Embed Size (px)
Citation preview
1
Consensus on core public health nutrition functions and
competencies
Report from the Curriculum Renewal in Public Health
Nutrition (CRIPHN) Project
Delphi Study
April- November 2011
Curriculum Renewal in Public Health Nutrition (CRIPHN) Project
Funded by the Australian Learning and Teaching Council
Support for this project/activity has been provided by the Australian Government Office for Learning and Teaching. The views in this project do not necessarily reflect the views of the Australian Government Office
for Learning and Teaching.

2
BACKGROUND The aim of this 2-phase CRIPHN project is to: • develop national academic standards (in the form of a competency framework that promotes
graduate employability) informed by consensus developed amongst key workforce stakeholders, and • guide future under-graduate and post-graduate curriculum renewal, workforce preparation strategy
and broader workforce development. This stage of the project builds on earlier Australian and international studies [1, 2] that focused on assessing and developing consensus about: • the work required (core functions) of a public health nutritionist, and • the knowledge, skills, attitudes and “ways of thinking” required to be able to capably perform this
work (i.e. competencies). This report serves to summarise the process and results from the 2011 Delphi Survey conducted as part of this project. Why develop consensus amongst employers, academics and practitioners? Central to this activity is the objective of maximising graduate employability, being work ready, of value to employers, the graduates themselves and the communities in which they work. In order to achieve this objective, the knowledge, experience and expectations of various stakeholders need to be considered. Earlier work on developing consensus about the competencies required for effective public health nutrition practice have demonstrated that practitioners/employers and academics have largely consistent opinions about the competencies required, albeit favouring competencies reflecting their practice context (academics placing more emphasis on analytical competencies and practitioners more emphasis on program management and policy process competencies). Why use a Delphi technique? The Delphi technique usually involves a series of 3 survey rounds amongst a panel of experts to assess and develop consensus via a process of iteration and managed feedback. The Delphi study’s primary advantages in this context are cost-effectiveness and the ability to harness the anonymous ideas and opinions of a range of experts/stakeholders in different geographic locations. The Delphi method is a frequently used technique to measure and aid forecasting and decision making in a variety of disciplines[3, 4], including competency requirements in healthcare settings[3]. Four key features define the Delphi method including anonymity, iteration, controlled feedback and the statistical aggregation of group response[4]. The methodology employed in this latest study is described as follows.

3
METHODS A modified Delphi study, based on an earlier consensus development studies focusing on public health nutrition core functions and competencies[1, 2], was implemented amongst a purposively sampled panel of workforce development stakeholders across Australia, and included a sub-sample of international PHN exemplars. It included, as shown in Figure 1, a definition of the issues, identification and recruitment of panellists followed by a three step process for identifying consensus in the panel.
Expert panel recruitment
The Delphi method does not call for expert panels to be representative samples for statistical purposes. Representativeness is assessed on the qualities of the expert panel rather than its numbers[5]. There seems to be very little actual empirical evidence on the effect of the number of participants on the reliability or validity of consensus processes[3]. Limited guidance therefore exists on the minimum or maximum number of experts on a Delphi panel. It appears to be related to common sense and practical logistics[6]. Earlier studies assessing agreement about competencies in this field had expert panel sizes ranging in size from 20-52[1, 2].
An e-mail contact list for Australian public health nutrition workforce development stakeholders (broadly categorised as academics, practitioners and/or employers) was developed, from existing academic and professional networks (APHNAC, FANSIG, DAA-SIG) and complemented by snow-ball sampling. The inclusion criteria for individuals invited to become panellists was that they were required to be in positions relevant to influencing and practicing workforce development (e.g. Employers in public health agencies, academics, senior practitioners). The assumption used when identifying panellists this way was that individuals employed or practicing in senior level positions within health and academic institutions had the necessary experience and insight to be considered experts in this context. An international sub-sample of PHN exemplars was recruited from the membership of the World Public Health Nutrition Association by direct invitation.
The final contact list of 81 identified experts (Australians=66, internationals=15) were formally invited via e-mail to join the expert panel and participate in the Delphi process with explicit requests to either self nominate or forward invitations to known experts (snowballing). Panellists who accepted the invitation (i.e. expert self selection) where forwarded the first Delphi questionnaire as an e-mail attachment and as a web-link to Lime Survey for either web-based or manual completion and e-mail return. Figure 1 illustrates the process used in this study.
4
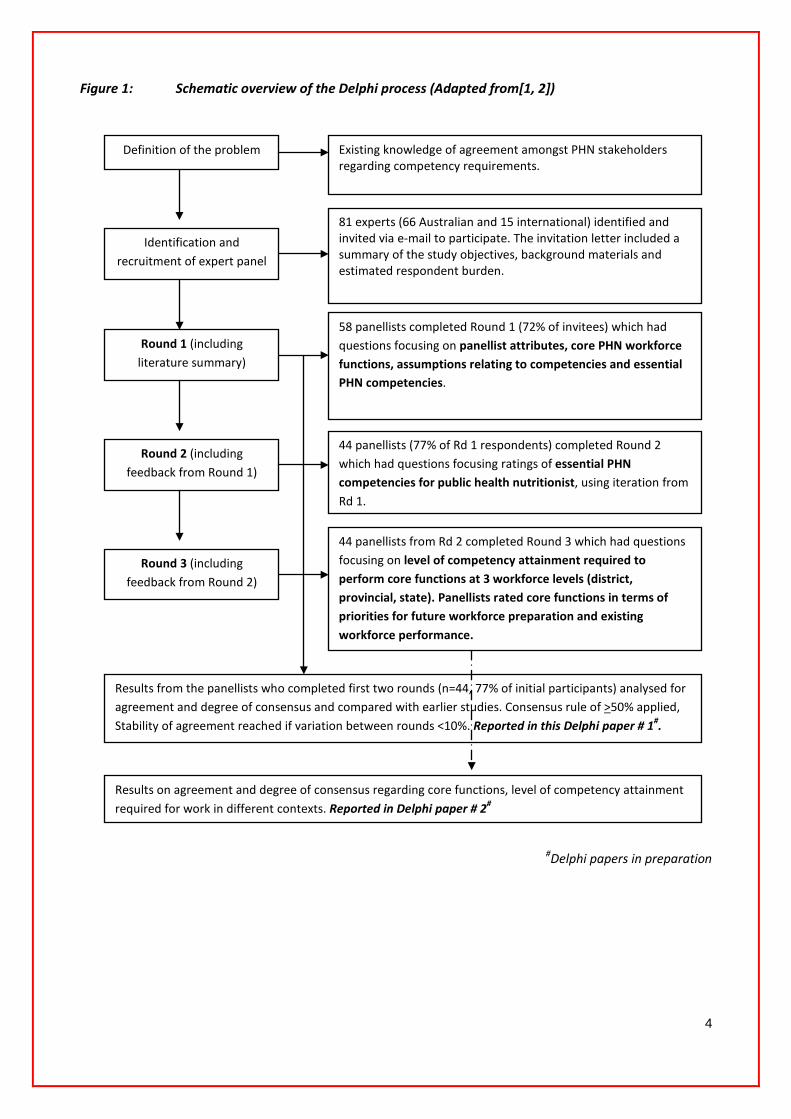
Figure 1: Schematic overview of the Delphi process (Adapted from[1, 2])
#Delphi papers in preparation
Definition of the problem
Identification and recruitment of expert panel
Round 1 (including literature summary)
Round 2 (including feedback from Round 1)
Round 3 (including feedback from Round 2)
Existing knowledge of agreement amongst PHN stakeholders regarding competency requirements.
81 experts (66 Australian and 15 international) identified and invited via e-mail to participate. The invitation letter included a summary of the study objectives, background materials and estimated respondent burden.
58 panellists completed Round 1 (72% of invitees) which had questions focusing on panellist attributes, core PHN workforce functions, assumptions relating to competencies and essential PHN competencies.
44 panellists (77% of Rd 1 respondents) completed Round 2 which had questions focusing ratings of essential PHN competencies for public health nutritionist, using iteration from Rd 1.
44 panellists from Rd 2 completed Round 3 which had questions focusing on level of competency attainment required to perform core functions at 3 workforce levels (district, provincial, state). Panellists rated core functions in terms of priorities for future workforce preparation and existing workforce performance.
Results from the panellists who completed first two rounds (n=44, 77% of initial participants) analysed for agreement and degree of consensus and compared with earlier studies. Consensus rule of >50% applied, Stability of agreement reached if variation between rounds <10%. Reported in this Delphi paper # 1#.
Results on agreement and degree of consensus regarding core functions, level of competency attainment required for work in different contexts. Reported in Delphi paper # 2#

5
Survey instruments
Each survey round of the Delphi process used survey instruments based on earlier studies that assessed consensus amongst an international panel regarding the essential competencies required for effective PHN practice. The competency units tested in these survey rounds were originally constructed from competency standards in the public health, health promotion and dietetics fields of practice[2, 7], including competency compilations by APHNAC[8] and the WPHNA[9]. The present study varied from the traditional Delphi method in that structured questions informed by these earlier studies were used rather than open ended questions.
Data analysis
Responses to each round of Delphi surveys were exported from LimeSurvey to SPSS for storage and analysis. Descriptive analysis via frequency of response distributions is presented in this preliminary analysis. To assess difference in responses by panellist attributes, chi-square analysis was conducted for academic versus employer panellists and Australian versus internationals . The level of significance was taken as p<0.05.
