Embed Size (px)
Citation preview

The Journal of the Irish Practice Nurses AssociationIssue 5 Volume 5 September / October 2012
CONTrACePTION ANd fAmIly PlANNINg
Caitriona Gaffney
ChIldhOOd fOOd Allergy: SOlvINg
The PuzzleRuth Charles
TwITTer – hOw TO fOllOwLisa Nolan
ASThmA IN ChIldreN
Niamh O Regan
ChOleSTerOl lOwerINg PlAN Part 2Linda Main
Are your patients at risk?
Pneumococcal DiseaseVaccinate your at-risk patients and those 65 years and over against serious pneumococcal disease.
08/12 IR00150b
age 65+
chronic lung, heart or renal
disease
weakenedimmunesystem
other at-risk groups*smoker
diabetes
Marketing authorisation holder: Sanofi Pasteur MSD Limited, Block A, Second Floor, Cookstown Court, Old Belgard Road, Tallaght, Dublin 24. Marketing authorisation number: PA 544/21/3 Legal category: POM
Information about adverse event reporting can be found at www.imb.ie. Adverse events and inadvertent vaccination during pregnancy should also be reported to Sanofi Pasteur MSD by calling 00 44 1628 785291.Further information is available on request or in the SPC.
* See Immunisation Guidelines for Ireland www.immunisation.ie
v is i t pneumo. ie
SPMSD1192 pneumovax reminder NIGP strip 90x210 v3.indd 1 07/09/2012 14:51

Multicentre, randomised, double-blind controlled study involving 1,072 free-living adults aged over 70 years of age consuming Actimel (2x100g) daily for 3 months. Reduction in the average duration per episode of common infectious diseases (CIDs) by 19% vs. control (p= 0.008) including rhinopharyngitis (p<0.001). Common infectious diseases include both upper respiratory and gastrointestinal tract infections.
Guillemard et al 2010 Actimel Group n=537Control Group n=535
Reduction in duration of Common Infectious Diseases2
Controlled pilot study involving 360 people over 60 years consuming Actimel (2x100g) daily for 3 weeks. Reduction in duration of winter infections by 20% vs. control (p=0.024). Winter infections include influenza syndromes, respiratory disease, ear, nose and throat pathologies, gastrointestinal syndromes.
Turchet et al 2003 Actimel Group n=180Control Group n=180
Reduction in duration of Winter infections1
10
2
345678910
7.0
Control Actimel10
2
345678910
8.77.0
Control Actimel
Tim
e (in
day
s) -20%
10
2
345678910
7.0
Control Actimel10
2
345678910
6.5
Actimel
Tim
e (in
day
s) 8.0
Control
-19%
Studies have shown that Danone Actimel®* may be beneficial, in older adults, in helping to reduce the duration of common winter infections such as gastrointestinal and upper respiratory tract infections.
For more information visit www.probioticsinpractice.ie
*Danone Actimel is a probiotic food containing the exclusive probiotic culture Lactobacillus casei DN 114 001. Danone Actimel helps strengthen the natural defences when consumed daily as part of a healthy diet & lifestyle. These studies are part of an overall body of scientific evidence on Danone Actimel (28 publications).
1 Turchet P, et al. Effect of fermented milk containing the probiotic Lactobacillus casei DN-114 001 on winter infections in free living elderly subjects: a randomised, controlled pilot study. J Nutr Health Aging 2003;7(2):75-77.
2 Guillemard E. et al. Consumption of a fermented dairy product containing the probiotic Lactobacillus casei DN-114 001 reduces the duration of respiratory infections in the elderly in a randomised controlled trial; Br J Nutr. 2010;103, 58–68.
A Support In Winter*

1
editorial
Annual conference – not to be missed
The IPNA are fast approaching its 12th annual conference and AGM which will be held on the 5th and 6th October in the Tullamore Court Hotel. The Cavan/Monaghan branch will host to this year’s conference and have chosen the theme ‘Empowering people in challenging times’.
The conference will open on Friday afternoon with three workshops on vascular assessment of the lower limb, ear irrigation and otoscopy examination and caring for patients on warfarin therapy. The workshops will focus on the practical elements of these subjects which practice nurses encounter on a daily basis and will be delivered by experienced practitioners.
The keynote speaker will address his personal experience of growing up with diabetes and will be delivered by Dr Tony O’Sullivan, a GP from Irishtown in Dublin. Saturday morning will open with an address from Ms Roisin Shortall, TD with responsibility for primary care. This will be followed by presentations on the menopause, chronic renal disease and rheumatoid arthritis. A number of awards will be presented throughout the conference which includes the return of the Practice Nurse of the Year Award. The pharmaceutical exhibition, is once again, well supported and provides practice nurses with up to date clinical knowledge and research.
The focus of the year’s conference on chronic illness is timely as there is a drive through the clinical care programmes to reorganise the delivery of chronic illness. People with any chronic illness require access to services which are timely and appropriate to enable them to become empowered in managing their condition. Many of these services are currently provided in secondary care which may not be the most appropriate setting. How and where these services are delivered will, no doubt, be the subject of many discussions. Will they be delivered through general practice, by nurse specialists from secondary care coming into the community or by some other means? Given the financial and resource restraints in the health service at the moment, health professionals will have to redefine and reorganise the way they currently deliver services in order to meet the growing demand of our aging population who are living longer and living with chronic illness. In general practice, we are seeing more and more patients being put on disease modifying drugs (DMARDS) which require regular monitoring and review. We are being encouraged to carry out screening such as spirometry to identify early COPD. Laboratories are now providing estimated glomerular filtration rate (eGFR) analysis as part of renal function analysis so as to identify early chronic kidney disease. Ultimately, this adds to an already bulging outpatient department in secondary care.
This year’s conference provides us with up to date clinical evidence in a number of chronic conditions and how we can best care for patients in primary care within our resources. As usual, the conference provides us with an opportunity to network and gain much needed support and friendship from our colleagues. Following the conclusion of the conference, the IPNA AGM takes place which I would encourage all members to attend. It is through such a forum, we can collectively continue to progress nursing in general practice.
Ruth Morrow

PREVENTIONSTROKE
Capsules containing 110 mg or 150 mg dabigatran etexilate (as mesilate) Action: Direct thrombin inhibitor Indication: Prevention of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation with one or more of the following risk factors: Previous stroke, transient ischemic attack, or systemic embolism (SEE); Left ventricular ejection fraction < 40 %; Symptomatic heart failure, ≥ New York Heart Association (NYHA) Class 2; Age ≥ 75 years; Age ≥ 65 years associated with one of the following: diabetes mellitus, coronary artery disease, or hypertension Dose and Administration: Renal function should be assessed by calculating CrCL prior to initiation to exclude patients with severe renal impairment (CrCL < 30 ml/min). Recommended daily dose 300 mg taken as one 150 mg capsule twice daily. Therapy should be continued long term. In case of intolerability to dabigatran, patients should be instructed to immediately consult their doctor. Elderly: Aged ≥ 80 years 220 mg taken as one 110 mg capsule twice daily; 75 – 80 years consider 220 mg taken as one 110 mg capsule twice daily. As renal impairment may be frequent in the elderly (> 75 years), assess renal function by calculating CrCL prior to initiation to exclude patients with severe renal impairment (CrCL < 30 ml/min). Renal function should also be assessed at least once a year or more frequently as needed in certain clinical situations when it is suspected that the renal function could decline or deteriorate. Patients with an increased risk of bleeding: closely monitor clinically looking for signs of bleeding or anaemia. Dose adjustment should be decided at the discretion of the physician, following assessment of the potential benefit and risk to an individual patient. A coagulation test may help identify increased risk patients. Patients with gastritis, esophagitis, or gastroesophageal reflux consider 220 mg taken as one 110 mg capsule twice daily due to the elevated risk of major gastro-intestinal bleeding. Renal impairment: contraindicated in severe renal impairment (CrCL < 30 ml/min); patients with renal impairment and a high risk of bleeding consider 220 mg taken as one 110 mg capsule twice daily. Close clinical surveillance is recommended in patients with renal impairment. As above assess renal function prior to initiation to exclude patients with severe renal impairment and assess renal function at least once a year or more frequently as needed. Concomitant verapamil 220 mg taken as one 110 mg capsule twice daily; Pradaxa and verapamil should be taken at the same time. No dose adjustment required but close clinical surveillance in patients < 50 kg. Not recommended if liver enzymes > 2 Upper Limit of Normal (ULN). If switching from Pradaxa to parenteral anticoagulant wait 12 hours after the last dose of Pradaxa; if switching from parenteral anticoagulants to Pradaxa then Pradaxa should be given 0-2 hours prior to the time that the next dose of the alternate therapy would be due, or at the time of discontinuation in case of continuous treatment; if switching from Pradaxa to VKA adjust the starting time of the VKA based on CrCL; if switching from VKA to Pradaxa stop VKA and give Pradaxa once INR <2.0. Cardioversion patients can stay on Pradaxa whilst being cardioverted. Not recommended aged < 18 years. Pradaxa should be swallowed whole with water, with or without food. Patients should be instructed not to open the capsule as this may increase the risk of bleeding. Contraindications: Hypersensitivity to any component; severe renal impairment (CrCL < 30 ml/min); active clinically significant bleeding; lesion or condition at significant risk of major bleeding such as current or recent gastrointestinal ulceration, presence of malignant neoplasms at high risk of bleeding, recent brain or spinal injury, recent brain, spinal or ophthalmic surgery, recent intracranial haemorrhage, known or suspected oesophageal varices, arteriovenous malformations, vascular aneurysms or major intraspinal or intracerebral vascular abnormalities; concomitant treatment with any other anticoagulant agent e.g. unfractionated heparin (UFH), low molecular weight heparins (enoxaparin, dalteparin etc), heparin derivatives (fondaparinux etc), oral anticoagulants (warfarin, rivaroxaban, apixaban etc) except under the circumstances of switching therapy to or from
Pradaxa or when UFH is given at doses necessary to maintain an open central venous or arterial catheter; hepatic impairment or liver disease expected to have any impact on survival; concomitant systemic ketoconazole, cyclosporine,
itraconazole, tacrolimus. Warnings and Precautions: Not recommended if liver enzymes > 2 ULN. Haemorrhagic risk: Close clinical surveillance (signs of bleeding or anaemia) is recommended throughout the treatment period, especially when haemorrhagic risk is increased or risk factors combined. Factors which may increase haemorrhagic risk: age ≥ 75 years; moderate renal impairment (CrCL 30 – 50 ml/min); P-glycoprotein inhibitor co-medication; body weight < 50 kg; acetylsalicylic acid (aspirin); NSAID; clopidogrel; selective serotonin re-uptake inhibitors (SSRIs) or selective serotonin norepinephrine re-uptake inhibitors (SNRIs); other drugs which may impair haemostasis; diseases/procedures associated with a risk of bleeding such as coagulation disorders, thrombocytopenia or functional platelet defects, recent biopsy, major trauma, bacterial endocarditis, esophagitis, gastritis or gastroesophageal reflux. The measurement of dabigatran related anticoagulation may be helpful to avoid excessive high exposure to dabigatran in the presence of additional risk factors. Patients who develop acute renal failure must discontinue Pradaxa. If severe bleeding occurs, discontinue treatment and investigate the source of the bleeding. Avoid or use with caution agents which may increase the risk of haemorrhage. The use of fibrinolytic agents for the treatment of acute ischemic stroke may be considered if the patient presents with a dTT, ECT or aPTT not exceeding the ULN according to the local reference range. Avoid concomitant administration with P-gp inducers. Patients on dabigatran etexilate who undergo surgery or invasive procedures are at increased risk for bleeding therefore surgical interventions may require the temporary discontinuation of dabigatran etexilate; prescribers should consult the Summary of Product Characteristics for further information. Procedures such as spinal anaesthesia may require complete haemostatic function. The risk of spinal or epidural haematoma may be increased in cases of traumatic or repeated puncture and by the prolonged use of epidural catheters. After removal of a catheter, an interval of at least 2 hours should elapse before the administration of the first dose of dabigatran etexilate; these patients require frequent observation for neurological signs and symptoms of spinal or epidural haematoma. Treat with caution patients at high surgical mortality risk and with intrinsic risk factors for thromboembolic events. Myocardial infarction. Contains Sunset Yellow (E110) which may cause allergic reactions. Interactions: Anticoagulants and antiplatelet aggregation agents; Strong P-gp inhibitors e.g. amiodarone, quinidine, verapamil, clarithromycin co-administration (close clinical surveillance); verapamil co-administration - reduce Pradaxa dose to 220 mg (see above); not recommended for concomitant treatment posaconazole, dronedarone, protease inhibitors including ritonavir and its combinations with other protease inhibitors; avoid with P-gp inducers e.g. rifampicin, St John’s wort, carbamazepine, phenytoin; SSRIs or SNRIs. Dabigatran etexilate and dabigatran are not metabolised by cytochrome CYP450 system, therefore related medicinal product interactions not expected. Pantoprazole and other proton-pump inhibitors (PPI) were co-administered with Pradaxa in clinical trials and concomitant PPI treatment did not appear to reduce the efficacy of Pradaxa. Ranitidine administration together with Pradaxa had no clinically relevant effect on the extent of absorption of dabigatran. Fertility, pregnancy and lactation: Avoid pregnancy during treatment. Do not use in pregnancy unless clearly necessary. Discontinue breast-feeding during treatment. Undesirable effects: Most commonly reported adverse reactions are bleedings occurring in total in approximately 16.5 % in patients with atrial fibrillation treated for the prevention of stroke and SEE. Common (≥ 1/100, <1/10): anaemia; epistaxis; gastrointestinal haemorrhage; abdominal pain; diarrhoea; dyspepsia; nausea; hepatic function abnormal/liver function test abnormal; genitourological haemorrhage (150 mg). Prescribers should consult the Summary of Product Characteristics for further information on side effects. Pack sizes: 110 mg 60 capsules 150 mg 60 capsules Legal category POM MA numbers: 110 mg EU/1/08/442/007 (60 capsules) 150 mg EU/1/08/442/011 (60 capsules) Marketing Authorisation Holder: Boehringer Ingelheim International GmbH, Binger Str. 173, D-55216 Ingelheim am Rhein, Germany. Prescribers should consult the Summary of Product Characteristics for full prescribing information. Additional information is available on request from Boehringer Ingelheim Ireland Ltd, Corrig Court, Corrig Road, Sandyford Business Estate, Dublin 18. Prepared in July 2012.
Prescribing Information (SPAF - Ireland) PRADAXA® (dabigatran etexilate)
For more information, including an educational pack, go to www.pradaxa.ie/SPAFeducationalpack or call the Pradaxa® information line on 1850 946100
References: 1. Boehringer Ingelheim. Pradaxa® 150mg hard capsules Summary of Product Characteristics. 2. Patel MR, Mahaffrey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011; 365:883-891. 3. Patel MR, Mahaffrey KW, Garg J, et al. Supplementary appendix to Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011; 365:883-891. 4. Boehringer Ingelheim. Pradaxa® 110mg hard capsules Summary of Product Characteristics. 5. Connolly S, Ezekowitz MD, et al. Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N Engl J Med 2009; 361:1139-1151. 6. Connolly S, Ezekowitz MD, et al. Newly identified events in the RE-LY trial. N Engl J Med 2010; 363:1875-1876.
Date of preparation: July 2012 Job code: IRE/DBG-121447d•
The only licensed oral anticoagulant to show superior efficacy to warfarin for prevention of both ischaemic and haemorrhagic stroke – Pradaxa® 150mg b.d.1-3
Pradaxa® is licensed for the prevention of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation with one or more risk factors.1,4
Pradaxa® 150mg b.d. Superior prevention of stroke and systemic embolism (p=0.0001) with similar rates of major bleeding vs warfarin.1,5,6
Pradaxa® 110mg b.d. Similar prevention of stroke and systemic embolism with significantly lower rates of major bleeding vs warfarin (p=0.003).4-6
19907 BIP SPAF - Brain Ad_NGP - Irish P4P.indd 1 13/08/2012 15:21

