Embed Size (px)
Citation preview
Contemporary Oral Medicine
Leticia Ferreira, DDS, MSDepartment of Dental Practice
Arthur A. Dugoni School of Dentistry University of the Pacific
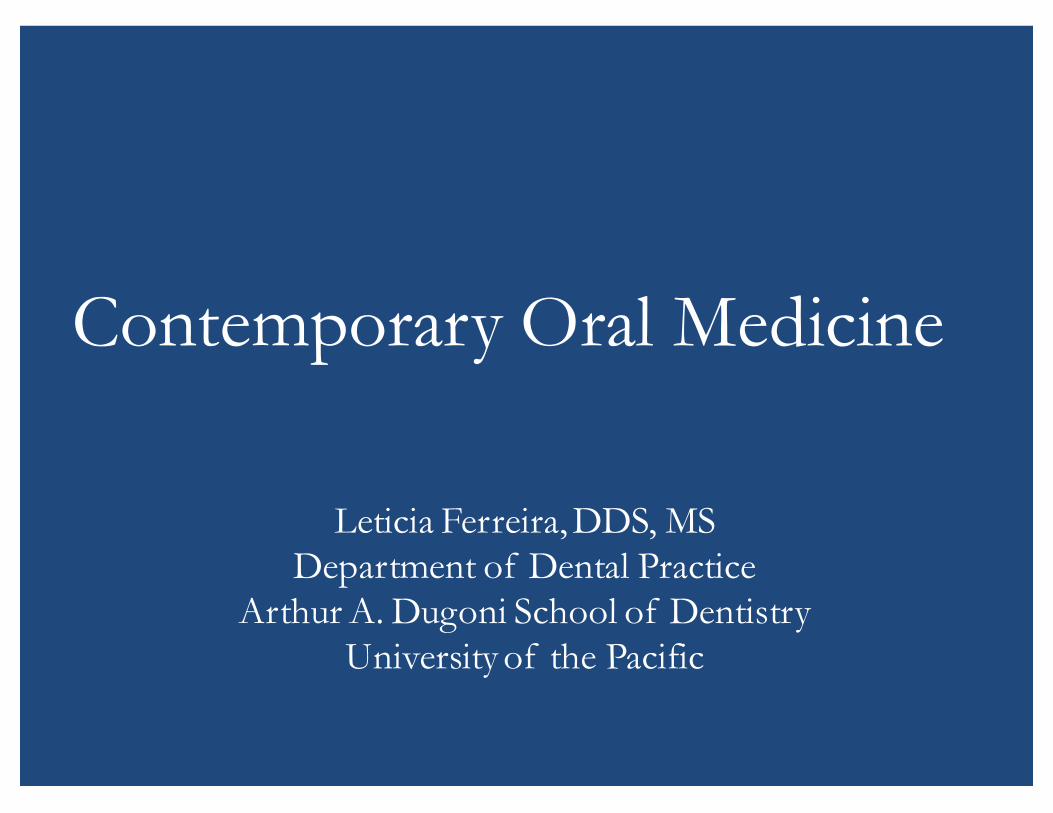
7385 Patients Disease Frequency (BCD, July 2010)Lichen planus (897) 12.1%
Xerostomia (799) 10.8%
Chronic candidiasis (741) 10.0%
Sjogren’s syndrome (431) 5.8%
Aphthae & other ulcerations (501) 6.8%
Allergic reactions (262) 3.5%
Burning mouth syndrome (295) 3.9%
Mucous membranepemphigoid
(199) 2.7%
Hyperkeratosis (156) 2.1%
Migratory glossitis (130) 1.7%
Oral malignancies (50) 0.7%
TOTAL (4461) 60.4%
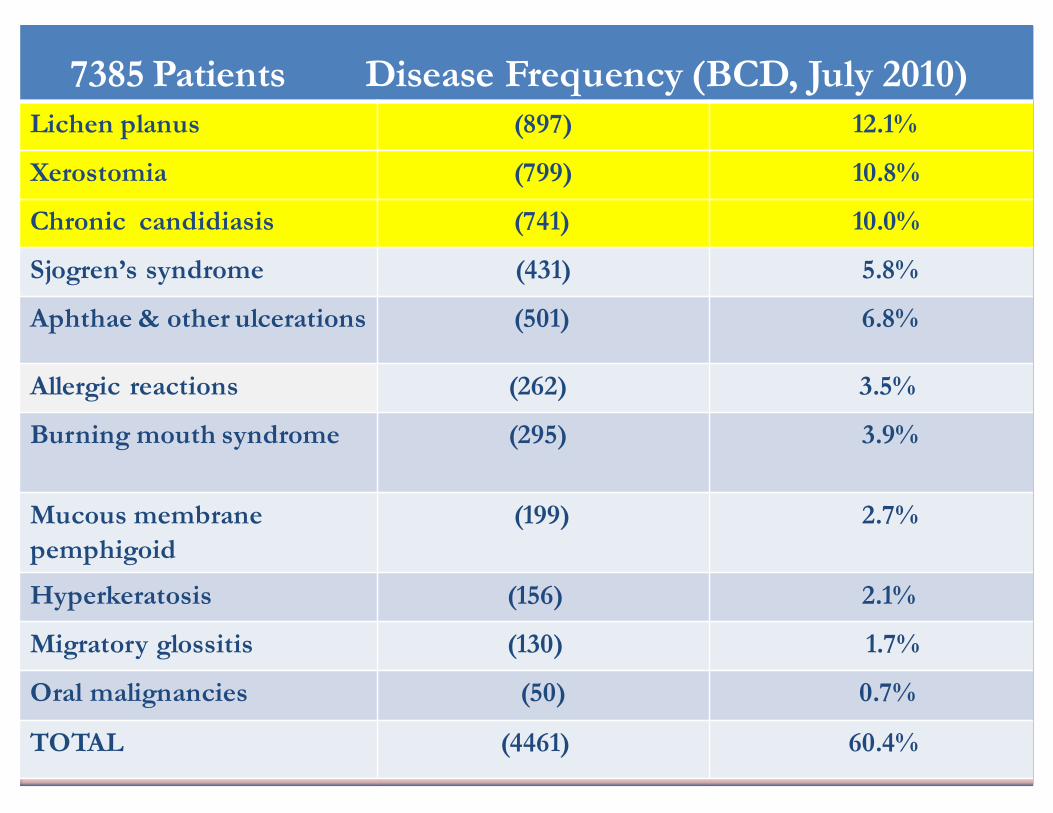
Miscellaneous Disorders (BCD, July 2010)Pemphigus 49
Graft vs. host disease 30
Lupus erythematosus 16
Erythema multiforme 13
Proliferative verrucous leukoplakia 10
Scleroderma 9
Chronic ulcerative stomatitis 8
Sarcoidosis 8
Langerhans cell histiocytosis 4
Epidermolysis bullosa 4
Pyostomatitis vegetans 3

Lichen Planus• Immunologically (T-cell) mediated disorder• Middle-aged females• Affects both skin and oral mucosa• Skin: purple, pruritic, polygonal papules• Oral– Reticular
• Wickham’s striae– Erosive (ulcerative)– Atrophic– Bullous– Plaque-like– Papular
(Eisen, 2002) (Lodi et al 2005) (Lozada-Nur 1997)
Lichen Planus
• 76.5% Female average age 57.2
• 23.5% Male average age 51.8
• Combined average age 56.0
Oral Lichen Planus (BCD, July 2010)Based on 897 patients
