Embed Size (px)
Citation preview

Considerations for
Resuming Visiting for Older Adults
in Hospital and Congregate Settings
amid COVID-19
FINAL
June 12, 2020
Special thanks to the following for sharing their documents and ideas:
The Hospital for Sick Children
North East Specialized Geriatric Centre / Health Sciences North

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 1
INTRODUCTION
In May 2020, the NSM SGS program released a discussion paper entitled “The Need for a Multi-
Dimensional Strategy to Address the Care of Older Adults & Their Caregivers in COVID-19”.
Within that paper, a strategy is proposed to better support the breadth of needs of older adults
and their caregivers during COVID-19. The strategy is based on four dimensions:
Dimension 1 – COVID-19: The Disease
Dimension 2 – Urgent Non-COVID Issues
Dimension 3 – Impact of COVID-19 Restrictions
Dimension 4 – Broader Impact of COVID-19
Dimension 3 includes a focus on the impact of social isolation in older adults, including
recommendations regarding the lifting of visiting restrictions for older adults in hospital and
congregate settings. COVID-19 visiting restrictions were implemented in these settings in mid-
March and have had a significant impact on the health and well-being of older adults and their
caregivers. On June 11 2020, the government updated Directive #3 and released guidelines to
begin re-opening RHs and to resume visiting in LTCHs and other congregate settings.
With much research already underway on this topic prior to the provincial announcements on
June 11, the NSM SGS program thought it would be helpful to share the information with local
health service providers to support planning and discussion around policies and practices
related to older adults.
CONSIDERING THE ENVIRONMENT
Recent news and social media has been focused on the COVID-19 imposed visiting restrictions
across hospitals and congregate settings. It is with great relief and excitement that we see new
Ministry direction emerging!
The Importance of Restrictions
One of the fundamental considerations in the delivery of health care is safety. This is especially
true today. Health care providers continue to be focused on the most immediate concern of
COVID-19 – protecting individuals by reducing the spread.
Reducing spread is especially critical in older adults. Global, national and provincial reports
have highlighted the impact of COVID-19 on older adults. The impact has been greatest in
congregate settings like LTCH and RH settings. In an examination of international trends 1, it was
found that across 13 countries, the overall share of COVID-19 deaths that could be attributed to
care home residents ranged from a low of 19% in Hungary to a high of 62% in Canada. Key
1 Comas-Herrera A, Zalakaín J, Litwin C, Hsu AT, Lane N and Fernández J-L (2020) Mortality associated with
COVID-19 outbreaks in care homes: early international evidence. Article in LTCcovid.org, International
Long-Term Care Policy Network, CPEC-LSE, 3 May 2020. https://ltccovid.org/wp-
content/uploads/2020/05/Mortality-associated-with-COVID-3-May-final-1.pdf

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 2
findings from a June 4 2020 national LTCH report 2 show:
An estimated case fatality rate of 36% (range 20 to 42%) among residents in Canadian
long-term care homes.
Deaths in long-term care residents currently represent up to 85% of all COVID-19 deaths
in Canada.
Visiting restrictions reduce the risk to older adults by limiting contact with potential symptomatic
and asymptomatic individuals from the community. In so doing, the restrictions reduce
morbidity, mortality and associated costs to the health care system. At June 7 2020, the
National Institute on Aging LTC COVID-19 Tracker 3 reported 416 affect homes, 9,430 COVID-19
positive cases and 1,932 deaths in Ontario. These volumes are overwhelming. The number of
COVID-19 related cases and deaths would likely have been much worse if facilities across the
province had not implemented strict visiting restrictions in mid-March.
Implications:
It will be integral to continue to protect older adults in hospital and congregate
settings through thoughtful and strategic visiting policies. Finding the right balance
for ‘safety’ will be critical – protection from the disease vs the impact on the health
and well-being of the older adult. This balance will become more difficult to find in
the coming weeks with the concurrent direction to open LTCHs and RHs to
admissions.
A Commentary on “Visitors”
Before we go too far in this document, there is a need to address the value of visitors. Visitors are
incredibly important to the health and well-being of older adults in hospitals and congregate
settings. In addition to supporting their physical, mental and emotional health, “visitors” are their
voices, their advocates and their essential partners in care.
To promote safety during COVID-19 a blanket approach to visiting restrictions was implemented,
limiting visitors to exceptional circumstances. There are several important pieces to consider in
this. First, because of restrictions, the vast majority of older adults have been alone, separated
from family and friends. While Ministry direction did allow visiting in exceptional circumstances
many organizations restricted all visitors.
Second, in implementing a blanket approach, the health system treated all visitors the same.
While all visitors to hospitals or congregate settings may be “outsiders” to the operations of the
organization, one could argue that not all are visitors by definition. According to Meriam-
Webster, a visitor is one who visits. The word is synonymous with caller, drop-in, frequenter and
2 Amy T. Hsu, Natasha Lane, Samir K. Sinha, Julie Dunning, Misha Dhuper, Zaina Kahiel, Heidi Sveistrup.
Report: Understanding the impact of COVID-19 on residents of Canada’s long-term care homes – ongoing
challenges and policy responses. p.2. International LTC Policy Network (June 4 2020).
https://ltccovid.org/wp-content/uploads/2020/06/LTCcovid-country-reports_Canada_June-4-2020-1.pdf
Accessed 7 Jun. 2020. 3 NIA Long-Term Care COVID-19 Tracker. https://ltc-covid19-tracker.ca/ Accessed 7 Jun. 2020

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 3
guest. Google shows the definition of visitor as being “a person visiting a person or place,
especially socially or as a tourist”. While many of the visitors within hospitals and congregate
settings may be ‘callers’ or ‘social drop-ins’, most are close family and friends who are important
to an older adult’s sense of meaning and purpose. Still others are essential caregivers. The role
they play in delivering care may be equal in importance to that provided by formal health
service providers. In many cases, it may be more important. We, in truth, shut the door to not
just visitors, but to important care partners and essential caregivers.
Third, in pediatrics the physical presence of parents and guardians is an expectation. Many
would argue there should be a similar expectation in the case of older adults and their
caregivers, especially when the abilities of older adults are impaired and they rely of their
caregivers for support.
Finally, in higher risk settings like hospitals and congregate settings, movement has been limited
in and out of the building for months for both visitors and older adults. The only movement in/out
has been staff and essential workers. As such, new initial cases in these settings since April
started with community-transmission (someone bringing it in). Visitors are at equal risk to
acquiring COVID-19 in the community as staff and essential workers. Precautions have been put
in place (i.e. screening, PPE, testing, etc.) to reduce the risk of community-transmission.
Implications:
Exceptional circumstances will continue. Organizations need to consider how to
incorporate this into policy to ensure all older adults have access to, at minimum
essential caregivers, at all times.
Policy and practices need to once again enable the important role of caregivers.
It would be important to build in and recognize the various types of visitors (essential
caregivers, important care partners, visitors) and align roles, expectations and
restrictions accordingly.
Expectations and limitations placed around parents and guardians in pediatric
environments should be comparable to expectations and limitations for older adults
and their essential caregivers, especially when the abilities of the older adult is
impaired and they rely on that caregiver for support.
The precautions and training established to reduce the risk of community transmission
from staff/essential workers to older adults could be applied to essential caregivers.
Appreciating the Impact of 3 months of Restrictions
The Experience of the Older Adult
As per the Regional Geriatric Program of Toronto’s Senior Friendly 7 toolkit, social engagement is
defined as an “involvement in meaningful activities with others and maintaining close, fulfilling

