Embed Size (px)
Citation preview

8/14/2019 Continence Audit
http://slidepdf.com/reader/full/continence-audit 1/6
Age and Ageing The Author 2007. Published by Oxford University Press on behalf of the British Geriatrics Society.doi:10.1093/ageing/afm163 All rights reserved. For Permissions, please email: [email protected]
National audit of continence care for older
people: management of urinary incontinenceADRIAN WAGG
1, JONATHAN POTTER 2, PENNY PEEL
2, PENNY IRWIN2, DEREK LOWE
2, MICHAEL PEARSON2
1Geriatric Medicine, University College Hospital, 25 Grafton Way, London WC1E 6AU, UK 2Clinical Effectiveness and Evaluation Unit, Royal College of Physicians of London, London NW1 4LE, UK
Address correspondence to: Adrian Wagg. Tel: 0207 380 9910; Fax: 0207 380 9652. Email: [email protected]
Abstract
Introduction: the Department of Health report ‘Good practice in continence services’ highlights the need for proper
assessment and management of urinary incontinence. The National Service Framework for Older People required serviceproviders to establish integrated continence services by April 2004. A national audit was conducted to assess the quality of continence care for older people and whether these requirements have been met.Method: the audit studied incontinent individuals of 65 years and over. Each site returned data on organisational structureand the process of 20 patients’ care. Data were submitted via the internet, and all were anonymous.Results: thenationalauditwas conductedacross England,Walesand Northern Ireland. Data on thecare of patients/residents
with bladder problems were returned by 141/326 (43%) of primary care trusts (PCT), by 159/196 (81%) of secondary caretrusts (involving 198 hospitals) and by 29/309 (9%) of invited care homes. In all 58% of PCT, 48% of hospitals and 74% of care homes reported that integrated continence services existed in their area. Whilst basic provision of care appeared to bein place, the audit identified deficiencies in the organisation of services, and in the assessment and management of urinary incontinence in the elderly.Conclusion: the results of this audit indicate that the requirement for integrated continence services has not yet been met.
Assessment and care by professionals directly looking after the older person were often lacking. There is an urgent need tore-establish the fundamentals of continence care into the practice of medical and nursing staff and action needs to be taken
with regard to the establishment of truly integrated, quality services in this neglected area of practice.
Keywords: urinary incontinence, older people, audit, clinical effectiveness, elderly
Introduction
Urinary incontinence (UI) is associated with a range of medical conditions, many of which are common withincreasing age. UI affects some 20% of community dwelling older people and 30–60% of people in institutionalcare [1–4]. It remains an under-reported problem despitea significant impact on quality of life and associatedmorbidity [5, 6]. Many sufferers either do not present forcare, cope in silence or do not receive effective treatment fortheir condition [7, 8].
Caring for a person with UI has an equally negativeimpact on quality of life of the carer [9], and UI may often precipitate a move to institutional care [10]. The coststo both health and social care services of providing careare considerable [11] so, there is a great opportunity forimproving the lot of older people if UI can be betterassessed and managed. The Department of Health report
Good Practice in Continence Services (2000) recognised the
need for proper assessment and management, identified
a wide geographical variation in access to services and
called for regular audit [12]. The National Service Framework for
Older People (2001) required the establishment of integrated
continence services for older people by April 2004 but
allocated no resources to promote this objective [13]. Recent
evidence suggests that there has been only limited action
toward this end [14]
The Clinical Effectiveness and Evaluation Unit has
developed measures for defining the quality of continence
care and a comprehensive audit package to assess this across
primary, secondary and care homes [3, 15–17]. The aims of
this National audit were to describe the organisation and
processes of care for older people with continence problems
to describe variation in care and to produce data to enable
the comparison of care between organisations.
1
Age and Ageing Advance Access published November 21, 2007

8/14/2019 Continence Audit
http://slidepdf.com/reader/full/continence-audit 2/6
A. Wagg et al .
Method
Audit tool development
Full details of the audit tool development have beenpublished elsewhere [18]. Patients’ views on the quality of services added patient-defined standards [19]. The resulting package was piloted and modified [20].
