Embed Size (px)
Citation preview

C
EAo
JBFIHFVALa
b
c
d
e
f
g
h
i
j
k
l
m
n
o
p
q
r
s
t
u
v
w
x
y
z
a
a
a
a
a
a
a
a
a
h0n
Resuscitation 105 (2016) 188–195
Contents lists available at ScienceDirect
Resuscitationjou rn al hom epage : w ww.elsev ie r .com/ locate / resusc i ta t ion
linical paper
uReCa ONE—27 Nations, ONE Europe, ONE Registry prospective one month analysis of out-of-hospital cardiac arrestutcomes in 27 countries in Europe�
an-Thorsten Gräsnera,b,∗, Rolf Leferingc, Rudolph W. Kosterd, Siobhán Mastersone,ernd W. Böttiger f, Johan Herlitzg, Jan Wnenta,b, Ingvild B.M. Tjelmelandh,ernando Rosell Ortiz i, Holger Maurer j, Michael Baubink, Pierre Mols l,rzal Hadzibegovicm, Marios Ioannidesn, Roman Skuleco, Mads Wissenbergp, Ari Saloq,ervé Hubert r, Nikolaos I. Nikolaous, Gerda Lóczi t, Hildigunnur Svavarsdóttiru,ederico Semerarov, Peter J. Wrightw, Carlo Clarensx, Ruud Pijlsy, Grzegorz Cebulaz,itor Gouveia Correiaaa, Diana Cimpoesuab, Violetta Raffayac, Stefan Trenklerad,ndrej Markotaae, Anneli Strömsöeaf, Roman Burkartag, Gavin D. Perkinsah,eo L. Bossaertai, on behalf of EuReCa ONE Collaborators1
University Hospital Schleswig-Holstein, Dep. Anaesthesiology and Intensive Care Medicine, Kiel, GermanyUniversity Hospital Schleswig-Holstein, Institute for Emergency Medicine, Kiel, GermanyUniversity Witten/Herdecke, Cologne, GermanyAcademic Medical Center, Amsterdam, The NetherlandsNational University of Ireland Galway, IrelandUniversity Hospital of Cologne, GermanyUniversity of Borås, Sahlgrenska University Hospital, SwedenNorwegian National Advisory Unit on Prehospital Emergency Medicine (NAKOS), Oslo, NorwayEmpresa Pública de Emergencias Sanitarias, Almería, SpainUniversity Hospital Schleswig-Holstein, Dep. Anaesthesiology and Intensive Care Medicine, Campus Lübeck, GermanyUniversity Hospital Innsbruck, AustriaCentre Hospitalier Universitaire Saint-Pierre, Université Libre de Bruxelles, BelgiumMedical Faculty Osijek, Josip Juraj Strossmayer University, Osijek, CroatiaNicosia General Hospital, CyprusEmergency Medical Service of the Central Bohemian Region, Kladno, and J.E. Purkinje University, Masaryk Hospital Usti nad Labem, Czech RepublicEmergency Medical Services Copenhagen, University of Copenhagen, DenmarkEmergency Medical Services, Department of Emergency Medicine, University of Helsinki and Helsinki University Hospital, Helsinki, FinlandUniversity of Lille, FranceKonstantopouleio General Hospital, Athens, GreeceHealth Care Centers of Csongrad County Hódmezovásárhely - Makó, HungaryAkureyri Hospital/University of Akureyri, IcelandOspedale Maggiore “Carlo Alberto Pizzardi” AUSL Bologna, ItalyHealth Service Executive Ballyshannon, IrelandLuxembourg Resuscitation Council, LuxembourgMaastricht University, The NetherlandsJagiellonian University, Kraków, Poland
a Servic o de Emergência Médica Regional - SEMER/EMIR, Portugalb University of Medicine and Pharmacy Gr.T. Popa and University County Hospital Sf. Spiridon, Ias i, Romaniac Municipal Institute for Emergency Medicine Novi Sad, Serbiad
P.J.Safarik University, Kosice, Slovakiae University Medical Centre Maribor, Maribor, Sloveniaf Mälardalens University, Västerås, Swedeng Fondazione Ticino Cuore, Breganzona, Switzerlandh University of Warwick and Heart of England NHS Foundation Trust, Coventry, United Kingdomi University of Antwerp, Department of Medicine and Health Sciences, Antwerp, Belgium� A Spanish translated version of the summary of this article appears as Appendix in the final online version at http://dx.doi.org/10.1016/j.resuscitation.2016.06.004.∗ Corresponding author at: University Hospital Schleswig-Holstein, Institute for Emergency Medicine, Germany.
E-mail address: [email protected] (J.-T. Gräsner).1 Names listed at the end of the manuscript.
ttp://dx.doi.org/10.1016/j.resuscitation.2016.06.004300-9572/© 2016 The Author(s). Published by Elsevier Ireland Ltd. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-c-nd/4.0/).

a
ARRA
KCRERE
I
ihacaa
ascsftoiCtAc
bphrco
ifEtot(
M
opOr
J.-T. Gräsner et al. / Resuscitation 105 (2016) 188–195 189
r t i c l e i n f o
rticle history:eceived 19 May 2016eceived in revised form 31 May 2016ccepted 8 June 2016
eywords:ardiac arrestesuscitationpidemiologyesuscitation registrymergency medicine, Europe
a b s t r a c t
Introduction: The aim of the EuReCa ONE study was to determine the incidence, process, and outcome forout of hospital cardiac arrest (OHCA) throughout Europe.Methods: This was an international, prospective, multi-centre one-month study. Patients who suffered anOHCA during October 2014 who were attended and/or treated by an Emergency Medical Service (EMS)were eligible for inclusion in the study. Data were extracted from national, regional or local registries.Results: Data on 10,682 confirmed OHCAs from 248 regions in 27 countries, covering an estimated pop-ulation of 174 million. In 7146 (66%) cases, CPR was started by a bystander or by the EMS. The incidenceof CPR attempts ranged from 19.0 to 104.0 per 100,000 population per year. 1735 had ROSC on arrival athospital (25.2%), Overall, 662/6414 (10.3%) in all cases with CPR attempted survived for at least 30 daysor to hospital discharge.Conclusion: The results of EuReCa ONE highlight that OHCA is still a major public health problem account-ing for a substantial number of deaths in Europe.
EuReCa ONE very clearly demonstrates marked differences in the processes for data collection andreported outcomes following OHCA all over Europe. Using these data and analyses, different countries,regions, systems, and concepts can benchmark themselves and may learn from each other to furtherimprove survival following one of our major health care events.
