Embed Size (px)
Citation preview
Volume 114
Number 3 Distal coronary pressure and collaterals
artery collateral visualization during acute coronary occlu- sion.t\m J Cardiol 1985;55:1216. -
16. Wahr DW. Ports TA. Botvinick EH. Dae M. Schechtmann N. Huberty J; Hattner RS, O’Connell JW, Turkey K. The effects of coronary angioplasty and reperfusion on distribution of myocardial flow. Circulation 1985;72:334.
17. Arani DT, Greene DG, Bunnell IL, Smith GL, Klocke FJ. Reductions in coronary flow under resting conditions in collateral-dependent myocardium of patients with complete occlusion of the left anterior descending coronary artery. J Am Co11 Cardiol 1984;3:668.
18. Canty JM, Klocke FJ. Reduced regional myocardial perfu-
sion in the presence of pharmacologic vasodilator reserve. Circulation 1985;71:370.
19. Aversano T. Becker LC. Persistence of coronarv vasodilator reserve desdite functionally significant flow reduction. Am J Physiol 1985;248(Heart Circ Physiol 17):H403.
20. MacDonald RG, Hill JA, Feldman RL. ST segment response to coronary occlusion: Dependence on collateral function. J Am Co11 Cardiol 1986;7:192A.
‘21. Busch UW, Sebening H, Beeretz R, Heinze R. Reliability of pressure recordings via catheters used for transluminal coro- nary angioplasty. Tex Heart Inst J 1984;11:160.
Contrast perfusion echocardiography: Identification of area at risk of dyskinesis during percutaneous transluminal coronary angioplasty
Two-dimensional contrast perfusion echocardiography was performed in 14 patients who underwent percutaneous transiuminai coronary angiopiasty to test the efficacy of this new technique for defining the area at risk of dyskinesis during acute coronary occlusion. in nine patients (group A) selective coronary injection of echocontrast medium through the central lumen of the angiopiasty catheter was performed immediately before balloon inflation. This produced regional myocardiai enhancement that defined the area of dyskinesis after balloon inflation. in five patients (group B) who underwent left coronary angiopiasty, echocontrast medium was injected through the introducer catheter positioned in the left main coronary artery during balloon inflation. in each case this produced regional myocardiai enhancement remote from the area of dyskinesis. There were no complications related to the intracoronary echocontrast injections, which produced no discernible exacerbation of chest pain or left ventricular contractile dysfunction. These data indicate that selective coronary injection of echocontrast medium defines the perfusion territory of the artery injected and also provides a means of identifying the area at risk of dyskinesis after balloon occlusion of the artery. (AM HEART J 1987;114:497.)
Brian Griffin, M.B., M.R.C.P.I., Adam D. Timmis, M.D., M.R.C.P., Robert A. Henderson, M.B., M.R.C.P., and Edgar Sowton, M.D., F.R.C.P. London, England
Contrast perfusion echocardiography is a new tech- nique that in animal studies has been shown to
t define the area at risk of infarction after acute coronary occlusion. l-* Recent studies in humans have indicated that this technique defines the perfusion territory of normal coronary arteries without serious
From the Department of Cardiology, Guy’s Hospital.
Received for publication Oct. 21, 1986, accepted April 3, 1987.
Reprint requests: Brian Griffin, M.B., M.R.C.P.I., Department of Cardiol- ogy, Guy’s Hospital, St. Thomas St., London SE1 9RT.
adverse effects.5p6 Percutaneous transluminal coro- nary angioplasty provides a useful human model of acute coronary occlusion. In this study we have applied contrast perfusion echocardiography during angioplasty to test the efficacy of this new technique for defining the area of dyskinesis after balloon occlusion of the coronary artery. Therefore, the aim of this study is entirely different from that reported by Lang et al.,7 who examined the potential of coronary angioplasty to improve regional myocardi- al perfusion by performing contrast perfusion echo- cardiography before and after the procedure. Our
497
498 Griffin et al. September 1987
American Heart Journal
Table I. Patient details
Patient Age (Yr) Sex
NYHA
functional class
Diseased vessels
(% stenosis) Vessel Echo
LAD CX RCA for PTCA window
Group A 1 2 3
4 5
6
8 9
Group B
2 3
4
5
50 M 28 M 43 M 64 M 59 M 43 M 54 M 52 M 73 M
53 M 63 M 55 M
66 M 62 M
3 4 4
3
0 70
80 0
0 90
0 0
95
80 95
70*
70t 0
70t
0 0
80 0 0
70 0 0
0 0
0
80 0
RCA PSA LAD A4C LAD A4C cx PSAIAIC RCA PSA LAD LA CX PSA RCA PSA LAD A4C
LAD PSA LAD A4C LAD A4C
cx A4C LAD A4C
NYHA = New York Heart Association; LAD = left anterior descending coronary artery; Cx = circumflex coronary artery; RCA = right coronary artery; percutaneous transluminal coronary angioplasty; PSA = parasternal short axis; A4C = apical four chamber; LA = long axis. *Proximal stenosis. tDista1 stenosis.