Patient inclusion and data retrieval
Data were returned on 20 patients aged 65 andabovewith UIas defined by the clinical record in each participating site. Inacute care hospitals, consecutive patients were identifiedfrom current inpatients. In primary care hospitals they came from the records of a single GP practice; data wereobtained from any practice records and computer systems.In care homes, residents were identified and data obtainedfrom the care home records.
Recruitment of sites
Theaudit included England,Wales, NorthernIreland and theChannel Islands. Primary care trusts (PCTs)/Local HealthBoards were identified and each was asked to identify one of their GP practices for the audit. Totally, 326 invitations weresent, of which 179 registered an interest to participate. Allacutecare National Health Service Trusts were identified andof 196 invited to participate 175 registered to do so. Majorcare home providers were invited with a target total of 100homes; 309 invitations were sent and 85 registered. Regional
workshops were held for training with the audit tool prior todata collection.
Data were submitted via the Internet to a secure website, and all were anonymous. Help buttons were provided
online alongside the questions and an extensive printed helpbooklet was also issued to participants. Each participating site was asked to use another auditor to independently audit their first five cases to conduct a reliability study (results not presented here).
Data were expressed in percentage and absolute termsand where data were not applicable the denominator wasadjusted accordingly. Missing data were regarded in thenegative. The input method guaranteed that missing datalevels (i.e. ‘blank’ entries) were very low (less than 1%).
Analyses were performed using SPSS v11.5.No ethical committee permission was sought for this
clinical effectiveness work which involved no intervention.Data transfer was in accordance with standards of practicelaid out by the Patient Information Advisory Group.
Results
In all, 138 primary care sites, 195 hospitals and 27 carehomes returned data, these included information on 2,717primary care, 3,683 hospital and 488 care home patients andresidents.
Organisation of care
Fifty eight percent of PCTs (79/137), 48% (94/195) of hospitals and 74% (20/27) of care homes (CHs) reportedthat integrated services existed in their area, but in only 67% (53) of PCTs, 53% (50) of hospitals and 50% (10)of CHs did that integrated service have a designated leadclinician. Seventy-five percent of PCTs, 90% of hospitalsand 100% of CHs had a policy of routinely asking patientsabout bladder problems, but fewer of them guaranteed anassessment should a problem be found. Of the hospitalbased services only 32% had a written policy for managing continence, 49% had a structured training programme and35% performed regular audit.
Specialist assessments were performed by staff trained tocarry out abdominal, vaginal and rectal examinations in only 54% of cases. The number of specialist continence advisorsis summarised in Table 1.
Where a written policy for continence care existed,services reported that products were supplied on the basis
of clinical need rather than cost in 88% (71/81) of PCTs,76% (48/63) of hospitals and 86% (19/22) of CHs. In 84%(108/128) of PCTs, 53% (86/163) of hospitals and 76%(19/25) of CH patients’ views were sought in selecting therange of products supplied. Despite this there was evidenceof rationing in both PCT (104/129) sites and CH (19/25)sites, this practice being less common in hospitals (39/166sites). The median number of products supplied per patient per day in each sector was four.
Patients surveyed
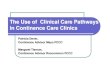
Patients/residents were older in hospitals (mean 82, SD8 years) and in CHs (mean 86, SD 8 years) than in PCTs(mean 80, SD 8 years). The majority of the sample for whichdata were available had significant levels of cognitive and
functional impairment (Figure 1). Seven percent (196) of PCT patients, 2% (61) of hospital patients and 2% (99)of CH residents had no reported associated co-morbidity.
The distribution of continence-associated co-morbidities isshown in Table 2.
Process of care
A continence history was documented in 73% (1984/2,717)of PCT patients, 70% (344/488) of CH and 45%
Table 1. Numbers of continence advisors available to sites
Number of WTE
con tinence specialist Primary Seco ndary Ca re
available care care homes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .From the PCT 121 sites 109 sites 13 sites
Median 1.8 1.6 1.0
Interquartile range 1.0 –2.7 1.0 –3.0 0.6 –6.0
From the hospital 80 sites 134 sites 8 sites
Median 0 0.6 1.0
Interquartile range 0– 1 0– 1.0 0– 2.8
2

8/14/2019 Continence Audit
http://slidepdf.com/reader/full/continence-audit 3/6
Audit of continence care for older people
0
10
20
30
40
50
60
70
80
Yes Mild Moderate Severe Yes Mild Moderate Severe
Cogniti ve impai rment Functional impai rment
%
Primary care
Secondary Care
Care Homes
Figure 1. Proportion of cognitive and functional impairment by care setting.