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 4
relationships”4. Social isolation and loneliness, which can occur when social engagement is
compromised, can affect 5:
Physical health contributing to problems like early mortality, strokes, elevated blood
pressure and malnutrition
Mental health, leading to issues like depression, anxiety and increased risk of substance
misuse and suicide; and,
Functional status, with impact including functional decline as well as physical and/or
cognitive deterioration.
In a recent publication, people with dementia in care homes in the UK and Wales are ‘switching
off’ amid reduced medical care and family visits 6. England and Wales have seen an 83% and
54% increase respectively in deaths from dementia and Alzheimer’s Disease. Local leaders link
the increase to several causes including, “isolation, the reduction in essential care as family
carers cannot visit, and the onset of depression as people with dementia do not understand
why loved ones are no longer visiting, causing them to lose skills and independence, such as the
ability to speak or even stopping eating and drinking”. In a survey of 128 care homes by that
region’s Alzheimer’s Society, they found 79% reported the lack of social contact was negatively
impacting the health and well-being of residents with dementia with families reporting their
loved ones were feeling confused and abandoned. 79% is a shocking statistic, not because it is
so high but because it is seemingly low – begging the question whether health care providers
are appreciating the relationship between social contact and health and well-being.
Implications:
The loss of both usual routine/activities and usual caregivers (staff and families)
coupled with a reduction in the availability of staff (due to staff shortages, additional
time required for PPE) AND up to three months of social isolation has taken its toll on
many older adults. For family and friends, any deterioration will be upsetting and
maybe surprising, especially for those that have had limited virtual contact. Early
visits will likely be an emotional time for all.
The Experience of Family and Friends, including Essential Caregivers
“The familiar faces of family and friends are gone, and carers are behind masks and
can’t touch or comfort the residents,” he said. “Yvonne has lost her sparkle, she’s in a
world she doesn’t understand. The staff at the care home are doing an amazing job
looking after the residents, but we’ve only got video calls to keep in touch, and Yvonne
4 RGP Toronto Senior Friendly 7 Toolkit, p.79 https://www.rgptoronto.ca/wp-content/uploads/2018/04/SF7-
Toolkit.pdf. Accessed 6 Jun. 2020. 5 RGP Toronto Senior Friendly 7 Toolkit. https://www.rgptoronto.ca/wp-content/uploads/2018/04/SF7-
Toolkit.pdf. Accessed 6 Jun. 2020. 6 Extra 10,000 dementia deaths in England and Wales in April. The Guardian, Published June 5, 2020.
https://www.theguardian.com/world/2020/jun/05/covid-19-causing-10000-dementia-deaths-beyond-
infections-research-says Accessed 6 Jun. 2020.

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 5
doesn’t always understand them. If lockdown continues, I’m really fearful my wife won’t
be able to recognise me at the end of all this.” 7
Older adults rely on social engagement with their family and friends and vice versa. It is
important to shared meaning and sense of purpose. The news and social media have been
filled with stories of families desperate to visit loved ones in hospitals and congregate settings.
Standing at windows hoping to see each other. Connecting via technology. While many have
appreciated any opportunity for contact, they will all tell you it has not been enough.
Within the NSM region, our team and partners noted increased stress among caregivers who
were anxious to visit their loved ones in person. Caregivers experienced anxiety, guilt, worry and
fear. With the passing of time, frustration and anger became increasingly evident. For many,
fears were exacerbated by the military report, which raised concern about the quality of care in
five Ontario LTCH settings. While this report heightened awareness, it also became seen
mistakenly by many as a reflection of the situation present in all homes across the province.
Implications:
While most family and friends will just be happy to return, some will come back into
facilities fearful, cautious, observant (especially given the military report) and maybe
even angry. Staff should be prepared to deal with this variety of feelings and
emotions.
We need to think about how to welcome family and friends back, how to re-engage
visitors safely, how to allow essential caregivers to resume their roles and how to re-
build any relationships that may have been damaged through the imposed
restrictions.
The Impact on the Health Care System
Family and friends are critical partners. In some congregate settings, essential caregivers are
considered extended family of the setting. In hospitals and congregate settings, these
individuals attend to the needs of the older adult and contribute to their health and well-bring:
Improved function and cognitive status by promoting activity, supporting mobilization,
providing relevant cognitive stimulation.
Improved nutrition and hydration status by encouraging fluids, bringing food from home
and supporting feeding in those that may require assistance.
Early identification of changes in medical status by noticing subtle changes in baseline
abilities.
Reduced loneliness, anxiety and depression through social engagement.
Through this support, they help reduce unnecessary ED visits as well as hospital and LTC
admissions.
7 Extra 10,000 dementia deaths in England and Wales in April. The Guardian, Published June 5, 2020.
https://www.theguardian.com/world/2020/jun/05/covid-19-causing-10000-dementia-deaths-beyond-
infections-research-says Accessed 6 Jun. 2020.

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 6
The loss of visitors in hospital and congregate settings has likely affected the health and well-
being of some staff due to the loss of relationships and daily support. Some staff are new to the
settings and may not be familiar to/with the families and friends of the older adults. Amid
COVID-19, less availability of staff coupled with limited visitors means staff may, at times, have
made difficult decisions to prioritize care needs, sometimes delaying usual care in favour of
other clinical priorities. Those in LTCHs have felt the weight of the military report and the
associated public response. Many feel ‘beat up’ and undervalued despite their efforts to
provide the best care possible within the current circumstances. Staff may also be tired
because of staffing shortages, the loss of support from visitors, additional IPAC requirements and
general system stress from COVID-19. Finally, visitors are being re-introduced to an environment
that has changed with new policies and practices in place. Together, these will all affect the
quality of interaction between staff and visitors
Implications:
The mental and emotional health of staff has been impacted by COVID-19. As we
transition them from their most current norm to yet another new norm that includes
the re-introduction of visitors, consideration should be given to assessing, monitoring
and supporting their mental and emotional health and well-being.
Staff will need to be prepared for visitor re-introduction. This will include the need for
clear communication around policies and practices.
CONSIDERING MINISTRY DIRECTION & THE WORK OF OTHERS
Appendix A highlights some of the key ideas regarding visitors within provincial directives,
guidance documents and communication (at June 12, 2020). Appendix B provides a summary
of approaches to visitors from other jurisdictions and sectors. Together these offer lessons to
guide planning and next steps.
Common Themes
Provincial documents and approaches from other jurisdictions and sectors share many common
themes that can be used to guide visitor policy and practices:
Evidence of phasing, with initial phases starting with outdoor visits.
Reference to essential visitors or caregivers.
A requirement for adherence to (and education regarding) IPAC protocols, inclusive of
hand hygiene, physical distancing and PPE.
Regular screening and the passing of screens to gain entry.
The importance of developing policy to support practices.
Maintaining visitor logs to support contact tracing.
Many of these are addressed within the most recent provincial documents.
Implications:
These common themes provide a good foundation to support the development of
policies and practices for visitors of older adults in hospitals and congregate settings.

