 4 ) 4 3 4 – 4 4 0
accurately measureexcessive adiposity inboth healthy and dis-eased populations.8
Others have pointedout that the protectiveeffect of a higher BMIin patients withestablished chronicdiseases is to beexpected.7 For exam-ple, many chronic dis-eases are complicatedby muscle wastingand nutritional inade-quacy associated witha lower BMI. Recentlyhowever, a growingbody of evidence sug-gests that CRF mayprovide the mostcomplete explanation
for the obesity paradox.9 That is, CRF may, at least in part,account for the inverse association between obesity andmortality observed in patients with established CV disease.In this article, we review five observational cohort studiesthat investigate the modifying influence of CRF on the obesityparadox in patients with CV diseases, and discuss possiblemechanisms underlying these effects.
Low CRF as a CV disease risk factor
Low CRF has long been established as an independentpredictor of CV morbidity,10 and mortality,11,12 as well asmortality from all-causes.13,14 However, due to difficultiesmeasuring CRF, along with the lack of operational definitionof “fitness,” it is often underutilized as a clinical CV diseaserisk factor.15 CRF measurements are obtained from special-ized exercise tests, which require expensive laboratoryequipment and trained personnel. Whereas conventionalrisk factors, like blood lipid panels, are routinely performedin preventive screenings, typically only patients with knownor suspected CV disease are referred for exercise testing.Another obstacle concerns the absence of a standardizedclassification system as exists, for example, for BMI. This hasled to some variations as to what constitutes “low” CRF. In thefirst ACLS report on CRF andmortality, fitness categories werebased on age and sex norms of treadmill time with low CRFdefined as the lowest 20%.13 Other studies of CRF andmortality in patients with CV diseases have used absolutecutoff points to define low CRF based on metabolic equiva-lents (METs) of 4,16 5,14 and 6.17 When expressed as percen-tiles of their respective populations, these MET values rangefrom approximately the lowest 20%14 to the lowest 40%.16,17
Regardless of the classification system used, however, it isworth noting that “low” CRF is consistently associated withhigher risk of mortality.14,16,17
Recent longitudinal data reporting on changes in CRFprovide more compelling evidence of the prognostic power ofCRF on CV morbidity and mortality. In one ACLS study18 of14,345 men, maintaining or improving CRF over a period of6.3 years was associated with substantially lower CV diseasemortality, regardless of BMI change [HR (95% CI): 0.56(0.37–0.85) and 0.59 (0.37–0.95) for maintaining or improvingCRF, respectively]. In another ACLS study19 of 3148 healthyadults, the development of CV disease risk factors associatedwith global fat gain over a period of 2.1 years was attenuatedwhen CRF was maintained or improved. The importance ofCRF in predicting adverse health outcomes is underscored bythe American Heart Association's recent policy statementadvocating for the development of a national adult CRFregistry to provide a sufficiently representative sample ofthe US population for accurate interpretation of CRFmeasures.20 Whereas most studies about the obesity paradoxinclude adjustments for traditional CV risk factors such ashypertension and smoking history, measurements of CRF aremissing in all but a few recent studies.9 Given that low CRF issuch a powerful predictor of CV disease and mortality risk, itis plausible that it represents an unmeasured confounderof the obesity paradox that could have considerable explan-atory power.
CRF and the obesity paradox in CV diseases
A comprehensive literature search was conducted using thePUBMED database (National Library of Medicine, Bethesda,MD) inclusively through July 2013 on epidemiologicalstudies using the keywords: obesity; cardiorespiratoryfitness; and cardiovascular diseases. References withinidentified papers as well as articles that had come to theattention of the authors through other means were alsoexamined for suitability. Six studies were identified exam-ining the obesity paradox in patients with CV diseases, thatalso included objectively measured CRF.16,17,21–24 Onestudy21 provided only unadjusted mortality rates, whichprecluded meaningful comparisons with other studies.Therefore, we evaluated five studies that included adjustedmultivariate analyses for combined fitness-adiposity cate-gories and summarized key findings by order of publicationbelow (see Table 1).