Table 2. Distribution of co-morbidity
Primary Secondary Care
care (2,717) care (3,682) homes (488)
(%, N ) (%, N ) (%, N ). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Bladder cancer/stones 1 34 2 60 2 11
Chronic cough 7 196 4 153 5 22
Dementia 14 375 31 1,125 41 199
Depression 11 296 11 394 17 81
Diabetes 16 431 15 564 9 45
Faecal loading or chronic constipation 4 118 8 307 13 62
Heart failure 14 365 16 597 20 99
Hypertension 30 814 29 1,074 17 82
Impaired mobility 26 710 48 1,767 66 324
Neurological disease 7 193 14 504 12 57
Obesity 8 219 3 121 7 36
Pelvic radiotherapy 0.8 23 0.4 15 0 0
Pelvic surgery 12 322 4 159 2 9
Prolapse 8 217 3 98 1 7
Prostate disease or surgery 9 252 8 293 5 24
Recurrent falls 6 157 22 792 22 108
Spinal cord disease/trauma 3 79 2 69 2 12
Smoking 5 126 5 195 2 9
Stroke 12 325 30 1,106 28 137
Trauma at childbirth 2 44 0.4 13 0 0
Urinary tract infection 19 502 26 974 20 100
Other∗ 31 836 29 1,060 29 140
No documentation of any including ‘other’ 7 196 2 61 2 9
∗ Other included nocturnal polyuria ‘incontinence’, ‘loss of control’, renal cancer.
(1,651/3,682) of hospital patients. The most common
lower urinary tract symptoms documented were: in
PCTs— urgency (43%, 1,158/2,717), urgency inconti-
nence (42%, 1,143/2,717) and stress incontinence (40%,
1,094/2,717); in hospitals—urinary frequency (22%,
806/3,682), nocturnal frequency (22%, 799/3,682) and noc-
turnal enuresis (21%, 774/3,682); and in CHs—nocturnalenuresis (43%, 211/488), nocturnal frequency (33%,162/488) and urinary frequency (32%, 156/488). Perma-
nent catheters were present in 17% (618/3,682) of hospital
patients, 13% (62/488) of CH residents and 3% (87/2,717)of PCT patients. Among 2,176 PCT patients with doc-
umentation of symptoms, 36% (788) had a diagnosis of
stress incontinence (SUI), 42% (904) had urgency inconti-
nence (UUI) and 19% (404) had mixed urinary incontinence
(MUI). Among 1,746 secondary care patients with documen-tation 18% (314) had a diagnosis of UUI, 12% (204) had SUI
and 8% (132) had MUI.
Details of assessment and management of UI are shown
in Table 3.It was found that 89% (435) of CH residents had a
documented care plan, compared with 51% (1,398) of PCT
and 41% (1,513) of hospital patients. In all 94% (1,416) of
hospital patients and 82% (356) of care home residents hadbeenreviewedwithin the last6 months, though longer review
times were evident in PCT patients. Where appropriate
3