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 7
Opportunities
In reviewing all documents, including the most recent provincial ones, there are some interesting
observations and ideas that may help inform the development of policies and practices:
The concept of a visit does not take into account the breadth of a relationship between
the older adult and his/her family and friends.
o Contact for 30min in an outdoor setting with a requirement to maintain physical
distance is reflective of a social drop-in. While it will be sufficient for some, most
will struggle to be limited to this type of interaction.
o Directive #3 defines essential visitors as including a person performing essential
support services (e.g., food delivery, inspector, maintenance, or health care
services (e.g., phlebotomy)) or a person visiting a very ill or palliative resident. In
the directive, essential visitors are the only type of visitors allowed when a resident
is self-isolating or symptomatic or when a home is in outbreak. The Resumption of
Visitors in LTCHs document uses the term essential family caregiver and defines
that as people capable of providing caregiving support (feeding, social support,
etc.) and who had done this in the home prior to COVID-19. This document does
not reference essential visitors. What is clear is that if a home enters outbreak, all
non-essential visits cease, which would include those by essential family
caregivers. As such, we continue to hold the door shut to even the older adult’s
most important people.
o Providing clarity in terms and roles would be helpful. As noted in the bullet above,
the Resumption of Visiting in LTCH document uses the term essential family
caregivers as part of priority in-home visiting in phase 2. There would be benefit
to: further categorize this broad group; limit the volumes/designate individuals to
better control flow and support training/education; and align roles, expectations
and restrictions with outbreak phases. Of note, one organization required picture
identification from designated essential caregivers as they noted cards/badges
were being passed between family and friends.
While the documents take a phased approach to resumption of visiting, the focus of
phasing is tied to the outbreak status of the setting:
o While there is an assumption the reference is to COVID-19, there may be other
types of outbreaks that occur and clarification within policy may be important.
o A standard provincial date for the resumption of visiting is set for June 18th. While
direction considers the status of the home, it does not consider the status of the
community of the phase of regional re-opening. There may be merit to engage
the ministry in conversation around a phased approach that considers these
conditions to enhance safety. If this is coupled with a categorization of visitor
types/associated roles there could be an earlier and safer return of essential
caregivers (vs all visitors) in regions where community spread remains a concern.
In alignment with government directions, there should be information provided around
IPAC protocols, including hand hygiene, physical distancing and PPE. Consideration
could be given to mandatory orientation and ongoing training for essential caregivers as
well as return demonstrations to ensure appropriate practice. Some jurisdictions have

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 8
developed FAQ documents, used visual signage (i.e. posters) as reminders, and
implemented signed agreements with essential caregivers that clarify roles, expectations
and outcomes should roles and expectations not be met.
Directive #3 indicates that LTCH policy must clearly state that if the home is not able to
provide surgical/procedure masks, no family visitors should be permitted inside the home.
The Resumption of Visitors in LTCHs document states that visitors are responsible for
bringing their own face coverings and that LTCH are to provide surgical/procedure
masks and masks to outdoor visitors without one.
o To optimize support for outdoor visits, the LTCHs should consider securing and
appropriately laundering cloth face masks to support, at minimum, outdoor visits
should surgical/procedure masks be in limited supply.
o While it is important to protect PPE, it may be important to develop a strategy
that does find a way to make available surgical/procedure masks to support
visitors within the home.
Implications:
There are numerous lessons that can be learned from other jurisdictions and sectors
that could help inform the development of policies and practices for visitors of older
adults in hospitals and congregate settings.
SUMMARY OF RECOMMENDATIONS FOR CONSIDERATION
The following are recommended for consideration and discussion in the development of visiting
policies and practices as they pertain to older adults in congregate settings:
Collaborating to Achieve ‘Right Care, Right Time, Right Place’
Organizations must determine the right balance for their individual organization. They must
consider whether they can achieve ‘right care right time, right place’ in regard to:
Their level of risk readiness;
The organization’s ability to support visitors (i.e. sufficient space to support physical
distancing, access to PPE, ability to support additional screening and tracking/logging of
visitors, etc.); and,
The local level of COVID-19 risk and defined phase of community re-opening.
Ideally, a coordinated and consistent approach to regional and/or sector plans, processes and
practices should be considered to help support communication and clarity. All plans should be
developed and implemented in collaboration with local health units and in alignment with
Ministry direction and guidance.
Building a Supportive Environment
Preparing & Welcoming Family & Friends
Family and friends will be anxious to visit their loved ones. Most will have had some virtual
contact but some will have had none. Rebuilding relationships with visitors, including
essential caregivers will be important. The goal should be to create a good first encounter,
Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 9
without overwhelming either visitors or the older adult. In addition to provincial guidelines
(i.e. min 30min visits, one visit/wk./resident, masks and physical distancing, etc.), the following
is offered for consideration:
o Have knowledgeable staff dedicated to outdoor visiting areas to answer any
questions that may arise (i.e. health of the older adult, changes to visiting policy and
practices, etc.) and to provide oversight to the interactions (in case reminders
regarding safety best practices are required). It will also be important for these staff
to monitor and address signs of overstimulation or fatigue in the older adult.
o Develop FAQ questions and use visible signage (as appropriate) to address safety
best practices and changes to visiting policy and practices.
o In advance of initial visits, send communication regarding the process, the
experience (i.e. what will they see, etc.) and expectations during the visit (i.e.
screening, can they bring food or gifts, etc.). It may also be important to consider
including general commentary on the fact that the abilities of the older adult may
have changed from the last in-person visit. It would be helpful to have someone
available to answer questions prior to the visit if required.
o Provide information around ways to re-engage and interact with the older adult.
These strategies should consider the impact the COVID-19 restrictions on their loved
one and could include ideas to stimulate social engagement, cognitive function,
mobility/activity and nutrition/hydration status.
o Find a way to safely celebrate and welcome visitors back to the hospital or
congregate setting. Consideration should be given to re-building any damaged
relationships and demonstrating the value and importance of family and friends as
partners in care.
Supporting Staff
While many will be excited to see the return of visitors, it is important to consider the pressures
facing staff. The following is offered for consideration:
o Provide communication regarding new policies and procedures, including posting
and circulating materials as appropriate. Everyone should be clear on the plan prior
to the arrival of the first visitors.
o Engage staff in conversation around what the re-introduction of visitors will look like
within the setting and support them (in advance) to address situations that may arise
(i.e. what should they expect to see, what questions visitors may have, timelines/next
steps, how to address situations that may arise like a break in physical distancing,
etc.)
o Designate an individual(s) as a resource for staff should any questions or issues arise.
o Assess and monitor the mental and emotional health and well-being of staff over the
coming months. This could be done through brief staff surveys or individual targeted
staff conversations. Through regular monitoring, issues can be addressed early,
proper supports can be put in place and/or links can be made.
o Visitors will take additional staff time and focus, especially in the early days as visitors
will require education around safety best practices. If possible, schedule extra staff