In the first study,22 12,417 middle-aged men from theVeterans Exercise Testing Study (VETS) with a mean follow-up of 7.7 years for all-cause mortality, both fitness and BMIwere independently and inversely associated with mortality.When jointly modeled, a significantly lower mortality riskwas found for men classified with high fitness (>10 METs)/overweight [HR (95% CI): 0.43 (0.32–0.59)] and high fitness/obese [HR (95% CI): 0.52 (0.34–0.82)], compared to the referencegroup (high fitness/normal weight). Conversely, mortality riskwas 1.5 to 4.5 times higher for men with low CRF (<5 METs)across BMI categories, with the highest mortality risk seen inthe underweight subgroup [HR (95% CI): 4.48 (3.06–6.57)]. Thus,fitness altered the obesity paradox in that overweight andobesity were only protective against premature mortality in

Table 1 – Studies of obesity paradox and fitness in patients with known or suspected cardiovascular disease.
Author,Year(Reference) Participants
AdiposityClassification
FitnessClassification
Mean Follow-up,Years (AnnualMortality %)
Fitness-AdiposityGroups
AdjustedHazardRatio(95% CI) ⁎
McAuleyet al.,201022
12,417 men referredfor exercise testing,aged 40–70 years(mean age 57 years)
BMI (kg/m2): Estimated METsfrom time on rampexercise test:
7.7 (2.9%) High fit/underweight –High fit/normal 1 (reference)High fit/overweight 0.43 (0.32–0.59)High fit/obese 0.52 (0.34–0.82)Mod. fit/underweight 3.09 (2.17–4.38)Mod. fit/normal 1.65 (1.34–2.04)Mod. fit/overweight 1.15 (0.93–1.42)
Normal(18.5–24.9)
Low (<5.0)
Mod. fit/obese 0.99 (0.80–1.23)
Overweight(25.0–29.9) Mod. (5.0–10.0)
Low fit/underweight 4.48 (3.06–6.57)Low fit/normal 2.03 (1.60–2.58)
Obese(≥30.0)
High (>10.0)
Low fit/overweight 1.79 (1.43–2.25)Low fit/obese 1.61 (1.27–2.03)
Goel et al.,201124
855 CHD patients(80% men), meanage 62 years
BMI (kg/m2): Sex-specificmedian peakVO2 (ml/kg/min)using the acceleratedNaughton protocol:
9.7 (1.9%) High fit/normal BMI 1 (reference)Normal(18.5–24.9)
Low (<21.5, men;<16.8, women)
High fit/overweight 2.2 (0.63–7.4)
Overweight(25.0–29.9)
High (≥21.5, men;≥16.8, women)
High fit/obese 3.2 (0.88–11.4)
Obese (≥30)
Low fit/normal BMI 9.6 (2.9–31.8)Low fit/overweight 6.8 (2.1–22.2)
WHR:Low fit/obese 3.3 (0.96–11.4)
Low (<0.85, women;<0.90, men)
High fit/low WHR 1 (reference)
High (≥0.85,women;≥0.90, men)
High fit/high WHR 2.3 (1.0–5.4)Low fit/low WHR 4.2 (1.8–9.8)Low fit/high WHR 6.1 (2.7–13.6)
McAuleyet al.,201225
9,563 men withknown or suspectedCHD, meanage 47 years
BMI (kg/m2): Age-specific tertilesof time on modifiedBalke protocol:
13.4 (0.6%) High fit/normal BMI 1 (reference)Normal(18.5–<25.0)
Low (tertile 1)High (tertiles 2 and 3)
High fit/overweight 0.84 (0.68–1.03)
Overweight(25.0–<30.0)
High fit/obese I 0.65 (0.38–1.10)
Obese I(30.0–<35.0)
High fit/obese II/III 2.46 (0.61–9.96)
Obese II/III (≥35.0)
Low fit/normal BMI 1.60 (1.24–2.05)
WC tertiles (cm):
Low fit/overweight 1.09 (0.88–1.36)
Low (<90)
Low fit/obese I 1.38 (1.04–1.82)
Middle (90–98)
Low fit/obese II/III 2.43 (1.55–3.80)
Upper (>98)