Definition and stability of the consensus
The literature doesn’t provide any agreed standard on how to measure consensus[4]. Arbitrary and pre-defined consensus rules were used to judge agreement amongst the panellists and define when consensus had been developed. The consensus standard was arbitrarily set at ≥ 50% agreement (i.e. majority rule) in all three Delphi rounds. The consensus was considered to have reached stability if group ratings on suggested competencies varied ≤10% between rounds. This approach to define stability of the consensus has been used in previous studies[2, 10].
6
THE DELPHI PANEL
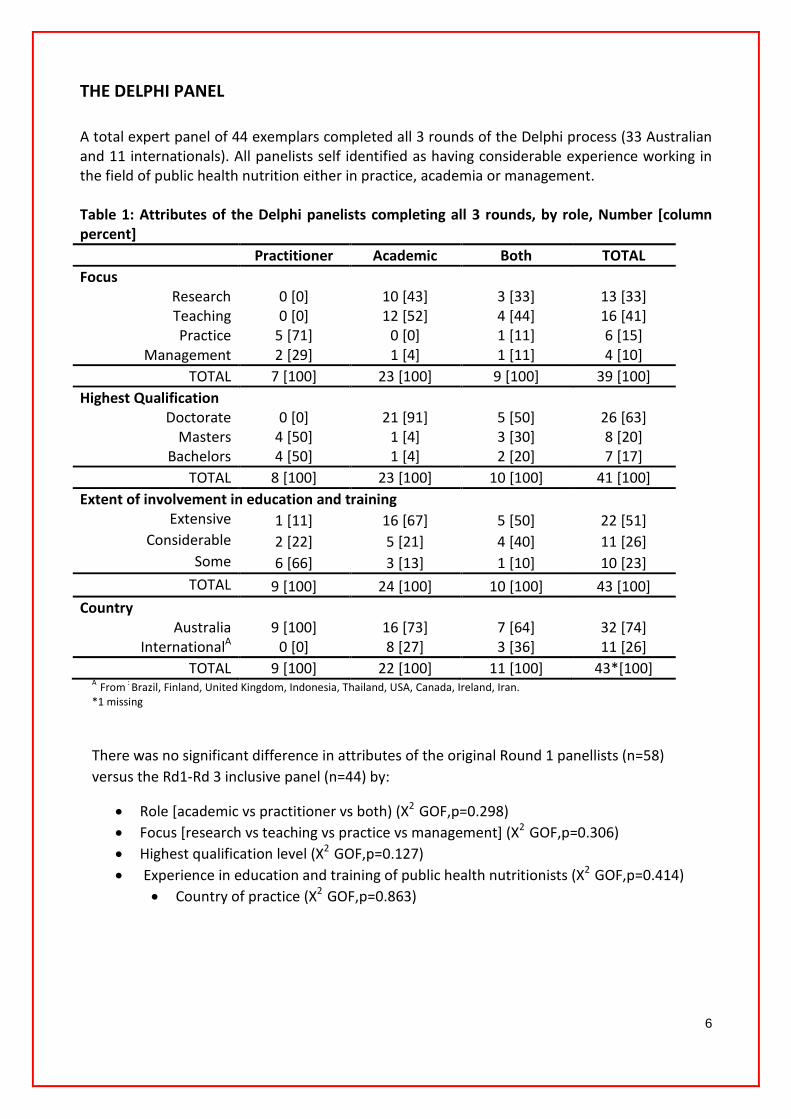
A total expert panel of 44 exemplars completed all 3 rounds of the Delphi process (33 Australian and 11 internationals). All panelists self identified as having considerable experience working in the field of public health nutrition either in practice, academia or management. Table 1: Attributes of the Delphi panelists completing all 3 rounds, by role, Number [column percent]
Practitioner Academic Both TOTAL Focus
Research 0 [0] 10 [43] 3 [33] 13 [33] Teaching 0 [0] 12 [52] 4 [44] 16 [41] Practice 5 [71] 0 [0] 1 [11] 6 [15]
Management 2 [29] 1 [4] 1 [11] 4 [10] TOTAL 7 [100] 23 [100] 9 [100] 39 [100]
Highest Qualification Doctorate 0 [0] 21 [91] 5 [50] 26 [63]
Masters 4 [50] 1 [4] 3 [30] 8 [20] Bachelors 4 [50] 1 [4] 2 [20] 7 [17]
TOTAL 8 [100] 23 [100] 10 [100] 41 [100] Extent of involvement in education and training
Extensive 1 [11] 16 [67] 5 [50] 22 [51] Considerable 2 [22] 5 [21] 4 [40] 11 [26]
Some 6 [66] 3 [13] 1 [10] 10 [23] TOTAL 9 [100] 24 [100] 10 [100] 43 [100]
Country Australia 9 [100] 16 [73] 7 [64] 32 [74]
InternationalA 0 [0] 8 [27] 3 [36] 11 [26] TOTAL 9 [100] 22 [100] 11 [100] 43*[100]
A From : Brazil, Finland, United Kingdom, Indonesia, Thailand, USA, Canada, Ireland, Iran. *1 missing
There was no significant difference in attributes of the original Round 1 panellists (n=58) versus the Rd1-Rd 3 inclusive panel (n=44) by:
• Role [academic vs practitioner vs both) (X2 GOF,p=0.298) • Focus [research vs teaching vs practice vs management] (X2 GOF,p=0.306) • Highest qualification level (X2 GOF,p=0.127) • Experience in education and training of public health nutritionists (X2 GOF,p=0.414)
• Country of practice (X2 GOF,p=0.863)

7
CORE FUNCTIONS....THE WORK OF PUBLIC HEALTH NUTRITION
It has been argued previously that workforce development specific to public health nutrition should be directed by a clear understanding of what constitutes the work of a public health nutritionist, informed by:
• analysis of public health nutrition problems, • prioritisation of work effort based on intelligence about the most effective interventions, and • consideration of the essential work required to effectively intervene [11].
Earlier attempts to codify core functions for public health nutrition have been made in an attempt to describe the work required of the public health nutrition workforce[12]. In this case the proposed core functions for public health nutrition where underpinned by a number of relevant assumptions, including that: • Public health nutrition functions are defined as those activities (processes, practices, services and
programs) which are undertaken by the workforce in order to promote optimal nutrition, health and well-being in populations.
• Core public health nutrition functions are those functions that are regarded as absolutely necessary, without which gaps would exist in public health capacity.
• The relative importance of functions may vary depending on the jurisdiction or workforce level. • Core functions are inter-related and complementary • Core functions articulate the work required to effectively address public health nutrition problems
or issues, and consequently provide a framework for identifying and conceptualising workforce development needs.
• Current public health nutrition work practices do not always align with these core functions. They are therefore aspirational, outlining the practices required for effective public health nutrition action and are a pointer to practice improvement[12].
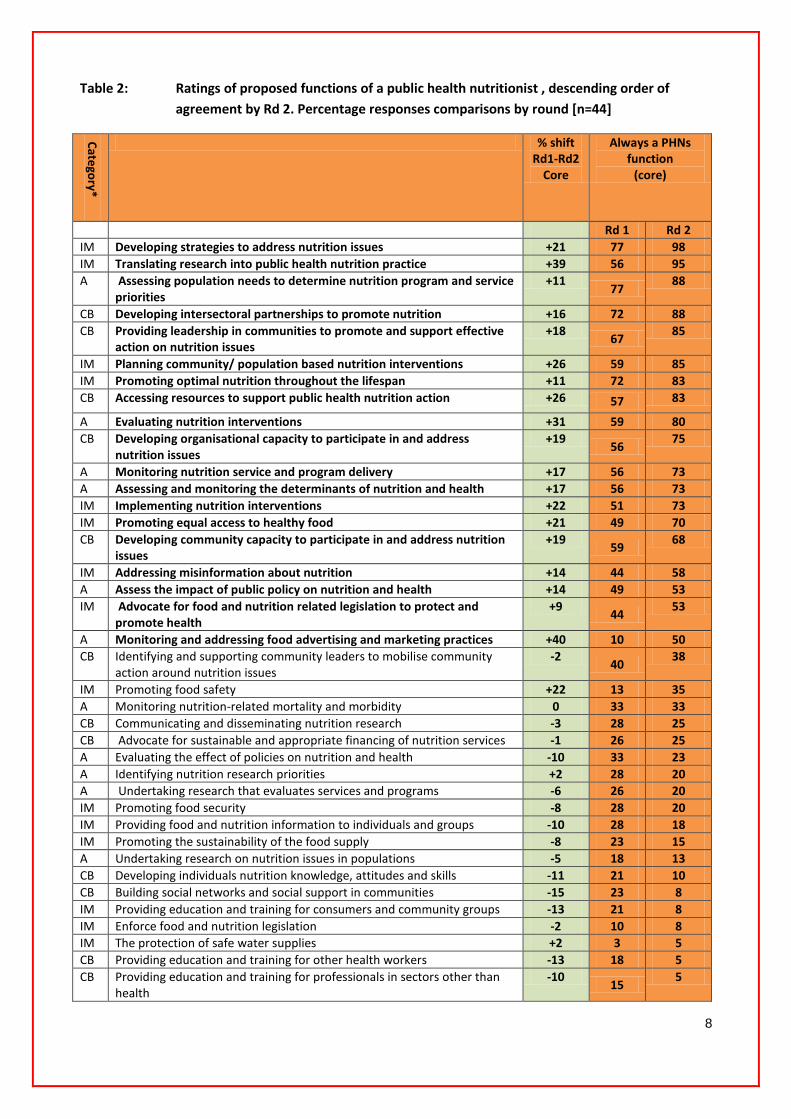
In the first and second survey rounds we invited panellists to rate the core functions of a public health nutritionist they believe are important for effective public health nutrition effort at a societal/community level, recognising that an individual public health nutritionist may have different functions and roles dependent on their employment context (eg. level in the health system, within other agencies, different populations etc). From an initial list of 46 functions rated in Rounds 1 and 2, fifteen (15; 33%) were rated as always a PHNs function (core) by the second round, above the consensus cut-off of 50% agreement. Table 2 illustrates the shifts in prioritization across the expert panel (n=43) between Rounds 1 and 2, trending to higher order agreement for functions identified as core in Rd 1.