Lichen Planus
• Skin 14%
• Genitalia 2.3%
Oral Lichen Planus (BCD, July 2010)Based on 897 patients

Lichen Planus
• Buccal Mucosa 62.8%• Gingiva 55.8%• Tongue 33.2% • Lips 8.4%• Palate 7.0%
• Gingiva only 20.6%• Buccal Mucosa only 12.4%
Lichen PlanusClinical Sites (BCD, July 2010)
Desquamative Gingivitis
• Lichen planus• Pemphigus• Pemphigoid• Allergy–Toothpaste –Cinnamon–Preservatives
Lichen Planus• Diagnosis
– Clinical Appearance• Presence of white striae bilaterally on posterior buccal mucosa
– Histopathologic examination• Erosive cases• Isolated lichenoid lesions (in order to rule out premalignancy or
malignancy– Immunofluorescence
• In order to rule out Pemphigus and Pemphigoid, lupus erythematosus and chronic ulcerative stomatitis
Lichen Planus• Treatment–Only for symptomatic patients• Topical corticosteroids • Systemic corticosteroids• Retinoids• Cyclosporine• Tacrolimus and Pimecrolimus
–Patients should be evaluated at least once a year
(Lodi et al 2005) (Al-Hashimi et al 2007)
Lichen Planus• High Potency Topical Corticosteroid
Rx: Fluocinonide gel 0.05% (Lidex)Disp: 15gm tubeSig: Apply to affected area 4x/day. Do not eat or drink for 45 minutes after application
• Highest Potency Topical Corticosteroid Rx Clobetasol 0.05% gel (Temovate)Disp: 15 gram tubeSig: Dry the area and apply a small amount 3-4x/day. Do not eat or drink for 45 minutes after application.
