Embed Size (px)
Citation preview
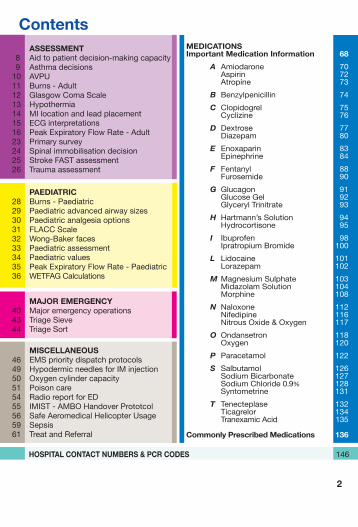
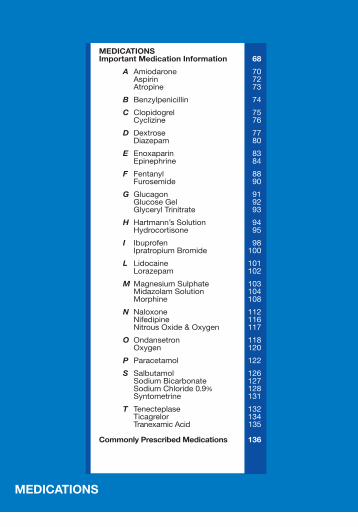
ContentsMEDICATIONS Important Medication Information 68
A Amiodarone 70 Aspirin 72 Atropine 73
B Benzylpenicillin 74
C Clopidogrel 75 Cyclizine 76
D Dextrose 77 Diazepam 80
EEnoxaparin 83 Epinephrine 84
F Fentanyl 88 Furosemide 90
G Glucagon 91 GlucoseGel 92 GlycerylTrinitrate 93
H Hartmann’sSolution 94 Hydrocortisone 95
I Ibuprofen 98 IpratropiumBromide 100
L Lidocaine 101 Lorazepam 102
MMagnesiumSulphate 103 MidazolamSolution 104 Morphine 108
N Naloxone 112 Nifedipine 116 NitrousOxide&Oxygen 117
O Ondansetron 118 Oxygen 120
P Paracetamol 122
S Salbutamol 126 SodiumBicarbonate 127 SodiumChloride0.9% 128 Syntometrine 131
T Tenecteplase 132 Ticagrelor 134 TranexamicAcid 135
Commonly Prescribed Medications 136
HOSPITAL CONTACT NUMBERS & PCR CODES 146
2
ASSESSMENT 8 Aidtopatientdecision-makingcapacity 9 Asthmadecisions10 AVPU11 Burns-Adult12 GlasgowComaScale13 Hypothermia14 MIlocationandleadplacement15 ECGinterpretations16 PeakExpiratoryFlowRate-Adult23 Primarysurvey24 Spinalimmobilisationdecision25 StrokeFASTassessment26 Traumaassessment
PAEDIATRIC28 Burns-Paediatric29 Paediatricadvancedairwaysizes30 Paediatricanalgesiaoptions31 FLACCScale32 Wong-Bakerfaces33 Paediatricassessment34 Paediatricvalues35 PeakExpiratoryFlowRate-Paediatric36 WETFAGCalculations
MAJOR EMERGENCY40 Majoremergencyoperations 43 TriageSieve 44 TriageSort
MISCELLANEOUS46 EMSprioritydispatchprotocols49 HypodermicneedlesforIMinjection50 Oxygencylindercapacity51 Poisoncare54 RadioreportforED55 IMIST-AMBOHandoverPrototcol56 SafeAeromedicalHelicopterUsage59 Sepsis61 TreatandReferral
3
Field GuidePublished 2014
ThePre-HospitalEmergencyCareCouncil(PHECC)isanindependentstatutorybodywithresponsibilityforstandards,educationandtraininginpre-hospitalemergencycareinIreland.PHECC’sprimaryroleistoprotectthepublic.
Mission Statement The Pre-Hospital Emergency Care Council protects the public by independently specifying, reviewing, maintaining and monitoring standards of excellence for the delivery of quality pre-hospital emergency care for people in Ireland.
TheCouncilwasestablishedasabodycorporatebytheMinisterforHealthandChildrenbyStatutoryInstrumentNumber109of2000(EstablishmentOrder)whichwasamendedbyStatutoryInstrumentNumber575of2004(AmendmentOrder).TheseOrdersweremadeundertheHealth(CorporateBodies)Act,1961asamendedandtheHealth(MiscellaneousProvisions)Act2007.
Medications UpdatePleaserefertowww.phecc.ieortheFieldGuideSmartPhoneAppforup-to-datemedicationsinformation.
PHECC Field Guide for Practitioners 2014Project Leader: MrJohnLally,MSc,ICTSupportOfficer,PHECC.
Clinical Editor:MrBrianPower,MScinEMS,MBA,NQEMT-AP,ProgrammeDevelopmentOfficer,PHECC.
Published by:ThePre-HospitalEmergencyCareCouncilAbbeyMoatHouse,AbbeyStreet,Naas,CoKildare,IrelandPhone:+353(0)45882042Fax:+353(0)45882089Email:[email protected]:www.phecc.ieISBN:978-0-9562261-5-0
©Pre-HospitalEmergencyCareCouncil2014
Anypartofthispublicationmaybereproducedforeducationalpurposesandqualityimprovementprogrammessubjecttotheinclusionofanacknowledgementofthesource.Itmaynotbeusedforcommercialpurposes.
AcknowledgementOurthankstothePractitioners(PaulKelly,BrianO’Moore,DesmondWade,JasonMasterson,OmarFitzell,GregCookeandThomasBrady)whohelpedtodevelopthisguidebyparticipatingintheconsultationprocess.
4
5
IntroductionThisFieldGuideisnotasubstituteforthepublishedClinicalPracticeGuidelines(CPGs).ItisaquickreferencetohelpPractitionersinthefieldparticularlywithmedicationcalculationsandinfrequentclinicalencounters.Italsogivesvaluesforclinicalmeasurementsi.e.GCS.
ThisFieldGuidedoesnotauthoriseskillsormedicationadministration.PractitionersshouldonlypracticewithintheirscopeofpracticeandinaccordancewiththeirlevelonthePHECCRegister.
Therouteofadministrationshouldbeappropriatetothepatient’sclinicalpresentation.
Medications may be administered provided1. ThePractitionerisingoodstandingonthePHECCRegister.
2. ThePractitionercomplieswiththeCPGspublishedbyPHECC.
3. ThePractitionerisacting(paidorvoluntary)onbehalfofan organisationthatisaPHECClicencedCPGprovider.
4. ThePractitionerisprivileged,bytheorganisationonwhosebehalfhe/sheisacting,toadministerthemedication.
5. ThePractitionerhasreceivedtrainingon,andiscompetentin,theadministrationofthemedication.
6. ThemedicationsarelistedintheMedicinalProducts7th Schedule.
Paediatric values ThisguidehasadoptedtheBroselowtapecolourschemetoassistwithcalculations.
3-5Kg 6-7Kg 10-11Kg 12-14Kg 15-18Kg 19-22Kg 24-28Kg 30-36Kg
Notes
6
ASSESSMENT
ASSESSMENT 8 Aidtopatientdecision-makingcapacity 9 Asthmadecisions10 AVPU11 Burns-Adult12 GlasgowComaScale13 Hypothermia14 MIlocationandleadplacement15 ECGinterpretations16 PeakExpiratoryFlowRate-Adult23 Primarysurvey24 Spinalimmobilisationdecision25 StrokeFASTassessment26 Traumaassessment
8
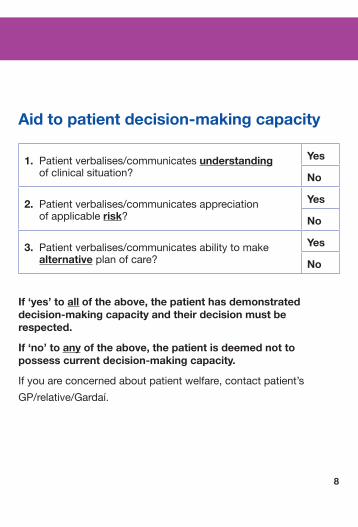
Aid to patient decision-making capacity
1. Patientverbalises/communicatesunderstandingofclinicalsituation?
Yes
No
2. Patientverbalises/communicatesappreciationofapplicablerisk?
Yes
No
3. Patientverbalises/communicatesabilitytomakealternativeplanofcare?
Yes
No
If ‘yes’ to all of the above, the patient has demonstrated decision-making capacity and their decision must be respected.
If ‘no’ to any of the above, the patient is deemed not to possess current decision-making capacity.
Ifyouareconcernedaboutpatientwelfare,contactpatient’s
GP/relative/Gardaí.
Assmt
9
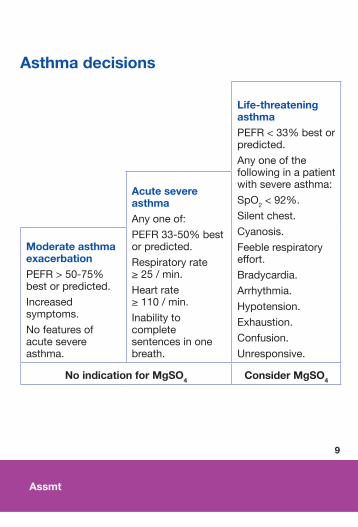
Asthma decisions
Life-threatening asthma PEFR<33%bestorpredicted.
Anyoneofthefollowinginapatientwithsevereasthma:
SpO2<92%.
Silentchest.
Cyanosis.
Feeblerespiratoryeffort.
Bradycardia.
Arrhythmia.
Hypotension.
Exhaustion.
Confusion.
Unresponsive.
Acute severe asthma Anyoneof:
PEFR33-50%bestorpredicted.
Respiratoryrate≥25/min.
Heartrate≥110/min.
Inabilitytocompletesentencesinonebreath.
Moderate asthma exacerbation PEFR>50-75%bestorpredicted.
Increasedsymptoms.
Nofeaturesofacutesevereasthma.
No indication for MgSO4 Consider MgSO4
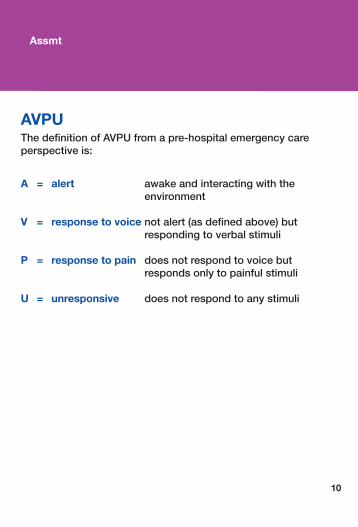
AVPUThe definition of AVPU from a pre-hospital emergency care perspective is:
A = alert awake and interacting with the environment
V = response to voice not alert (as defined above) but responding to verbal stimuli
P = response to pain does not respond to voice but responds only to painful stimuli
U = unresponsive does not respond to any stimuli
10
Assmt
Assmt
11
9%
1%
9%9%
18% 18%
Front of trunk 18%
Back of trunk 18%
Adult
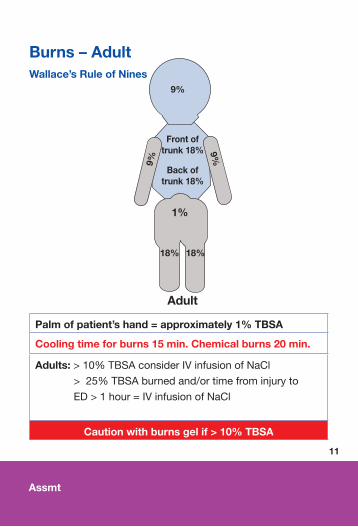
Burns – Adult Wallace’s Rule of Nines
Palm of patient’s hand = approximately 1% TBSA
Cooling time for burns 15 min. Chemical burns 20 min.
Adults:>10%TBSAconsiderIVinfusionofNaCl
>25%TBSAburnedand/ortimefrominjuryto
ED>1hour=IVinfusionofNaCl
Caution with burns gel if > 10% TBSA
Assmt
12
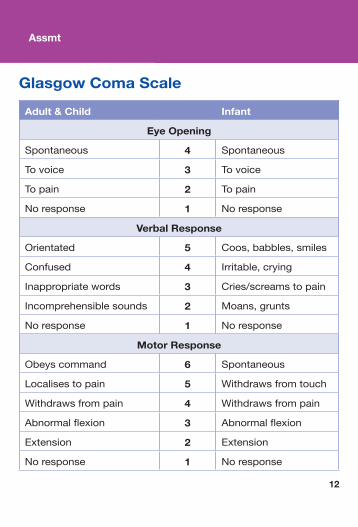
Glasgow Coma Scale
Adult & Child Infant
Eye Opening
Spontaneous 4 Spontaneous
Tovoice 3 Tovoice
Topain 2 Topain
Noresponse 1 Noresponse
Verbal Response
Orientated 5 Coos,babbles,smiles
Confused 4 Irritable,crying
Inappropriatewords 3 Cries/screamstopain
Incomprehensiblesounds 2 Moans,grunts
Noresponse 1 Noresponse
Motor Response
Obeyscommand 6 Spontaneous
Localisestopain 5 Withdrawsfromtouch
Withdrawsfrompain 4 Withdrawsfrompain
Abnormalflexion 3 Abnormalflexion
Extension 2 Extension
Noresponse 1 Noresponse
Assmt
13
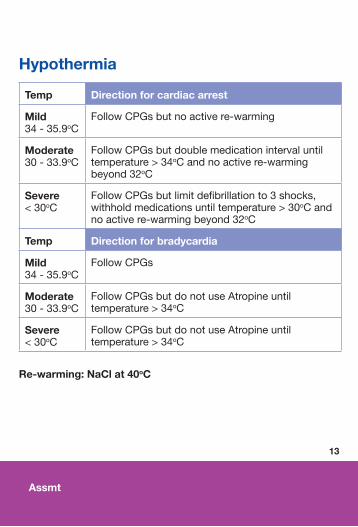
Hypothermia
Temp Direction for cardiac arrest
Mild34-35.9oC
FollowCPGsbutnoactivere-warming
Moderate30-33.9oC
FollowCPGsbutdoublemedicationintervaluntiltemperature>34oCandnoactivere-warmingbeyond32oC
Severe<30oC
FollowCPGsbutlimitdefibrillationto3shocks,withholdmedicationsuntiltemperature>30oCandnoactivere-warmingbeyond32oC
Temp Direction for bradycardia
Mild34-35.9oC
FollowCPGs
Moderate30-33.9oC
FollowCPGsbutdonotuseAtropineuntiltemperature>34oC
Severe<30oC
FollowCPGsbutdonotuseAtropineuntiltemperature>34oC
Re-warming: NaCl at 40oC
Assmt
14
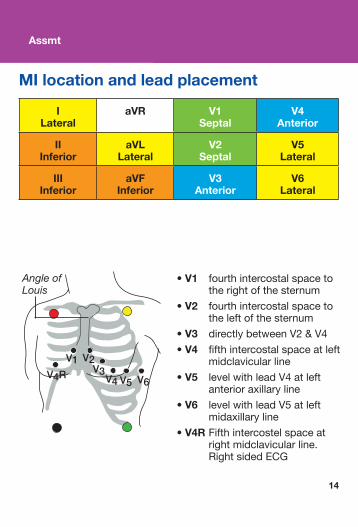
MI location and lead placement
I Lateral
aVR V1 Septal
V4 Anterior
II Inferior
aVL Lateral
V2 Septal
V5 Lateral
III Inferior
aVF Inferior
V3 Anterior
V6 Lateral
• V1 fourthintercostalspaceto therightofthesternum
• V2 fourthintercostalspaceto theleftofthesternum
• V3 directlybetweenV2&V4• V4 fifthintercostalspaceatleft
midclavicularline
• V5 levelwithleadV4atleftanterioraxillaryline
• V6 levelwithleadV5atleft midaxillaryline
• V4RFifthintercostelspaceat rightmidclavicularline. RightsidedECG
Angle of Louis
Assmt
15
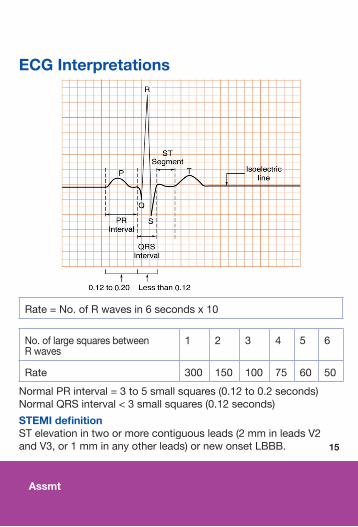
Rate=No.ofRwavesin6secondsx10
No.oflargesquaresbetweenRwaves
1 2 3 4 5 6
Rate 300 150 100 75 60 50
NormalPRinterval=3to5smallsquares(0.12to0.2seconds)NormalQRSinterval<3smallsquares(0.12seconds)
STEMI definitionSTelevationintwoormorecontiguousleads(2mminleadsV2andV3,or1mminanyotherleads)ornewonsetLBBB.
ECG Interpretations
Assmt
16
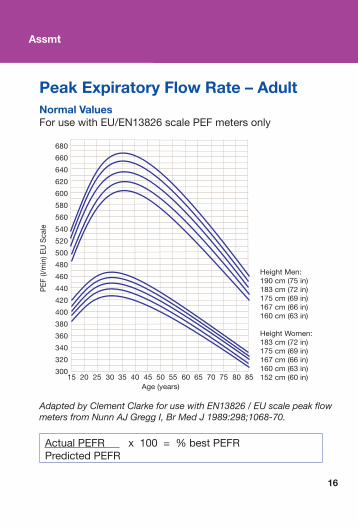
Peak Expiratory Flow Rate – AdultNormal ValuesForusewithEU/EN13826scalePEFmetersonly
Adapted by Clement Clarke for use with EN13826 / EU scale peak flow meters from Nunn AJ Gregg I, Br Med J 1989:298;1068-70.