© 2016 The Author(s). Published by Elsevier Ireland Ltd. This is an open access article under the CCBY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
ntroduction
Out-of-hospital cardiac arrest (OHCA) is a major health problemn Europe and in the United States. The numbers of patients whoave OHCA annually in these two parts of the world have tradition-lly been reported to be 275,000 and 420,000 respectively.1,2 Thisorresponds with an incidence rate of approximately 38.0–55.0ll-rhythm OHCAs per 100,000 person-years with resuscitationttempted by Emergency Medical Services (EMS).
The best way to describe the epidemiology of a disease is to cre-te a registry to which the disease is reported. With regard to OHCA,uch registries can involve an EMS service, a region, or a wholeountry. A registry can describe changes over time in incidence,urvival, and various modes of treatment. An important modifiableactor to measure in OHCA is bystander cardiopulmonary resuscita-ion (CPR) which reflects the community involvement in treatmentf this emergency condition. In terms of OHCA, a number of reg-stries have been built up outside Europe. Of particular note are theardiac Arrest Registry to Enhance Survival (CARES), the Resusci-ation Outcomes Consortium Epistry (ROC) in North America, thell-Japan Utstein Registry, and the Pan-Asian Resuscitation Out-omes Registry (PAROS).3–6
During the last decades a number of registries for OHCA haveeen implemented in Europe.7–17 These registries cover variedarts of the participating countries. The greater part of Europeowever is not included in a registry with the aim of continuouseporting of OHCA. A registry covering larger areas of Europe shouldreate the opportunity to build an overall picture of the epidemi-logy of OHCA in these areas.
The lack of a pan-European registry means there is still a gapn actual knowledge regarding the current incidence of OHCA andurthermore, the survival after OHCA. The aim of this project of theuropean Registry of Cardiac Arrest (EuReCa ONE) was to determinehe incidence, process, and outcome for OHCA in a large numberf countries in Europe. Major outcomes that were addressed inhis prospective analysis were return of spontaneous circulationROSC), admission to hospital, and/or 30-day survival.
ethods
EuReCa ONE was an international, prospective, multi-centrene-month study, designed as initial first step to establish a Euro-
Medical Service (EMS) were eligible for inclusion in the study.Patients were eligible for inclusion regardless of performanceor non-performance of a resuscitation attempt, arrest aetiology,initial arrest rhythm, age, or gender. The study dataset was devel-oped by the Steering Committee (SC) in accordance with Utsteindefinitions.19 A revised Utstein dataset was introduced close to thetime of study inception, which included a new category of aeti-ology i.e. ‘medical’. As well as ‘presumed cardiac’, the ‘medical’category includes all other medical causes in which there is no obvi-ous cause of cardiac arrest.14 In order to facilitate data collectionfrom existing systems, data on aetiology was collected for both the‘presumed cardiac’ and ‘medical’ categories. The EuReCa ONE studyis registered with ClinicalTrials.gov (T02236819). The study proto-col has been published previously and describes all questions to beaddressed in the EuReCa ONE Study (see Supplement S1).20
Countries were recruited to participate in EuReCa ONE throughan open invitation meeting during the European ResuscitationCouncil (ERC) Congress in 2013. The recruitment process resultedin 27 countries committing to participate in EuReCa ONE.
Each participating country was requested to identify oneNational Coordinator (NC). All NCs signed a Memorandum ofUnderstanding agreeing that they were responsible for obtainingethical approval/waiver for participation in EuReCa ONE, coor-dinating national data collection, assuring data quality, and forsubmitting de-identified data for analysis. National Coordinatorswere supplied with electronic copies of the dataset, coding, anddefinitions and given a contact for the Study Management Team(SMT) so that any specific queries could be dealt with by the SMTor escalated to the SC as required. Each SMT member acted as aliaison person for a group of countries and kept in contact with NCsin case of issues arising.
Data were extracted from national, regional or local OHCA reg-istries and databases, or by use of a paper version of the EuReCa ONEdatasheet for data collection. Data were obtained from: existingregistries with national coverage (five countries); existing registrieswith partial country coverage (eight countries); registries providedby the local Resuscitation Council (three countries); patient ambu-lance records (three countries). Eight countries used paper-baseddata collection and reported cases directly to the NC. Data ele-ments were de-identified and data was transcribed by each NConto a EuReCa ONE Data Export Template and submitted via pass-word encrypted secure electronic transfer to the specially designed
ean Registry of Cardiac Arrest (EuReCa).18 Patients who had anHCA during October 2014 which occurred in any participating
egion and who were attended and/or treated by an Emergency
EuReCa website. Prior to transcription, NCs were expected to assurethe quality of the data being sent in terms of comprehensivenessand adherence to data definitions and coding.
1 scitati
oN
S
repcfitrta
cg9
R
(tAfoo
ds
TS
90 J.-T. Gräsner et al. / Resu
After exploratory analysis on submitted data and clarification ofutstanding issues in relation to data quality were addressed withCs, the final data submission was completed in August 2015.
tatistical analysis
Incidence rates for one month were extrapolated to incidenceates per 100,000 population per year. In countries with partial cov-rage the covered population was calculated by adding regionalopulations. Descriptive analyses of patient demographics, caseharacteristics, and treatment and outcome variables were per-ormed for the whole group as well as for each participating countryn order to investigate the degree of variability between coun-ries and regions. Survival was derived from status at 30 days, andeplaced by hospital discharge status in case of missing 30 days sta-us. Statistical analysis is based on cases where CPR was started by
bystander or by the EMS.In order to limit statistical uncertainty, for some analyses only
ountries with ten or more cases were included. For selected cate-orical variables, e.g. ROSC or survival, 95% confidence intervals (CI5) were calculated based on the Poisson distribution.
ole of the funding source
The study was funded by the European Resuscitation CouncilERC) and by the individual registries within participating coun-ries. Co-funding was provided by the German Anaesthesiologyssociation (BDA). The Laerdal Foundation for Acute Medicine co-
unded a meeting of the NCs, the SMT, and the SC. The fundingrganisations had no influence on the data analysis or preparation
f the manuscript.The ERC appointed a SC that was responsible for the studyesign, conduct, and data analyses. Technical and administrativeupport was given by the SMT. Members of the SC had full access
able 1ummary data for all participating countries.