• Widespread gingival involvement:– “suck-down” tray filled with gel and used 2x/day for 15-20
min
• Systemic CorticosteroidRx Prednisone 10 mg tabletDisp: 40 tabsSig: Two tabs bid x 7 days, then 1 tab bid X 4 days, the 1 tab daily until gone
Lichen Planus

Lichen Planus
• Side-effects of topical corticosteroid therapy:–Candidiasis
Lichen Planus
• Combined Topical Therapy–Topical corticosteroid
+Clotrimazole 10 mg Troche 1-3xs daily
orNystatin Oral Suspension 1 tsp 2xs daily
• Pre-malignant potential??– Controversial issue– Clinical studies and case reports suggest that OLP
patients are at a greater risk of developing OSCC• Great variation in source of data, inclusion criteria, length of
follow-up and design– Lichenoid dysplasia vs. lichen planus– Large independent controlled retrospective studies have
shown a significant risk• 1% over a 5 year period
– A minimum of one follow-up visit per year is recommended
Lichen Planus
(Markopoilos et al 1997) ( Lo Muzio et al 1998 ) (Fang et al 2009) (Gandolfo et al 2004) (van der Meij et al 1999)(Al-Hashimi et al 2007)
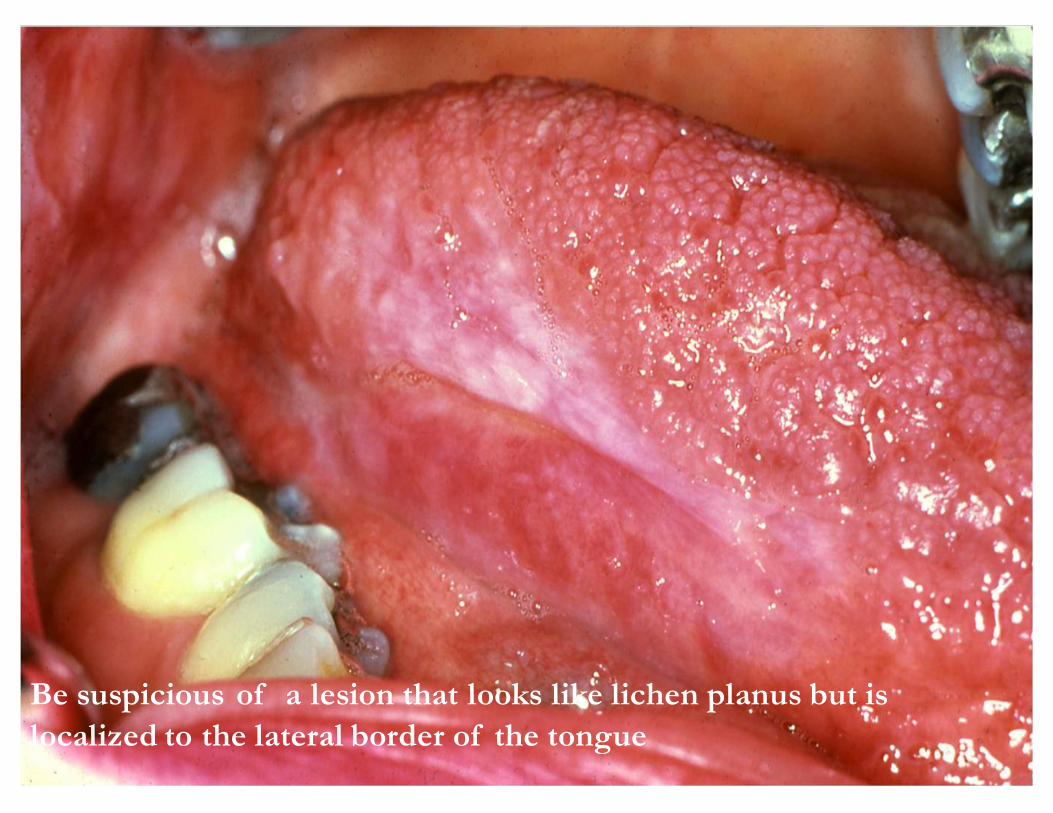
Be suspicious of a lesion that looks like lichen planus but is localized to the lateral border of the tongue
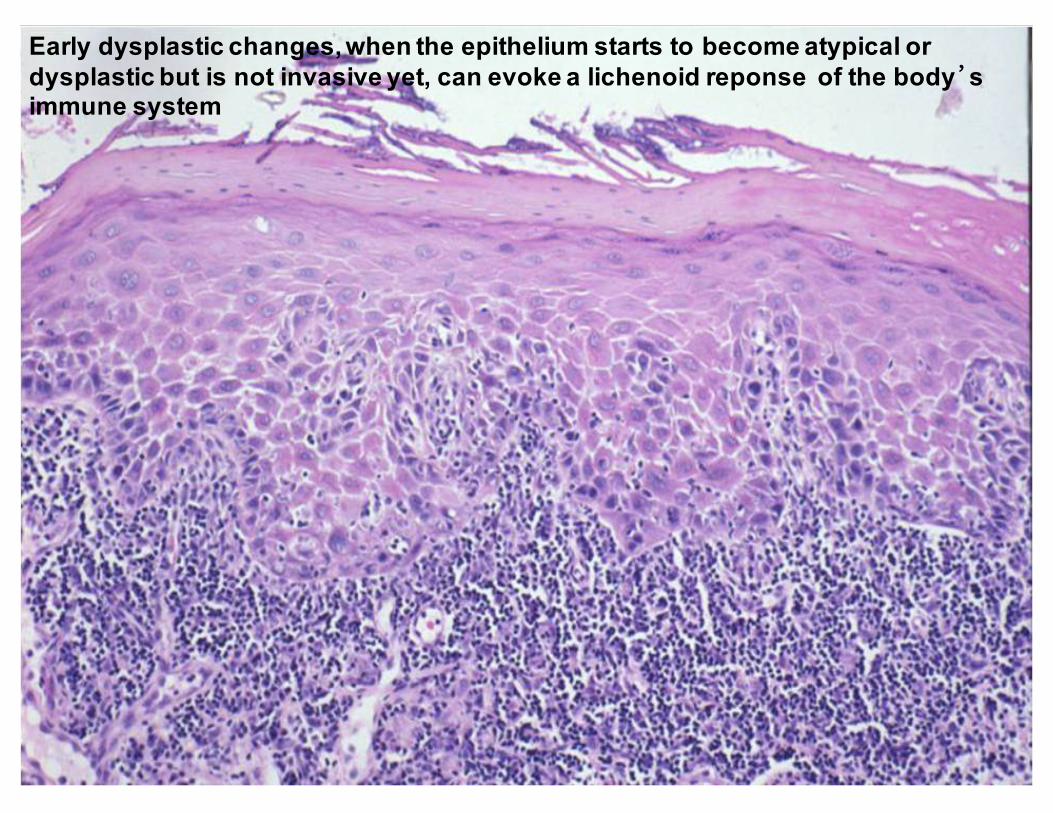
agEarly dysplastic changes, when the epithelium starts to become atypical or dysplastic but is not invasive yet, can evoke a lichenoid reponse of the body’s immune system
Lichenoid Reactions
• Most common lichenoid reactions:–Non-steroidal anti-inflammatory drugs
(NSAIDs)–Antihypertensives–Cinnamic aldehyde flavoring –Mercury
(Miller et al 1992) (Allen & Blozis 1988) (Issa et al 2005) (Moller 2002)
Lichenoid Reactions
• NSAIDs 19• Cardiovascular drugs 10• Mercury (amalgams) 10• Cinnamic aldehyde 9• Antidiabetics 9• Anti-lipemic 4• Gold salts 2
(BCD) 63 patients (04/05)
Drugs causing lichenoid drug reaction
Allopurinol Gold PractololAmiphenazole Hydroxychloroquine PropanololAtorvastatin (Lipitor) Ketoconazole PyrimethamineCaptopril Labetanol QuinidineCarbamazetine Mercury QuinacrineChloroquine Methyldopa SpironolactoneChlorpropamide Metopromazine Streptomycin Cyanamide NSAID TetracyclineDapsone Oxyprenolol ThiazidesEnalapril Palladium TolbutamideErythromycin Para-amino salicylate TriprolidineFenclofenac Penicillamine ZoloftFurosemide Phenothiazines
Candidiasis
