Embed Size (px)
Citation preview

•1
February 18, 2009 Contra Costa EMS
Contra Costa STEMI System Oversight Meeting
Welcome to the first oversight meeting of Contra Costa STEMI System launched on September 8, 2009.

•2
February 18, 2009 Contra Costa EMS
STEMI Meeting Agenda
– Introductions & Welcome– STEMI System Performance
• Prehospital and System Overview • STEMI Center presentations
– STEMI System Improvement Opportunities• East County destination decision-making• Status report: False Positives• 12 lead ECG Transmission & Reliability• Quality improvement process feedback and recognition
– Patient and Public education– Oversight meeting process
• Joint Contra Costa-Alameda Oversight Meetings •
Our agenda today will include

•3
February 18, 2009 Contra Costa EMS
Contra Costa STEMI System
– Where do we stand?• 1 of 11 STEMI Systems in California• 1 of 148 STEMI Systems in the US• Mission Lifeline Member
– What is the Ideal? (Mission Lifeline)• STEMI POE protocols• 12 lead transmission• EMS-Cath team activation• STEMI Referral Hospitals• Coordinated training & feedback• National guideline compliance
“In the ideal system for EMS and EDs, standardized point of entry protocols (created by state-based coalitions of EMS personnel, emergency physicians, and cardiologists and supported by payers and administrators) would establish which patients are transported to the nearest hospital and which patients are transported to the nearest STEMI-Receiving hospital. This will be based in part on the acquisition, interpretation, and transmission of a pre-hospital 12-lead electrocardiogram (ECG).The catheterization laboratory team would be activated by EMS personnel in the field or by emergency physicians after receiving the transmitted ECG. Patients transported to a STEMI Referral hospital by EMS would remain on the stretcher with EMS personnel in attendance until the decision about whether to transport to a STEMI-Receiving hospital is rendered.For patients who transport themselves to a STEMI Referral hospital and require primary PCI, activation of EMS via a 9-1-1 system would occur. An ideal system would also foster a coordinated curriculum to teach EMS providers and ED staff to care for STEMI patients and provide feedback on performance and compliance with guidelines.” Mission Lifeline 2009

•4
February 18, 2009 Contra Costa EMS
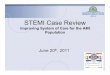
12-Lead ECG's Done - 2008
475 466
535506
570 573 580611 601
675
618 624
0
100
200
300
400
500
600
700
800
JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC
AMR Data 2008
This is data from AMR, which represents around 92% of all transports in Contra Costa, and also reflects 12-leads done by first-responder paramedic agencies working in tandem with AMR. This chart represents the number of patients who had a 12-lead ECG performed in the field for any reason by month in 2008. As you can see, the total number has increased steadily over the last year, and with the extra number of cases that Moraga-Orinda Fire and San Ramon Valley Fire does, means that we are doing around 25 12-lead ECG’s per day at this point. This represents roughly one out of every seven patients we transport.

•5
February 18, 2009 Contra Costa EMS
Reasons for Obtaining 12-Lead - 2008
Atypical Pain6%
Respiratory Symptoms
10%
Neurologic Symptoms (ALOC, stroke)
6%Other
6%
Non-specific Symptoms
(weak/dizzy)13%
Chest Pain43%
Other Cardiac Symptoms (e.g.,
syncope, rhythm)16%
AMR Data 2008
From the AMR data, we also see the reasons that the 12-lead ECG’s were done. A small number are done in the setting of arrhythmia (only perhaps 1-2 percent) whereas the rest are done in search of STEMI. Chest pain is the most prominent reason, but there are many non-specific presentations or patients with anginal equivalents who receive 12-leads. We know we have some cases that may represent a “fishing expedition” but most non-chest pain cases are done because of other presenting symptoms. Because the positive predictive value of a 12-lead in settings of presentations other than chest pain is less, we may see more potential false positives in this group (something that will needs study in larger numbers across the nation). At this point we have not tried to limit the application because we continue to try to identify as many true STEMI patients as possible.