3
Issue 5 Volume 2 September / October2009
ContentsThe Journal of the Irish Practice Nurses Association
Nursing in General Practice is published by GreenCross Publishing, 7 Adelaide Court, Adelaide Road, Dublin 2. Tel: 4189799 Fax: 4789449Email: [email protected]
EDITORMaura Henderson
CONSULTING EDITORSDarina Lane and Ruth Morrow
COMMISSIONING EDITORJudith Leavy
DESIGNERBarbara Vasic
PUBLISHERSGraham CookeMaura Henderson
DisclaimerThe views expressed in Nursing in General Practice are not necessarily those of the publishers, editor or editorial advisory board. While the publishers, editor and editorial advisory board have taken every care with regard to accuracy of editorial and advertisement contributions, they cannot be held responsible for any errors or omissions contained.
Issue 5 Volume 5 September / October 2012
*GreenCross Publishing was established in 2007 and is jointly owned by Graham Cooke and Maura Henderson.
© Copyright GreenCross Publishing 2012The contents of Nursing in General Practice are protected by copyright. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form by any means – electronic, mechanical or photocopy recording or otherwise – whole or in part, in any form whatsoever for advertising or promotional purposes without the prior written permission of the editor or publishers
PREVENTIONSTROKE
Capsules containing 110 mg or 150 mg dabigatran etexilate (as mesilate) Action: Direct thrombin inhibitor Indication: Prevention of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation with one or more of the following risk factors: Previous stroke, transient ischemic attack, or systemic embolism (SEE); Left ventricular ejection fraction < 40 %; Symptomatic heart failure, ≥ New York Heart Association (NYHA) Class 2; Age ≥ 75 years; Age ≥ 65 years associated with one of the following: diabetes mellitus, coronary artery disease, or hypertension Dose and Administration: Renal function should be assessed by calculating CrCL prior to initiation to exclude patients with severe renal impairment (CrCL < 30 ml/min). Recommended daily dose 300 mg taken as one 150 mg capsule twice daily. Therapy should be continued long term. In case of intolerability to dabigatran, patients should be instructed to immediately consult their doctor. Elderly: Aged ≥ 80 years 220 mg taken as one 110 mg capsule twice daily; 75 – 80 years consider 220 mg taken as one 110 mg capsule twice daily. As renal impairment may be frequent in the elderly (> 75 years), assess renal function by calculating CrCL prior to initiation to exclude patients with severe renal impairment (CrCL < 30 ml/min). Renal function should also be assessed at least once a year or more frequently as needed in certain clinical situations when it is suspected that the renal function could decline or deteriorate. Patients with an increased risk of bleeding: closely monitor clinically looking for signs of bleeding or anaemia. Dose adjustment should be decided at the discretion of the physician, following assessment of the potential benefit and risk to an individual patient. A coagulation test may help identify increased risk patients. Patients with gastritis, esophagitis, or gastroesophageal reflux consider 220 mg taken as one 110 mg capsule twice daily due to the elevated risk of major gastro-intestinal bleeding. Renal impairment: contraindicated in severe renal impairment (CrCL < 30 ml/min); patients with renal impairment and a high risk of bleeding consider 220 mg taken as one 110 mg capsule twice daily. Close clinical surveillance is recommended in patients with renal impairment. As above assess renal function prior to initiation to exclude patients with severe renal impairment and assess renal function at least once a year or more frequently as needed. Concomitant verapamil 220 mg taken as one 110 mg capsule twice daily; Pradaxa and verapamil should be taken at the same time. No dose adjustment required but close clinical surveillance in patients < 50 kg. Not recommended if liver enzymes > 2 Upper Limit of Normal (ULN). If switching from Pradaxa to parenteral anticoagulant wait 12 hours after the last dose of Pradaxa; if switching from parenteral anticoagulants to Pradaxa then Pradaxa should be given 0-2 hours prior to the time that the next dose of the alternate therapy would be due, or at the time of discontinuation in case of continuous treatment; if switching from Pradaxa to VKA adjust the starting time of the VKA based on CrCL; if switching from VKA to Pradaxa stop VKA and give Pradaxa once INR <2.0. Cardioversion patients can stay on Pradaxa whilst being cardioverted. Not recommended aged < 18 years. Pradaxa should be swallowed whole with water, with or without food. Patients should be instructed not to open the capsule as this may increase the risk of bleeding. Contraindications: Hypersensitivity to any component; severe renal impairment (CrCL < 30 ml/min); active clinically significant bleeding; lesion or condition at significant risk of major bleeding such as current or recent gastrointestinal ulceration, presence of malignant neoplasms at high risk of bleeding, recent brain or spinal injury, recent brain, spinal or ophthalmic surgery, recent intracranial haemorrhage, known or suspected oesophageal varices, arteriovenous malformations, vascular aneurysms or major intraspinal or intracerebral vascular abnormalities; concomitant treatment with any other anticoagulant agent e.g. unfractionated heparin (UFH), low molecular weight heparins (enoxaparin, dalteparin etc), heparin derivatives (fondaparinux etc), oral anticoagulants (warfarin, rivaroxaban, apixaban etc) except under the circumstances of switching therapy to or from
Pradaxa or when UFH is given at doses necessary to maintain an open central venous or arterial catheter; hepatic impairment or liver disease expected to have any impact on survival; concomitant systemic ketoconazole, cyclosporine,
itraconazole, tacrolimus. Warnings and Precautions: Not recommended if liver enzymes > 2 ULN. Haemorrhagic risk: Close clinical surveillance (signs of bleeding or anaemia) is recommended throughout the treatment period, especially when haemorrhagic risk is increased or risk factors combined. Factors which may increase haemorrhagic risk: age ≥ 75 years; moderate renal impairment (CrCL 30 – 50 ml/min); P-glycoprotein inhibitor co-medication; body weight < 50 kg; acetylsalicylic acid (aspirin); NSAID; clopidogrel; selective serotonin re-uptake inhibitors (SSRIs) or selective serotonin norepinephrine re-uptake inhibitors (SNRIs); other drugs which may impair haemostasis; diseases/procedures associated with a risk of bleeding such as coagulation disorders, thrombocytopenia or functional platelet defects, recent biopsy, major trauma, bacterial endocarditis, esophagitis, gastritis or gastroesophageal reflux. The measurement of dabigatran related anticoagulation may be helpful to avoid excessive high exposure to dabigatran in the presence of additional risk factors. Patients who develop acute renal failure must discontinue Pradaxa. If severe bleeding occurs, discontinue treatment and investigate the source of the bleeding. Avoid or use with caution agents which may increase the risk of haemorrhage. The use of fibrinolytic agents for the treatment of acute ischemic stroke may be considered if the patient presents with a dTT, ECT or aPTT not exceeding the ULN according to the local reference range. Avoid concomitant administration with P-gp inducers. Patients on dabigatran etexilate who undergo surgery or invasive procedures are at increased risk for bleeding therefore surgical interventions may require the temporary discontinuation of dabigatran etexilate; prescribers should consult the Summary of Product Characteristics for further information. Procedures such as spinal anaesthesia may require complete haemostatic function. The risk of spinal or epidural haematoma may be increased in cases of traumatic or repeated puncture and by the prolonged use of epidural catheters. After removal of a catheter, an interval of at least 2 hours should elapse before the administration of the first dose of dabigatran etexilate; these patients require frequent observation for neurological signs and symptoms of spinal or epidural haematoma. Treat with caution patients at high surgical mortality risk and with intrinsic risk factors for thromboembolic events. Myocardial infarction. Contains Sunset Yellow (E110) which may cause allergic reactions. Interactions: Anticoagulants and antiplatelet aggregation agents; Strong P-gp inhibitors e.g. amiodarone, quinidine, verapamil, clarithromycin co-administration (close clinical surveillance); verapamil co-administration - reduce Pradaxa dose to 220 mg (see above); not recommended for concomitant treatment posaconazole, dronedarone, protease inhibitors including ritonavir and its combinations with other protease inhibitors; avoid with P-gp inducers e.g. rifampicin, St John’s wort, carbamazepine, phenytoin; SSRIs or SNRIs. Dabigatran etexilate and dabigatran are not metabolised by cytochrome CYP450 system, therefore related medicinal product interactions not expected. Pantoprazole and other proton-pump inhibitors (PPI) were co-administered with Pradaxa in clinical trials and concomitant PPI treatment did not appear to reduce the efficacy of Pradaxa. Ranitidine administration together with Pradaxa had no clinically relevant effect on the extent of absorption of dabigatran. Fertility, pregnancy and lactation: Avoid pregnancy during treatment. Do not use in pregnancy unless clearly necessary. Discontinue breast-feeding during treatment. Undesirable effects: Most commonly reported adverse reactions are bleedings occurring in total in approximately 16.5 % in patients with atrial fibrillation treated for the prevention of stroke and SEE. Common (≥ 1/100, <1/10): anaemia; epistaxis; gastrointestinal haemorrhage; abdominal pain; diarrhoea; dyspepsia; nausea; hepatic function abnormal/liver function test abnormal; genitourological haemorrhage (150 mg). Prescribers should consult the Summary of Product Characteristics for further information on side effects. Pack sizes: 110 mg 60 capsules 150 mg 60 capsules Legal category POM MA numbers: 110 mg EU/1/08/442/007 (60 capsules) 150 mg EU/1/08/442/011 (60 capsules) Marketing Authorisation Holder: Boehringer Ingelheim International GmbH, Binger Str. 173, D-55216 Ingelheim am Rhein, Germany. Prescribers should consult the Summary of Product Characteristics for full prescribing information. Additional information is available on request from Boehringer Ingelheim Ireland Ltd, Corrig Court, Corrig Road, Sandyford Business Estate, Dublin 18. Prepared in July 2012.
Prescribing Information (SPAF - Ireland) PRADAXA® (dabigatran etexilate)
For more information, including an educational pack, go to www.pradaxa.ie/SPAFeducationalpack or call the Pradaxa® information line on 1850 946100
References: 1. Boehringer Ingelheim. Pradaxa® 150mg hard capsules Summary of Product Characteristics. 2. Patel MR, Mahaffrey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011; 365:883-891. 3. Patel MR, Mahaffrey KW, Garg J, et al. Supplementary appendix to Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011; 365:883-891. 4. Boehringer Ingelheim. Pradaxa® 110mg hard capsules Summary of Product Characteristics. 5. Connolly S, Ezekowitz MD, et al. Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N Engl J Med 2009; 361:1139-1151. 6. Connolly S, Ezekowitz MD, et al. Newly identified events in the RE-LY trial. N Engl J Med 2010; 363:1875-1876.
Date of preparation: July 2012 Job code: IRE/DBG-121447d•
The only licensed oral anticoagulant to show superior efficacy to warfarin for prevention of both ischaemic and haemorrhagic stroke – Pradaxa® 150mg b.d.1-3
Pradaxa® is licensed for the prevention of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation with one or more risk factors.1,4
Pradaxa® 150mg b.d. Superior prevention of stroke and systemic embolism (p=0.0001) with similar rates of major bleeding vs warfarin.1,5,6
Pradaxa® 110mg b.d. Similar prevention of stroke and systemic embolism with significantly lower rates of major bleeding vs warfarin (p=0.003).4-6
19907 BIP SPAF - Brain Ad_NGP - Irish P4P.indd 1 13/08/2012 15:21
1 edITOrIAl
4 NewS
8 AdverTOrIAl
The ulTImATe ChOleSTerOl lOwerINg PlAN – PArT 2 linda main
IN PrACTICe
16 TwITTer fOr NurSeS – hOw TO fOllOw
Part 2 of our series on Twitter – how and who to
follow on twitter. lisa Nolan
revIewS
11 ChIldhOOd fOOd Allergy: SOlvINg The Puzzle There are numerous myths surrounding childhood allergy.
ruth Charles
18 CONTrACePTION ANd fAmIly PlANNINg
Family planning is essential to securing the well-being and autonomy of women while supporting the
health and development of communities Caitriona gaffney
23 ASThmA IN ChIldreN
Asthma is the most common chronic disease of childhood, and is defined as intermittent, reversible obstructive airway disease
Niamh O regan
AbSTrACTS
29 meN’S heAlTh
31 OSTeOPOrOSIS
32 PrOduCTS
33 CrOSSwOrd

4
newsNEC NEWS
IPNA Conference/Agm – 5th and 6th October 2012, Tullamore Court hotel Registrations will remain open until Friday 21st September and all Practice Nurses currently working in Ireland are invited to attend. Registration Form and Conference Programme can be printed from the IPNA website (from either ‘News’ or ‘Events’ pages). Exhibitors who require information about stands can send an e-mail to: [email protected]
Agm 2012Saturday 6th October 2012 at 2.30pm, Tullamore Court Hotel, Tullamore. Only current members may attend the AGM. Motions for AGM will be circulated by email and posted on the IPNA website as soon as they have been finalised.
IPNA AwArdS 2012Best of luck to all who entered the four IPNA Educational Awards that were offered this year. Winners will be announced at the IPNA Conference on 5th and 6th October.
NeC meeTINgS 2012 Friday 5th October 2012, Tullamore Court Hotel – time tbc.
NeC meeTINgS februAry, mAy & SePTember 2013 Dates will be posted on the IPNA website as soon as they have been confirmed.
IPNA IS NOw ON TwITTerTo complement existing IPNA communication channels, the IPNA now has a Twitter account. If you have a Twitter account you can fol-low the handle @PracticeNurses to receive IPNA news, reminders & useful information from other groups – directly to your timeline.
IPNA webSITeThe IPNA website, www.irishpracticenurses.ie is updated constantly, so please log-in regularly to get the latest news on study days, new posts in the Discussion boards and more…
Lisa Nolan. Tel: 042-9692403 email: [email protected]
Voting for new Nursing and Midwifery Board underwayVoting for the new Board, the Nursing and Midwifery Board of Ire-land – Bord Altranais agus Cnáimhseachais na hÉireann – will com-mence on September 19, 2012 and will run until October 1, 2012.
For the first time, this election will be held electronically, and nurses and midwives may cast their votes by going to www.nurs-ingboard.ie and clicking the ‘Board Election 2012’ button.
By now all registered nurses and midwives will have received vot-ing information and instructions, including a personal Voting Regis-tration Number (VRN) at the top of the voting instructions document. You need your VRN to vote – you will not be able to vote without it.
If you need a new VRN number issued to you, contact An Bord Altranais at [email protected] by 1pm on September 27, 2012. VRN numbers may only be reissued by post, so requests for reissue must be received by this date and time to allow for a postal response within the election deadline.
Nurses and midwives will now be able to vote eight members onto the Board. The categories are: General Nursing; Children’s Nursing; Psychiatric Nursing; Intellectual Disability Nursing; Midwifery; Public Health Nursing; Nurses / Midwives Educator; and Nurse engaged in the care of older persons.
For the purposes of this first election to our new Board, the new procedures advise that those persons to be elected into seats rep-resenting General Nursing practice, Psychiatric Nursing practice, and Midwifery practice must be engaged in clinical practice.
While the term is not defined in the procedures, clinical practice may be understood to encompass the delivery of direct care, which may also be delivered indirectly through the provision of advice, guidance, education, management, and leadership in nurs-ing and midwifery to clinical facilities.
Any candidate seeking a nomination under those categories requiring engagement in clinical practice must highlight their ex-perience of clinical practice. Indeed any nominee in any category will have to demonstrate how he or she is eligible for election in that category. If a nominee’s demonstration of eligibility satisfies the Returning Officer, then that nominee will be put forward for election. It then falls to voting registrants to elect Board members under each category as they see fit.
Women’s Aid – ‘Don’t be Afraid’ campaignWomen’s Aid, working to make women and children in Ireland safe from domestic violence for nearly 40 years, is currently run-ning it’s ‘Don’t Be Afraid’ national public awareness campaign to promote its National Freephone Helpline 1800 341 900. The Women’s Aid Helpline provides free, confidential support and information to women experiencing domestic violence any-where in the Republic of Ireland.
As part of this campaign, we will be distributing materials promoting our services widely to professionals who work with women experiencing domestic violence, and to other places where women may seek help or information.
We would be delighted to send a pack of information (includ-ing leaflets, posters, wallet sized cards, and pens) to all Practice Nurses who would like to have information displayed, or on hand to distribute in order to refer women to specialist domes-tic violence support as appropriate. The Women’s Aid Helpline is also available to provide information to professionals as you support women experiencing domestic violence.
Contact Laura Shehan at [email protected] or on 01 678 8858 to request materials be sent out to you free of charge.
Call for volunteersWomen’s Aid is currently recruiting volunteers for their National Freephone Helpline (1800 341 900) which is based at their offic-es at 5 Wilton Place, Dublin 2. Our National Freephone Helpline and One to One Support Services provide support, information, and referral to women being physically, emotionally, sexually, and financially abused by their intimate partners.
Information and application form are available fromwww.womensaid.ie/support/volunteer. For more
information contactDeirdre on (01) 678 8858 or by email [email protected] is 5pm, Monday 24th September 2012.Women’s Aid National Freephone Helpline 1800 341 90010am to 10pm, 7 days a weekWebsite: www.womensaid.ie

5
newsOnline resource for Alzheimer’s carers Some 75% of people who care for a loved one living with Alzhei-mer’s disease state that the burden of care resulted in additional strain between them and other members of their family, with 67% of respondents finding it difficult to get commitment from others regarding the sharing of care. These findings were revealed at the launch of www.mypeaceofmind.ie which was developed to provide practical tools and advice for those living with Alzheimer’s disease and their carers. The website provides guidance from a range of Irish experts including Dr Nina Byrnes, GP, Oakwood Medical Clinic and media medical expert and Jill Kerby, personal finance expert.
The My Peace of Mind research investigated a range of issues including knowledge and understanding of the symptoms of Alzheimer’s disease as well as the emotional and financial impact associated with caring for someone with the disease. The re-search revealed that over two-thirds (67%) of all participants were prompted to take their loved one to a doctor by observing one of the symptoms of Alzheimer’s disease; with ‘confusion with time or place’ (78%) as the most common symptom. The research revealed that over half (53%) of all diagnoses occurred at the moderate stage of the disease.
Speaking at the launch, Jill Kerby, personal finance expert, said, “It is totally understandable that financial and legal planning is put on the back burner when a loved one receives an Alzheimer’s disease diagnosis however, this can have very significant implications in the longer term. Engaging a solicitor to create an enduring power of attorney can go a long way to helping you to plan for the future.”
dr Nina byrnes, gP, Oakwood medical Clinic, personal finance expert, Jill Kerby, and michelle mahon from wexford who helps to care for her 77-year-old mother.
down with blood pressure!
The Irish Heart Foundation is driving awareness among adults that the only way to know you have high blood pressure is to get it checked. To drive home this vital health message, the Foundation is launching a national blood pressure mobile roadshow offering FREE blood pressure checks at more than 50 locations nationwide including selected Lidl stores and community groups. According to the national charity fighting heart disease and stroke, 60% of adults over 45 have high blood pressure and of those, half of them do not know it. The Foundation stressed that high blood pressure is a silent killer with no symptoms, silently causing damage to blood vessels which can later lead to heart attack, stroke and heart or kidney failure.
Don, Rob and Ben Morgan, sons of late comedian Dermot Morgan, as launched the Irish Heart Foundation’s September Heart Month campaign. Inspired by their father’s death from heart attack 14 years ago, the trio embraced the ‘Father Ted’ spirit outside government buildings as they encouraged Irish adults to reduce their risk of cardiovascular disease and get their blood pressure checked.
Middle son Rob Morgan, aged 32, said: “Dermot was just 45 years old when he died suddenly of heart attack which is too young by anyone’s measure. I think it’s often easy to think we are invincible and that blood pressure checks are for someone else or for someone older. But as I know firsthand, heart attacks and strokes can happen when you least expect it. Ever since Dermot died, I’m paranoid about getting checked for my blood pressure and it’s a good thing too.
Part time practice nurse sought for gP practice in South
dublin
Ideally should be trained in phlebotomy, smear taking, ECG recording and vaccinations.
enquiries to [email protected] or telephone 01 2835747.
Part time practice nurserequired
3-4 sessions per week, for modern computerised practice North County Dublin. Attractive working conditions. Job spec available on request.
Please send Cv to Susan, Portmarnock family Practice, 7 Portmarnock Shopping Arcade, Portmarnock, dublin, or email [email protected].

6
news
mSc in health Informatics part-time
Applications are invited for the MSc in Health Informatics which runs part-time over two years, on Friday afternoons and Saturday mornings.
Run jointly with the School of Medicine at TCD, this course aims to educate people who will play leadership roles in the effective use of information and communications technology in the delivery of healthcare.
A key strength of this Master’s degree is the student mix from both health science and IT backgrounds: those with IT backgrounds learn from their clinical classmates and vice versa, and all learn to communicate more effectively with each other. A second strength is the contribution by international experts to teaching and assessment.
The course has been running for more than ten years, and its graduates are in key positions throughout the healthcare system in Ireland. Some are driving hospital IT projects; others are involved in national IT integration initiatives. Some are working with healthcare software suppliers; others are bringing IT to their allied healthcare professional colleagues.
Applicants should hold a good honours degree in a professional (health sciences or computer/engineering) discipline. However other qualifications and/or experience may be acceptable. No prior knowledge of computing is required.
The course takes up to 25 students each year and is funded under the National Development Plan (Postgraduate Skills Conversion Programme) with reduced fees for EU students.
For more information email: [email protected]
www.scss.tcd.ie
New to Ireland health and wellness Coaching Certificate
The Institute of Health Sciences has introduced a new Health & Wellness Coaching Certificate for healthcare professionals from 29th September – 2nd October 2012 in the Education & Research Centre, Our Lady’s Hospice, Harold’s Cross, Dublin.
Health and Wellness Coaching is an emerging area of healthcare designed to help guide and empower patients towards taking responsibility for their own health and adopting long-term lifestyle changes, which can dramatically improve patient compliance and practitioner success rates.
According to US research, anywhere between 40 – 80% of the medical information received by patients is forgotten immediately and approximately 30% of new prescriptions for diabetes, high blood pressure and high cholesterol go unfilled. The use of health coaching strategies alongside conventional healthcare practice has demonstrated significant improvements in depression scores, exercise behaviours and reduction in hospital admissions and A&E visits.
A first of its kind in Ireland, the course is being run by Dr Michael Arloski PhD, US based licensed psychologist and professional certified coach with over 30 years› experience in the field and author of Wellness Coaching For Lasting Lifestyle Change.
The course is CPD/CME accredited by the ICGP and An Bord Altranais. To book call (076) 603 0746 or for more information,
www.instituteofhealthsciences.com
diabetes Ireland training dates
Diabetes Ireland has a structured patient diabetes education programme designed for nurses and dietitians who have diabetes expertise. This is a unique opportunity to avail of free facilitation and CODE training.
facilitation skills and COde trainingFacilitation: 19th and 20th OctoberCODE Training: November dates to be decided by
attendees Time of course: 9.30am – 4.30pm Location: Dublin (accommodation will be provided
for night of 19th if required)
• A recognised diabetes qualification equal to a Level 2 FETAC course or higher.
• At present, the recognised qualifications for practice nurses are the Bradford
Course, Warwick Diploma, Dublin City and Galway University diabetes modules and the ICGP course – all equal to or greater than 5 credits.
A booking fee of €50 (refundable at attendance) guarantees a place.
If you or any of your colleagues are interested in pursuing this opportunity please contact Sinead Hanley on 01 8363022 or e-mail [email protected] by 28th September.
Important Dates:
Social Functions:
Call for Workshops Proposal OCT 2, 2012
Call for Abstract OCT 2, 2012
Workshops Submission Deadline NOV 15, 2012
Abstracts Submission Deadline JAN 15, 2013
Welcome Reception at the Convention Centre Dublin MAY 29, 2013
Gala Dinner at the Mansion House, official residence of the Lord Mayor of Dublin
MAY 31, 2013
38th Annual MeetingINTERNATIONAL UROGYNECOLOGICALASSOCIATION
with
CONTINENCEFOUNDATION OF IRELAND
MAY 28 - June 1, 2013

LAMA = long-acting muscarinic antagonist.
References: 1. SPIRIVA® 18 μg Inhalation powder, hard capsule - Summary of Product Characteristics. http://www.medicines.ie. Accessed August 2012. 2. Tashkin DP et al. for the UPLIFT Study Investigators. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med 2008;359:1543–1554.
Prescribing Information (Ireland) SPIRIVA® (tiotropium) Inhalation powder, hard capsules containing 18 microgram tiotropium (as bromide monohydrate). Indication: Tiotropium is indicated as a maintenance bronchodilator treatment to relieve symptoms of patients with chronic obstructive pulmonary disease (COPD). Dose and Administration: Adults only age 18 years or over: Inhalation of the contents of one capsule once daily from the HandiHaler® device. Contraindications: Hypersensitivity to tiotropium bromide, atropine or its derivatives, or to the excipient lactose monohydrate which contains milk protein. Warnings and Precautions: Not for the initial treatment of acute episodes of bronchospasm, i.e. rescue therapy. Immediate hypersensitivity reactions may occur after administration of tiotropium bromide inhalation powder. Caution in patients with narrow-angle glaucoma, prostatic hyperplasia or bladder-neck obstruction. Inhaled medicines may cause inhalation-induced bronchospasm. In patients with moderate to severe renal impairment (creatinine clearance ≤ 50 ml/min) tiotropium bromide should be used only if the expected benefit outweighs the potential risk. Patients should be cautioned to avoid getting the drug powder into their eyes. They should be advised that this may result in precipitation or worsening of narrow-angle glaucoma, eye pain or discomfort, temporary blurring of vision, visual halos or coloured images
in association with red eyes from conjunctival congestion and corneal oedema. Should any combination of these eye symptoms develop, patients should stop using tiotropium bromide and consult a specialist immediately. Tiotropium bromide should not be used more frequently than once a day. Spiriva capsules contain 5.5 mg lactose monohydrate. Interactions: Although no formal drug interaction studies have been performed tiotropium bromide inhalation powder has been used concomitantly with other drugs without clinical evidence of drug interactions. These include sympathomimetic bronchodilators, methylxanthines, oral and inhaled steroids, commonly used in the treatment of COPD. The co-administration of tiotropium bromide with other anticholinergic-containing drugs has not been studied and is therefore not recommended. Fertility, Pregnancy and Lactation: No clinical data on exposed pregnancies are available. The potential risk for humans is unknown. Spiriva should therefore only be used during pregnancy when clearly indicated. It is unknown whether tiotropium bromide is excreted in human breast milk. Use of Spiriva is not recommended during breast feeding. A decision on whether to continue or discontinue breast feeding or therapy with tiotropium bromide should be made taking into account the benefit of breast feeding to the child and the benefit of tiotropium bromide therapy to the woman. Clinical data on fertility are not available for
tiotropium. Effects on ability to drive and use machines: No studies have been performed. The occurrence of dizziness, blurred vision, or headache may influence the ability to drive and use machinery. Undesirable effects: Common (≥1/100, <1/10): Dry mouth. Uncommon (≥1/1,000, <1/100): Dizziness, headache, taste disorders, vision blurred, cough, pharyngitis, dysphonia, rash, oropharyngeal candidiasis, dysuria, urinary retention, gastrooesophageal reflux disease, atrial fibrillation, constipation. Serious undesirable effects consistent with anticholinergic effects include glaucoma, constipation and intestinal obstruction including ileus paralytic as well as urinary retention. An increase in anticholinergic effects may occur with increasing age. Prescribers should consult the Summary of Product Characteristics for further information on side effects. Pack sizes: HandiHaler device and 30 capsules (3 blister strips); HandiHaler device plus 10 capsules (1 blister strip); 30 capsules (3 blister strips). Marketing authorisation number: PA 775/2/1. Legal category: POM. Marketing Authorisation Holder: Boehringer Ingelheim International GmbH, D-55216 Ingelheim am Rhein, Germany. For full prescribing information please see Summary of Product Characteristics. Prepared in August 2012.
Producing winners since 2002
Founded on a decade of proven success
With a long-term record of success in reducing symptoms, exacerbations and hospitalisations vs placebo, SPIRIVA® is a LAMA you can count on to help lead your COPD patients to everyday victories.1,2
IRE/SPI-121396Date of preparation: August 2012
5079 Spiriva A4 Ad_IRE.indd 1 20/08/2012 12:26