Public health nutrition functions are defined as those activities (processes, practices, services and programs) which are undertaken in order to promote optimal nutrition, health and well-being in populations.
Core public health nutrition functions are those functions that are regarded as absolutely necessary, without which would imply gaps in public health capacity.
8
Table 2: Ratings of proposed functions of a public health nutritionist , descending order of agreement by Rd 2. Percentage responses comparisons by round [n=44]
Category*
% shift Rd1-Rd2
Core
Always a PHNs function
(core)
Rd 1 Rd 2 IM Developing strategies to address nutrition issues +21 77 98 IM Translating research into public health nutrition practice +39 56 95 A Assessing population needs to determine nutrition program and service
priorities +11
77 88
CB Developing intersectoral partnerships to promote nutrition +16 72 88 CB Providing leadership in communities to promote and support effective
action on nutrition issues +18
67 85
IM Planning community/ population based nutrition interventions +26 59 85 IM Promoting optimal nutrition throughout the lifespan +11 72 83 CB Accessing resources to support public health nutrition action +26 57 83
A Evaluating nutrition interventions +31 59 80 CB Developing organisational capacity to participate in and address
nutrition issues +19
56 75
A Monitoring nutrition service and program delivery +17 56 73 A Assessing and monitoring the determinants of nutrition and health +17 56 73 IM Implementing nutrition interventions +22 51 73 IM Promoting equal access to healthy food +21 49 70 CB Developing community capacity to participate in and address nutrition
issues +19
59 68
IM Addressing misinformation about nutrition +14 44 58 A Assess the impact of public policy on nutrition and health +14 49 53 IM Advocate for food and nutrition related legislation to protect and
promote health +9
44 53
A Monitoring and addressing food advertising and marketing practices +40 10 50 CB Identifying and supporting community leaders to mobilise community
action around nutrition issues -2
40 38
IM Promoting food safety +22 13 35 A Monitoring nutrition-related mortality and morbidity 0 33 33 CB Communicating and disseminating nutrition research -3 28 25 CB Advocate for sustainable and appropriate financing of nutrition services -1 26 25 A Evaluating the effect of policies on nutrition and health -10 33 23 A Identifying nutrition research priorities +2 28 20 A Undertaking research that evaluates services and programs -6 26 20 IM Promoting food security -8 28 20 IM Providing food and nutrition information to individuals and groups -10 28 18 IM Promoting the sustainability of the food supply -8 23 15 A Undertaking research on nutrition issues in populations -5 18 13 CB Developing individuals nutrition knowledge, attitudes and skills -11 21 10 CB Building social networks and social support in communities -15 23 8 IM Providing education and training for consumers and community groups -13 21 8 IM Enforce food and nutrition legislation -2 10 8 IM The protection of safe water supplies +2 3 5 CB Providing education and training for other health workers -13 18 5 CB Providing education and training for professionals in sectors other than
health -10
15 5
9
IM Review, formulate and promote health legislation -16 21 5 IM Community-based growth monitoring -20 23 3 A Economically evaluating nutrition programs or problems -7 10 3 IM Promoting equal access to physical activity -5 8 3 IM Using mass media for nutrition education -7 10 3 IM Developing dietary treatment strategies and plans for patients with
chronic disease -2
5 3
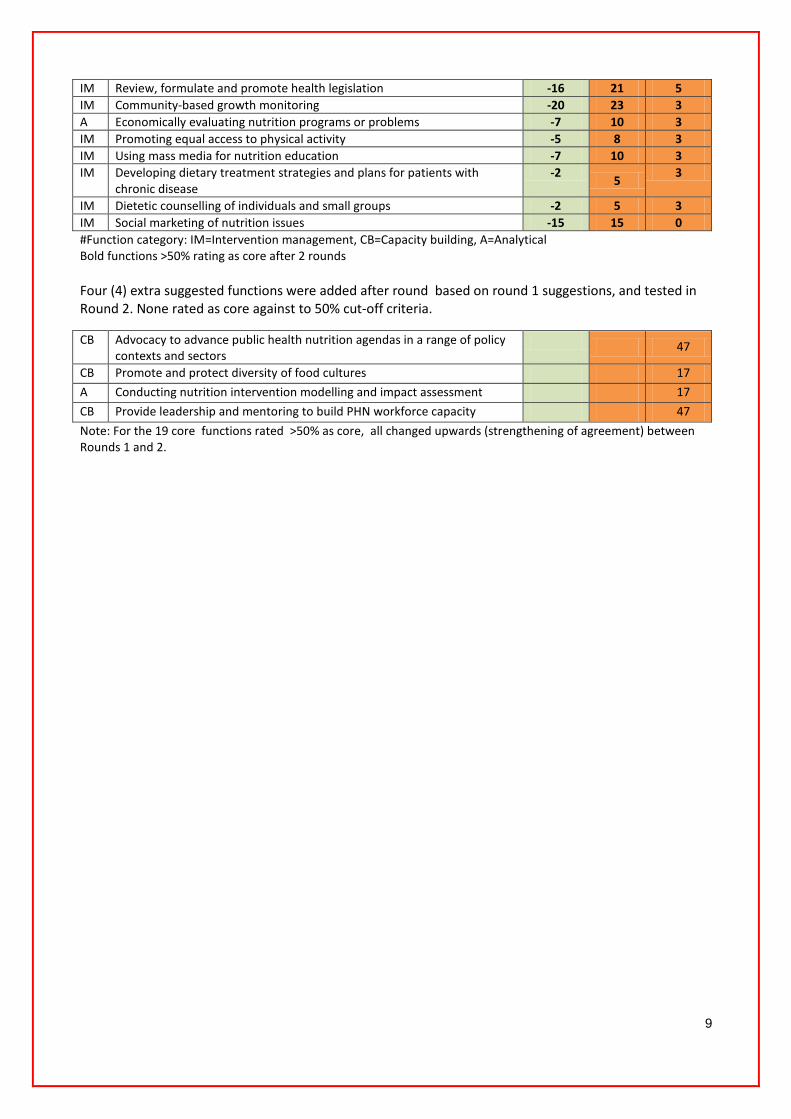
IM Dietetic counselling of individuals and small groups -2 5 3 IM Social marketing of nutrition issues -15 15 0 #Function category: IM=Intervention management, CB=Capacity building, A=Analytical Bold functions >50% rating as core after 2 rounds Four (4) extra suggested functions were added after round based on round 1 suggestions, and tested in Round 2. None rated as core against to 50% cut-off criteria.
CB Advocacy to advance public health nutrition agendas in a range of policy contexts and sectors
47
CB Promote and protect diversity of food cultures 17
A Conducting nutrition intervention modelling and impact assessment 17
CB Provide leadership and mentoring to build PHN workforce capacity 47
Note: For the 19 core functions rated >50% as core, all changed upwards (strengthening of agreement) between Rounds 1 and 2.

10
PERFORMANCE EXPECTATIONS IN DIFFERENT PRACTICE JURISDICTIONS
In Rounds 1 & 2, the practice context (e.g. level, location, population etc) was noted by panellist as a major issue when responding to questions about the type of work (functions) and competencies need to perform this work. This emphasised the importance of the context of practice. In Round 3 we challenged panellists to nominate what level of competency attainment (Table 4) [using a 5 point likert scale derived from the Dreyfus model of skills acquisition with 1= entry level increasing to 5= expert], they believed is needed in each of the 19 core function areas prioritised in Rds 1 & 2, at three different practice levels/jurisdictions (Table 3).
Table 3: Level of practice/jurisdiction
District level
Practice aligns with local community-level health service delivery e.g. a PHN employed in a local community health service.
Provincial level
Practice usually aligns with area-wide (more than one local level service provider) or state level responsibilities for program delivery, with less direct community contact and covering planning, coordination, management, delivery and evaluation of programs and workforce issues.
State/National Level
Practice usually aligns with state/national government level health system funding, planning, monitoring & surveillance, policy development and alignment, program evaluation.
Table 4: Level of competency required- definitions
Level Label Definition# 1 Entry-Level Operates through rules and regulations and requires guidance. Usually has good
disciplinary knowledge but has had limited opportunity to practice in public health. Responsibility usually limited in scope and the majority of decisions are routine in nature.
2 Capable Still rules based, but employ more complicated rules and procedures derived from experience to solve problems. Use public health specific competencies in daily practice and starting to demonstrate independence in practice.
3 Competent Have experience in practice, recognize that the complexity of certain elements in their work requires non-routine decision making, to which hard and fast rules do not clearly apply. i.e. apply practice-based judgment (aka “clinical judgement”). Might supervise other staff.
4 Proficient Make decisions by using intuition coupled with analytical thinking. See situations wholistically, using systems-level thinking when making decisions and assume leadership roles. May oversee multiple supervisors.