High fit/low WC 1 (reference)
Body fattertiles (%):
High fit/mod. WC 0.89 (0.71–1.19)
Low (<20)
High fit/high WC 0.77 (0.58–1.02)
Mod. (20–25)
Low fit/low WC 1.67 (1.28–2.18)
High (>25)
Low fit/mod. WC 1.05 (0.81–1.37)Low fit/high WC 1.34 (1.07–1.67)
High fit/low %BF 1 (reference)High fit/mod. %BF 0.85 (0.68–1.08)High fit/high %BF 0.96 (0.74–1.25)Low fit/low %BF 1.79 (1.35–2.38)Low fit/mod. %BF 1.28 (0.99–1.67)Low fit/high %BF 1.26 (1.01–1.57)
Lavie et al.,201316
2066 patientswith systolic heartfailure (79% men),mean age 56 years
BMI (kg/m2): Peak VO2
(ml/kg/min) usingstandard progressiveCPX protocols:
2.1 (4.9%) High fit/normal BMI 1 (reference)Normal (<25.0)
Low (<14)
High fit/overweight Not significantOverweight andObese (≥25.0)
High (≥14)
Low fit/normal BMI 1 (reference)Low fit/overweight 0.61 (0.42–0.89)
Uretskyet al.,201317
5203 patients withsuspected CHD(37% men), meanage 60 years
BMI (kg/m2): Estimated METsfrom time on Bruceexercise test:
8.1 (2.2%) High fit/normal BMI 2.2 (1.44–3.30)Normal(18.5–24.9)
Low fit (<6.0)
High fit/overweight 1.3 (0.86–1.96)
Overweight(25.0–29.9) High fit (≥6.0)
High fit/obese 1 (reference)
Obese (≥30)
Low fit/normal BMI 3.5 (2.16–5.66)Low fit/overweight 2.1 (1.24–3.42)Low fit/obese 1.7 (1.00–2.76)
⁎ All-cause mortality adjusted for age, gender (where applicable), and multiple risk factors.
436 P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S E S 5 6 ( 2 0 1 4 ) 4 3 4 – 4 4 0

437P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S E S 5 6 ( 2 0 1 4 ) 4 3 4 – 4 4 0
the highly fit men. Within fitness strata, however, an obesityparadox persisted andmay be due to unique characteristics ofthis population. Namely, that men qualifying for militaryservice have to meet fitness and weight criteria at the time oftheir enlistment. Therefore, the VETS cohort consists of onlyindividuals who were fit and not obese and were free of pre-existing serious health problems at the time of their enlist-ment. This is known as the “veteran effect” which has beenpreviously described.25
Findings for low CRF and mortality are in generalagreement with the second study by Goel et al.,23 whofollowed 855 patients with coronary heart disease (CHD)from the Mayo Clinic for an average of 9.7 years. Even afteradjustment for BMI and waist-to-hip ratio (WHR), lowfitness (<21.5 mL O2 · kg−1 · min−1 for men and <16.8 mLO2 · kg−1 · min−1 for women) was associated with a nearlythreefold increase in mortality. When stratified into sub-groups, low-fitness/normal-BMI and overweight patientshad a significantly higher risk of mortality as compared tothe high-fitness/normal-BMI reference group; a findingwhich was replicated when using WHR in lieu of BMI. Incontrast, mortality risk for patients with high fitness in thesubgroups of overweight and obese did not differ from thenormal-weight reference subgroup. It should be noted,however, that the small sample size and relatively fewdeaths (n = 159) in this study attribute to the extremelylarge confidence intervals, thus caution is warranted wheninterpreting these results.