• Candida albicans• Dimorphism: yeast and hyphal forms• Most common oral fungal infection
Candidiasis
• Predisposing factors:
– Antibiotic therapy– Cancer chemotherapy– Corticosteroid therapy– Dentures– Diabetes mellitus– Pregnancy– Iron deficiency
– Newborns’ immature immune system
– Advanced malignancy– Xerostomia– Immunocompromised
states• HIV/AIDS• Transplant patients
Candidiasis• Pseudomembranous candidiasis– “Thrush”–White material that can be wiped off– Erythematous mucosa underneath– Burning sensation–Metallic taste
Candidiasis
• Erythematous “acute atrophic” candidiasis– Often associated with antibiotics
• “Antibiotic sore mouth”
– Painful– Loss of filiform papillae on tongue
Candidiasis
• Chronic atrophic candidiasis– “Denture stomatitis”– Erythematous mucosa– Palate and maxillary alveolar ridge– Usually asymptomatic
Candidiasis
• Angular cheilitis– Labial commissures– Erythema, fissuring and scaling– Reduced vertical dimension
Candidiasis
• Mucosal smear and tissue culture• Oral antifungal therapy– Nystatin oral suspension, pastilles or ointment
• Systemic antifungal therapy– Fluconazole (Diflucan)– Ketoconazole
• Very common: 20%– Affects children and young adults more frequently
• Unknown etiology– The cause appears to be “different things in
different people”
• Immune mediated, self-limiting ulceration– CD8 T-cells produce cytokines which lyse
epithelial cells
Recurrent Aphthous Stomatitis (recurrent aphthous ulcerations)
“canker sores”
• Trauma (dental procedure)
• Emotional stress• Nutritional deficiencies• Socio-economic level• Genetic predisposition• Chemicals in food
• Immunologic factors• AIDS• Endocrine imbalance• Infectious agents• Allergies• Smoking cessation
Recurrent Aphthous Stomatitis (recurrent aphthous ulcerations)
“canker sores”
• Minor
• Major
• Herpetiform
Recurrent Aphthous Stomatitis (recurrent aphthous ulcerations)
“canker sores”
• Minor aphthae (80%)– Childhood to adolescents– ↑ Females– Less than 1 cm– On moveable mucosa (not covering bone)– Painful ulcer with erythematous border– Heal spontaneously in 7 to 14 days w/o scarring
Recurrent Aphthous Stomatitis (recurrent aphthous ulcerations)
“canker sores”
• Major aphthae (10%)– Larger than 1.5 cm– Deeper than minor aphthae– ↑↑ soft palate, tonsillar fauces, and labial
mucosa– Can take several weeks to months heal–May cause scarring
Recurrent Aphthous Stomatitis (recurrent aphthous ulcerations)