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 10
(or redeploy leaders or other staff) as ‘Visitor Champions’ to help support some of
these additional needs.
Policy & Practice Considerations
Developing a Family Presence Policy
Organizations could use this opportunity to develop a policy that meets short-term needs
related to COVID-19 but lays the foundation for evolution to a more fulsome family presence
policy that recognizes family and friends as integral partners in care.
Incorporate Exceptional Circumstances
All organizations are encouraged to ensure that regardless of outbreak status, there is within
the policy clear guidelines that allow for targeted visits in exceptional circumstances,
including end-of-life visits for COVID+ older adults.
Address Other Outbreaks
Ensure the policy recognizes that COVID-19 is one disease that can lend to an outbreak but
that there are others as well. Clarification may be required within policy around whether
actions differ if one or both are present within the organization.
Defining Visitors
The term visitor should be defined in policy. Consideration should be given to including and
defining types of visitors in hospital and congregate settings. This would give greater ability
to designate essential caregivers, allowing them to continue to play an important role for
older adults if ever the outbreak status of an organizations changes. Three types are
proposed for consideration:
o Essential Caregivers – in the most recent provincial LTC documents, essential [family]
caregivers are defined as people capable of providing caregiving support (feeding,
social support, etc.) and having provided this support in the LTCH home prior to
COVID-19. It is difficult to define and quantify ‘caregiving support’ as the importance
of support will be subject to the needs and perceptions of the older adult. What may
be more important is building a process that allows the older adult or his/her SDM to
designate the individuals that they consider ‘essential’. To keep volumes
manageable, consideration should be given to limiting the number of designated
essential caregivers (i.e. to two individuals per older adult).
o Important Care Partners – family or friends who come to the setting to provide
support to the older adult and are important to their sense of health and well-being.
o Visitors – extended family or friends who come to the facility for the sole purpose of a
social drop-in.
Roles, expectations and restrictions should be aligned with visitor types. These could be
further aligned with outbreak status, similar to how recent provincial documents have
allowed for in-home visits by essential family caregivers in LTC ahead of other visitors. It
would also be important to consider continuity in language in reference to pediatrics and
parents/ guardians and older adults and their essential caregivers.

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 11
Roles & Expectations of Visitors
In addition to provincial direction to date (i.e. masks, hand hygiene, physical distancing,
screening, visitor log, etc.), policies and practice could include the following:
o Family and friends should only be allowed into one hospital/congregate setting.
There should not be travel/visits between facilities.
o If they are able to tolerate masks and use them appropriately, older adults could
wear masks when visitors are present.
o Commentary should be included related to bringing gifts or food/drink in the facility
as well as access to common areas, cafeterias and bathrooms.
o Masks – there should be a balance between preserving PPE, promoting safety and
facilitating contact with family and friends:
While cloth masks are recognized as effective, effectiveness is based on them
being clean. If sufficient supplies exist, providing surgical/procedure masks for
both indoor and outdoor visits could be a consideration.
If surgical/procedure masks are limited:
For outdoor visits, if the visitors are not arriving with masks, settings
could secure and launder cloth face masks to support the visit.
For indoor visits, it will be important to develop a creative strategy to
make surgical/procedure masks available to support visitors.
o The timing and volume of individuals arriving on site to spend time with older adults
may need to be managed to limit volumes and ensure physical distancing. New
Brunswick, as an example, is only allowing 10% of residents a visitor on any given day
in the early stages. If this is adopted, scheduling will be critical and a plan should be
in place for those that arrive without a scheduled appointment.
o Screening of older adults (residents, family and friends) does include recognition of
assessment of both typical and atypical symptoms. It is important to remember that
older adults may present WITHOUT an elevated temperature.
Additional Roles & Expectations of Essential Caregivers
Essential caregivers should be designated, with identity confirmed via picture identification
(if the staff are not familiar with the individual) prior to admission. They should follow staff
protocols for screening and testing. They should receive an initial orientation and ongoing
training/education regarding IPAC, including hand hygiene, physical distancing and PPE.
Return demonstrations for PPE could help ensure proper procedure is followed in donning/
doffing.
If Possible: Enhance the Approach to Phasing, Including Consideration of Community Spread
Provincial direction clearly outline a phased approach to the resumption of visiting. If
possible and appropriate, the phases could be more structured, aligned with visitor types
and better recognize the importance of community spread. This would need to align with
provincial direction and be developed in collaboration with public health. For example:
o Level 1 (Red) – COVID Outbreak in the facility and/or high/moderate community
spread:

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 12
In an organizations-specific outbreak, visitors should be restricted. Essential
caregivers could be allowed with tight restrictions:
- Maximum two designated essential caregivers per older adult, identified
by the older adult or SDM in collaboration with a representative from the
unit and the attending provider. Only one would be allowed in the facility
at a time.
- Signed contract with an agreed schedule and clear expectations/
boundaries. If not met, designation could be revoked.
- Be required to follow staff screening guidelines. All screening must be
passed to enter/remain on-site.
- Be required to complete similar training/ongoing education to staff
regarding IPAC, including hand hygiene and PPE with return
demonstration required. PPE would be defined based on organization
policy and clinical scenario.
If high/moderate community spread, the facility should be closed to all
visitors, except essential caregivers who could be allowed with tight
restrictions (as above).
o Level 2 (Orange) – No COVID cases in the facility + small community spread:
Essential caregivers only, with implementation of tight restrictions (see Level 1).
Permitting of outdoor visits with important care partners. Based on the space
available, could have more than one care partner as long as physical
distancing can be maintained. Masks and hand hygiene required.
o Level 3 (Yellow) – No COVID cases in the facility + no new community cases in the
last 14 days:
Essential caregivers and important care partners only with restrictions and
precautions in place in alignment with best practices and organization policy.
Permitting of outdoor space visits with visitors. Based on the space available,
could have more than one visitor as long as physical distancing can be
maintained. Masks and hand hygiene required.
o Level 4 (Green) – Pandemic clear
Essential caregivers, important care partners and visitors with restrictions and
precautions in place in alignment with best practices and organization policy.
CONCLUSION
The purpose of this discussion paper is to provide health system leaders with some thoughts for
considerations in developing policies and practices related to the resumption of visiting for older
adults in hospitals and congregate care settings amid COVID-19. It is not comprehensive, nor is
it complete. We hope it will:
Highlight key considerations related to older adults and their caregivers for consideration
in planning.
Emphasize the important role the Ministry and public health will play in providing

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 13
direction to begin to safely resume visiting.
Promote discussion in local regions around a phased, coordinated and consistent
approach to resume visiting that optimizes the safety, health and well-being of older
adults, their family and friends, health care providers and the community.
Encourage organizations to consider current and future needs and work toward a “new
normal” family presence policy that embraces the role of family and friends as partners
in care.