Code Country Totalpopulation(in thousands)
Populationcovered(in thousands)
Percentagecovered
A Austria 8474 1538 18%
B Belgium 11,200 1530 14%
CRO Croatia 4285 1893 44%
CYP Cyprus 0.800 0.200 25%
CZ Czech Rep. 10,520 4359 41%
DK Denmark 5614 1726 31%
SF Finland 5439 4445 82%
F France 66,318 17,166 26%
D Germany 80,620 13,416 17%
GR Greece 11,030 6144 56%
H Hungary 9909 1288 13%
ICE Iceland 0.328 0.328 100%
IRL Ireland 4588 4588 100%
I Italy 59,830 8015 13%
LUX Luxemburg 0.549 0.549 100%
NL Netherlands 16,800 4870 29%
N Norway 5048 3931 78%
PL Poland 38,530 2265 6%
P Portugal 10,460 0.262 3%
RO Romania 19,960 5344 27%
SRB Serbia 7164 3200 45%
SK Slovakia 5421 5421 100%
SLO Slovenia 2050 0.660 32%
E Spain 47,270 47,270 100%
S Sweden 9593 7482 78%
CH Switzerland 8081 0.346 4%
UK United Kingdom 64,597 26,346 41%
Total 514,478 174,582 34%
a B, S, UK: only cases with cardiopulmonary resuscitation (CPR) attempted.
on 105 (2016) 188–195
to the study data and all NCs were responsible for critical revisionof the submitted version of the manuscript.
Results
Patient and process characteristics
Data on 10,682 confirmed OHCAs were collected from 248 dif-ferent regions in 27 countries, covering an estimated population of174 million (34%) of 514 million people living in these Europeancountries (Table 1). Seven countries provided national data, othercountries reported data from selected regions within the country(range 1–51 regions). The population covered varied from 3% to100% of the total population of the country. Three countries pro-vided only cases when CPR was started. The lowest number ofreported patients for one country was four (Cyprus) and the highestnumber was 1536 (United Kingdom). In 7146 cases, CPR was startedby a bystander or by the EMS. We found an OHCA incidence rate of84.0 per 100,000 population for patients considered for resuscita-tion by the EMS. The incidence of CPR attempts ranged from 19.0to 104.0 per 100,000 population per year (Table 1).
The following calculations are based on all cases where CPR wasstarted by EMS or bystander. Mean patient age was 66.5 (SD 18.6)years, and the median age was 70.0 years, (range 0–104) (Table 2).The majority of patients were male (66.3%). The majority of OHCAs(69.4%) occurred in a private residence. In 54.3% of cases the col-lapse was witnessed by bystanders and in 11.9% by the EMS. In47.4% of cases CPR was initiated by a bystander. The cause of OHCAwas presumed to be medical in 91.4% of cases. This included caseswhere the presumed cause was reported as unknown or where data
was missing (24.0%), as these are also considered medical (includ-ing cardiac) following the Utstein recommendations.19 A traumaticcause was reported in 4.1% of cases (range 0–16.0%). The propor-tion of telephone assisted CPR was reported from 21 countries. TheRegions Caseswith CA
CA per 100,000per year
CPRattempted
CPR per100,000 peryear
7 71 55 54 426 105 a 105 826 98 62 66 421 6 36 4 247 886 244 379 1041 116 81 101 70
20 467 126 216 5844 855 60 743 5251 1369 122 738 66
7 253 49 165 323 127 118 85 796 13 58 10 441 209 76 155 414 773 116 428 643 46 102 28 623 250 62 190 47
11 188 57 167 511 275 146 133 701 35 160 16 733 378 85 229 517 488 183 159 601 670 148 343 764 38 69 25 45
17 1107 28 756 1920 301 a 301 48
1 22 76 14 4812 1536 a 1536 70
248 10,682 – 7146 –

J.-T. Gräsner et al. / Resuscitation 105 (2016) 188–195 191
Table 2Selected summary findings from all countries. Results are presented as overall mean value or percentage of all cases, and median with range of the individual country values.Calculations are based on all cases where CPR was started by EMS or bystander.
No. of countries No. of cases Overall average Median of country values Range of country values
Cases with CPR attempted 27 7146 264.7 159 4–1536Mean age (years) 27 6826 66.5 66.0 58.4–75.6Male gender (%) 27 7004 66.3 65.7 50.0–90.0Medical/cardiac causea (%) 27 7146a 91.4 90.1 78.1–100Traumatic cause (%) 27 7146a 4.1 3.7 0–16.5Location: residence (%) 27 7052 69.4 67.1 46.4–79.9Telephone CPR (%) 21 3439 29.9 30.4 0–100Collapse witnessed (%) 27 6815 66.1 67.5 37.4–93.5Bystander CPR (%) 27 6619 47.4 50.0 6.3–78.0Shockable rhythm (%) 26 6533 22.2 23.6 4.4–50.0
28
ar
O
wRr
O
R
FR
ROSC (%) 27 6963
a Missing or unknown values were considered as medical/cardiac.
verage percentage was 30.0%. A shockable initial rhythm waseported in 22.2% of patients, ranging between 4.4% and 50.0%.
utcomes
Data on return of spontaneous circulation at any stage (ROSC)as available for 6963 of 7146 patients (97.4%) (Fig. 1). PercentageOSC for all countries was 28.6% (n = 1994) (Fig. 2). There was a wideange of percentage ROSC reported (9.0–50.0%). Some countries
Confirmed cases of OHCA
N=10,682
Cases with CPR attempted
N=7,146
CPR not attempted
N=3,536
ROSC status available
N=6,963
ROSC status missing
N=183
Admiss ion status missing
N=79
Survival status missing
N=646
Survival t o 30 da ys / hospital d ischarge
569 of 1,829 (31.1%)
Hospital treatme nt
N=2,475
Survival in all cases with hospital outcome
662 of 2,005 (33.0%)
Survival in all cases with CPR att empted
662 of 6,414 (10.3%)
Hospita l a dmission statu s avail able
N=6884
ROSC 1,735 / ongoing CPR 740 / dead 4,409
HCA= out of hospital cardiac arrest,
OSC= Return of spontaneous circulation, CPR= cardiopulmonary resuscitation
ig. 1. Flow chart with number of cases. OHCA = out of hospital cardiac arrest,OSC = return of spontaneous circulation, CPR = cardiopulmonary resuscitation.
.6 30.6 9.1–50.0
with a small number of cases reported high proportions of ROSCwith wide confidence intervals, but the range of reported ROSCfrom countries with larger numbers of cases and narrow confidenceintervals also varied from less than 10.0% to more than 40.0%. Theincidence rate of ROSC ranged between 6.0 and 32.0 per 100,000population per year.
