Embed Size (px)
Citation preview

FA M I LY H EA LTH O UTCO M ES PR O JECT
Continuous Quality Improvement Efforts for MCAH Populations
This project was supported by funds received from the State of California, Department of Public Health, Maternal, Child and Adolescent Health Division

Learning Objectives
Participants will be able to:
• Understand the definition(s) of quality assurance (QA), quality improvement (QI), continuous quality improvement (CQI) and Program Fidelity Assurance and particular utility of each
• Articulate how QA, QI and CQI relate to and emerge from the CA MCAH planning and evaluation processes.
• Articulate how these differ from program evaluation • Describe 3 models for implementing CQI:
1. Health Resources & Services Administration/Institute of Medicine (HRSA/IOM)
2. Public Health (PH) Accreditation Board
3. HRSA Office of Adolescent Health

Learning Objectives Cont.
Articulate the benefits and challenges to implementing a CQI program
Describe some program models utilizing CQI Model for QI for statewide Home visiting program YMCA of Greater Seattle Youth program CQI model Evaluating mental health programs for trauma informed care in
Chicago, IL Prenatal Care Model for CQI for Access to Care: Case Study
Articulate lessons learned

Definitions of Quality Assurance
Assuring ↑ quality of community health programs/health services = constantly measuring the effectiveness of health service providers and the programs and organizations that provide services
Institutionalized activities and programs intended to assure or improve the quality of services/programs in either a defined medical setting or a program
Often measure compliance with state, national or professional standards/policies/ licensing etc.

Examples of Quality Assurance Activities
Annual monitoring of kindergarten immunization rates
Annual child abuse and domestic violence training with pre-post
test
Chart review for compliance with recommended preventive services, i.e. blood pressure, lab tests, pap smears
Utilization review of patient care – necessity, quality, appropriate, LOS

HRSA and IOM definitions
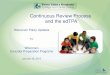
HRSA: Quality improvement consists of systematic and continuous actions that lead to measurable improvement in health care services and the health status of targeted patient groups.
IOM: Quality in healthcare = direct correlation between the level of improved health services and desired health outcomes of individuals & populations.
HRSA Basic Model

Definition of QI In Public Health
“Quality improvement in public health is the use of a deliberate
and defined improvement process, such as Plan-Do-Check-Act, which is focused on activities that are responsive to community needs and improving population health.”
“It refers to a continuous and ongoing effort to achieve
measurable improvements in the efficiency, effectiveness, performance, accountability, outcomes, and other indicators of quality in services or processes which achieve equity and improve the health of the community.”
This definition was developed by the Accreditation Coalition Workgroup (Les Beitsch, Ron Bialek, Abby Cofsky, Liza Corso, Jack Moran, William Riley,
and Pamela Russo) and approved by the Accreditation Coalition on June 2009.

Program Evaluation
Should be done when initiating a new service or program to determine effectiveness
Requires a program logic model that defines inputs, resources, activities as well as process and program outcomes as well as health/public health outcomes
Requires Adequate expertise Staff and financial resources Staff and partner buy –in Evaluation tools

Poll Question 1
Carol Hathaway, the Perinatal Services Coordinator (PSC) from Happy County is headed to Dr. Welby’s office to review a sample of charts from the doctor’s patients receiving CPSP services. PSC’s conducting chart reviews is: Quality Improvement Program Evaluation Quality Assurance All of the above None of the above

They Are Not the Same
Quality Assurance
Reactive Works on problems after
they occur Regulatory usually by State or
Federal Law Led by management Periodic look-back Responds to a mandate or
crisis or fixed schedule Meets a standard (Pass/Fail)
Quality Improvement
Proactive Works on processes Seeks to improve (culture
shift) Led by staff Continuous Proactively selects a process
to improve Exceeds expectations

They Are Not the Same
Program Evaluation Assess a program at a
moment in time Static Does not include
identification of the source of a problem or potential solutions
Does not measure improvements
Program-focused A step in the QI process
Quality Improvement Understand the process that
is in place Ongoing/dynamic Entails finding the root
cause of a problem and interventions targeted to address it
Focused on making measurable improvements
Customer-focused Includes evaluation

Continuous Quality Improvement
A formal ongoing cycle of activities that includes
Measuring inputs Monitoring processes Monitoring outcomes Reviewing results Creating a remediation plan Monitoring the implementation plan

