Embed Size (px)
Citation preview
CLINICAL COMMUNICATION
Contact lens management of keratoconus in a patient with residualastigmatism resulting from implantation of a toric intraocular lens
Clin Exp Optom 2013; 96: 238–241 DOI:10.1111/cxo.12036
Richard G Lindsay* BScOptom MBAFAAO(DipCL) FCCLSA FACOBenjamin J Connell† BMBS FRANZCOMPHGrant R Snibson†§ MBBS FRACSFRANZCO FRCOphth FAICD* Private Practice, Melbourne, Victoria, Australia† Royal Victorian Eye & Ear Hospital, Melbourne,Victoria, Australia§ Centre for Eye Research Australia, The University ofMelbourne, Melbourne, Victoria, AustraliaE-mail: [email protected]
Toric intraocular lenses (IOLs) are increasingly being used at the time of cataract surgery totreat regular refractive astigmatism. This paper outlines the contact lens management of apatient with keratoconus, who had marked residual astigmatism post-operatively due toimplantation of a toric IOL during cataract surgery. It is strongly recommended that toricIOLs should only be prescribed for patients who have mild forms of keratoconus, with onlyslight irregular astigmatism that has been stable for at least the previous 12 months andacceptable vision with spectacles.
Submitted: 16 October 2012Revised: 28 November 2012Accepted for publication:4 December 2012
Key words: cataract, contact lens, keratoconus, residual astigmatism, toric intraocular lens
The contact lens correction of residual astig-matism in a patient with keratoconus, whois required to wear rigid gas-permeablecontact lenses due to the significant natureof their condition, will increase the complex-ity of the contact lens fitting. This paperoutlines the contact lens management of apatient with keratoconus who had signifi-cant residual astigmatism post-operativelydue to implantation of a toric intraocularlens (IOL) during cataract surgery.