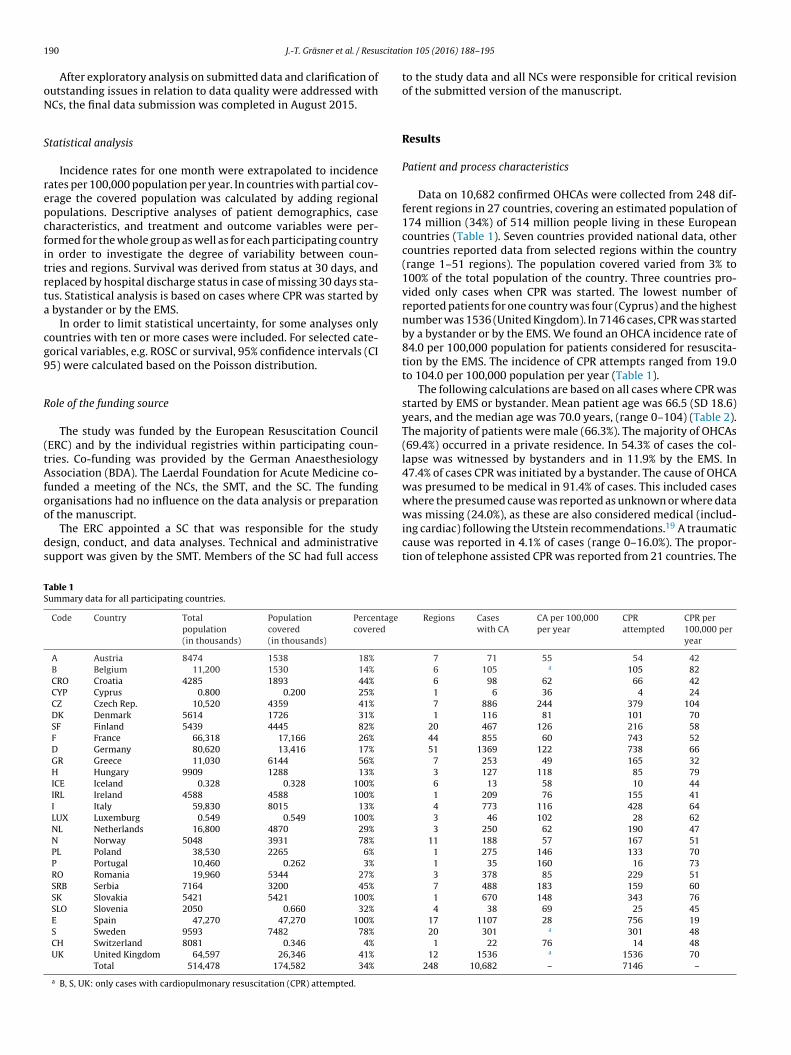
The status on arrival at hospital was known for 6884 of the7146 patients (96.3%) for whom a resuscitation attempt was started(Fig. 3). Of these patients, 4409 died on scene or en route to the hos-pital (64.0%). One fourth of patients (n = 1735) had sustained ROSCon arrival at ED (ROSC at hospital) (25.2%), and 740 patients (10.7%)arrived with ongoing CPR. Of the patients with ROSC at hospital forwhom survival data was available, 543/1291 (42.0%) survived for30 days or to hospital discharge. Of the patients with ongoing CPRfor whom data was available, 26/538 (4.8%) survived for at least 30days or to hospital discharge (Fig. 4).
Data on survival to 30 days or to hospital discharge was avail-able for 2005 of patients admitted to hospital, including those withongoing CPR and missing ROSC at hospital data. Of these patients,662 (33.0%,) survived. The values of the participating countriesranged from 6.4% to 66.7%. In all patients where CPR was started,and hospital outcome was available (n = 6414), 10.3% survived forat least 30 days after OHCA or to hospital discharge (Fig. 5). Thispercentage ranged from 1.1% and 30.8% among the participating
countries. The extrapolated incidence rate of survival for admittedpatients ranged between 0.2 and 17.3 per 100,000 population peryear (Supplementary Table S3).Fig. 2. ROSC rate in patients with CPR attempted. The vertical lines represent the 95%confidence intervals (CI). The graph includes 6963 patients from 27 countries (rangeper country 4 – 1475). The overall result is 28.6%. Abbreviations: ROSC = return ofspontaneous circulation. Abbreviations for Countries names are explained in Table 1.
192 J.-T. Gräsner et al. / Resuscitation 105 (2016) 188–195
Fig. 3. Status on hospital admission (n = 6884)*. Abbreviations: ROSC = Return ofspontaneous circulation; CPR = cardiopulmonary resuscitation; Abbreviations forcer
O
btaScwotOhip
Fafi1T
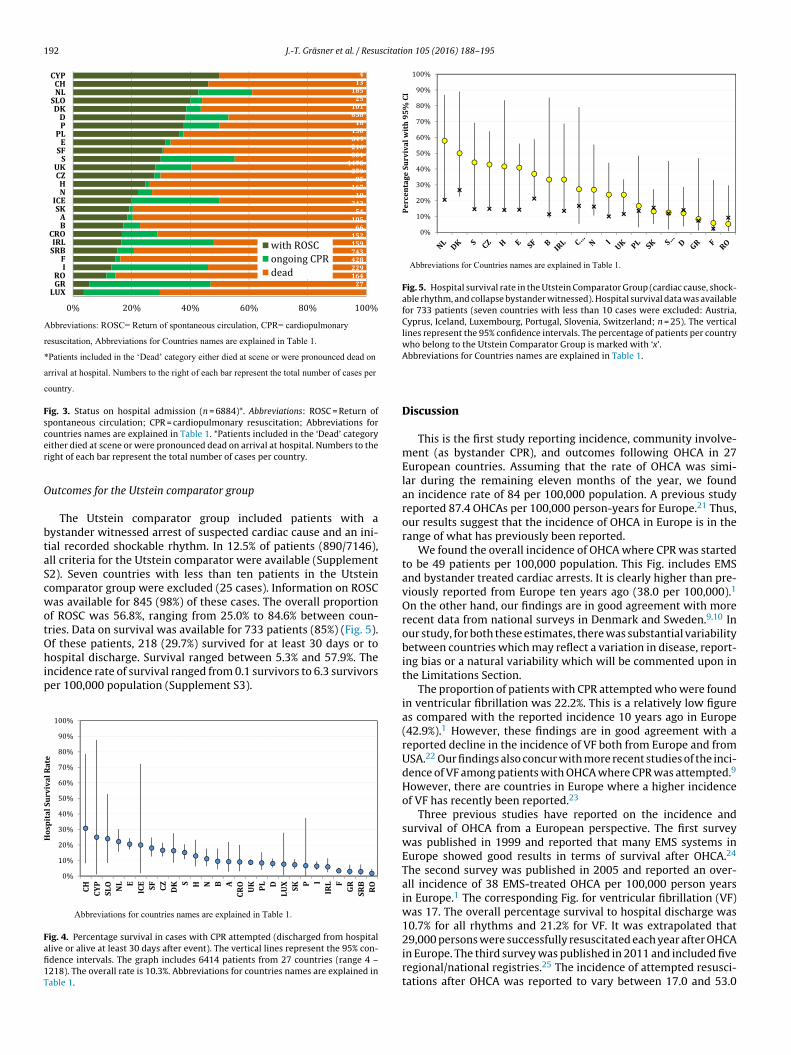
Fig. 5. Hospital survival rate in the Utstein Comparator Group (cardiac cause, shock-able rhythm, and collapse bystander witnessed). Hospital survival data was availablefor 733 patients (seven countries with less than 10 cases were excluded: Austria,Cyprus, Iceland, Luxembourg, Portugal, Slovenia, Switzerland; n = 25). The verticallines represent the 95% confidence intervals. The percentage of patients per countrywho belong to the Utstein Comparator Group is marked with ‘x’.