ActualPEFRx100=%bestPEFRPredictedPEFR
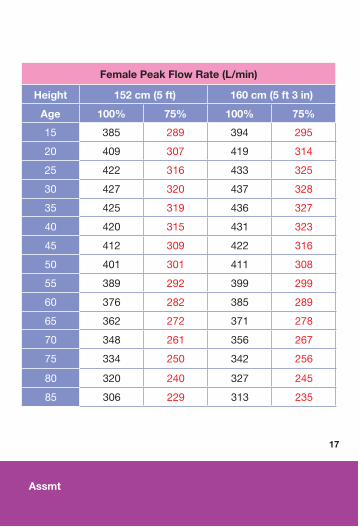
Female Peak Flow Rate (L/min)
Height 152 cm (5 ft) 160 cm (5 ft 3 in)
Age 100% 75% 100% 75%
15 385 289 394 295
20 409 307 419 314
25 422 316 433 325
30 427 320 437 328
35 425 319 436 327
40 420 315 431 323
45 412 309 422 316
50 401 301 411 308
55 389 292 399 299
60 376 282 385 289
65 362 272 371 278
70 348 261 356 267
75 334 250 342 256
80 320 240 327 245
85 306 229 313 235
17
Assmt
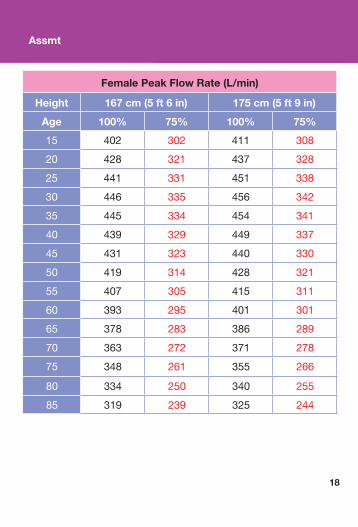
Female Peak Flow Rate (L/min)
Height 167 cm (5 ft 6 in) 175 cm (5 ft 9 in)
Age 100% 75% 100% 75%
15 402 302 411 308
20 428 321 437 328
25 441 331 451 338
30 446 335 456 342
35 445 334 454 341
40 439 329 449 337
45 431 323 440 330
50 419 314 428 321
55 407 305 415 311
60 393 295 401 301
65 378 283 386 289
70 363 272 371 278
75 348 261 355 266
80 334 250 340 255
85 319 239 325 244
18
Assmt
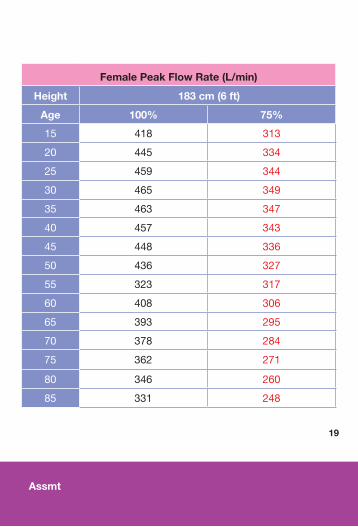
Female Peak Flow Rate (L/min)
Height 183 cm (6 ft)
Age 100% 75%
15 418 313
20 445 334
25 459 344
30 465 349
35 463 347
40 457 343
45 448 336
50 436 327
55 323 317
60 408 306
65 393 295
70 378 284
75 362 271
80 346 260
85 331 248
19
Assmt
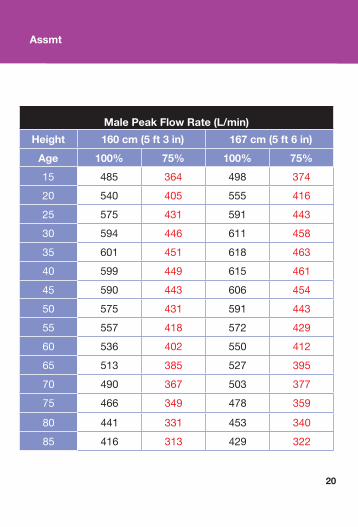
Male Peak Flow Rate (L/min)
Height 160 cm (5 ft 3 in) 167 cm (5 ft 6 in)
Age 100% 75% 100% 75%
15 485 364 498 374
20 540 405 555 416
25 575 431 591 443
30 594 446 611 458
35 601 451 618 463
40 599 449 615 461
45 590 443 606 454
50 575 431 591 443
55 557 418 572 429
60 536 402 550 412
65 513 385 527 395
70 490 367 503 377
75 466 349 478 359
80 441 331 453 340
85 416 313 429 322
20
Assmt
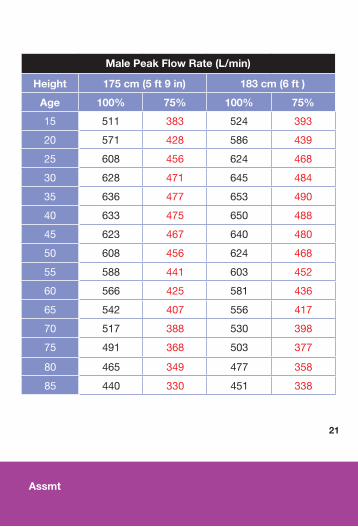
Male Peak Flow Rate (L/min)
Height 175 cm (5 ft 9 in) 183 cm (6 ft )
Age 100% 75% 100% 75%
15 511 383 524 393
20 571 428 586 439
25 608 456 624 468
30 628 471 645 484
35 636 477 653 490
40 633 475 650 488
45 623 467 640 480
50 608 456 624 468
55 588 441 603 452
60 566 425 581 436
65 542 407 556 417
70 517 388 530 398
75 491 368 503 377
80 465 349 477 358
85 440 330 451 338
Assmt
21
22
Assmt
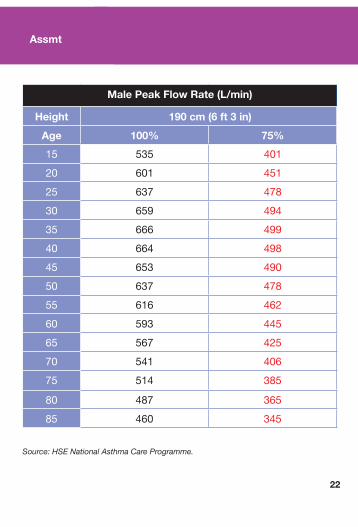
Male Peak Flow Rate (L/min)
Height 190 cm (6 ft 3 in)
Age 100% 75%
15 535 401
20 601 451
25 637 478
30 659 494
35 666 499
40 664 498
45 653 490
50 637 478
55 616 462
60 593 445
65 567 425
70 541 406
75 514 385
80 487 365
85 460 345
Source: HSE National Asthma Care Programme.
23
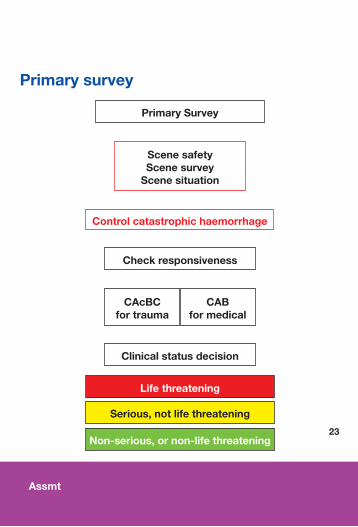
Primary survey
Primary Survey
Clinical status decision
Life threatening
Serious, not life threatening
Non-serious, or non-life threatening
CAcBC for trauma
CAB for medical
Control catastrophic haemorrhage
Scene safety Scene survey
Scene situation
Check responsiveness
Assmt
Assmt
24
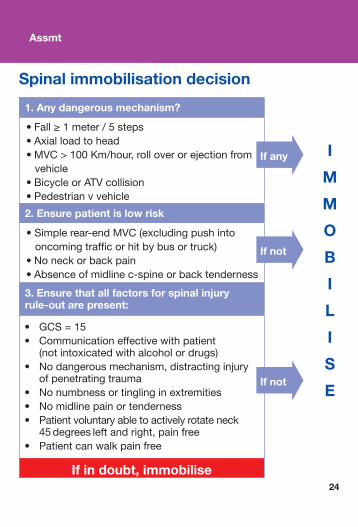
Spinal immobilisation decision
1. Any dangerous mechanism?
•Fall≥1meter/5steps•Axialloadtohead•MVC>100Km/hour,rolloverorejectionfromvehicle•BicycleorATVcollision•Pedestrianvvehicle
2. Ensure patient is low risk
•Simplerear-endMVC(excludingpushintooncomingtrafficorhitbybusortruck)•Noneckorbackpain•Absenceofmidlinec-spineorbacktenderness
3. Ensure that all factors for spinal injury rule-out are present:
If in doubt, immobilise
I
M
M
O
B
I
L
I
S
E
If any
If not
If not
• GCS=15• Communicationeffectivewithpatient (notintoxicatedwithalcoholordrugs)• Nodangerousmechanism,distractinginjury ofpenetratingtrauma• Nonumbnessortinglinginextremities• Nomidlinepainortenderness• Patientvoluntaryabletoactivelyrotateneck 45degreesleftandright,painfree• Patientcanwalkpainfree
25
Stroke FAST assessmentF – Facial weakness •Canthepatientsmile? •Hasthemouthoraneyedrooped? •Whichside?
A – Arm weakness •Canthepatientraisebotharmsandmaintainfor5seconds?
S – Speech problems •Canthepatientspeakclearlyandunderstandwhatyousay?
T – Time when last normal •Onsetlessthan4.5hours
Don’t forget to check glucose!
RefertoFAST+inASHICEmessage.
Assmt
Assmt
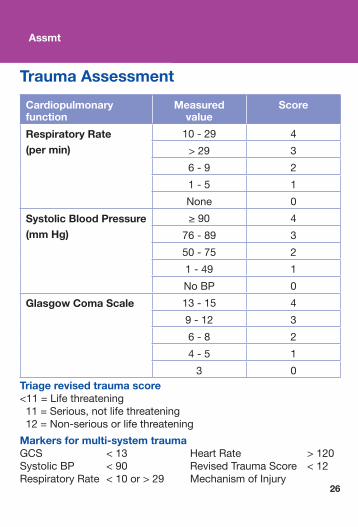
Trauma Assessment
Cardiopulmonary function
Measured value
Score
Respiratory Rate(per min)
10-29 4
>29 3
6-9 2
1-5 1
None 0
Systolic Blood Pressure (mm Hg)
≥90 4
76-89 3
50-75 2
1-49 1
NoBP 0
Glasgow Coma Scale 13-15 4
9-12 3
6-8 2
4-5 1
3 0Triage revised trauma score<11=Lifethreatening11=Serious,notlifethreatening12=Non-seriousorlifethreatening
Markers for multi-system trauma GCS <13 HeartRate >120SystolicBP <90 RevisedTraumaScore <12RespiratoryRate<10or>29 MechanismofInjury
26
PAEDIATRIC
PAEDIATRIC28 Burns-Paediatric29 Paediatricadvancedairwaysizes30 Paediatricanalgesiaoptions31 FLACCScale32 Wong-Bakerfaces33 Paediatricassessment34 Paediatricvalues35 PeakExpiratoryFlowRate-Paediatric36 WETFAGCalculations
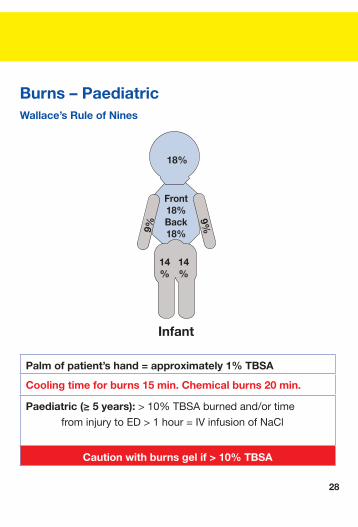
Burns – Paediatric Wallace’s Rule of Nines
Palm of patient’s hand = approximately 1% TBSA
Cooling time for burns 15 min. Chemical burns 20 min.
Paediatric (≥ 5 years): >10%TBSAburnedand/ortime
frominjurytoED>1hour=IVinfusionofNaCl
Caution with burns gel if > 10% TBSA
18%
9%9%
14%
14%
Front 18%Back 18%
Infant
28
Paed
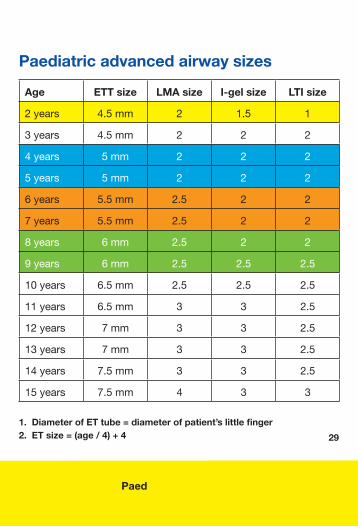
Paediatric advanced airway sizes
Age ETT size LMA size I-gel size LTI size
2years 4.5mm 2 1.5 1
3years 4.5mm 2 2 2
4years 5mm 2 2 2
5years 5mm 2 2 2
6years 5.5mm 2.5 2 2
7years 5.5mm 2.5 2 2
8years 6mm 2.5 2 2
9years 6mm 2.5 2.5 2.5
10years 6.5mm 2.5 2.5 2.5
11years 6.5mm 3 3 2.5
12years 7mm 3 3 2.5
13years 7mm 3 3 2.5
14years 7.5mm 3 3 2.5
15years 7.5mm 4 3 3
1. Diameter of ET tube = diameter of patient’s little finger 2. ET size = (age / 4) + 4 29
Paed
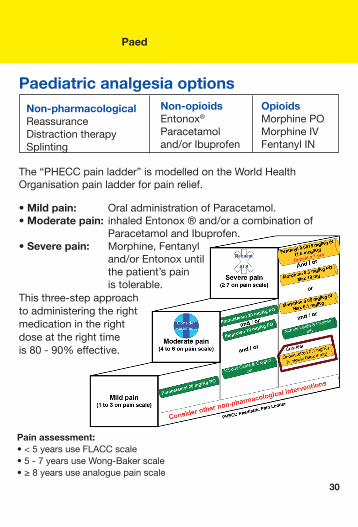
Paediatric analgesia optionsNon-pharmacological ReassuranceDistractiontherapySplinting
The“PHECCpainladder”ismodelledontheWorldHealthOrganisationpainladderforpainrelief.
• Mild pain: OraladministrationofParacetamol.• Moderate pain: inhaledEntonox®and/oracombinationof ParacetamolandIbuprofen.• Severe pain: Morphine,Fentanyl and/orEntonoxuntil thepatient’spain istolerable.Thisthree-stepapproachtoadministeringtherightmedicationintherightdoseattherighttimeis80-90%effective.
Non-opioids Entonox®Paracetamoland/orIbuprofen
Opioids MorphinePOMorphineIVFentanylIN
30
Pain assessment:•<5yearsuseFLACCscale•5-7yearsuseWong-Bakerscale•≥8yearsuseanaloguepainscale
Paed
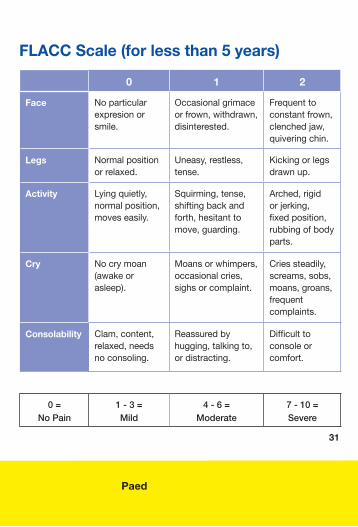
FLACC Scale (for less than 5 years)
0 1 2
Face Noparticularexpresionorsmile.
Occasionalgrimaceorfrown,withdrawn,disinterested.
Frequenttoconstantfrown,clenchedjaw,quiveringchin.
Legs Normalpositionorrelaxed.
Uneasy,restless,tense.
Kickingorlegsdrawnup.
Activity Lyingquietly,normalposition,moveseasily.
Squirming,tense,shiftingbackandforth,hesitanttomove,guarding.
Arched,rigidorjerking,fixedposition,rubbingofbodyparts.
Cry Nocrymoan(awakeorasleep).
Moansorwhimpers,occasionalcries,sighsorcomplaint.
Criessteadily,screams,sobs,moans,groans,frequentcomplaints.
Consolability Clam,content,relaxed,needsnoconsoling.
Reassuredbyhugging,talkingto,ordistracting.
Difficulttoconsoleorcomfort.
0 =No Pain
1 - 3 =Mild
4 - 6 =Moderate
7 - 10 =Severe
31
Paed
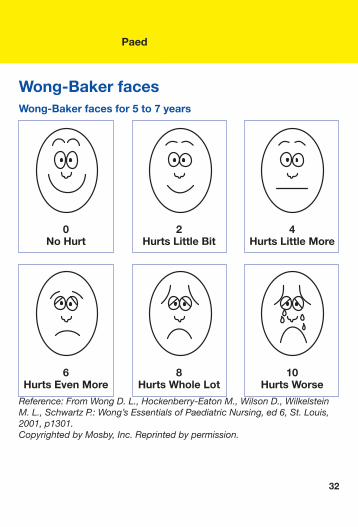
Wong-Baker faces Wong-Baker faces for 5 to 7 years Reference: From Wong D. L., Hockenberry-Eaton M., Wilson D., Wilkelstein M. L., Schwartz P.: Wong’s Essentials of Paediatric Nursing, ed 6, St. Louis, 2001, p1301.Copyrighted by Mosby, Inc. Reprinted by permission.
0 No Hurt
6 Hurts Even More
2 Hurts Little Bit
8 Hurts Whole Lot
4 Hurts Little More
10 Hurts Worse
32
Paed
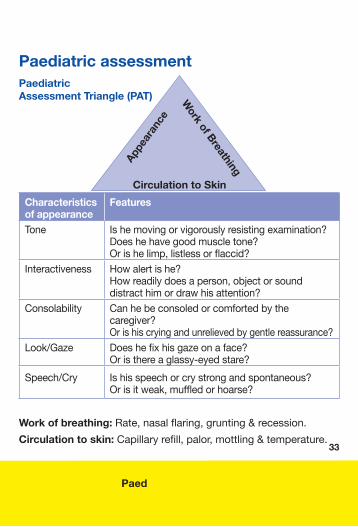
Paediatric assessment Paediatric Assessment Triangle (PAT)
Characteristics of appearance
Features
Tone
Ishemovingorvigorouslyresistingexamination?Doeshehavegoodmuscletone?Orishelimp,listlessorflaccid?
Interactiveness
Howalertishe?Howreadilydoesaperson,objectorsounddistracthimordrawhisattention?
Consolability
Canhebeconsoledorcomfortedbythecaregiver?Orishiscryingandunrelievedbygentlereassurance?
Look/Gaze Doeshefixhisgazeonaface?Oristhereaglassy-eyedstare?
Speech/Cry Ishisspeechorcrystrongandspontaneous?Orisitweak,muffledorhoarse?
Work of breathing:Rate,nasalflaring,grunting&recession.
Circulation to skin:Capillaryrefill,palor,mottling&temperature.
Appe
aran
ce
Circulation to SkinW
ork of Breathing
33
Paed
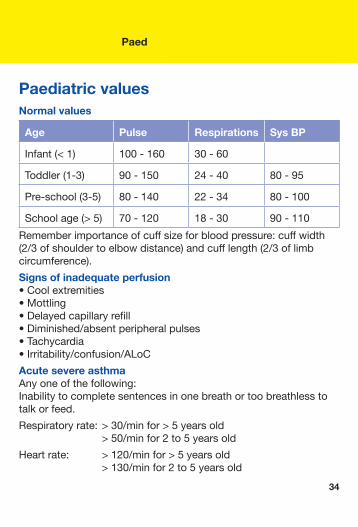
Paediatric values Normal values
Age Pulse Respirations Sys BP
Infant(<1) 100-160 30-60
Toddler(1-3) 90-150 24-40 80-95
Pre-school(3-5) 80-140 22-34 80-100
Schoolage(>5) 70-120 18-30 90-110
Rememberimportanceofcuffsizeforbloodpressure:cuffwidth(2/3ofshouldertoelbowdistance)andcufflength(2/3oflimbcircumference).
Signs of inadequate perfusion •Coolextremities •Mottling•Delayedcapillaryrefill•Diminished/absentperipheralpulses•Tachycardia•Irritability/confusion/ALoC
Acute severe asthma Anyoneofthefollowing:Inabilitytocompletesentencesinonebreathortoobreathlesstotalkorfeed.
Respiratoryrate:>30/minfor>5yearsold >50/minfor2to5yearsold
Heartrate: >120/minfor>5yearsold >130/minfor2to5yearsold
34
Paed
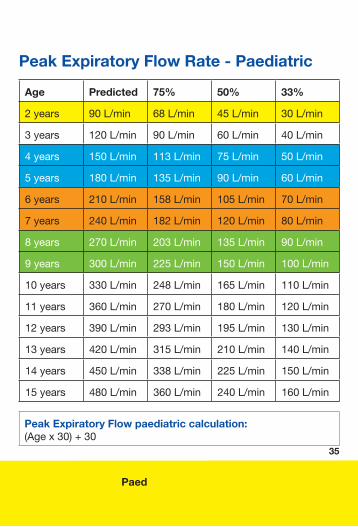
Peak Expiratory Flow Rate - Paediatric
Age Predicted 75% 50% 33%
2years 90L/min 68L/min 45L/min 30L/min
3years 120L/min 90L/min 60L/min 40L/min
4years 150L/min 113L/min 75L/min 50L/min
5years 180L/min 135L/min 90L/min 60L/min
6years 210L/min 158L/min 105L/min 70L/min
7years 240L/min 182L/min 120L/min 80L/min
8years 270L/min 203L/min 135L/min 90L/min
9years 300L/min 225L/min 150L/min 100L/min
10years 330L/min 248L/min 165L/min 110L/min
11years 360L/min 270L/min 180L/min 120L/min
12years 390L/min 293L/min 195L/min 130L/min
13years 420L/min 315L/min 210L/min 140L/min
14years 450L/min 338L/min 225L/min 150L/min
15years 480L/min 360L/min 240L/min 160L/min
Peak Expiratory Flow paediatric calculation: (Agex30)+30
35
Paed
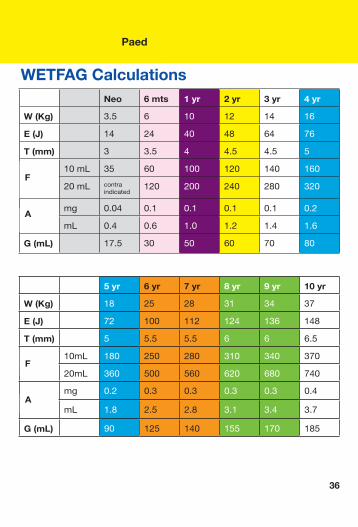
5 yr 6 yr 7 yr 8 yr 9 yr 10 yr
W (Kg) 18 25 28 31 34 37
E (J) 72 100 112 124 136 148
T (mm) 5 5.5 5.5 6 6 6.5
10mL 180 250 280 310 340 370
20mL 360 500 560 620 680 740
mg 0.2 0.3 0.3 0.3 0.3 0.4
mL 1.8 2.5 2.8 3.1 3.4 3.7
G (mL) 90 125 140 155 170 185
WETFAG Calculations
36
Neo 6 mts 1 yr 2 yr 3 yr 4 yr
W (Kg) 3.5 6 10 12 14 16
E (J) 14 24 40 48 64 76
T (mm) 3 3.5 4 4.5 4.5 5
10mL 35 60 100 120 140 160
20mL contraindicated
120 200 240 280 320
mg 0.04 0.1 0.1 0.1 0.1 0.2
mL 0.4 0.6 1.0 1.2 1.4 1.6
G (mL) 17.5 30 50 60 70 80
A
F
A
F
Paed
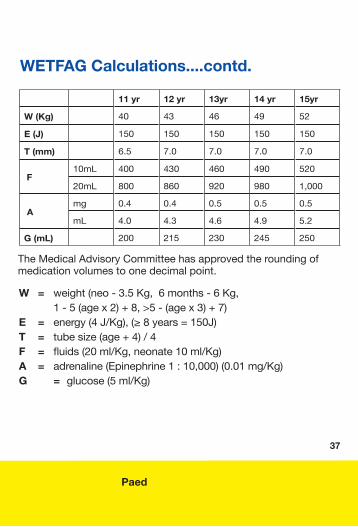
11 yr 12 yr 13yr 14 yr 15yr
W (Kg) 40 43 46 49 52
E (J) 150 150 150 150 150
T (mm) 6.5 7.0 7.0 7.0 7.0
F 10mL 400 430 460 490 520
20mL 800 860 920 980 1,000
A mg 0.4 0.4 0.5 0.5 0.5
mL 4.0 4.3 4.6 4.9 5.2
G (mL) 200 215 230 245 250
W = weight(neo-3.5Kg,6months-6Kg, 1-5(agex2)+8,>5-(agex3)+7)E = energy(4J/Kg),(≥8years=150J)T = tubesize(age+4)/4F = fluids(20ml/Kg,neonate10ml/Kg)A = adrenaline(Epinephrine1:10,000)(0.01mg/Kg)G = glucose(5ml/Kg)
WETFAG Calculations....contd.