5 Expert Level 5 practitioners zero in on the central aspects of a problem, perform intuitively with only occasional need for deliberation. Spend substantial time reflecting on how systems work, assume leadership roles and assign leadership to others. They assess the quality of work done in their agency, making decisions with an eye to the big picture.
# Adapted from Koo & Miner. Outcome based workforce development and education in public health. Ann Rev Public Health. 2010 , 31; 253-269.
Table 5 summarises the most common (modal) ratings by expert panellists of level of competency attainment by level /jurisdiction of practice.

11
Table 5: Panellists ratings of competency attainment required for core functions performance, by level of practice, mode, n=44, percent responses
District Provincial State/ National
Developing strategies to address nutrition issues Competent [39%]
Proficient [34%]
Proficient [40%]
Translating research into public health nutrition practice Capable [34%]
Proficient [42%]
Proficient [42%]
Assessing population needs to determine nutrition program and service priorities
Competent [26%]
Proficient [40%]
Expert [37%]
Developing intersectoral partnerships to promote nutrition Capable [29%]
Proficient [42%]
Expert [42%]
Providing leadership in communities to promote and support effective action on nutrition issues
Competent [50%]
Proficient [53%]
Expert [43%]
Planning community/ population based nutrition interventions Proficient [26%]
Competent [45%]
Competent [46%]
Promoting optimal nutrition throughout the lifespan Entry-level [40%]
Competent [34%]
Competent [32%]
Accessing resources to support public health nutrition action Competent [37%]
Proficient [45%]
Expert [40%]
Evaluating nutrition interventions Competent [29%]
Proficient [37%]
Proficient [45%]
Developing organisational capacity to participate in and address nutrition issues
Competent [47%]
Proficient [49%]
Expert [45%]
Monitoring nutrition service and program delivery Competent [37%]
Competent [47%]
Proficient [34%]
Assessing and monitoring the determinants of nutrition and health Competent [50%]
Competent [42%]
Competent [26%]
Implementing nutrition interventions Entry-level [32%]
Competent [45%]
Competent [32%]
Promoting equal access to healthy food Competent [37%]
Competent [45%]
Expert [37%]
Developing community capacity to participate in and address nutrition issues
Competent [47%]
Competent [50%]
Proficient [45%]
Addressing misinformation about nutrition Entry-level [31%]
Competent [47%]
Expert [32%]
Assess the impact of public policy on nutrition and health Proficient [29%]
Proficient [53%]
Expert [63%]
Advocate for food and nutrition related legislation to protect and promote health
Capable [26%]
Proficient [37%]
Expert [63%]
Monitoring and addressing food advertising and marketing practices Competent [26%]
Competent [50%]
Competent [32%]
Darker shading implies higher level of competency attainment required.
12
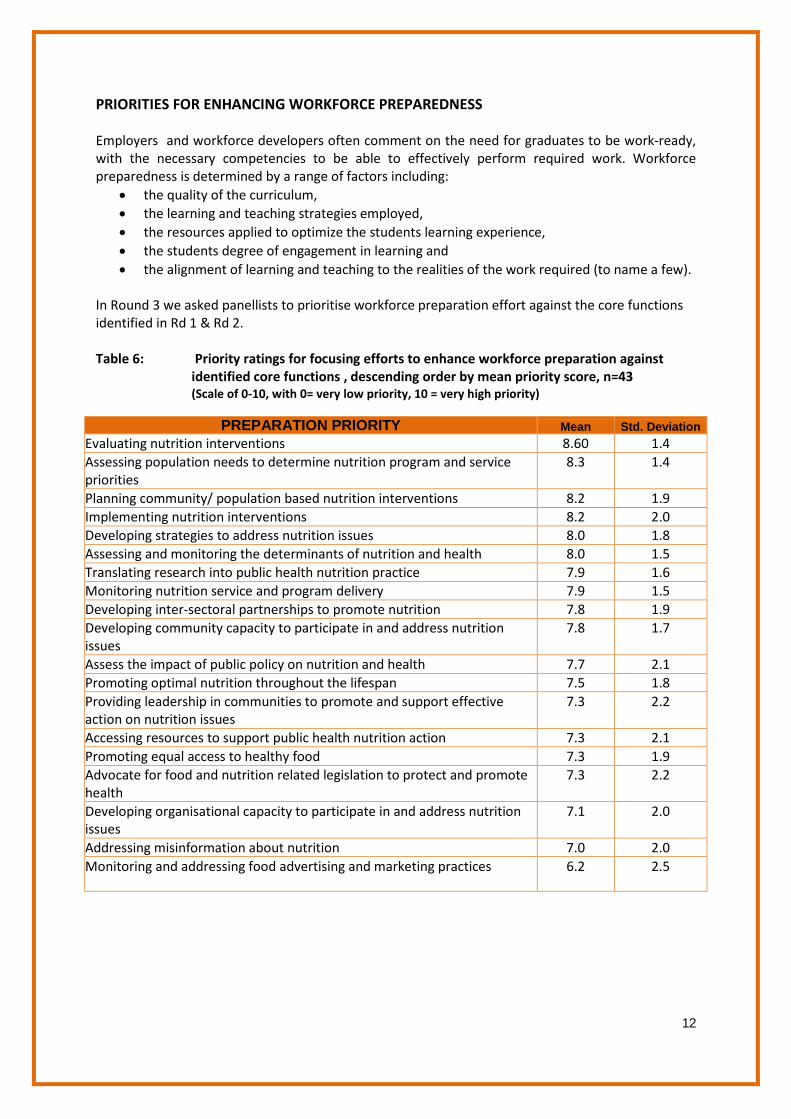
PRIORITIES FOR ENHANCING WORKFORCE PREPAREDNESS Employers and workforce developers often comment on the need for graduates to be work-ready, with the necessary competencies to be able to effectively perform required work. Workforce preparedness is determined by a range of factors including:
• the quality of the curriculum, • the learning and teaching strategies employed, • the resources applied to optimize the students learning experience, • the students degree of engagement in learning and • the alignment of learning and teaching to the realities of the work required (to name a few).
In Round 3 we asked panellists to prioritise workforce preparation effort against the core functions identified in Rd 1 & Rd 2. Table 6: Priority ratings for focusing efforts to enhance workforce preparation against
identified core functions , descending order by mean priority score, n=43 (Scale of 0-10, with 0= very low priority, 10 = very high priority)
PREPARATION PRIORITY Mean Std. Deviation Evaluating nutrition interventions 8.60 1.4 Assessing population needs to determine nutrition program and service priorities
8.3 1.4
Planning community/ population based nutrition interventions 8.2 1.9 Implementing nutrition interventions 8.2 2.0 Developing strategies to address nutrition issues 8.0 1.8 Assessing and monitoring the determinants of nutrition and health 8.0 1.5 Translating research into public health nutrition practice 7.9 1.6 Monitoring nutrition service and program delivery 7.9 1.5 Developing inter-sectoral partnerships to promote nutrition 7.8 1.9 Developing community capacity to participate in and address nutrition issues
7.8 1.7
Assess the impact of public policy on nutrition and health 7.7 2.1 Promoting optimal nutrition throughout the lifespan 7.5 1.8 Providing leadership in communities to promote and support effective action on nutrition issues
7.3 2.2
Accessing resources to support public health nutrition action 7.3 2.1 Promoting equal access to healthy food 7.3 1.9 Advocate for food and nutrition related legislation to protect and promote health
7.3 2.2
Developing organisational capacity to participate in and address nutrition issues
7.1 2.0
Addressing misinformation about nutrition 7.0 2.0 Monitoring and addressing food advertising and marketing practices 6.2 2.5
13
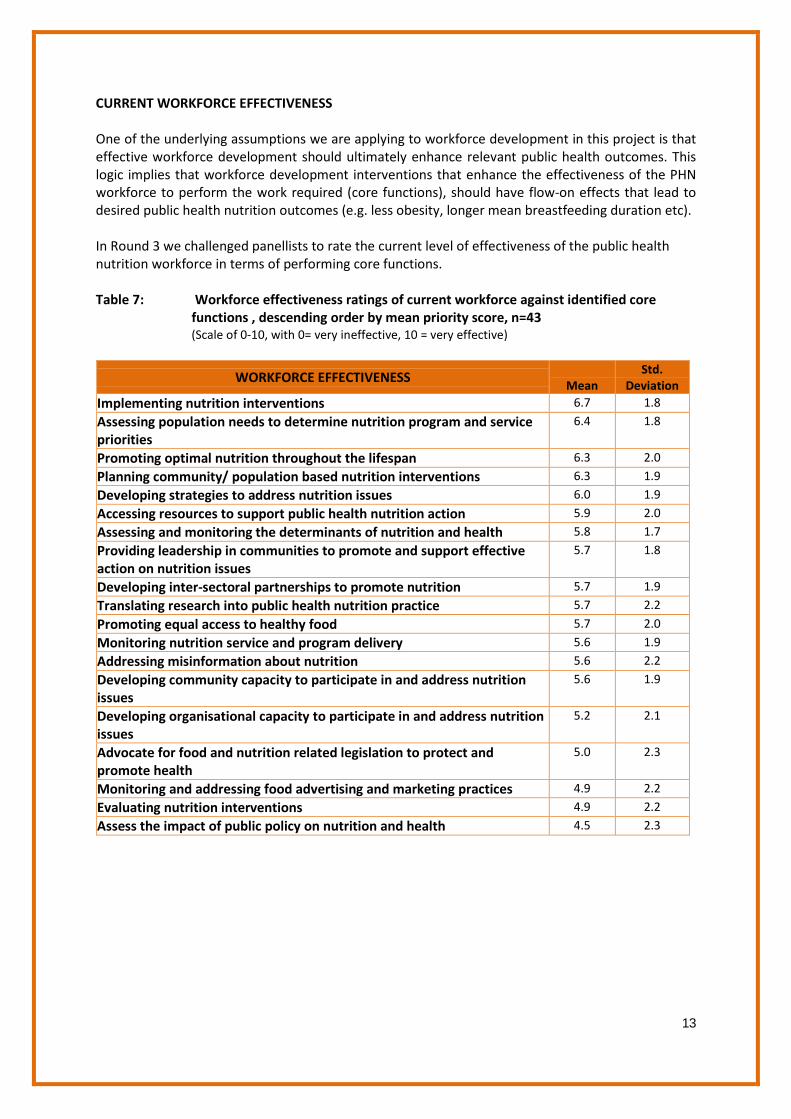
CURRENT WORKFORCE EFFECTIVENESS One of the underlying assumptions we are applying to workforce development in this project is that effective workforce development should ultimately enhance relevant public health outcomes. This logic implies that workforce development interventions that enhance the effectiveness of the PHN workforce to perform the work required (core functions), should have flow-on effects that lead to desired public health nutrition outcomes (e.g. less obesity, longer mean breastfeeding duration etc). In Round 3 we challenged panellists to rate the current level of effectiveness of the public health nutrition workforce in terms of performing core functions. Table 7: Workforce effectiveness ratings of current workforce against identified core