ountries names are explained in Table 1. *Patients included in the ‘Dead’ categoryither died at scene or were pronounced dead on arrival at hospital. Numbers to theight of each bar represent the total number of cases per country.
utcomes for the Utstein comparator group
The Utstein comparator group included patients with aystander witnessed arrest of suspected cardiac cause and an ini-ial recorded shockable rhythm. In 12.5% of patients (890/7146),ll criteria for the Utstein comparator were available (Supplement2). Seven countries with less than ten patients in the Utsteinomparator group were excluded (25 cases). Information on ROSCas available for 845 (98%) of these cases. The overall proportion
f ROSC was 56.8%, ranging from 25.0% to 84.6% between coun-ries. Data on survival was available for 733 patients (85%) (Fig. 5).f these patients, 218 (29.7%) survived for at least 30 days or to
ospital discharge. Survival ranged between 5.3% and 57.9%. Thencidence rate of survival ranged from 0.1 survivors to 6.3 survivorser 100,000 population (Supplement S3).
ig. 4. Percentage survival in cases with CPR attempted (discharged from hospitallive or alive at least 30 days after event). The vertical lines represent the 95% con-dence intervals. The graph includes 6414 patients from 27 countries (range 4 –218). The overall rate is 10.3%. Abbreviations for countries names are explained inable 1.
Abbreviations for Countries names are explained in Table 1.
Discussion
This is the first study reporting incidence, community involve-ment (as bystander CPR), and outcomes following OHCA in 27European countries. Assuming that the rate of OHCA was simi-lar during the remaining eleven months of the year, we foundan incidence rate of 84 per 100,000 population. A previous studyreported 87.4 OHCAs per 100,000 person-years for Europe.21 Thus,our results suggest that the incidence of OHCA in Europe is in therange of what has previously been reported.
We found the overall incidence of OHCA where CPR was startedto be 49 patients per 100,000 population. This Fig. includes EMSand bystander treated cardiac arrests. It is clearly higher than pre-viously reported from Europe ten years ago (38.0 per 100,000).1
On the other hand, our findings are in good agreement with morerecent data from national surveys in Denmark and Sweden.9,10 Inour study, for both these estimates, there was substantial variabilitybetween countries which may reflect a variation in disease, report-ing bias or a natural variability which will be commented upon inthe Limitations Section.
The proportion of patients with CPR attempted who were foundin ventricular fibrillation was 22.2%. This is a relatively low figureas compared with the reported incidence 10 years ago in Europe(42.9%).1 However, these findings are in good agreement with areported decline in the incidence of VF both from Europe and fromUSA.22 Our findings also concur with more recent studies of the inci-dence of VF among patients with OHCA where CPR was attempted.9
However, there are countries in Europe where a higher incidenceof VF has recently been reported.23
Three previous studies have reported on the incidence andsurvival of OHCA from a European perspective. The first surveywas published in 1999 and reported that many EMS systems inEurope showed good results in terms of survival after OHCA.24
The second survey was published in 2005 and reported an over-all incidence of 38 EMS-treated OHCA per 100,000 person yearsin Europe.1 The corresponding Fig. for ventricular fibrillation (VF)was 17. The overall percentage survival to hospital discharge was10.7% for all rhythms and 21.2% for VF. It was extrapolated that29,000 persons were successfully resuscitated each year after OHCAin Europe. The third survey was published in 2011 and included five
regional/national registries.25 The incidence of attempted resusci-tations after OHCA was reported to vary between 17.0 and 53.0
scitati
pb
5Dsaip
fsisshRtabpwachAto
csi
L
bwvtCdaf
pc96brstqfeoidctcr
a
J.-T. Gräsner et al. / Resu
er 100,000 person-years. There was a wide variability in terms ofystander CPR and early survival.
Our study reports variability of ROSC from less than 10.0% up to0.0%, and hospital survival ranging from less than 5.0% to 30.0%.ifferences in EMS structures and CPR practices may be a rea-
on for this and it should be remembered that reported data areverage values from every country. Nevertheless, we found a sim-lar difference within the systems and variability in the outcomearameters.26
The “Utstein comparator group” is one way of defining a uni-orm population of victims of OHCA with the best chance ofurvival. Within this group we also found a wide variability ofncidence, ROSC, admission to hospital, discharge and/or 30-dayurvival. It may seem reasonable to assume that there should beimilar numbers of survivors in this group. However we foundospital survival rates ranging from less than 6.0% up to 55.0%.ecent publications describe a 30-day survival ranging from 20o 31% in victims with witnessed cardiac arrest and VF.11,27 In
longitudinal study from North America, an increasing num-er of survivors were found but also with variability within thearticipating systems.28 In relation to these outcome differences,e might assume differences in bystander-CPR, quality of CPR
nd post-ROSC treatment in our study group within the differentountries and systems. Recommendations for unique CPR metricsave been published and should be used for describing quality.29
lso, a risk adjustment with more details about the victims andhe setting might be helpful to understand the variability inutcome.30
Europe is a continent with different nations, cultures, medi-al treatment standards and OHCA outcomes. Differences in EMSystems and community factors including bystander CPR may alsonfluence the outcome after cardiac arrest.
imitations
First, the methods of data collection were not standardisedetween contributing countries and regions and quality controlas limited to queries to the NCs. This may explain some of the
ariation of incidence rates of initiated resuscitation between coun-ries with ranges between 24 and 104 per 100,000 patients per year.onsidering that some variables had missing data, it is possible thatata were difficult to obtain in certain subgroups, such as patientsttended by the EMS for whom resuscitation was consideredutile.