TheMedicalAdvisoryCommitteehasapprovedtheroundingofmedicationvolumestoonedecimalpoint.
37
F
A

Notes
38
MAJOR EMERGENCY
MAJOR EMERGENCY
40 Majoremergencyoperations 43 TriageSieve 44 TriageSort
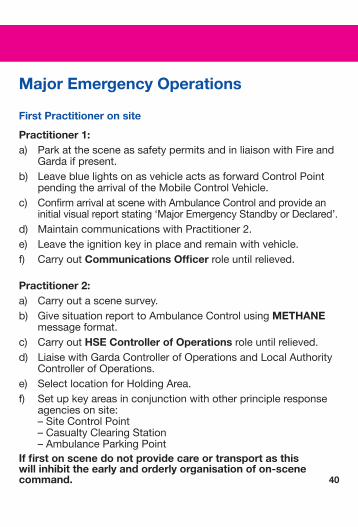
Major Emergency Operations
First Practitioner on site
Practitioner 1:a) ParkatthesceneassafetypermitsandinliaisonwithFireand
Gardaifpresent.b) LeavebluelightsonasvehicleactsasforwardControlPoint
pendingthearrivaloftheMobileControlVehicle.c) ConfirmarrivalatscenewithAmbulanceControlandprovidean
initialvisualreportstating‘MajorEmergencyStandbyorDeclared’.d) MaintaincommunicationswithPractitioner2.e) Leavetheignitionkeyinplaceandremainwithvehicle.f) CarryoutCommunications Officerroleuntilrelieved.
Practitioner 2:a) Carryoutascenesurvey.b) GivesituationreporttoAmbulanceControlusingMETHANE
messageformat.c) CarryoutHSE Controller of Operationsroleuntilrelieved.d) LiaisewithGardaControllerofOperationsandLocalAuthority
ControllerofOperations.e) SelectlocationforHoldingArea.f) Setupkeyareasinconjunctionwithotherprincipleresponse
agenciesonsite:–SiteControlPoint–CasualtyClearingStation–AmbulanceParkingPoint
If first on scene do not provide care or transport as this will inhibit the early and orderly organisation of on-scene command. 40
Maj Emg
41
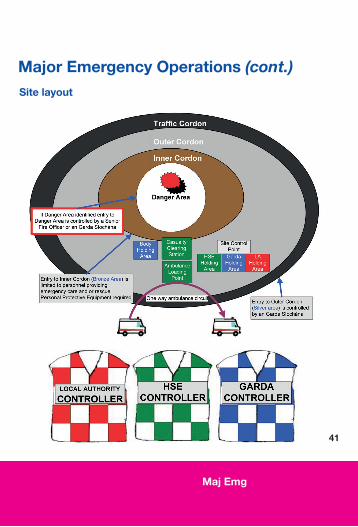
Major Emergency Operations (cont.)Site layout
Maj Emg
42
Major Emergency Operations (cont.)
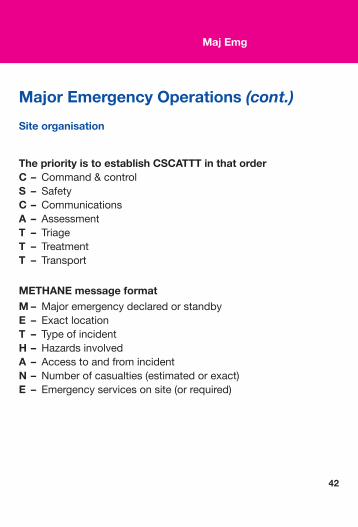
The priority is to establish CSCATTT in that order C – Command&controlS – SafetyC – CommunicationsA – AssessmentT – TriageT – TreatmentT – Transport
METHANE message format M – MajoremergencydeclaredorstandbyE – ExactlocationT – TypeofincidentH – HazardsinvolvedA – AccesstoandfromincidentN – Numberofcasualties(estimatedorexact)E – Emergencyservicesonsite(orrequired)
Site organisation
Maj Emg
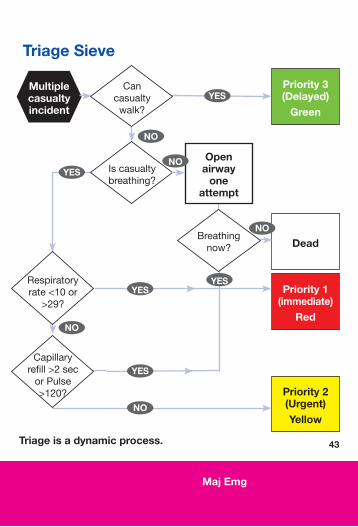
Triage Sieve
Triage is a dynamic process.
Multiple casualty incident
Cancasualtywalk?
Iscasualtybreathing?
Open airway
one attempt
Respiratoryrate<10or
>29?
Breathingnow?
Priority 3 (Delayed)
Green
Dead
Priority 1 (immediate)
Red
Priority 2 (Urgent)Yellow
NO
NO
NO
NO
YES
YES
YES
NO
43
Capillaryrefill>2secorPulse>120?
YESYES
Maj Emg
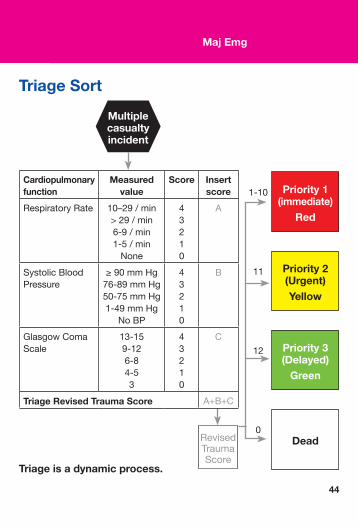
Triage Sort
RevisedTraumaScore
Priority 3 (Delayed)
Green
Dead
Priority 1 (immediate)
Red
Priority 2 (Urgent)Yellow
Triage is a dynamic process.
Cardiopulmonary function
Measured value
Score Insert score
RespiratoryRate 10–29/min>29/min6-9/min1-5/minNone
43210
A
SystolicBloodPressure
≥90mmHg76-89mmHg50-75mmHg1-49mmHg
NoBP
43210
B
GlasgowComaScale
13-159-126-84-53
43210
C
Triage Revised Trauma Score A+B+C
1-10
11
12
0
Multiple casualty incident
44
MISCELLANEOUS
46 EMSprioritydispatchprotocols49 HypodermicneedlesforIMinjection50 Oxygencylindercapacity51 Poisoncare54 RadioreportforED55 IMIST-AMBOHandoverPrototcol56 SafeAeromedicalHelicopterUsage59 Sepsis61 TreatandReferral
EMS Priority Dispatch Protocolsa) AMPDSisusedtoidentifyanappropriatechiefcomplaintcode
followingcallerinterrogationbythecalltakers.
b) Dispatchcrossreference(DCR)codesarefixedbyAMPDS andcannotbechangedastheyarelinkedtosoftwareandfield responderguide,etc.
c) AMPDShassixdesignatedresponselevels(Echo,Delta,Charlie,Bravo,AlphaandOmega),whicharelinkedtotheDCRcodes.
d) PHECCpublishedanEMSPriorityDispatchStandardwhich designatesanappropriateresponsetoeachofthesix responselevels.
e) TheresponseleveltoeachDCRcodeisagreedbyPHECC’sPriorityDispatchCommittee(PDC).
f) TheresponseforspecificDCRcodesmeetsIrishclinical standards.
g) Ambulancecontrol,whenactivatingaresponsetoanincident, willgivetheDCRcodeforinformationabouttheincidentto thePractitioners(de-emphasisingtheletterinthecode)and aPDC-agreedresponselevelofEcho,Delta,Charlie,Bravo, AlphaorOmega.
h) DCRcodesanddispatchlevelsareupdatedregularly.
46
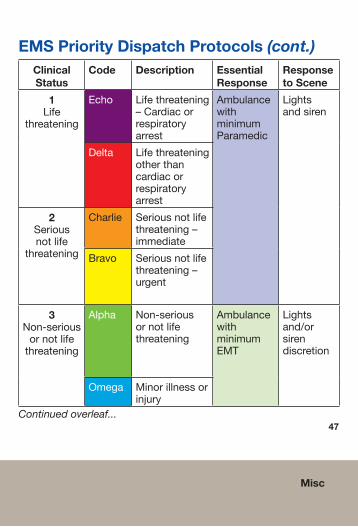
EMS Priority Dispatch Protocols (cont.)Clinical Status
Code Description Essential Response
Response to Scene
1Life
threatening
Echo Lifethreatening–Cardiacorrespiratoryarrest
AmbulancewithminimumParamedic
Lightsandsiren
Delta Lifethreateningotherthancardiacorrespiratoryarrest
2Seriousnotlife
threatening
Charlie Seriousnotlifethreatening–immediate
Bravo Seriousnotlifethreatening–urgent
3Non-seriousornotlifethreatening
Alpha Non-seriousornotlifethreatening
AmbulancewithminimumEMT
Lightsand/orsirendiscretion
Omega Minorillnessorinjury
Continued overleaf...
Misc
47
Misc
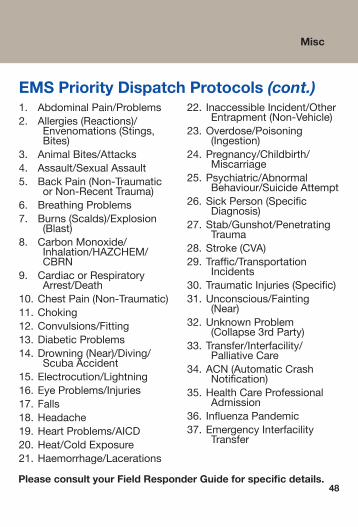
EMS Priority Dispatch Protocols (cont.)1. AbdominalPain/Problems2. Allergies(Reactions)/
Envenomations(Stings,Bites)
3. AnimalBites/Attacks4. Assault/SexualAssault5. BackPain(Non-Traumatic
orNon-RecentTrauma)6. BreathingProblems7. Burns(Scalds)/Explosion
(Blast)8. CarbonMonoxide/
Inhalation/HAZCHEM/CBRN
9. CardiacorRespiratoryArrest/Death
10.ChestPain(Non-Traumatic)11.Choking12.Convulsions/Fitting13.DiabeticProblems14.Drowning(Near)/Diving/
ScubaAccident15.Electrocution/Lightning16.EyeProblems/Injuries17.Falls18.Headache19.HeartProblems/AICD20.Heat/ColdExposure21.Haemorrhage/Lacerations
22. InaccessibleIncident/OtherEntrapment(Non-Vehicle)
23.Overdose/Poisoning(Ingestion)
24.Pregnancy/Childbirth/Miscarriage
25.Psychiatric/AbnormalBehaviour/SuicideAttempt
26.SickPerson(SpecificDiagnosis)
27.Stab/Gunshot/PenetratingTrauma
28.Stroke(CVA)29.Traffic/Transportation
Incidents30.TraumaticInjuries(Specific)31.Unconscious/Fainting
(Near)32.UnknownProblem
(Collapse3rdParty)33.Transfer/Interfacility/
PalliativeCare34.ACN(AutomaticCrash
Notification)35.HealthCareProfessional
Admission36. InfluenzaPandemic37. EmergencyInterfacility
Transfer
48Please consult your Field Responder Guide for specific details.
Misc
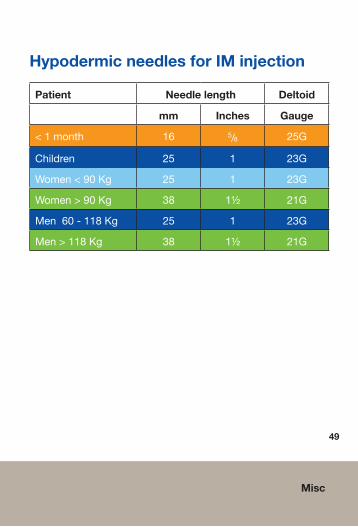
Hypodermic needles for IM injection
Patient Needle length Deltoid
mm Inches Gauge
<1month 16 5/8 25G
Children 25 1 23G
Women<90Kg 25 1 23G
Women>90Kg 38 1½ 21G
Men60-118Kg 25 1 23G
Men>118Kg 38 1½ 21G
49
Misc
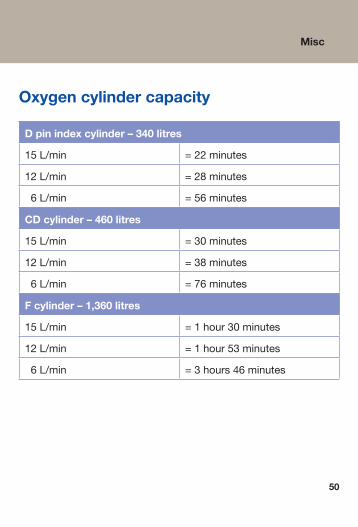
Oxygen cylinder capacity
D pin index cylinder – 340 litres
15L/min =22minutes
12L/min =28minutes
6L/min =56minutes
CD cylinder – 460 litres
15L/min =30minutes
12L/min =38minutes
6L/min =76minutes
F cylinder – 1,360 litres
15L/min =1hour30minutes
12L/min =1hour53minutes
6L/min =3hours46minutes
50
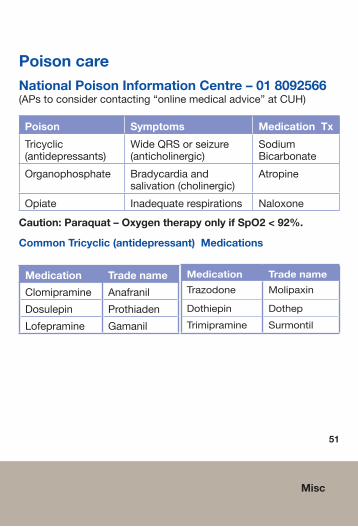
Poison careNational Poison Information Centre – 01 8092566 (APstoconsidercontacting“onlinemedicaladvice”atCUH)
Poison Symptoms Medication Tx
Tricyclic(antidepressants)
WideQRSorseizure(anticholinergic)
SodiumBicarbonate
Organophosphate Bradycardiaandsalivation(cholinergic)
Atropine
Opiate Inadequaterespirations Naloxone
Caution: Paraquat – Oxygen therapy only if SpO2 < 92%.
Common Tricyclic (antidepressant) Medications
Medication Trade name
Clomipramine Anafranil
Dosulepin Prothiaden
Lofepramine Gamanil
Medication Trade name
Trazodone Molipaxin
Dothiepin Dothep
Trimipramine Surmontil
51
Misc
Misc
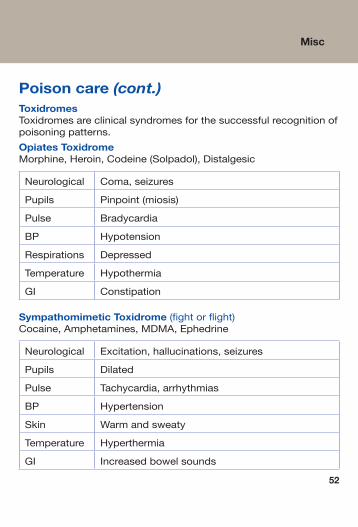
Poison care (cont.)ToxidromesToxidromesareclinicalsyndromesforthesuccessfulrecognitionofpoisoningpatterns.
Opiates ToxidromeMorphine,Heroin,Codeine(Solpadol),Distalgesic
Neurological Coma,seizures
Pupils Pinpoint(miosis)
Pulse Bradycardia
BP Hypotension
Respirations Depressed
Temperature Hypothermia
GI Constipation
Sympathomimetic Toxidrome (fightorflight)Cocaine,Amphetamines,MDMA,Ephedrine
Neurological Excitation,hallucinations,seizures
Pupils Dilated
Pulse Tachycardia,arrhythmias
BP Hypertension
Skin Warmandsweaty
Temperature Hyperthermia
GI Increasedbowelsounds
52
Misc
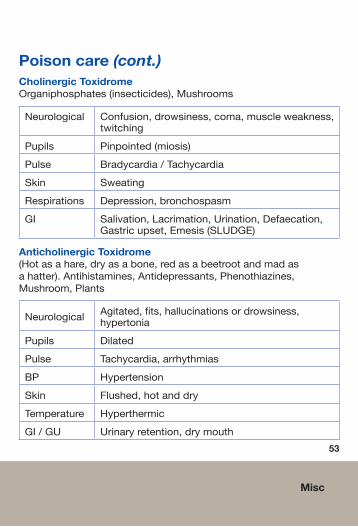
Poison care (cont.)Cholinergic ToxidromeOrganiphosphates(insecticides),Mushrooms
Neurological Confusion,drowsiness,coma,muscleweakness,twitching
Pupils Pinpointed(miosis)
Pulse Bradycardia/Tachycardia
Skin Sweating
Respirations Depression,bronchospasm
GI Salivation,Lacrimation,Urination,Defaecation,Gastricupset,Emesis(SLUDGE)
Anticholinergic Toxidrome(Hotasahare,dryasabone,redasabeetrootandmadasahatter).Antihistamines,Antidepressants,Phenothiazines,Mushroom,Plants
Neurological Agitated,fits,hallucinationsordrowsiness,hypertonia
Pupils Dilated
Pulse Tachycardia,arrhythmias
BP Hypertension
Skin Flushed,hotanddry
Temperature Hyperthermic
GI/GU Urinaryretention,drymouth
53
Misc
54
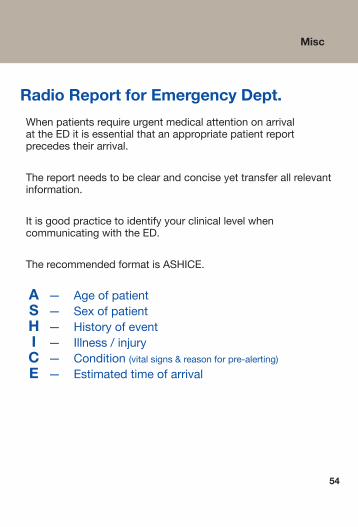
Radio Report for Emergency Dept.
WhenpatientsrequireurgentmedicalattentiononarrivalattheEDitisessentialthatanappropriatepatientreportprecedestheirarrival.
Thereportneedstobeclearandconciseyettransferallrelevantinformation.
ItisgoodpracticetoidentifyyourclinicallevelwhencommunicatingwiththeED.
TherecommendedformatisASHICE.
A — Ageofpatient S — Sexofpatient H — Historyofevent I — Illness/injury C — Condition(vitalsigns&reasonforpre-alerting) E — Estimatedtimeofarrival
Misc
55
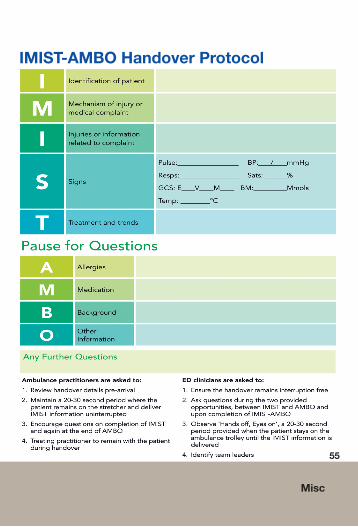
IMIST-AMBO Handover Protocol
Misc
Safe Aeromedical Helicopter Usage
TherearecurrentlytwoservicesinIrelandprovidingaeromedicaltransport,theEAS(EmergencyAeromedicalService)andtheIrishCoastGuard.
Differentaircraftareoperatedbyeachorganisation.Regardlessofthetype,thesamesafetyprecautionsmustbeadheredto.