“canker sores”
• Herpetiform aphthae (10%)– Adulthood– 1 to 3 mm ulcers occurring in clusters– Any oral mucosal site may be involved– vs. herpes simplex– Heal in 7-10 days
Recurrent Aphthous Stomatitis (recurrent aphthous ulcerations)
“canker sores”
• Diagnosis:– Diagnosis by history and clinical features– Biopsy shows nonspecific ulceration– Patients with severe disease:
• Rule out systemic causes• Patch tests for antigen stimuli• Elimination of potential antigens:
– Sodium lauryl sulfate in toothpaste– NSAIDs, various beta blockers, nicorandil– Streptococci, Helicobacter pylori, HSV, VZV, and CMV– Many foods: cheese, coffee, cow’s milk, gluten, nuts,
strawberries, tomatoes, flavoring agents, preservatives
Recurrent Aphthous Stomatitis (recurrent aphthous ulcerations)
“canker sores”
• Treatment:– High-potency topical steroids– Chlorhexidine– Amlexanox 5% (Aphthasol)
Recurrent Aphthous Stomatitis (recurrent aphthous ulcerations)
“canker sores”
Rx Fluocinonide gel or cream 0.05% (Lidex)Disp: 15 or 30 gram tubeSig: Dry the area and apply a small amount 3-4x/day. Do not eat or drink for one hour after application
Rx Amlexanox oral paste 5% (Aphthasol)Disp: 5 gmSig: Apply to affected area qid
Recurrent Aphthous Stomatitis (recurrent aphthous ulcerations)
“canker sores”
Benign Mucous Membrane Pemphigoid
• “Cicatricial Pemphigoid”• Chronic, autoimmune disease• 3x as common as pemphigus vulgaris• Average age 50-60, 2x more common in
females• Oral, ocular, and genital mucosa ± others
•Gingiva (desquamative gingivitis)(Scully et al 1999 )(Bagan et al 2005)
Benign Mucous Membrane Pemphigoid
• Autoantibodies to hemidesmosomes• Is a family of diseases, different antigens• BP 180, BP 230, laminin-5, etc• Separation of the epithelium from the CT• + Nikolsky’s sign
Benign Mucous Membrane Pemphigoid
–72.4% Female average age 59.6
–27.6% Male average age 63.8
–Combined average age 60.8
(BCD, July 2010)Based on 199 patients
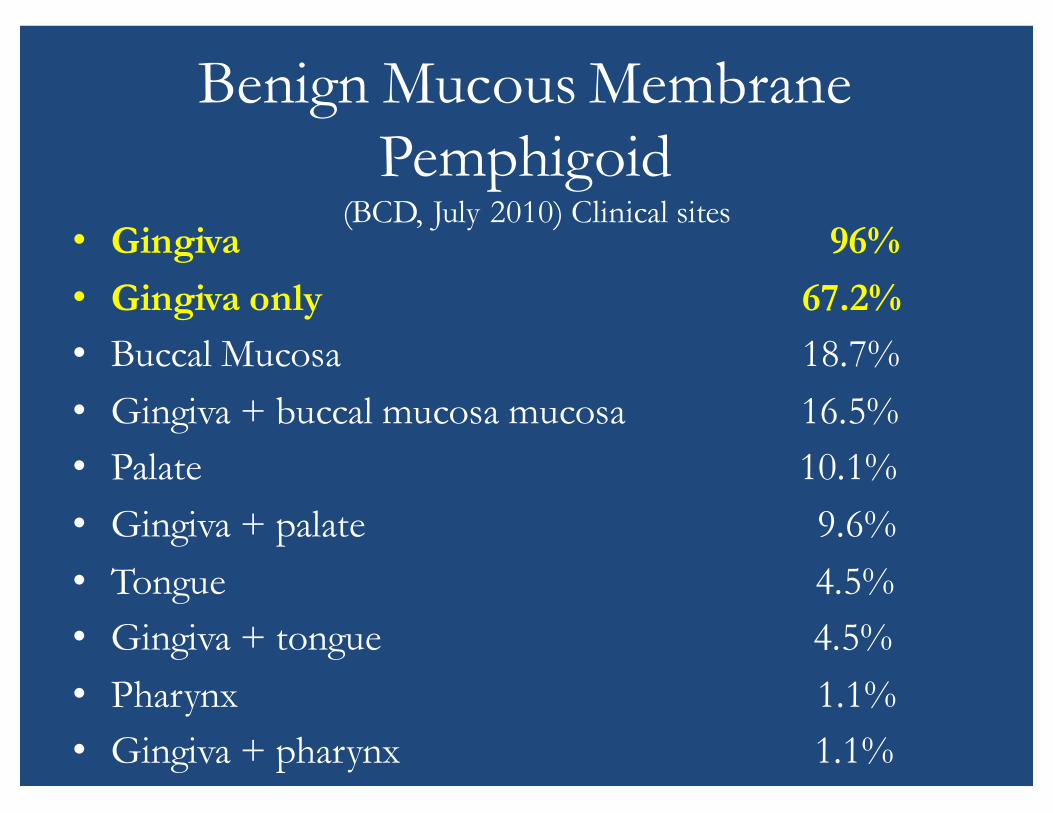
Benign Mucous Membrane Pemphigoid
• Gingiva 96%• Gingiva only 67.2%• Buccal Mucosa 18.7%• Gingiva + buccal mucosa mucosa 16.5%• Palate 10.1%• Gingiva + palate 9.6%• Tongue 4.5%• Gingiva + tongue 4.5%• Pharynx 1.1%• Gingiva + pharynx 1.1%
(BCD, July 2010) Clinical sites
Benign Mucous Membrane Pemphigoid
• Diagnosis–Histologic appearance:• Subepithelial split with separation at the