•6
February 18, 2009 Contra Costa EMS
Percentage of Patients with 12-lead Performed -Patients with Chest Pain - Suspected Cardiac Origin
69% 66%
75%78% 78%
82% 82%89% 87% 88% 85%
92%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DECMonth - 2008
AMR Data 2008
Again, with AMR data, we see increasing use of 12-lead in the patients we most need to address – those with suspected cardiac ischemia. When we implemented 12-lead in late 2006 and throughout 2007, our numbers were in the 60-65% range, but now we see that the number has climbed considerably. We do not know exactly why this number is not 100% or close to it, but the trends are quite good. We implemented the STEMI system in September and we can see that in preparation for the startup, the numbers climbed considerably, and continue to climb.

•7
February 18, 2009 Contra Costa EMS
Percent of Chest Pain / ACS Transports to STEMI and Other Receiving Centers
Pre- and Post-System Implementation
59.0%
43.8% 41.0%
56.2%
0%
10%
20%
30%
40%
50%
60%
70%
Pre-System (1/08 to 8/08) Post-System (10/1/08 to 2/16/09)
STEMI Centers Other Receiving Centers
AMR Data 2008-2009
One concern that systems may have is whether 12-lead ECG in the setting of the STEMI system has a “halo effect” - whether patients other than those with STEMI are being diverted from other facilities to STEMI centers even without qualifying ECG’s. Using AMR data, we measured the transports to STEMI Centers versus other receiving centers in the 8 months prior to system startup to the numbers in the 4½ months following startup (excluding the month of September when the system was implemented). The impact has been small, and in total numbers represents around 25 total patients in 4½ months who potentially may have been diverted from other hospitals. At this point (and we will continue measuring this), we do not feel that there is an issue with “halo effect,” at least for the patients with the paramedic impression of chest pain suspicious for ACS.

•8
February 18, 2009 Contra Costa EMS
Percent of Transports - Chest Pain /ACSto STEMI Centers and Other Receiving Centers
30%
35%
40%
45%
50%
55%
60%
65%
JAN 08 FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC JAN 09 FEB
STEMI Centers Other Receiving Centers
STEMI System Start - 9/8/2008
AMR Data 2008
This is a month-by-month representation of transports to STEMI Centers and to other Receiving hospitals. The numbers are small (averaging 202 patient transports with chest pain per month over the months studied), but there may have been a slight increase just after system startup, but it the last few months appear to show no increasing issue with diversion of overall numbers of chest pain patients to STEMI centers.

•9
February 18, 2009 Contra Costa EMS
Chest Pain / ACS Patient Origin
Central County42%
86 patients/month
East County32%
65 patients/month
West County26%
53 patients/month
AMR Data 2008
This slide shows the proportion of patients from each area of the county presenting with chest pain. Because this does not include data from our transporting fire agencies, the Central County number is understated by perhaps 7-8%. East County is defined as Pittsburg eastward, and West County is Crockett and westward to Richmond and El Cerrito.

•10
February 18, 2009 Contra Costa EMS
STEMI Alerts - Patient OriginSince System Inception
Central County58%East County
21%
West County21%
EMS STEMI Database N=63 STEMI Alerts Date Range 9/8/08 to 1/31/09
Source: EMS STEMI Database N=63 STEMI Alerts Date Range 9/8/08 to 1/31/09This shows the proportion of patients in our STEMI database (all STEMI alerts) for the date range, showing proportion from each part of the county.

•11
February 18, 2009 Contra Costa EMS
STEMI Alert DestinationsSince System Inception
San Ramon5%
Kaiser - WC10%
John Muir - WC17%
Doctor's - San Pablo22%
John Muir - Concord
46%
EMS STEMI Database N=63 STEMI Alerts Date Range 9/8/08 to 1/31/09
Source: EMS STEMI Database N=63 STEMI Alerts Date Range 9/8/08 to 1/31/09This slide shows the destinations of patients with STEMI alert. John Muir Concord has received East County STEMI traffic to this point.