8/14/2019 Continence Audit
http://slidepdf.com/reader/full/continence-audit 4/6
A. Wagg et al .
Table 3. Assessment and care
Primary Secondary Care
care (2, 717) car e ( 3,68 2) h omes ( 488). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ASSESSMENT % N % N % N Documented evidence of:
Rectal examination 10 272 24 902 9 43
Urinalysis 72 1,969 73 2,672 65 317
Use of a bladder diary 32 779/2,466 16 441/2,725 34 115/341
Evidence that medication that may exacerbate urinary incontinence has
been reviewed/altered to minimise impact
33 739/2,222 23 623/2,703 29 100/339
Specialist examination performed (YES) 37 997 52 1,897 20 100
Documented evidence of:
Examination of abdomen for palpable mass or bladder retention 60 600 92 1,748 77 77
Examination of perineum and pelvis to identify prolapse and excoriation,
and to assess pelvic floor contraction and urogenital atrophy
52 520 22 412 44 44
Rectal examination to exclude faecal loading/prostate size 25 246 36 680 25 25
Measurement of post-void residual volume (PVR) using ultrasound or
catheterisation
25 641/2,608 22 735/3,403 20 90/448
C lea r id enti fic at ion of t he t ype/ca use of uri na ry i nc onti nence 63 1,670/2,633 25 919/3,609 40 166/418
Specific treatment plan 68 1,835 45 1,670 82 400
TREATMENT (used or planned)
Advice on general health 33 907 9 338 25 122 Advice on lifestyle 18 477 4 133 16 79
Behaviour modification 5 146 4 147 6 29
Bladder training regimens 16 429 8 279 16 80
Containment 48 1,294 56 2,070 63 307
Electrical stimulation 0.6 16 0.3 11 0 0
Management of faecal impaction 2 61 6 229 16 79
Oestrogen treatment 3 76 0.8 28 0.4 2
Pelvic floor training 22 596 3 120 3 15
Pharmacological interventions 23 634 12 446 14 68
Surgery 5 149 3 101 1 5
Toileting schedules 12 320 16 583 60 291
Treatment of co-morbidities 5 148 14 527 10 48
Treatment of urinary tract infection 16 426 24 868 22 105
Other 10 274 8 295 6 28
None of above documented including ‘other’ 12 317 19 687 6 29
46% (1,112/2,443) of PCT patients, 21% (528/2,508) of hospital patients and 41% (122/299) of CH residents hada documented discussion about the cause and treatment of their incontinence.
Discussion
This is the largest and widest study of continence care inthe United Kingdom and provides a picture that reflects thecurrent state of services and care in primary and hospitalcare. Given the different considerations which affect thethree different settings, the level of engagement with thisfirst round of national audit was encouraging.
Hospitals
Most hospitals were able to complete the audit and animpressive 81% returned good data. Cases were identifiedby audit departments and clinical staff with an interest incontinencecare. Casesshouldhave beenconsecutive,but thismay not have been as rigidly applied as intended. Some sitesreported difficulty in accessing records and may thereforehave submitted a small sample of patients that was not
truly representative of their normal case mix. The samplein hospitals was, for the most part, drawn from inpatientsunder thecare of geriatricians— this introduces some bias, to
what extent fitter, although incontinent, older people might populate other wards is not known, but our results shouldbe viewed in this light. Nevertheless, the data are likely to begenerally representative of care in this sector.
Primary care
Primary care participation was good; this may reflect thebudgetary importance of continence and the fact that Continence Advisors were the professional group most motivated to carry out the audit. However, only one practiceper PCT was nominated to take part and it may not be
possible for the results to be generalised across the wholearea. A high proportion of primary care sites returned data via their continence services and thus these results may therefore not represent the experience of the ‘average’ GPpatient. Using the GP record as a source for patient notesproved difficult as there was often no mention of continencestatus; linking these records to those held by district nursing,
4

8/14/2019 Continence Audit
http://slidepdf.com/reader/full/continence-audit 5/6
Audit of continence care for older people
product supply databases or continence service records wasthen necessary, but again difficult.
Care homes
It was particularly difficult to recruit care homes, and thosethat were recruited had difficulties with data collection. Thishighlighted the challenge of carrying out audit in settings
where resources, staffing and culturedo notroutinely support it. A lack of access to a single central set of records, limitedinformation technology and staff shortage was often cited asa contributing difficulty. Many homes noted that continencestatus was assessed prior to admission and that the roleof care home staff was to enact a management plan ratherthan repeat the assessment process. It is also likely that only enthusiasticcare homes took part andthus theability to draw conclusions regarding care in that sector is severely limited.
The reported organisation of services suggests a goodbasic provision of care, particularly within primary care.Sectors ranged from 48 to 74% in reporting access to anintegratedservice but many had missing elements,suggesting that the perception of integration was optimistic and varieddepending upon the perspective of the reporting site. Thelack of a designated lead in most services is a specific barrierto development and quality improvement. The ultimate goalcontained in the NSF for Older People has not been met.
In general
The reported availability of specialist continence advisorsrepresents approximately one continence advisor per 40,000population over 65 years or about 8,400 men and women
withUI. This seemstoo fewpersonnelto provide anadequateservice for so many, particularly given the variable remit of existingadvisors, themajorityof whomwill coverbladderand
bowel care for the entire population. Department of Healthguidance unfortunately makes no firm recommendation onstaffing levels upon which to base these figures.