Continuous Quality Improvement
Source: https://deming.org/management-system/pdsacycle

Definition of Program Fidelity
HRSA Office of Adolescent Health Definition: Degree to which a program is implemented with adherence to its core components — the key ingredients related to achieving the outcomes associated with the program model 2 categories of core components:
1. Program Content 2. Program Delivery
Ideally, program developers and evaluators determine a program’s core components
Core components can include program content only, or program delivery methods only, or both

Program Fidelity Process

Poll Question 2
You just finished conducting your first Blue Dot campaign with stakeholders from your local MCAH Advisory Board. You are interested in learning if the campaign impacted your stakeholders view of how important it is to address perinatal mood and anxiety disorders in pregnant and postpartum women. To get a better understanding of the impact on stakeholders, you should conduct a
Quality Improvement Project Quality Assurance Project Program Evaluation Project All of the above None of the above

Benefits
CQI processes provide: Real-time monitoring Critical information on fidelity of program to an evidence
based model Information on program’s acceptability to target population Information on whether alterations have been a success
Overall provides feedback to and engages staff in more
effective efforts to manage program and improve performance

Challenges
Requires significant targeting of resources and expertise
Requires resources to collect and analyze data throughout project cycle
Sometimes results in fewer resources available for program implementation
Rigid program model can limit ability of staff and community members to make alterations that better serve a particular community

Poll Question 3
Carla has been leading safe sleep workshops for local daycare providers in Happy County for the last two years. The workshops take place over a weekend, but Carla has recently noticed that attendance on day 2 of the workshop has dropped off. Now, upwards of 30% of attendees are not earning their workshop completion certificates. If Carla wants to increase attendance on day 2, what type of project should she initiate?
Program Evaluation Quality Improvement Quality Assurance All of the above None of the above

Statewide Home visiting CQI Program
Program goals are to improve parenting skills and connect families to needed services and improve health of service population Evaluation system is designed to: 1. Integrate evaluation into daily workflow 2. Utilize standardized screening & evaluation tools 3. Facilitate culture of CQI in program management 4. Facilitate scientifically rigorous evaluations


Question One
What are the key elements in this process?
Are there more that one functions within this comprehensive overview?

YMCA of Greater Seattle's CQI initiative
Youth Program Quality Intervention (YPQI) model helps improve youth program quality by providing research-based standards & a process for achieving those standards Randomized trial research has found intervention to be
effective at improving program quality Designed to be used with Youth Program Quality
Assessment (YPQA), a research-based instrument to assess quality of service at point where staff and youth interact
Five step process: prepare, assess, plan, improve, repeat

YPQI Step
YPQI Elements
The Y’s 2010 Plan What Actually happened
Prepare Identify Leadership
Identify two project leads.
Two mid-level executives shared the leadership role; each brought experience implementing the YPQI model at a pilot site. Leads completed trainings offered by the Weikart Center in preparation for the role.
Develop Project Plan, Budget, Timeline
Leads make decisions based on local considerations and resources about how the process will take place.
Program participants included teen and young adult programs, Y branches and camps. A spring and fall assessment schedule was set.
Project Communication
Two leads share communication work, with one managing school-based programs and the other managing branch-based programs (ongoing). Both leads introduce YPQI to staff and manage buy-in process.
Leads introduced staff to the process via email invitations to initial trainings (December 2009–January 2010). One lead held monthly meetings with school-based staff and bi-weekly meetings with site supervisors. One lead was on leave March–August 2010, decreasing communication with branch-based programs.

YPQI Step
YPQI Elements
The Y’s 2010 Plan What Actually happened
Assess Training to Conduct Self-Assessment
Thirty staff representing twenty- six programs to participate in initial training to use YPQA tool (January 2010).
Forty staff participated in optional training (January 2010).
Training for External Assessors
Ten management-level staff and staff with YPQA experience to be trained to be external assessors (January 2010).
Thirteen staff were trained to be external assessors (January 2010).
Baseline Self- Assessment and External Assessment
Twenty-four school-year programs to conduct at least one self-assessment and invite one external peer assessment by a colleague (February–April 2010). Two summer programs to conduct at least one self- assessment and invite one peer assessment (July–August 2010).
Twenty school-year programs conducted a total of twenty-nine self- assessments and twenty-four peer assessments (March–June 2010). No summer programs conducted baseline assessments.