8
advertorial
The ultimate Cholesterol lowering Plan© – Part 2lINdA mAIN bSC rd, DIETETIC ADVISER, HEART UK – THE CHOLESTEROL CHARITY
Part I focused on how diet is important in lowering LDL cholesterol and reducing cardiovascular disease (CVD) risk. Part II investigates the Ultimate Cholesterol Lowering Plan© (UCLP©) – the step-by-step flexible approach to cholesterol reduction. The UCLP© builds on a heart
healthy foundation diet (low saturated fat, at least 5 fruit and vegetable portions daily and a weekly serving of oil-rich fish) by offering the patient four key cholesterol lowering foods to select from – soya, plant stanols and sterols, soluble fibre and/or nuts. Each key component of the UCLP© has been scientifically proven to provide a dose response effect to cholesterol reduction or CVD risk, thus allowing the patient the flexibility to choose part or all of the recommendations. The UCLP© has the potential to lower LDL cholesterol by a minimum of 5% to a maximum of 24% dependent upon the number of elements adopted.1 At the core of the UCLP© is the use of motivational interviewing, a client centred approach to help optimise dietary behaviour change.
The uClP© and motivational Interviewing: a patient centred approachTraditional patient advice and education do not work for all patients. Healthcare providers increasingly recognise motivational interviewing (MI) as an important tool in changing patient behaviour and improving health outcomes. Their role is to direct interviews in such a way as to explore the patient’s intrinsic motivation to change and agree strategies to facilitate this change. Well phrased questions encourage the patient to reflect on what actions they are willing to take, so leading them along the process of change.
heart healthy foundation dietSaturated fatSaturated fat increases blood cholesterol levels by influencing LDL receptors and membrane fluidity.2 Only 35% of Irish adults (18-64 years) achieve national recommendations.3 Main sources include fresh meat, biscuits, cakes, pastries, buns and cheese.3
Fruit and vegetables – at least 5 servings dailyFruit and vegetables are a valuable source of fibre, minerals and vitamins whilst providing few calories. Furthermore, higher fruit and vegetable intakes are inversely associated with CVD risk.4,5
Oil-rich fishOil-rich fish provide the main dietary source of very long chain omega 3 fatty acids which improve endothelial function and have anti-inflammatory and antithrombotic effects.6
uClP© four key foodsSoya foodsAdding just 15g soya protein (equivalent to two glasses of soya milk alternative or a handful of soya nuts) to a heart healthy diet can provide LDL cholesterol reductions of up to 10%.1,7,8 The LDL cholesterol lowering impact of soya is two-fold: firstly, soya protein has been proven to actively lower cholesterol, and although the mechanisms is still being debated, it is thought that the protein molecules of soya down-regulate LDL cholesterol synthesis in the
Table 1: Implementing the uClP© – a stage by stage approach
Stage 1 – motivational Interviewing
Establish rapport with patient and agree agenda for discussion.
Explore reasons for changing dietary habits and the patient’s readiness to change.
Assess the patient’s confidence to make changes. Discuss concerns and explore how to increase the chance of success.
Agree and document best strategies, realistic timescales and goals.
Agree how best to work with the patient to support their progress.
Stage 2 – baseline cholesterol lowering
gOAl Strategy – help the patient to:
Adopt a healthy eating pattern.
Be more aware of what they eat by keeping a food diary.
Reduce saturated fat. Recognise sources of saturated fat and agree how they might replace these with unsaturated fats.
5+ portions of fruit and vegetables daily.
Be aware of their fruit and vegetable intake and agree how they might increase it.
At least one portion of oil-rich fish per week.
Consider their oil-rich fish intake with a view to eating at least one portion each week.
Stage 3 – Consolidating initial behaviour change
Focus on positive change.
Enable patients to view setbacks as a valuable insight into their behaviour rather than undermining progress.
Use their food diary to help to reinforce change and as a discussion tool.
Explore and agree further strategies that might help them.
Stage 4 – Adopting the uClP© foods
gOAl STrATegy:
Further cholesterol lowering through dietary adoption of one, two, three or all four UCLP© cholesterol lowering foods
Introduce the patient to the 4 key UCLP© cholesterol lowering foods
• Soya foods• Foods fortified with Stanols or Sterols• Nuts• Oat beta-glucan, and other forms of soluble
fibre
Explore with the patient which of these they might wish to adopt and how they could incorporate them into their diet.
Emphasise that they can choose any one, two, three or all of the above options to add to their heart healthy foundation diet. They should choose the option/s they feel most comfortable with.
Using their food and drink diary, help guide them to the most appropriate option/s.
Remind them that all options will help lower their cholesterol and it is best to take one step at a time.
When they are ready, they can incorporate more options – the more options they include, the bigger the benefit.
Stage 5 – review and consolidate dietary and behaviour change
Help the patient review their goals.
Focus on positive changes and what impact these have had on cholesterol levels.• 12-14 weeks after adopting dietary changes is the ideal time to check
cholesterol levels for improvements.
Agree the need for further change.
Agree the need for further support.
Sponsored by an educational grant from Alpro

9
advertorial
liver. Secondly, many soya foods are naturally low in saturated fat and when introduced to a diet, they often displace higher saturated fat animal sources such as dairy or meat.1,7,8 Soya products in the supermarkets today, not only taste great but are available in a variety of formats to suit all, such as milk, yogurt, cream, dessert, custard or meat alternatives.
Plant sterols and stanolsA 1.5-2.4g daily intake can provide a 7-10% reduction in circulating cholesterol levels after 2-3 weeks.9 Plant sterols and stanols compete with cholesterol in the gut causing cholesterol loss through faeces.10
NutsNuts are high in dietary fibre, monounsaturated fatty acids, protein, vitamin E, naturally occurring plant sterols, minerals and other bioactive ingredients. Every 10g of nuts can result in a minimum 1% reduction of LDL cholesterol and a 2% risk reduction in CHD.11, 12 Nuts increase satiety, delay hunger and help modify overall calorie intake.13
Oat beta-glucan and other sources of soluble fibreThe viscosity of soluble fibres in the gut, interferes with bile acid (and therefore LDL cholesterol) absorption.14-16 Oats, beans, pulses, whole grain cereal, fruit and vegetables are all good sources and should be encouraged. Beta-glucan – the soluble fibre from oats – is the most well researched with conclusive evidence for its cholesterol lowering function.16
Changing dietary behaviour is far from easy. Health care professionals can support this process by helping their patients to identify small accessible steps that over time add up to a bigger change. Whilst this structured approach takes time, it is worth the investment, and can help facilitate gradual change and improved dietary habits that last a lifetime.
Table 3: Some practical tips on incorporating the uClP© foods to a standard diet
uClP© fOOdSThe patient can choose one or more of the following uClP© foods
dAIly INTAKe OPTIONSThe quantity and types of foods needed to be consumed daily to achieve the effective ldl cholesterol lowering dose
Soya foodsGoal: 15g per day
• 2 glasses (2x250ml) soya milk alternative – used in tea, coffee, cooking, on cereal, to make milkshakes OR
• 1 glass (250ml) soya milk alternative plus 4 tbsp. fresh or frozen young soya beans in a salad OR
• 200g soya pouring yogurt alternative poured over cereal or fruit salad plus 50g soya mince OR
• One handful or roasted soya /Edamame beans OR
• Soya burger plus plus 125g soya custard
Sterol or stanol fortified foodsGoal: 1.5-2.4g per day
• One mini-drink – dairy or dairy free ORAny 2-3 of the following fortified with stanols/sterols:• 2 tsp. (10-12g) spread• 250ml milk• 120g pot yogurtShould always be taken with meals to optimise impact
Nuts – unsaltedGoal: 30g per day
• A handful of any nuts including peanuts – almonds, walnuts, pecans, pistachios
Great as a snack or added to breakfast cereals or salads
Oat beta-glucanGoal: 3g daily
Any 3 of the following:• Porridge (30g oats) or a sachet instant porridge
oats• 1 Oatibix• 2 slices Hovis Hearty Oats™ bread• 3 oatcakes
Other soluble fibre sources
Encourage• 80-100g beans or pulses• Whole grain cereals e.g. brown rice, whole grain
pasta• At least five servings fruit and vegetables
Table 2: Potential cholesterol lowering effect of the uClP© key dietary strategies
Strategy Cholesterol lowering effect1,17
reduce saturated fat 5-10%
Soya foods 4.5-10%
Plant sterols 7-10%
Nuts 3-7.5%
Oat beta-glucan plus other sources of soluble fibre
5-10%
Note: Individual genetic variation, baseline diet and the amount of sustained dietary change will ultimately influence overall cholesterol reduction
Sponsored by an educational grant from Alpro
references:1. HEART UK. The UCLP©: Eating to our heart’s content, saving lives and money, 2011:
London, Nutrilicious. www.heartuk.org.uk/partners/partnership-activities/uclp or www.alpro.com/
2. Fernandez, M. and K. West, Mechanisms by which Dietary Fatty Acids Modulate Plasma Lipids. J Nutr, 2005. 135: p. 2075-2078.
3. Tierney, A., et al., Intake of total fat, saturated, monounsaturated and polyunsaturated fatty acids in an Irish adult population. Proceedings of the Nutrition Society, 2011. 70 (OCE6): p. E391.
4. Law MR, Morris JK. By how much does fruit and vegetable consumption reduce the risk of ischaemic heart disease? Eur J Clinic Nutr, 1998;52:549-56.
5. Steffen LM, Jacobs DR, Stevens J et al. Assoications of whole grain, refined grain and fruit and vegetable consmption with risks of all-cause mortiality and incident coronary artery disease and ischaemic stroke. The Atheroslcerois Risk in Communities (ARC) study. Am J Clin Nutr 2003;78:383-390
6. Begg A, C.S., Halcox J, Kaba A, Main L, Ray K, Purcell H, Williams H, Yellon D Omega-3 fatty acids in cardiovascular disease: re-assessing the evidence. British Journal of Cardiology, 2012. 19 p. 79-84.
7. Harland, J. and T. Haffner, Systematic review, meta-analysis and regression of randomised controlled trials reporting an association between an intake circa 25g soy protein per day and blood cholesterol. Atherosclerosis, 2008. 200: p. 13-27.
8. Jenkins, D., et al., Soy Protein Reduces Serum Cholesterol by Both Intrinsic and Food Displacement Mechanisms. The Journal of Nutrition, 2010.
9. EFSA, Plant Sterols and Blood Cholesterol: Scientific substantiation of a health claim related to plant sterols and lower/reduced blood cholesterol and reduced risk of (coronary) heart disease pursuant to Article 14 of Regulation (EC) No 1924/20061. Official Journal of the European 2008. 781: p. 1-12.
10. Ostlund, R.E., Jr., Phytosterols in human nutrition. Annu Rev Nutr, 2002. 22: p. 533-49.11. Sabate, J., K. Oda, and E. Ros, Nut Consumption and Blood Lipid Levels – A Pooled Analysis
of 25 Intervention Trials. JAMA, 2010. 170(10): p. 821-827.12. Jenkins, D., et al., Dose Response of Almonds on Coronary Heart Disease Risk Factors:
Blood Lipids Oxidized Low-Density Lipoproteins, Lipoprotein(a), Homocysteine, and Pulmonary Nitric Oxide : A Randomized, Controlled, Crossover Trial. Circulation, 2002. 106: p. 1327-1332.
13. Mozaffarian, D., et al., Changes in Diet and Lifestyle and Long-Term Weight Gain in Women and Men. N Eng J Med 2011. 364: p. 2392-2404.
14. Lui, S., et al., A prospective study of dietary fibre intake and risk of cardiovascular disease among women J Am Coll Cardiol, 2002. 39: p. 49-56.
15. Thuewissen E, Mensink RP. Water-soluble dietary fibres and cardiovascular health. Physi and Behav 2008;94:285-292
16. EFSA, Scientific Opinion on the substantiation of a health claim related to oat beta-glucan and lowering blood cholesterol and reduced risk of (coronary) heart disease pursuant to Article 14 of Regulation (EC) No 1924/20061. Official Journal of the European Union, 2010. 8(12): p. 1885.
17. Bruckert, E. and D. Rosenbaum, Lowering LDL cholesterol through diet: potential role in the statin era. Curr Opinion in Lipidology, 2011. 22: p. 43-48.
For the full UCLP© scientific report and/or if you have yet to receive your free UCLP© teaching toolkit – please email ‘NiGP UCLP’ to [email protected].
For further information on the UCLP©, visit: www.heartuk.org.uk/partners/partnership-activities/uclp/ OR
http://uk.health.alprosoja.com/uclp.html

The 3-step programme that is changing cholesterol lowering advice.
Two thirds of the UK population have elevated cholesterol levels - one of the biggest risk factors for coronary heart disease.
The Ultimate Cholesterol Lowering Plan (UCLP), is a revolutionary dietary and behaviour change programme underpinned by a wealth of compelling clinical evidence. The UCLP was developed in collaboration with HEART UK - The Cholesterol Charity - and seven leading health and diet experts.
Combining the science with behavioural strategies, the patient-led programme is practical, flexible and motivational – resulting in a minimum cholesterol drop of 5% and with a potential 24% cholesterol drop.
STEP 1 – Motivational interviewing is integral to the process. It enables the patient to identify their motivational triggers and work through their barriers.
STEP 2 – Building strong foundations: Reducing Saturated Fat – 5-a-day – Oil-Rich Fish.
STEP 3 – A pick ‘n’ mix of four cholesterol lowering foods all proven to lower cholesterol on their own and when combined result in a cumulative cholesterol lowering effect.
l SOYA FOODS – as little as 15g of soya protein has been clinically proven to lower serum cholesterol levels by around 4-10%. This equates to 2 glasses of soya milk alternative, a handful of soya nuts (roasted Edamame beans) or 20g unhydrated soya mince.
l NUTS – Just a handful. Due to their high unsaturated fat content – all nuts have demonstrated some cholesterol lowering properties.
l BETA-GLUCAN – the unique fibre mainly found in oats and barley, can reduce cholesterol absorption from the gut. 2-3 servings of oat-based bread slices, oat-based cereals, oat bran or oat cakes.
l STANOL/STEROL containing products can lower serum cholesterol by up to 10% at 1.5g - 2.4g per day. There are many formats now available for consumers including one shot drinks, spreads and milks.
THE EXTREMELY POPULAR UCLP TEACHING TOOLKIT IS NOW AVAILABLE FREE to all health professionals. The toolkit comprises of: A deskTop flip chArT to help take your patient step by step through the Uclp process, providing you with the detail whilst your patient views simple images and food portion photography. A pATienT Uclp informATion sheeT. A summary of the Ulcp, with practical examples and allowing for tailored advice. Your patient can record their motivational triggers and barriers discussed and fill in the food, drink, mood and hunger score diary. TO ORDER SIMPLY EMAIL ‘UCLP TOOLKIT’ to [email protected]
THE UCLP: EATING TO OUR HEARTS CONTENT, SAVING LIVES AND MONEY. The authoritative report presenting an overview of the Uk cholesterol dilemma and its current management and the compelling evidence for the Uclp’s impact on the health of the nation and the nhs economic burden. electronic version available free to all health professionals. SIMPLY EMAIL ‘UCLP REPORT’ to [email protected] or download from http://health.alprosoya.co.uk/uclp.html or http://www.heartuk.org.uk/healthprofessionals/index.php/uclp/
@alpro_uk #plantpower

11
clinical review
Childhood food allergy: solving the puzzleThere are numerous myths surrounding childhood allergy, but in fact allergy affects approximately 5% of children.
ruTh ChArleS, PAEDIATRIC DIETITIAN, BALLINDERRY CLINIC, ST. FRANCIS HOSPITAL, MULLINGAR, CO. WESTMEATH
fact or fiction? • Food allergy is not common in infancy? • Consumption of milk and dairy products leads to mucus in
the upper and lower respiratory tracts? • Goat and soy milk are suitable alternatives if cow’s milk al-
lergy is suspected? • Allergy tests (skin prick and serum specific IgE) have no rel-
evance in early infancy? • The next allergic reaction will be worse than the previous?
These are just five of the most common myths that exist around food allergy – they are all untrue! It is not uncommon for food allergy to be mis – or undiagnosed especially consider-ing that there is no fully resourced service for paediatric allergy in the Republic of Ireland. Food allergy in childhood does exist. It presents mainly in the community and primary care settings and affects 5-6% of young children.1 Milk, egg, peanut and tree-nut are the most common food allergens in children under 3 years: nut, fish and shellfish are more common in older children.
Food allergy often exists with other allergic diseases (mostly eczema, followed by asthma and rhinitis). The Allergy March2 is a concept that describes the relationships between them.
what happens?On first contact with a food (consumed, inhaled, rubbed on skin, lips or into the eye) the immune system becomes sensitized to the allergen it contains. On subsequent contact (accidentally or otherwise), the immune system reacts resulting in symptoms within minutes, hours or days of the contact. The timing of the reaction is an important distinguishing feature between IgE mediated (usually rapid onset within minutes) and non IgE mediated (usually delayed onset from 2-48 hours) food allergy. The UK National Institute for Clinical Excellence (NICE) produced clinical guideline 116 in 2011 which is an excellent summary of best practice advice on the care of children and young people with suspected food allergies.3
Lactose intolerance does not cause an allergic reaction. Con-

12
clinical review
genital lactose intolerance is rare. Primary lactose intolerance is unlikely to become symptomatic until late childhood. Transient intolerance can result after any insult to the brush border of the intestinal epithelium where lactase production or its action is affected e.g. gastroenteritis. It usually resolves within 6-8 weeks, so the long term or indefinite use lactose free infant formula is unlikely to be helpful.
TestingSerum specific IgE and food specific skin prick tests indicate sensitization to an allergen but do not always predict whether a child will or will not have an allergic reaction. This is further evidence of the importance of a focused clinical history and examination. NICE recommend that allergy tests should only be done by healthcare professionals with the appropriate com-
Signs, symptoms and differentials are described as follows:
Ige mediated food allergy Non Ige mediated food allergy
Skin
Pruritus Erythema Acute urticaria – localised or generalised Acute angioedema – most commonly of the lips, face and around the eyes
Pruritus Erythema Atopic eczema
gut
Angioedema of the lips, tongue and palate Oral pruritus NauseaAbdominal pain Vomiting Diarrhoea
Gastro-oesophageal reflux disease Loose or frequent stools Blood and/or mucus in stools Colicky abdominal pain/Infantile colic Food refusal or aversion Constipation Perianal redness Pallor and tiredness Faltering growth in conjunction with at least one or more gastrointestinal symptoms above (with or without significant atopic eczema)
respiratory (usually with one or more of the above)
Nasal itching SneezingRhinorrhoea Congestion Cough Chest tightness Wheeze Shortness of breath
Other
Signs or symptoms of anaphylaxis or other systemic allergic reactions
The Allergy march
Typical age of onset
Asthma
rhinitis
food allergy
eczema
birth
3 m
onths
1 ye
ar
2 ye
ars
3 ye
ars
7 ye
ars
15 y
ears
petencies to select, perform and interpret them and that skin prick tests should only be undertaken where there are facilities to deal with an anaphylactic reaction.3 What is clear is that vega testing, applied kinesiology, hair analysis or serum-specific IgG and IgA have no role in the diagnosis of food allergy.3
remove food or not?If a particular food is suspected, but there is no evidence of any immediate or delayed reaction after it’s been eaten, then that food should not be removed from the diet and should be put back in if it has been removed. Removing any food from a child’s diet is a major decision and there needs to be a clear rationale for so doing. The child and family will need significant support as there are many social issues to consider (quality of life, grocery shopping, cost etc.).