A third paper examining the contribution of CRF to theobesity paradox, utilizing several measures of adiposity,was recently published in a study of 9563 ACLS men withknown or suspected CHD.24 Unlike most previous studiesthat classified obesity solely based on BMI, this investiga-tion also included indices of body fat percentage (%BF) andwaist circumference (WC). During a mean follow-up of13.4 years, there were 733 deaths, resulting in 57.2 all-cause and 27.2 CV-related deaths per 10,000 person-yearsof follow-up. CRF tertiles were based on age- and sex-specific MET levels achieved on a modified Balke maximaltreadmill exercise test as previously described.26 In accor-dance with prior work, high CRF (tertiles 2 and 3) wasinversely associated with CV disease and all-cause mortal-ity. For men with high CRF, mortality risk was notsignificantly different across adiposity levels compared totheir respective reference groups. However, mortality riskwas higher for most, but not all low CRF subgroups (i.e.overweight, moderate WC, and moderate %BF), comparedto their high CRF/normal counterparts. (Interestingly, theresults for WC and %BF were similar to those for BMIsuggesting that the obesity paradox is not simply anartifact of BMI, as some have suggested.8) Collectively,these findings demonstrate that standard measures of %BFand distribution exert less influence on survival in CHDpatients compared to CRF.
A fourth study16 was a multicenter analysis of 2066patients with heart failure (HF) who were referred forcardiopulmonary exercise testing. Adiposity was assessedusing dichotomous categorical variables for BMI (<25 and≥ 25 kg/m2) and peak oxygen consumption (<14 and ≥14 mL
O2 · kg−1 · min−1) to define low and high CRF. Afteradjusting for age and sex, in patients in the low CRFsubgroup, BMI ≥ 25 kg/m2 was associated with lowermortality risk [HR (95% CI): 0.61 (0.42–0.89)] compared withBMI <25 kg/m2. In contrast, there was no significantdifference in mortality risk between BMI groups in thehigher-CRF subgroup.
The final study17 included in this review was therecently published report on 5203 patients undergoingstress–rest perfusion single-photon emission computedtomography (SPECT) imaging (2697 completed an exercisetest and 2506 underwent pharmacologic stress becausethey could not exercise). Patients completing the exercisetest were categorized into two groups based on theirexercise capacity (low fitness, <6 METs; high fitness, ≥6METs) and were further divided into three subgroupsbased on their BMI category (normal-weight, overweight,and obese). Compared to the obese, high-fitness referencegroup, adjusted multivariate risk for all-cause mortalitywas higher across low-fitness subgroups of normal weight[HR (95% CI): 3.5 (2.16–5.66)], overweight [HR (95% CI): 2.1(1.24–3.42)], and obese [HR (95% CI): 1.7 (1.00–2.76)] and forthe normal-weight, high-fitness group [HR (95% CI): 2.2(1.44-3.30)]. However, mortality risk for the overweight,high-fitness group did not differ significantly from thereference group. These findings are in general agreementwith previous studies that found an obesity paradoxamong participants with low fitness, but differ in thatthe obesity paradox persisted among patients withhigh fitness.
In summary, as expected, patients with high fitness hadbetter survival compared to patients with low fitness from thesame BMI category. A commonality observed across allstudies was that among patients with low fitness, higherBMI was protective for all-cause mortality. However, somedifferences were noted among patients with high fitness.Whereas in three of the studies,16,23,24 an obesity paradox wasabsent across the BMI subgroups, in two studies,17,22 over-weight and obese patients with high fitness had lowermortality compared to their normal-weight counterparts.Differences in population characteristics may partially ex-plain this discrepancy. In the studies reporting an obesityparadox in the high-fitness group, one22 included middle-aged male veterans and the other17 men and women with anormal stress–rest SPECT. Factors such as age and healthstatus of these populations may have contributed to thesedifferences, but further study is required to fully elucidatethese inconsistencies.
Potential mechanisms underlying theCRF-mediated alteration of the obesity paradox
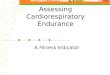
Higher CRF is associated with a more favorable CV andmetabolic risk factor profile.19 Several potential mecha-nisms acting individually and/or in concert underlie theseassociations (Figure 1). In the normal population, CRFcounteracts the development of adverse health outcomesassociated with obesity. However, in patients with CHD, the

Genetic factorsGrowth/development
AgingAerobic exercise training
CRF
Central obesity↓abdominal fat↓liver fat↓adipokines↑adiponectin
Hypertension↓epinephrine↓renin↓angiotensin↑vascular control
Dyslipidemia↓interleukin-6↓TNF-α↓lypolysis
Hyperglycemia↑IRS protein↑GLUT 4
Independent of CRF Independent
of CRF
Fig. 1 – Potential mechanisms for cardiorespiratory fitness (CRF)-mediated attenuation of cardiometabolic risk (reproducedwith permission from John Wiley & Sons, Ltd.).