All settings reported a very high level of regard for privacy anddignityin relationto continence care.Thisis a particularly important observation given the sensitivities of bladder andbowel management and the importance given to privacy anddignity in the NSF follow-up document ‘A new ambition forold age’ [21]. There is concern that the impression of careproviders may not be shared by olderpeople themselves [22].
There may be institutionalised ‘blindness’ to deficiencies andan acceptance of a level of privacy and dignity, which might not meet the true wishes of older people.
These real-life, cross-sectional data illustrate the realnature of UI in the elderly in terms of medical co-morbidity;
cognitive and functional impairment. The audited samplerevealed a high distribution of functional and cognitiveimpairment, the ‘fittest’ patients being in the primary caregroup as might be expected. The small number of patients
with available AMTS or Barthel scores was not reported inour results, which therefore underestimate the true level of associated functional or cognitive impairment.
Most sectors claimed to ask routinely about bladderproblems but unfortunately, in many sites, elicitation of a positive response to the question did not guarantee anassessment of the problem and audit of the process of care
gave further cause for concern. A history was seldom takenin hospital, suggesting that continence is not a priority inacute care. A bladder diary, an essential component of theassessment, was seldom used in primary care, where onemight expect its uptake to be high. Likewise, a review of medication was seldom performed. Although recommendedas part of the specialist assessment, a rectal examination isinfrequently done.Very few people underwentan assessment of post-micturition residual urine as part of their evaluation.
Although there are no published data which support theroutine performance of this procedure in women, it is wellestablished that in men thepresence or absence of symptomsdo not predict finding of a significant residual, requiring thispart of the examination.
Importantly, a clear cause of incontinence was docu-
mented in only 25–63% of cases. Without a known cause,evidence-based, effective treatment could not be provided.Given the reported levels of training in assessment
and management across all sites, there appears to be adisparity between education, training and practice. This isnot uncommon, but does not serve patients well.
Management plans where they existed, alltoo often,reliedon containment. There was also ample evidence of rationing of continence products despite ‘free pads’ being availableto those in care homes. This is consistent with previous
work which suggests that the NHS provides only a thirdof the pad requirement associated with UI [23]. Patients
within the hospitals appeared to have unfettered access topads and products, perhaps reflecting the different budgetary pressures but encouraging indiscriminate usage.
Theremayhavebeenmarkeddifferencesinhowapatient’s
incontinence was managed in practice and that which wasdocumented. It is unlikely however, that key elements of theexamination areroutinely notdocumented and thus theaudit is likely to reflect actual practice in these areas.
This audit demonstrates that the requirement for inte-grated continence services contained within the NationalService Framework for Older People has not yet been met.
Action stillneedsto be takenwith regardto theestablishment of truly integrated, quality services in this neglected area of practice. Many services appeared to be reliant upon the input from specialist continence advisors at the expense of basicassessment and care undertaken by clinical staff. Regardlessof the organisation of care, these data illustrated an urgent need to re-establish the fundamentals of continence care
within the daily practice of medical and nursing staff looking
after patients. The cost of continence care is high, whether measuredin health care or financial terms. Services which deliverhigh quality evidence-based care should be able to manageand thus reduce the associated morbidity and ensure that financial costs are based on cost-effective decisions. If specialist continence services are to cater to the needs of
5

8/14/2019 Continence Audit
http://slidepdf.com/reader/full/continence-audit 6/6
A. Wagg et al .
all people with continence problems then there is a largeresource problem, particularly in the lightof current financialpressure which has resulted in a withdrawal of continencecare in some areas of the country.
Key points• Assessment and management of older people is under-
assessed and under-treated.• There is an over-reliance on containment as the sole
source of management of the condition.• The rectal examination is seldom undertaken as part of
the assessment of urinary incontinence.• There is a great opportunity to improve the treatment and
lot of older people with bladder problems.
Conflicts of interest
None
Acknowledgements
To the Continence Working Party, for their support andguidance
To all those nationally who gave time and energy insubmitting data to the audit.
References
1. Thomas TM, Plymat KR, Blannin J et al . Prevalence of urinary incontinence. Br Med J 1980; 281: 1243 –45.
2. Perry S, Shaw C, Assassa P et al . An epidemiological study toestablish the prevalence of urinary symptoms and felt need inthe community: The Leicestershire MRC Incontinence Study.