Up to 80% of sexually active women become infected with an HPV type in their lifetime1
Why gamble?
Most women under 45 years of age can gain some protection from Gardasil® against HPV
types 6, 11, 16 & 18 regardless of past or current infection2
Gardasil® – continuing to pave the way for the prevention of cervical cancer and other HPV genital diseases
06/12 IR00131
Information about adverse event reporting can be found at www.imb.ie. Adverse events and inadvertent vaccination during pregnancy should also be reported to Sanofi Pasteur MSD by calling 00 44 1628 785291.
Abridged Prescribing Information GARDASIL® (Human Papillomavirus Vaccine [Types 6, 11, 16, 18] (Recombinant, adsorbed)). Refer to Summary of Product Characteristics for full product information before prescribing. Additional information is available on request. Presentation: Gardasil is supplied as a single dose pre-filled syringe containing 0.5 millilitre of suspension. Each dose of the quadrivalent vaccine contains highly purified virus-like particles (VLPs) of the major capsid L1 protein of Human Papillomavirus (HPV). These are type 6 (20 mg), type 11 (40 mg), type 16 (40 mg) and type 18 (20 mg). Indications: Gardasil is a vaccine for use from the age of 9 years for the prevention of premalignant genital lesions (cervical, vulvar and vaginal), and cervical cancer causally related to certain oncogenic Human Papillomavirus (HPV) types and genital warts (condyloma acuminata) causally related to specific HPV types. The indication is based on the demonstration of efficacy of Gardasil in females 16 to 45 years of age and in males 16 to 26 years of age and on the demonstration of immunogenicity of Gardasil in 9- to 15-year old children and adolescents. Dosage and administration: The primary vaccination series consists of 3 separate 0.5 millilitre doses administered according to the following schedule: 0, 2, 6 months. If an alternate schedule is necessary the second dose should be administered at least one month after the first and the third dose at least three months after the second. All three doses should be given within a 1 year period. The need for a booster dose has not been established. The vaccine should be administered by intramuscular injection. Contraindications: Hypersensitivity to any component of the vaccine. Hypersensitivity after previous administration of Gardasil. Acute severe febrile illness. Warnings and precautions: The decision to vaccinate an individual should take into account the risk for previous HPV exposure and potential benefit from vaccination. As with all vaccines, appropriate medical treatment should always be available in case of rare anaphylactic reactions. The vaccine should be given with caution to individuals with thrombocytopaenia or any coagulation disorder because bleeding may occur following an intramuscular administration in these individuals. Syncope,
sometimes associated with falling, has occurred after vaccination with Gardasil; vaccinees should be carefully observed for approximately 15 minutes after vaccination. There is insufficient data to recommend use of Gardasil during pregnancy therefore the vaccination should be postponed until after completion of the pregnancy. The vaccine can be given to breastfeeding women. Gardasil will only protect against diseases that are caused by HPV types 6, 11, 16 and 18 and to some limited extent against diseases caused by certain related HPV types. Vaccination is not a substitute for routine cervical screening. Individuals with impaired immune responsiveness, due to either the use of potent immunosuppressive therapy, a genetic defect, or other causes, may not respond to the vaccine. As with any vaccine, vaccination with Gardasil may not result in protection in all vaccine recipients. There are no safety, immunogenicity or efficacy data to support interchangeability of Gardasil with other HPV vaccines. Undesirable effects: Very common side effects include: headache and at the injection site, erythema, pain and swelling. Common side effects include bruising and pruritus at the injection site, pyrexia, nausea and pain in the extremity. Rarely urticaria and very rarely bronchospasm has been reported. Idiopathic thrombocytopenic purpura, Guillain-Barré Syndrome and hypersensitivity reactions including anaphylactic/anaphylactoid reactions have also been reported. For a complete list of undesirable effects please refer to the Summary of Product Characteristics. Package quantities: Single pack containing one 0.5 millilitre dose pre-filled syringe with two separate needles. Marketing authorisation holder: Sanofi Pasteur MSD SNC, 8 rue Jonas Salk, F-69007, Lyon, France. Marketing authorisation number: EU/1/06/357/007 (pre-filled syringe with two separate needles). Legal category: POM ® Registered trademark. Date of last review: May 2012. References: 1. Health Protection Surveillance Centre. http://www.hpsc.ie/hpsc/A-Z/Hepatitis/HPV/Factsheet/. Accessed June 2012. 2. Summary of Product Characteristics.
GARDASIL_why gamble_A4.indd 1 07/09/2012 13:12

14
clinical review
Elimination needs to be carried out as part of an overall management plan and for a defined length of time. In all cases of cow’s milk exclusion and exclusion of more than one food the child should be referred to a Community or Paediatric Dietitian. The cornerstone of any elimination is the substitu-tion or replacement with a suitable age appropriate nutritional equivalent otherwise growth faltering, rickets, nutritional compromise, food aversion and cross reactivity are potentially real consequences. Cow’s milk substitutes are a particular case in point: soy formula or goat’s milk are not always suitable because of the risk of cross reactivity. Rice, oat, almond or other plant derived milks are not always nutritionally suitable for children.
If following diagnosis, long term dietary elimination of a food is indicated, then the issue of when and how to reintroduce it has to be addressed and should be included in the overall man-agement plan. The natural history of food allergy appears to be changing – most children are expected to outgrow early food allergies by about age 8 but the only definitive way of knowing is by clinical re evaluation over a defined period of time.
medicationThere is no cure for food allergy but it can be managed. Medi-cation will form part of a comprehensive agreed management plan. A non sedating antihistamine is indicated for managing mild to moderate allergic reactions. Following a comprehensive clinical history, examination and risk assessment it is usually clear if a child is at risk of an allergic reaction requiring the use of an age/weight appropriate adrenalin auto injector (AAI). International best practice guidelines describe in detail the ra-tionale for prescribing and using AAIs.5 At the time of prescrip-tion those requiring AAIs must be given clear instruction on when and how to use them and these competencies should be reassessed on a regular basis.
managementTake a focused history as described above. Optimize treatment and assess compliance if there is existing eczema, asthma or rhinitis. Refer to a local community/paediatric dietitian espe-cially if cow’s milk or multiple foods are avoided. Assess the need for allergy medication. Parents need a clear plan, includ-
ing information for pre-school etc. that addresses all aspects of food allergy specific to the needs of their child. If food allergy is suspected or if it’s unclear, NICE recommend assessment and management by a healthcare professional with the appropriate competencies.3 Any practitioner who’s uncertain or unhappy with their level of competence should refer onwards.
There are a number of paediatricians nationwide with specialist training or a special interest in food allergy: Prof Jonathan Hourihane, CUH, Cork Dr John Fitzsimons, OLOLH, Drogheda, Prof Alan Irvine, OLCH, Crumlin Dr Imelda Lambert, MRH, Mullingar Dr Edina Moylett, UCH, Galway.
Food allergy mostly presents to a primary care setting in which there currently is no training or education for practition-ers. The Irish Food Allergy Network was formed in October 2010 as a professional working group with a common interest in food allergy. Its Core Working Group is in the process of taking steps to address the service gaps that exist by producing diagnostic algorithms and care pathways for primary and secondary care; these are in draft form and hope to be finalized by year end.
references1. Sampson HA. Update on Food Allergy. J Allergy Clin Immunol 2004;
113(5): 805-819. 2. Leap. www.leapstudy.co.uk/amarch.html. 3. NICE food allergy in children and young people, February 2011 http://
guidance.nice.org.uk/CG116 4. Fitzsimons J, Kieran E. Paediatric food allergies and intolerances. ICGP
Forum Distance training module 166: June 2011. 5. Muraro A, et al. The management of anaphylaxis in childhood: position
paper of the European academy of allergology and clinical immunology. Allergy 2007; 62: 857-871.
The diagnosis relies on a comprehensive history with special focus on:4
what happened? Were the symptoms consistent with the features described above? Importantly, were there any features of anaphylaxis?
Timing. Minutes to < two hours – immediate allergy: > two hours – possibly delayed allergy.
what food was suspected? Any food may cause an allergic reaction but there are the usual suspects.
how much of the food was consumed? IgE-mediated reactions may occur after exposures to tiny amounts of food or contamination.
has this happened before? Food allergy reactions often occur a number of times before the link is realised
what happened after the reaction? Did the reaction progress?
how long did symptoms persist? Urticarial reactions lasting longer than 24 hours are unlikely to be food allergy.
how did it resolve? Were antihistamines required?
does the child have any risk factors for food allergy?
Most notably eczema or other food allergies. Is there a family history?
has the child had the food since with any reaction?
Food allergic reactions will tend to be consistent occurring on every exposure.
does the child eat a regular portion of all foods?
Food avoidance may be a sign of food allergy.
Think food allergy in a child – with faltering growth and one or more gastrointestinal symptoms. – with early onset severe atopic eczema. – where optimal treatment to date for eczema and the GIT has not responded.
Soy formula or goat’s milk are not always suitable because of the risk of cross reactivity.

15
clinical review
The online election for eight nurses and midwives to Bord Altranais agus Cnáimhseachais na hÉireann, the Nursing and Midwifery Board of Ireland, opens on Wednesday September 19 at 9.00am.
Vote by logging onto www.nursingboard.ie. To vote you will need your Voting Registration Number (VRN) and your date of birth.
By now all registered nurses and midwives will have received voting information, including a personal VRN. If you do not have your VRN, contact [email protected] before 1pm on September 27 and a replacement number will be sent to you in the post.
Ballot open from September 19 – October 1, 2012
An Bord AltranaisNursing Board Board Election 2012
D.i.G.P.
Diabetes in General Practice
“Towards Integrated Diabetes Care”5th Annual Collaborative diabetes Conference
Wednesday 26th September 2012 Oriel House Hotel, Ballincollig, Co.Cork
12md-6pm
Keynote Speaker: Dr Velma Harkins (Joint National Clinical Lead Diabetes Clinical Care Programme)
“barriers & facilitators of Optimal diabetes management in general Practice – A Qualitative Study” Dr Sheena McHugh (UCC)
National foot Care Programme Emily Haworth (Clinical Specialist Podiatrist CUH)
workshops:1. The identification and treatment of high risk patients2. Assessing for Depression in Diabetes3. Physical Activity-The New Vital Sign?4. Weight Management in Diabetes5. Achieving HbA1c Target’s6. Cardiovascular Risk Management in Type 2 and Pre-Diabetes7.Renal Disease in Diabetes8. Diabetes Prevention Programme
The Conference is Free to Participants Closing date friday 7th September 2012
For Further Information/Booking Form Contact: Katie Murphy
email: [email protected]: 086 0566077

16
in practice
Twitter for Nurses
How to FollowIf you have followed the instructions from the last issue and now have a Twitter account – well done! Now you can start making connections, building your own online network of like-minded people and learning from them – by finding and following – the right people.
lISA NOlAN
Perhaps you have already found some great accounts to follow. Maybe you have been wandering aimlessly around the site, not really sure what the fuss is about. You might have gotten side-tracked and followed your friends, people who post motivational quotes or
controversial opinions (fist in mouth – can’t believe they said that!). To get the best value out of Twitter, you need to follow 50 to 100 people who educate you or share handy tips and
relevant news. Life is short, so make sure you also find people who entertain you, brighten your day and whose content makes you look forward to checking your Twitter feed. Such people are not hiding in rock pools – they are right there on Twitter, just waiting for you to connect with them.
So follow the next batch of step by step instructions below, say goodbye to the empty Twitter feed on your screen and charge up your smartphone/laptop – you might be here for a while!
figure 1
1. Log in to your Twitter account.
2. Click on Home (top left of screen) to show your timeline. (Figure 1).
3. Left click in the ‘Search’ box at the top right of your screen. Type in the name of someone you would like to follow, e.g. HSE, or their Twitter handle if you know it, e.g. @HSElive and then click the magnifying glass icon or press enter on your keyboard.
4. If, for example, you searched for @HSElive, the screen in Figure 2 will appear. You can see the HSE logo under the heading ‘People’ on the top left of the screen. You will also see a list of HSE tweets or messages by others in which the HSE is mentioned.
5. Hover your mouse over the logo on the left and you will see the full name ‘HSE Ireland’ which helps to confirm that this is who you were searching for. Click on this logo to bring up a preview window that shows a summary of the HSE Twitter account. (Figure 3).
6. If you would like to follow HSE Ireland immediately, you can click on the ‘Follow’ button in the preview window. If you would prefer to read more tweets to help you decide wheth-er to follow or not (and I would personally recommend this, especially when search terms such as nurse can yield what can only be described as ‘alternative’ results), you can click on the name at the very top of the preview window. This will bring up the full @HSElive profile, as in Figure 4.
7. Don’t forget you are still logged into your own Twitter account and what you are looking at now is the HSE Ireland Twitter profile, which shows how many tweets they have broadcast, how many people they are following and how many followers they have (see circled area). You can choose to follow HSE Ireland in this screen as well, by clicking on the ‘Follow’ button. Once you have clicked on the Follow button, it will change to a blue ‘Following’ button.
figure 2

17
in practice
8. When you follow other people, their Tweets will automatically appear in your Twitter feed (i.e. on your Twitter Homepage), with the most recent at the top.
There are several ways find great people to follow:
9. Use the ‘Search’ box as described above to search for individuals or groups by name.
10. You can also use the ‘Search’ box to find people who Tweet about a particular subject. For example if you search for ‘Immunisation’, the search results will show people or groups who have mentioned immunisation.
11. See who other people are following. This is a fast and efficient way of finding like-minded people.
If you decide to unfollow someone, go into the list of accounts you are following (under your profile name on your Home page). When you hover over the blue ‘Following’ button beside each name, it turns to a red ‘Unfollow’ button. Just click this to unfollow. People follow and unfollow others all the time on Twitter, so don’t worry that you will offend someone if you unfollow them – it’s your right to choose!
Twitter for Nurses – who to follow‘Great!’ you say, “but I’m having difficulty finding health-related Tweeps!’ If it helps to get you started, below are just some examples of groups (name, Twitter handle and bio) that are active on Twitter and who provide relevant news and updates that Practice Nurses may be interested in.
IrishPracticeNurses @PracticeNursesPromoting Professional Development for Practice Nurses in Ireland.
hSe Ireland @HSEliveThe HSE provides health and social services to everyone living in Ireland.
review Nursing @ReviewNursingSimple concise nursing review guide for students and nurses. Concentrated answers to relevant test questions in nursing school and randomized NCLEX exam.
NurChat @NurChatFortnightly nurse tweet chats, visit our site to find out more info, enjoy our last chat and contribute to the next!
weNurses @WeNursesConnecting, driving and supporting the nurse community through nurse twitter chats & nurse social media resources
Nursegroups @NurseGroupsThe social career resource for nurses. Tweeting daily nursing and health news.
Nursing Ideas @nursingideasSharing ideas and passion to improve nursing, health and healthcare.
Nursezone @NurseZoneEverything Nurses Need to Know.
medscape Nurses @MedscapeNursesMedscape Nurses helps you stay current with breaking medical news; quickly look up drugs, diseases, and procedures; and complete free CE activities.
rN.com @RNdotcomRN.com is dedicated to providing the nursing community with the highest quality, ANCC accredited online nursing continuing education courses.
Irish College of gPs @ICGPnewsThe Irish College General Practitioners (ICGP) is the professional body for general practice in Ireland.
medical Independent @med_indonewsmedicalindependent.ie is a website that wants to inform and engage with Irish doctors and NCHDs by providing them with breaking news.
rCPI @RCPI_newsThe Royal College of Physicians of Ireland is Ireland’s largest postgraduate medical education and training body.
gP update @GP_UpdateGP Update is run entirely by coal-face GPs to bring you up to speed on the latest issues, literature, research and guidelines affecting all primary care staff
bmJ @bmj_latestBMJ – British Medical Journal aims to lead the debate on health, and to engage doctors, researchers and health professionals to improve outcomes for patients.
Lisa NolanVirtual Administrator at IPNA and Aslan Virtual Admin.Tweets from @AslanVA
figure 3
figure 4

18
clinical review
Contraception and family planningCAITrIONA gAffNey, RGN, BNS, H. DIP, CNS/PN, GRAIGUENAMANAGH MEDICAL CENTRE, CO KILKENNY
The World Health Organistaion (WHO, 2008) defines family planning as “allowing individuals and couples to anticipate and attain their desired number of children and determine the spacing of pregnancies. It is achieved through the use of contraceptive
methods”. Family planning is essential to securing the well-being and autonomy of women while supporting the health and development of communities. Contraceptive choices for effective family planning have never been greater for women and men, with numerous options available here in Ireland.
family planning facts• In Ireland the age of sexual consent for both sexes is 17 years
of age• It is estimated that approximately half of all pregnancies
across the world are unplanned, with 1 in 8 pregnancies classified as a crisis pregnancy (ICCP, 2010)
• 45% of men and 26% of women agree that drinking alcohol has contributed to them having sex without using contraception (ICCP, 2004)
• It is against the law to have an abortion in Ireland, but not to travel abroad in order to have one in any country where the procedure is legal
• More that 4,000 Irish women travel abroad every year to have an abortion, mostly to the United Kingdom (IFPA, 1969).
• ‘Rogue agencies’ are unregistered agencies that exist specifically to persuade women not to obtain an abortion. These agencies are not Government funded or endorsed and issue inaccurate information.
The choicesOnly total abstinence offers 100% protection against pregnancies and Sexual Transmitted Infections (STIs), however there are several choices for prevention of both.
Optimal contraception should be reliable, easily accessible, reversible, easy to use, free from side effects and inexpensive. Options include:• short-acting methods and• long acting methods.
Short-acting methods1. Combined oral contraceptives (COCs)These are tablets containing oestrogen and progesterone and work by preventing a woman from releasing an egg every month (ovulation). When used correctly they are 99% effective. They are suitable for young women who can reliably take pills.

19
clinical review
Not everyone can use COCs however, for example, breast feeding mothers and women with a family history of arterial disease and/or a history of thromboembolism. COCs contain ethinyl oestradiol which is thrombogenic; therefore they must be used with caution in women who may be at risk of cerebrovascular and cardiovascular disease.
2. Progesterone only pills (POPs)These consist of a daily dose of oral progesterone which primarily works by preventing sperm entering the womb. These are suitable for women who cannot or do not want to take oestrogen and can often be used by women with conditions which prelude the use of COCs. There are two POPs available in Ireland which require consistent use everyday; therefore this form of contraception is not useful for forgetful users as it is not as effective if not taken on time. Depending on the pill, it must be taken within 3 or 12 hours of when it is normally taken or else additional contraception is required. The main side effects with POPs are menstrual irregularity – from amenorrhoea to heavier more frequent periods.
3. CondomsA barrier method that the man or woman can use. The male condom is made of very thin rubber and is put over the erect penis and stops sperm from entering the womb.
The female condom consists of a soft polyurethane sheath which lines the vagina and the area just outside. It also prevents sperm from entering the womb.
Both methods avoid the use of hormones and offer protection against STIs. Drawbacks: putting them on involves interruption, male condoms can split and female condoms can move out of place.
4. Diaphragms or capsThis is a barrier method that fits inside the vagina, covering the cervix. It is useful for those wishing to avoid hormones and does not interfere with the menstrual cycle. Disadvantages include that it also involves interruption of intercourse and may cause dysuria. The woman needs to ensure that she knows how to insert the device correctly themselves
long-acting methods5. Intrauterine System (IUS)This is a small T-shaped plastic device which releases a small daily dose of progesterone into the cavity of the uterus. It is a highly effective form of contraception and remains in situ for 5 years with rapid return of fertility after removal. There is only one IUS available at the moment in Ireland, called Mirena. The IUS reduces blood loss, sometimes amenorrhoea, and results in less dysmenorrhoea. It can be used in nullaparious women and can be inserted 8/10 weeks post partum. If the woman is having menorrhagia, inserting the IUS is not the immediate answer; the woman needs to be assessed for any pathological problems to determine if there are any other causes for the abnormal bleeding.
The IUS can result in menstrual disruption, PMS type symptoms and there may be bleeding/frequent spotting in the first 3-6 months.
6. Copper-bearing intrauterine devices (IUDs)Some women do not want to use hormones of any description. The copper coil is a device that is similar to the IUS but is made of copper wire and it is the copper that inhibits ovulation, as copper is toxic to sperm. It can also be used as a form of emergency contraception for up to 5 days and must be inserted by a specially trained doctor. The copper coil is also a good alternative when non-hormonal contraception is advised by medical specialists. Disadvantages include menorrhagia and risk of expulsion.
IUDs can be inserted immediately after an abortion or miscarriage if the pregnancy is less than 24 weeks.
7. ImplantThis consists of a small flexible rod which is inserted into the inner part of the upper arm. It slowly releases progesterone into the body and gives contraceptive protection for 3 years. It is rapidly reversible and can be replaced every three years as long as it is suitable. It is useful for women who forget to take their pill daily and for women who cannot take oestrogen. The implant must be inserted by a specially trained doctor or nurse. It can cause irregular menstrual bleeding; including excessive prolonged and more frequent bleeding. It is important to inform the woman of the menstrual changes beforehand otherwise she may feel that the bleeding is abnormal and may want the device removed.
COCs contain ethinyl oestradiol which is thrombogenic; therefore they must be used with caution in women who may be at risk of cerebrovascular and cardiovascular disease.