basement membrane•Non-specific inflammation
–Direct Immunofluorescence• IgG and/or C3 at basement membrane
zone•Occasionally IgA, IgM
Benign Mucous Membrane Pemphigoid
• Treatment– Referral to an ophthalmologist– Topical corticosteroids– Good oral hygiene measures can help to decrease
severity– Carrier trays– Dapsone– Tetracycline or minocycline and niacinamide– Systemic corticosteroids– Systemic corticosteroids + Cyclophosphamide– Intravenous (IV) human immunoglobulin
• Highest Potency Topical Corticosteroid Rx Clobetasol 0.05% gel (Temovate)Disp: 15 gram tubeSig: Dry the area and apply a small amount 3-4x/day. Do not eat or drink for one hour after application.
• Systemic CorticosteroidRx Prednisone 10 mg tabletDisp: 40 tabsSig: Two tabs bid x 7 days, then 1 tab bid X 4 days, the 1 tab daily until gone
Benign Mucous Membrane Pemphigoid
Oral Allergic Reactions
• Cinnamon/Toothpaste/Preservatives 59• Drug Lichenoid 53• Dental Restorative Materials 45• Non specific 11
Types of Allergic Reactions (BCD, January 2004)
Allergic Contact Stomatitis
• Acute–Burning, erythema
• Chronic–Erythematous or white
Oral Allergic Reactions
• Clinical:– Involvement of cheek and tongue on same side– Gingival desquamation
• Signs of Dentifrice Allergy
– Generalized or localized gingivitis (desquamativegingivitis)
–Mucositis/glossitis– Cheilitis– Lip edema– Perioral dermatitis
Toothpaste Hypersensitivity
• Flavoring agents as sensitizers:– Cinnamon oil– Cinnamic aldehyde–Menthol (also in pepermint)–Mint/Spearmint– Eugenol (from eucalyptus oil)– Essential oils– L-carvone– Anethole
Toothpaste Hypersensitivity

Xerostomia
• Subjective sensation of a dry mouth• Common problem and in 25% of older
adults• Multiple causes• Complications: – Candidiasis– Prone to cervical and root caries– Alteration of taste
Common Causes for Xerostomia
• Medications• Caffeine/alcohol• Smoking• Radiation therapy to head and neck• Sjögren’s syndrome• Primary Biliary cirrhosis• Diabetes mellitus• Sarcoidosis• Surgery of salivary glands
Diagnosis of Xerostomia
• A positive response to any of the following questions has been associated with reduced saliva:– Does the amount of saliva in your mouth seem to be
too little?– Does your mouth feel dry when eating a meal?– Do you sip liquids to aid in swallowing dry food?– Do you have difficulty swallowing?