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 14
APPENDIX A
Summary of Ministry Direction Regarding Visitors at June 12, 2020
The following summarizes key or interesting considerations related to visitors within provincial
directives, guidance documents and communications.
Source Highlights Directive #5 for Hospitals
within the meaning of the
Public Hospitals Act and
LTCHs within the meaning of
the Long-Term Care Homes
Act, 2007 8
April 10, 2020
For LTCHs only, all staff and essential visitors must wear surgical/procedure
masks at all times for the duration of full shifts or visits, regardless of whether
the home is in outbreak or not.
This is to be implemented in conjunction with all other requirements
contained in Directive #3 dated April 8th 2020 or as amended.
COVID-19 Guidance: Long-
Term Care Homes 9
Version 4
April 15, 2020
Essential visitors include a person performing essential support services (e.g.,food
delivery, maintenance, family providing care services, and other health care) or
a person visiting a very ill or palliative resident. If an essential visitor is admitted to
the home, precautions must be taken as outlined in Directive #3 for Long-Term
Care Homes under the Long-Term Care Homes Act, 2007.
Guidance for Mask Use in
LTCH and Retirement Homes 10
Version 1
April 15, 2020
Essential visitors must wear a surgical/procedure mask at all times while in
the home. Any essential visitor in contact with a resident who has COVID-19,
should also wear appropriate PPE in accordance with Directive #1 and
Directive #5.
Essential visitors entering the home are expected to provide their own
surgical/ procedure masks and/or PPE as required (unless there are existing
arrangements with the home).
Every effort should be made to conserve masks and other supplies used as
PPE within a home. These supplies should be provided to support the safety
of staff, essential visitors and residents, but at no times should be overused
or used where not warranted.
COVID-19 Guidance: Hospice
Care 11
Version 1
May 7, 2020
Visitors should not be permitted in hospices, except for essential visitors.
Essential visitors include a person performing essential support services or a
person visiting a patient nearing the final days of their life.
Physical distancing, hand hygiene (washing hands or using hand sanitizer)
and respiratory etiquette (coughing or sneezing into sleeve/bend of arm)
8 Ontario Ministry of Health. April 10, 2020. Directive #5 for Hospitals within the meaning of the Public
Hospitals Act and Long-Term Care Homes within the meaning of the Long-Term Care Homes Act, 2007.
http://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/directives/public_hospitals
_act.pdf Accessed 6 Jun. 2020. 9 Ontario Ministry of Health. April 15, 2020. COVID-19 Guidance: Long-Term Care Homes.
http://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/2019_long_term_care_guid
ance.pdf Accessed 7 Jun. 2020 10 Ontario Ministry of Health. April 15, 2020. Guidance for mask use in long- term care homes and
retirement homes.
http://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/2019_guidance_ltc_retirem
ent_homes.pdf Accessed 6 Jun. 2020. 11 Ontario Ministry of Health. May 7, 2020. COVID-19 Guidance: Hospice Care.
http://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/2019_hospice_care_guida
nce.pdf Accessed 10 Jun. 2020.
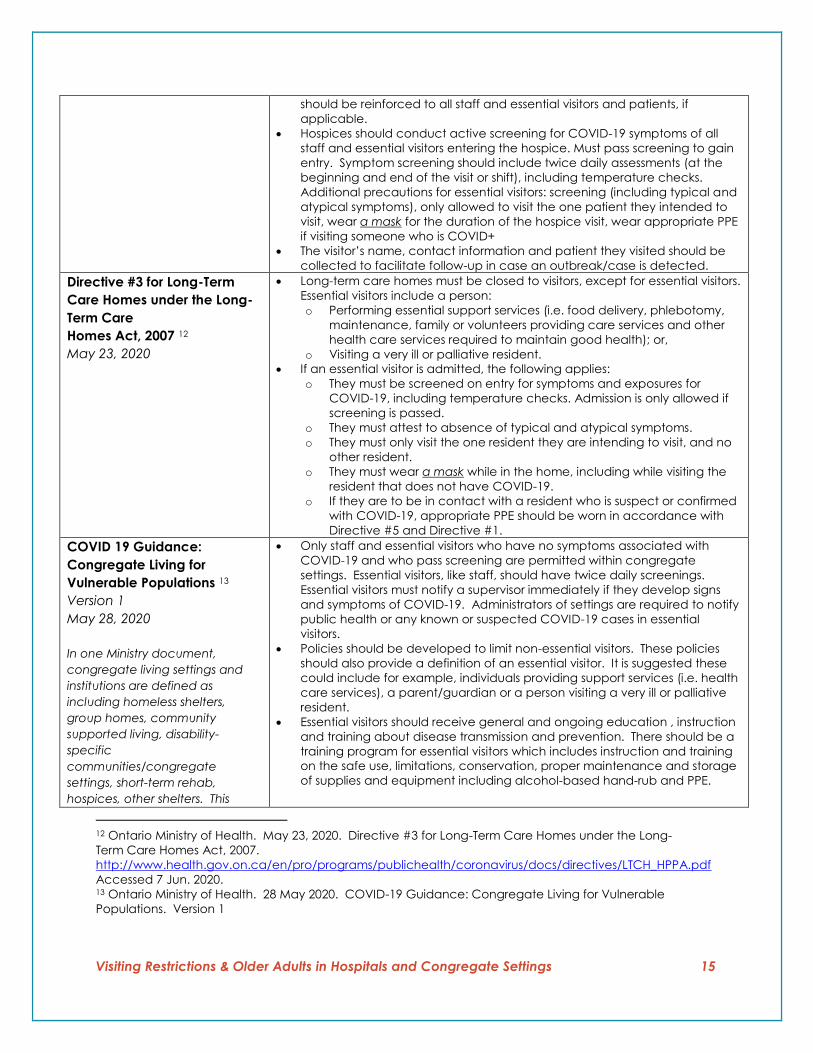
Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 15
should be reinforced to all staff and essential visitors and patients, if
applicable.
Hospices should conduct active screening for COVID-19 symptoms of all
staff and essential visitors entering the hospice. Must pass screening to gain
entry. Symptom screening should include twice daily assessments (at the
beginning and end of the visit or shift), including temperature checks.
Additional precautions for essential visitors: screening (including typical and
atypical symptoms), only allowed to visit the one patient they intended to
visit, wear a mask for the duration of the hospice visit, wear appropriate PPE
if visiting someone who is COVID+
The visitor’s name, contact information and patient they visited should be
collected to facilitate follow-up in case an outbreak/case is detected.
Directive #3 for Long-Term
Care Homes under the Long-
Term Care
Homes Act, 2007 12
May 23, 2020
Long-term care homes must be closed to visitors, except for essential visitors.
Essential visitors include a person:
o Performing essential support services (i.e. food delivery, phlebotomy,
maintenance, family or volunteers providing care services and other
health care services required to maintain good health); or,
o Visiting a very ill or palliative resident.
If an essential visitor is admitted, the following applies:
o They must be screened on entry for symptoms and exposures for
COVID-19, including temperature checks. Admission is only allowed if
screening is passed.
o They must attest to absence of typical and atypical symptoms.
o They must only visit the one resident they are intending to visit, and no
other resident.
o They must wear a mask while in the home, including while visiting the
resident that does not have COVID-19.
o If they are to be in contact with a resident who is suspect or confirmed
with COVID-19, appropriate PPE should be worn in accordance with
Directive #5 and Directive #1.
COVID 19 Guidance:
Congregate Living for
Vulnerable Populations 13
Version 1
May 28, 2020
In one Ministry document,
congregate living settings and
institutions are defined as
including homeless shelters,
group homes, community
supported living, disability-
specific
communities/congregate
settings, short-term rehab,
hospices, other shelters. This
Only staff and essential visitors who have no symptoms associated with
COVID-19 and who pass screening are permitted within congregate
settings. Essential visitors, like staff, should have twice daily screenings.
Essential visitors must notify a supervisor immediately if they develop signs
and symptoms of COVID-19. Administrators of settings are required to notify
public health or any known or suspected COVID-19 cases in essential
visitors.
Policies should be developed to limit non-essential visitors. These policies
should also provide a definition of an essential visitor. It is suggested these
could include for example, individuals providing support services (i.e. health
care services), a parent/guardian or a person visiting a very ill or palliative
resident.
Essential visitors should receive general and ongoing education , instruction
and training about disease transmission and prevention. There should be a
training program for essential visitors which includes instruction and training
on the safe use, limitations, conservation, proper maintenance and storage
of supplies and equipment including alcohol-based hand-rub and PPE.
12 Ontario Ministry of Health. May 23, 2020. Directive #3 for Long-Term Care Homes under the Long-
Term Care Homes Act, 2007.
http://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/directives/LTCH_HPPA.pdf
Accessed 7 Jun. 2020. 13 Ontario Ministry of Health. 28 May 2020. COVID-19 Guidance: Congregate Living for Vulnerable
Populations. Version 1