20
clinical review
8. Progesterone injectionsThese are long acting progesterons that are given by deep intramuscular injection. There is only one type available in Ireland and is called the Depo-Provera. The hormone is injected into a muscle, usually during the first five days of a period and further injections are needed every 12 weeks. The injection primarily works by preventing ovulation and there is no way of reversing the injection once it is given. Progesterone injections can result in changes in menstrual patterns and there may be a delay of up to one year in the return of fertility after stopping the use of these injections.
The use of the Depo-Provera injection also reduces oestrogen levels and is associated with significant loss of bone mineral density (BMD). Ideally, this form of contraception should be changed after 2-3 years but if the woman insists on staying on it then the risks should be reiterated and a DEXA scan should be encouraged. Women less that 20yrs should not use this as their bones are still forming.
9. Vaginal ringThis is a flexible, see-through plastic ring which is inserted by the woman herself and left in place for 3 weeks. This is followed by a ring-free break of 7 days. It gradually releases a low dose of oestrogen and progesterone and efficacy is not disturbed by GI upset. It is not advised for those who cannot take COCs. Drawbacks include: the woman has to be aware to remove the ring after 3 weeks and the partner may feel the ring during intercourse. There is only one licensed vaginal ring available in Ireland and is called the Nuva-Ring.
10. Natural methodsThere are a variety of methods to recognise or predict the timing of ovulation in order to identify the infertile period
– calendar method– temperature method– cervical mucus method
These methods require a motivated, committed couple and are only suitable for women with regular menstrual cycles. Men are fertile all the time; while women are only fertile one third of the time. The above methods avoid hormones or devices and can be used at all stages of reproductive life.
11. PatchThis is a thin patch containing oestrogen and progesterone, which is applied to the skin each week for 3 weeks with a week off each month. It works similarly to the COC as it prevents ovulation and induces changes to cervical mucus making it hostile to sperm penetration. There is only one such patch available in Ireland – the EVRA patch. This method of contraception is very useful for women who do shift work and those with different time-zones e.g. air hostesses, pilots. It may cause some local skin irritation, may be visible on the skin and is less effective in women > 90kgs. It has the same contraindications as the COC; if you cannot use the COC then you cannot use the patch.
12. SterilisationSterilisation needs to be strongly considered in both men and women as it is irreversible (or must be considered irreversible). Counselling should be provided prior to the procedure. The counselling ensures that the patient is properly informed and that there are no false expectations. All counselling should include failure rate, irreversibility and risks associated with the procedure.
• Vasectomy is a simple operation performed under local anaesthetic. It should be considered as being permanent and if it is reversed the patient should be made aware that reversal is not very successful. Male sterilisation is not effective immediately
• Tubal ligation is effective immediately and is permanent. It requires a general anaesthetic (GA) and the woman should be informed of the complications of having a GA.
ConclusionPrescribing of contraception should not solely target preventing pregnancy but also at enhancing the benefits, such as long-term reduction of risks and improvement in quality of life. New advances in contraception claim to offer such benefits which hope to maximise adherence and result in prevention of pregnancy.
references1. WHO (2008). Traditional medicine. Geneva, World Health
Organization, (Fact sheet no. 351; http:// www.who.int/mediacentre/factsheets/fs351/en/, accessed 12 August 2012).
2. McBride, Orla; Mongan, Karen and McGee, Hannah. 2012. The Irish Study of Contraception and Crisis Pregnancy 2010 (ICCP-2010). HSE Crisis Pregnancy Programme.
3. Rundle, K. McGee, H. & Layte, R. (2004). Irish Study of Contraception and Crisis Pregnancy (ICCP). A Survey of the General Population. Crisis Pregnancy Agency report No. 7.
4. IFPA (1969) http://www.ifpa.ie/node/501
“The ideal contraception would never need to be remembered, be 100% reliable, be totally free of side effects (some weight loss perhaps); increase a woman’s sexual responsiveness, guarantee an orgasm every time and taste of chocolate” Anne Furedi, Birth Control Trust, 1996

Information about adverse event reporting can be found at www.imb.ie. Adverse events and inadvertent vaccination during pregnancy should also be reported to Sanofi Pasteur MSD by calling 00 44 1628 785291.
08/12 IR00150
ABRIDGED PRESCRIBING INFORMATION PNEUMOVAX® II (Pneumococcal Polysaccharide Vaccine) Refer to summary of product characteristics for full product information before prescribing. Additional information is available upon request. Presentation: Pneumovax II is supplied as a single dose vial containing 0.5 millilitre of suspension. Each dose contains 25 micrograms of each polysaccharide type derived from capsules of the 23 most prevalent pneumococci, dissolved in isotonic saline solution containing 0.25% phenol. Indications: For active immunisation against disease caused by the pneumococcal serotypes included in the vaccine. The vaccine is recommended for individuals 2 years of age or older in whom there is an increased risk of morbidity and mortality from pneumococcal disease. Dosage and administration: One single dose of 0.5 millilitre is administered by intramuscular or subcutaneous injection. Special dosing: It is recommended that pneumococcal vaccine is given at least two weeks before elective splenectomy or the initiation of chemotherapy or other immunosuppressive treatment. Vaccination during chemotherapy or radiation therapy should be avoided and the vaccine should not be administered any sooner than three months after completion of such therapy. Persons with asymptomatic or symptomatic HIV infection should be vaccinated as soon as possible after diagnosis is confirmed. Revaccination: Healthy adults and children should not be re-vaccinated routinely. Revaccination at intervals of less than three years is not recommended because of an increased risk of adverse reactions. Revaccination may be considered for adults at increased risk of serious pneumococcal infection who were given pneumococcal vaccine more than five years earlier or for those known to have rapid decline in pneumococcal antibody levels. Revaccination after 3 years may be considered for selected populations (e.g. asplenics) who are known to be at high risk of fatal pneumococcal infections, and for children 10 years old or younger at highest risk of pneumococcal infection. Contraindications: Hypersensitivity to any component of the vaccine. Warnings and precautions: As with any vaccine, adequate medical treatment, including epinephrine (adrenaline), and supervision should always be available in case of an acute anaphylactic reaction. It is not known whether the vaccine can cause foetal harm or affect reproduction capacity when administered to a pregnant woman; the vaccine can be given to pregnant women only if clearly needed (potential benefit outweighs potential risk). It is not known whether this vaccine is excreted in human milk; caution should be exercised when the vaccine is administered to a nursing mother. Vaccination should be delayed in the presence of significant febrile illness or other active infection, except where delay involves greater risk. The vaccine should never be injected intravascularly. The vaccine should not be injected intradermally as injection by that route is associated with increased local reactions. If the vaccine is administered to patients who are immunosuppressed due to either an underlying condition or medical treatment (e.g. immunosuppressive therapy), the expected serum antibody response may not be obtained after a first or second dose, so such patients may not be as well protected against pneumococcal disease as immunocompetent individuals. Required prophylactic pneumococcal antibiotic therapy should not be stopped after vaccination. The vaccine may not be effective in preventing infection resulting from basilar skull fracture or from external communication with cerebrospinal fluid. As with any vaccine, vaccination with Pneumovax II may not result in complete protection in all recipients. Undesirable effects: Common side effects include: fever and injection site reactions such as pain, soreness, erythema, warmth, swelling and local induration. Other serious side effects have been reported and include thrombocytopenia in patients with stabilised idiopathic thrombocytopenic purpura, haemolytic anaemia in patients who have had other haematologic disorders, leukocytosis, anaphylactoid reactions, serum sickness, radiculoneuropathy, angioneurotic oedema, Guillain-Barré Syndrome and febrile convulsions. For a complete list of undesirable effects please refer to the Summary of Product Characteristics. Package quantities: Single pack containing one 0.5 millilitre single dose vial. Marketing authorisation holder: Sanofi Pasteur MSD Limited, Block A, Second Floor, Cookstown Court, Old Belgard Road, Tallaght, Dublin 24. Marketing authorisation number: PA 544/21/3 Legal category: POM Date of last review: June 2010
Are your patients at risk?
* See Immunisation Guidelines for Ireland www.immunisation.ie
Pneumococcal DiseaseVaccinate your at-risk patients and those 65 years and over against serious pneumococcal disease.
age 65+
chronic lung, heart or renal
disease
weakenedimmunesystem
other at-risk groups*smoker
diabetesvis i t pneumo. ie
4874.pneumovax A4 NIGP v4.indd 1 07/09/2012 14:45

• Superior Bronchodilation
versus tiotropium1,2,*
• 5 minute rapid onset of action3
A first line once daily maintenance treatment for COPD
1
Onbrez® Breezhaler®
ABBREVIATED PRESCRIBING INFORMATION
Please refer to Summary of Product Characteristics (SmPC) before prescribing. Presentation: Onbrez Breezhaler 150mcg and 300mcg inhalation powder hard capsules containing indacaterol maleate, and separate Onbrez Breezhaler inhaler. Indications: For maintenance bronchodilator treatment of airflow obstruction in adult patients with chronic obstructive pulmonary disease (COPD). Dosage and administration: Recommended dose is the inhalation of the content of one 150mcg capsule once a day, administered at the same time of the day each day, using the Onbrez Breezhaler inhaler. Capsules must not be swallowed. Dose should only be increased on medical advice. The inhalation of the content of one 300mcg capsule once a day has been shown to provide additional clinical benefit with regard to breathlessness, particularly for patients with severe COPD. Maximum dose is 300mcg once daily. No dose adjustment required in elderly patients, for patients with mild and moderate hepatic impairment or for patients with renal impairment. No data available for use in patients with severe hepatic impairment. No relevant use in the paediatric population. Contraindications: Hypersensitivity to the active substance, to lactose or to any of the other excipients. Warnings/Precautions: Asthma: ◆ONBREZ BREEZHALER SHOULD NOT BE USED IN ASTHMA. Paradoxical bronchospasm: ◆If paradoxical bronchospasm occurs Onbrez Breezhaler should be discontinued immediately and alternative therapy substituted. Deterioration of disease: ◆Not indicated for treatment of acute episodes of bronchospasm, i.e. as rescue therapy. Systemic effects: ◆Indacaterol should be used with caution in patients with cardiovascular disorders (coronary artery disease, acute myocardial infarction, cardiac arrhythmias, hypertension), in patients with convulsive disorders or thyrotoxicosis, and in patients who are unusually responsive to beta2-adrenergic agonists. Cardiovascular effects: ◆Indacaterol may produce a clinically significant cardiovascular effect in some patients as measured by increases in pulse rate, blood pressure, and/or symptoms, ECG changes. In case such effects occur, treatment may need to be discontinued. Hypokalaemia: ◆ Beta2-adrenergic agonists may produce significant hypokalaemia in some patients, which has the potential to produce cardiovascular effects. In patients with severe COPD, hypokalaemia may be potentiated by hypoxia and concomitant treatment which may increase the susceptibility to cardiac arrhythmias. Hyperglycaemia: ◆Inhalation of high doses of beta2-adrenergic agonists may produce increases in plasma glucose. Upon initiation of treatment with Onbrez Breezhaler plasma glucose should be monitored more closely in diabetic patients. ◆During clinical studies, clinically notable changes in blood glucose were generally more frequent by 1-2% on Onbrez Breezhaler at the recommended doses than on placebo. Onbrez Breezhaler has not been investigated in patients with not well controlled diabetes mellitus. Pregnancy and Lactation: ◆No data available from the use of indacaterol in pregnant women. Onbrez Breezhaler should only be used during pregnancy if the expected benefits outweigh the potential risks. ◆Not known whether indacaterol / metabolites are excreted in human milk. A decision must be made whether to discontinue breast-feeding or discontinue Onbrez Breezhaler therapy, taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman. Interactions: ◆Concomitant administration of other sympathomimetic agents may potentiate the undesirable effects of Onbrez Breezhaler. Onbrez Breezhaler should not be used in conjunction with other long-acting beta2-adrenergic agonists or medicinal products containing long-acting beta2-adrenergic agonists. ◆Concomitant hypokalaemic treatment with methylxanthine derivatives, steroids, or non-potassium-sparing diuretics may potentiate the possible hypokalaemic effect of beta2-adrenergic agonists, therefore use with caution. ◆Indacaterol should not be given together with beta-adrenergic blockers (including eye drops) as these may weaken or antagonise the effect of beta2-adrenergic agonists. Where required, cardioselective beta-adrenergic blockers should be preferred, although they should be administered with caution. ◆Inhibition of the key contributors of indacaterol clearance, CYP3A4 and P-gp, does not raise any safety concerns given the safety experience of treatment with Onbrez Breezhaler. ◆Indacaterol has not been shown to cause interactions with co-medications. Adverse reactions: ◆The most common adverse reactions with Onbrez Breezhaler are: nasopharyngitis, upper respiratory tract infection, sinusitis, diabetes mellitus and hyperglycaemia, headache, ischaemic heart disease, cough, pharyngolaryngeal pain, rhinnorrhoea, respiratory tract congestion, muscle spasm, peripheral oedema. ◆Uncommon: paraesthenia, atrial fibrillation and non-cardiac chest pain. ◆Please refer to SmPC for a full list of adverse events for Onbrez Breezhaler. Legal Category: POM Pack sizes: Carton containing 30 capsules (3x10 capsule blister strips) and one Onbrez Breezhaler inhaler. Marketing Authorisation Holder: Novartis Europharm Limited, Wimblehurst Road, Horsham, West Sussex, RH12 5AB, United Kingdom. Marketing Authorisation Numbers: EU/1/09/593/002 & 007. Full prescribing information is available on request from Novartis Ireland Ltd, Beech Hill Office Campus, Clonskeagh, Dublin 4. Tel: 01 2601255 or at www.medicines.ie Date of Creation of API Text: Jan 2010 Date of Preparation: March 2011 NO0311145 References: 1. Onbrez Breezhaler SmPC. Available at www.medicines.ie 2. Donohue JF et al. Once daily Bronchodilators for Chronic Obstructive Lung Disease: Indacaterol versus Tiotropium. Am J Crit Care Med. Vol 182. Pp 155-162, 2010. 3. Balint et al. Onset of action of indacaterol in patients with COPD: Comparison with salbutamol and salmeterol-fluticasone. International Journal of COPD.2010:5 311-318. * INHANCE Study comparitor was open label tiotropium.
ICGP Yearbook advert 12/10/2011 10:18 Page 1

23
clinical review
Asthma in childrenNIAmh O regAN, PAEDIATRIC RESPIRATORY NURSE
Asthma is the most common chronic disease of child-hood, and is defined as intermittent, reversible ob-structive airway disease. It is a chronic inflammatory disorder of the airways and manifests as recurrent episodes of wheezing, dyspnoea, chest tightness,
and cough. These episodes are associated with variable airflow obstruction that is reversible.1
Asthma is a considerable cause of illness in children and has been shown by The International Study of Asthma and Allergy in Children to place Ireland in the top four countries worldwide for asthma prevalence.2 Asthma currently affects one in seven children in Ireland and is the most common group of diagnosis responsible for hospital admissions to paediatric units.
PresentationA family history of asthma, atopy, or allergic disease is common in patients. It is important to include the following in the initial assessment of the patient:• Duration and nature of symptoms• Treatments used (relievers, preventers); and response to
these treatments• Method of delivery of treatments – pMDI, pMDI and spacer,
or nebulised and the technique used• Trigger factors (including upper respiratory tract infection,
allergy, passive smoking)• Pattern and course of previous acute episodes e.g. admission
or ICU admissions• Parental understanding of the treatment of acute episodes; and• The presence of interval symptoms
• Consider other causes of wheeze e.g. bronchiolitis, aspiration, foreign body, anaphylaxis.
AssessmentThe most important parameters in the assessment of the severity of acute childhood asthma exacerbations are general appearance/mental state and work of breathing (accessory muscle use, recession), as indicated in the table below.• Initial SaO2 in air, heart rate and ability to talk are helpful but
less reliable additional features• Wheeze intensity is not reliable• Asymmetry on auscultation is often found due to mucous
plugging, but warrants consideration of foreign body or pneumothorax
• A prolonged expiratory phase is often a very sensitive sign of diffuse small airway obstruction and will almost always be present, as will expiratory muscle use.Chest x-ray is not generally required as the information
gained is limited. In the case of patients with diffuse bilateral wheeze, bacterial infection is rarely implicated. Antibiotics are only rarely needed in acute asthma as pneumonia is uncommon. Always ask about a temperature. Without a fever, serious bacterial infection is unlikely.
Blood gases are rarely required in the assessment of acute asthma in children.
In the severe or critical episode, a venous blood gas measurement may be useful. However, a normal venous pCO2 value does not rule out a critical problem and should be interpreted with caution.
• Superior Bronchodilation
versus tiotropium1,2,*
• 5 minute rapid onset of action3
A first line once daily maintenance treatment for COPD
1
Onbrez® Breezhaler®
ABBREVIATED PRESCRIBING INFORMATION
Please refer to Summary of Product Characteristics (SmPC) before prescribing. Presentation: Onbrez Breezhaler 150mcg and 300mcg inhalation powder hard capsules containing indacaterol maleate, and separate Onbrez Breezhaler inhaler. Indications: For maintenance bronchodilator treatment of airflow obstruction in adult patients with chronic obstructive pulmonary disease (COPD). Dosage and administration: Recommended dose is the inhalation of the content of one 150mcg capsule once a day, administered at the same time of the day each day, using the Onbrez Breezhaler inhaler. Capsules must not be swallowed. Dose should only be increased on medical advice. The inhalation of the content of one 300mcg capsule once a day has been shown to provide additional clinical benefit with regard to breathlessness, particularly for patients with severe COPD. Maximum dose is 300mcg once daily. No dose adjustment required in elderly patients, for patients with mild and moderate hepatic impairment or for patients with renal impairment. No data available for use in patients with severe hepatic impairment. No relevant use in the paediatric population. Contraindications: Hypersensitivity to the active substance, to lactose or to any of the other excipients. Warnings/Precautions: Asthma: ◆ONBREZ BREEZHALER SHOULD NOT BE USED IN ASTHMA. Paradoxical bronchospasm: ◆If paradoxical bronchospasm occurs Onbrez Breezhaler should be discontinued immediately and alternative therapy substituted. Deterioration of disease: ◆Not indicated for treatment of acute episodes of bronchospasm, i.e. as rescue therapy. Systemic effects: ◆Indacaterol should be used with caution in patients with cardiovascular disorders (coronary artery disease, acute myocardial infarction, cardiac arrhythmias, hypertension), in patients with convulsive disorders or thyrotoxicosis, and in patients who are unusually responsive to beta2-adrenergic agonists. Cardiovascular effects: ◆Indacaterol may produce a clinically significant cardiovascular effect in some patients as measured by increases in pulse rate, blood pressure, and/or symptoms, ECG changes. In case such effects occur, treatment may need to be discontinued. Hypokalaemia: ◆ Beta2-adrenergic agonists may produce significant hypokalaemia in some patients, which has the potential to produce cardiovascular effects. In patients with severe COPD, hypokalaemia may be potentiated by hypoxia and concomitant treatment which may increase the susceptibility to cardiac arrhythmias. Hyperglycaemia: ◆Inhalation of high doses of beta2-adrenergic agonists may produce increases in plasma glucose. Upon initiation of treatment with Onbrez Breezhaler plasma glucose should be monitored more closely in diabetic patients. ◆During clinical studies, clinically notable changes in blood glucose were generally more frequent by 1-2% on Onbrez Breezhaler at the recommended doses than on placebo. Onbrez Breezhaler has not been investigated in patients with not well controlled diabetes mellitus. Pregnancy and Lactation: ◆No data available from the use of indacaterol in pregnant women. Onbrez Breezhaler should only be used during pregnancy if the expected benefits outweigh the potential risks. ◆Not known whether indacaterol / metabolites are excreted in human milk. A decision must be made whether to discontinue breast-feeding or discontinue Onbrez Breezhaler therapy, taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman. Interactions: ◆Concomitant administration of other sympathomimetic agents may potentiate the undesirable effects of Onbrez Breezhaler. Onbrez Breezhaler should not be used in conjunction with other long-acting beta2-adrenergic agonists or medicinal products containing long-acting beta2-adrenergic agonists. ◆Concomitant hypokalaemic treatment with methylxanthine derivatives, steroids, or non-potassium-sparing diuretics may potentiate the possible hypokalaemic effect of beta2-adrenergic agonists, therefore use with caution. ◆Indacaterol should not be given together with beta-adrenergic blockers (including eye drops) as these may weaken or antagonise the effect of beta2-adrenergic agonists. Where required, cardioselective beta-adrenergic blockers should be preferred, although they should be administered with caution. ◆Inhibition of the key contributors of indacaterol clearance, CYP3A4 and P-gp, does not raise any safety concerns given the safety experience of treatment with Onbrez Breezhaler. ◆Indacaterol has not been shown to cause interactions with co-medications. Adverse reactions: ◆The most common adverse reactions with Onbrez Breezhaler are: nasopharyngitis, upper respiratory tract infection, sinusitis, diabetes mellitus and hyperglycaemia, headache, ischaemic heart disease, cough, pharyngolaryngeal pain, rhinnorrhoea, respiratory tract congestion, muscle spasm, peripheral oedema. ◆Uncommon: paraesthenia, atrial fibrillation and non-cardiac chest pain. ◆Please refer to SmPC for a full list of adverse events for Onbrez Breezhaler. Legal Category: POM Pack sizes: Carton containing 30 capsules (3x10 capsule blister strips) and one Onbrez Breezhaler inhaler. Marketing Authorisation Holder: Novartis Europharm Limited, Wimblehurst Road, Horsham, West Sussex, RH12 5AB, United Kingdom. Marketing Authorisation Numbers: EU/1/09/593/002 & 007. Full prescribing information is available on request from Novartis Ireland Ltd, Beech Hill Office Campus, Clonskeagh, Dublin 4. Tel: 01 2601255 or at www.medicines.ie Date of Creation of API Text: Jan 2010 Date of Preparation: March 2011 NO0311145 References: 1. Onbrez Breezhaler SmPC. Available at www.medicines.ie 2. Donohue JF et al. Once daily Bronchodilators for Chronic Obstructive Lung Disease: Indacaterol versus Tiotropium. Am J Crit Care Med. Vol 182. Pp 155-162, 2010. 3. Balint et al. Onset of action of indacaterol in patients with COPD: Comparison with salbutamol and salmeterol-fluticasone. International Journal of COPD.2010:5 311-318. * INHANCE Study comparitor was open label tiotropium.
ICGP Yearbook advert 12/10/2011 10:18 Page 1

24
clinical review
Objective assessment of the paediatric asthma patientIn the assessment of children the following are important considerations:
Pulse oximetryAccurate measurements of oxygen saturation are essential in the assessment of all children with acute wheezing. Oxygen saturation monitors should be available for use by all health professionals assessing acute asthma in both primary and secondary care settings. Low oxygen saturations after initial bronchodilator treatment select a more severe group of patients. Consider further treatment for children with SpO2 <92% in room air after initial bronchodilator treatment.
Pef or fev1There are significant limitations in the use of PEF in children with acute asthma, however PEF measurements may be of benefit in assessing some children who are familiar with the use of such devices. In general peak flow is rarely relied upon in the acute management of children’s asthma in the ED setting. However, when used, the best of three PEF measurements, ideally expressed as a percentage of personal best, can be useful in assessing the response to treatment. A measurement of <50% predicted PEF or FEV1 with poor improvement after initial bronchodilator treatment is predictive of a more prolonged asthma attack.
Acute treatment during an exacerbationThe goal of treatment in an asthma exacerbation is to relieve the airflow obstruction. This is achieved through:• Repetitive administration of rapid-acting inhaled ß2-agonist
bronchodilator through a spacer device in mild to moderate episodes.
• Early introduction of systemic glucocorticosteroids;• Oxygen supplementation.
OxygenMany patients with acute severe asthma are hypoxemic (low blood oxygen). Supplementary oxygen should be given urgently to hypoxemic patients, using a face mask, Venturi mask or nasal cannula with flow rates adjusted as necessary to maintain SpO2 of 92%. It is important to maintain a SpO2 level of 92%. A lack of pulse oximetry should not prevent the use of oxygen.
bronchodilators – repeated administration of rapid-acting inhaled ß2-agonistIn most cases inhaled ß2-agonists given in high doses act quickly to relieve bronchospasm with few side effects. There is no evidence for any difference in efficacy between salbutamol and terbutaline.
In acute asthma without life-threatening features, ß2-agonists should be administered by repeated activations of a MDI via an appropriate spacer or, if a spacer/MDI is unavailable, by wet nebulisation driven by oxygen. Metered dose inhalers with spacers can be used for patients with exacerbations of asthma other than life-threatening. The bronchodilator therapy delivered via a metered-dose inhaler (MDI), ideally with a spacer, produces at least an equivalent improvement in lung function as the same dose delivered via nebuliser. This route of delivery is the most cost effective, provided patients are able to use an MDI.
Mild exacerbations: in children under 6 years of age 6 puffs every 20 minutes, over 6 years of age 12 puffs every 20 minutes for the first hour. Continue with 6-12 puffs every one-to – four hours. No additional medication is necessary if the rapid-acting inhaled ß2-agonist produces a complete response (FEV1 or PEF returns to greater than 80% of predicted or personal best) and the response lasts for 3 to 4 hours.
Oxygen-driven nebulisers are preferred for nebulising ß2-agonist bronchodilators because of the risk of oxygen desaturation while using air-driven compressors. Emergency oxygen should be available in hospitals, ambulances and primary care. A flow rate of 6 litres/min is required to drive most nebulisers. In hospital, ambulance and primary care, nebulised ß2-agonist bronchodilators should preferably be driven by oxygen. Repeat doses of ß2-agonists at 15-30 minute intervals or give continuous nebulisation of salbutamol at 5-10mg/hour (requires appropriate nebuliser) if there is an inadequate response to initial treatment.
glucocorticosteroids (steroids)Steroids reduce mortality, relapses, subsequent hospital admission and requirement for ß2 agonist therapy. The earlier they are given in the acute attack the better the outcome. Oral glucocorticosteroids (1mg of prednisolone/kg or equivalent during a 24-hour period) should be used to treat exacerbation, especially if they develop after instituting other short-term treatment options recommended for loss of control.
Prednisolone 1mg/kg/day (up to a maximum of 40mg daily) for 3 days or parenteral hydrocortisone 4mg/kg up to a maximum of 160mg is as effective as higher doses. Where necessary soluble prednisolone (sodium phosphate) 5mg tablets can be used.
The assessment of asthma control includes assessment of the clinical manifestations of the condition. This can be challenging in children under the age of five.