Requesting a Helicopter: Shouldyourequirehelicopterevacuation,yourrequestshouldgotoambulancecontrol,whowillliaisewiththeNACC(NationalAeromedicalCoordinationCentre).Anaccuratepatientlocationisvitalingettingthehelicoptertoyourlocationwithminimaldelay.IfyouhaveelectedtobeginyourjourneytohospitalbyroaditisnottoolatetorequestahelicopterandtheNACCwillprovidearendezvouspointforyoutomeetthehelicopter.
Helicopter is on the way:Thepatientmustremainintheambulancewiththedoorsclosed.Ideallyyouwillhavethepatientonacarryingsheetwhichwillaidswiftloadingofthepatientontothehelicopter.Althoughitisnotyourresponsibilitytopreparealandingsite,itishelpfultoknowwhatthehelicoptercrewwillbelookingforusingthis5pointchecklist:1.Aflatareaapproximatelythesizeofhalfafootballfie (atleast50mx50m).2.Nowirescrossingthelandingarea.3.Noobviouswiresimpedingtheflightpath.4.TheLZmustbefreeoflivestockandpeople.
56
57
Safe Aeromedical Helicopter Usage...contd.
5. Ifyougetachance,walktheareaandcollectFOD (ForeignObjectDebris)suchastrafficcones,clothing,rubbish anythingthatcanbeblownupinthehelicopter’sstrong downwashandcauseahazardtothehelicopterorthose around.
Confirmthe5pointchecklistwithambulancecontrol.Sportsfieldsoftenmakeideallandingsites.
The landing:Thehelicoptercrewwillgenerallylandintowind.Whileitislandingmakesurenociviliansapproachthelandingarea.Ifsafetyandsecurityiscompromisedthecrewwillnotland.Neverapproachahelicopterunlesssignalledbythecrewtodoso.
Loading the patient:TheAPorCrewmanwillcometoyouanddecidewhethertheaircraftwillshutdownorarotors-runningloadingwilltakeplace.Ifarotors-runningloadingistotakeplacethereareanumberofhazardstoconsider.ListentothebriefgiventoyoubytheAP/Crewmanandadheretoalldirectionsinrelationtosafety,PPEetc.
Take-Off:Clinicalpersonnelshouldremainatthelandingzonefor5minutesafterthehelicopterhastakenoff,thiswayifthehelicopterdevelopsatechnicalfaultearlyintheflightthecrewcanreturntotheLZandoffloadthepatienttoyou.
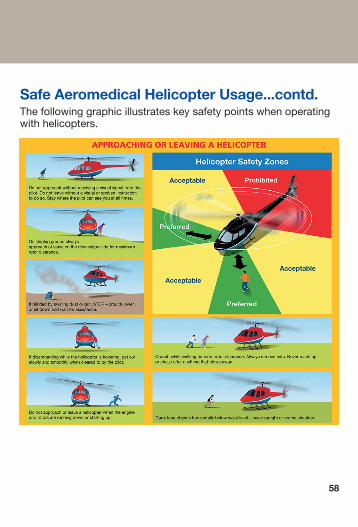
Safe Aeromedical Helicopter Usage...contd.Thefollowinggraphicillustrateskeysafetypointswhenoperatingwithhelicopters.
58
Sepsis
SIRS (Systemic inflammatory response syndrome):Theclincialsyndromethatresultsfromaderegulatedinflammatoryresponseortoanon-infectionsinsult.
Sepsis:SIRSthatissecondarytoinfectionthathasbeendisagnosedclinically.
Severe Sepsis:Sepsisplusatleastonesignofhypoperfusionororgandysfunctionthatisnewandnotexplainedbyotherknownetiologyoforgandysfunction.
Septic Shock:Severesepsisassociatedwithrefractoryhypotension(BP<90/60mmHg)despiteadequatefluidresuscitationand/orserumlactatelevel≥4.0mmol/L.
59
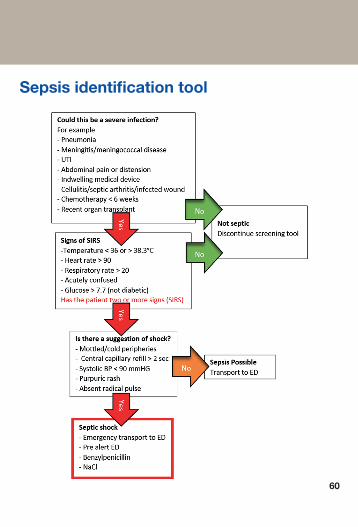
Sepsis identification tool
60
61
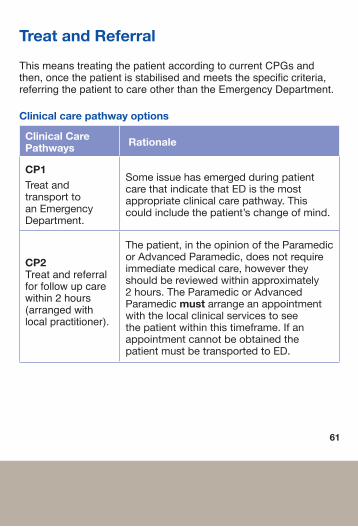
Treat and Referral
This means treating the patient according to current CPGs and then, once the patient is stabilised and meets the specific criteria, referring the patient to care other than the Emergency Department.
Clinical care pathway options
Clinical Care Pathways Rationale
CP1TreatandtransporttoanEmergencyDepartment.
SomeissuehasemergedduringpatientcarethatindicatethatEDisthemostappropriateclinicalcarepathway.Thiscouldincludethepatient’schangeofmind.
CP2Treat and referral for follow up care within 2 hours (arranged with local practitioner).
Thepatient,intheopinionoftheParamedicorAdvancedParamedic,doesnotrequireimmediatemedicalcare,howevertheyshouldbereviewedwithinapproximately2hours.TheParamedicorAdvancedParamedicmustarrangeanappointmentwiththelocalclinicalservicestoseethepatientwithinthistimeframe.IfanappointmentcannotbeobtainedthepatientmustbetransportedtoED.
Treat and Referral....contd.
Clinical care pathway options...contd
Clinical Care Pathways Rationale
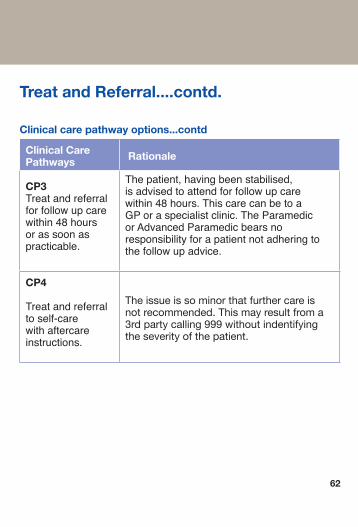
CP3Treat and referral for follow up care within 48 hours or as soon as practicable.
The patient, having been stabilised, is advised to attend for follow up care within 48 hours. This care can be to a GP or a specialist clinic. The Paramedic or Advanced Paramedic bears no responsibility for a patient not adhering to the follow up advice.
CP4
Treat and referral to self-care with aftercare instructions.
Theissueissominorthatfurthercareisnotrecommended.Thismayresultfroma3rdpartycalling999withoutindentifyingtheseverityofthepatient.
62
Treat and Referral....contd.
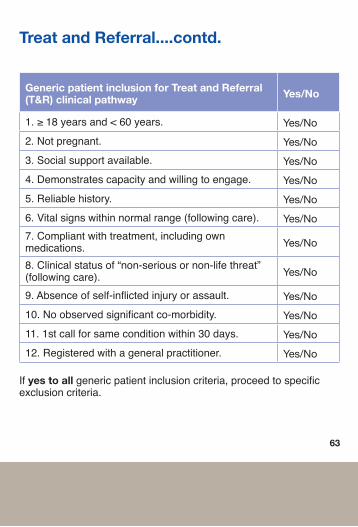
Generic patient inclusion for Treat and Referral(T&R) clinical pathway Yes/No
1. ≥ 18 years and < 60 years. Yes/No
2. Not pregnant. Yes/No
3. Social support available. Yes/No
4. Demonstrates capacity and willing to engage. Yes/No
5. Reliable history. Yes/No
6. Vital signs within normal range (following care). Yes/No
7. Compliant with treatment, including own medications. Yes/No
8. Clinical status of “non-serious or non-life threat” (following care). Yes/No
9. Absence of self-inflicted injury or assault. Yes/No
10. No observed significant co-morbidity. Yes/No
11. 1st call for same condition within 30 days. Yes/No
12. Registered with a general practitioner. Yes/No
If yes to all generic patient inclusion criteria, proceed to specific exclusion criteria.
63
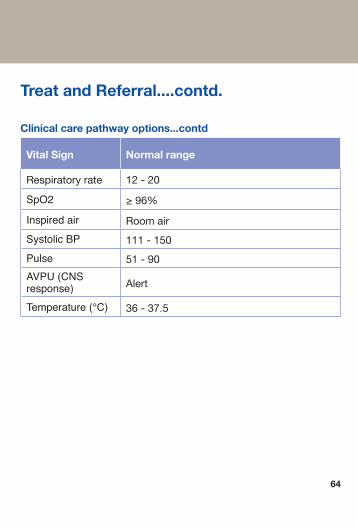
Treat and Referral....contd.
Clinical care pathway options...contd
Vital Sign Normal range
Respiratoryrate 12-20
SpO2 ≥96%
Inspired air Roomair
Systolic BP 111-150
Pulse 51-90
AVPU (CNS response) Alert
Temperature (°C) 36-37.5
64
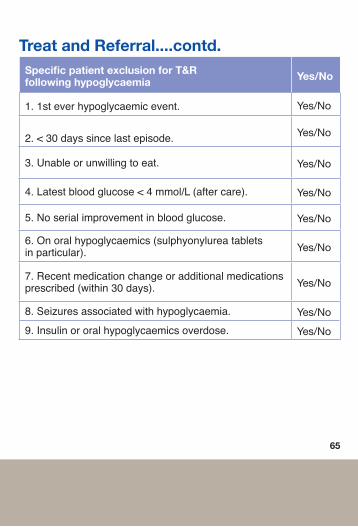
Treat and Referral....contd.Specific patient exclusion for T&R following hypoglycaemia Yes/No
1. 1st ever hypoglycaemic event. Yes/No
2. < 30 days since last episode. Yes/No
3. Unable or unwilling to eat. Yes/No
4. Latest blood glucose < 4 mmol/L (after care). Yes/No
5. No serial improvement in blood glucose. Yes/No
6. On oral hypoglycaemics (sulphyonylurea tablets in particular). Yes/No
7. Recent medication change or additional medications prescribed (within 30 days). Yes/No
8. Seizures associated with hypoglycaemia. Yes/No
9. Insulin or oral hypoglycaemics overdose. Yes/No
65
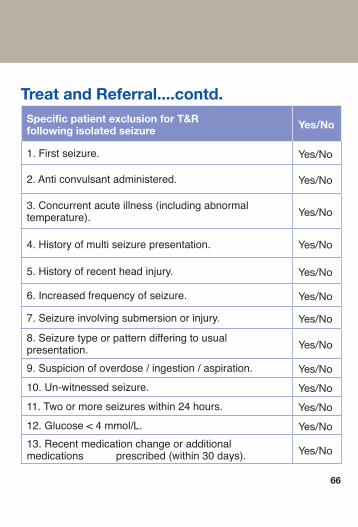
Treat and Referral....contd.Specific patient exclusion for T&R following isolated seizure Yes/No
1. First seizure. Yes/No
2. Anti convulsant administered. Yes/No
3. Concurrent acute illness (including abnormal temperature). Yes/No
4. History of multi seizure presentation. Yes/No
5. History of recent head injury. Yes/No
6. Increased frequency of seizure. Yes/No
7. Seizure involving submersion or injury. Yes/No
8. Seizure type or pattern differing to usual presentation. Yes/No
9. Suspicion of overdose / ingestion / aspiration. Yes/No
10. Un-witnessed seizure. Yes/No
11. Two or more seizures within 24 hours. Yes/No
12. Glucose < 4 mmol/L. Yes/No
13. Recent medication change or additional medications prescribed (within 30 days). Yes/No
66
MEDICATIONS
MEDICATIONS Important Medication Information 68
A Amiodarone 70 Aspirin 72 Atropine 73
B Benzylpenicillin 74
C Clopidogrel 75 Cyclizine 76
D Dextrose 77 Diazepam 80
EEnoxaparin 83 Epinephrine 84
F Fentanyl 88 Furosemide 90
G Glucagon 91 GlucoseGel 92 GlycerylTrinitrate 93
H Hartmann’sSolution 94 Hydrocortisone 95
I Ibuprofen 98 IpratropiumBromide 100
L Lidocaine 101 Lorazepam 102
MMagnesiumSulphate 103 MidazolamSolution 104 Morphine 108
N Naloxone 112 Nifedipine 116 NitrousOxide&Oxygen 117
O Ondansetron 118 Oxygen 120
P Paracetamol 122
S Salbutamol 126 SodiumBicarbonate 127 SodiumChloride0.9% 128 Syntometrine 131
T Tenecteplase 132 Ticagrelor 134 TranexamicAcid 135
Commonly Prescribed Medications 136
Important medication information Thefollowingpagescontainquickreferencesformedications.Calculationsforpaediatric doses are based on a specific concentrationofthemedication,asoutlinedonthetopofeachpage.
Theformulaforestimatingweightis
neonate: 3.5 Kg
6 months: 6 Kg
1-5 years: (age in years x 2) + 8 Kg
> 5 years: (age in years x 3) + 7 Kg.
ToconvertlbstoKg,dividelbsby2.2.
Volumesareroundeduptothenearest0.1mL.
Wherecalculationsexceedtheadultdosetheadultdoseapplies.
If other concentrations of the medication are used these specific calculations do not apply, and the Practitioner is required to make the calculations by other means.
Want (mg)
Simple Version
Have (mg)x Vol (mL) = Vol to Administer (mL)
Dose Required (mg)
Formula for medication calculation
Dose in Container (mg)x Vol of Solution (mL) = Vol to Administer (mL)
68

Notes
69
A - D
A - D
Medications
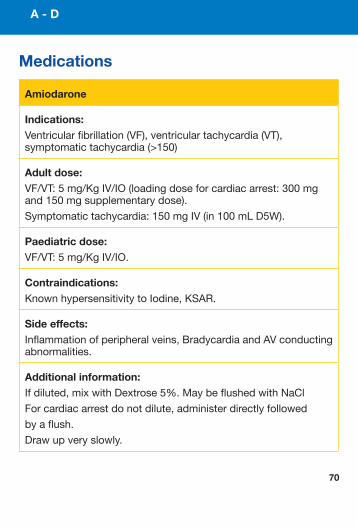
Amiodarone
Indications: Ventricularfibrillation(VF),ventriculartachycardia(VT),symptomatictachycardia(>150)
Adult dose: VF/VT:5mg/KgIV/IO(loadingdoseforcardiacarrest:300mgand150mgsupplementarydose).
Symptomatictachycardia:150mgIV(in100mLD5W).
Paediatric dose: VF/VT:5mg/KgIV/IO.
Contraindications: KnownhypersensitivitytoIodine,KSAR.
Side effects: Inflammationofperipheralveins,BradycardiaandAVconductingabnormalities.
Additional information: Ifdiluted,mixwithDextrose5%.MaybeflushedwithNaCl
Forcardiacarrestdonotdilute,administerdirectlyfollowed
byaflush.
Drawupveryslowly.
70
71
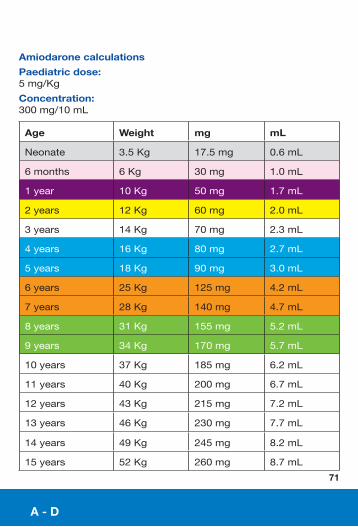
Amiodarone calculations
Paediatric dose: 5mg/Kg
Concentration: 300mg/10mL
Age Weight mg mL
Neonate 3.5Kg 17.5mg 0.6mL
6months 6Kg 30mg 1.0mL
1year 10Kg 50mg 1.7mL
2years 12Kg 60mg 2.0mL
3years 14Kg 70mg 2.3mL
4years 16Kg 80mg 2.7mL
5years 18Kg 90mg 3.0mL
6years 25Kg 125mg 4.2mL
7years 28Kg 140mg 4.7mL
8years 31Kg 155mg 5.2mL
9years 34Kg 170mg 5.7mL
10years 37Kg 185mg 6.2mL
11years 40Kg 200mg 6.7mL
12years 43Kg 215mg 7.2mL
13years 46Kg 230mg 7.7mL
14years 49Kg 245mg 8.2mL
15years 52Kg 260mg 8.7mL
A - D
A - D
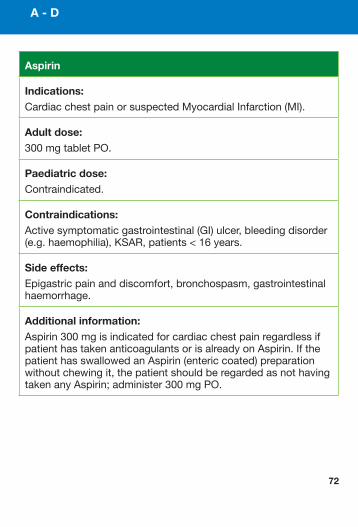
Aspirin
Indications: CardiacchestpainorsuspectedMyocardialInfarction(MI).
Adult dose: 300mgtabletPO.
Paediatric dose: Contraindicated.
Contraindications: Activesymptomaticgastrointestinal(GI)ulcer,bleedingdisorder(e.g.haemophilia),KSAR,patients<16years.
Side effects: Epigastricpainanddiscomfort,bronchospasm,gastrointestinalhaemorrhage.
Additional information: Aspirin300mgisindicatedforcardiacchestpainregardlessifpatienthastakenanticoagulantsorisalreadyonAspirin.IfthepatienthasswallowedanAspirin(entericcoated)preparationwithoutchewingit,thepatientshouldberegardedasnothavingtakenanyAspirin;administer300mgPO.
72
A - D
Atropine
Indications: Symptomaticbradycardia,Cholinergicpoisonwithbradycardiaandsalivation.
Adult dose: Cholinergicpoisonwithbradycardiaandsalivation:1mgIV.Repeatat5minintervalstoensureminimalsalivarysecretions.
SymptomaticBradycardia:0.6mg(600mcg)IV.Repeatat
3-5minintervalstoMax3mg.
Paediatric dose: Notindicated.
Contraindications: KSAR,post-cardiactransplantation.
Side effects: Tachycardia,drymouth,dilatedpupils.
Additional information: Accidentalexposuretoeyescausesblurredvision.
73
Benzylpenicillin
Indications: Severesepsis-Adult.
Suspectedorconfirmedmeningococcalsepsis-Paediatric.
Adult dose: 1,200mgIV/IO/IM.
Paediatric dose: <1yr:300mgIV/IO/IM.
1-8yrs:600mgIV/IO/IM.
>8yrs:1,200mgIV/IO/IM.
Contraindications: KSAR.
Side effects: Gastrointestinaldisturbances,hypersensitivityreactions.
Additional information: AlsocalledPenicillinG.
74
A - D
Clopidogrel
Indications: STElevationMyocardialInfarction(STEMI)ifpatientisnotsuitableforPPCI.
Adult dose: 300mgPO.
≥75years:75mgPO.
Paediatric dose: Notindicated.
Contraindications: KSAR,activepathologicalbleeding,severeliverimpairment.
Side effects: Abdominalpain,dyspepsia,diarrhoea.
Additional information:Ifapatienthasbeenloadedwithananti-plateletmedication(otherthanAspirin),priortothearrivalofthepractitioner,thepatientshouldnotbeadministeredClopidogrel.
75
A - D
A - D
76
Cyclizine
Indications: Management,preventionandtreatmentofnauseaandvomiting.
Adult dose: 50mgslowIV/IO/IM.
Paediatric dose: Notindicated.
Contraindications: KSAR.
Side effects: Tachycardia,drymouthandsedation.
A - D
77
Dextrose 5% solution
Indications: UseasadilutantforAmiodaroneinfusion
Adult dose: DiluteappropriatedoseofAmiodaronein100mLor500mL.
Paediatric dose: Notindicated.
Contraindications: KSAR.
Side effects: NecrosisoftissuearoundIVaccess.
Additional Information: ParamedicsareauthorisedtocontinuetheestablishedinfusionintheabsenceofanAdvancedParamedicordoctorduringtransportation.
A - D
78
Dextrose 10% solution
Indications: Hypoglycaemicemergency.Bloodglucose<4mmol/L.
Adult dose: 250mLIV/IOinfusion(repeatx1prn).
Paediatric dose: 5mL/KgIV/IO(repeatx1prn).
Contraindications: KSAR.