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 16
document specifically excludes
adult correctional facilities.
All staff and essential visitors should wear non-medical masks while in the
setting for the duration of their shift or visit. Staff providing direct care
should consider PPE (“non-medical masks are not defined as PPE”) based
on the nature of the planned interaction with the resident and his/her
known health status.
COVID-19 Testing for Long-
Term Care Home Staff 14
Communication to LTCH
Licensees
May 31, 2020
It is intended that all LTC home staff be tested, at reasonable intervals, a
minimum twice in the month of June. LTC homes should continue testing
residents based on COVID-19 Provincial Testing Guidance.
Testing for LTC home staff will include all individuals working in the LTC home
(e.g., front-line workers, management, food-service workers, contracted
service providers, etc.).
COVID-19 Guidance: Acute
Care 15
Version 5
June 5, 2020
Acute care settings must conduct active screening for COVID-19 symptoms
on everyone entering the facility.
It is currently recommended only essential visitors be allowed into the
facility. Examples of individuals who could be determined by the hospital as
essential visitors include those visiting:
o A patient who is dying or very ill;
o A parent/guardian of an ill child or youth;
o A visitor of a patient undergoing surgery; and/or,
o A woman giving birth.
Recommendations for
Regional Health Care Delivery
During the COVID-19
Pandemic: Outpatient Care,
Primary Care, and Home and
Community Care 16
June 8, 2020
Patients, clients, and essential caregivers/visitors should wear a mask for
source control (cloth or surgical/procedural) and should be encouraged to
bring their own if possible
Directive #3 for Long-Term
Care Homes under the Long-
Term Care
Homes Act, 2007 17
June 10, 2020
Active screening of all visitors which includes twice daily symptom screening
and temperature check. The screening must be passed to gain entry.
Homes must have a visitor policy in place that is compliant with the
Directive and guided by applicable policies. At minimum, visitor policies
must:
o Be informed by the ongoing COVID-19 situation in the community and
the home and be flexible to be reassessed as circumstances change.
o Be based on principles such as safety, emotional well-being, and
flexibility and address concepts such as compassion, equity, non-
maleficence, proportionality (i.e., to the level of risk), transparency
and reciprocity (i.e., providing resources to those who are
disadvantaged by the policy).
o Include education about physical distancing, respiratory etiquette,
hand hygiene, IPAC and proper use of PPE.
o Include allowances and limitations regarding indoor and outdoor
visiting options.
14 Ontario Ministry of Health. May 31 2020. Communication to LTCH Licensees. COVID-19 Testing for LTCH
Staff. 15 Ontario Ministry of Health. June 5 2020. COVID-19 Guidance: Acute Care. Version 5 16 Ontario Ministry of Health. June 8 2020. Recommendations for Regional Health Care Delivery During the
COVID-19 Pandemic: Outpatient Care, Primary Care, and Home and Community Care 17 Ontario Ministry of Health. May 23, 2020. Directive #3 for Long-Term Care Homes under the Long-
Term Care Homes Act, 2007.
http://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/directives/LTCH_HPPA.pdf
Accessed 12 Jun. 2020.

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 17
o Include criteria for defining the number and types of visitors allowed
per resident when the home is not in an outbreak. When the home is
in an outbreak, only essential visitors (as defined below) are permitted
in the home.
o Include screening protocols, specifically that visitors be actively
screened on entry for symptoms and exposures for COVID-19,
including temperature checks and not be admitted if they do not
pass the screening.
o Include visitor attestation to not be experiencing any of the typical
and atypical symptoms.
o Comply with the home’s IPAC protocols, including donning and
doffing of PPE.
o Clearly state that if the home is not able to provide
surgical/procedure masks, no family visitors should be permitted inside
the home. Essential visitors who are provided with appropriate PPE
from their employer, may enter the home.
o Include a process for communicating with residents and families
about policies and procedures including the gradual resumption of
family visits and the associated procedures.
o State that non-compliance with the home’s policies could result in a
discontinuation of visits for the non-compliant visitor.
o Include a process for gradual resumption of family visitors that
stipulates:
Visits should be pre-arranged.
Family visitors to begin with one visitor at a time.
Must only visit the one resident they are intending to visit, and no
other resident.
Family visitors should use a face covering if the visit is outdoors. If
the visit is indoors, a surgical/procedure mask must be worn at all
times.
Family visits are not permitted when: a resident is self-isolating or
symptomatic, or a home is in an outbreak.
o Specify that essential visitors:
Be defined as including a person performing essential support
services (e.g., food delivery, inspector, maintenance, or health
care services (e.g., phlebotomy)) or a person visiting a very ill or
palliative resident.
Providing direct care to a resident must use a
surgical/procedure mask surgical/procedure mask while in the
home, including while visiting the resident that does not have
COVID-19 in their room.
Who are in contact with a resident who is suspect or confirmed
with COVID-19, must wear appropriate PPE in accordance with
Directive #5 and Directive #1.
Are the only type of visitors allowed when: A resident is self-
isolating or symptomatic, or a home is in an outbreak.
LTCHs must keep families informed about COVID-19, including frequent and
ongoing communication during outbreaks. Signage must be clear about
COVID-19, including signs and symptoms of COVID-19, and steps that must
be taken if COVID-19 is suspected or confirmed in staff or a resident.
Resuming Visits in LTCHs 18
June 11, 2020
Provides guidance to LTCHs and is intended to supplement the updated
Directive #3. To the extent that anything in the document conflicts with the
18 Ontario Ministry of LTC. June 11 2020. Resuming Visits in LTCHs. https://files.ontario.ca/mltc-resuming-
visits-long-term-care-homes-en-2020-06-11.pdf Accessed 11 Jun. 2020.