Xarelto 10 mg film-coated tablets (Rivaroxaban).Please refer to full SmPC before prescribing. Presentation: Film-coated tablet containing 10mg rivaroxaban. Indication: Prevention of venousthromboembolism (VTE) in adult patients undergoing elective hip or knee replacement surgery. Dosage and Administration: Recommendeddose is 10 mg rivaroxaban taken orally once daily. The initial dose should be taken 6 to 10 hours after surgery, provided that haemostasis hasbeen established. Duration of treatment depends on the individual risk of the patient for VTE which is determined by the type of orthopaedicsurgery. For patients undergoing major hip surgery, treatment duration of 5 weeks is recommended. For major knee surgery, treatment durationof 2 weeks is recommended. Renal impairment: No dose adjustment is necessary in patients with mild or moderate renal impairment. Use withcaution in patients with severe renal impairment. Not recommended in patients with creatinine clearance <15 ml/min. Hepatic impairment:Contraindicated in patients with hepatic disease associated with coagulopathy and clinically relevant bleeding risk, including cirrhotic patientswith Child Pugh B and C. Paediatric population: Xarelto is not recommended for use in children below 18 years of age, no data is available in thispopulation. Contraindications: Hypersensitivity to the active substance or to any of the excipients; clinically significant active bleeding; hepaticdisease associated with coagulopathy and clinically relevant bleeding risk including cirrhotic patients with Child Pugh B and C hepatic impairment;pregnancy and breast feeding. Warnings and Precautions: Not recommended: in patients receiving concomitant systemic treatment with strongCYP3A4 and P-gp inhibitors, i.e. azole-antimycotics or HIV protease inhibitors; patients with severe renal impairment (creatinine clearance <15ml/min); patients below 18 years of age (due to lack of data); patients undergoing hip fracture surgery (due to lack of data), in patients treatedconcomitantly with dronedarone. Use with caution: in patients with severe renal impairment (creatinine clearance 15 - 29 ml/min) or moderaterenal impairment (creatinine clearance 30 49 ml/min) or with renal impairment concomitantly receiving other medicinal products which increaserivaroxaban plasma concentrations; patients treated concomitantly with medicinal products affecting haemostasis (such as NSAIDs, acetylsalicylicacid, platelet aggregation inhibitors, other antithrombotic agents) or with strong CYP3A4 inducers; in patients with increased bleeding risk; whenneuraxial anaethesisa or spinal/epidural puncture is employed; patients with congenital or acquired bleeding disorders, uncontrolled severe arterialhypertension, active ulcerative gastrointestinal disease, recent gastrointestinal ulcerations, vascular retinopathy, recent intracranial or intracerebralhaemorrhage, intraspinal or intracerebral vascular abnormalities, recent brain, spinal or ophthalmological surgery, bronchiectasis or history ofpulmonary bleeding. In patients at risk of ulcerative gastrointestinal disease prophylactic treatment may be considered. There is no need formonitoring of coagulation parameters during treatment with rivaroxaban in routine clinical situations. If clinically indicated rivaroxaban levels canbe measured by calibrated quantitative anti-Factor Xa tests. Xarelto contains lactose. Undesirable effects: Common: anaemia (incl. respectivelaboratory parameters), dizziness, headache, syncope, eye haemorrhage, tachycardia, hypotension, haematoma, epistaxis, gastrointestinal tracthaemorrhage (incl. gingival bleeding and rectal haemorrhage), abdominal and gastrointestinal pain, dyspepsia, nausea, constipation, diarrhoea,vomiting, pruritus (incl. uncommon cases of generalised pruritus), rash, ecchymosis, pain in extremity, urogenital tract haemorrhage (incl. haematurisand menorrhagia), fever, peripheral oedema, decreased general strength and energy (incl. fatigue and asthenia), increase in transaminases, post-procedural haemorrhage (incl. post-operative anaemia and wound haemorrhage), contusion, wound secretion. Uncommon: thrombocythaemia(incl. platelet count increased), allergic reaction, dermatitis allergic, cerebral and intracranial haemorrhage, haemoptysis, dry mouth, hepatic functionabnormal, urticaria, cutaneous and subcutaneous haemorrhage, haemarthrosis, renal impairment (incl. blood creatinine increased, blood ureaincreased), feeling unwell (incl. malaise), localised oedema, increases in: bilirubin, blood alkaline phosphatase, LDH, lipase, amylase and GGT.Rare: jaundice, muscle haemorrhage, bilirubin conjugated increased (with or without concomitant increased ALT.) Frequency not known:pseudoaneurysm formation following percutaneous intervention, compartment syndrome secondary to a bleeding, renal failure/acute renal failuresecondary to a bleeding sufficient to cause hypoperfusion. Prescription only. Marketing Authorisation Holder: Bayer Pharma AG, D-13342Berlin, Germany. MA numbers: EU/1/08/472/006 - 008 Further information available from: Bayer Ltd., The Atrium, Blackthorn Road, Dublin18. Tel: 01 2999313. Date of Preparation: 6/2012.
Xarelto 15mg and 20mg film-coated tablets (Rivaroxaban).Please refer to full SmPC before prescribing. Presentation: Film-coated tablet containing 15mg or 20mg of rivaroxaban. Indication: Preventionof stroke and systemic embolism in adult patients with non-valvular atrial fibrillation with one or more risk factors, such as congestive heart failure,hypertension, age ≥ 75 years, diabetes mellitus, prior stroke or transient ischaemic attack. Treatment of deep vein thrombosis (DVT) and preventionof recurrent DVT and pulmonary embolism (PE) following an acute DVT in adults. Dosage and Administration: : Prevention of stroke and systemicembolism: The recommended dose is 20 mg once daily, which is also the recommended maximum dose. Treatment of DVT and prevention of recurrentDVT and PE: The recommended dose for the initial treatment of acute DVT is 15 mg twice daily for the first three weeks followed by 20 mg oncedaily for the continued treatment and prevention of recurrent DVT and PE. Renal impairment: No dose adjustment is necessary in patients with mildrenal impairment. Patients with moderate or severe renal impairment, for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation, the recommended dose is 15mg once daily, and for the treatment of DVT and prevention of recurrent DVT and PE, treatmentshould be 15mg twice daily for the first 3 weeks, thereafter the recommended dose is 15mg once daily. Hepatic impairment: Contraindicated inpatients with hepatic disease associated with coagulopathy and clinically relevant bleeding risk including cirrhotic patients with Child Pugh B andC. Contraindications: Hypersensitivity to the active substance or any of the excipients; clinically significant active bleeding; hepatic diseaseassociated with coagulopathy and clinically relevant bleeding risk including cirrhotic patients with Child Pugh B and C hepatic impairment; pregnancyand breast feeding. Warnings and Precautions: Not recommended: in patients receiving concomitant systemic treatment with strong concurrentCYP3A4- and P-gp-inhibitors, i.e. azole-antimycotics or HIV protease inhibitors; in patients with severe renal impairment (creatinine clearance <15ml/min); in the treatment of acute pulmonary embolism; in patients below 18 years of age or with prosthetic heart valves or in patients concomitantlytreated with dronedarone due to lack of data. Use with caution: in patients with severe renal impairment (creatinine clearance 15 - 29 ml/min) orwith renal impairment concomitantly receiving other medicinal products which increase rivaroxaban plasma concentrations; patients concomitantlytreated with medicinal products affecting haemostasis (such as NSAIDs, acetylsalicylic acid, platelet aggregation inhibitors, other antithromboticagents) or with strong CYP3A4 inducers; in patients with increased bleeding risk; patients with congenital or acquired bleeding disorders, uncontrolledsevere arterial hypotension, active ulcerative gastrointestinal disease, recent gastrointestinal ulcerations, vascular retinopathy, recent intracranial orintracerebral haemorrhage, intraspinal or intracerebral vascular abnormalities, recent brain, spinal or opthalmological surgery, bronchiectasis orhistory of pulmonary bleeding. In patients at risk of ulcerative gastrointestinal disease an appropriate prophylactic treatment may be considered.Clinical surveillance in line with anticoagulation practice is recommended throughout the treatment period. There is no need for monitoring ofcoagulation parameters during treatment with rivaroxaban in routine clinical situations. If clinically indicated rivaroxaban levels can be measured bycalibrated quantitative anti-Factor Xa tests. Xarelto contains lactose. Undesirable effects: Common: anaemia, dizziness, headache, syncope, eyehaemorrhage, tachycardia, hypotension, haematoma, epistaxis, gastrointestinal tract haemorrhage, gastrointestinal and abdominal pains, dyspepsia,nausea, constipation, diarrhoea, vomiting, pruritus, rash, ecchymosis, pain in extremity, urogenital tract haemorrhage, fever, peripheral oedema,decreased general strength and energy, increase in transaminases, post-procedural haemorrhage, contusion, wound secretion. Uncommon:thrombocythemia, allergic reaction, dermatitis allergic, cerebral and intracranial haemorrhage, haemoptysis, dry mouth, hepatic function abnormal,urticaria, cutaneous and subcutaneous haemorrhage, haemarthrosis, renal impairment, feeling unwell, localised oedema, increases in: bilirubin,blood alkaline phosphatase, LDH, lipase, amylase, GGT. Rare: jaundice, muscle haemorrhage and conjugated bilirubin increased. Frequency not known:pseudoaneurysm following percutaneous intervention, compartment syndrome or (acute) renal failure secondary to a bleeding. Prescription only.Marketing Authorisation Holder: Bayer Pharma AG, D-13342 Berlin, Germany. MA numbers: EU/1/08/472/011-21. Further informationavailable from: Bayer Ltd., The Atrium, Blackthorn Road, Dublin 18. Tel: 01 2999313. Date of Preparation: 6/2012.
References: 1. Xarelto® 10mg Summary of Product Characteristics. 2. Eriksson et al, Oral rivaroxaban for the prevention of symptomatic venous thromboembolism after elective hip and knee replacement. J Bone Joint Surg [Br] 2009;91-B:636-44. 3. Turpie G et al.Rivaroxaban versus enoxaparinfor thromboprophylaxis after total knee arthroplasty (RECORD4): a randomised trial. Lancet 2009; 373: 1673–80. 4. Xarelto® 15/20mg Summary of Product Characteristics.
Xarelto®: One Anticoagulant ProtectingAgainst and Treating Many Clot Threats
Widely approved
Prevention of venous thromboembolism (VTE) in adult patients undergoing elective hip or knee replacement surgery1
• Licenced since 2008 in this indication
• Proven superiority versus enoxaparin in RECORD trial programme2,3
Newly approved
Prevention of stroke and systemic embolism in adultpatients with non�valvular atrial fibrillation (AF) withone or more risk factors, such as congestive heart failure,hypertension, age ≥ 75 years, diabetes mellitus, priorstroke or transient ischaemic attack4
Treatment of deep vein thrombosis (DVT), and preventionof recurrent DVT and pulmonary embolism (PE) following an acute DVT in adult patients4
L.IE.GM.07.2012.0030
Xarelto Combi A4 Irish Pharmacist(F):Layout 1 16/08/2012 17:28 Page 1

26
clinical review
Following recovery from the acute exacerbation steroids when given for less than 7 days can be stopped abruptly. Doses do not need tapering provided the patient receives inhaled steroids. It is not known if inhaled steroids provide further benefit in addition to systemic steroids. Inhaled steroids should however be started, or continued as soon as possible to commence the chronic asthma management plan.
Ipratropium bromide Combining nebulised ipratropium bromide with a nebulised ß2-agonist produces significantly greater bronchodilation than a ß2-agonist alone in moderate – to – severe asthma exacerbations, leading to a faster recovery and shorter duration of admission. Anticholinergic treatment is not necessary and may not be beneficial in milder exacerbations of asthma or after stabilisation.3
Asthma controlThe goal of asthma management is to achieve and maintain control of the disease. The assessment of asthma control includes assessment of the clinical manifestations of the condition. This can be challenging in children under the age of five as it is dependant on reports from parents and caregiver’s. GINA (2009) has developed a guide to assist in assessing asthma control in this age group. (Table 2)
Asthma managementManagement of asthma can include non pharmacological approaches including the development of a partnership with family and the healthcare team, avoidance of risk factors, appropriate planning, assessing and treatment of asthma symptoms and the development of an asthma management plan than can guide treatment in the home environment.
Common environmental triggers include pollens, moulds, house dust mites, animal dander, cigarette smoke and pollution. Drugs such as the non steroidal anti inflammatories can also trigger an asthma response.
Avoidance measures should be advised in relation to these triggers. Tobacco smoke damages the lungs by reducing the effectiveness of the cilia in removing irritants from the airways. It also affects the ability of inhaled corticosteroids to reduce inflammation leading to a need for higher doses, increase in
symptoms and decline in lung function. Tobacco smoke should be avoided with parents, care givers advised to stop smoking. Referral to smoking cessation supports may assist with this.
Reasonable methods within the home to reduce exposure to triggers such as the house dust mite include washing linen in a hot wash weekly, use of mattress and pillow casings, reduction of clutter in the bedroom and not having the child there when vacuuming.
Where there are pets in the family home they should ideally be housed outside and kept out of bedrooms. Frequent washing of pets can reduce dander. To reduce exposure to pollens close windows and doors during peak pollen time and change clothes and wash hands and face when coming into the house to reduce exposure time.
educationAt diagnosis and following an exacerbation it is important to assess the patient’s and carer’s asthma knowledge re the disease process, use of medications, trigger avoidance and inhaler technique. Nurses have a particular role to play in helping patients/carers to achieve control of their asthma, guiding the use of asthma management plans, addressing concerns regarding medication use, reviewing and assessing asthma control and offering advice on issues related to asthma management.4
Education regarding correct inhaler technique is an important part of asthma education. There is a range of devices available for children and the choice depends on the child’s needs, ability to use, compliance to treatment and cost. Information regarding the correct technique is available on www.asthmasociety.ie.
references1. Global Initiative for Asthma (GINA) Global Strategy for
Asthma Management and Prevention, 2010.2. Prevalence of symptoms of severe asthma and allergies in
Irish school children: an ISAAC protocol study, 1995-2007. Int J Environ Res Public Health. 2011 Aug ;8(8):3192-201. Epub 2011 Aug 2.
3. National Clinical Care Programme for Asthma, Paediatric Asthma Emergency Guidelines (2012).
4. http://www.nursinginpractice.com/article/ascend-module-4.
Table 2: levels of asthma control (children under 5 years|)
Characteristic Controlled(All of the following)
Partly controlled(Any measure present in any week)
Uncontrolled(Three or more features of partly controlled asthma in any week)
daytime symptoms: wheeze, cough, difficult breathing
None(<twice/week, typically for short periods, relieved by use of reliever)
More than twice/ week(<twice/week, typically for short periods, relieved by use of reliever)
More than twice/ week(typically lasts minutes /hours or recur, partly or fully relieved by use of reliever)
limitations on activities None(child is fully active, runs without symptoms)
Any(may cough, wheeze or have difficulty breathing during exercise, vigorous play or laughing)
Any(may cough, wheeze or have difficulty breathing during exercise, vigorous play or laughing)
Nocturnal symptoms / awakening
None Any Any
Need for reliever / rescue treatment
≤ 2 days / week > 2 days/ week > 2 days / week
* any exacerbation should prompt a review of maintenance treatment to ensure that it is adequate. Although patients with current clinical control are less likely to experience exacerbations, they are still at risk during viral upper respiratory tract infections and may have one or more exacerbations per year.

1 sachet daily
Protelos is proven to be an effective long term 1st line treatment option in postmenopausal osteoporosis to reduce vertebral and hip fractures, by rebalancing bone turnover in favour of bone formation 1
Protelos (strontium ranelate) abbreviated prescribing information: Please refer to the Summary of product Characteristics before prescribing. Presentation: Sachet containing 2g of strontium ranelate granules for oral suspension. Indication: Treatment of postmenopausal osteoporosis to reduce the risk of vertebral and hip fractures. Dosage and Administration: The recommended daily dose is one 2g sachet once daily by oral administration at bedtime, preferably at least two hours after eating. The granules in the sachets must be taken as a suspension in a glass of water. Due to the nature of the treated disease, strontium ranelate is intended for long-term use. Generally, calcium and vitamin D supplements are advised in women with low dietary intake. Elderly (>65): No dosage adjustment is required in relation to the elderly. Renal Impairment: No dosage adjustment is required in patients with mild-to-moderate renal impairment (30-70 ml/min creatinine clearance). Strontium ranelate is not recommended for patients with severe renal impairment (creatinine clearance below 30 ml/min). Hepatic Impairment: As strontium ranelate is not metabolised, no dosage adjustment is required in patients with hepatic impairment. Paediatric Population: The safety and efficacy of Protelos in children aged below 18 years have not been established. No data are available. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Precautions: VTE: Protelos is associated with an increased risk for venous thrombo-embolic events (VTE). The cause of this finding is unknown. Protelos should be used with caution in patients at increased risk of VTE, including patients with a past history of VTE. Skin reactions: Cases of severe hypersensitivity syndromes, including, in particular, drug rash with eosinophilia and systemic symptoms (DRESS), sometimes fatal, have been reported with use. Interaction with laboratory test: Strontium interferes with colorimetric methods for the determination of blood and urinary calcium concentrations. Therefore, in medical practice, inductively coupled plasma atomic emission spectrometry or atomic absorption spectrometry methods should be used to ensure an accurate assessment of blood and urinary calcium concentrations. Excipient: Protelos contains a source of phenylalanine which could be harmful for people with phenylketonuria. Interactions: Food, milk and derivative products, and medicinal products containing calcium may reduce the bioavailability of strontium ranelate, therefore, administration of Protelos and such products should be separated by at least two hours. It is preferable to take antacids at least two hours after Protelos, however, when this dosing regimen is impractical due to the recommended administration of Protelos at bedtime, concomitant intake remains acceptable. Protelos therapy should be temporarily suspended if a patient is on a course of oral quinolone or tetracycline antibiotics as it may hinder their absorption. Fertility, pregnancy and lactation: Protelos is only intended for use in postmenopausal women. There are no data from the use of strontium ranelate in pregnant women. Physicochemical data suggest excretion of strontium ranelate in human milk. Protelos should not be used during breast-feeding. No effects were observed on males and females fertility in animal studies. Undesirable effects: Overall incidence rates for adverse events with strontium ranelate did not differ from placebo and adverse events were usually mild and transient. The most common adverse events (frequencies versus placebo) consisted of nausea (7.1% vs. 4.6%), and diarrhoea (7.0% vs. 5.0%), which were generally reported at the beginning of treatment with no noticeable difference between groups afterwards. Other adverse events included: headache (3.3% vs. 2.7%), memory loss (2.5% vs. 2.0%), disturbance of
consciousness (2.6% vs. 2.1%), dermatitis (2.3% vs. 2.0%), eczema (1.8% vs. 1.4%), venous thromboembolism (2.7% vs. 1.9%), increases in blood creatinine kinase (1.4% vs. 0.6%). Other adverse reactions where frequency was unknown include: Severe hypersensitivity skin reactions including Stevens-Johnson syndrome and DRESS; alopecia; oral mucosal irritation; bronchial hyperreactivity, hepatobiliary disorders, bone marrow failure insomnia, dyspepsia, gastroesophageal reflux, constipation, flatulence and hepatitis. Undesirable effects associated with hypersensitivity skin reactions include pyrexia, lymphadenopathy and eosinophilia. See Summary of Product Characteristics for further details. Presentation: Box containing 28 sachets. Legal Category: POM. Marketing Authorisation Numbers and Holder: EU/1/04/288/001-006, Les Laboratoires Servier, 50, rue Carnot 92284 Suresnes cedex France. Date of Preparation or Last Review: December 2011. Full prescribing information is available from: Servier Laboratories, Block 2, West Pier Business Campus, Old Dunleary Road, Dun Laoghaire, Co. Dublin. Tel: (01) 6638110, Fax: (01) 6638120. Date of Preparation of Item: December 2011.
1. Protelos Summary of Product Characteristics PRTPA002
Strontium ranelate
Improve Strength Reduce Fractures1
Advert.indd 1 19/12/2011 14:34