own study concentrates exclusively on events during balloon occlusion of the coronary artery.
METHODS
Patients. Fourteen patients undergoing elective single- vessel coronary angioplasty were studied. Ail patients gave informed consent for inclusion in the study, which had received the approval of the hospital ethical committee. The patients were men aged 55 f 11 (SD) years. All had single-vessel disease except one patient with double-vessel disease in whom the right coronary artery was occluded. Coronary stenoses (>70%) were proximal in all but two patients, both of whom had left anterior descending disease. In one of these patients the stenosis was located distally whereas in the other both proximal and distal stenoses were present. Stenoses were in the left anterior descending coronary artery in eight cases, the right coro- nary artery in three cases, and the circumflex coronary artery in three cases. In none of the patients did the preangioplasty arteriogram show evidence of collateral flow sufficient to opacify the distal portion of the treated artery.
Protocol. After completion of the penultimate balloon inflation of the angioplasty procedure the patients were divided arbitrarily into two groups, A and B. In every case the transstenotic pressure gradient had been reduced to 15 mm Hg or less except for the patient with double left anterior descending stenoses in whom the distal lesion was dilated first. In group A (nine patients) the guide wire was removed from the balloon catheter and 2 ml echo- contrast was injected down its central lumen into the distal coronary artery. The area of myocardial con-
trast enhancement was monitored by two-dimensional echocardiography with videotape recording. Immediately after the contrast injection the balloon was inflated for a period of 60 seconds. Echocardiographic monitoring con- tinued throughout this period of balloon inflation and during the recovery period to identify areas of regional dyskinesis.
Group B consisted of five patients undergoing left anterior descending (n = 4) and circumflex (n = 1) coro- nary angioplasty. During the final balloon inflation of the angioplasty procedure, 2 ml echocontrast was injected through the introducer catheter, which was positioned in the left main coronary artery. Two-dimensional echocar- diography permitted identification of myocardial contrast enhancement and regional dyskinesis. In one patient with double left anterior descending coronary stenoses contrast injections were made during dilatation of each of the stenoses.
AnQlOplsSty procedure. All procedures were performed by modified Judkins’ technique from the right femoral artery. After introduction of the introducer catheter into the orifice of the coronary artery, a 3.0 mm balloon (SciMed Life Systems Inc, Minneapolis, Minn.) was posi- tioned across the coronary stenosis with a steerable guide wire. Intermittent 60-second balloon inflations were con- tinued until the transstenotic pressure gradient had been reduced to 15 mm Hg or less. Details of drug regimens have been reported previously.s
Echocontrast medium. A 50% solution of Urografin 370 and normal saline was hand agitated for at least 2 minutes. This provided the echocontrast medium, 2 ml of which was used for each contrast injection.

Volume 114
Number 3 Contrast perfusion echocardiography during PTCA 499
-
Area of contrast Area of
enhancement dyskinesis
Inferoseptum Septum Septum Lateral wall Inferoseptum Septum Lateral wall Inferoseptum Septum
Inferoseptum Septum Septum Lateral wall Inferoseptum Septum Lateral wall Inferoseptum Septum
Inferolateral wall Lateral wall Lateral wall Upper septum and lateral wall Septum Upper septum and lateral wall
Anteroseptum Septum-apex Septum-apex Lower septum-apex Lateral wall Lower septum-apex
Echocardiography. A two-dimensional scanner (Hew- lett-Packard Co., Palo Alto, Calif.) was used to record ultrasound signals. Before the angioplasty procedure the patients were examined in the supine position to deter- mine the most satisfactory ultrasound window. For all right coronary artery procedures the parasternal short axis window at papillary muscle level was used. For circumflex and left anterior descending coronary artery procedures any of the parasternal short-axis, parasternal long-axis, or apical four-chamber windows were used. All ultrasound images were recorded on videotape.