J Public Health Med 2000; 22: 427– 34.
3. Royal College of Physicians. Incontinence: Causes,Management and Provision of Services. London: The RoyalCollege of Physicians, 1995.
4. Peet SM, Castleden SM, McGrotherCW. Prevalence of urinary and faecal incontinence in hospitals and residential and nursing homes for older people. Br Med J 1995; 311: 1063– 4.
5. Dugan E, Roberts CP, Cohen SJ et al . Why older community-dwelling adults do not discuss urinary incontinence with theirprimary care physicians. J Am Geriatr Soc 2001; 49: 462–5.
6. Wagg AS, Malone-Lee JG. Urinary incontinence in the elderly.Br J Urol 1998; 82(Suppl. 1): 11 –7.
7. Teunissen TA, de Jonge A, van Weel C et al . Treating urinary incontinence in the elderly–conservative therapies that work:
a systematic review. J Fam Pract 2004; 53: 25– 32.8. Burgio K, Locher JL, Goode PS. Combined behavioural and
drug therapy for urge incontinence in older women. J AmGeriatr Soc 2000; 48: 370– 4.
9. Cassells C, Watt E. The impact of incontinence on olderspousal caregivers. J Adv Nurs 2003; 42: 607– 16.
10. ThomDH, HaanMN, vanden EedenSK. Medically recognisedurinary incontinence and risks of hospitalisation, nursing home
admission and mortality. Age Ageing 1997; 26: 367–74.11. Making the Case for Investment in an Integrated ContinenceService. London: The Continence Foundation, 2000.
12. Department of Health. Good Practice in Continence Services.London: HMSO, 2000.
13. Department of Health. National Service Framework for OlderPeople. London: HMSO, 2001.
14. Thomas S. Is Policy Translated into Action? A Report by the Royal College of Nursing Continence care Forum and
the Continence Foundation. London: Continence Foundation,2003.
15. Royal College of Physicians. Promoting Continence. Clinicalaudit Scheme for the Management of Urinary and FaecalIncontinence. London: Royal College of Physicians, 1998.
16. Royal College of Physicians of London. The CAREScheme– Continuous Assessment, Review and Evaluation.Clinical Audit of Long-Term Care of Elderly People, 2nd
edition. Prepared by Professor John Brocklehurst and DrEdward Dickinson, 1999.
17. Georgiou A, Potter JM, Brocklehurst J et al . Measuring thequality of continence care in long term care facilities: ananalysis of outcome indicators. Age Ageing 2001; 30: 63–6.
18. Mian S, Wagg A, Potter J et al . National audit of continencecare for older people: resources and method. J Eval Clin Pract
2005; 11: 533–43.19. WaggA, Billings J. Involving older users of continence services
in developing standards of care: Differences and similaritiesbetween professional and user’s views. In: Proceedings of theInternational Continence Society Meeting, Paris, 2004.
20. WaggA, MianS, LoweD et al . The national auditof continencecare for older people: results of a pilot study. J Eval Clin Pract 2005; 11: 525–32.
21. Philp I. A New Ambition for Old Age: Next steps inImplementing the National Service Framework for Older
People. London: Department of Health, 2006.22. Billings J, Wagg A. A study to involve older continence service
users in the development of quality standards in continenceservices. In: Proceedings of the International ContinenceSociety, Christchurch, New Zealand, 2006; pp. 203–4.
23. Wagg A, Cox J, Porkess S, Das Gupta R. Pad use and cost in women seeking care for their urinary incontinence in the
UK/RoI: Data from the PURE study (UK). In: Proceedingsof the International Urogynaecology Society, Athens, 2006.
Received 19 November 2006; accepted in revised form 19 June
2007
6



![Improving Continence Care in Older People · 2020. 9. 8. · 2020 Improving Continence Care in Older People CQ - Clinical Quality - CQ - Patient Safety [ 106 ] Implementation of continence](https://img.pdfslide.us/doc/110x75/611ac639260ae10c6508b335/improving-continence-care-in-older-people-2020-9-8-2020-improving-continence.jpg)
