Think Choice
CIALIS* (TADALAFIL) REPUBLIC OF IRELAND ABBREVIATED PRESCRIBING INFORMATION Presentation Tablets 2.5mg, 5mg, 10mg, or 20mg of tadalafil. Also contains lactose. Uses Treatment of erectile dysfunction in adult males. Dosage and Administration Adult men: The recommended dose is 10mg orally, taken at least 30 minutes prior to sexual activity. In those patients in whom tadalafil 10mg does not produce an adequate effect, 20mg might be tried. Maximum dosing frequency, once per day. 10mg or 20mg tadalafil is not recommended for continuous daily use. In patients who anticipate a frequent use of Cialis (ie, at least twice weekly), a once daily regimen with the lowest doses of Cialis might be considered. The recommended dose is 5mg taken once a day at approximately the same time of day. The dose may be decreased to 2.5mg once a day based on individual tolerability. The appropriateness of continued use of the daily regimen should be reassessed periodically. Elderly: Dosage adjustment not required. Impaired renal or hepatic function: In patients with severe renal impairment the maximum recommended dose is 10mg. Once a day dosing of Cialis is not recommended in patients with severe renal impairment. In men with hepatic impairment the recommended dose is 10mg. There are no available data about the administration of doses higher than 10mg of tadalafil to patients with hepatic impairment. There is limited clinical data on the safety of Cialis in patients with severe hepatic impairment; if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Once a day dosing has not been evaluated in patients with hepatic impairment; therefore, if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Diabetes: Dosage adjustment not required. Use in children and adolescents: Cialis should not be used in individuals below 18 years of age. Not indicated for use by women. In clinical trials, Cialis demonstrated improvement in patients’ erectile function and the ability to have successful sexual intercourse up to 36 hours following dosing. Contra-indications Known hypersensitivity to any ingredient. Patients using any form of organic nitrates. In men with cardiac disease for whom sexual activity is inadvisable. Physicians should consider the potential cardiac risk of sexual activity in patients with pre-existing cardiovascular disease. Patients with myocardial infarction within the last 90 days, patients with unstable angina or angina occurring during sexual intercourse, patients with New York Heart Association class 2 or greater heart failure in the last 6 months, patients with uncontrolled arrhythmias, hypotension (<90/50mmHg), or uncontrolled hypertension, patients with a stroke within the last 6 months. Cialis is contra-indicated in patients who have loss of vision in one eye because of non-arteritic anterior ischaemic optic neuropathy (NAION), regardless of whether this episode was in connection or not with previous PDE5 inhibitor exposure. Warnings and Special Precautions Prior to any treatment for erectile dysfunction, physicians should consider the cardiovascular status of their patients, since there is a degree of cardiac risk associated with sexual activity. Tadalafil has vasodilator properties, resulting in mild and transient decreases in blood pressure. It augments the hypotensive effect of nitrates. Tadalafil (2.5mg and 5mg): In patients receiving concomitant antihypertensive medicines, tadalafil may induce a blood pressure decrease. When initiating daily treatment with tadalafil, appropriate clinical considerations should be given to a possible dose adjustment of the antihypertensive therapy. Serious cardiovascular events were reported either post-marketing and/or in clinical trials. Although most of the patients in whom these events have been observed had pre-existing cardiovascular risk factors, it is not possible to determine whether these events are related directly to these risk factors, to Cialis, to sexual activity, or to a combination of these or other factors. Visual defects and cases of NAION have been reported in connection with the intake of Cialis and other PDE5 inhibitors. In case of sudden visual defect, patients should be advised to stop taking Cialis and consult a physician immediately. Due to increased tadalafil exposure (AUC), limited clinical experience, and the lack of ability to influence clearance by dialysis, once a day dosing of Cialis is not recommended in patients with severe renal impairment. There is limited clinical data on the safety of single-dose administration of tadalafil in patients with severe hepatic insufficiency (Child-Pugh class C); if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Use with caution in patients who have conditions that might predispose them to priapism, or in patients with anatomical deformation of the penis. Patients who experience erections lasting 4 hours or more should be instructed to seek medical assistance. If priapism is not treated immediately, penile tissue damage and permanent loss of potency may result. It is not known if Cialis is effective in patients who have undergone pelvic surgery or radical non-nerve-sparing prostatectomy. Cialis should not be administered to patients with hereditary problems of galactose intolerance, the Lapp lactase deficiency, or glucose-galactose malabsorption. In patients who are taking alpha1-blockers, concomitant administration of Cialis may lead to symptomatic hypotension in some patients. The combination of tadalafil and doxazosin is not recommended. Caution should be exercised when prescribing Cialis to patients using potent CYP3A4 inhibitors (ritonavir, saquinavir, ketoconazole, itraconazole, and erythromycin) as increased tadalafil exposure (AUC) has been observed if the drugs are combined. The safety and efficacy of combinations of tadalafil and other PDE5 inhibitors or other treatments for erectile dysfunction have not been studied. Patients should be informed not to take Cialis with such combinations. Pregnancy and Lactation Not indicated for use by women. There are limited data from the use of tadalafil in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition, or postnatal development. As a precautionary measure, it is preferable to avoid the use of Cialis during pregnancy. Available pharmacodynamic/toxicological data in animals have shown excretion of tadalafil in milk. A risk to the suckling child cannot be excluded. Cialis should not be used during breast-feeding. Driving, etc No studies on the effect on the ability to drive and use machines have been performed. Although the frequency of reports of dizziness in placebo and tadalafil arms in clinical trials was similar, patients should be aware of how they react to Cialis before driving or operating machinery. Undesirable Effects Very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), and not known (events not reported in registration trials cannot be estimated from post-marketing spontaneous reports). Very common: Headache. Common: Dizziness, flushing, dyspepsia, nasal congestion, back pain, myalgia. Uncommon: Hypersensitivity reactions, blurred vision, sensations described as eye pain, tachycardia, palpitations, hypotension (more commonly reported when tadalafil is given to patients who are already taking antihypertensive agents), hypertension, abdominal pain, gastro-oesophageal reflux, rash, hyperhidrosis (sweating), chest pain(1). Rare: Stroke(1) (including haemorrhagic events), syncope, transient ischaemic attacks(1), migraine(3), visual field defect, swelling of eyelids, conjunctival hyperaemia, myocardial infarction, urticaria, Stevens-Johnson syndrome(3), exfoliative dermatitis(3), prolonged erections, priapism(3), facial oedema(3), seizures, transient amnesia, NAION(3), retinal vascular occlusion(3), sudden hearing loss(2), unstable angina pectoris(3), ventricular arrhythmia(3), epistaxis, sudden cardiac death(1, 3). (1)Most of the patients in whom these events have been reported had pre-existing cardiovascular risk factors. (2)Sudden decrease or loss of hearing has been reported in a small number of post-marketing and clinical trial cases with the use of all PDE5 inhibitors, including tadalafil. (3)Post-marketing surveillance reported adverse reactions not observed in placebo-controlled clinical trials. Adverse reactions reported with tadalafil were transient, and generally mild or moderate. Adverse reaction data are limited in patients >75 years. A slightly higher incidence of ECG abnormalities, primarily sinus bradycardia, has been reported in patients treated with tadalafil once a day as compared with placebo. Most of these ECG abnormalities were not associated with adverse reactions. For full details of these and other side-effects, please see the Summary of Product Characteristics, which is available at http://www.medicines.ie/. Legal Category POM Marketing Authorisation Numbers and Holder EU/1/02/237/001 EU/1/02/237/002 EU/1/02/237/003 EU/1/02/237/004 EU/1/02/237/005 EU/1/02/237/006 EU/1/02/237/007 EU/1/02/237/008. Eli Lilly Nederland BV, Grootslag 1-5 3991, RA Houten, The Netherlands. Date of Preparation or Last Review March 2011. Full Prescribing Information is Available From Eli Lilly and Company Limited Lilly House, Priestley Road Basingstoke, Hampshire, RG24 9NL. Telephone: Basingstoke (01256) 315 000 E-mail: [email protected] or Eli Lilly and Company (Ireland) Limited Hyde House, 65 Adelaide Road, Dublin 2, Republic of Ireland. Telephone: Dublin (01) 661 4377. E-mail: [email protected]. *CIALIS (tadalafil) is a trademark of Eli Lilly and Company. Reference 1. Cialis Summary of Product Characteristics. Eli Lilly and Company Limited.
Date of Preparation: April 2012. IECLS00208
can offer couples the freedom to choose whenthe time is right for them1

29
abstracts
Optimizing treatment outcomes with phosphodiesterase type 5 inhibitors for erectile dysfunction
Sadovsky r, et al.State University
of New York Health Science Center at
Brooklyn and Kings County Hospital
Center, Brooklyn, New York, USA.
Phosphodiesterase type 5 (PDE5) inhibitors have proved to be efficacious, safe, and well tolerated, in clinical trials and practice, for men with erectile dysfunction (ED). However, many patients are not satisfied with treatment and discontinue it prematurely. This review discusses evidence-based strategies that nurse practitioners (NPs) can use to improve diagnosis of ED, optimize patient outcomes, and identify opportunities to detect other potentially serious comorbid conditions.
This article was based on a previously published review, which involved a PubMed-MEDLINE search of the clinical literature from January 1, 1998 (year of sildenafil’s approval in many markets), through August 30, 2008 (date of search). Strategies to optimize responses to PDE5 therapy are summarized by the mnemonic EPOCH: Evaluating and educating to ensure realistic expectations of therapy; Prescribing a treatment individualized to the couple’s needs and preferences; Optimizing drug dose/regimen and revisiting key educational messages at follow-up visits; Controlling comorbidities via lifestyle counseling, medications, and/or referrals; and Helping patients and their partners to seek other forms of therapy if they have decided not to use a PDE5 inhibitor.
The EPOCH mnemonic may remind NPs of steps to optimize treatment outcomes with PDE5 inhibitors.
Discussing a sensitive topic: communication strategies in managing patients with erectile dysfunction
green r, Kodish S.The Little Clinic,
Phoenix, Arizona, USA.
To examine strategies used by nurse practitioners (NPs) and physician assistants (PAs) when discussing the sensitive topic of erectile dysfunction (ED) with patients. A total of 456 NPs and PAs combined responded to a 22-item online survey posted on NP and PA association websites. Four derived categories reflect communication strategies that NPs and PAs applied when addressing ED: initiating the topic directly, initiating the topic with an introduction, initiating the topic when there is a high risk factor, and allowing the patient to bring up the topic. There was also interest in continuing education on the topic of ED and a perceived need for greater emphasis on developing communication strategies within the patient-provider relationship.
There is no one best way to address the topic and different situations may require an approach best suited to the specifics of the situation. Therefore, no single ‘best practice’ of discussing sensitive topics can be identified. Critical thinking skills and the ability to comprehend the totality of the situation are likely to be of higher importance.
Sexual functioning and obesity: a review
Kolotkin rl, zunker C, Ostbye T.Obesity and Quality
of Life Consulting, Durham, NC and
Department of Community and
Family Medicine, Duke University Medical Center,
Durham NC.
The authors reviewed the literature on the relationship between obesity and sexual functioning. Eleven population-based studies, 20 cross-sectional non-population-based studies, and 16 weight loss studies are reviewed. The consistency of findings suggests that the relationship between obesity and reduced sexual functioning is robust, despite diverse methods, instruments, and settings. In most population-based studies, erectile dysfunction (ED) is more common among obese men than among men of recommended weight. Studies of patients in clinical settings often include individuals with higher degrees of obesity, with most studies showing a relationship between obesity and lower levels of sexual functioning, especially ED. The few studies that include both genders generally report more problems among women. Most studies of patients with comorbidities associated with obesity also find an association between obesity and reduced sexual functioning. Most weight loss studies demonstrate improvement in sexual functioning concurrent with weight reduction despite varying study designs, weight loss methods, and follow-up periods. The authors recommend that future studies investigate differences and similarities between men and women with respect to obesity and sexual functioning, use instruments that go beyond the assessment of sexual dysfunction to include additional concepts such as sexual satisfaction, interest, and arousal and, assess how and the degree to which obese individuals are affected by sexual difficulties. Given the high prevalence of obesity and the inverse association between body mass and sexual functioning, they also recommend that sexual functioning should be more fully addressed by clinicians, both in general practice and in weight loss programmes.
FOcuS On: MEn’S HEALTH
Think Choice
CIALIS* (TADALAFIL) REPUBLIC OF IRELAND ABBREVIATED PRESCRIBING INFORMATION Presentation Tablets 2.5mg, 5mg, 10mg, or 20mg of tadalafil. Also contains lactose. Uses Treatment of erectile dysfunction in adult males. Dosage and Administration Adult men: The recommended dose is 10mg orally, taken at least 30 minutes prior to sexual activity. In those patients in whom tadalafil 10mg does not produce an adequate effect, 20mg might be tried. Maximum dosing frequency, once per day. 10mg or 20mg tadalafil is not recommended for continuous daily use. In patients who anticipate a frequent use of Cialis (ie, at least twice weekly), a once daily regimen with the lowest doses of Cialis might be considered. The recommended dose is 5mg taken once a day at approximately the same time of day. The dose may be decreased to 2.5mg once a day based on individual tolerability. The appropriateness of continued use of the daily regimen should be reassessed periodically. Elderly: Dosage adjustment not required. Impaired renal or hepatic function: In patients with severe renal impairment the maximum recommended dose is 10mg. Once a day dosing of Cialis is not recommended in patients with severe renal impairment. In men with hepatic impairment the recommended dose is 10mg. There are no available data about the administration of doses higher than 10mg of tadalafil to patients with hepatic impairment. There is limited clinical data on the safety of Cialis in patients with severe hepatic impairment; if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Once a day dosing has not been evaluated in patients with hepatic impairment; therefore, if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Diabetes: Dosage adjustment not required. Use in children and adolescents: Cialis should not be used in individuals below 18 years of age. Not indicated for use by women. In clinical trials, Cialis demonstrated improvement in patients’ erectile function and the ability to have successful sexual intercourse up to 36 hours following dosing. Contra-indications Known hypersensitivity to any ingredient. Patients using any form of organic nitrates. In men with cardiac disease for whom sexual activity is inadvisable. Physicians should consider the potential cardiac risk of sexual activity in patients with pre-existing cardiovascular disease. Patients with myocardial infarction within the last 90 days, patients with unstable angina or angina occurring during sexual intercourse, patients with New York Heart Association class 2 or greater heart failure in the last 6 months, patients with uncontrolled arrhythmias, hypotension (<90/50mmHg), or uncontrolled hypertension, patients with a stroke within the last 6 months. Cialis is contra-indicated in patients who have loss of vision in one eye because of non-arteritic anterior ischaemic optic neuropathy (NAION), regardless of whether this episode was in connection or not with previous PDE5 inhibitor exposure. Warnings and Special Precautions Prior to any treatment for erectile dysfunction, physicians should consider the cardiovascular status of their patients, since there is a degree of cardiac risk associated with sexual activity. Tadalafil has vasodilator properties, resulting in mild and transient decreases in blood pressure. It augments the hypotensive effect of nitrates. Tadalafil (2.5mg and 5mg): In patients receiving concomitant antihypertensive medicines, tadalafil may induce a blood pressure decrease. When initiating daily treatment with tadalafil, appropriate clinical considerations should be given to a possible dose adjustment of the antihypertensive therapy. Serious cardiovascular events were reported either post-marketing and/or in clinical trials. Although most of the patients in whom these events have been observed had pre-existing cardiovascular risk factors, it is not possible to determine whether these events are related directly to these risk factors, to Cialis, to sexual activity, or to a combination of these or other factors. Visual defects and cases of NAION have been reported in connection with the intake of Cialis and other PDE5 inhibitors. In case of sudden visual defect, patients should be advised to stop taking Cialis and consult a physician immediately. Due to increased tadalafil exposure (AUC), limited clinical experience, and the lack of ability to influence clearance by dialysis, once a day dosing of Cialis is not recommended in patients with severe renal impairment. There is limited clinical data on the safety of single-dose administration of tadalafil in patients with severe hepatic insufficiency (Child-Pugh class C); if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Use with caution in patients who have conditions that might predispose them to priapism, or in patients with anatomical deformation of the penis. Patients who experience erections lasting 4 hours or more should be instructed to seek medical assistance. If priapism is not treated immediately, penile tissue damage and permanent loss of potency may result. It is not known if Cialis is effective in patients who have undergone pelvic surgery or radical non-nerve-sparing prostatectomy. Cialis should not be administered to patients with hereditary problems of galactose intolerance, the Lapp lactase deficiency, or glucose-galactose malabsorption. In patients who are taking alpha1-blockers, concomitant administration of Cialis may lead to symptomatic hypotension in some patients. The combination of tadalafil and doxazosin is not recommended. Caution should be exercised when prescribing Cialis to patients using potent CYP3A4 inhibitors (ritonavir, saquinavir, ketoconazole, itraconazole, and erythromycin) as increased tadalafil exposure (AUC) has been observed if the drugs are combined. The safety and efficacy of combinations of tadalafil and other PDE5 inhibitors or other treatments for erectile dysfunction have not been studied. Patients should be informed not to take Cialis with such combinations. Pregnancy and Lactation Not indicated for use by women. There are limited data from the use of tadalafil in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition, or postnatal development. As a precautionary measure, it is preferable to avoid the use of Cialis during pregnancy. Available pharmacodynamic/toxicological data in animals have shown excretion of tadalafil in milk. A risk to the suckling child cannot be excluded. Cialis should not be used during breast-feeding. Driving, etc No studies on the effect on the ability to drive and use machines have been performed. Although the frequency of reports of dizziness in placebo and tadalafil arms in clinical trials was similar, patients should be aware of how they react to Cialis before driving or operating machinery. Undesirable Effects Very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), and not known (events not reported in registration trials cannot be estimated from post-marketing spontaneous reports). Very common: Headache. Common: Dizziness, flushing, dyspepsia, nasal congestion, back pain, myalgia. Uncommon: Hypersensitivity reactions, blurred vision, sensations described as eye pain, tachycardia, palpitations, hypotension (more commonly reported when tadalafil is given to patients who are already taking antihypertensive agents), hypertension, abdominal pain, gastro-oesophageal reflux, rash, hyperhidrosis (sweating), chest pain(1). Rare: Stroke(1) (including haemorrhagic events), syncope, transient ischaemic attacks(1), migraine(3), visual field defect, swelling of eyelids, conjunctival hyperaemia, myocardial infarction, urticaria, Stevens-Johnson syndrome(3), exfoliative dermatitis(3), prolonged erections, priapism(3), facial oedema(3), seizures, transient amnesia, NAION(3), retinal vascular occlusion(3), sudden hearing loss(2), unstable angina pectoris(3), ventricular arrhythmia(3), epistaxis, sudden cardiac death(1, 3). (1)Most of the patients in whom these events have been reported had pre-existing cardiovascular risk factors. (2)Sudden decrease or loss of hearing has been reported in a small number of post-marketing and clinical trial cases with the use of all PDE5 inhibitors, including tadalafil. (3)Post-marketing surveillance reported adverse reactions not observed in placebo-controlled clinical trials. Adverse reactions reported with tadalafil were transient, and generally mild or moderate. Adverse reaction data are limited in patients >75 years. A slightly higher incidence of ECG abnormalities, primarily sinus bradycardia, has been reported in patients treated with tadalafil once a day as compared with placebo. Most of these ECG abnormalities were not associated with adverse reactions. For full details of these and other side-effects, please see the Summary of Product Characteristics, which is available at http://www.medicines.ie/. Legal Category POM Marketing Authorisation Numbers and Holder EU/1/02/237/001 EU/1/02/237/002 EU/1/02/237/003 EU/1/02/237/004 EU/1/02/237/005 EU/1/02/237/006 EU/1/02/237/007 EU/1/02/237/008. Eli Lilly Nederland BV, Grootslag 1-5 3991, RA Houten, The Netherlands. Date of Preparation or Last Review March 2011. Full Prescribing Information is Available From Eli Lilly and Company Limited Lilly House, Priestley Road Basingstoke, Hampshire, RG24 9NL. Telephone: Basingstoke (01256) 315 000 E-mail: [email protected] or Eli Lilly and Company (Ireland) Limited Hyde House, 65 Adelaide Road, Dublin 2, Republic of Ireland. Telephone: Dublin (01) 661 4377. E-mail: [email protected]. *CIALIS (tadalafil) is a trademark of Eli Lilly and Company. Reference 1. Cialis Summary of Product Characteristics. Eli Lilly and Company Limited.
Date of Preparation: April 2012. IECLS00208
can offer couples the freedom to choose whenthe time is right for them1