The area of myocardial enhancement after echocontrast injection and the area of dyskinesis during balloon infla- tion were determined qualitatively by consensus among two observers. Dyskinesis was defined as absence of systolic thickening of the myocardium. Particular atten- tion was directed toward establishing the degree of con- cordance (in group A) or discordance (in group B) between areas of myocardial contrast enhancement and dyskine- sis.
RESULTS
Individual data are shown in Table I, which shows the area of myocardial enhancement after coronary injection of echocontrast medium and the area of dyskinesis during inflation of the angioplasty bal- loon. In every case the procedures were completed without complication. None of the patients had symptoms as a result of the echocontrast injec- tions.
Group A. Selective injection of echocontrast medi- um through the central lumen of the angioplasty catheter produced regional myocardial enhance-
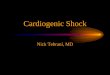
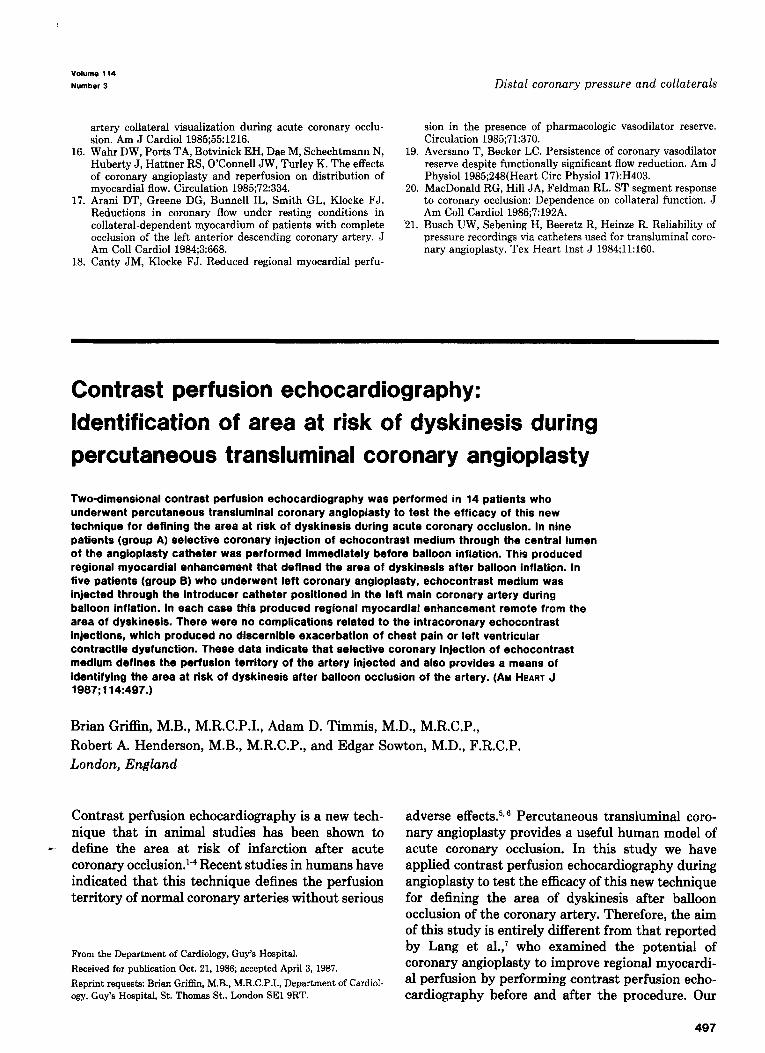
ment in the predicted distribution of the artery injected. Thus left anterior descending and circum- flex coronary artery injections always enhanced the septum and lateral wall of the left ventricle, respec- tively (Figs. 1 and 2). Right coronary artery injec- tions enhanced the inferoseptal wall of the left ventricle. After inflation of the angioplasty balloon, dyskinesis developed in the area of myocardial contrast enhancement. In every case the area of dyskinesis was confined to and defined by the area of contrast enhancement. In every case, myocardial enhancement and dyskinesis regressed rapidly after deflation of the balloon. Left ventricular dyskinesis was most marked during left anterior descending coronary angioplasty. During one procedure the septal papillary muscle, which had become enhanced after echocontrast injection, was seen to prolapse during balloon inflation.