•12
February 18, 2009 Contra Costa EMS
Gender - STEMI Alerts and PCI
46
30
17
50
5
10
15
20
25
30
35
40
45
50
STEMI Alert To PCI
Male Female
EMS STEMI Database N=63 STEMI Alerts Date Range 9/8/08 to 1/31/09
Source: EMS STEMI Database N=63 STEMI Alerts Date Range 9/8/08 to 1/31/09Of interest, we see male:female ratio of STEMI alerts of approximately 3:1, but for those patients who truly make it to the cath lab and get PCI, the ratio is 6:1. We do not fully understand this phenomenon, and the numbers are small so it may be a statistical anomaly. Hospitals report that the ratio is around 3:1 overall (counting all STEMI patients to PCI regardless of mode of transport). So it may mean that there is a higher likelihood that females present via private auto than males. Again, with small numbers, it is hard to make firm conclusions, but it is somewhat suspicious. The other notable issue is that the ratio of STEMI alerts to completed PCI in females is much higher, meaning a higher percentage are false positives. Again, there are small numbers but it begs the question as to whether ECG’s done for atypical presentations may be more prominent in females than males, and the incidence of false positives may be higher because of the lower predictive value of the ECG in these atypical settings. We will further examine this when we have more data and look at our current data to see if we can break out and analyze atypical presentation STEMI alerts from those with more classic presentations.

•13
February 18, 2009 Contra Costa EMS
STEMI Alerts
35
ED ECG Verifies STEMI
23 (63%)
ED ECG Does Not Verify
STEMI
12 (37%)
To Cath Lab
22 (96%)
Not to Cath Lab
1 (4%)
PCI Done
18 (82%)
No PCI Done
4 (18%)
Thrombolysis
1 (100%)
Machine Overread
7 (58%)
Artifact
4 (33%)
Unknown
1 (8%)
STEMI Alerts
3 – Tachycardia with ST Elevation 1 – Bradycardia with ST Elevation 2 – Incomplete blocks with ST Elevation 1 - ? J-Point Elevation (MD Office ECG)
17 Immediate PCI cases (One delayed due to busy cath lab ): Average / Median – EMS Contact to PCI = 87 minutes / 89 minutes Percent <90 minutes = 53% Percent <120 minutes = 100%
Average / Median – Door to PCI = 58 minutes / 53 minutes Percent <90 minutes = 94% Percent <120 minutes = 100%
Contra Costa EMSSTEMI System Outcomes
4th Quarter 2008
Date Range 10/1/08 to 12/131/09
Source: EMS STEMI Database N=35 STEMI Alerts Date Range 10/1/08 to 12/131/09This chart reflects the outcomes of STEMI alerts in the last quarter of 2008. The STEMI alert is defined as a patient transported by EMS, the hospital acknowledges the case as a STEMI alert. There are a few patients in whom the EMS crew documented alert but the hospital did not acknowledge the report as an alert - it is hard to decipher what happened to communication in these cases – but they are excluded from this analysis. There is no accepted standard definition for what a “false positive” alert is nationwide, but we saw that we had 12 cases in which a 12-lead in the field stated STEMI, yet the ECG in the ED did not verify this. Of those not verified, none went to cath lab. Seven of them were “machine overreads” and the reasons are listed below. Four were cases with significant baseline artifact that truly were user error and should not have resulted in activation. Those have diminshed in number subsequent to this time – the last incident occurred in late November and none in 2009 has been noted, so we believe through feedback and education that we have diminished the incidence of this. The machine overreads are problematic, and many other systems have reported numbers in the 20% range (which is what we have – 7 of 35 cases). We believe that ECG transmission in the long run will be a help in avoiding inappropriate cath lab activations. However, the bottom line on the patients who ended up going to PCI is that the median Door-to-PCI time was 53 minutes. We believe these excellent result are in part attributable to the willingness of our hospitals to activate their cath lab on our alert rather than on arrival.