functions , descending order by mean priority score, n=43 (Scale of 0-10, with 0= very ineffective, 10 = very effective)
WORKFORCE EFFECTIVENESS Mean
Std. Deviation
Implementing nutrition interventions 6.7 1.8
Assessing population needs to determine nutrition program and service priorities
6.4 1.8
Promoting optimal nutrition throughout the lifespan 6.3 2.0
Planning community/ population based nutrition interventions 6.3 1.9
Developing strategies to address nutrition issues 6.0 1.9
Accessing resources to support public health nutrition action 5.9 2.0
Assessing and monitoring the determinants of nutrition and health 5.8 1.7
Providing leadership in communities to promote and support effective action on nutrition issues
5.7 1.8
Developing inter-sectoral partnerships to promote nutrition 5.7 1.9
Translating research into public health nutrition practice 5.7 2.2
Promoting equal access to healthy food 5.7 2.0
Monitoring nutrition service and program delivery 5.6 1.9
Addressing misinformation about nutrition 5.6 2.2
Developing community capacity to participate in and address nutrition issues
5.6 1.9
Developing organisational capacity to participate in and address nutrition issues
5.2 2.1
Advocate for food and nutrition related legislation to protect and promote health
5.0 2.3
Monitoring and addressing food advertising and marketing practices 4.9 2.2
Evaluating nutrition interventions 4.9 2.2
Assess the impact of public policy on nutrition and health 4.5 2.3

14
COMPETENCIES Competencies are promoted as important frameworks and benchmarks for workforce development that map out the knowledge, skills, personal attributes and “ways of thinking” necessary to effectively perform the work required to achieve public health nutrition outcomes. There have been numerous attempts world-wide to develop public health competencies, including competencies specific to public health nutrition. What is a competency? What is a competency
framework? How are competency
frameworks useful? Competencies are generally defined as the:
• knowledge • skills • personal attributes,
and • “ways of thinking”
necessary to effectively perform a certain role or task. A competency statement usually outlines the task/role that needs to be performed and codifies behavioural indicators which outline the skills and behaviours necessary to undertake the role/task effectively.
A competency framework is a complete collection of competencies and behavioural indicators. They usually contain detailed behavioural indicators related to specific roles and tasks, which by nature enable assessment of performance.
Competency frameworks provide the architecture for: • Curriculum development
and renewal • Assessment of
competence • Continuing professional
development planning • Recruitment and
performance management of staff (i.e. inform position description development)
• Credentialing–by providing standards that can be used as benchmarks for practitioner recognition or registration
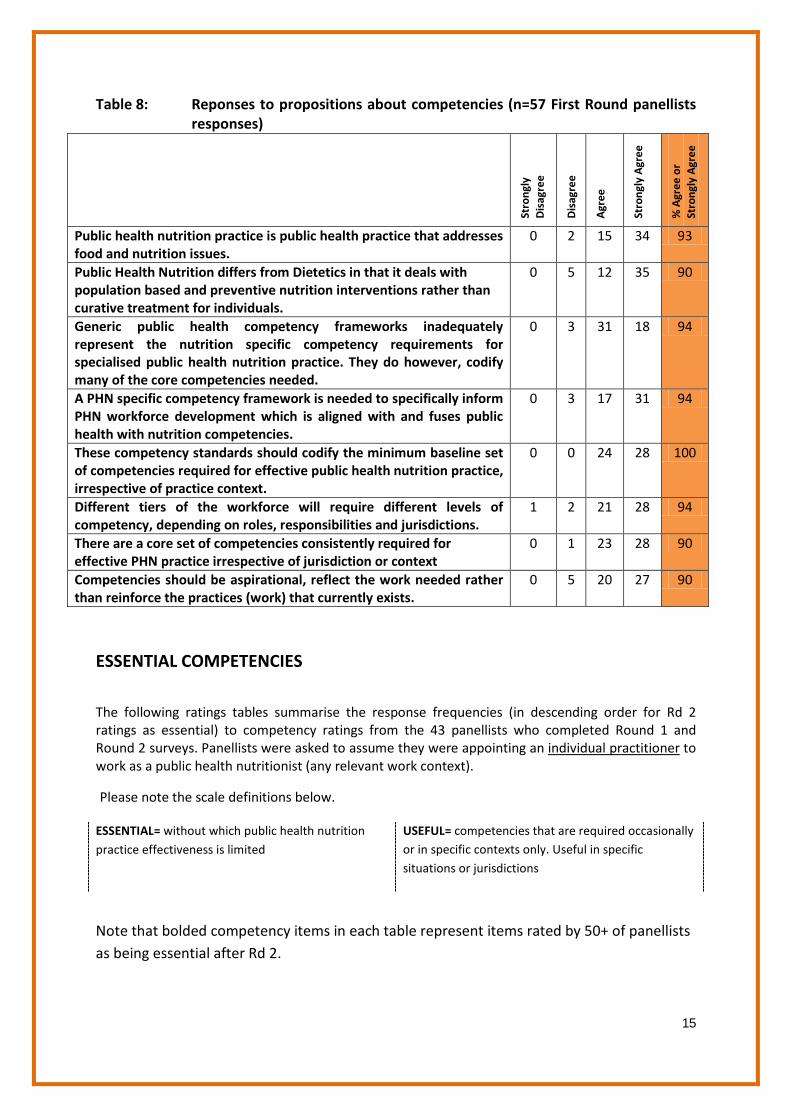
ASSUMPTIONS ABOUT COMPETENCIES In Round 1 we asked the 57 panellists in this round to rate their level of agreement with the following propositions about competencies (Table 8).
15
Table 8: Reponses to propositions about competencies (n=57 First Round panellists responses)
Stro
ngly
D
isag
ree
Dis
agre
e
Agr
ee
Stro
ngly
Agr
ee
% A
gree
or
Stro
ngly
Agr
ee
Public health nutrition practice is public health practice that addresses food and nutrition issues.
0 2 15 34 93
Public Health Nutrition differs from Dietetics in that it deals with population based and preventive nutrition interventions rather than curative treatment for individuals.
0 5 12 35 90
Generic public health competency frameworks inadequately represent the nutrition specific competency requirements for specialised public health nutrition practice. They do however, codify many of the core competencies needed.
0 3 31 18 94
A PHN specific competency framework is needed to specifically inform PHN workforce development which is aligned with and fuses public health with nutrition competencies.
0 3 17 31 94
These competency standards should codify the minimum baseline set of competencies required for effective public health nutrition practice, irrespective of practice context.
0 0 24 28 100
Different tiers of the workforce will require different levels of competency, depending on roles, responsibilities and jurisdictions.
1 2 21 28 94
There are a core set of competencies consistently required for effective PHN practice irrespective of jurisdiction or context
0 1 23 28 90
Competencies should be aspirational, reflect the work needed rather than reinforce the practices (work) that currently exists.
0 5 20 27 90
ESSENTIAL COMPETENCIES
The following ratings tables summarise the response frequencies (in descending order for Rd 2 ratings as essential) to competency ratings from the 43 panellists who completed Round 1 and Round 2 surveys. Panellists were asked to assume they were appointing an individual practitioner
Please note the scale definitions below.
to work as a public health nutritionist (any relevant work context).
ESSENTIAL= without which public health nutrition practice effectiveness is limited
USEFUL= competencies that are required occasionally or in specific contexts only. Useful in specific situations or jurisdictions
Note that bolded competency items in each table represent items rated by 50+ of panellists as being essential after Rd 2.