YPQI Step YPQI Elements
The Y’s 2010 Plan What Actually happened
Plan
Action Planning
Invite all participating staff to Planning with Data workshop (April 2010). Twenty-four sites complete action plans (mid-May 2010 due date).
Approximately twenty-five staff attended Planning with Data workshop (April 2010). Fourteen action plans completed (July 2010).
Improve Youth Work Methods Trainings
Staff participates in Voice and Choice and Reframing Conflict workshops (November 2010).
Thirty-three staff participated in Voice and Choice or Reframing Conflict workshops (November 2010).
Coaching for Managers or Staff
Coaching is informal, delivered by initiative leads and staff supervisors (ongoing).
Informal coaching was delivered by initiative leads and staff supervisors, but not tracked (ongoing).

YPQI Step
YPQI Elements
The Y’s 2010 Plan What Actually happened
Repeat Post-Initiative Assessment
Twenty-four school year programs complete a second peer and self-assessment (November 2010).
Eighteen school year programs completed a second wave of assessments, with twelve self- and nine peer observations conducted and scored (November 2010).
Continuous Quality Improvement
Twenty-four sites complete or update action plans after the post-assessment, kicking off a continuous quality improvement cycle (December 2010).
Thirteen action plans completed (December 2010).

Question Two
What are the differences between this type of schematic and the previous one ?
What is missing? What is added? What would be most useful from your point of view

Making Change Last: Taking a Trauma-Informed System from Theory to Continuous Improvement
2011 System of Care Community Training of Federal Substance Abuse and Mental Health Services Administration, Chicago, IL CQI designed to: 1. Educate providers on trauma-informed principles and difference
between trauma-informed and trauma-specific service 2. Assess and measure whether services are trauma-informed 3. Identify technical assistance needs with stakeholders based on
assessment outcomes 4. Understand how youth and family define quality 5. Demonstrate how CQI can sustain a system of care provided by
DHHS, in partnership with family and youth

Involving Youth and Family
Phase Role of Youth and Family How? Youth and Family...
Planning Create framework and questions; provide feedback and suggestions.
...identified what is most important to them.
...made sure key components include youth and family priorities.
...drafted definitions and questions.
Pilot Testing Test and refine questions, methods and framework.
...helped an evaluator to conduct key informant interviews.
...brainstormed ways to reach family and youth.
...pilot tested final data collection instruments.
...suggested changes.
Implementation
Ensure data collection is family and youth friendly. Review responses and suggest best practices to ensure family/youth are reached. Interpret results.
...provided technical assistance to agencies.
...helped youth/families respond to the assessment.
...reviewed quarterly report on the number of responses.
...made suggestions based on report.
...reviewed final data results.

Statewide CQI Plan
Conduct TIAA Assessment
Prioritize Areas of Need
Create Continuous
Quality Improvement Plan for DHHS
Contract
Implement CQI Plan / Plan Do
Study Acts
Technical Assistance from Thrive Consultants/ Use of “Guide to Trauma-Informed Organizational
Development”
Additional Technical
Assistance as needed
Agency and DHHS Review
Results
Guidance from DHHS Regional Coordinator leads to initial contact
with Thrive
Prenatal Care Model for CQI for Access to Care: HRSA Case Study
Happy Farms Health Center: full-scope, primary care, & inpatient services to a large, sparsely-populated agricultural region. One main site & two small satellite sites located in different sectors of their service area. Staff: 2 family physicians, 1 physician’s assistant, 1 part-time certified nurse-midwife Problem: Center noticed ↑ number of patients were arriving
for prenatal care in their second or third trimester Initiated a process that included: developing an aims statement, creating
infrastructure for improvement, and gaining commitment from leadership Developed a model of a critical pathway for access to care