Side effects: NecrosisoftissuearoundIVaccess.
Additional information: AlsocalledGlucose.
Cannulapatencywillreducetheeffectoftissuenecrosis.
A - D
79
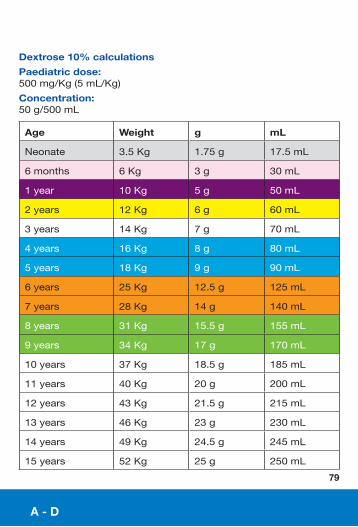
Dextrose 10% calculations
Paediatric dose: 500mg/Kg(5mL/Kg)
Concentration:50g/500mL
Age Weight g mL
Neonate 3.5Kg 1.75g 17.5mL
6months 6Kg 3g 30mL
1year 10Kg 5g 50mL
2years 12Kg 6g 60mL
3years 14Kg 7g 70mL
4years 16Kg 8g 80mL
5years 18Kg 9g 90mL
6years 25Kg 12.5g 125mL
7years 28Kg 14g 140mL
8years 31Kg 15.5g 155mL
9years 34Kg 17g 170mL
10years 37Kg 18.5g 185mL
11years 40Kg 20g 200mL
12years 43Kg 21.5g 215mL
13years 46Kg 23g 230mL
14years 49Kg 24.5g 245mL
15years 52Kg 25g 250mL
A - D
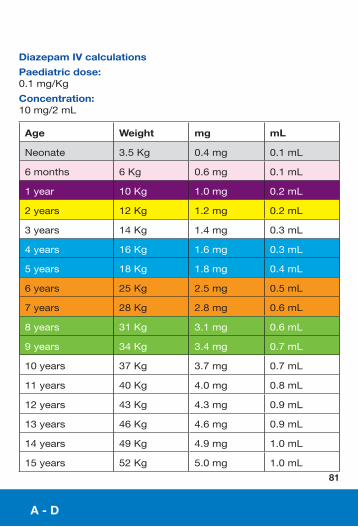
Diazepam IV
Indications: Seizure.
Adult dose: 5mgIV/IO(repeatx1prn).
Paediatric dose: 0.1mg/KgIV/IO(repeatx1prn).
Contraindications: Respiratorydepression,KSAR,shock,depressedvitalsignsoralcoholrelatedALoC.
Side effects: Hypotension,respiratorydepression,drowsinessandlight-headedness(thenextday).
Additional information: DiazepamIV/IOshouldbetitratedtoeffect.
ThemaximumdoseofDiazepamincludesthatadministeredbycarerpriortoarrivalofPractitioner.
80
A - D
Diazepam IV calculations
Paediatric dose: 0.1mg/Kg
Concentration:10mg/2mL
Age Weight mg mL
Neonate 3.5Kg 0.4mg 0.1mL
6months 6Kg 0.6mg 0.1mL
1year 10Kg 1.0mg 0.2mL
2years 12Kg 1.2mg 0.2mL
3years 14Kg 1.4mg 0.3mL
4years 16Kg 1.6mg 0.3mL
5years 18Kg 1.8mg 0.4mL
6years 25Kg 2.5mg 0.5mL
7years 28Kg 2.8mg 0.6mL
8years 31Kg 3.1mg 0.6mL
9years 34Kg 3.4mg 0.7mL
10years 37Kg 3.7mg 0.7mL
11years 40Kg 4.0mg 0.8mL
12years 43Kg 4.3mg 0.9mL
13years 46Kg 4.6mg 0.9mL
14years 49Kg 4.9mg 1.0mL
15years 52Kg 5.0mg 1.0mL
81
A - D
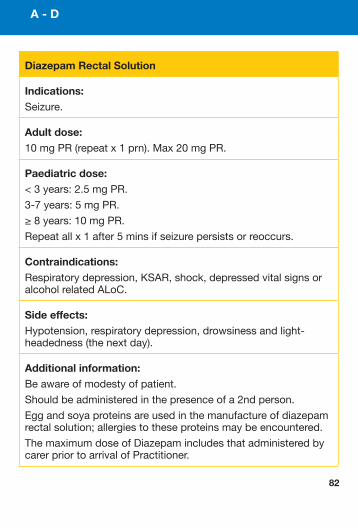
Diazepam Rectal Solution
Indications: Seizure.
Adult dose: 10mgPR(repeatx1prn).Max20mgPR.
Paediatric dose: <3years:2.5mgPR.
3-7years:5mgPR.
≥8years:10mgPR.
Repeatallx1after5minsifseizurepersistsorreoccurs.
Contraindications: Respiratorydepression,KSAR,shock,depressedvitalsignsoralcoholrelatedALoC.
Side effects: Hypotension,respiratorydepression,drowsinessandlight-headedness(thenextday).
Additional information: Beawareofmodestyofpatient.
Shouldbeadministeredinthepresenceofa2ndperson.
Eggandsoyaproteinsareusedinthemanufactureofdiazepamrectalsolution;allergiestotheseproteinsmaybeencountered.
ThemaximumdoseofDiazepamincludesthatadministeredbycarerpriortoarrivalofPractitioner.
82
83
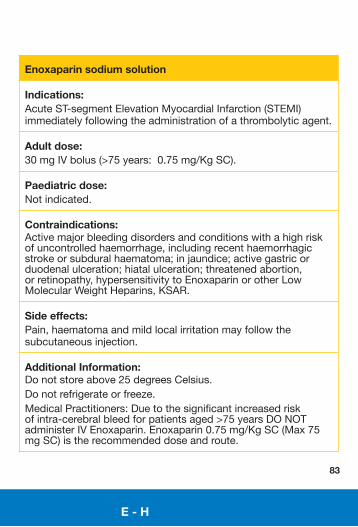
Enoxaparin sodium solution
Indications: AcuteST-segmentElevationMyocardialInfarction(STEMI)immediatelyfollowingtheadministrationofathrombolyticagent.
Adult dose: 30mgIVbolus(>75years:0.75mg/KgSC).
Paediatric dose: Notindicated.
Contraindications: Activemajorbleedingdisordersandconditionswithahighriskofuncontrolledhaemorrhage,includingrecenthaemorrhagicstrokeorsubduralhaematoma;injaundice;activegastricorduodenalulceration;hiatalulceration;threatenedabortion,orretinopathy,hypersensitivitytoEnoxaparinorotherLowMolecularWeightHeparins,KSAR.
Side effects: Pain,haematomaandmildlocalirritationmayfollowthesubcutaneousinjection.
Additional Information: Donotstoreabove25degreesCelsius.Donotrefrigerateorfreeze.MedicalPractitioners:Duetothesignificantincreasedriskofintra-cerebralbleedforpatientsaged>75yearsDONOTadministerIVEnoxaparin.Enoxaparin0.75mg/KgSC(Max75mgSC)istherecommendeddoseandroute.
E - H
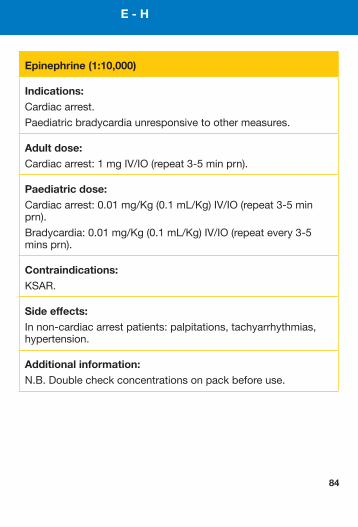
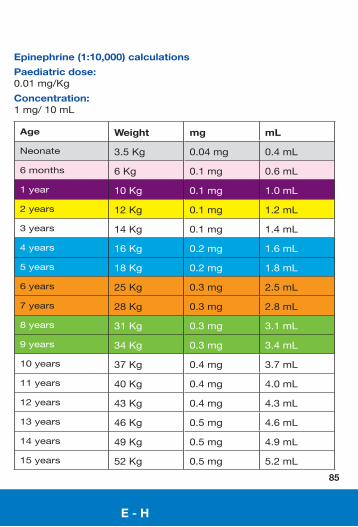
Epinephrine (1:10,000)
Indications: Cardiacarrest.
Paediatricbradycardiaunresponsivetoothermeasures.
Adult dose: Cardiacarrest:1mgIV/IO(repeat3-5minprn).
Paediatric dose: Cardiacarrest:0.01mg/Kg(0.1mL/Kg)IV/IO(repeat3-5minprn).
Bradycardia:0.01mg/Kg(0.1mL/Kg)IV/IO(repeatevery3-5minsprn).
Contraindications: KSAR.
Side effects: Innon-cardiacarrestpatients:palpitations,tachyarrhythmias,hypertension.
Additional information: N.B.Doublecheckconcentrationsonpackbeforeuse.
84
E - H
E - H
Epinephrine (1:10,000) calculations
Paediatric dose: 0.01mg/Kg
Concentration:1mg/10mL
Age Weight mg mL
Neonate 3.5Kg 0.04mg 0.4mL
6months 6Kg 0.1mg 0.6mL
1year 10Kg 0.1mg 1.0mL
2years 12Kg 0.1mg 1.2mL
3years 14Kg 0.1mg 1.4mL
4years 16Kg 0.2mg 1.6mL
5years 18Kg 0.2mg 1.8mL
6years 25Kg 0.3mg 2.5mL
7years 28Kg 0.3mg 2.8mL
8years 31Kg 0.3mg 3.1mL
9years 34Kg 0.3mg 3.4mL
10years 37Kg 0.4mg 3.7mL
11years 40Kg 0.4mg 4.0mL
12years 43Kg 0.4mg 4.3mL
13years 46Kg 0.5mg 4.6mL
14years 49Kg 0.5mg 4.9mL
15years 52Kg 0.5mg 5.2mL
85
E - H
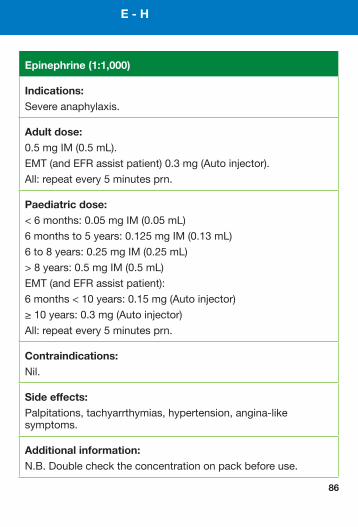
Epinephrine (1:1,000)
Indications: Severeanaphylaxis.
Adult dose: 0.5mgIM(0.5mL).
EMT(andEFRassistpatient)0.3mg(Autoinjector).
All:repeatevery5minutesprn.
Paediatric dose: <6months:0.05mgIM(0.05mL)
6monthsto5years:0.125mgIM(0.13mL)
6to8years:0.25mgIM(0.25mL)
>8years:0.5mgIM(0.5mL)
EMT(andEFRassistpatient):
6months<10years:0.15mg(Autoinjector)
≥10years:0.3mg(Autoinjector)
All:repeatevery5minutesprn.
Contraindications: Nil.
Side effects: Palpitations,tachyarrthymias,hypertension,angina-likesymptoms.
Additional information: N.B.Doublechecktheconcentrationonpackbeforeuse.
86

Notes
E - H
87
E - H
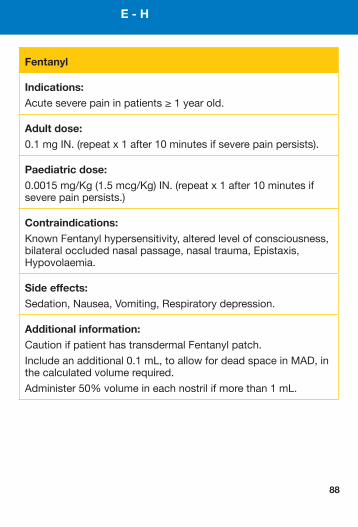
Fentanyl
Indications: Acuteseverepaininpatients≥1yearold.
Adult dose: 0.1mgIN.(repeatx1after10minutesifseverepainpersists).
Paediatric dose: 0.0015mg/Kg(1.5mcg/Kg)IN.(repeatx1after10minutesifseverepainpersists.)
Contraindications: KnownFentanylhypersensitivity,alteredlevelofconsciousness,bilateraloccludednasalpassage,nasaltrauma,Epistaxis,Hypovolaemia.
Side effects: Sedation,Nausea,Vomiting,Respiratorydepression.
Additional information: CautionifpatienthastransdermalFentanylpatch.
Includeanadditional0.1mL,toallowfordeadspaceinMAD,inthecalculatedvolumerequired.
Administer50%volumeineachnostrilifmorethan1mL.
88
89
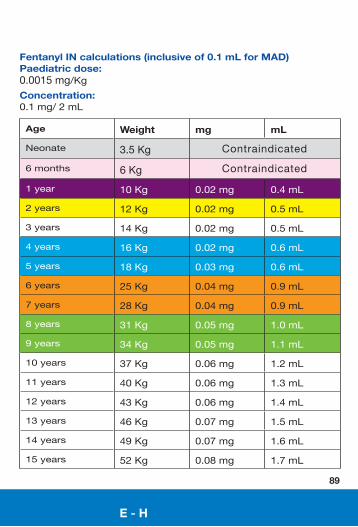
Fentanyl IN calculations (inclusive of 0.1 mL for MAD)Paediatric dose: 0.0015mg/KgConcentration:0.1mg/2mL
Age Weight mg mL
Neonate 3.5Kg
6months 6Kg
1year 10Kg 0.02mg 0.4mL
2years 12Kg 0.02mg 0.5mL
3years 14Kg 0.02mg 0.5mL
4years 16Kg 0.02mg 0.6mL
5years 18Kg 0.03mg 0.6mL
6years 25Kg 0.04mg 0.9mL
7years 28Kg 0.04mg 0.9mL
8years 31Kg 0.05mg 1.0mL
9years 34Kg 0.05mg 1.1mL
10years 37Kg 0.06mg 1.2mL
11years 40Kg 0.06mg 1.3mL
12years 43Kg 0.06mg 1.4mL
13years 46Kg 0.07mg 1.5mL
14years 49Kg 0.07mg 1.6mL
15years 52Kg 0.08mg 1.7mL
Contraindicated
Contraindicated
E - H
Furosemide injection
Indications: Pulmonaryoedema.
Adult dose: 40mgslowIV.
Paediatric dose: Notindicated.
Contraindications: Pregnancy,hypokalaemia,KSAR.
Side effects: Headache,dizziness,hypotension,arrhythmias,transientdeafness,diarrhoea,nauseaandvomiting.
Additional information: Protectfromlight.
90
E - H
91
Glucagon
Indications: HypoglycaemiainpatientsunabletotakeoralglucoseorunabletogainIVaccess,withabloodglucoselevel<4mmol/L.
Adult dose: 1mgIM.
Paediatric dose: ≤8years:0.5mgIM.
>8years:1mgIM.
Contraindications: Phaechromocytoma,KSAR.
Side effects: Rare:maycausehypotension,dizziness,headache,nauseaandvomiting.
Additional information: Maybeineffectiveinpatientswithlowstoredglycogene.g.prioruseinprevious24hours,alcoholicpatientswithliverdisease.
Storeinrefrigerator.
Protectfromlight.
E - H
E - H
92
Glucose Gel
Indications: Hypoglycaemia,bloodglucose<4mmol/L.
Adult dose: 10-20gbuccal.
Repeatprn.
Paediatric dose: ≤8years:5-10gbuccal.
>8years:10-20gbuccal.
Repeatprn.
Contraindications: KSAR.
Side effects: Maycausevomitinginpatientsunder5ifadministeredtooquickly.
Additional information: Glucosegelwillmaintainglucoselevelsonceraisedbutshouldbeusedsecondarytodextrosetoreversehypoglycaemia.
Proceed with caution: Patientswithairwaycompromise.Alteredlevelofconsciousness.
93
Glyceryl Trinitrate
Indications: Angina,suspectedMyocardialInfarction(MI),AdvancedParamedicandParamedic-pulmonaryoedema.
Adult dose: AnginaorMI:0.4mgsublingual
(repeat3-5minprn,toMax1.2mg).
Pulmonaryoedema:0.8mgsublingual(repeatx1prn).
Paediatric dose: Notindicated.
Contraindications: SBP<90mmHg,Viagraorotherphosphodiesterasetype5inhibitors(Sildenafil,TadalafilandVardenafil)usedwithinprevious24hours,KSAR.
Side effects: Headache,transienthypotension,flushing,dizziness.
Additional information: Ifthepumpisneworhasnotbeenusedforaweekormore,thefirstsprayshouldbereleasedintotheair.
E - H
94
Hartmann’s Solution
Indications: WhenNaClisunavailableitmaybesubstitutedwithHartmann’sSolutionIV/IO,exceptforcrushinjuries,burns,renalfailureandhyperglycaemia.
Adult dose: SeeNaCl.
Paediatric dose: SeeNaCl.
Contraindications: KSAR.
Side effects: Ifadministeredinlargeamountsmaycauseoedema.
Additional information: Observecautionwithpatientswithhistoryofheartfailure.AlsocalledSodiumLactateIntravenousSolutionorCompoundRingerLactateSolutionforInjection.Warmfluidspriortoadministrationifpossible.
E - H
Hydrocortisone
Indications: Severeorrecurrentanaphylacticreactions.AsthmarefractorytoSalbutamolandIpratropiumBromide.ExacerbationofCOPD(AP).
Adrenalinsufficiency(P).
Adult dose: AnaphylacticreactionandexacerbationofCOPD(AP):200mgIV(infusionin100mLNaCl)orIM.Asthma(AP):100mgIV(infusionin100mLNaCl).Adrenalinsufficiency(P&AP):100mgIV(infusionin100mLNaCl)orIM.
Paediatric dose: Anaphylacticreaction(AP):<1year:25mgIV(infusionin100mLNaCl)orIM.1to5years:50mgIV(infusionin100mLNaCl)orIM.>5years:100mgIV(infusionin100mLNaCl)orIM.
Asthma(AP):
<1year:25mgIV(infusionin100mLNaCl).
1to5years:50mgIV(infusionin100mLNaCl).
>5years:100mgIV(infusionin100mLNaCl).Adrenalinsufficiency(P&AP):6monthsto≤5years:50mgIV(AP)(infusionin100mLNaCl)orIM(P).>5years:100mgIV(AP)(infusionin100mLNaCl)orIM(P).
95
E - H
Hydrocortisone ...contd
Contraindications: Nomajorcontraindicationsinacutemanagementofanaphylaxis.
Side effects: CCF,hypertension,abdominaldistension,vertigo,headache,nausea,malaise,hiccups.
Additional information: Intramuscularinjectionshouldavoidthedeltoidareabecauseofthepossibilityoftissueatrophy.
Dosageshouldnotbelessthan25mg.
IVisthepreferredrouteforadrenalcrisis.
96
E - H
97
Notes
I - N
I - NI - N
Ibuprofen
Indications: Mildtomoderatepain.
Adult dose: 400mgPO.
Paediatric dose: 10mg/KgPO.
Contraindications: Notsuitableforchildrenunder3months,patientwithhistoryofasthmaexacerbatedbyAspirin,pregnancy,pepticulcerdisease,KSAR.
Side effects: Skinrashes,gastrointestinalintoleranceandbleeding.
Additional information: IfIbuprofenadministeredinprevious6hours,adjustthedosedownwardbytheamountgivenbyothersourcesresultinginamaximumof10mg/Kg.
Cautionwithsignificantburnsorpoorperfusionduetoriskofkidneyfailure.
CautionifconcurrentNSAIDsuse.
98
I - N
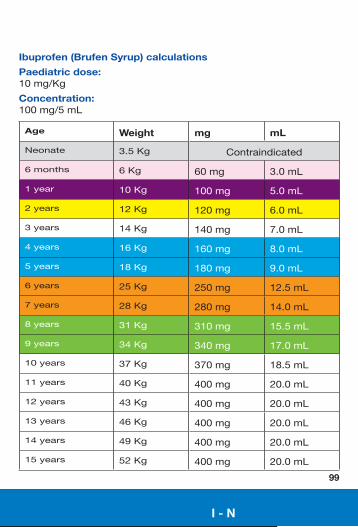
Ibuprofen (Brufen Syrup) calculations
Paediatric dose: 10mg/Kg
Concentration: 100mg/5mL
Age Weight mg mL
Neonate 3.5Kg Contraindicated
6months 6Kg 60mg 3.0mL
1year 10Kg 100mg 5.0mL
2years 12Kg 120mg 6.0mL
3years 14Kg 140mg 7.0mL
4years 16Kg 160mg 8.0mL
5years 18Kg 180mg 9.0mL
6years 25Kg 250mg 12.5mL
7years 28Kg 280mg 14.0mL
8years 31Kg 310mg 15.5mL
9years 34Kg 340mg 17.0mL
10years 37Kg 370mg 18.5mL
11years 40Kg 400mg 20.0mL
12years 43Kg 400mg 20.0mL
13years 46Kg 400mg 20.0mL
14years 49Kg 400mg 20.0mL
15years 52Kg 400mg 20.0mL
99
I - N
I - N
Ipratropium Bromide
Indications: AcutemoderateasthmaorexacerbationofCOPDnotrespondingtoinitialSalbutamoldose.