Second, the results of our study show large differences in therocesses for data collection and outcomes between countries. Per-entage ROSC following a resuscitation attempt varied between.0% and 50.0%, survival to discharge varied between 6.4% and6.7%. This wide variation may be due to genuine differencesetween countries, similar to the large variation in outcome aseported for the Resuscitation Outcome Consortium centres.4 Thattudy employed rigid and standardised methods of data collec-ion within one nation, to ensure data completeness and datauality. They reported a five-fold range, much less than the 20-old range in survival rate that is reported in our study. Severalxplanations therefore may play a role in the wide variability inutcomes in our study. First, our study is a snapshot of OHCAn one month. Given the inherent variability of outcomes of car-iac arrest, especially in small samples in part of the contributingountries, the comparison between countries over such a shortime period has limitations. However, the combined data of all
ountries may add to the robustness of the overall outcome aseported.Third, variation in incidence rate may be due to seasonal vari-tions or indicate, legal, cultural, and religious differences in the
on 105 (2016) 188–195 193
willingness to activate EMS and to initiate resuscitation when a lowprobability of success is expected, or to terminate efforts in the field,which may affect admission rates. Three countries only reportedcases where resuscitation was started or continued by EMS staff.Another issue that can influence outcome is the actual availabil-ity of EMS resources to the population served. Higher availabilitymay promote the decision to start resuscitation, especially coun-tries where bystander CPR is lower. These factors are not recordedand it is not known how they may have affected individual cases.This limits our interpretation of the data and attribution of thesedifferences to biological patient factors or to system paramaters ofhealth care for OHCA.
Conclusions
The results of EuReCa ONE highlight that OHCA is still a majorpublic health problem accounting for a substantial number ofdeaths in Europe.
EuReCa ONE very clearly demonstrates marked differences inthe processes for data collection and reported outcomes follow-ing OHCA all over Europe. Using these data and analyses, differentcountries, regions, systems, and concepts can benchmark them-selves and may learn from each other to further improve survivalfollowing one of our major health care events.
Funding
The study was funded by the European Resuscitation Council(ERC) and by the individual registries within participating coun-tries. Co-funding was provided by the German AnaesthesiologyAssociation (BDA). The Laerdal Foundation for Acute Medicine co-funded a meeting of the NCs, the SMT and the SC. The open-AccessOption was funded by the German Resuscitation Registry. Thefunding organisations had no influence on the data analysis orpreparation of the manuscript.
EuReCa ONE-Local Contributor Group:
Austria: Marc Kaufmann, Markus Thaler, Martin Maier, GerhardPrause, Helmut Trimmel, Belgium: Diane de Longueville, ThierryPreseau, Dominique Biarent, Christian Melot, Nicolas Mpotos,Koen Monsieurs, Patrick Van de Voorde, Marie Vanhove, PascaleLievens, Mathias Faniel, Croatia: Slobodanka Keleuva, MilanLazarevic, Radmila Majhen Ujevic, Mato Devcic, Branka Bardak,Fabijan Barisic, Silvija Hunyadi Anticevic, Cyprus: Marios Georgiou,Czech Republic: Anatolij Truhlár, Jirí Knor, Eva Smrzová, RomanSviták, Robin Sín, Petr Mokrejs, Denmark: Freddy K. Lippert,Finland: Juhana Hallikainen, Marko Hoikka, Timo Iirola, Timo Jama,Helena Jäntti, Raimo Jokisalo, Milla Jousi, Hetti Kirves, MarkkuKuisma, Jukka Laine, Sami Länkimäki, Petri Loikas, Vesa Lund,Teuvo Määttä, Heini Nal, Heimo Niemelä, Petra Portaankorva,Marko Pylkkänen, Marko Sainio, Piritta Setälä, Jerry Tervo, TaneliVäyrynen, Timo Jama, France: Davy Murgue, Anne Champenois,Marc Fournier, Daniel Meyran, Romain Tabary, Aurélie Avondo,Gelin Gelin, Bruno Simonnet, Marc Joly, Isabelle Megy-Michoux,Xavier Paringaux, Yves Duffait, Michael Vial, Julien Segard, SophieNarcisse, David Hamban, Jonathan Hennache, Sylvain Thiriez,Mathieu Doukhan, Carine Vanderstraeten, Jean-Charles Morel,Gilles Majour, Corinne Michenet, Laurent Tritsch, Marc Dubesset,Olivier Peguet, David Pinero, Fréderic Guillaumee, Patrick Fuster,Jean-Franc ois Ciacala, Benoît Jardel, Jean-Yves Letarnec, Frank Goes,
Pierre Gosset, Muriel Vergne, Christian Bar, Fabienne Branche,Stevens Prineau, Steven Lagadec, Carole Cornaglia, Cécile Ursat,Philippe Bertrand, Jean-Marc Agostinucci, Pierre Nadiras, GéraldineGonzales de Linares, Line Jacob, Franc ois Revaux, Thomas Pernot,
1 scitati
NGWBPJATRCTKLGSPHFHGMKSHPGPMSNKMEMMLDMFRPNAMKMVAHJZSGRBJQLAABYDLCV
1
1
1
1
1
1
1
1
1
1
94 J.-T. Gräsner et al. / Resu
athalie Roudiak, Agnès Ricard-Hibon, Laurent Villain-Coquet,ermany: Stefan Beckers, Thomas Hanff, Bernd Strickmann, Nicolaiiegand, Petra Wilke, Harald Sues, Stefan Bogatzki, Wolfgang
