EMERGENCY DEPARTMENT CASE PRESENTATION 19TH OF MARCH 2014
EMERGENCY DEPARTMENTCASE PRESENTATION19TH OF MARCH 2014INTAN
EKARULITAMELISA AYUName: Mr. D U
Address : Jalan Adan RT 6/11, Rawa Belong, Jakarta Barat
Date of Birth: 04th of July 1968
Age: 46 years oldIDENTITYChief Complaint:Chest pain since 6
hours before he came to hospital
Additional Complaints :Shortness of breathDizziness
History TakingPatient came with chest pain since 6 hours before
he came to the hospital.The pain felt all over his chest area.It
happened suddenly after he got cough.The pain felt like his chest
pressed which worsens while he was walking.It felt continuously and
did not radiate to any other parts of his body. Disease
ProgressionShortness of breathIt felt at the same time with his
chest pain.It was getting better when he was lying down and getting
worse when he was walking. DizzinessIt was the first time he felt
this symptomsHe used one pillow while lying down.Palpitation (-),
abdominal discomfort (-)Disease ProgressionThe patient is a smoker
since 25 years ago.10 cigarettes per dayDisease ProgressionTaking
drugs (-)Heart disease (-)Diabetes Mellitus (-)High Cholesterol
(-)Hypertension (+)Since 2 years agoDid not take any medicine
Diseases HistoryGeneral State : Appeared severely illAwareness:
Compos MentisVital Signs:BP: 130/80 mmHgHR: 83 x/minuteRR: 20
x/minuteTemp: 36,7CPhysical ExaminationHead: normocephal
Eyes: anemic conjunctiva -/-, icteric sclera -/-, palpebral
edema -/-, pupil isokor, light reflexes +/+
ENT: nostril breath (-), secrete (-), hyperemic pharynx (-),
tonsils T2-T2
Neck: impalpable lymph node, JVP 5+2cmH20 Thorax: normochest,
discoloration (-) Lungs:hemithorax moved symmetrically, retraction
(-)vocal fremitus : symmetricSonor in all area of the
thoraxVesicular breath sound, wheezing (-/-), rhonki(-/-)
Heart:Ictus cordis : invisible, palpable at ICS V midclavicular
line sinistraHearts borderlineRight : ICS V parasternal dextraApex
: ICS V midclavicular sinistraSuperior: ICS II parasternal
sinistraS I&II regular, murmur (-), gallop (-)
AbdomenSupel, spider naevi (-), scar (-), caput medusa
(-)Distention (-), skin turgor : normal, pain on palpation (-),
massa (-), hepar and spleen : normalTymphanic sound on all area of
abdomenPeristaltic (+), normalExtremitiesWarm on all four
extremitiesNo edema on all extremitiesNo clubbing
fingersECGRoentgen ThoraxLaboratory Test : CKMB, troponin I dan T,
HDL, LDL, TG, Cholesterol Total, and Random Blood
Glucose.Diagnostic ToolsLAB RESULTSHb 14.5Ht 44%Eri 5.9Leukocytes
13400Thrombocytes 373000CPK 1012CKMB 166Ureum 45Kreatinin 1.7GDS
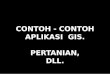
147Na/K/Cl 138/4.4/102ECG
ST Elevation in lead IST Depression in lead III
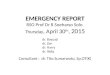
ECGST Elevation in Lead I, aVL, V6ST Elevation Myocard
InfarctWorking DiagnosisO2 in nasal cannuleCPG 4 x 75 mgAspirin 1 x
160 mgSimvastatin 1 x 20 mgISDN 1 x 5 mg sublingualStreptokinase
1.5 millions Unit in 1000 NaCl drips in 60 minutes
TREATMENTTHANK YOUAnamesis sudah menunjukan gejala typical
anginaFoto rontgen seharusnya tetap dilakukan untuk mengetahui
adanya hipertrophy jantung untuk menentukan KIPI score sebagai
prognosisMenentukan TIMI score Pengobatan terbaik seharusnya PCI
namun tidak dilakukan di IGDCOMMENTS