Adult dose: 0.5mgNEB.
Paediatric dose: <12years:0.25mgNEB.
≥12years:0.5mgNEB.
Contraindications: KSAR.
Side effects: Transientdrymouth,blurredvision,tachycardia,headache.
100
Lidocaine
Indications: WhenAmiodaroneisunavailableitmaybesubstitutedwithLidocaineforVF/VTarrests.
Adult dose: 1-1.5mg/KgIV/IO(Max:3mg/Kg).
Paediatric dose: Notindicated.
Contraindications: Nocontraindicationsforcardiacarrest.
Side effects: Drowsiness,dizziness,twitching,paraesthesia,convulsions,bradycardia,respiratorydepression.
Additional information: LidocainemaynotbeadministeredifAmiodaronehasbeenadministered.
101
I - N
I - N
Lorazepam
Indications: Combativewithhallucinationsorparanoiaandrisktoselforothers.
Adult dose: 2mgPO.
Paediatric dose: Notindicated.
Contraindications: Historyofsensitivitytobenzodiazepines,severehepaticorpulmonaryinsufficiency,suspectedsignificantalcoholand/orsedativesingested,KSAR.
Side effects: Drowsiness,confusion,headache,dizziness,blurredvisionandnausea/vomiting.
Onrareoccasions–hypotension,hypertension.
102
I - N
Magnesium Sulphate Injection
Indications: Torsadesdepointes,persistentbronchospasm,seizureassociatedwitheclampsia.
Adult dose: Pulselesstorsadesdepoints:2gIV/IO.
Torsadesdepointes:2gIV(infusionin100mLNaCl).
Persistentbronchospasm:2gIV(infusionin100mLNaCl).
Seizureassociatedwithpre-eclampsia:4gIV(infusionin100mLNaCl).
Paediatric dose: Notindicated.
Contraindications: Noneincardiacarrest,KSAR.
Side effects: Decreaseddeep-tendonreflexes,respiratorydepression,bradycardia,hypothermia.
103
I - N
Indications: Seizures,combativewithhallucinationsorparanoiaandrisktoselforothers.
Adult dose: Seizureorcombativepatient:2.5mgIV/IO(AP)or5mgIMor10mgbuccalor5mgintranasal(P&AP).(repeatx1prn).Paramedic:IM,buccalorINonly.
Paediatric dose: Seizure:<1year:2.5mgbuccal1yearto<5years:5mgbuccal5yearsto<10years:7.5mgbuccal≥10years:10mgbuccal.or0.2mg/Kgintranasalor0.1mg/KgIV/IO.(repeatx1prn).Paramedic:buccalorINonly.
Contraindications: Shock,depressedvitalsignsoralcohol-relatedALoC,respiratorydepression,KSAR.
Side effects: Respiratorydepression,headache,hypotension,drowsiness.
Additional information: MidazolamIVshouldbetitratedtoeffect.Ensureoxygenandresuscitationequipmentareavailablepriortoadministration.Nomorethantwodosesbypractitioners.Practitionersshouldtakeintoaccountthedoseadministeredbycarerspriortoarrivalofpractitioner.Contraindications,otherthanKSAR,refertononseizingpatients.
Midazolam Solution
104
105
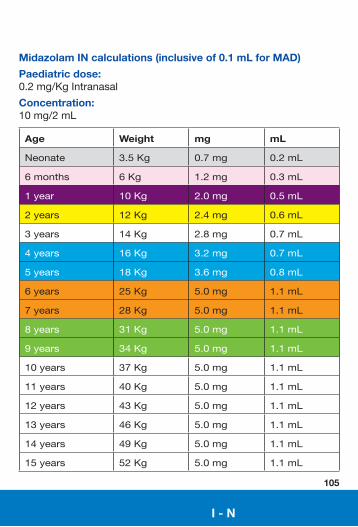
Midazolam IN calculations (inclusive of 0.1 mL for MAD)
Paediatric dose: 0.2mg/KgIntranasal
Concentration: 10mg/2mL
Age Weight mg mL
Neonate 3.5Kg 0.7mg 0.2mL
6months 6Kg 1.2mg 0.3mL
1year 10Kg 2.0mg 0.5mL
2years 12Kg 2.4mg 0.6mL
3years 14Kg 2.8mg 0.7mL
4years 16Kg 3.2mg 0.7mL
5years 18Kg 3.6mg 0.8mL
6years 25Kg 5.0mg 1.1mL
7years 28Kg 5.0mg 1.1mL
8years 31Kg 5.0mg 1.1mL
9years 34Kg 5.0mg 1.1mL
10years 37Kg 5.0mg 1.1mL
11years 40Kg 5.0mg 1.1mL
12years 43Kg 5.0mg 1.1mL
13years 46Kg 5.0mg 1.1mL
14years 49Kg 5.0mg 1.1mL
15years 52Kg 5.0mg 1.1mL
I - N
I - N
106
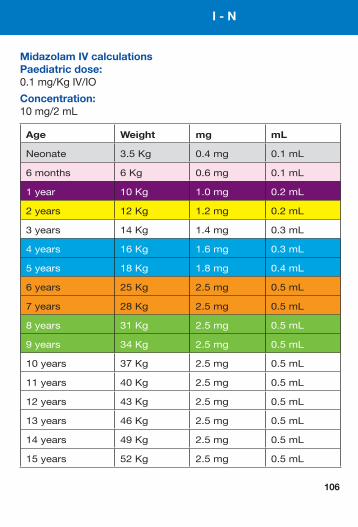
Midazolam IV calculationsPaediatric dose: 0.1mg/KgIV/IO
Concentration: 10mg/2mL
Age Weight mg mL
Neonate 3.5Kg 0.4mg 0.1mL
6months 6Kg 0.6mg 0.1mL
1year 10Kg 1.0mg 0.2mL
2years 12Kg 1.2mg 0.2mL
3years 14Kg 1.4mg 0.3mL
4years 16Kg 1.6mg 0.3mL
5years 18Kg 1.8mg 0.4mL
6years 25Kg 2.5mg 0.5mL
7years 28Kg 2.5mg 0.5mL
8years 31Kg 2.5mg 0.5mL
9years 34Kg 2.5mg 0.5mL
10years 37Kg 2.5mg 0.5mL
11years 40Kg 2.5mg 0.5mL
12years 43Kg 2.5mg 0.5mL
13years 46Kg 2.5mg 0.5mL
14years 49Kg 2.5mg 0.5mL
15years 52Kg 2.5mg 0.5mL

I - N
107
Notes
I - N
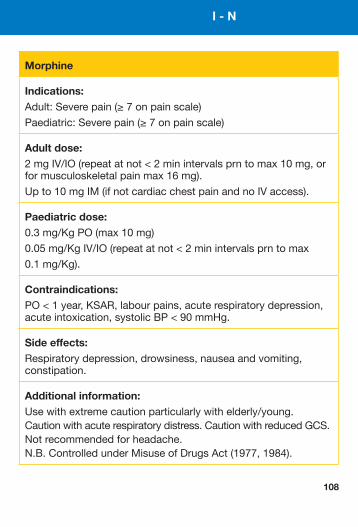
Morphine
Indications: Adult:Severepain(≥7onpainscale)
Paediatric:Severepain(≥7onpainscale)
Adult dose: 2mgIV/IO(repeatatnot<2minintervalsprntomax10mg,orformusculoskeletalpainmax16mg).
Upto10mgIM(ifnotcardiacchestpainandnoIVaccess).
Paediatric dose: 0.3mg/KgPO(max10mg)
0.05mg/KgIV/IO(repeatatnot<2minintervalsprntomax
0.1mg/Kg).
Contraindications: PO<1year,KSAR,labourpains,acuterespiratorydepression,acuteintoxication,systolicBP<90mmHg.
Side effects: Respiratorydepression,drowsiness,nauseaandvomiting,constipation.
Additional information: Usewithextremecautionparticularlywithelderly/young.Cautionwithacuterespiratorydistress.CautionwithreducedGCS.Notrecommendedforheadache.N.B.ControlledunderMisuseofDrugsAct(1977,1984).
108
I - N
109
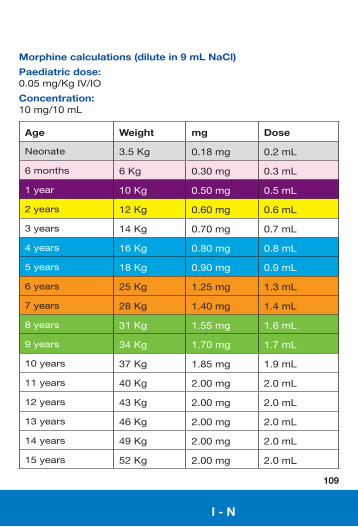
Morphine calculations (dilute in 9 mL NaCl)
Paediatric dose: 0.05mg/KgIV/IO
Concentration: 10mg/10mL
Age Weight mg Dose
Neonate 3.5Kg 0.18mg 0.2mL
6months 6Kg 0.30mg 0.3mL
1year 10Kg 0.50mg 0.5mL
2years 12Kg 0.60mg 0.6mL
3years 14Kg 0.70mg 0.7mL
4years 16Kg 0.80mg 0.8mL
5years 18Kg 0.90mg 0.9mL
6years 25Kg 1.25mg 1.3mL
7years 28Kg 1.40mg 1.4mL
8years 31Kg 1.55mg 1.6mL
9years 34Kg 1.70mg 1.7mL
10years 37Kg 1.85mg 1.9mL
11years 40Kg 2.00mg 2.0mL
12years 43Kg 2.00mg 2.0mL
13years 46Kg 2.00mg 2.0mL
14years 49Kg 2.00mg 2.0mL
15years 52Kg 2.00mg 2.0mL
I - N
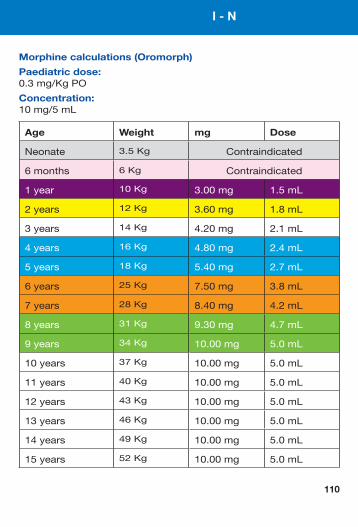
Morphine calculations (Oromorph)
Paediatric dose: 0.3mg/KgPO
Concentration: 10mg/5mL
Age Weight mg Dose
Neonate 3.5Kg Contraindicated
6months 6Kg Contraindicated
1year 10Kg 3.00mg 1.5mL
2years 12Kg 3.60mg 1.8mL
3years 14Kg 4.20mg 2.1mL
4years 16Kg 4.80mg 2.4mL
5years 18Kg 5.40mg 2.7mL
6years 25Kg 7.50mg 3.8mL
7years 28Kg 8.40mg 4.2mL
8years 31Kg 9.30mg 4.7mL
9years 34Kg 10.00mg 5.0mL
10years 37Kg 10.00mg 5.0mL
11years 40Kg 10.00mg 5.0mL
12years 43Kg 10.00mg 5.0mL
13years 46Kg 10.00mg 5.0mL
14years 49Kg 10.00mg 5.0mL
15years 52Kg 10.00mg 5.0mL
110

I - N
111
Notes
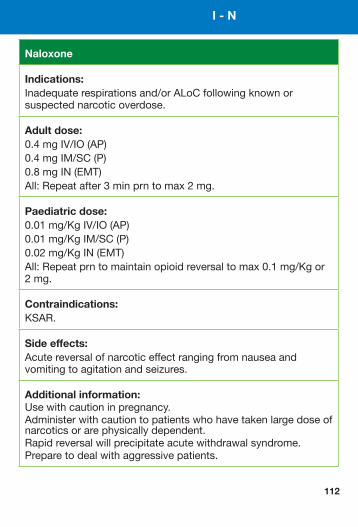
Naloxone
Indications: Inadequaterespirationsand/orALoCfollowingknownorsuspectednarcoticoverdose.
Adult dose: 0.4mgIV/IO(AP)0.4mgIM/SC(P)0.8mgIN(EMT)All:Repeatafter3minprntomax2mg.
Paediatric dose: 0.01mg/KgIV/IO(AP)0.01mg/KgIM/SC(P)0.02mg/KgIN(EMT)All:Repeatprntomaintainopioidreversaltomax0.1mg/Kgor2mg.
Contraindications: KSAR.
Side effects: Acutereversalofnarcoticeffectrangingfromnauseaandvomitingtoagitationandseizures.
Additional information: Usewithcautioninpregnancy.Administerwithcautiontopatientswhohavetakenlargedoseofnarcoticsorarephysicallydependent.Rapidreversalwillprecipitateacutewithdrawalsyndrome.Preparetodealwithaggressivepatients.
112
I - N
113
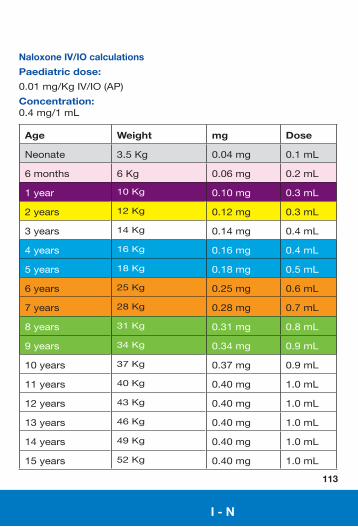
Naloxone IV/IO calculations
Paediatric dose:
0.01mg/KgIV/IO(AP)
Concentration: 0.4mg/1mL
Age Weight mg Dose
Neonate 3.5Kg 0.04mg 0.1mL
6months 6Kg 0.06mg 0.2mL
1year 10Kg 0.10mg 0.3mL
2years 12Kg 0.12mg 0.3mL
3years 14Kg 0.14mg 0.4mL
4years 16Kg 0.16mg 0.4mL
5years 18Kg 0.18mg 0.5mL
6years 25Kg 0.25mg 0.6mL
7years 28Kg 0.28mg 0.7mL
8years 31Kg 0.31mg 0.8mL
9years 34Kg 0.34mg 0.9mL
10years 37Kg 0.37mg 0.9mL
11years 40Kg 0.40mg 1.0mL
12years 43Kg 0.40mg 1.0mL
13years 46Kg 0.40mg 1.0mL
14years 49Kg 0.40mg 1.0mL
15years 52Kg 0.40mg 1.0mL
I - N
114
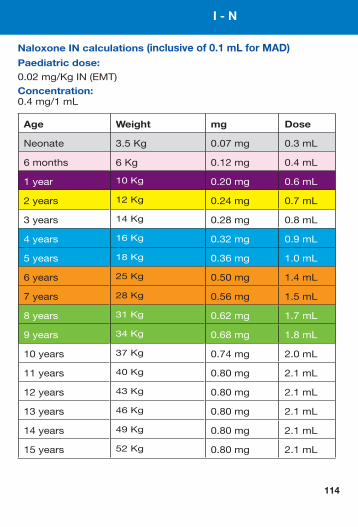
Naloxone IN calculations (inclusive of 0.1 mL for MAD)Paediatric dose: 0.02mg/KgIN(EMT)
Concentration: 0.4mg/1mL
Age Weight mg Dose
Neonate 3.5Kg 0.07mg 0.3mL
6months 6Kg 0.12mg 0.4mL
1year 10Kg 0.20mg 0.6mL
2years 12Kg 0.24mg 0.7mL
3years 14Kg 0.28mg 0.8mL
4years 16Kg 0.32mg 0.9mL
5years 18Kg 0.36mg 1.0mL
6years 25Kg 0.50mg 1.4mL
7years 28Kg 0.56mg 1.5mL
8years 31Kg 0.62mg 1.7mL
9years 34Kg 0.68mg 1.8mL
10years 37Kg 0.74mg 2.0mL
11years 40Kg 0.80mg 2.1mL
12years 43Kg 0.80mg 2.1mL
13years 46Kg 0.80mg 2.1mL
14years 49Kg 0.80mg 2.1mL
15years 52Kg 0.80mg 2.1mL
I - N
115
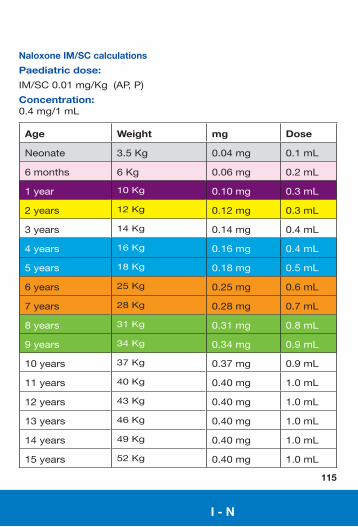
Naloxone IM/SC calculations
Paediatric dose:
IM/SC0.01mg/Kg(AP,P)
Concentration: 0.4mg/1mL
Age Weight mg Dose
Neonate 3.5Kg 0.04mg 0.1mL
6months 6Kg 0.06mg 0.2mL
1year 10Kg 0.10mg 0.3mL
2years 12Kg 0.12mg 0.3mL
3years 14Kg 0.14mg 0.4mL
4years 16Kg 0.16mg 0.4mL
5years 18Kg 0.18mg 0.5mL
6years 25Kg 0.25mg 0.6mL
7years 28Kg 0.28mg 0.7mL
8years 31Kg 0.31mg 0.8mL
9years 34Kg 0.34mg 0.9mL
10years 37Kg 0.37mg 0.9mL
11years 40Kg 0.40mg 1.0mL
12years 43Kg 0.40mg 1.0mL
13years 46Kg 0.40mg 1.0mL
14years 49Kg 0.40mg 1.0mL
15years 52Kg 0.40mg 1.0mL
I - N
I - N
116
Nifedipine
Indications: Prolapsedcord.
Adult dose:20mgPO.
Paediatric dose: Notindicated.
Contraindications: Hypotension,KSAR.
Side effects: Hypotension,headache,bradycardia,nausea&vomiting
Additional information: ClosemonitoringofmaternalpulseandBPisrequiredandcontinuousfoetalmonitoringshouldbecarriedoutifpossible.
O - T
117
Nitrous Oxide 50% & Oxygen 50%
Indications: Painrelief.
Adult dose: Self-administereduntilpainrelieved.
Paediatric dose: Self-administereduntilpainrelieved.
Contraindications: ALoC,chestinjury/pneumothorax,shock,recentscubadive,decompressionsickness,intestinalobstruction,inhalationinjury,carbonmonoxidepoisoning,KSAR.
Side effects: Disinhibition,decreasedlevelsofconsciousness,lightheadedness.
Additional information: Donotuseifpatientunabletounderstandinstructions.Incoldtemperatureswarmcylinderandinverttoensuremixofgases.AdvancedParamedicsmayusediscretionwithminorchestinjuries.Brandname:Entonox®.Hasanaddictiveproperty.CautionwhenusingEntonoxforgreaterthanonehourforSickleCellCrisis.
O - T
O - TO - T
118
Ondansetron
Indications: Management,preventionandtreatmentofnauseaandvomiting.
Adult dose:4mgslowIV.
Paediatric dose: 0.1mg/KgIVslowlytoMaxof4mg.
Contraindications: KSAR.
Side effects: Headache,sensationofwarmth,flushing,hiccups.