Critical Pathway for First Trimester Prenatal Care Access Potential Factors that Have an Impact on Access
1. Woman of
reproductive age presents for care
2. Preventative care
needs are assessed as part of intake-family
planning, pregnancy plans
3. Education
provided related to contraception, preconception,
preventative health services
available
4. Patient presents
for pregnancy test – with
positive results
5. Patient is
scheduled for initial prenatal
visit with provider
6. The pregnant
woman is seen in the first trimester
Patient Care Team Health System
Patient Care Team Health System
Patient Care Team Health System
Patient Care Team Health System
Patient Care Team Health System
Patient Care Team Health System
Source: https://www.hrsa.gov/quality/toolbox/methodology/index.html
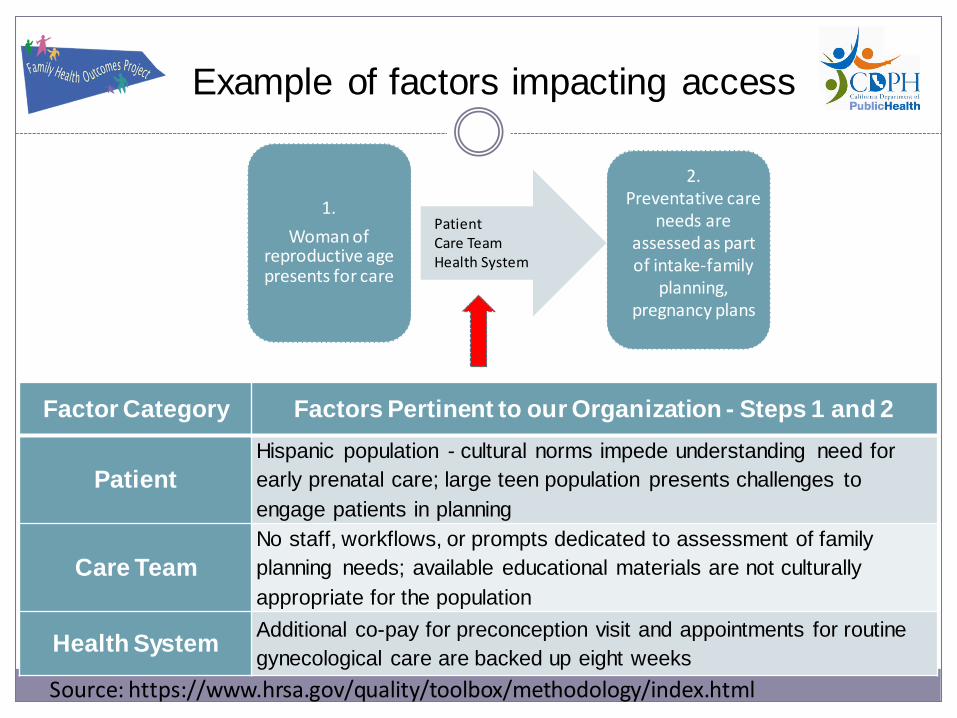
Example of factors impacting access
Factor Category Factors Pertinent to our Organization - Steps 1 and 2
Patient Hispanic population - cultural norms impede understanding need for early prenatal care; large teen population presents challenges to engage patients in planning
Care Team No staff, workflows, or prompts dedicated to assessment of family planning needs; available educational materials are not culturally appropriate for the population
Health System Additional co-pay for preconception visit and appointments for routine gynecological care are backed up eight weeks
1. Woman of
reproductive age presents for care
2. Preventative care
needs are assessed as part of intake-family
planning, pregnancy plans
Patient Care Team Health System
Source: https://www.hrsa.gov/quality/toolbox/methodology/index.html

Area of Critical Pathway Patient Changes Care Team Changes Health System Changes
A woman of reproductive age presents for care
Patient educational resources regarding importance of early prenatal care routinely given Create expectation that patient must take responsibility to assure early prenatal care
Care team members knowledgeable about importance of early prenatal care and can reinforce with messaging and materials during well-woman exams
Health system understands importance of early prenatal care
Preventive care needs are assessed as part of intake family planning, pregnancy plans
Educational materials are available regarding signs of pregnancy Education materials regarding the importance of good health before pregnancy
Care team knowledgeable regarding clinical guidelines for preventive care
Clinical guidelines for preventive care embedded in health system
Education provided related to contraception, pre-conception, and preventative health service
Education provided regarding contraception, preconception, and preventative care
Care team knowledgeable regarding clinical guidelines and understanding of latest contraceptive methods, including risk assessments for contraception, etc.
Education is provided related to contraception, preconception, and preventative health
Patient presents for pregnancy test with positive result
Patient educated on signs of pregnancy and the importance of early prenatal care
Care team members knowledgeable about importance of early prenatal care
Patient is scheduled for initial prenatal visit with provider
Patient understands importance of early prenatal care
Care team members knowledgeable about importance of early prenatal care
Health System understands the need for early prenatal care
The pregnant woman is seen during her first trimester
Changes That Work
Source: https://www.hrsa.gov/quality/toolbox/methodology/index.html

Question 3
What kind of approach does this plan take?
What are the advantages of this approach?