16
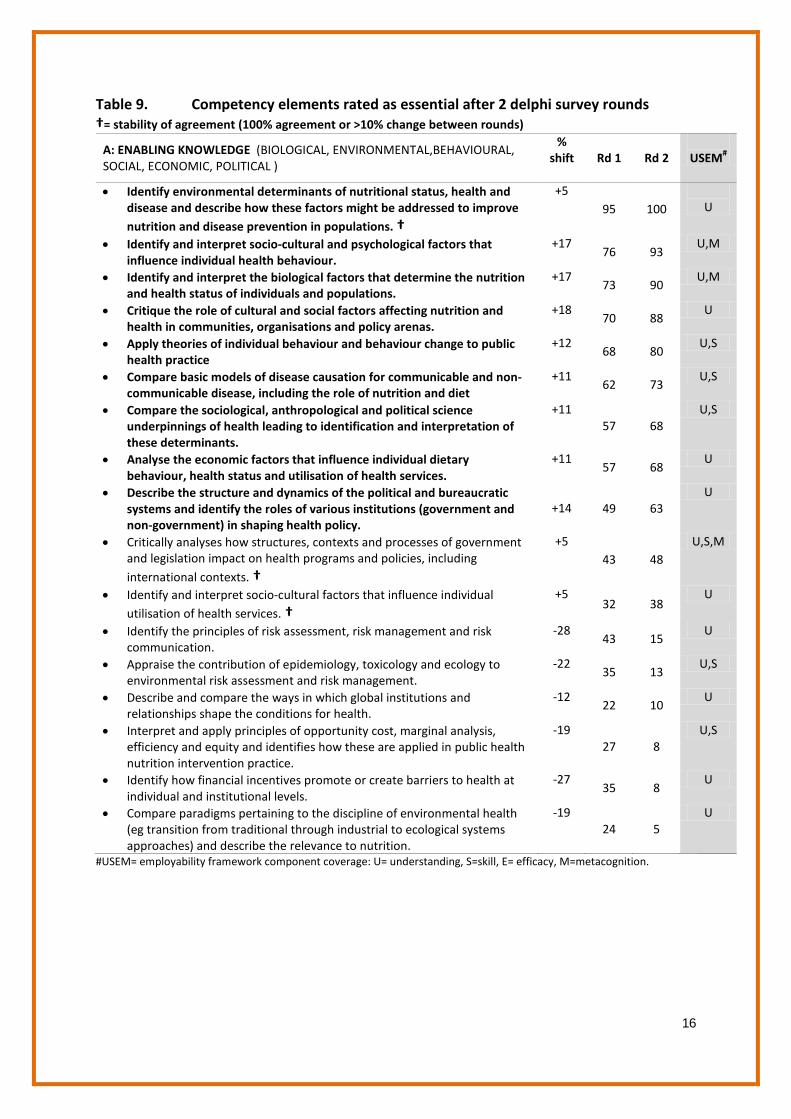
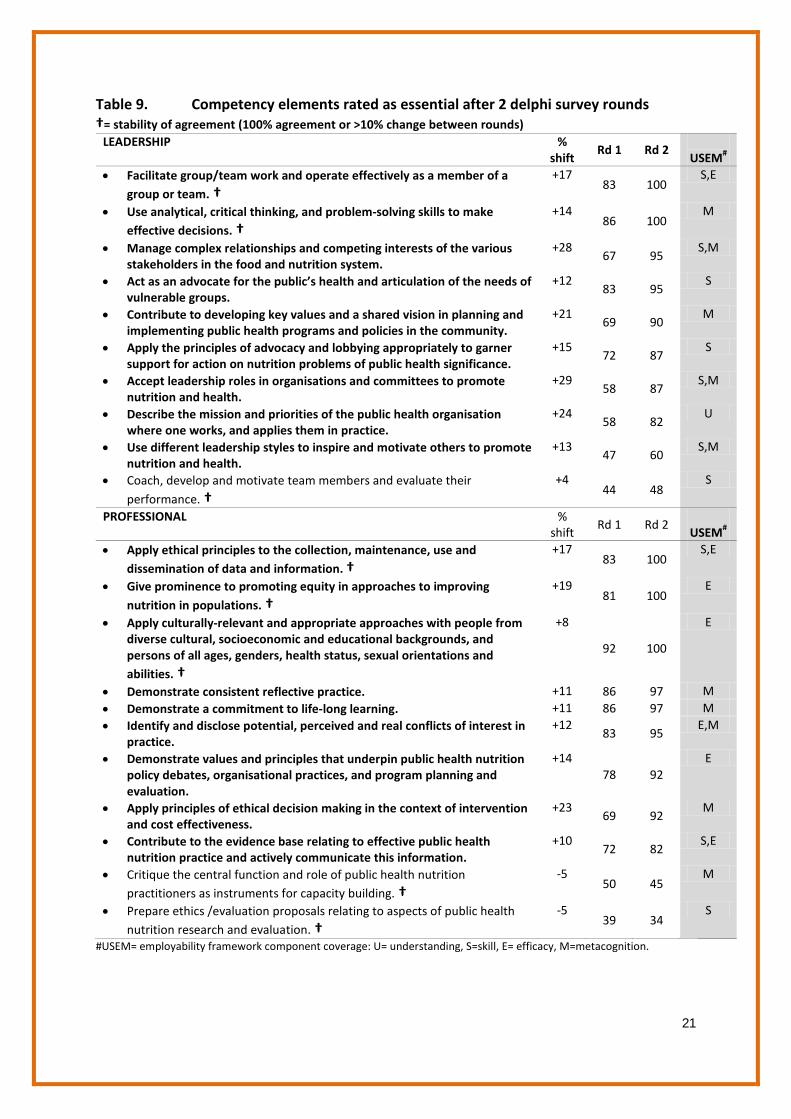
Table 9. Competency elements rated as essential after 2 delphi survey rounds †= stability of agreement (100% agreement or >10% change between rounds)
A: ENABLING KNOWLEDGE (BIOLOGICAL, ENVIRONMENTAL,BEHAVIOURAL, SOCIAL, ECONOMIC, POLITICAL )
% shift
Rd 1 Rd 2
USEM#
• Identify environmental determinants of nutritional status, health and disease and describe how these factors might be addressed to improve nutrition and disease prevention in populations. †
+5 95 100
U
• Identify and interpret socio-cultural and psychological factors that influence individual health behaviour.
+17 76 93
U,M
• Identify and interpret the biological factors that determine the nutrition and health status of individuals and populations.
+17 73 90
U,M
• Critique the role of cultural and social factors affecting nutrition and health in communities, organisations and policy arenas.
+18 70 88
U
• Apply theories of individual behaviour and behaviour change to public health practice
+12 68 80
U,S
• Compare basic models of disease causation for communicable and non-communicable disease, including the role of nutrition and diet
+11 62 73
U,S
• Compare the sociological, anthropological and political science underpinnings of health leading to identification and interpretation of these determinants.
+11 57 68
U,S
• Analyse the economic factors that influence individual dietary behaviour, health status and utilisation of health services.
+11 57 68
U
• Describe the structure and dynamics of the political and bureaucratic systems and identify the roles of various institutions (government and non-government) in shaping health policy.
+14 49 63
U
• Critically analyses how structures, contexts and processes of government and legislation impact on health programs and policies, including international contexts. †
+5 43 48
U,S,M
• Identify and interpret socio-cultural factors that influence individual utilisation of health services. †
+5 32 38
U
• Identify the principles of risk assessment, risk management and risk communication.
-28 43 15
U
• Appraise the contribution of epidemiology, toxicology and ecology to environmental risk assessment and risk management.
-22 35 13
U,S
• Describe and compare the ways in which global institutions and relationships shape the conditions for health.
-12 22 10
U
• Interpret and apply principles of opportunity cost, marginal analysis, efficiency and equity and identifies how these are applied in public health nutrition intervention practice.
-19 27 8
U,S
• Identify how financial incentives promote or create barriers to health at individual and institutional levels.
-27 35 8
U
• Compare paradigms pertaining to the discipline of environmental health (eg transition from traditional through industrial to ecological systems approaches) and describe the relevance to nutrition.
-19 24 5
U
#USEM= employability framework component coverage: U= understanding, S=skill, E= efficacy, M=metacognition.