O - TO - T
119
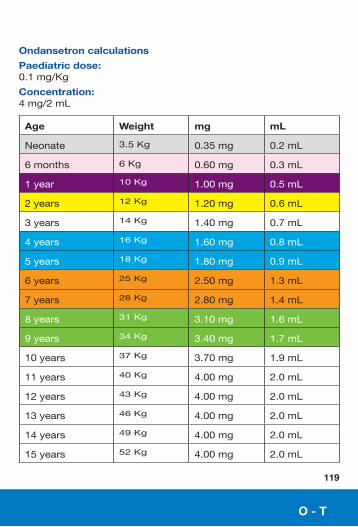
Ondansetron calculations
Paediatric dose: 0.1mg/Kg
Concentration: 4mg/2mL
Age Weight mg mL
Neonate 3.5Kg 0.35mg 0.2mL
6months 6Kg 0.60mg 0.3mL
1year 10Kg 1.00mg 0.5mL
2years 12Kg 1.20mg 0.6mL
3years 14Kg 1.40mg 0.7mL
4years 16Kg 1.60mg 0.8mL
5years 18Kg 1.80mg 0.9mL
6years 25Kg 2.50mg 1.3mL
7years 28Kg 2.80mg 1.4mL
8years 31Kg 3.10mg 1.6mL
9years 34Kg 3.40mg 1.7mL
10years 37Kg 3.70mg 1.9mL
11years 40Kg 4.00mg 2.0mL
12years 43Kg 4.00mg 2.0mL
13years 46Kg 4.00mg 2.0mL
14years 49Kg 4.00mg 2.0mL
15years 52Kg 4.00mg 2.0mL
O - TO - T
120
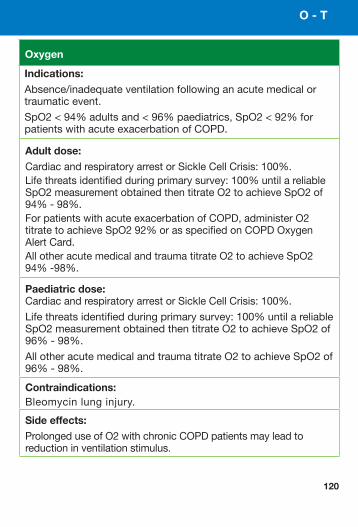
Oxygen
Adult dose: CardiacandrespiratoryarrestorSickleCellCrisis:100%.Lifethreatsidentifiedduringprimarysurvey:100%untilareliableSpO2measurementobtainedthentitrateO2toachieveSpO2of94%-98%.ForpatientswithacuteexacerbationofCOPD,administerO2titratetoachieveSpO292%orasspecifiedonCOPDOxygenAlertCard.AllotheracutemedicalandtraumatitrateO2toachieveSpO294%-98%.
Paediatric dose: CardiacandrespiratoryarrestorSickleCellCrisis:100%.
Lifethreatsidentifiedduringprimarysurvey:100%untilareliableSpO2measurementobtainedthentitrateO2toachieveSpO2of96%-98%.
AllotheracutemedicalandtraumatitrateO2toachieveSpO2of96%-98%.
Contraindications: Bleomycinlunginjury.
Side effects: ProlongeduseofO2withchronicCOPDpatientsmayleadtoreductioninventilationstimulus.
Indications: Absence/inadequateventilationfollowinganacutemedicalortraumaticevent.
SpO2<94%adultsand<96%paediatrics,SpO2<92%forpatientswithacuteexacerbationofCOPD.
O - T
121
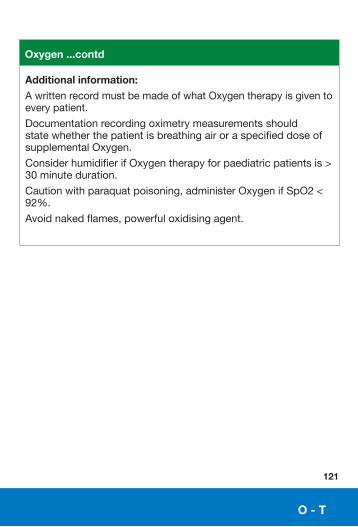
Oxygen ...contd
Additional information: AwrittenrecordmustbemadeofwhatOxygentherapyisgiventoeverypatient.
DocumentationrecordingoximetrymeasurementsshouldstatewhetherthepatientisbreathingairoraspecifieddoseofsupplementalOxygen.
ConsiderhumidifierifOxygentherapyforpaediatricpatientsis>30minuteduration.
Cautionwithparaquatpoisoning,administerOxygenifSpO2<92%.
Avoidnakedflames,powerfuloxidisingagent.
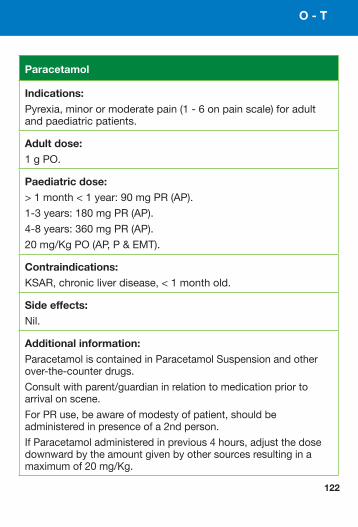
Paracetamol
Indications: Pyrexia,minorormoderatepain(1-6onpainscale)foradultandpaediatricpatients.
Adult dose: 1gPO.
Paediatric dose: >1month<1year:90mgPR(AP).
1-3years:180mgPR(AP).
4-8years:360mgPR(AP).
20mg/KgPO(AP,P&EMT).
Contraindications: KSAR,chronicliverdisease,<1monthold.
Side effects: Nil.
Additional information: ParacetamoliscontainedinParacetamolSuspensionandotherover-the-counterdrugs.
Consultwithparent/guardianinrelationtomedicationpriortoarrivalonscene.
ForPRuse,beawareofmodestyofpatient,shouldbeadministeredinpresenceofa2ndperson.
IfParacetamoladministeredinprevious4hours,adjustthedosedownwardbytheamountgivenbyothersourcesresultinginamaximumof20mg/Kg.
O - T
122
123
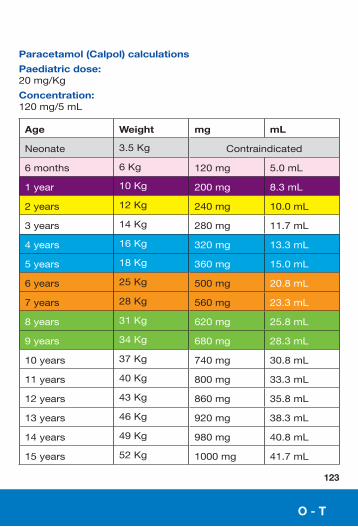
Paracetamol (Calpol) calculations
Paediatric dose: 20mg/Kg
Concentration: 120mg/5mL
Age Weight mg mL
Neonate 3.5Kg Contraindicated
6months 6Kg 120mg 5.0mL
1year 10Kg 200mg 8.3mL
2years 12Kg 240mg 10.0mL
3years 14Kg 280mg 11.7mL
4years 16Kg 320mg 13.3mL
5years 18Kg 360mg 15.0mL
6years 25Kg 500mg 20.8mL
7years 28Kg 560mg 23.3mL
8years 31Kg 620mg 25.8mL
9years 34Kg 680mg 28.3mL
10years 37Kg 740mg 30.8mL
11years 40Kg 800mg 33.3mL
12years 43Kg 860mg 35.8mL
13years 46Kg 920mg 38.3mL
14years 49Kg 980mg 40.8mL
15years 52Kg 1000mg 41.7mL
O - T

Paracetamol 6+
Indications: Pyrexia,minorormoderatepain(1-6onpainscale)foradultandpaediatricpatients.
Adult dose: 1gPO
Paediatric dose: 20mg/KgPO(AP,PandEMT).
Contraindications: KSAR,chronicliverdisease,<1monthold.
Side effects: Nil.
Additional information: ParacetamoliscontainedinParacetamolSuspensionandotherover-the-counterdrugs.
Consultwithparent/guardianinrelationtomedicationpriortoarrivalonscene.
IfParacetamoladministeredinprevious4hours,adjustthedosedownwardbytheamountgivenbyothersourcesresultinginamaximumof20mg/Kg.
124
O - T
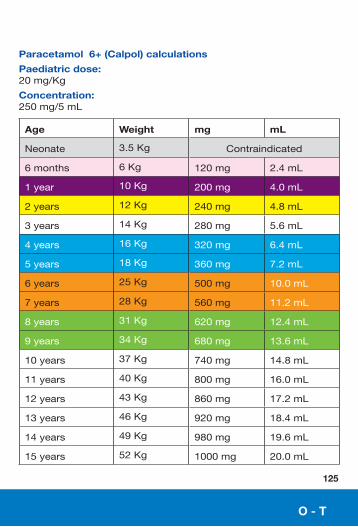
Paracetamol 6+ (Calpol) calculations
Paediatric dose: 20mg/Kg
Concentration: 250mg/5mL
Age Weight mg mL
Neonate 3.5Kg Contraindicated
6months 6Kg 120mg 2.4mL
1year 10Kg 200mg 4.0mL
2years 12Kg 240mg 4.8mL
3years 14Kg 280mg 5.6mL
4years 16Kg 320mg 6.4mL
5years 18Kg 360mg 7.2mL
6years 25Kg 500mg 10.0mL
7years 28Kg 560mg 11.2mL
8years 31Kg 620mg 12.4mL
9years 34Kg 680mg 13.6mL
10years 37Kg 740mg 14.8mL
11years 40Kg 800mg 16.0mL
12years 43Kg 860mg 17.2mL
13years 46Kg 920mg 18.4mL
14years 49Kg 980mg 19.6mL
15years 52Kg 1000mg 20.0mL
125
O - T
126
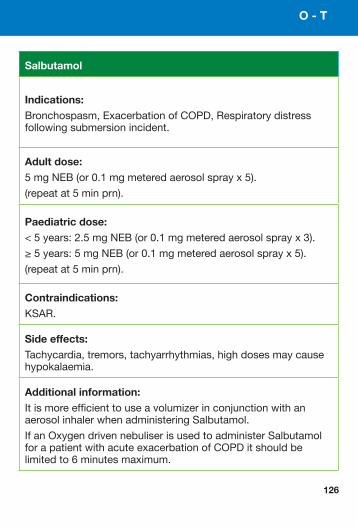
Salbutamol
Indications: Bronchospasm,ExacerbationofCOPD,Respiratorydistressfollowingsubmersionincident.
Adult dose: 5mgNEB(or0.1mgmeteredaerosolsprayx5).
(repeatat5minprn).
Paediatric dose: <5years:2.5mgNEB(or0.1mgmeteredaerosolsprayx3).
≥5years:5mgNEB(or0.1mgmeteredaerosolsprayx5).
(repeatat5minprn).
Contraindications: KSAR.
Side effects: Tachycardia,tremors,tachyarrhythmias,highdosesmaycausehypokalaemia.
Additional information:ItismoreefficienttouseavolumizerinconjunctionwithanaerosolinhalerwhenadministeringSalbutamol.
IfanOxygendrivennebuliserisusedtoadministerSalbutamolforapatientwithacuteexacerbationofCOPDitshouldbelimitedto6minutesmaximum.
O - T
127
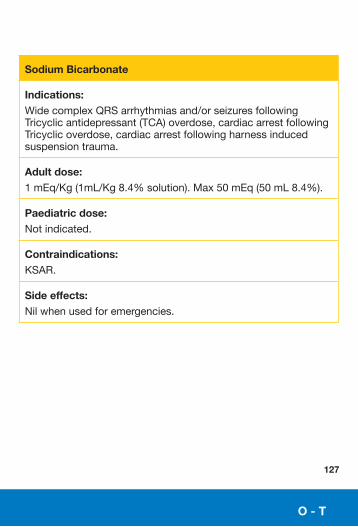
Sodium Bicarbonate
Indications: WidecomplexQRSarrhythmiasand/orseizuresfollowingTricyclicantidepressant(TCA)overdose,cardiacarrestfollowingTricyclicoverdose,cardiacarrestfollowingharnessinducedsuspensiontrauma.
Adult dose:1mEq/Kg(1mL/Kg8.4%solution).Max50mEq(50mL8.4%).
Paediatric dose: Notindicated.
Contraindications: KSAR.
Side effects: Nilwhenusedforemergencies.
O - T
128
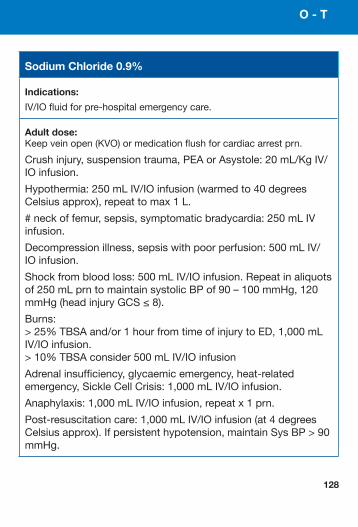
Sodium Chloride 0.9%
Indications:
IV/IOfluidforpre-hospitalemergencycare.
Adult dose: Keepveinopen(KVO)ormedicationflushforcardiacarrestprn.
Crushinjury,suspensiontrauma,PEAorAsystole:20mL/KgIV/IOinfusion.
Hypothermia:250mLIV/IOinfusion(warmedto40degreesCelsiusapprox),repeattomax1L.
#neckoffemur,sepsis,symptomaticbradycardia:250mLIVinfusion.
Decompressionillness,sepsiswithpoorperfusion:500mLIV/IOinfusion.
Shockfrombloodloss:500mLIV/IOinfusion.Repeatinaliquotsof250mLprntomaintainsystolicBPof90–100mmHg,120mmHg(headinjuryGCS≤8).
Burns:>25%TBSAand/or1hourfromtimeofinjurytoED,1,000mLIV/IOinfusion.>10%TBSAconsider500mLIV/IOinfusion
Adrenalinsufficiency,glycaemicemergency,heat-relatedemergency,SickleCellCrisis:1,000mLIV/IOinfusion.
Anaphylaxis:1,000mLIV/IOinfusion,repeatx1prn.
Post-resuscitationcare:1,000mLIV/IOinfusion(at4degreesCelsiusapprox).Ifpersistenthypotension,maintainSysBP>90mmHg.
O - T
O - T
129
Sodium Chloride 0.9% ....contd
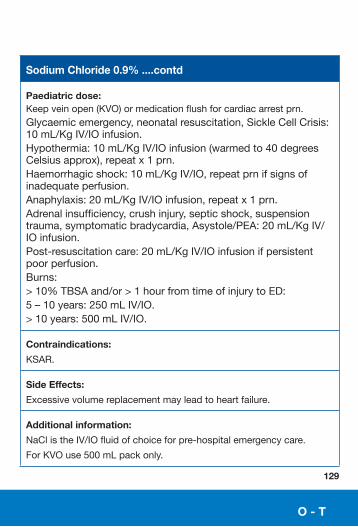
Paediatric dose: Keepveinopen(KVO)ormedicationflushforcardiacarrestprn.Glycaemicemergency,neonatalresuscitation,SickleCellCrisis:10mL/KgIV/IOinfusion.Hypothermia:10mL/KgIV/IOinfusion(warmedto40degreesCelsiusapprox),repeatx1prn.Haemorrhagicshock:10mL/KgIV/IO,repeatprnifsignsofinadequateperfusion.Anaphylaxis:20mL/KgIV/IOinfusion,repeatx1prn.Adrenalinsufficiency,crushinjury,septicshock,suspensiontrauma,symptomaticbradycardia,Asystole/PEA:20mL/KgIV/IOinfusion.Post-resuscitationcare:20mL/KgIV/IOinfusionifpersistentpoorperfusion.Burns:>10%TBSAand/or>1hourfromtimeofinjurytoED:5–10years:250mLIV/IO.>10years:500mLIV/IO.
Contraindications:
KSAR.
Side Effects:
Excessivevolumereplacementmayleadtoheartfailure.
Additional information:
NaClistheIV/IOfluidofchoiceforpre-hospitalemergencycare.
ForKVOuse500mLpackonly.
130
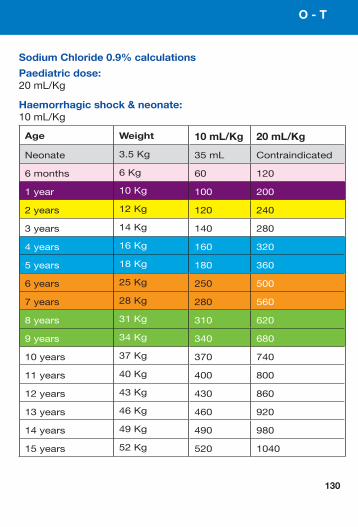
Sodium Chloride 0.9% calculations
Paediatric dose: 20mL/Kg
Haemorrhagic shock & neonate: 10mL/Kg
Age Weight 10 mL/Kg 20 mL/Kg
Neonate 3.5Kg 35mL Contraindicated
6months 6Kg 60 120
1year 10Kg 100 200
2years 12Kg 120 240
3years 14Kg 140 280
4years 16Kg 160 320
5years 18Kg 180 360
6years 25Kg 250 500
7years 28Kg 280 560
8years 31Kg 310 620
9years 34Kg 340 680
10years 37Kg 370 740
11years 40Kg 400 800
12years 43Kg 430 860
13years 46Kg 460 920
14years 49Kg 490 980
15years 52Kg 520 1040
O - T
131
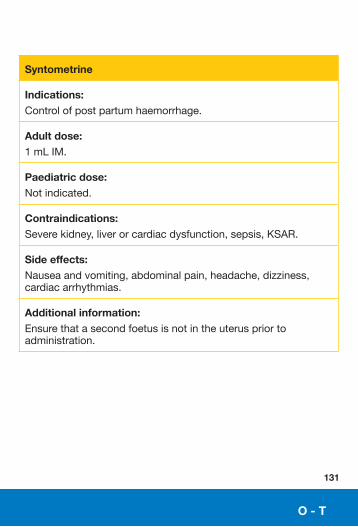
Syntometrine
Indications: Controlofpostpartumhaemorrhage.
Adult dose:1mLIM.
Paediatric dose: Notindicated.
Contraindications: Severekidney,liverorcardiacdysfunction,sepsis,KSAR.
Side effects: Nauseaandvomiting,abdominalpain,headache,dizziness,cardiacarrhythmias.
Additional information: Ensurethatasecondfoetusisnotintheuteruspriortoadministration.
O - T
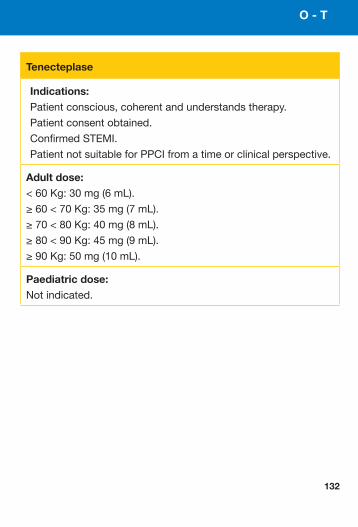
Tenecteplase
Indications: Patientconscious,coherentandunderstandstherapy.
Patientconsentobtained.
ConfirmedSTEMI.
PatientnotsuitableforPPCIfromatimeorclinicalperspective.
Adult dose:<60Kg:30mg(6mL).
≥60<70Kg:35mg(7mL).
≥70<80Kg:40mg(8mL).
≥80<90Kg:45mg(9mL).
≥90Kg:50mg(10mL).
Paediatric dose:Notindicated.
132
O - T
133
O - T
Tenecteplase ....contd
Contraindications: Haemorrhagicstrokeorstrokeofunknownoriginatanytime.Ischaemicstrokeinprevious6months.Centralnervoussystemdamageorneoplasms.Recentmajortrauma/surgery/headinjury(within3weeks).Gastro-intestinalbleedingwithinthelastmonth.Activepepticulcer.Knownbleedingdisorder.Oralanticoagulanttherapy.Aorticdissection.Transientischaemicattackinpreceding6months.Pregnancyandwithinoneweekpost-partum.Non-compressiblepunctures.Traumaticresuscitation.Refractoryhypertension(SysBP>180mmHg).Advancedliverdisease.Infectiveendocarditis.
Side effects: Haemorrhagepredominantlysuperficialattheinjectionsite,ecchymosesareobservedcommonlybutusuallydonotrequireanyspecificaction,stroke(includingintracranialbleeding)andotherseriousbleedingepisodes.
Additional Information:Enoxaparinshouldbeusedasantithromboticadjunctivetherapy.
Ticagrelor
Indications: IdentificationofSTElevationMyocardialInfarction(STEMI)iftransportingtoPPCIcentre.
Adult dose:Loadingdoseof180mgPO.
Paediatric dose: Notindicated.
Contraindications: Hypersensitivitytotheactivesubstance(Ticagrelor)ortoanyoftheexcipients,activepathologicalbleeding,historyofintracranialhaemorrhage,moderatetoseverehepaticimpairment.
Side effects: Dyspnoea,epistaxis,gastrointestinalhaemorrhage,subcutaneousordermalbleeding,bruisingandproceduralsitehaemorrhage.
Otherundesirableeffectsincludeintracranialbleeding,elevationsofserumcreatinineanduricacidlevels.ConsultSmPCforafulllistofundesirableeffects.
Additional information: Specialauthorisation:AdvancedParamedicsandParamedicsareauthorisedtoadministerTicagrelor180mgPOfollowingidentificationofSTEMIandmedicalpractitionerinstruction.
Ifapatienthasbeenloadedwithananti-plateletmedication(otherthanAspirin),priortothearrivalofthepractitioner,thepatientshouldnothaveTicagreloradministered.
134
O - T
Tranexamic Acid
Indications: Suspectedsignificantinternalorexternalhaemorrhageassociatedwithtrauma.
Adult Dose: 1gIV/IO(infusionin100mLNaCl).
Paediatric Dose: Notindicated.
Contraindications: Hypersensitivitytotheactivesubstanceortoanyoftheexcipients,acutevenousorarterialthrombosis,historyofconvulsions,severehepaticimpairment.
Side Effects: Diarrhoea,vomiting,nausea.Otherundesirableeffectsincludevisualdisturbance,impairedcolouredvision,dizzinessandheadache.