CASE REPORT
A 48-year-old female patient presented withthe complaint of blurred vision inher right eye following cataract surgerynine months earlier. Her ocular history wasnotable for having been diagnosed with bothmyopia (when she was nine) and kerato-conus (in her early 20s). Soft contact lenseshad been worn on a full-time basis from theage of 18 to 22, at which time she was refittedwith rigid gas-permeable contact lenses, asshe was no longer able to achieve acceptablevision with either spectacles or soft contactlenses. The patient also had suffered a
retinal detachment in her right eye in 1986that was treated with cryotherapy and ascleral buckle, as well as retinal holes in herleft eye that were treated with cryotherapy in1992 and 1994.
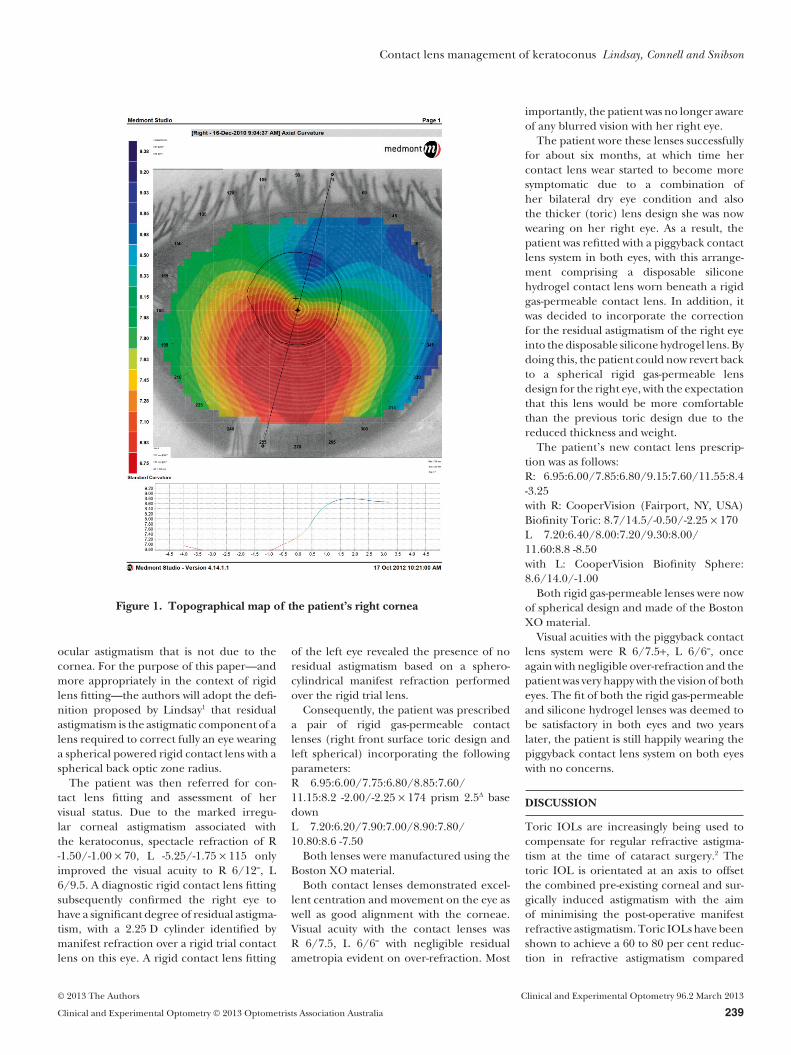
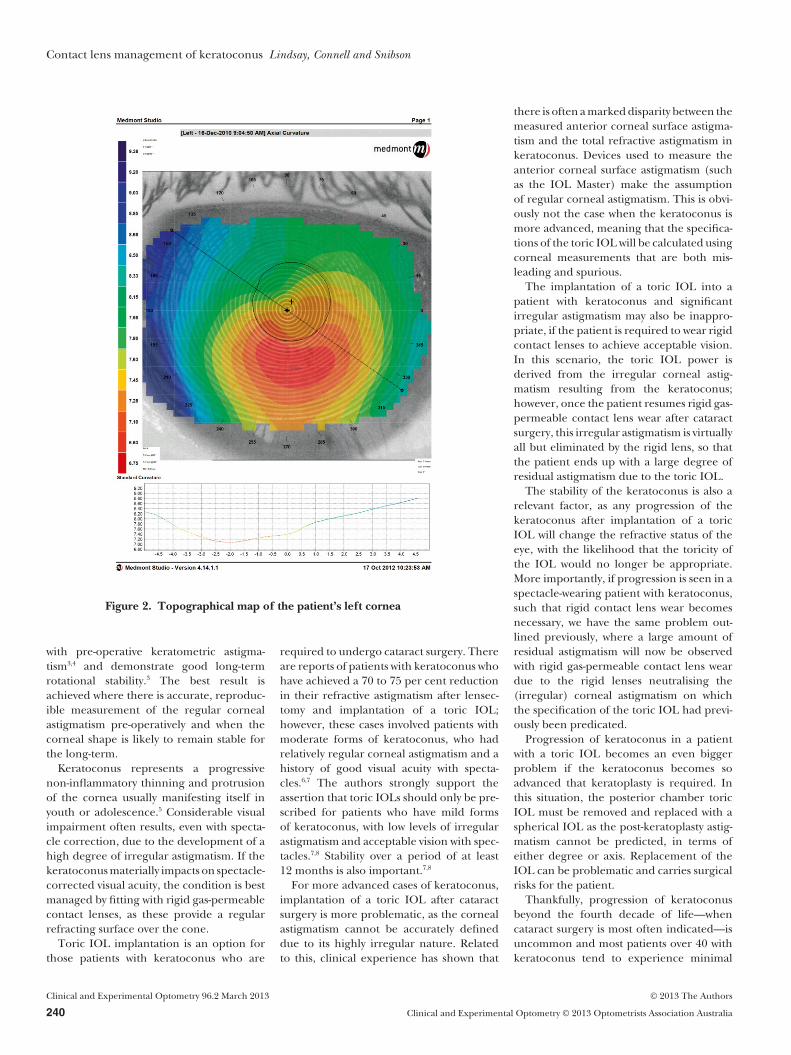
Examination at presentation revealedmoderate bilateral keratoconus, slightlymore advanced in the right eye. This wasconfirmed by videokeratoscopy (Figures 1and 2) with the E300 Corneal Topographer(Medmont Pty Ltd, Melbourne, Victoria,Australia) that showed sagging (oval) conesin both eyes. A posterior chamber intra-ocular lens was observed in the right eye,while the crystalline lens of the left eye wasstill relatively clear. No corneal scarring wasnoted, although the patient was observedto have a mild tear film dysfunction bilater-ally. Dilated fundus examination revealedhealthy optic nerves and maculae.