• Costs 40% less thannearest competitor1*
• No.1 in Ireland*
• Available in 100 tablet and 60 tablet packs
CALCICHEW-D3 FORTE CHEWABLE TABLETS PRESCRIBING INFORMATION.(Please refer to full Summary of Product Characteristics whenprescribing). Presentation: Chewable tablet containing 1250mg calciumcarbonate (equivalent to 500mg of elemental calcium) plus 400IU colecalciferol(equivalent to 10 micrograms vitamin D3). Uses: Prevention and treatment ofvitamin D/calcium deficiency. Supplementation of vitamin D and calcium as anadjunct to specific therapy for osteoporosis, in pregnancy, in established vitaminD dependent osteomalacia and in other situations requiring therapeuticsupplementation of malnutrition. Dosage and administration: Oral (suck orchew). Adults and elderly: Two tablets daily. Children: Not intended for use inchildren. Hepatic impairment: No dose adjustment required. Renal impairment:Should not be used in patients with severe renal impairment.Contraindications: Diseases and/or conditions resulting in hypercalcaemiaand/or hypercalciuria, severe renal impairment, renal stones, hypervitaminosisD, hypersensitivity to ingredient(s) Precautions: Monitor serum calcium andcreatinine levels, particularly in patients on cardiac glycosides or diuretics andin patients with high tendency to calculus formation. Use with caution inpatients with impaired renal function. Take into account risk of soft tissuecalcification. Avoid in patients with phenylketonuria or sugar intolerance.
Prescribe with caution in patients with sarcoidosis. Use with caution inimmobilised patients. Additional doses of calcium or vitamin D should only betaken under close medical supervision. Interactions: Tetracyclines (take 2hours before, or 4 to 6 hours after Calcichew-D3 Forte), bisphosphonates orsodium fluoride (take 3 hours before Calcichew-D3 Forte), Quinolone antibiotics(take two hours before or after), levothyroxine (take four hours before or after),thiazide diuretics, corticosteroids, cardiac glycosides, ion exchange resins(cholestyramine), laxatives (paraffin oil). Calcichew-D3 Forte should not betaken within 2 hours of eating foods high in oxalic acid (e.g. spinach andrhubarb) or phytic acid (e.g. whole cereals). Side effects: Hypercalcaemia,hypercalciuria, constipation, dyspepsia, flatulence, nausea, abdominal pain,diarrhoea, pruritus, rash, urticaria. Very rarely (usually only seen on overdose)milk-alkali syndrome. Use in pregnancy and lactation: Can be used in case ofcalcium and vitamin D deficiency. Daily intake in pregnancy should not exceed1500mg calcium and 600IU colecalciferol (15 micrograms vitamin D3). Avoidoverdose as permanent hypercalcaemia affects developing foetus. Calcium andvitamin D3 pass into breast milk so consider this when giving additional vitaminD to the child. Pharmaceutical precautions: Do not store above 30°C. Keepcontainer tightly closed to protect from moisture. Legal category: Pharmacy
product. Product Authorisation No: 535/1/3. Product Authorisation holder:Shire Pharmaceuticals Ltd., Hampshire International Business Park, Chineham,Basingstoke, Hampshire RG24 8EP UK. Distributed in Republic of Ireland by:Cahill May Roberts, P.O. Box 1090, Chapelizod, Dublin 20, Republic of Ireland.Further information is available on request. Date of revision: May 2011.CALCICHEW is a registered trademark of Shire Pharmaceuticals Ltd in theRepublic of Ireland.
Adverse events should be reported to the Pharmacovigilance Unit atthe Irish Medicines Board (IMB) ([email protected]).Information about adverse event reporting can be found on the IMBwebsite (www.imb.ie). Adverse events may also be reported to ShirePharmaceuticals Ltd on +44 1256 894000.
Reference: 1. MIMS May 2012.
Date of preparation: June 2012.Item Code: IRE/BU/CDF/12/0007.*According to IMS unit sales data April 2012.
Their strength is our forte
HELP PROTECT THEFRAGILE ELDERLY
NEW60 TABLETPACK
Calcichew New Pack A4_Layout 1 03/07/2012 15:30 Page 1

31
abstracts
Longitudinal study on physical fitness parameters influencing bone mineral density reduction in middle-aged and elderly women: bone mineral density in the lumbar spine, femoral neck, and femur
Iida T, et alDepartment of
Public Health, Fujita Health University
School of Medicine, Japan
The prolongation of the average life span of women has been associated with the rapidly aging society. However, serious problem have arisen as a result, such as an increase in the number of bed-ridden elderly patients with osteoporosis-associated femoral neck fracture. As preventive measures against osteoporosis for middle-aged to elderly women, 10,000 steps per day and intense exercise have been reported to inhibit bone mineral density (BMD) reduction. However, only a few studies have concretely reported on the type of physical fitness that is effective for BMD in particular parts of the body. In this study, a one-year longitudinal survey was performed involving generally healthy postmenopausal women to investigate physical fitness parameters influencing BMD in the lumbar spine, femoral neck, and femur. The subjects were 38 female residents of M City, aged 49-73 years. As physical fitness parameters, sit-ups, anteflexion in a sitting position, grip strength, mean amount of exercise (kcal), and area of outer body sway on standing straight with the eyes closed (m2) were measured. The BMD was measured in the lumbar spine (L2-L4), femoral neck, and femur. Logistic regression analysis was performed regarding the physical fitness parameters as explanatory variables and groups with and without BMD reduction over one year as those with and without risk as dependent variables. The number of sit-ups (odds ratio: 0.76, 95% CI: 0.61-0.96, p=0.022) was a preventive factor against BMD reduction of the lumbar spine, and ante flexion in a sitting position was a preventive factor against BMD reduction of the femoral neck (odds ratio: 0.88, 95% CI: 0.78-0.99, p=0.029). Regarding BMD reduction of the femur, the area of outer body sway on standing straight with the eyes closed tended to be not significant to the risk. It is suggested that physical fitness and local muscle strength are associated with BMD reduction in the lumbar spine, femoral neck, and femur.
Position of the uS Academy of nutrition and Dietetics: the impact of fluoride on health
Palmer CA, gilbert JA.
It is the position of the Academy of Nutrition and Dietetics to support optimal systemic and topical fluoride as an important public health measure to promote oral health and overall health throughout life. Fluoride is an important element in the mineralization of bone and teeth. The proper use of topical and systemic fluoride has resulted in major reductions in dental caries and its associated disability. Dental caries remains the most prevalent chronic disease in children and affects all age groups of the population. The Centers for Disease Control and Prevention has named fluoridation of water as one of the 10 most important public health measures of the 21st century. Currently, >72% of the US population that is served by community water systems benefits from water fluoridation. However, only 27 states provide fluoridated water to more than three quarters of the state’s residents on public water systems. Fluoride also plays a role in bone health. However, at this time, use of high doses of fluoride for osteoporosis prevention is considered experimental only. Dietetics practitioners should routinely monitor and promote the use of fluorides for all age groups.
FOcuS On: OSTEOPOrOSiS
• Costs 40% less thannearest competitor1*
• No.1 in Ireland*
• Available in 100 tablet and 60 tablet packs
CALCICHEW-D3 FORTE CHEWABLE TABLETS PRESCRIBING INFORMATION.(Please refer to full Summary of Product Characteristics whenprescribing). Presentation: Chewable tablet containing 1250mg calciumcarbonate (equivalent to 500mg of elemental calcium) plus 400IU colecalciferol(equivalent to 10 micrograms vitamin D3). Uses: Prevention and treatment ofvitamin D/calcium deficiency. Supplementation of vitamin D and calcium as anadjunct to specific therapy for osteoporosis, in pregnancy, in established vitaminD dependent osteomalacia and in other situations requiring therapeuticsupplementation of malnutrition. Dosage and administration: Oral (suck orchew). Adults and elderly: Two tablets daily. Children: Not intended for use inchildren. Hepatic impairment: No dose adjustment required. Renal impairment:Should not be used in patients with severe renal impairment.Contraindications: Diseases and/or conditions resulting in hypercalcaemiaand/or hypercalciuria, severe renal impairment, renal stones, hypervitaminosisD, hypersensitivity to ingredient(s) Precautions: Monitor serum calcium andcreatinine levels, particularly in patients on cardiac glycosides or diuretics andin patients with high tendency to calculus formation. Use with caution inpatients with impaired renal function. Take into account risk of soft tissuecalcification. Avoid in patients with phenylketonuria or sugar intolerance.
Prescribe with caution in patients with sarcoidosis. Use with caution inimmobilised patients. Additional doses of calcium or vitamin D should only betaken under close medical supervision. Interactions: Tetracyclines (take 2hours before, or 4 to 6 hours after Calcichew-D3 Forte), bisphosphonates orsodium fluoride (take 3 hours before Calcichew-D3 Forte), Quinolone antibiotics(take two hours before or after), levothyroxine (take four hours before or after),thiazide diuretics, corticosteroids, cardiac glycosides, ion exchange resins(cholestyramine), laxatives (paraffin oil). Calcichew-D3 Forte should not betaken within 2 hours of eating foods high in oxalic acid (e.g. spinach andrhubarb) or phytic acid (e.g. whole cereals). Side effects: Hypercalcaemia,hypercalciuria, constipation, dyspepsia, flatulence, nausea, abdominal pain,diarrhoea, pruritus, rash, urticaria. Very rarely (usually only seen on overdose)milk-alkali syndrome. Use in pregnancy and lactation: Can be used in case ofcalcium and vitamin D deficiency. Daily intake in pregnancy should not exceed1500mg calcium and 600IU colecalciferol (15 micrograms vitamin D3). Avoidoverdose as permanent hypercalcaemia affects developing foetus. Calcium andvitamin D3 pass into breast milk so consider this when giving additional vitaminD to the child. Pharmaceutical precautions: Do not store above 30°C. Keepcontainer tightly closed to protect from moisture. Legal category: Pharmacy
product. Product Authorisation No: 535/1/3. Product Authorisation holder:Shire Pharmaceuticals Ltd., Hampshire International Business Park, Chineham,Basingstoke, Hampshire RG24 8EP UK. Distributed in Republic of Ireland by:Cahill May Roberts, P.O. Box 1090, Chapelizod, Dublin 20, Republic of Ireland.Further information is available on request. Date of revision: May 2011.CALCICHEW is a registered trademark of Shire Pharmaceuticals Ltd in theRepublic of Ireland.
Adverse events should be reported to the Pharmacovigilance Unit atthe Irish Medicines Board (IMB) ([email protected]).Information about adverse event reporting can be found on the IMBwebsite (www.imb.ie). Adverse events may also be reported to ShirePharmaceuticals Ltd on +44 1256 894000.
Reference: 1. MIMS May 2012.
Date of preparation: June 2012.Item Code: IRE/BU/CDF/12/0007.*According to IMS unit sales data April 2012.
Their strength is our forte
HELP PROTECT THEFRAGILE ELDERLY
NEW60 TABLETPACK
Calcichew New Pack A4_Layout 1 03/07/2012 15:30 Page 1

32
product news
New paediatric presentation for EnbrelPfizer Healthcare Ireland recently announced the launch of Enbrel 10mg paediatric presentation which will replace Enbrel 25mg paediatric presentation. The current standard 25mg Enbrel pow-der and solvent for solution for injection remains available.
It is estimated that approximately 1 in 1,000 children has juvenile arthritis. Every year about 1 in 10,000 children in Ireland is diagnosed with the condition making it almost as common as childhood diabetes. It can begin at any age, although it most commonly shows up in younger children. It can develop in boys or girls, although most types are more common in girls.
Enbrel (etanercept) is approved in the following paediatric indications:
Polyarticular juvenile idiopathic arthritis (JIA): Treatment of active polyarticular juvenile idiopathic arthritis in children and adolescents from the age of 2 years who have had an inadequate response to, or who have proved intolerant of, methotrexate.
Paediatric plaque psoriasis: Treatment of chronic severe plaque psoriasis in children and adolescents from the age of 6 years who are inadequately controlled by, or are intolerant to, other systemic therapies or phototherapies.
For children with JIA (age 2 years and above), the recommend-ed dose is 0.4 mg/kg (up to a maximum of 25 mg per dose), given twice weekly as a subcutaneous injection with an interval of 3-4 days between doses. Discontinuation of treatment should be considered in patients who show no response after 4 months.
In children with paediatric plaque psoriasis (age 6 years and above) the recommended dose is 0.8 mg/kg (up to a maximum of 50 mg per dose) once weekly for up to 24 weeks. Treatment should be discontinued in patients who show no response after 12 weeks. If re-treatment with Enbrel is indicated, the above guid-ance on treatment duration should be followed.
The Enbrel 10 mg paediatric and “Standard” 25 mg packs contain graduated syringes to facilitate accurate dosing. It is recommended that the 10 mg paediatric vial be used for doses less than 10 mg and the 25 mg vial should be used for doses less than 25 mg. Both vials are intended for “single-use” as they do not contain a preservative and unused product should be disposed of immediately.
Should you have any medical queries about Enbrel please con-tact the Pfizer Medical Information Department Freephone 1800 633 363. An up to date approved Enbrel Summary of Product Characteristics is available on www.medicines.ie.
Irbesartan Clonmel
Clonmel Healthcare has announced the launch of Irbesartan Clonmel (Irbesartan) 75mg, 150mg and 300mg Film-coated tablets.
Irbesartan Clonmel Film-coated tablets (Irbesartan) 75mg, 150mg and 300mg are indicated for: • Treatment of essential hypertension• Treatment of renal disease in patients with hypertension
and type 2 diabetes mellitus as part of an antihypertensive medicinal product regimenIrbesartan Clonmel Film-coated tablets are available in a 28 pack. Full prescribing information for Irbesartan Clonmel is
available on request or go to www.clonmel-health.ie . This Product is subject to medical prescription. Irbesartan Clonmel is GMS reimbursable from 1st September 2012.
Please contact Clonmel Healthcare on 01-6204000 if you require any additional information on Irbesartan Clonmel.
Procoralan now recognised in new ESC guidelines for the treatment of heart failureLess than 2 years after the publication in The Lancet of the SHIFT study results demonstrating its benefits in heart failure, Procora-lan is now integrated in the new ESC guidelines for the manage-ment of heart failure.
The guidelines presented at the recent ESC Heart Failure Congress in Belgrade, Serbia, have been updated for the first time since 2008. They make recommendations for treatment based upon evidence for established and new diagnostic tests, and therapies for heart failure.
“The revised ESC Heart Failure guidelines aim to help phy-sicians in everyday clinical medical decision-making and if implemented offer a real opportunity to improve the outcome of patients with this condition,” commented John McMurray, Professor of Medical Cardiology at the University of Glasgow and principal author of the new ESC guidelines. Heart failure patients with elevated heart rates are at a significantly greater risk of death or hospitalisation, which both impacts patients’ quality of life and ultimate outcome and puts pressure on healthcare systems.
In addition, a new indication for ivabradine in chronic heart fail-ure was granted by the European Medicines Agency in February 2012. This was based on new data from the SHIFT study in which patients with an elevated heart rate of greater than or equal to 75 beats per minute (bpm) showed a significant reduction in the primary composite endpoint (CV death and hospitalisation for worsening heart failure) of 24% (p<0.0001), reduction in risk of cardiovascular death by 17% (p=0.0166), all-cause death by 17% (p=0.0109) and heart failure hospitalisation by 30% (p<0.0001).
The new indication and the new ESC guidelines for the treat-ment of heart failure are the two major advances which will allow heart failure patients to benefit from ivabradine.
Dr Vincent Maher, Consultant Cardiologist, Heart Efficiency Unit, AMNCH, who was present in Belgrade commented “Guide-lines are integral to ensuring a standardized and high level of care for all patients with heart failure. The inclusion of ivabradine in the guidelines is a step further in the management of heart failure patients with elevated heart rate. Ivabradine can provide additional benefits for these patients in sinus rhythm with high heart rates, by improving not only their symptoms and quality of life, but helping also to avoid hospitalisation or death.”

33
crossword
Name:
Address:
Email:
Congratulations to the winner of last month’s crossword, Kathleen Renehan, Health Centre, Johnstown, Co Kilkenny
Please send your answers to the Editor, Nursing in General Practice, GreenCross Publishing, 7 Adelaide Court, Adelaide Road, Dublin 2. Closing date for entries: 1 November 2012.Winner will receive v50. Please note: the winners’ cheques will be sent out within 45 days.
Caltrate is a trademark. PA 172/38/1. Full prescribing information available from Pfizer Consumer Healthcare Ltd., 9 Riverwalk, National Digital Park, Citywest Business Campus, Dublin 24 or from www.medicines.ie
1 2 3 4 5 6
7
8 9
10 11 12 13
14
15 16 17 18
19
2120
ANSwerS TO lAST mONTh’S CrOSSwOrdAcross: 1 Digests, 4 Group, 7 Femoral, 8 Rodeo, 9 Orderly, 10 Simian, 12 Adieux, 15 Turnkey, 17 Video, 19 Palmist, 20 Crick, 21 Captain. down: 1 Defer, 2 Sarcoma, 3 Seldom, 4 Cupid, 5 Observe, 6 Pharynx, 10 Satanic, 11 Martini, 13 Develop, 14 Myopic, 16 Knock, 18 Often.
ACrOSS1 The breastbone of Munster (7)4 The I.C. for a moral code (5)7 This could be bloody pernicious (7)8 M.P. sum adds up to parotid gland problem
(5)9 Notice verbose altercation (7)10 Discordant opuses for marriage partner (6)12 Sickness caused by a U.N. sea (6)15 Ken and lady cavorting in the nude! (7)17 Evade an American car! (5)19 Print a hub slip, perhaps (7)20 View is part of the act, in play! (5)21 John Steed, Purdy or Emma Peel (7)
dOwN1 Assorted maps about the south leading to
Cramp? (5)2 Mixed semen is ones downfall! (7)3 A dog went to mow one, in song (6)4 Peers using modified laser (5)5 The funny-bone? (7)6 Hole in smashed car causes acute infection
of small intestine (7)10 Sewing vocalists? (7)11 Teak roe hybrid produced from an acorn
(3,4)13 Blue aid can be heard (7)14 It is short-sighted of one to have this
condition! (6)16 Ball (5)18 Oddly, three was a number used by
anaesthetists! (5)

Convenient to take
20% more calcium than the market leader2
Calcium (as carbonate) / CholecalciferolCalcium (as carbonate) / Cholecalciferol( )
For Long Lasting Bones
ABBREVIATED PRESCRIBING INFORMATION(Please refer to Summary of Product Characteristics before prescribing)
CALTRATE* 600 mg/400 IU, fi lm-coated tabletPresentation: Each tablet contains 600 mg of calcium (as calcium carbonate) & 10 micrograms of cholecalciferol (equal to 400 IU vitamin D3). Contains sucrose & partially hydrogenated soya bean oil. Indications: Correction of combined vitamin D & calcium defi ciencies in the elderly. As an adjunct to specifi c treatments for osteoporosis, in patients where combined vitamin D & calcium defi ciencies have been diagnosed or those at high risk of defi ciency. Dosage & Administration: Adults & Elderly: One tablet twice a day (morning/evening). Pregnant women One tablet a day. Oral (Swallow with 200mls water). The elderly or patients with known diffi culties in swallowing, may break the tablet into two parts before taking with water. Do not suck or chew. Contraindications: Hypersensitivity to any ingredients including peanut or soya. Patients who now have, or have had renal failure, kidney stones, hypervitaminosis D, hypercalciuria & hypercalcaemia & diseases &/or conditions that lead to hypercalcaemia &/or hypercalciuria. Precautions: In prolonged treatment, check calcaemia & renal function, particularly in the elderly (see interactions). If renal function deteriorates, the dose must be reduced or treatment interrupted. Caution is advised in immobile patients. This product contains vitamin D; further administration of vitamin D or calcium must be medically supervised with regular monitoring of calcaemia & calciuria. Patients with sarcoidosis calcaemia & calciuria must be monitored. Risk of soft tissue calcifi cation must be considered. In severe renal insuffi ciency, vitamin D3 as cholecalciferol is not metabolised normally & other forms of vitamin D3 must be used. Cases of asphyxiation due to tablet choking have been reported. This product contains sucrose; patients with sugar intolerance should not take this medicine. Not intended for use in children & adolescents. Interactions: Thiazide diuretics & systemic corticosteroids (calcium monitoring required). Orlistat, combined ion-exchange resins (cholestyramine) or laxatives (paraffi n oil) can reduce the GI absorption of vitamin D3. Take tetracycline 2 hours before or 4 to 6 hours after taking calcium. Cardiac glycosides (monitor patients regularly with ECG check & calcaemia). Phenytoin or barbiturates (may reduce the activity of vitamin D3). Iron, zinc or strontium preparations, estramustin or thyroid hormones should be spaced at least 2 hours from calcium medicines. Bisphosphonate, sodium fl uoride or fl uoroquinolone administration, Caltrate should be spaced by at least 3 hours from these medicines. Oxalic acid (found in spinach & rhubarb) & phytic acid (found in wholegrain cereals) can inhibit calcium absorption by forming insoluble compounds with calcium ions. Patients must not take calcium containing-products in the two hours after consumption of foods rich in oxalic acid & phytic acid. Pregnancy & lactation: Caltrate may be used during pregnancy & breastfeeding. Daily intake in pregnancy should not exceed 1500mg calcium & 600IU cholecalciferol. Avoid prolonged use as hypercalcaemia can aff ect the developing foetus. Calcium & vitamin D3 pass into breast milk, this should be considered when vitamin D3 is given concomitantly to infants. Side-eff ects: Hypercalcaemia, hypercalciuria, constipation, fl atulence, nausea, abdominal pain, diarrhoea, pruritis, rash & urticaria. Legal Category: P. Pack Size: 90 tablets. PAH: Pfi zer Consumer Healthcare Ltd., Sandwich, Kent, CT13 9NJ, United Kingdom. PA number: PA172/38/1. Further information is available upon request from Pfi zer Consumer Healthcare Ltd., Citywest, Dublin 24. or look up, www.medicines.ieDate of preparation: June 2010.
Reference: 1 Based on sales (data on fi le). 2 MIMS Ireland Jan 2011, Pg 299.Artwork version Mar 11 Ref: 11 101 Med. * Trade Mark.
calcium & vitamin D3















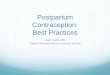






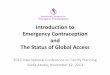

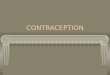




![[Insert Lecture Name Here] Long Acting Reversible ... Hathaway 042712.pdf · [Insert Lecture Name Here] Long Acting Reversible Contraception Methods (LARC): Improving Family Planning](https://img.pdfslide.us/doc/110x75/5d1efdd188c9933c558cba67/insert-lecture-name-here-long-acting-reversible-hathaway-042712pdf-insert.jpg)