Additional Information: Cautionwithheadinjury.
135
O - T
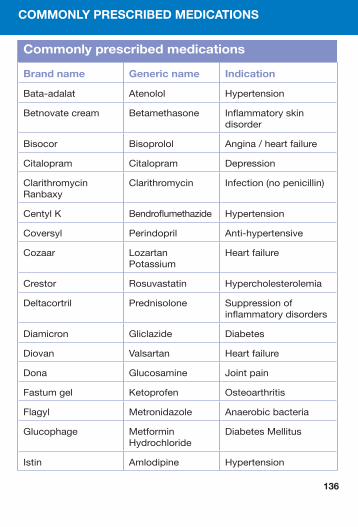
Commonly prescribed medications
Brand name Generic name Indication
Bata-adalat Atenolol Hypertension
Betnovatecream Betamethasone Inflammatoryskindisorder
Bisocor Bisoprolol Angina/heartfailure
Citalopram Citalopram Depression
ClarithromycinRanbaxy
Clarithromycin Infection(nopenicillin)
CentylK Bendroflumethazide Hypertension
Coversyl Perindopril Anti-hypertensive
Cozaar LozartanPotassium
Heartfailure
Crestor Rosuvastatin Hypercholesterolemia
Deltacortril Prednisolone Suppressionofinflammatorydisorders
Diamicron Gliclazide Diabetes
Diovan Valsartan Heartfailure
Dona Glucosamine Jointpain
Fastumgel Ketoprofen Osteoarthritis
Flagyl Metronidazole Anaerobicbacteria
Glucophage MetforminHydrochloride
DiabetesMellitus
Istin Amlodipine Hypertension
COMMONLY PRESCRIBED MEDICATIONS
136

Commonly prescribed medications ...contd
Brand name Generic name Indication
Lamictal Lamotrigine Seizurecontrol
Lexapro Escitalopram Depression
Lipitor Atorvastatin Hypercholesterolemia
Lipostat PravastatinSodium
Hyperlipidaemias
Losamel Omeprazole Duodenalulcer
Motilium Demperidone Anti-emetic
Nexium Esomeprazole Gastricoversecretionofhydrochloricacid
Omnexel Tamsulosin Benignprostatichypertrophy
Serc Betahistine Vertigo,tinnitus
Stilnoct Zolpidem Insomnia
Tritrace Ramipril Hypertension
Vibramycin Doxycycline Infection
Xanax Alprazolam Anxiety
Zimovane Zopiclone Insomnia
Zoton Lansoprazole Gastricoversecretionofhydrochloricacid
Zydol Tramadol Pain
137
COMMONLY PRESCRIBED MEDICATIONS
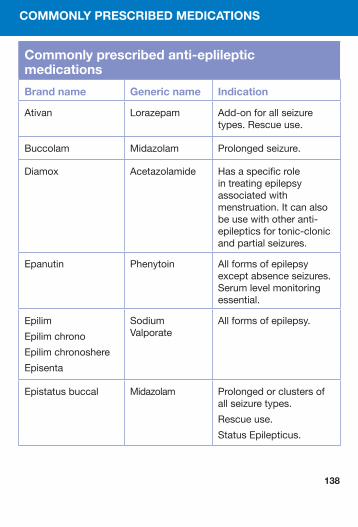
COMMONLY PRESCRIBED MEDICATIONS
138
Commonly prescribed anti-eplileptic medications
Brand name Generic name Indication
Ativan Lorazepam Add-onforallseizuretypes.Rescueuse.
Buccolam Midazolam Prolongedseizure.
Diamox Acetazolamide Hasaspecificroleintreatingepilepsyassociatedwithmenstruation.Itcanalsobeusewithotheranti-epilepticsfortonic-clonicandpartialseizures.
Epanutin Phenytoin Allformsofepilepsyexceptabsenceseizures.Serumlevelmonitoringessential.
Epilim
Epilimchrono
Epilimchronoshere
Episenta
SodiumValporate
Allformsofepilepsy.
Epistatusbuccal Midazolam Prolongedorclustersofallseizuretypes.
Rescueuse.
StatusEpilepticus.
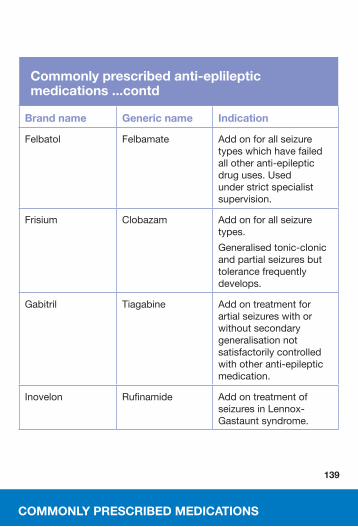
139
Commonly prescribed anti-eplileptic medications ...contd
Brand name Generic name Indication
Felbatol Felbamate Addonforallseizuretypeswhichhavefailedallotheranti-epilepticdruguses.Usedunderstrictspecialistsupervision.
Frisium Clobazam Addonforallseizuretypes.
Generalisedtonic-clonicandpartialseizuresbuttolerancefrequentlydevelops.
Gabitril Tiagabine Addontreatmentforartialseizureswithorwithoutsecondarygeneralisationnotsatisfactorilycontrolledwithotheranti-epilepticmedication.
Inovelon Rufinamide AddontreatmentofseizuresinLennox-Gastauntsyndrome.
COMMONLY PRESCRIBED MEDICATIONS
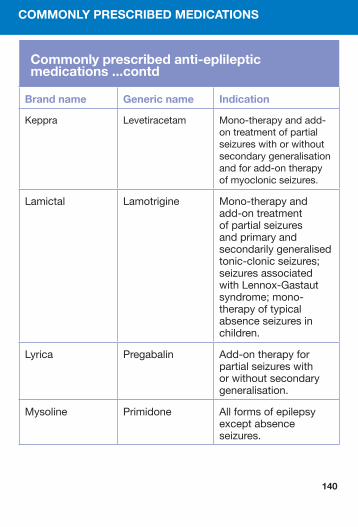
Commonly prescribed anti-eplileptic medications ...contd
Brand name Generic name Indication
Keppra Levetiracetam Mono-therapyandadd-ontreatmentofpartialseizureswithorwithoutsecondarygeneralisationandforadd-ontherapyofmyoclonicseizures.
Lamictal Lamotrigine Mono-therapyandadd-ontreatmentofpartialseizuresandprimaryandsecondarilygeneralisedtonic-clonicseizures;seizuresassociatedwithLennox-Gastautsyndrome;mono-therapyoftypicalabsenceseizuresinchildren.
Lyrica Pregabalin Add-ontherapyforpartialseizureswithorwithoutsecondarygeneralisation.
Mysoline Primidone Allformsofepilepsyexceptabsenceseizures.
COMMONLY PRESCRIBED MEDICATIONS
140
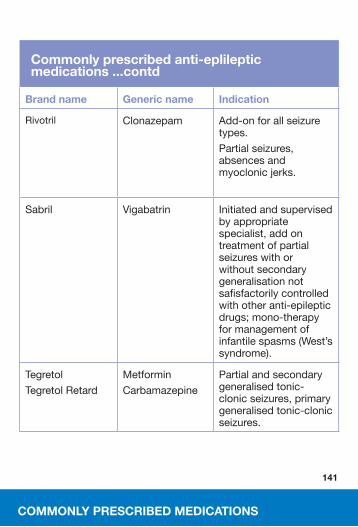
Commonly prescribed anti-eplileptic medications ...contd
Brand name Generic name Indication
Rivotril Clonazepam Add-onforallseizuretypes.
Partialseizures,absencesandmyoclonicjerks.
Sabril Vigabatrin Initiatedandsupervisedbyappropriatespecialist,addontreatmentofpartialseizureswithorwithoutsecondarygeneralisationnotsafisfactorilycontrolledwithotheranti-epilepticdrugs;mono-therapyformanagementofinfantilespasms(West’ssyndrome).
Tegretol
TegretolRetard
Metformin
Carbamazepine
Partialandsecondarygeneralisedtonic-clonicseizures,primarygeneralisedtonic-clonicseizures.
141
COMMONLY PRESCRIBED MEDICATIONS
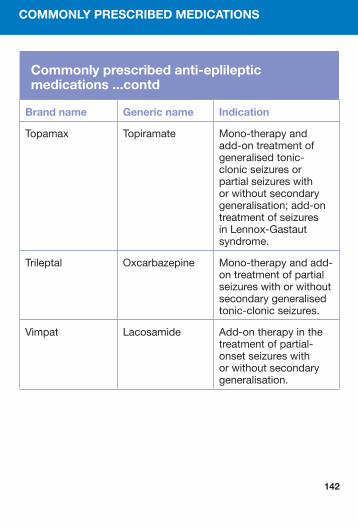
142
Commonly prescribed anti-eplileptic medications ...contd
Brand name Generic name Indication
Topamax Topiramate Mono-therapyandadd-ontreatmentofgeneralisedtonic-clonicseizuresorpartialseizureswithorwithoutsecondarygeneralisation;add-ontreatmentofseizuresinLennox-Gastautsyndrome.
Trileptal Oxcarbazepine Mono-therapyandadd-ontreatmentofpartialseizureswithorwithoutsecondarygeneralisedtonic-clonicseizures.
Vimpat Lacosamide Add-ontherapyinthetreatmentofpartial-onsetseizureswithorwithoutsecondarygeneralisation.
COMMONLY PRESCRIBED MEDICATIONS
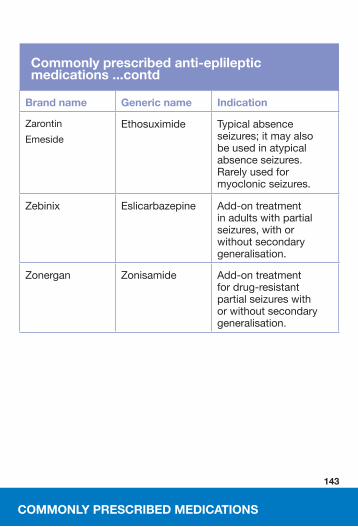
Commonly prescribed anti-eplileptic medications ...contd
Brand name Generic name Indication
Zarontin
Emeside
Ethosuximide Typicalabsenceseizures;itmayalsobeusedinatypicalabsenceseizures.Rarelyusedformyoclonicseizures.
Zebinix Eslicarbazepine Add-ontreatmentinadultswithpartialseizures,withorwithoutsecondarygeneralisation.
Zonergan Zonisamide Add-ontreatmentfordrug-resistantpartialseizureswithorwithoutsecondarygeneralisation.
143
COMMONLY PRESCRIBED MEDICATIONS
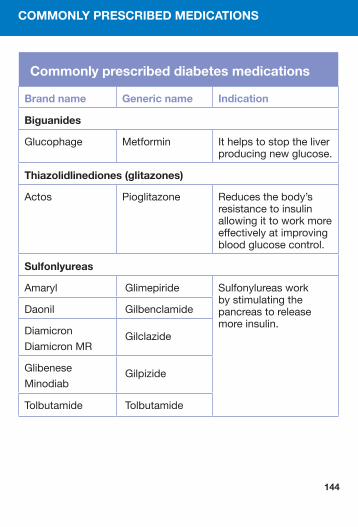
144
Commonly prescribed diabetes medications
Brand name Generic name Indication
Biguanides
Glucophage Metformin Ithelpstostoptheliverproducingnewglucose.
Thiazolidlinediones (glitazones)
Actos Pioglitazone Reducesthebody’sresistancetoinsulinallowingittoworkmoreeffectivelyatimprovingbloodglucosecontrol.
Sulfonlyure as
Amaryl Glimepiride Sulfonylureasworkbystimulatingthepancreastoreleasemoreinsulin.
Daonil Gilbenclamide
Diamicron
DiamicronMRGilclazide
Glibenese
MinodiabGilpizide
Tolbutamide Tolbutamide
COMMONLY PRESCRIBED MEDICATIONS
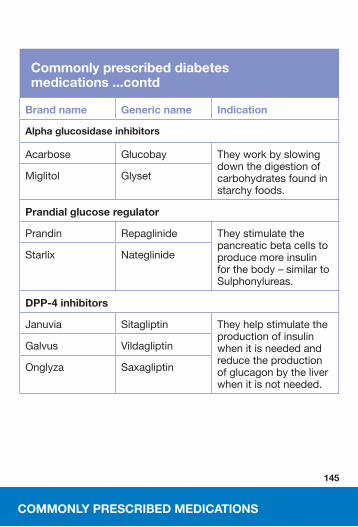
Commonly prescribed diabetes medications ...contd
Brand name Generic name Indication
Alpha glu cosidase inhibitors
Acarbose Glucobay Theyworkbyslowingdownthedigestionofcarbohydratesfoundinstarchyfoods.
Miglitol Glyset
Prandial glucose regulator
Prandin Repaglinide Theystimulatethepancreaticbetacellstoproducemoreinsulinforthebody–similartoSulphonylureas.
Starlix Nateglinide
DPP-4 inhib itors
Januvia Sitagliptin Theyhelpstimulatetheproductionofinsulinwhenitisneededandreducetheproductionofglucagonbytheliverwhenitisnotneeded.
Galvus Vildagliptin
Onglyza Saxagliptin
145
COMMONLY PRESCRIBED MEDICATIONS
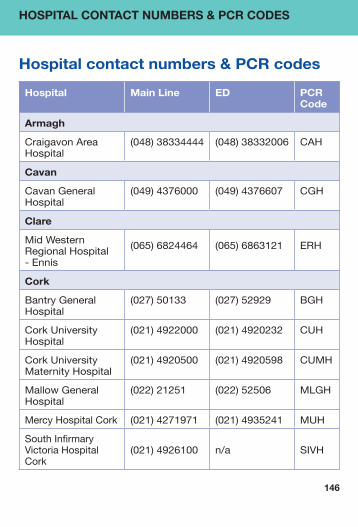
Hospital contact numbers & PCR codes
Hospital Main Line ED PCR Code
Armagh
CraigavonAreaHospital
(048)38334444 (048)38332006 CAH
Cavan
CavanGeneralHospital
(049)4376000 (049)4376607 CGH
Clare
MidWesternRegionalHospital-Ennis
(065)6824464 (065)6863121 ERH
Cork
BantryGeneralHospital
(027)50133 (027)52929
BGH
CorkUniversityHospital
(021)4922000 (021)4920232 CUH
CorkUniversityMaternityHospital
(021)4920500 (021)4920598 CUMH
MallowGeneralHospital
(022)21251 (022)52506
MLGH
MercyHospitalCork (021)4271971 (021)4935241 MUH
SouthInfirmaryVictoriaHospitalCork
(021)4926100 n/a SIVH
146
HOSPITAL CONTACT NUMBERS & PCR CODES

Hospital Main Line ED PCR Code
Derry
AthnagelvinHospital (048)71345171 (048)71611379 AHD
Donegal
LetterkennyGeneralHospital
(074)9125888 (074)9123595
LGH
Down
DaisyHillHospital,Newry
(048)30835000 (048)30832406
DHH
Dublin
AMNCH(Tallaght)–Adult
(01)4142000
(01)4143601 AMNA
AMNCH(Tallaght)–Paediatric
(01)4142000 (01)4143510 AMNC
BeaumontHospital (01)8093000 (01)8092714 BHD
ConnollyHospitalBlanchardstown
(01)8213844
(01)6466250 CHD
CoombeWomen’sHospital
(01)4085200
(01)4085531 CWH
MaterMisericordiaeHospital
(01)8032000 (01)8032651
MMH
NationalChildren’sHospital(TempleSt)
(01)8784200 (01)8784829
TCH
147
HOSPITAL CONTACT NUMBERS & PCR CODES
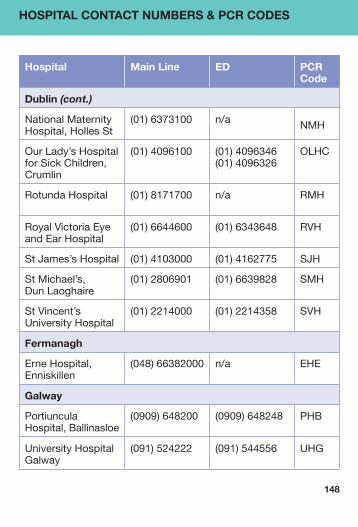
Hospital Main Line ED PCR Code
Dublin (cont.)
NationalMaternityHospital,HollesSt
(01)6373100 n/a NMH
OurLady’sHospitalforSickChildren,Crumlin
(01)4096100
(01)4096346(01)4096326
OLHC
RotundaHospital (01)8171700 n/a RMH
RoyalVictoriaEyeandEarHospital
(01)6644600 (01)6343648 RVH
StJames’sHospital (01)4103000 (01)4162775 SJH
StMichael’s,DunLaoghaire
(01)2806901 (01)6639828 SMH
StVincent’sUniversityHospital
(01)2214000 (01)2214358 SVH
Fermanagh
ErneHospital,Enniskillen
(048)66382000
n/a EHE
Galway
PortiunculaHospital,Ballinasloe
(0909)648200
(0909)648248
PHB
UniversityHospitalGalway
(091)524222 (091)544556 UHG
148
HOSPITAL CONTACT NUMBERS & PCR CODES
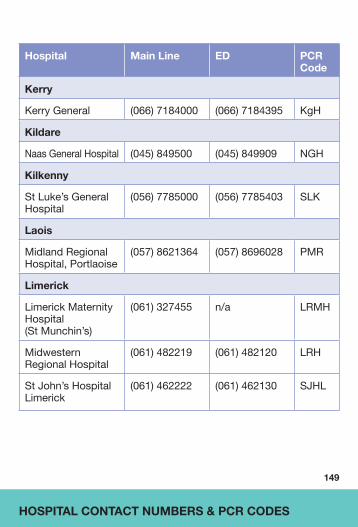
149
Hospital Main Line ED PCR Code
Kerry
KerryGeneral (066)7184000 (066)7184395 KgH
Kildare
NaasGeneralHospital (045)849500 (045)849909 NGH
Kilkenny
StLuke’sGeneralHospital
(056)7785000 (056)7785403 SLK
Laois
MidlandRegionalHospital,Portlaoise
(057)8621364
(057)8696028 PMR
Limerick
LimerickMaternityHospital(StMunchin’s)
(061)327455
n/a
LRMH
MidwesternRegionalHospital
(061)482219 (061)482120 LRH
StJohn’sHospitalLimerick
(061)462222 (061)462130 SJHL
HOSPITAL CONTACT NUMBERS & PCR CODES
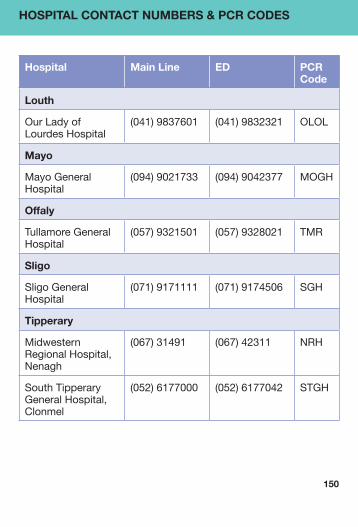
Hospital Main Line ED PCR Code
Louth
OurLadyofLourdesHospital
(041)9837601 (041)9832321 OLOL
Mayo
MayoGeneralHospital
(094)9021733 (094)9042377 MOGH
Offaly
TullamoreGeneralHospital
(057)9321501
(057)9328021
TMR
Sligo
SligoGeneralHospital
(071)9171111
(071)9174506 SGH
Tipperary
MidwesternRegionalHospital,Nenagh
(067)31491
(067)42311
NRH
SouthTipperaryGeneralHospital,Clonmel
(052)6177000
(052)6177042
STGH
150
HOSPITAL CONTACT NUMBERS & PCR CODES

151
Hospital Main Line ED PCR Code
Waterford
WaterfordRegionalHospital
(051)848000 (051)842445 WRH
Westmeath
MidlandRegionalHospital-Mullingar
(044)9340221
(044)9394121 MMR
Wexford
WexfordGeneralHospital
(053)9153000
(053)9153313
WGH
HOSPITAL CONTACT NUMBERS & PCR CODES

152
Notes

153
Notes
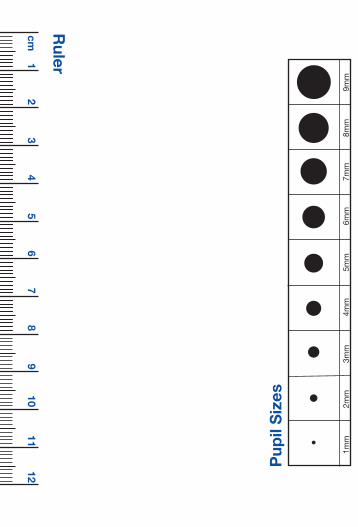
Pup
il S
izes
1mm
2mm
3mm
4mm
5mm
6mm
7mm
8mm
9mm
cm 1
2 3
4 5
6 7
8 9
10 11
12
Ruler