Further investigation revealed that thepatient’s cataract surgery on the right eyenine months earlier had involved an un-eventful phacoemulsification followed byimplantation of a posterior chamber toricIOL (Staar AA403TL +10.5/+3.5 D) into thecapsular bag with the lens selection and ori-
entation based on ocular biometry per-formed with the IOLMaster 500 (Carl ZeissMeditec, Jena, Germany). Slitlamp examina-tion estimated the IOL to be positionedwithin five degrees of the specified axis. Post-operatively the patient had noticed that hervisual acuity with the right eye wearing a rigidgas-permeable contact lens was now blurred,despite the spherical power of the contactlens being modified to take into accountthe change in the patient’s spherical equiva-lent brought about by the insertion ofthe IOL. Subsequent yttrium aluminumgarnet (YAG) laser posterior capsulotomyabout four months after the cataract surgerydid not bring about any significant improve-ment in the visual acuity of this eye.
It was postulated that the blurred vision inthe right eye was probably not due to theslight misalignment of the toric IOL butrather the result of residual astigmatismcreated by the implantation of a toric IOL inan eye, which had keratoconus (and there-fore a significant degree of irregular cornealastigmatism). Note that the term ‘residualastigmatism’ can be defined in various ways,most commonly as the component of the
C L I N I C A L A N D E X P E R I M E N T A L
OPTOMETRY
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
238 Clinical and Experimental Optometry © 2013 Optometrists Association Australia
ocular astigmatism that is not due to thecornea. For the purpose of this paper—andmore appropriately in the context of rigidlens fitting—the authors will adopt the defi-nition proposed by Lindsay1 that residualastigmatism is the astigmatic component of alens required to correct fully an eye wearinga spherical powered rigid contact lens with aspherical back optic zone radius.
The patient was then referred for con-tact lens fitting and assessment of hervisual status. Due to the marked irregu-lar corneal astigmatism associated withthe keratoconus, spectacle refraction of R-1.50/-1.00 ¥ 70, L -5.25/-1.75 ¥ 115 onlyimproved the visual acuity to R 6/12=, L6/9.5. A diagnostic rigid contact lens fittingsubsequently confirmed the right eye tohave a significant degree of residual astigma-tism, with a 2.25 D cylinder identified bymanifest refraction over a rigid trial contactlens on this eye. A rigid contact lens fitting
of the left eye revealed the presence of noresidual astigmatism based on a sphero-cylindrical manifest refraction performedover the rigid trial lens.
Consequently, the patient was prescribeda pair of rigid gas-permeable contactlenses (right front surface toric design andleft spherical) incorporating the followingparameters:R 6.95:6.00/7.75:6.80/8.85:7.60/11.15:8.2 -2.00/-2.25 ¥ 174 prism 2.5D basedownL 7.20:6.20/7.90:7.00/8.90:7.80/10.80:8.6 -7.50
Both lenses were manufactured using theBoston XO material.
Both contact lenses demonstrated excel-lent centration and movement on the eye aswell as good alignment with the corneae.Visual acuity with the contact lenses wasR 6/7.5, L 6/6= with negligible residualametropia evident on over-refraction. Most
importantly, the patient was no longer awareof any blurred vision with her right eye.
The patient wore these lenses successfullyfor about six months, at which time hercontact lens wear started to become moresymptomatic due to a combination ofher bilateral dry eye condition and alsothe thicker (toric) lens design she was nowwearing on her right eye. As a result, thepatient was refitted with a piggyback contactlens system in both eyes, with this arrange-ment comprising a disposable siliconehydrogel contact lens worn beneath a rigidgas-permeable contact lens. In addition, itwas decided to incorporate the correctionfor the residual astigmatism of the right eyeinto the disposable silicone hydrogel lens. Bydoing this, the patient could now revert backto a spherical rigid gas-permeable lensdesign for the right eye, with the expectationthat this lens would be more comfortablethan the previous toric design due to thereduced thickness and weight.