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 18
Directive, the Directive prevails, and LTCHs must take all reasonable steps to
follow the Directive.
Visitors are not allowed in the LTCH if the home is in outbreak.
The LTCH is to develop procedures for the resumption of visits and a process
for communicating these with residents, families, visitors and staff, including
but not limited IPAC, scheduling and any setting-specific policies including:
sharing information on IPAC, wearing a mask, movement within the home,
approach to dealing with non-adherence to home P&P (including
discontinuation of visits).
A list of visitors is to be maintained.
Visitors must pass screening prior to each visit, attest that they have tested
negative within the last 2wks and not positive since (LTCH not responsible for
testing)
Must comply with IPAC protocols including proper use of surgical/
procedure mask – face covering if outdoors and surgical/procedure mask if
indoors. Face masks to be worn at all times. Visitors responsible for bringing
own face coverings, LTCH to provide surgical/procedure masks and masks
to outdoor visitors without one.
Visitor is defined as any family member, close friend or neighbour. They can
also be essential family caregivers. Essential family caregivers are those
people capable of providing caregiving support (feeding, social support,
etc.) and has done this before in the home prior to COVID-19.
Phase 1 – June 18 start - outdoor visiting
One visitor/resident at time, visit scheduling required to ensure physical
distancing and staff coverage, visits can be time limited but cant restrict
<30min, equitable access to visits must be provided for all residents; allow
for one visit min/wk per resident; staff support transfer of residents in/out of
home;
Phase 2A – start one wk after lifting emergency orders - outdoor visiting
expanded
Similar to Phase 1 but up to 2 visitors at a time
Phase 2B – start one wk after lifting emergency orders - indoor visiting for
essential family caregivers only
Similar to Phase 1 + one visitor at a time, procedure required to escort
visitors to homes, no overcrowding in room, min one visit/wk/per resident
but for essential family caregivers on agreement with home for more
frequent schedule should be permitted
Phase 3 – at max one month after limiting emergency measures - outdoor
visiting and indoor visiting expanded
Similar to Phase 2 + up to 2 visitors as long as physical distancing can be
accommodated, can regulate number of visitors
Reopening RHs 19
June 11, 2020
Re-opening should take place in a gradual, phased manner that meets the
health and safety needs of residents, staff, and visitors. Additionally, to
ensure maximum resident and staff safety, a RH co-located with a LTCH will
adopt LTCH visitation policies if those policies are more restrictive
Visitors not allowed if on outbreak
Required to dedicate area for indoor/outdoor visits with staff to maintain
highest IPAC standards prior/after visits
RH plans need to consider access to adequate testing/plan in place,
adequate PPE; IPAC standards including essential cleaning and
disinfection; physical distancing – able to facilitate and protocols to support
Visitors can only visit designated indoor/outdoor areas, suites
19 Ontario Ministry of Health. June 11 2020. Reopening RHs. https://files.ontario.ca/msaa-reopening-
retirement-homes-en-2020-06-11.pdf Accessed 11 Jun. 2020.

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 19
Can start June 18.
Screening, attestation re negative testing, IPAC, masks (like LTC)
# visitors/resident/day determined by home, visits need to be scheduled
and can be time limited
Resuming Visits in Congregate
Settings 20
June 11, 2020
An essential visitor is generally a person (including a contractor) who
performs essential services to support the ongoing operation of a service
agency or is a person considered necessary by a service agency to
maintain the health, wellness and safety, or any applicable legal rights, of a
resident.
Although the direction on non-essential visitors does not place a blanket
prohibition on all visitors, it is intended to greatly limit entry into the
congregate living setting to help prevent transmission of COVID-19 and to
protect residents and staff during the outbreak. The role that families, visitors
and loved ones play in providing caregiving and emotional supports is
important in the quality of life for those living in congregate living settings. To
support visits while protecting residents and staff, the ministry is proposing
resumption of personal visits, provided they take place outdoors and are
guided by some key principles.
20 Ontario Ministry of Children Community & Social Services. June 11 2020. Resuming Visits in Congregate
Settings. https://files.ontario.ca/mccss-resuming-visits-in-congregate-living-settings-en-2020-06-11.pdf
Accessed 11 Jun. 2020.

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 20
APPENDIX B
Other Jurisdictions & Sectors
North East Specialized Geriatric Centre / Health Sciences North
Health Sciences North has established a Family and Caregiver Presence (Visitor) Policy Working
Group. The North East Specialised Geriatric Centre is involved in that work. Within that Working
Group, a process is being established to ensure essential visitors are identified and that there is
an internal process for communication regarding essential visitors.
With the goal to achieve family care partner/presence and participation in a manner that is
safe for patients and staff, a decision guide is being developed. The guide will help staff decide
whether a visitor is essential. Essential visitors include support persons as well those supporting
individuals at the end of life or those requiring emergency/unplanned surgery. Support persons
include, for example, those supporting communication, ambulation and/or cognitive
impairment. It also includes those providing emotional support or those requiring training to
support discharge.
Pediatrics & Toronto’s Hospital for Sick Children
Pediatrics offers an interesting lens for consideration. Similar to providing care for older adults,
the world of pediatrics values, recognizes and promotes the importance of family and friends in
meeting the daily needs of their population.
Since the start of the outbreak, HSC has put visiting restrictions in place to protect the health and
well-being of their children while recognizing the essential role of family. The following measures
are in place:
One adult is allowed to accompany a child to the hospital. Inpatients staying overnight
are allowed two designated adult caregivers to take turns in providing care but only one
is allowed in the building at any time.
Designated caregivers are provided with a badge and must present the badge and
picture identification at screening to gain entrance.
Siblings under 18 and other visitors are not allowed at this time. No individual under age
18 is permitted, unless they are the parents.
Family members are provided with Level 1 masks by the organization. Family of
inpatients are asked to wear masks if they are unable to maintain a 2m distance within
the room.
Children over 6 are now masked if they are able to wear if safely and tolerate it.
Screening occurs prior to entry. Family of inpatients who stay overnight are screened
daily on the units.
IPAC training occurs with designated caregivers.
Prince Edward Island
PEI is currently limited to outdoor visits only:
Designated spaces only, cleaned between use, "hosted" visits, maximum of 1 hour

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 21
2 designated visitors per resident, may visit together or separately
Hand hygiene and physical distancing required (non-medical mask required if physical
distancing might not be maintained, i.e. cognitive impairment)
Scheduled ahead of time
Palliative visits are permitted at the bedside with 6 designated visitors per resident, who may visit
together or separately. Hand hygiene and physical distancing is required.
In the next stage, likely starting June 26 the following will apply:
Outdoor visits will continue with the same conditions applying except that individuals are
allowed 6 designated visitors per resident, with a maximum of 2 visitors at a time
Indoor visits will be added in designated spaces only (not bedside or in common rooms).
These areas will be cleaned between use, "hosted" visits, maximum of 1 hour. 2
designated visitors per resident will be allowed and they can visit together or separately.
Hand hygiene and physical distancing will be required (non-medical mask required if
physical distancing might not be maintained, i.e. cognitive impairment). Visits will be
scheduled ahead of time.
Palliative visits would continue as per present practice
New Brunswick
Outdoor Visits at Facility (started June 5, 2020):
2 visitors per resident at a time
Physical distancing (area must have sufficient space for distancing)
Appointment ahead of time
Number of visits at one time limited to respect the current “gathering” guidelines
Palliative Visits in LTCF (new policy, June 5, 2020):
Palliative Performance Scale score of 30% or less are eligible for visitors and bed ridden (if
PPS 20% or less, 2 visitors may visit at one time)
Resident may select 10 members of their immediate family/friends, to visit one at a time
(unless support is required)
Facility should be provided a list of these individuals.
Out of province may apply for exemption to cross border (call 1-800-863-6582)
Indoor visits expected to start June 19.
Visits may occur within the facility, and will be subject to maximum visitation capacity
limits (10% of residents per day)
Resident must select 1 visitor, they will be the only visitor permitted to enter the facility
during this phase
10% of residents can have 1 visit per day (for example, a 100-bed facility would have 10
visits per day). Assumption that every resident may have 1 visit every 10 days
Active screening of visitors, mandatory mask use, hand hygiene, disinfecting high-touch
areas are some of the mandatory measures to mitigate the risks