438 P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S E S 5 6 ( 2 0 1 4 ) 4 3 4 – 4 4 0
effects may be greater for normal-weight patients who areat higher risk. In this section, we briefly summarize theprimary mechanisms by which higher CRF may improvetraditional CV disease risk factors and thereby lower CVmortality risk.
Altered fat distribution is associated with lower risk ofCV diseases, independent of total adiposity.27 Availableevidence suggests that ectopic fat depots may be lower infit individuals independent of BMI,28 and in a study of over13,000 men with hypertension from the ACLS29 amongthose with high CRF, those with a high WC had no greaterCVD mortality risk compared with those having a normalWC. This indicates that ectopic fat depots may be lower infit individuals independent of subcutaneous abdominaladiposity. More direct evidence for the impact of CRF onectopic fat independent of global adiposity was reported byJohnson et al.30 who found a 21% reduction in hepatic lipidconcentration after 4 weeks of aerobic exercise trainingthat increased CRF by 13% in 19 obese men and women,but without any change in body weight or abdominaladipose tissue. Further study will be required to determinewhether this effect can explain the differential mortalityrisks at different levels of CRF in patients exhibiting anobesity paradox.
Another mechanism may be related to inflammatoryadipose tissue-derived cytokines or adipokines.31 Chronicinflammation is a strong, independent predictor ofincident CV disease and mortality, and evidence suggeststhat exercise training, when conducted in individualswith higher baseline inflammation, or which results ineven a slight amount of weight reduction, is beneficialfor reducing inflammatory burden.32 Moreover, higherlevels of CRF are inversely associated with inflammationas measured by white blood cell count as, for example,in one study of 103 men with the metabolic syndromethose with low CRF had a 13.5% higher white blood cellcount compared to those with high CRF.33 While thismay partially explain the CRF-mediated uncoupling ofBMI and mortality risk, the relationship between adipose
tissue-derived inflammatory cytokines and CV risk is notwell understood.34
Another CV risk factor influenced by CRF is hyperten-sion. Exercise training is known to reduce resting systolicand diastolic blood pressure in hypertensive adults dueto several neurohormonal adaptations including lowerlevels of plasma norepinephrine, renin, and angiotensin.35
However, results from a meta-analysis of randomizedcontrol trials indicate only a modest reduction of ~4 mmHg in systolic blood pressure in response to short-term(<6 months) exercise training.36 It is uncertain, therefore,whether blood pressure plays a significant role in theCRF-mediated alteration of the obesity paradox.
Finally, higher CRF is associated with favorable changes inblood lipids and blood glucose. Wei and colleagues37 exam-ined the effect of exercise on blood lipids in 780 active men inthe ACLS during a 1-year period. Compared to men who didnot change their exercise routine, men who increased theirexercise had a significantly greater increase in high-densitylipoprotein cholesterol (mean 4.76 versus 2.83 mg/dL,p < 0.005) and a significantly greater decrease in triglycerides(mean −18.2 versus −6.27 mg/dL, p < 0.001). Exercise traininghas been shown to increase lipoprotein lipase activity inskeletal muscle resulting in a decrease in plasmatriglycerides.38 Recent animal studies have shed further lighton the underlying mechanisms for better glucose regulationfollowing regular exercise training, in particular, the training-induced increase in insulin receptor substrate (IRS) protein39
and glucose transporter (GLUT)-4.40 However, further study isneeded to examine the extent to which favorable changes inblood chemistry after exercise training can explain the CRF-mediated alteration of the obesity paradox.
Conclusions
Mounting evidence suggests that CRF modifies the associationbetween adiposity and mortality. In the general population,higher CRF is associated with improvements in obesity-related

439P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S E S 5 6 ( 2 0 1 4 ) 4 3 4 – 4 4 0
cardiometabolic risk factors resulting in improved survivalcomparable to fit and normal-weight individuals. However, inpatients with established CV disease, in whom an obesityparadox exists, higher CRF reduces CV disease mortalityassociated with normal weight. The mechanisms underlyingthis effect may be due to modification of one or more of the CVdisease risk factors, or may simply reflect a better state ofgeneral health. Data summarized here suggest that CRF largelyexplains the obesity paradox in middle-aged and older menwith established CV disease. Future research should aim tocharacterize the CV disease-specific impact of CRF on theobesity paradox in diverse populations of men and women.