The patient’s new contact lens prescrip-tion was as follows:R: 6.95:6.00/7.85:6.80/9.15:7.60/11.55:8.4-3.25with R: CooperVision (Fairport, NY, USA)Biofinity Toric: 8.7/14.5/-0.50/-2.25 ¥ 170L 7.20:6.40/8.00:7.20/9.30:8.00/11.60:8.8 -8.50with L: CooperVision Biofinity Sphere:8.6/14.0/-1.00
Both rigid gas-permeable lenses were nowof spherical design and made of the BostonXO material.
Visual acuities with the piggyback contactlens system were R 6/7.5+, L 6/6=, onceagain with negligible over-refraction and thepatient was very happy with the vision of botheyes. The fit of both the rigid gas-permeableand silicone hydrogel lenses was deemed tobe satisfactory in both eyes and two yearslater, the patient is still happily wearing thepiggyback contact lens system on both eyeswith no concerns.
DISCUSSION
Toric IOLs are increasingly being used tocompensate for regular refractive astigma-tism at the time of cataract surgery.2 Thetoric IOL is orientated at an axis to offsetthe combined pre-existing corneal and sur-gically induced astigmatism with the aimof minimising the post-operative manifestrefractive astigmatism. Toric IOLs have beenshown to achieve a 60 to 80 per cent reduc-tion in refractive astigmatism compared
Figure 1. Topographical map of the patient’s right cornea
Contact lens management of keratoconus Lindsay, Connell and Snibson
© 2013 The Authors Clinical and Experimental Optometry 96.2 March 2013
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 239
with pre-operative keratometric astigma-tism3,4 and demonstrate good long-termrotational stability.3 The best result isachieved where there is accurate, reproduc-ible measurement of the regular cornealastigmatism pre-operatively and when thecorneal shape is likely to remain stable forthe long-term.
Keratoconus represents a progressivenon-inflammatory thinning and protrusionof the cornea usually manifesting itself inyouth or adolescence.5 Considerable visualimpairment often results, even with specta-cle correction, due to the development of ahigh degree of irregular astigmatism. If thekeratoconus materially impacts on spectacle-corrected visual acuity, the condition is bestmanaged by fitting with rigid gas-permeablecontact lenses, as these provide a regularrefracting surface over the cone.
Toric IOL implantation is an option forthose patients with keratoconus who are
required to undergo cataract surgery. Thereare reports of patients with keratoconus whohave achieved a 70 to 75 per cent reductionin their refractive astigmatism after lensec-tomy and implantation of a toric IOL;however, these cases involved patients withmoderate forms of keratoconus, who hadrelatively regular corneal astigmatism and ahistory of good visual acuity with specta-cles.6,7 The authors strongly support theassertion that toric IOLs should only be pre-scribed for patients who have mild formsof keratoconus, with low levels of irregularastigmatism and acceptable vision with spec-tacles.7,8 Stability over a period of at least12 months is also important.7,8
For more advanced cases of keratoconus,implantation of a toric IOL after cataractsurgery is more problematic, as the cornealastigmatism cannot be accurately defineddue to its highly irregular nature. Relatedto this, clinical experience has shown that
there is often a marked disparity between themeasured anterior corneal surface astigma-tism and the total refractive astigmatism inkeratoconus. Devices used to measure theanterior corneal surface astigmatism (suchas the IOL Master) make the assumptionof regular corneal astigmatism. This is obvi-ously not the case when the keratoconus ismore advanced, meaning that the specifica-tions of the toric IOL will be calculated usingcorneal measurements that are both mis-leading and spurious.
The implantation of a toric IOL into apatient with keratoconus and significantirregular astigmatism may also be inappro-priate, if the patient is required to wear rigidcontact lenses to achieve acceptable vision.In this scenario, the toric IOL power isderived from the irregular corneal astig-matism resulting from the keratoconus;however, once the patient resumes rigid gas-permeable contact lens wear after cataractsurgery, this irregular astigmatism is virtuallyall but eliminated by the rigid lens, so thatthe patient ends up with a large degree ofresidual astigmatism due to the toric IOL.