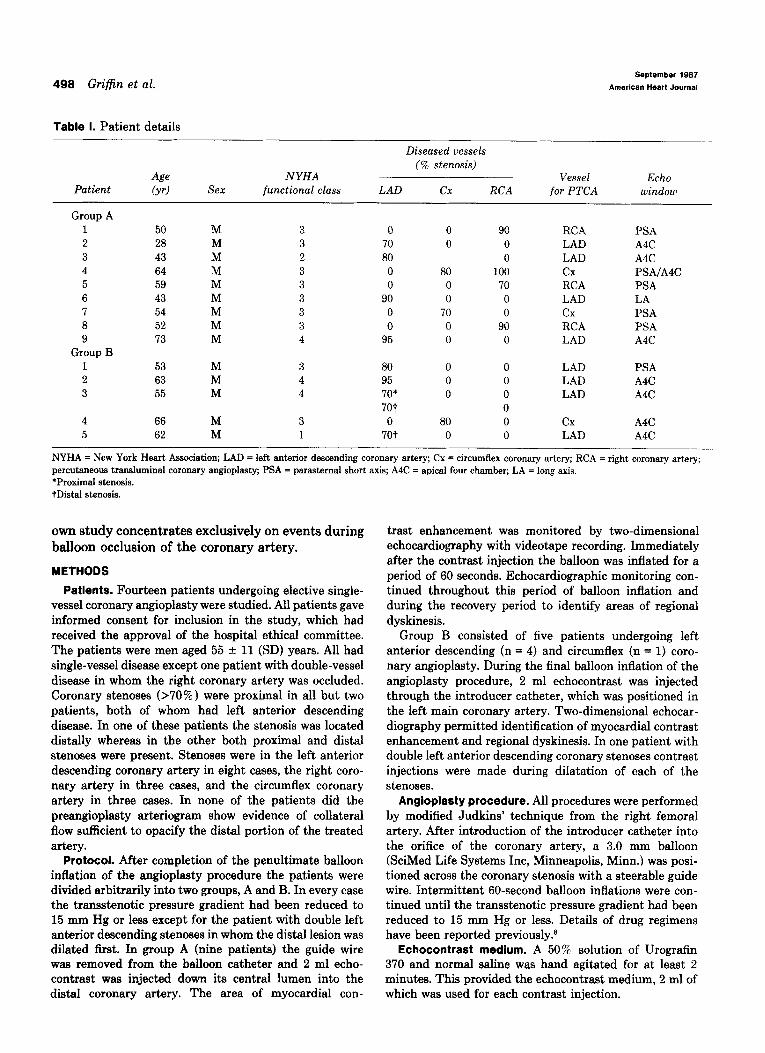
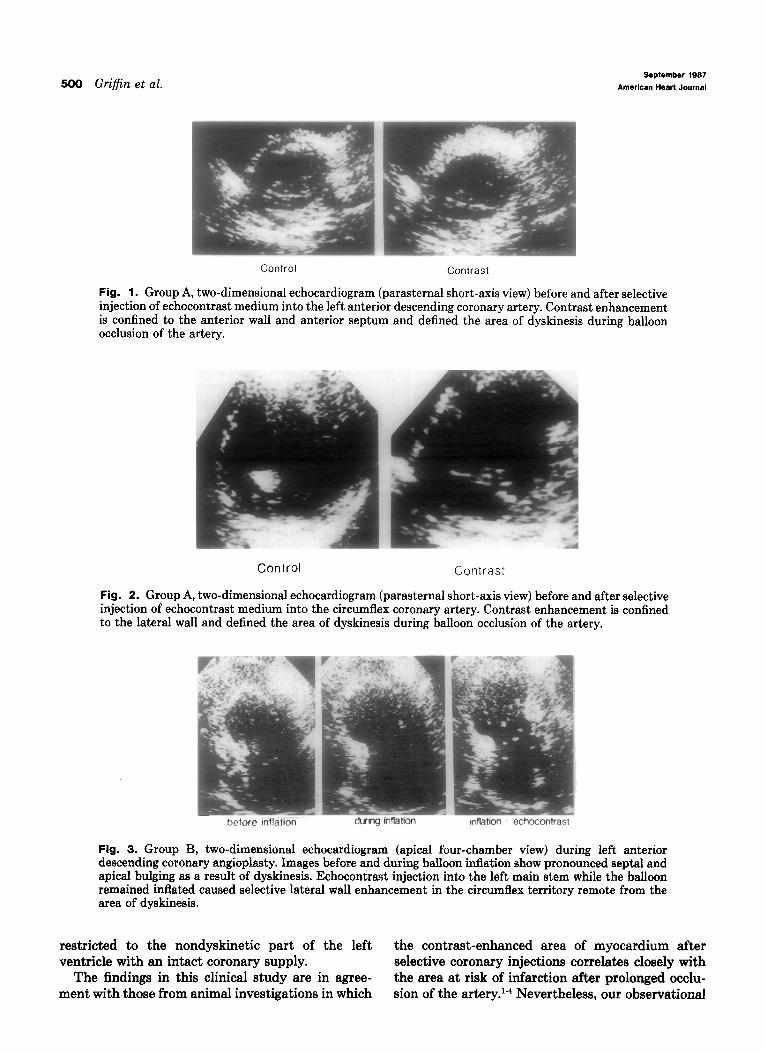
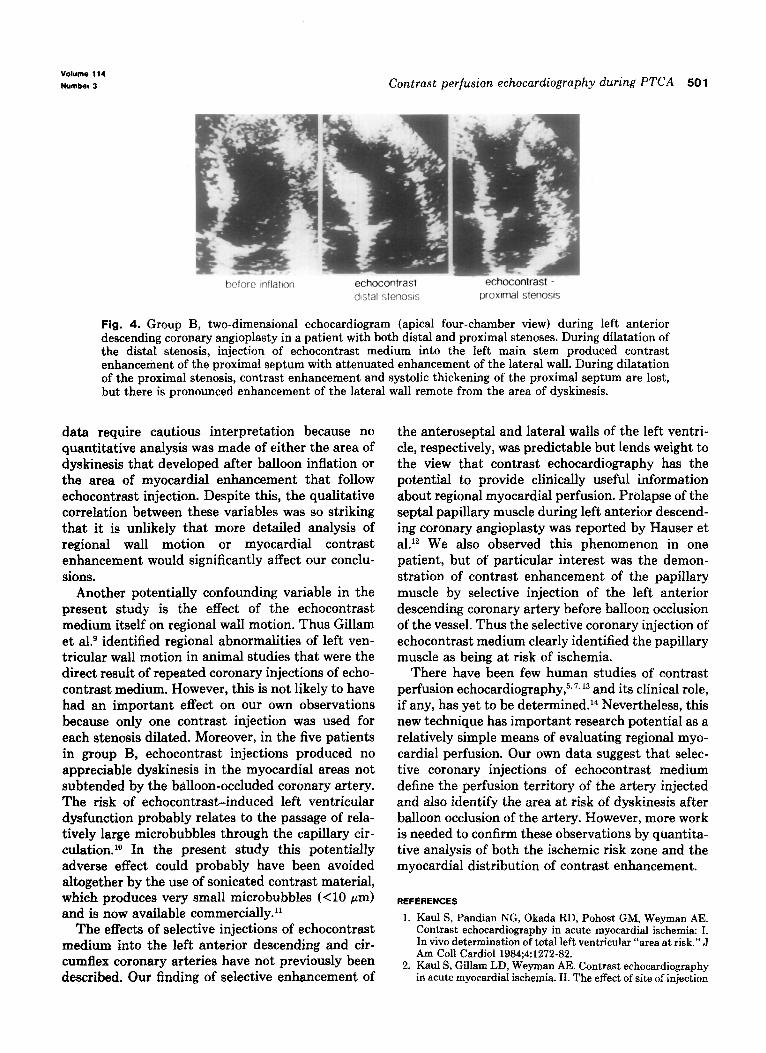
Group 6. During balloon inflation, echocontrast medium was injected through the introducer cathe- ter positioned in the left main coronary artery. In the patient with circumflex disease this produced selective enhancement of the septal and apical myo- cardium remote from the dyskinetic lateral wall, which showed no contrast enhancement. On the other hand, in the patients with left anterior descending disease, contrast injections produced selective enhancement of the lateral wall of the left ventricle whereas dyskinesis was confined to the septal or apical areas (Fig. 3). Nevertheless, the two patients with distal left anterior descending stenoses also showed enhancement of the proximal part of the septum, which continued to thicken normally during balloon inflation. Interestingly, in one of these patients who had double stenoses, there was no contrast enhancement of the septum during dilatation of the stenosis proximal to the first septal branch (Fig. 4).