Lessons Learned
Organizations that achieved improvement shared 3 characteristics 1. Clear Direction
Developed an appropriate aim statement (essentially a SMART Objective) Additional resources: Readiness Assessment & Developing Project AIMS
2. Functional infrastructure for quality improvement
Need a systematic approach to measuring performance, testing small changes, and tracking the impact of those changes over time
Essential infrastructure components: a) Quality improvement teams b) Tools and resources c) Organizing improvements d) Building on the efforts of others by using changes that worked
3. Commitment from Leadership
Source: https://www.hrsa.gov/quality/toolbox/methodology/index.html

Functional Infrastructure for Quality Improvement
Multi-disciplinary Quality improvement team – members bring expertise knowledge about what they do, need willingness to improve and ability to think from a systems perspective
Tools and resources – Organize meetings efficiently Tips for Effective Meetings Manage data for performance improvement – e.g. a data dashboard
Managing data from performance improvement Planning an approach to change is essential, adopt a model (e.g., Link to
PDSA worksheet) to guide the actual change process and managing how changes are made
Build on the Efforts of Others by Using Changes that Worked - steal shamelessly
Source: https://www.hrsa.gov/quality/toolbox/methodology/index.html

How organization can make changes: Organizing for Improvement
1. Model for Improvement The Model for Improvement identifies aims,
measure, and change strategies w/ 3 questions: 1. What are we trying to accomplish? 2. How do we know that change is an improvement? 3. What changes can we make that will result in
improvement? Questions are followed by use of learning cycles
(e.g. Plan-Do-Study-Act cycles) to plan and test changes in systems and processes
Source: https://www.hrsa.gov/quality/toolbox/methodology/index.html

Model for Improvement
Source: http://www.ihi.org/resources/Pages/HowtoImprove/default.aspx

Tips for Testing Changes
Keep the changes small Involve care teams Study results after each change Involve others who do the work Make sure that overall aims are improving; changes in one
part of a complex system sometimes have an adverse effect in another
Source: https://www.hrsa.gov/quality/toolbox/methodology/index.html

How organization can make changes: Organizing for Improvement (cont.)
2. Process Mapping Provides a visual diagram of a sequence of events that result
in a particular outcome Purpose is to use diagramming to understand current process
(i.e., how a process currently works within the organization) and identify opportunities for improvement
Can be used before or in conjunction with PDSA cycle Mapping out the current process often uncovers unwanted
variation (different staff/practices, time day/week) Additional Resources for Process Mapping: Redesigning a
System of Care to Promote QI
Source: https://www.hrsa.gov/quality/toolbox/methodology/index.html

Holding gains and spreading improvements
Ongoing monitoring QI data ensures that an organization holds the gains over time
Can reduce the frequency of monitoring the process, BUT some ongoing assessment of the measure is necessary
Processes that work well now may need to change as environment shifts e.g. Population mix change
Successful QI effort that were started out small or impacted only a particular population can be spread organization-wide
Source: https://www.hrsa.gov/quality/toolbox/methodology/index.html

References
Gorenflo, G; Moran, J. The ABCs of PDCA. Public Health Foundation. 2010 Health Information Technology Research Center; The National Learning
Consortium. Continuous Quality Improvement (CQI) Strategies to Optimize your Practice. April 30, 2013.
Hunter, S; Kilburn, R; Mattox, T; Wiseman, S. Getting to Outcomes for Home Visiting: How to Plan, Implement, and Evaluate a Program in Your Community to Support Parents and their Young Children. RAND Corporation. 2013.
Murray, M. Lessons for Youth Program Quality Improvement Initiatives: A Summary of the YMCA of Greater Seattle’s Initiative. MEMconsultants. January 2012.
U. S. Department of Health and Human Services Health Resources and Services Administration. Developing and Implementing a QI Plan. https://www.hrsa.gov/quality/toolbox/methodology/developingandimplementingaqiplan/part4.html. 2011.