The stability of the keratoconus is also arelevant factor, as any progression of thekeratoconus after implantation of a toricIOL will change the refractive status of theeye, with the likelihood that the toricity ofthe IOL would no longer be appropriate.More importantly, if progression is seen in aspectacle-wearing patient with keratoconus,such that rigid contact lens wear becomesnecessary, we have the same problem out-lined previously, where a large amount ofresidual astigmatism will now be observedwith rigid gas-permeable contact lens weardue to the rigid lenses neutralising the(irregular) corneal astigmatism on whichthe specification of the toric IOL had previ-ously been predicated.
Progression of keratoconus in a patientwith a toric IOL becomes an even biggerproblem if the keratoconus becomes soadvanced that keratoplasty is required. Inthis situation, the posterior chamber toricIOL must be removed and replaced with aspherical IOL as the post-keratoplasty astig-matism cannot be predicted, in terms ofeither degree or axis. Replacement of theIOL can be problematic and carries surgicalrisks for the patient.
Thankfully, progression of keratoconusbeyond the fourth decade of life—whencataract surgery is most often indicated—isuncommon and most patients over 40 withkeratoconus tend to experience minimal
Figure 2. Topographical map of the patient’s left cornea
Contact lens management of keratoconus Lindsay, Connell and Snibson
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
240 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

changes in their corneal curvature.5,9 Whilestability of the keratoconus could not bedocumented for the patient in this casereport, it was noted that the patient had notrequired refitting in either eye for threeyears prior to the cataract surgery on herright eye.
In routine contact lens practice, residualastigmatism will only very occasionally needto be corrected in cases where the patient isfitted well with a rigid gas-permeable contactlens using a spherical back optic zone.Therefore, such a lens requires a toroidalfront surface and lens rotation must beavoided, otherwise visual disturbance willresult. Consequently, rigid lenses with aspherical back optic zone and a toroidalfront surface (front surface toric lenses) willgenerally incorporate some form of lens sta-bilisation, such as prism ballast or trunca-tion. Prism ballast is the most commonlyused method of lens stabilization—as in thiscase—with anywhere between one and threeprism dioptres of base-down prism beingincorporated into the lens.1 Unfortunately,for patients with significant keratoconus, atoroidal back optic zone cannot be used tostabilise the lens, as it will not align well onthe irregular (conical) cornea.1
Prism ballasting can often cause rigidlenses to sit inferiorly, resulting in patientsexperiencing symptoms of discomfort andflare. Hence, trying to correct for residualastigmatism by means of a front surface toricrigid gas-permeable lens in advanced casesof keratoconus can be quite problematic,especially if the patient has a sagging (oroval) cone. In this situation, an alternativesolution is simply to incorporate the correc-tion for the residual astigmatism into a spec-tacle prescription, which is worn over thecontact lens.
Another possible option when a patientwith keratoconus has residual astigmatism isto use a piggyback contact lens system. Thissystem would consist of a toric soft contactlens (usually a disposable silicone hydrogellens) to correct for the residual astigma-tism worn underneath a rigid gas-permeablelens.10 Piggyback contact lens systems aregenerally used in contact lens practice whenfitting with just a rigid gas-permeable lensmay lead to areas of significant corneal insultdue to an underlying ocular surface diseaseand/or a highly irregular cornea. Placing asoft lens under the rigid gas-permeable lenshelps to protect the cornea from any exces-sive lens bearing, thereby minimising thepossibility of complications associated with
contact lens wear and also greatly improvingcontact lens comfort.11 There is also the addi-tional advantage, as demonstrated here, ofbeing able to incorporate the correctionfor residual astigmatism into the (toric) softlens, so that the rigid gas-permeable lens canbe spherical and therefore not require any ofthe lens stabilisation features that may makethe lens less comfortable on the eye.