aumeier, Kai Pohl, Bert Werner, Hans Fischer, Torsten Zeng, Erikopp, Andreas Günther, Andreas Hochberg, Alex Lechleuthner,ens-Christian Schewe, Hans Lemke, Erich Wranze-Bielefeld,ndreas Bohn, Markus Roessler, Frank Naujoks, Frank Sensen,orben Esser, Matthias Fischer, Martin Messelken, Christopherose, Gabriele Schlüter, Wolfgang Lotz, Michael Corzilius,laus-Martin Muth, Christian Diepenseifen, Björn Tauchmann,orsten Birkholz, Andreas Flemming, Stefanie Herrmann, Uwereimeier, Clemens Kill, Frank Marx, Ralph Schröder, Wolfgangenz, Greece: Glykeria Botini, Barakos Grigorios, Nikolaosiannakoudakis, Michail Zervopoulos, Dimitrios Papangelis,ofia Petropoulou-Papanastasiou, Themistoklis Liaskos, Spyridonapanikolaou, Andreas Karabinis, Hungary: Attila Zentay, Iceland:ólmgeir Þorsteinsson, Anna Gilsdóttir, Svavar A. Birgisson, Fjölnirreyr Guðmundsson, Hallgrímur Hreiðarsson, Björgvin Árnason,ermann Hermannsson, Gísli Björnsson, Brynjar Þór Friðriksson,unnar Baldursson, Ármann Höskuldsson, Jórunn Valgarðsdottir,atthildur Ásmundardóttir, Guðmundur Guðmundsson, Hjörtur
ristjánsson, Eyþór Rúnar Þórarinsson, Jón Guðlaugsson, Sigurðurkarphéðinsson, Ireland: National Ambulance Service of theealth Service Executive Dublin Fire Brigade, Dublin, Italy: Albertoeratoner, Andrea Santarelli, Cesare Sabetta, Giovanni Gordini,iovanni Sesana, Riccardo Giudici, Simone Savastano, Tommasoellis, Luxembourg: Jean Beissel, Jean Uhrig, Tom Manderscheid,arco Klop, Pascal Stammet, Marc Koch, Philippe Welter, Robert
chuman, The Netherlands: Wendy Bruins, Hesam Amin, Norway:ina Braa, Staale Bratland, Eirik Alnes Buanes, Tomas Draegni,nut Roar Johnsen, Wenche Torunn Mathisen, Terje Oedegaarden,arie Oppedal, Alf Stolt-Nielsen Reksten, Mats Eirik Roedsand, Jon
rik Steen-Hansen, Poland: Marta Dyrda, Anna Frejlich, Sławomiraciag, Sonia Osadnik, Ireneusz Weryk, Portugal: Eugénioendonc a, Carlos Freitas, Pinto Cruz, Carmo Caldeira, José Barros,
uis Vale, António Brazão, Nuno Jardim, Fernanda Rocha, Ricardouarte, Nicodemos Fernandes, Pedro Ramos, Margarida Jardim,iguel Reis, Romulo Ribeiro, Sérgio Zenha, Jorge Fernandes, Juan
rancisco, David Assis, Fernanda Abreu, Dinarte Freitas, Leonardoibeiro, Paulo Azevedo, Débora Calafatinho, Rui Jardim, Aleixoestana, Rui Faria, Romania: Bogdan Oprita, Alis Grasu, Pauledelea, Sorina Sovar, Florin Agapi, Serbia: Aleksandar Klickovic,leksandra Lazic, Bogdan Nikolic, Bogdan Zivanovic, Branislavartinovic, Dusan Milenkovic, Huseinovic Damir, Jovanka
oprivica, Kornelija Horvat Jaksic, Margit Pajor, Sasa Milic,irko Vidovic, Radojka Petrovic Glamoclija, Sladjana Andjelic,
lajovic Sladjana, Zlatko Babic, Zlatko Fiser, Slovakia: Peterndrovic, Lubica Bajerovska, Miroslav Chabron, Viliam Dobias, Evaavlikova, Bozena Horanova, Renata Kratochvilova, Dana Kubova,
an Murgas, Juraj Patras, Ladislav Simak, Vladimir Snarskij, Zuzanaaviaticova, Marcela Zuffova, Spain: Francesc Escalada Roig, Luisánchez Santos, Alfredo Echarri Sucunza, Juan A. Cordero Torres,uadalupe Inza Munoz, Marta Martínez del Valle, Isabel Cenicerosozalen, Enrique Martín Sánchez, María Victoria Raúl Canabalerlanga, Karlos Ibarguren Olalde, José I. Ruiz Azpiazu, María
osé García-Ochoa, Rafael Zoyo López-Navarro, José M. Adsuaruesada, José A. Cortés Ramas, Francisco J. Mellado Vergel, Juan B.ópez Messa, Patricia Fernández del Valle, Sweden: The Swedishssociation of Local Authorities and Regions, Switzerland: Lucianonselmi, Federazione Cantonale Ticinese Servizi Ambulanze,reganzona Claudio Benvenuti, United Kingdom: Nigel Batey,orkshire Ambulance, Scott Booth, Patricia Bucher, Charles
. Deakin, Jay Duckett, Chen Ji, Nancy Loughlin, Jennyumley-Holmes, Jessica Lynde, Frank Mersom, Carly Ramsey,lare Robinson, Robert Spaight, Sukhdeep Dosanjh, Gurkamalirdi, Andrew Whittington.2
on 105 (2016) 188–195
Conflict of interest statement
There are no financial and personal relationships with other peo-ple or organisations that could influence this paper. COI statementsare available for all authors.
Appendix A. Supplementary data
Supplementary data associated with this article can be found,in the online version, at http://dx.doi.org/10.1016/j.resuscitation.2016.06.004.
References
1. Atwood C, Eisenberg MS, Herlitz J, Rea TD. Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation 2005;67:75–80.
2. Rea TD, Eisenberg MS, Sinibaldi G, White RD. Incidence of EMS-treated out-of-hospital cardiac arrest in the United States. Resuscitation 2004;63:17–24.
3. Chan PS, McNally B, Tang F, Kellermann A. Recent trends in survival fromout-of-hospital cardiac arrest in the United States. Circulation 2014;130:1876–82.
4. Nichol G, Thomas E, Callaway CW, et al. Regional variation in out-of-hospitalcardiac arrest incidence and outcome. JAMA - Journal of the American MedicalAssociation 2008;300:1423–31.
5. Ong ME, Shin SD, De Souza NN, et al. Outcomes for out-of-hospital cardiac arrestsacross 7 countries in Asia: The Pan Asian Resuscitation Outcomes Study (PAROS).Resuscitation 2015;96:100–8.