DISCUSSION
This article presents clinical observations on the use of contrast perfusion echocardiography during balloon occlusion of a coronary artery. The data indicate that the area of myocardial enhancement after selective coronary injection of echocontrast medium defines the perfusion territory of that artery. Thus after balloon occlusion of the artery, the area of dyskinesis is confined to and defined by the area of myocardial enhancement, which proba- bly, therefore, identifies the area at risk of infarc- tion. Moreover, when echocontrast medium is injected into the left main coronary artery after balloon occlusion of one or another of its major branches, myocardial contrast enhancement is
500 Griffin et al. September 1987
American Heart Journal
Control Contrast
Fig. 1. Group A, two-dimensional echocardiogram (parasternal short-axis view) before and after selective injection of echocontrast medium into the left anterior descending coronary artery. Contrast enhancement is confined to the anterior wall and anterior septum and defined the area of dyskinesis during balloon occlusion of the artery.
Control Contrast
Fig. 2. Group A, two-dimensional echocardiogram (parasternal short-axis view) before and after selective injection of echocontrast medium into the circumflex coronary artery. Contrast enhancement is confined to the lateral wall and defined the area of dyskinesis during balloon occlusion of the artery.
Fig. 3. Group B, two-dimensional echocardiogram (apical four-chamber view) during left anterior descending coronary angioplasty. Images before and during balloon inflation show pronounced septal and apical bulging as a result of dyskinesis. Echocontrast injection into the left main stem while the balloon remained inflated caused selective lateral wall enhancement in the circumflex territory remote from the area of dyskinesis.
restricted to the nondyskinetic part of the left the contrast-enhanced area of myocardium after ventricle with en intact coronary supply. selective coronary injections correlates closely with
The findings in this clinical study are in agree- the erea at risk of infarction after prolonged occlu- ment with those from animal investigations in which sion of the artery. l-4 Nevertheless, our observational
vOlume 114
Number 3 Contrast perfusion echocardiography during PTCA 501
belore mflaton echocontrast - echocontrast -
distal slenosfs poxfmal stenosis
Fig. 4. Group B, two-dimensional echocardiogram (apical four-chamber view) during left anterior descending coronary angioplasty in a patient with both distal and proximal stenoses. During dilatation of the distal stenosis, injection of echocontrast medium into the left main stem produced contrast enhancement of the proximal septum with attenuated enhancement of the lateral wall. During dilatation of the proximal stenosis, contrast enhancement and systolic thickening of the proximal septum are lost, but there is pronounced enhancement of the lateral wall remote from the area of dyskinesis.
data require cautious interpretation because no quantitative analysis was made of either the area of dyskinesis that developed after balloon inflation or the area of myocardial enhancement that follow echocontrast injection. Despite this, the qualitative correlation between these variables was so striking that it is unlikely that more detailed analysis of regional wall motion or myocardial contrast enhancement would significantly affect our conclu- sions.
Another potentially confounding variable in the present study is the effect of the echocontrast medium itself on regional wall motion. Thus Gillam et al9 identified regional abnormalities of left ven- tricular wall motion in animal studies that were the direct result of repeated coronary injections of echo- contrast medium. However, this is not likely to have had an important effect on our own observations because only one contrast injection was used for each stenosis dilated. Moreover, in the five patients in group B, echocontrast injections produced no appreciable dyskinesis in the myocardial areas not subtended by the balloon-occluded coronary artery. The risk of echocontrast-induced left ventricular dysfunction probably relates to the passage of rela- tively large microbubbles through the capillary cir- culation.sO In the present study this potentially adverse effect could probably have been avoided altogether by the use of sonicated contrast material, which produces very small microbubbles (<lo pm) and is now available commercially.”
The effects of selective injections of echocontrast medium into the left anterior descending and cir- cumflex coronary arteries have not previously been described. Our finding of selective enhancement of
the anteroseptal and lateral walls of the left ventri- cle, respectively, was predictable but lends weight to the view that contrast echocardiography has the potential to provide clinically useful information about regional myocardial perfusion. Prolapse of the septal papillary muscle during left anterior descend- ing coronary angioplasty was reported by Hauser et a1.12 We also observed this phenomenon in one patient, but of particular interest was the demon- stration of contrast enhancement of the papillary muscle by selective injection of the left anterior descending coronary artery before balloon occlusion of the vessel. Thus the selective coronary injection of echocontrast medium clearly identified the papillary muscle as being at risk of ischemia.