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest.
Acknowledgments
The authors have no relevant conflict of interest to disclose.
R E F E R E N C E S
1. Wei M, Kampert JB, Barlow CE, et al. Relationship between lowcardiorespiratory fitness and mortality in normal-weight,overweight, and obese men. JAMA. 1999;282:1547-1553.
2. Lee CD, Blair SN, Jackson AS. Cardiorespiratory fitness, bodycomposition, and all-cause and cardiovascular disease mor-tality in men. Am J Clin Nutr. 1999;69:373-380.
3. McAuley PA, Blair SN. Obesity paradoxes. J Sports Sci. 2011;29:773-782.
4. Fogelholm M. Physical activity, fitness and fatness: relationsto mortality, morbidity and disease risk factors. A systematicreview. Obes Rev. 2010;11:202-221.
5. Gruberg L, Weissman NJ, Waksman R, et al. The impact ofobesity on the short-term and long-term outcomes afterpercutaneous coronary intervention: the obesity paradox?J Am Coll Cardiol. 2002;39:578-584.
6. Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovasculardisease: risk factor, paradox, and impact of weight loss. J AmColl Cardiol. 2009;53:1925-1932.
7. Lainscak M, von Haehling S, Doehner W, et al. The obesityparadox in chronic disease: facts and numbers. J CachexiaSarcopenia Muscle. 2012;3:1-4.
8. Gielen S, Sandri M. The obesity paradox—a scientific artifact?Int J Cardiol. 2013;162:140-142.
9. Lavie CJ, De Schutter A, Patel DA, et al. Does fitnesscompletely explain the obesity paradox? Am Heart J. 2013;166:1-3.
10. Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitnessas a quantitative predictor of all-cause mortality and cardio-vascular events in healthy men and women: a meta-analysis.JAMA. 2013;301:2024-2035.
11. Ekelund LG, Haskell WL, Johnson JL, et al. Physical fitness as apredictor of cardiovascular mortality in asymptomatic NorthAmerican men. The Lipid Research Clinics Mortality Follow-up Study. N Engl J Med. 1988;319:1379-1384.
12. Gupta S, Rohatgi A, Ayers CR, et al. Cardiorespiratory fitnessand classification of risk of cardiovascular disease mortality.Circulation. 2011;123:1377-1383.
13. Blair SN, Kohl III HW, Paffenbarger Jr RS, et al. Physical fitnessand all-cause mortality. A prospective study of healthy menand women. JAMA. 1989;262:2395-2401.
14. Myers J, Prakash M, Froelicher V, et al. Exercise capacity andmortality among men referred for exercise testing. N Engl JMed. 2002;346:793-801.
15. Lavie CJ, Swift DL, Johannsen NM, et al. Physical fitness: anoften forgotten cardiovascular risk factor. J GlycomicsLipidomics. 2012;2:e104.
16. Lavie CJ, Cahalin LP, Chase P, et al. Impact of cardiorespiratoryfitness on the obesity paradox in patients with heart failure.Mayo Clin Proc. 2013;88:251-258.
17. Uretsky S, Supariwala A, Gurram S, et al. The interaction ofexercise ability and body mass index upon long-termoutcomes among patients undergoing stress–rest perfusionsingle-photon emission computed tomography imaging. AmHeart J. 2013;166:127-133.
18. Lee DC, Sui X, Artero EG, et al. Long-term effects of changesin cardiorespiratory fitness and body mass index on all-cause and cardiovascular disease mortality in men: theAerobics Center Longitudinal Study. Circulation. 2011;124:2483-2490.
19. Lee DC, Sui X, Church TS, et al. Changes in fitness andfatness on the development of cardiovascular diseaserisk factors hypertension, metabolic syndrome, andhypercholesterolemia. J Am Coll Cardiol. 2012;59:665-672.