6. Hasegawa K, Tsugawa Y, Camargo Jr CA, Hiraide A, Brown DF. Regional variabil-ity in survival outcomes of out-of-hospital cardiac arrest: the All-Japan UtsteinRegistry. Resuscitation 2013;84:1099–107.
7. Gräsner JT, Meybohm P, Fischer M, et al. A national resuscitation registryof out-of-hospital cardiac arrest in Germany-a pilot study. Resuscitation2009;80:199–203.
8. Sedgwick ML, Dalziel K, Watson J, Carrington DJ, Cobbe SM. Performance of anestablished system of first responder out-of-hospital defibrillation. The resultsof the second year of the Heartstart Scotland Project in the ‘Utstein Style’. Resus-citation 1993;26:75–88.
9. Stromsoe A, Svensson L, Axelsson AB, et al. Improved outcome in Swedenafter out-of-hospital cardiac arrest and possible association with improve-ments in every link in the chain of survival. European heart journal 2015;36:863–71.
0. Wissenberg M, Lippert FK, Folke F, et al. Association of national initiatives toimprove cardiac arrest management with rates of bystander intervention andpatient survival after out-of-hospital cardiac arrest. Jama 2013;310:1377–84.
1. Masterson S, Wright P, O’Donnell C, et al. Urban and rural differences in out-of-hospital cardiac arrest in Ireland. Resuscitation 2015;91:42–7.
2. Blom MT, Beesems SG, Homma PC, et al. Improved survival after out-of-hospital cardiac arrest and use of automated external defibrillators. Circulation2014;130:1868–75.
3. Cebula GM, Osadnik S, Wysocki M, et al. Comparison of the early effects of out-of-hospital resuscitation in selected urban and rural areas in Poland. A preliminaryreport from the Polish Cardiac Arrest Registry by the Polish Resuscitation Coun-cil. Polish Heart Journal 2016;74:143–8.
4. Van Hoeyweghen RJ, Bossaert LL, Mullie A, et al. Quality and efficiency ofbystander CPR. Belgian Cerebral Resuscitation Study Group. Resuscitation1993;26:47–52.
5. Hubert H, Tazarourte K, Wiel E, et al. Rationale, methodology, implementation,and first results of the French out-of-hospital cardiac arrest registry. PrehospitalEmergency Care: Official Journal of the National Association of EMS Physiciansand the National Association of State EMS Directors 2014;18:511–9.
6. Ristagno G, Semeraro F, Radeschi G, et al. The “Italian Registry of CardiacArrest - RIAC”, a National achievement to portrait the Italian reality and tocontribute to the wider European vision by “EuReCa”. Resuscitation 2014;85:e193–4.
7. Rosell Ortiz F, Mellado Vergel F, Lopez Messa JB, et al. Survival and neurologicoutcome after out-of-hospital cardiac arrest. Results of the andalusian out-of-hospital cardiopulmonary arrest registry. In: Revista espanola de cardiologia;2016 [English ed].
8. Gräsner JT, Bottiger BW, Bossaert L. European Registry of Cardiac Arrest ONESC,EuReCa ONESMT. EuReCa ONE – ONE month – ONE Europe – ONE goal. Resus-citation 2014;85:1307–8.
9. Perkins GD, Jacobs IG, Nadkarni VM, et al. Cardiac arrest and cardiopulmonaryresuscitation outcome reports: update of the utstein resuscitation registry tem-plates for out-of-hospital cardiac arrest: a statement for healthcare professionalsfrom a Task Force of the International Liaison Committee on Resuscitation(American Heart Association, European Resuscitation Council, Australian andNew Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada,InterAmerican Heart Foundation, Resuscitation Council of Southern Africa,
Resuscitation Council of Asia); and the American Heart Association EmergencyCardiovascular Care Committee and the Council on Cardiopulmonary, CriticalCare, Perioperative and Resuscitation. Resuscitation 2015;96:328–40.0. Wnent J, Masterson S, Gräsner JT, et al. EuReCa ONE - 27 Nations, ONEEurope, ONE Registry: a prospective observational analysis over one month in

scitati
2
2
2
2
2
2
2
2
2
J.-T. Gräsner et al. / Resu
27 resuscitation registries in Europe – the EuReCa ONE study protocol. Scandi-navian Journal of Trauma, Resuscitation and Emergency Medicine 2015;23:7.
1. Berdowski J, Berg RA, Tijssen JG, Koster RW. Global incidences of out-of-hospitalcardiac arrest and survival rates: Systematic review of 67 prospective studies.Resuscitation 2010;81:1479–87.
2. Keller SP, Halperin HR. Cardiac arrest: the changing incidence of ventricular fib-rillation. Current Treatment Options in Cardiovascular Medicine 2015;17:392.
3. Hulleman M, Zijlstra JA, Beesems SG, et al. Causes for the declining propor-tion of ventricular fibrillation in out-of-hospital cardiac arrest. Resuscitation2015;96:23–9.
4. Herlitz J, Bahr J, Fischer M, Kuisma M, Lexow K, Thorgeirsson G. Resuscitation inEurope: a tale of five European regions. Resuscitation 1999;41:121–31.
5. Gräsner JT, Herlitz J, Koster RW, Rosell-Ortiz F, Stamatakis L, Bossaert L. Qual-ity management in resuscitation—towards a European cardiac arrest registry(EuReCa). Resuscitation 2011;82:989–94.
3
on 105 (2016) 188–195 195
6. Neukamm J, Gräsner JT, Schewe JC, et al. The impact of response time reliabilityon CPR incidence and resuscitation success: a benchmark study from the GermanResuscitation Registry. Critical Care 2011;15:R282.
7. Ringh M, Jonsson M, Nordberg P, et al. Survival after public access defibrillationin Stockholm, Sweden—a striking success. Resuscitation 2015;91:1–7.
8. Daya MR, Schmicker RH, Zive DM, et al. Out-of-hospital cardiac arrest sur-vival improving over time: results from the Resuscitation Outcomes Consortium(ROC). Resuscitation 2015;91:108–15.
9. Meaney PA, Bobrow BJ, Mancini ME, et al. Cardiopulmonary resuscitationquality: [corrected] improving cardiac resuscitation outcomes both inside and
outside the hospital: a consensus statement from the American Heart Associa-tion. Circulation 2013;128:417–35.0. Gräsner JT, Meybohm P, Lefering R, et al. ROSC after cardiac arrest—the RACAscore to predict outcome after out-of-hospital cardiac arrest. European HeartJournal 2011;32:1649–56.





