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 22
Saskatchewan
On June 3, 2020 the Saskatchewan Health Authority (SHA) expanded criteria for compassionate
reasons related to visitation restrictions in both hospitals and LTCH settings 21. To support this work
a Family Presence Expert Panel was established with representation from patients, families,
public health and IPAC experts. They have developed and published guidance and FAQ
documents, a family presence commitment statement, a family presence poster and posters
outlining visitor items and restrictions. The family presence commitment statement outlines the
roles of both health service providers and the family with information around who to contact for
more information.
Within the context of these documents:
Compassionate care includes, but is not limited to end-of-life care, major surgery,
intensive care/critical care, or a care partner aiding in clinical care (at the discretion of
the patient's care provider).
Under the concept of compassionate care, older adults can have a designated family
member or support person if their quality of life and/or care needs cannot be met
without that person’s assistance. This has been further clarified:
o The support person can include a loved one, friend, religious/spiritual care
provider, paid caregiver, or other support person of the patient/resident’s
choosing.
o Inpatients, outpatients, emergency/urgent care patients can designate one
support person. In LTC settings, two individuals can be designated but only 1 can
visit at a time.
o Assistance is considered required in those with compromised comprehension,
decision making or mobility due to disability or onset of a medical condition (for
example but not limited to: mobility, hearing, speech including communication
barriers, compromised cognitive functioning (i.e. mental illness, intellectual
disability, dementia), visual or memory impairment).
o Determination is made by the attending physician and unit manager/ charge
nurse in consultation with the designated support person(s).
Screening, including temperature check and questionnaire, is required prior to entry with
visitors required to perform hand hygiene and wear a medical grade mask if tolerated.
Other PPE may be required based on the circumstances.
Visitors are not permitted in waiting rooms or common areas.
Food and beverages are permitted to be brought into facilities with certain guidelines
defined.
LTCHs are now allowing outdoor visitation. Visiting must be arranged in advance and
more than one visitor is allowed as long as physical distancing can be maintained
21 Saskatchewan Government. Visiting SHA Facilities. https://www.saskatchewan.ca/government/health-
care-administration-and-provider-resources/treatment-procedures-and-guidelines/emerging-public-health-
issues/2019-novel-coronavirus/visiting-sha-facilities?fbclid=IwAR04Qpp8FGq-
V5naM3zOuipB6yKzW2nbTXCFzu0kgrRASJjVKQJIdEMHBlo Accessed 7 Jun. 2020.

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 23
(exception: family members from same household). If it cannot be maintained, masks
are to be worn and hand hygiene performed.
Quebec
The province of Quebec website has a page specifically dedicated to informal and family
caregivers during COVID-19. 22 This website recognizes the value of informal caregivers, outlines
what to expect in the changing environment and addresses the importance of IPAC measures
like hand hygiene and PPE. Within this site, they also clearly outline key definitions and processes
to support the role of informal caregivers.
Informal caregivers are now able to provide assistance or significant support to an individual
living in a facility, as long as they comply with specific conditions and precautions.
Informal caregivers are considered those who provide, or who would like to provide,
significant assistance and support to a loved one to meet their needs and contribute to
their integrity and well-being. Examples of support included: helping with meals,
supervising and being attentive to the person’s overall condition, supporting various daily
or recreational activities, assistance with walking and/or providing moral support and
comfort.
The term “significant support” is defined as a “regular basis, every day or several times a
week” with the key being that the support of the caregiver is contributing to their loved
one’s integrity and well-being.
More than one informal caregiver may be authorized to provide support to the same
person in a facility but only one is allowed in the facility at any given time.
Informal caregivers decide themselves when they will visit and the length/frequency of
visits. They must comply with visit conditions within the facility. They may receive an
arrival and departure time to minimize contact with others.
They are required to sign a consent form stating that their decision was informed and
voluntary, they understood the risks of infection and that they promise to adhere to the
precautions to maintain the safety of residents, themselves and others in the facility.
They are required to self-monitor for symptoms and are not allowed to enter the facility if
they are COVID+ or if they have been in contact with an individual who is COVID+. A 14-
day isolation period is required and they must test negative to gain re-entry.
Informal caregivers need to sign a register to facilitate contact tracing, if required.
They are allowed to provide care and support to only one person. In some facilities/
circumstances there are no exceptions to this rule. In others, it is possible if two people in
the same unit receive regular, significant support from the same informal caregiver.
They must wear clean clothes when they go to the facility. They are not allowed to bring
clothes or other items from home (i.e. purses, lunch bags, documents) and if they do,
they will be prevented from bringing them home.
They are encouraged to minimize travel outside their homes to reduce risk.
22 Province of Quebec website. https://www.quebec.ca/en/health/health-issues/a-z/2019-
coronavirus/caregivers-during-the-covid-19-pandemic/ Accessed 10 Jun. 2020

Visiting Restrictions & Older Adults in Hospitals and Congregate Settings 24
Within the facility, movement within the facility is limited with no access to common
areas and physical distancing required. Directions are provided around which
bathrooms are allowed for use.
New Zealand
On May 13, 2020 New Zealand 23 moved into Alert Level 2 24 status (Level 4 = lockdown)
signifying the disease was contained with the risk of community transmission remaining. While
many precautions remained in place (i.e. physical distancing, border controls, testing, isolation
and contact tracing of those unwell), their society began to re-open. Gathering sizes were
increased from 10 to 100. Gyms re-opened with restrictions. Restaurants and businesses
opened, as did schools and day cares with physical distancing required. Museums, theatres
and public spaces re-opened with a requirement to maintain records to support contact
tracing.
Within Alert Level 2 there were specific guidelines for aged care providers 25, including guidelines
for family visiting. At an Alert Level 4 or 3 family visits were limited to essential visitors (i.e.
palliative cases) with all visits scheduled and full precautions taken during the visit (i.e. screening,
hand hygiene, PPE, physical distancing). At an Alert Level 2 visiting was allowed, including
general family visits and non-essential service visits. These visits were managed in a controlled
way and precautions put in place. For example:
Visits were limited to designated visitors with a limit to the number of visitors allowed at
one time. Appointments and sign-ins were required. There were limits to the length of
the visit and/or the visit location based on the health status of the older adult and the
number of other visitors in the facility.
Health screening was completed on all visitors prior to entering the facility.
Visitors were required to follow the facility’s IPAC measures, including hand hygiene,
physical distancing and appropriate use of PPE.
23 New Zealand Ministry of Health website. https://www.health.govt.nz/ Accessed 7 Jun. 2020. 24 On June 8, 2020 New Zealand moved to Level 1 status 25 New Zealand Ministry of Health. COVID-19: Aged Care Providers. https://www.health.govt.nz/our-
work/diseases-and-conditions/covid-19-novel-coronavirus/covid-19-resources-health-professionals/covid-
19-health-sector-providers/covid-19-aged-care-providers Accessed 7 Jun. 2020.