There have been few human studies of contrast perfusion echocardiography,5s7* l3 and its clinical role, if any, has yet to be determined.14 Nevertheless, this new technique has important research potential as a relatively simple means of evaluating regional myo- cardial perfusion. Our own data suggest that selec- tive coronary injections of echocontrast medium define the perfusion territory of the artery injected and also identify the area at risk of dyskinesis after balloon occlusion of the artery. However, more work is needed to confirm these observations by quantita- tive analysis of both the ischemic risk zone and the myocardial distribution of contrast enhancement.
REFERENCES
1. Kaul 8, Pandian NG, Okada RD, Pohost GM, Weyman AE. Contrast echocardiography in acute myocardial ischemia: I. In viva determination of total left ventricular “area at risk.” J Am Co11 Cardiol 1984;4:1272-82.
2. Kaul s, Gillam LD, Weyman AE. Contrast echocardiography in acute myocardial ischemia. II. The effect of site of injection

502 Griffin et al.
3.
4.
5.
6.
I.
8.
of contrast agent on the estimation of area at risk for necrosis after coronary occlusion. J Am Co11 Cardiol 1985;6:825-30. Kaul S, Pandian NG, Gillam LD, Newell JB, Okada RD, Weyman AE. Contrast echocardiography in acute myocardial ischemia. III. An in vivo comparison of the extent of abnor- mal wall wall motion with the area at risk for necrosis. J Am Co11 Cardiol 1986;7:383-92. Kemper AJ, Force T, Perkins L, Gilfoil M, Parisi AF. In vivo prodiction of the transmural extent of experimental acute myocardial infarction using contrast echocardiography. J Am Co11 Cardiol 1986;8:143-9. Santoso T, Roelandt J, Manoyoer H, Abdurahmn N, Meltzer RS, Hughenholtz PG. Myocardial perfusion imaging in humans by contrast echocardiography using polygelin colloid solution. J Am Co11 Cardiol 1985;6:612-20. Moore CA, Smucker ML, Kaul S. Myocardial contrast echo- cardiography in humans. I. Safety-a comparison with rou- tine coronary arteriography. J Am Co11 Cardiol 1986;8:1066- 12. Lang RM, Feinstein SB, Feldman T, Neumann A, Kok CC, Borow KM. Contrast echocardiography for evaluation of myocardial perfusion: effects of coronary angioplasty. J Am Co11 Cardiol 1986;8:232-5. Sowton E, Timmis AD, Crick JCP, Griffin B, Yates AK, Deverall P. Early results after percutaneous transluminal coronary angioplasty in 400 patients. Br Heart J 1986;56:115- 20.
9.
10.
11.
12.
13.
14.
Gillam LD, Kaul S, Fallon JT, et al. Functional and patho- logic effects of multiple echocardiographic injections on the myocardium, brain and kidney. J Am Co11 Cardiol1985;6:687- 94. Feinstein SB, Ten Cate FJ, Zwehl W, et al. Two-dimensional contrast echocardiography. I. In vitro development and quan- titative analysis of echocontrast agents. J Am Co11 Cardiol 1984;3:14-20. Feinstein SB, Shark PM, Bing RJ, et al. Microbubble dynam- ics visualized in the intact capillary circulation. J Am Co11 Cardiol 1984;4:595-600. Hauser AM, Gangadharan V, Ramos RG, Gordon S, Timmis GC. Sequence of mechanical, electrocardiographic and clini- cal effects of repeated coronary artery occlusion in human beings: echocardiographic observations during coronary angioplasty. J Am Co11 Cardiol 1985;5:193-7. Goldman ME, Mindich BP. Intraoperative cardioplegic con- trast echocardiography for assessing myocardial perfusion during open heart surgery. J Am Co11 Cardiol 1984;4:1029- 34. Meerbaum S. Promise and status of myocardial contrast- enhanced two-dimensional echocardiography: delineation of ischemic risk zone and quantitation of myocardial perfusion defects. J Am Co11 Cardiol 1986;7:395-6.