Concern is often expressed as to whetherthe oxygen transmissibility (Dk/t) through apiggyback contact lens system can reach thelevel required to avoid hypoxic stress to thecornea during daily wear.12 Weissman andYe13 have calculated that under open-eyeconditions, the oxygen supply to the corneais sufficient when both rigid gas-permeableand soft lenses have been manufacturedfrom materials that have oxygen permeabili-ties (Dk) greater than 60 Barrer. The piggy-back contact lens system prescribed for thepatient in this report incorporated a rigidlens manufactured from the Boston XOmaterial (Dk of 100 Barrer) and the dispos-able soft Biofinity lens (Dk of 128 Barrer).The thicker, toric soft lens for the right eyewould have a lower oxygen transmissibilitythan a spherical lens with a power equal tothe spherical equivalent of the toric lens;however, given the very high Dk of the lensmaterial, it would be expected that the pig-gyback system for this patient would stilladequately meet the Holden-Mertz criterionfor daily wear.12
CONCLUSION
This case highlights an important issue intoric IOL implantation at the time of cata-ract surgery in patients with keratoconuswho wear, or are likely to wear, rigid gas-permeable contact lenses. In fact, the sameissue needs to be considered in any patientundergoing cataract surgery, who has sig-nificant irregular corneal astigmatism. Atoric IOL provides the potential benefitof a reduction in refractive astigmatismand the secondary benefits of less specta-cle lens-induced image distortion (due tolower differential meridional magnifica-tion) and increased spectacle independ-ence. Notwithstanding these potentialbenefits, consideration needs to be givenpre-operatively to refractive difficulties thatmay result. As highlighted by this case,contact lens fitting may become complexand problematic, if significant residualastigmatism is present.
REFERENCES1. Lindsay RG. Toric rigid lens fitting. In: Efron N,
ed. Contact Lens Practice. 2nd ed. London:Butterworth-Heinemann, 2010.
2. Buckhurst PJ, Wolffsohn JS, Davies LN, Naroo SA.Surgical correction of astigmatism during cataractsurgery. Clin Exp Optom 2010; 93: 409–418.
3. Food and Drug Administration. Summary Informa-tion for: ACRYSOF® Toric Posterior ChamberIntraocular Lens—930014/S015—P930014/S015.US Food and Drug Administration [serial online]2005. Accessed August 5, 2012.
4. Statham M, Apel A, Stephensen D. Comparison ofthe AcrySof SA60 spherical intraocular lens and theAcrySof Toric SN60T3 intraocular lens outcomesin patients with low amounts of corneal astigma-tism. Clin Experiment Ophthalmol 2008; 37: 775–779.
5. Rabinowitz YS. Keratoconus. Surv Ophthalmol 1998;42: 297–319.
6. Visser N, Gast ST, Bauer NJ, Nuijts RM. Cataractsurgery with toric intraocular lens implantation inkeratoconus: a case report. Cornea 2011; 30: 720–723.
7. Jaimes M, Xacur-Garcia F, Alvarez-Melloni D,Graue-Hernandez EO, Ramirez-Luquin T, Navas A.Refractive lens exchange with toric intraocularlenses in keratoconus. J Refract Surg 2011; 27: 658–664.
8. Satjawatcharaphong P, Edrington TB. Toricintraocular lenses and keratoconus. Contact LensSpectrum 2012; 27: 21.
9. McMahon TT, Edrington TB, Szczotka-Flynn L,Olafsson HE, Davis LJ, Schechtman KB, CLEKStudy Group. Longitudinal changes in cornealcurvature in keratoconus. Cornea 2006; 25: 296–305.
10. Larson B, Edrington TB. Piggybacking with softtorics. Contact Lens Spectrum 2010; 25: 14.
11. Szczotka LB, Lindsay RG. Contact lens fitting fol-lowing corneal graft surgery. Clin Exp Optom 2003;86: 244–249.
12. Holden BA, Mertz G. Critical oxygen levels toavoid corneal oedema for daily and extended wearcontact lenses. Inv Ophthalmol Vis Sci 1984; 25:1161–1167.
13. Weissman BA, Ye P. Calculated tear oxygen tensionunder contact lenses offering resistance in series:piggyback and scleral lenses. Cont Lens Anterior Eye2006; 29: 231–237.
Contact lens management of keratoconus Lindsay, Connell and Snibson
© 2013 The Authors Clinical and Experimental Optometry 96.2 March 2013
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 241





