(Plemons et al 2014)
Clinical Signs and Symptoms of Xerostomia
• Teeth– Increased incidence of tooth decay (cervical and
incisal)– Enamel demineralization (chalky spots at the cervical
regions of the teeth)– Increased plaque accumulation– Enamel erosion and attrition– Increased tooth hypersensitivity
(Plemons et al 2014)
• Oral mucosa:– Mucositis– Mucosal desquamation– Atrophic mucosa– Allergic or contact stomatitis and lichenoid lesions
(mostly opposing metal restoration)– Recurrent oral candidiasis– Traumatic ulcerations on the lateral border of the
tongue and buccal mucosa– Painful or burning mouth
Clinical Signs and Symptoms of Xerostomia
(Plemons et al 2014)
Clinical Signs and Symptoms of Xerostomia
• Tongue– Dryness, fissuring, lobulation– Atrophy– Erythema– Loss of papillae– Crenations on tongue (scalloped borders)
Clinical Signs and Symptoms of Xerostomia
• Lips– Dryness, chapping– Peeling– Fissuring– Angular cheilitis
Clinical Signs and Symptoms of Xerostomia
• Major salivary glands– Poor salivary output– Frothy saliva– Absent or reduced salivary pooling– Swelling and enlargement of salivary glands– Recurrent sialadenitis affecting major salivary glands
• Oral cavity– Oral allergic or contact reactions– Halitosis– Difficulty talking, chewing or swallowing – Plaque accumulation– Altered taste– Food retention and debris on the teeth or tongue or
along gingival margins• Other– Dry eye accompanied by dry mouth (Sjogren syndrome)
Clinical Signs and Symptoms of Xerostomia
Management of Xerostomia• Patient education–Meticulous oral hygiene regimen– Elimination of alcohol, smoking, caffeine
consumption–Maintaining adequate hydration
• Management of systemic conditions and medication use in consultation with patient’s physician/oncologist
• Salivary stimulants (sialagogues): pilocarpine(Salagen), cevimeline (Evoxac)
Management of Xerostomia
• Sugarless candies, gum• Oral lubricants (mouthwash, gels, spray)• Candidiasis prevention and control • Patients with dry mouth, dry eyes and salivary
gland enlargement should be evaluated for Sjogren’s syndrome– 16-fold increased risk of developing lymphoma
• Oral lubricants– Xylimelts– Dentiva– Salese– Oramoist
• Sialagogues:Rx Pilocarpine (Salagen) 5 mg tablets
Disp: 120 tabletsSig: one tablet PO qid
Rx Cevimeline (Evoxac) 30 mg capsulesDisp: 90 capsulesSig: one capsule PO tid
Management of Xerostomia

Geographic tongue
• “Erythema migrans”• “Benign migratory glossitis”• Common• Unknown etiology
Geographic tongue• Clinical– 2/3 females– Dorsal and lateral tongue– Depapillated erythematous patch surrounded by a
yellow-white border– Heal spontaneously and recur at different site– Often associated with fissured tongue
Geographic tongue
• Treatment: Only for symptomatic patients– Topical corticosteroids
Rx Fluocinonide gel or cream 0.05% (Lidex)Disp: 15 or 30 gram tubeSig: Dry the area and apply a small amount 3-4x/day. Do not eat or drink for one hour after application
Rx Clobetasol 0.05% gel (Temovate)Disp: 15 gram tubeSig: Dry the area and apply a small amount 3-4x/day. Do not eat or drink for one hour after application.
– Zinc supplement: 220 mg daily
Pharmacologic Therapy for Common Oral Mucosal
Conditions
Anti-inflammatory/Immunosuppressants
• High Potency Topical Corticosteroids– Fluocinonide 0.05% (Lidex)– Fluocinolone 0.20% (Synalar HP)– Triamcinolone Acetonide 0.5% (Aristocort Kenalog)
• Kenalog in orabase 0.1%
– Desoximetasone 0.25% (Topicort)
• Highest Potency Topical Steroids– Clobetasol propionate 0.05% (Temovate)– Betamethasone dipropionate 0.05%
(Diprolene)– Halobetasol propionate ointment 0.05%
(Ultravate)
Anti-inflammatory/Immunosuppressants
Rx Fluocinonide gel or cream 0.05% (Lidex)Disp: 15 or 30 gram tubeSig: Dry the area and apply a small amount 3-4x/day. Do not eat or drink for one hour after application.
Rx Bethametasone dipropionate gel 0.05%Disp: 15 gmSig: Apply sparingly to affected areas bid
Rx Decadron Elixir 0.5mg/5mlDisp: two 100 ml bottlesSig: Rinse with 1 tsp for 3-4 min and expectorate after meals and at bedtime
Anti-inflammatory/Immunosuppressants

Rx Clobetasol 0.05% gel (Temovate)Disp: 15 gram tubeSig: Dry the area and apply a small amount 3-4x/day. Do not eat or drink for one hour after application.
Rx Prednisone 10 mg tabletDisp: 40 tabsSig: Two tabs bid x 7 days, then 1 tab bid X 4 days, the 1 tab daily until gone
Rx Amlexanox oral paste 5% (Aphthasol)Disp: 5 gmSig: Apply to affected area qid
Anti-inflammatory/Immunosuppressants
Antifungals
• Topical antifungal therapyRx: Nystatin (Mycostatin, Nilstat) oral suspension 100,000 U/mLDisp: 240 mlSig: Rinse with 1 tsp. qid for 3 min by the clock. Expectorate.
Clotrimazole (Mycelex) Troche 10 mg Disp: 70Sig: Dissolve one troche slowly in mouth 5Xs daily for 14 days.