20. Kaminsky LA, Arena R, Beckie TM, et al. The importance ofcardiorespiratory fitness in the United States: the need for anational registry: a policy statement from the American HeartAssociation. Circulation. 2013;127:652-662.
21. Johnson NP, Wu E, Bonow RO, et al. Relation of exercisecapacity and body mass index to mortality in patients withintermediate to high risk of coronary artery disease. Am JCardiol. 2008;102:1028-1033.
22. McAuley PA, Kokkinos PF, Oliveira RB, et al. Obesity paradoxand cardiorespiratory fitness in 12,417 male veterans aged 40to 70 years. Mayo Clin Proc. 2010;85:115-121.
23. Goel K, Thomas RJ, Squires RW, et al. Combined effect ofcardiorespiratory fitness and adiposity on mortality inpatients with coronary artery disease. Am Heart J. 2011;161:590-597.
24. McAuley PA, Artero EG, Sui X, et al. The obesity paradox,cardiorespiratory fitness, and coronary heart disease. MayoClin Proc. 2012;87:443-451.
25. McAuley P, Myers J, Abella J, Froelicher V. Body mass, fitnessand survival in veteran patients: another obesity paradox? AmJ Med. 2007;120:518-524.
26. Sui X, LaMonte MJ, Blair SN. Cardiorespiratory fitnessas a predictor of nonfatal cardiovascular events inasymptomatic women and men. Am J Epidemiol. 2007;165:1413-1423.
27. Després JP. Body fat distribution and risk of cardiovasculardisease: an update. Circulation. 2012;126:1301-1313.
28. Church TS, Kuk JL, Ross R, et al. Association ofcardiorespiratory fitness, body mass index, and waistcircumference to nonalcoholic fatty liver disease.Gastroenterology. 2006;130:2023-2030.
29. McAuley PA, Sui X, Church TS, et al. The joint effects ofcardiorespiratory fitness and adiposity on mortality riskin men with hypertension. Am J Hypertens. 2009;22:1062-1069.
30. Johnson NA, Sachinwalla T, Walton DW, et al. Aerobicexercise training reduces hepatic and visceral lipids in obeseindividuals without weight loss. Hepatology. 2009;50:1105-1112.
31. Kershaw EE, Flier JS. Adipose tissue as an endocrine organ.J Clin Endocrinol Metab. 2004;89:2548-2556.

440 P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S E S 5 6 ( 2 0 1 4 ) 4 3 4 – 4 4 0
32. Beavers KM, Brinkley TE, Nicklas BJ. Effect of exercise trainingon chronic inflammation. Clin Chim Acta. 2010;411:785-793.
33. Rana JS, Nasir K, Santos RD, et al. Increased level ofcardiorespiratory fitness blunts the inflammatory response inmetabolic syndrome. Int J Cardiol. 2006;110:224-230.
34. Unger RH, Scherer PE. Gluttony, sloth and the metabolicsyndrome: a roadmap to lipotoxicity. Trends Endocrinol Metab.2010;21:345-352.
35. Pescatello LS, Franklin BA, Fagard R, et al. Exercise andhypertension. Med Sci Sports Exerc. 2004;36:533-553.
36. Whelton SP, Chin A, Xin X, He J. Effect of aerobic exercise onblood pressure: a meta-analysis of randomized, controlledtrials. Ann Intern Med. 2002;136:493-503.
37. Wei M, Macera CA, Hornung CA, et al. Changes in lipidsassociated with change in regular exercise in free-living men.J Clin Epidemiol. 1997;50:1137-1142.
38. Budohoski L. Exercise-induced changes in lipoprotein lipaseactivity (LPLA) in skeletal muscles of the dog. Pflugers Arch.1985;405:188-192.
39. Hoene M, Lehmann R, Hennige AM. Acute regulation ofmetabolic genes and insulin receptor substrates in the liver ofmice by one single bout of treadmill exercise. J Physiol.2009;587(Pt 1):241-252.
40. Deshmukh AS, Hawley JA, Zierath JR. Exercise-inducedphospho-proteins in skeletal muscle. Int J Obes (Lond).2008;32(Suppl 4):S18-S23.