•14
February 18, 2009 Contra Costa EMS
No STEMI Alert -STEMI Noted in ED
8
To Cath Lab
8
PCI Done
7No PCI Done
1
1 – Initial ECG negative but STEMI suspected on ED ECG
3 – STEMI Activation not done or unclear communication ED to EMS 2 – 12-lead ECG not done in field 1 - Field ECG artifact precluded interpretation 1 – Cardiac Arrest – No field ECG 1 - Field ECG (-), subsequent positive ECG in ED
Patients to Cath LabWith No STEMI Alert
Average / Median EMS Contact to PCI = 122 minutes / 133 minutes Average / Median Door to PCI = 97 minutes / 109 minutes
Excluding one case with major delay (reason unknown): Average / Median EMS Contact to PCI = 104 minutes / 114 minutes Average / Median Door to PCI = 82 minutes / 92 minutes
Contra Costa EMSSTEMI System Outcomes
4th Quarter 2008
Date Range 10/1/08 to 12/131/09
Source: EMS STEMI Database Date Range 10/1/08 to 12/131/09Patients to Cath Lab with no STEMI Alert. This chart represents a group of patients transported by EMS who ended up going to cath lab, yet were not STEMI alerts. While we do not know if this represents all incidences, we know that there are some “lost opportunities” that we may be able to improve upon. Three cases were not activated because of communication errors. Two did not have ECG’s in the field despite presenting complaints that merited evaluation. In one case a quality ECG was not obtainable because of patient diaphoresis yet the STEMI was noted at the hospital. One was a case in which a field ECG was negative but the first one in the ED was positive, and a repeat ECG had not been done in the field. So we have room to improve in terms of communication, in terms of getting 12-leads done, and in terms of repeating ECG’s. These cases may not represent all of the lost opportunities to field activate, but show that some clearly exist. Also, in these cases with median door-to-PCI was much higher, which suggests that there is great value in the early alerts EMS can provide. Again these are small numbers but we believe there is work to do in this area to improve the system.

•15
February 18, 2009 Contra Costa EMS
STEMI Center Reports
– John Muir Concord– John Muir Walnut Creek– Kaiser Walnut Creek– San Ramon Regional– Doctors San Pablo
The following Centers will present their STEMI performance data.

•16
Contra Costa STEMI System
Opportunities for Improvement
Contra Costa STEMI system is new but we have great infrastructure in place to support excellence.

•17
February 18, 2009 Contra Costa EMS
East County STEMI Destination
– Sutter Delta STEMI Center Participation• Letter of interest 2/12/09• 24/7 coverage instituted• Application process to begin
– Current EMS Destination Guidelines• Patient Choice• < 30 minutes• Stable or unstable
East County STEMI destination challenges….new opportunities forth coming.

•18
February 18, 2009 Contra Costa EMS
Public Education50% of STEMI Patients Walk In
– “Act in Time” • Evidence-based NIH
patient education program
– STEMI Center PR representatives
– KCBS interview– Press releases– Front page Times– EMS1.com News– Community Outreach
Public Education is key to a successful STEMI system….goal is to increase the proportion of STEMI pts using 911 vs walking or driving in. This has big payoffs for the patient and the community we serve but resources are not always focused on this issue. We are again requesting that all stakeholder use a consistent message with the public by using the “Act in Time” patient educational materials. These materials are free for download on our website at www.cccems.org

•19
February 18, 2009 Contra Costa EMS
STEMI System Oversight Process
– Data Management– Performance Monitoring– Process Improvement
• Outcome reports• CQI process• Recognition
– Meetings• Frequency• Joint STEMI ALCO-COCO
Meetings
We have an accountable mechanism of CQI with tremendous cooperation between stakeholders. This is unique and will go far to improve performance, support excellence in patient care and nurture the new standard of cardiac care we have created in our community.

•20
February 18, 2009 Contra Costa EMS
Moving Forward….STEMI System Priorities
– 12-lead Transmission– Field to Cath Lab?– Public Education– Decreasing Scene Time– Teamwork– System confidence– Maintaining excellence!
Our system priorities are based on our performance monitoring.

•21
February 18, 2009 Contra Costa EMS
Support Needed
– Prehospital Education– Timely Constructive
Feedback– STEMI Newsletter– ECG Transmission
pilots– Recognition– Public Education
It is always exciting to start of new project and Contra Costa has had a great start but the system will only be as good as we make it.

•22
February 18, 2009 Contra Costa EMS
Oversight Meeting Process
– Quarterly Data Review– Oversight Frequency
• Face to Face• Conference Calls• Webnair
– Physician Leadership– Best Practice Networking
• Listserves• Email • Newsletters
•Goal is to make meetings effective and efficient.•How do we support these type of meetings and how often? •Are there better methods to facilitate oversight and decision making that are more efficient?•Your recommendations are welcome.

•23
February 18, 2009 Contra Costa EMS
Acknowledgements
– Prehospital Care Providers – Fire EMS CQI Coordinators– STEMI Center Coordinators– Cath Lab Teams– ED physicians and nurses– Cardiologists– AHA Mission Lifeline
Thanks to the many providers and stakeholder agencies for supporting this collaborative effort.