17
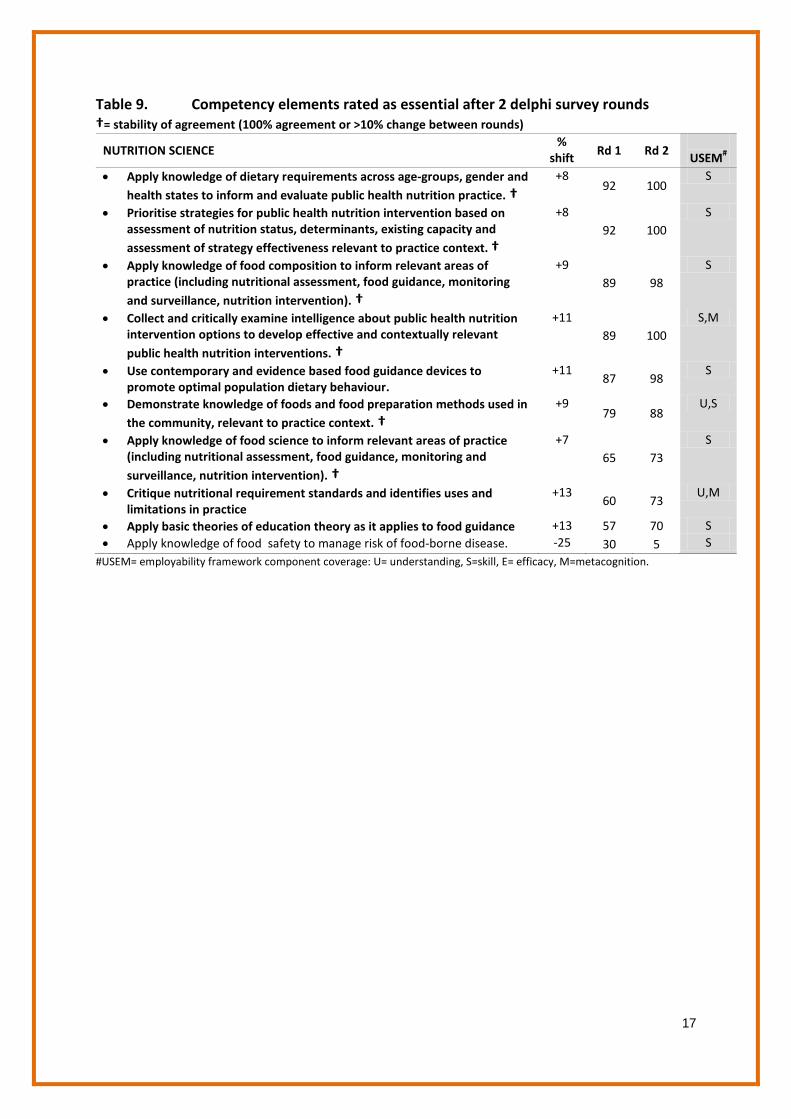
Table 9. Competency elements rated as essential after 2 delphi survey rounds †= stability of agreement (100% agreement or >10% change between rounds)
NUTRITION SCIENCE %
shift Rd 1 Rd 2
USEM# • Apply knowledge of dietary requirements across age-groups, gender and
health states to inform and evaluate public health nutrition practice. †
+8 92 100
S
• Prioritise strategies for public health nutrition intervention based on assessment of nutrition status, determinants, existing capacity and assessment of strategy effectiveness relevant to practice context. †
+8 92 100
S
• Apply knowledge of food composition to inform relevant areas of practice (including nutritional assessment, food guidance, monitoring and surveillance, nutrition intervention). †
+9 89 98
S
• Collect and critically examine intelligence about public health nutrition intervention options to develop effective and contextually relevant public health nutrition interventions. †
+11 89 100
S,M
• Use contemporary and evidence based food guidance devices to promote optimal population dietary behaviour.
+11 87 98
S
• Demonstrate knowledge of foods and food preparation methods used in the community, relevant to practice context. †
+9 79 88
U,S
• Apply knowledge of food science to inform relevant areas of practice (including nutritional assessment, food guidance, monitoring and surveillance, nutrition intervention). †
+7 65 73
S
• Critique nutritional requirement standards and identifies uses and limitations in practice
+13 60 73
U,M
• Apply basic theories of education theory as it applies to food guidance +13 57 70 S • Apply knowledge of food safety to manage risk of food-borne disease. -25 30 5 S
#USEM= employability framework component coverage: U= understanding, S=skill, E= efficacy, M=metacognition.
18
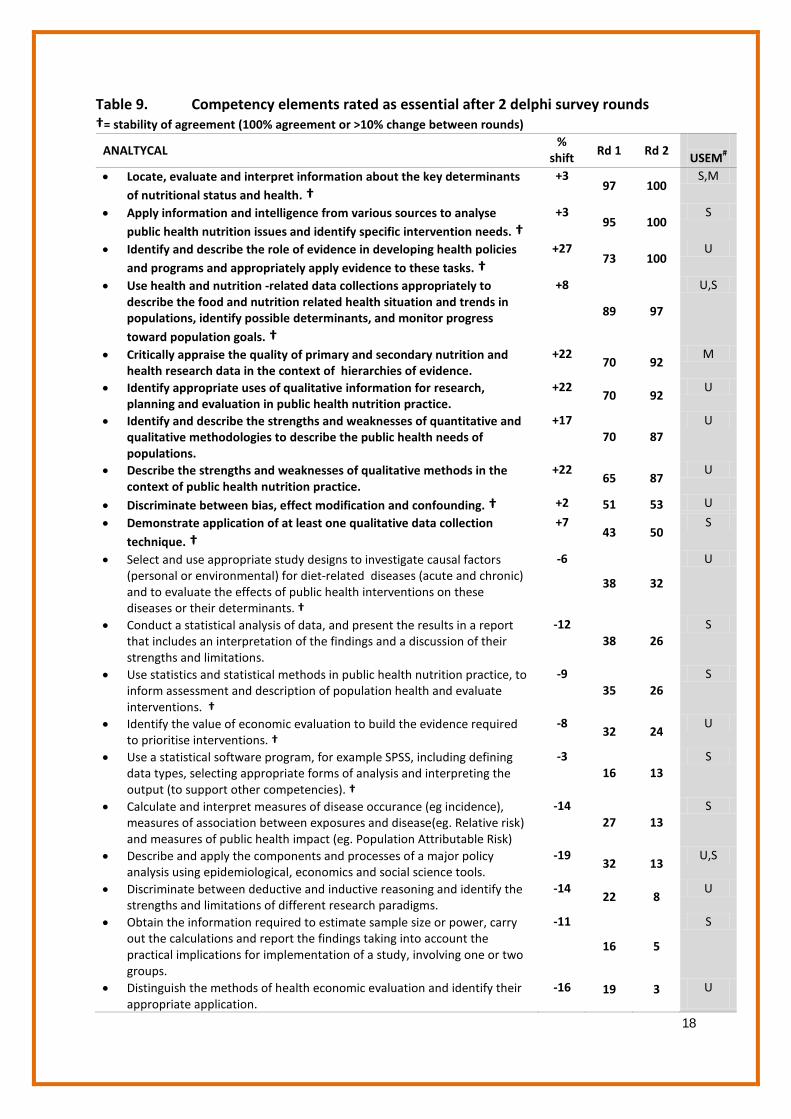
Table 9. Competency elements rated as essential after 2 delphi survey rounds †= stability of agreement (100% agreement or >10% change between rounds)
ANALTYCAL %
shift Rd 1 Rd 2
USEM# • Locate, evaluate and interpret information about the key determinants
of nutritional status and health. †
+3 97 100
S,M
• Apply information and intelligence from various sources to analyse public health nutrition issues and identify specific intervention needs. †
+3 95 100
S
• Identify and describe the role of evidence in developing health policies and programs and appropriately apply evidence to these tasks. †
+27 73 100
U
• Use health and nutrition -related data collections appropriately to describe the food and nutrition related health situation and trends in populations, identify possible determinants, and monitor progress toward population goals. †
+8
89 97
U,S
• Critically appraise the quality of primary and secondary nutrition and health research data in the context of hierarchies of evidence.
+22 70 92
M
• Identify appropriate uses of qualitative information for research, planning and evaluation in public health nutrition practice.
+22 70 92
U
• Identify and describe the strengths and weaknesses of quantitative and qualitative methodologies to describe the public health needs of populations.
+17 70 87
U
• Describe the strengths and weaknesses of qualitative methods in the context of public health nutrition practice.
+22 65 87
U
• Discriminate between bias, effect modification and confounding. † +2 51 53 U
• Demonstrate application of at least one qualitative data collection technique. †
+7 43 50
S
• Select and use appropriate study designs to investigate causal factors (personal or environmental) for diet-related diseases (acute and chronic) and to evaluate the effects of public health interventions on these diseases or their determinants. †
-6
38 32
U
• Conduct a statistical analysis of data, and present the results in a report that includes an interpretation of the findings and a discussion of their strengths and limitations.
-12 38 26
S
• Use statistics and statistical methods in public health nutrition practice, to inform assessment and description of population health and evaluate interventions. †
-9 35 26
S
• Identify the value of economic evaluation to build the evidence required to prioritise interventions. †
-8 32 24
U
• Use a statistical software program, for example SPSS, including defining data types, selecting appropriate forms of analysis and interpreting the output (to support other competencies). †
-3 16 13
S
• Calculate and interpret measures of disease occurance (eg incidence), measures of association between exposures and disease(eg. Relative risk) and measures of public health impact (eg. Population Attributable Risk)
-14 27 13
S
• Describe and apply the components and processes of a major policy analysis using epidemiological, economics and social science tools.
-19 32 13
U,S
• Discriminate between deductive and inductive reasoning and identify the strengths and limitations of different research paradigms.
-14 22 8
U
• Obtain the information required to estimate sample size or power, carry out the calculations and report the findings taking into account the practical implications for implementation of a study, involving one or two groups.
-11
16 5
S
• Distinguish the methods of health economic evaluation and identify their appropriate application.
-16 19 3 U

19
Table 9. Competency elements rated as essential after 2 delphi survey rounds †= stability of agreement (100% agreement or >10% change between rounds)
PUBLIC HEALTH SYSTEMS % shift
Rd 1 Rd 2
USEM# • Describe the major trends in health system development and identify
their implications for society. +73
22 95 U
• Contrast and use various approaches for setting priorities regarding problems and population groups to target, health and nutrition service development and investment, and nutrition-related research.
+26 64 90
U
• Identify and define the core functions of public health and identify the individual and organisational responsibilities within health and other sectors that fulfill these functions in a nutrition context.
+20 67 87
U
• Describe the interaction of public health with social and bureaucratic systems (including the health care system) to promote the health of populations.
+11 44 55
U
• Describe the structure and dynamics of the health system and the key dimensions of health system performance.
-20 31 11
U
• Describe financing arrangements and mechanisms for funding health services. †
-6 14 8
U
• Describe the historical development of public health and assess the implications of historical developments for current practice.