Antifungals• Systemic antifungal therapy
Rx: Fluconazole (Diflucan) tablets 100 mg Disp: 15 tabletsSig: Take 2 tablets on day 1, then 1 tablet daily
Antifungals
• Angular cheilitisRx: Ketoconazole (Nizoral) crm 2%Disp: 15 g tubeSig: Apply sparingly to corners of mouth after meals and before bed
Nystatin & triamcinolone acetonide ointment (Mycolog II, Mytrex) ointment Disp: 15 g tubeSig: Apply to affected sites after meals and before bed
Polymyxin B/Bacitracin (Polysporin) ointment (OTC)Disp: 15 g tubeSig: Apply to affected sites after meals and before bed.
Antifungals
• Treatment of dentures in patients with Candidiasis• Reinfection can occur if denture is not also treated• Options include soaking denture in 1:10 solution of
sodium hypochlorite & water overnight 3 times during treatment
Antivirals
• Primary Herpes– Systemic antiviral therapy
Rx: Acyclovir capsules 200 mgDisp: 42 capsulesSig: Take 2 capsules 3 times a day
Rx: Valacyclovir HCL (Valtrex) 1000 mg or Famciclovir(Famvir) 500 mgDisp: 14 capsSig: Take I caplet twice a day
• Recurrent Herpes– Treat during prodromal symptoms
• Topical antiviral therapyRx: Penciclovir cream 1%Disp: 1 tubeSig: Apply to area every 2 hours for 4 days, beginning with first symptoms
Antivirals
• Recurrent Herpes– Treat during prodromal symptoms
• Systemic antiviral therapyRx: Valacyclovir HCL (Valtrex) 1000 mgDisp: 4 capletsSig: Take 2 caplets at first sign of a cold sore, then 2 caplets 12 hours later
Rx: Famciclovir (Famvir) 500 mgDisp: 3 tabletsSig: Take 3 tablets as a single dose
Antivirals
Symptomatic Relief
Rx Mix Dimetapp Elixir 40 mlKaopectate 80 ml
Distilled water 120 mlSig: Rinse with 1 tsp and expectorate as
needed
Rx Benzocaine in Orabase OTC*Rx Xylocaine Viscous 2%*Disp: 100 mlSig: Rinse with 1 tsp as needed and expectorate
*Attention: Vicous lidocaine and topical benzocaine should be avoided in pediatric patients because of reports of lidocaine-induced seizures in children and an association between topical benzocaine and methemoglobinemia.
Symptomatic Relief
References• Eisen D. The clinical features, malignant potential, and systemic associations of oral
lichen planus; a study of 723 patients. J AM Acad Dermatol 2002; 46(2):207-14.• Lodi G, Scully C, Carrozzo M, Griffiths M, Sugerman PB, Thongprasom K. Current
controversies in oral lichen planus: report of an international consensus meeting. Part 2. Clinical management and malignant transformation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;100(2):164-78.
• Lozada-Nur F, Miranda C. Oral lichen planus: epidemiology, clinical characteristics, and associated diseases. Semin Cutan Med Surg 1997;16(4):273-7.
• Al-Hashimi I, Schifter M, Lockhart PB, Wray D, Brennan M, Migliorati CA, et al. Oral lichen planus and oral lichenoid lesions: diagnostic and therapeutic considerations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103 Suppl:S25 e1-12.
• Markopoulos AK, Antoniades D, Papanayotou P, Trigonidis G. Malignant potential of oral lichen planus; a follow-up study of 326 patients. Oral Oncol 1997;33(4):263-9.
• Lo Muzio L, Mignogna MD, Favia G, Procaccini M, Testa NF, Bucci E. The possible association between oral lichen planus and oral squamous cell carcinoma: a clinical evaluation on 14 cases and a review of the literature. Oral Oncol 1998;34(4):239-46.

• Fang M, Zhang W, Chen Y, He Z. Malignant transformation of oral lichen planus: a retrospective study of 23 cases. Quintessence Int 2009;40(3):235-42.
• Gandolfo S, Richiardi L, Carrozzo M, Broccoletti R, Carbone M, Pagano M, et al. Risk of oral squamous cell carcinoma in 402 patients with oral lichen planus: a follow-up study in an Italian population. Oral Oncol 2004;40(1):77-83.
• van der Meij EH, Schepman KP, Smeele LE, van der Wal JE, Bezemer PD, van der Waal I. A review of the recent literature regarding malignant transformation of oral lichen planus. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;88(3):307-10.
• Miller RL et al. Oral Surg Oral Med Oral Pathol 1992; 73:708-716.• Allen CM and Blozis GG. J Am Dent Assoc 1988; 115:664-667.• Issa Y et al. Br. Dent J. 2005;198:361-366.• Moller H. Contact Dermatitis 2002;47:63-66.• Scully C et al. Update on mucous membrane pemphigoid. Oral Surg Oral Med Oral
Pathol 1999; 88:56-68.• Bagan J et al. Number III mucous membrane pemphigoid. Oral Dis 2005;11:197-218
References