-17 22 5
U
FOOD AND NUTRITION SYSTEMS % shift Rd 1 Rd 2
USEM#
• Identify and categorise key stakeholders in the food and nutrition system. †
+11 89 100 U
• Describe the structure and dynamics of the food and nutrition system and the key dimensions of system performance.
+22 68 90 U
• Describe the major trends in food and nutrition system development and identify their implications for society.
+7 83 90 U
• Describe the mechanisms and impact of corporate profit motives and strategies that impact on food and nutrition.
-16 50 34 U
• Assess opportunities to improve nutrition and food standards within a food service .
-17 33 16 U
• Describe and compare food service systems. -14 22 8 U

20
Table 9. Competency elements rated as essential after 2 delphi survey rounds †= stability of agreement (100% agreement or >10% change between rounds)
NUTRITION EDUCATION % shift
Rd 1 Rd 2
USEM# • Translate technical nutrition information into practical advice and
guidance on food and eating. †
+8 89 97
S
• Develop nutrition education/guidance material that is evidence-based, culturally sensitive, and pitched at the appropriate literacy level, to meet the needs of the target group.
+14 83 97
S
• Communicate with individuals, groups, organisations and communities from various cultural socio-economic, organisational and professional backgrounds to enable them to take actions to improve nutrition and health outcomes.
+11
89 100
S
• Develop, implement and evaluate education programs to enable people to change their knowledge, attitudes and behaviour concerning health choices, taking account of the context in which target behaviours are performed.
+11
86 97
S
• Apply the basic principles of age-appropriate education and learning theories as they apply to public health nutrition practice.
+18 69 87
S
MANAGEMENT
% shift
Rd 1 Rd 2
USEM# • Describe and apply the procedures involved in translating policy into
organisational structures and plans. +43
44 87 U,S
• Describe and demonstrate in practice ethical financial management for health programs, including budgetary management.
+68 19 87
U,S
• Manage project resources achieving and reporting progress against budget and time-line contexts. †
+7 64 71
S
• Identify, estimate potential implications and manage risk as it applies to public health nutrition practice.
-29 61 32
S
• Apply human resource and industrial relations principles for organisational development, conflict resolution and the motivation and development of personnel.
+10 14 24
U,S
• Recognise and manage change taking into account educational, cultural, social, technical, economic and political considerations.
-28 36 8
S,M
#USEM= employability framework component coverage: U= understanding, S=skill, E= efficacy, M=metacognition.
21
Table 9. Competency elements rated as essential after 2 delphi survey rounds †= stability of agreement (100% agreement or >10% change between rounds)
LEADERSHIP % shift
Rd 1 Rd 2
USEM# • Facilitate group/team work and operate effectively as a member of a
group or team. †
+17 83 100
S,E
• Use analytical, critical thinking, and problem-solving skills to make effective decisions. †
+14 86 100
M
• Manage complex relationships and competing interests of the various stakeholders in the food and nutrition system.
+28 67 95
S,M
• Act as an advocate for the public’s health and articulation of the needs of vulnerable groups.
+12 83 95
S
• Contribute to developing key values and a shared vision in planning and implementing public health programs and policies in the community.
+21 69 90
M
• Apply the principles of advocacy and lobbying appropriately to garner support for action on nutrition problems of public health significance.
+15 72 87
S
• Accept leadership roles in organisations and committees to promote nutrition and health.
+29 58 87
S,M
• Describe the mission and priorities of the public health organisation where one works, and applies them in practice.
+24 58 82
U
• Use different leadership styles to inspire and motivate others to promote nutrition and health.
+13 47 60
S,M
• Coach, develop and motivate team members and evaluate their performance. †
+4 44 48
S
PROFESSIONAL % shift
Rd 1 Rd 2
USEM# • Apply ethical principles to the collection, maintenance, use and
dissemination of data and information. †
+17 83 100
S,E
• Give prominence to promoting equity in approaches to improving nutrition in populations. †
+19 81 100
E
• Apply culturally-relevant and appropriate approaches with people from diverse cultural, socioeconomic and educational backgrounds, and persons of all ages, genders, health status, sexual orientations and abilities. †
+8
92 100
E
• Demonstrate consistent reflective practice. +11 86 97 M • Demonstrate a commitment to life-long learning. +11 86 97 M • Identify and disclose potential, perceived and real conflicts of interest in
practice. +12
83 95 E,M
• Demonstrate values and principles that underpin public health nutrition policy debates, organisational practices, and program planning and evaluation.
+14 78 92
E
• Apply principles of ethical decision making in the context of intervention and cost effectiveness.
+23 69 92
M
• Contribute to the evidence base relating to effective public health nutrition practice and actively communicate this information.
+10 72 82
S,E
• Critique the central function and role of public health nutrition practitioners as instruments for capacity building. †
-5 50 45
M
• Prepare ethics /evaluation proposals relating to aspects of public health nutrition research and evaluation. †
-5 39 34
S
#USEM= employability framework component coverage: U= understanding, S=skill, E= efficacy, M=metacognition.
22
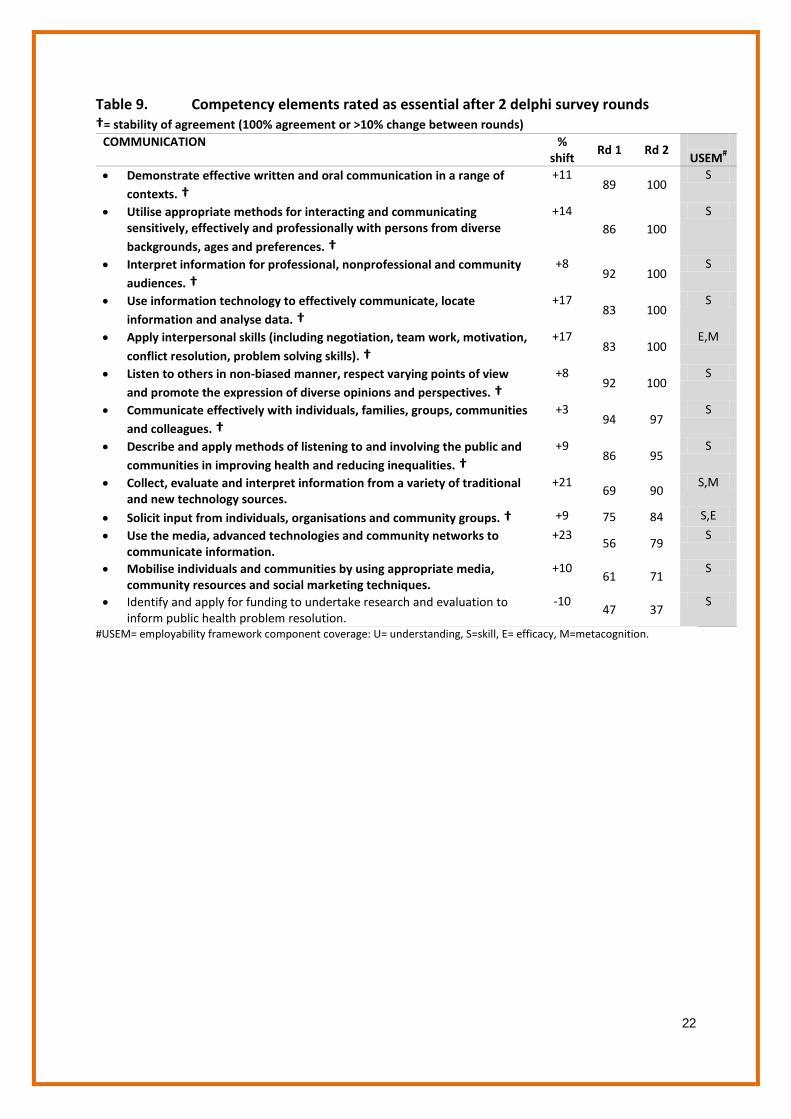
Table 9. Competency elements rated as essential after 2 delphi survey rounds †= stability of agreement (100% agreement or >10% change between rounds)
COMMUNICATION
% shift
Rd 1 Rd 2
USEM# • Demonstrate effective written and oral communication in a range of
contexts. †
+11 89 100
S
• Utilise appropriate methods for interacting and communicating sensitively, effectively and professionally with persons from diverse backgrounds, ages and preferences. †
+14 86 100
S
• Interpret information for professional, nonprofessional and community audiences. †
+8 92 100
S
• Use information technology to effectively communicate, locate information and analyse data. †
+17 83 100
S
• Apply interpersonal skills (including negotiation, team work, motivation, conflict resolution, problem solving skills). †
+17 83 100
E,M
• Listen to others in non-biased manner, respect varying points of view and promote the expression of diverse opinions and perspectives. †
+8 92 100
S
• Communicate effectively with individuals, families, groups, communities and colleagues. †
+3 94 97
S
• Describe and apply methods of listening to and involving the public and communities in improving health and reducing inequalities. †
+9 86 95
S
• Collect, evaluate and interpret information from a variety of traditional and new technology sources.
+21 69 90
S,M
• Solicit input from individuals, organisations and community groups. † +9 75 84 S,E
• Use the media, advanced technologies and community networks to communicate information.
+23 56 79
S
• Mobilise individuals and communities by using appropriate media, community resources and social marketing techniques.
+10 61 71
S
• Identify and apply for funding to undertake research and evaluation to inform public health problem resolution.
-10 47 37
S
#USEM= employability framework component coverage: U= understanding, S=skill, E= efficacy, M=metacognition.
23
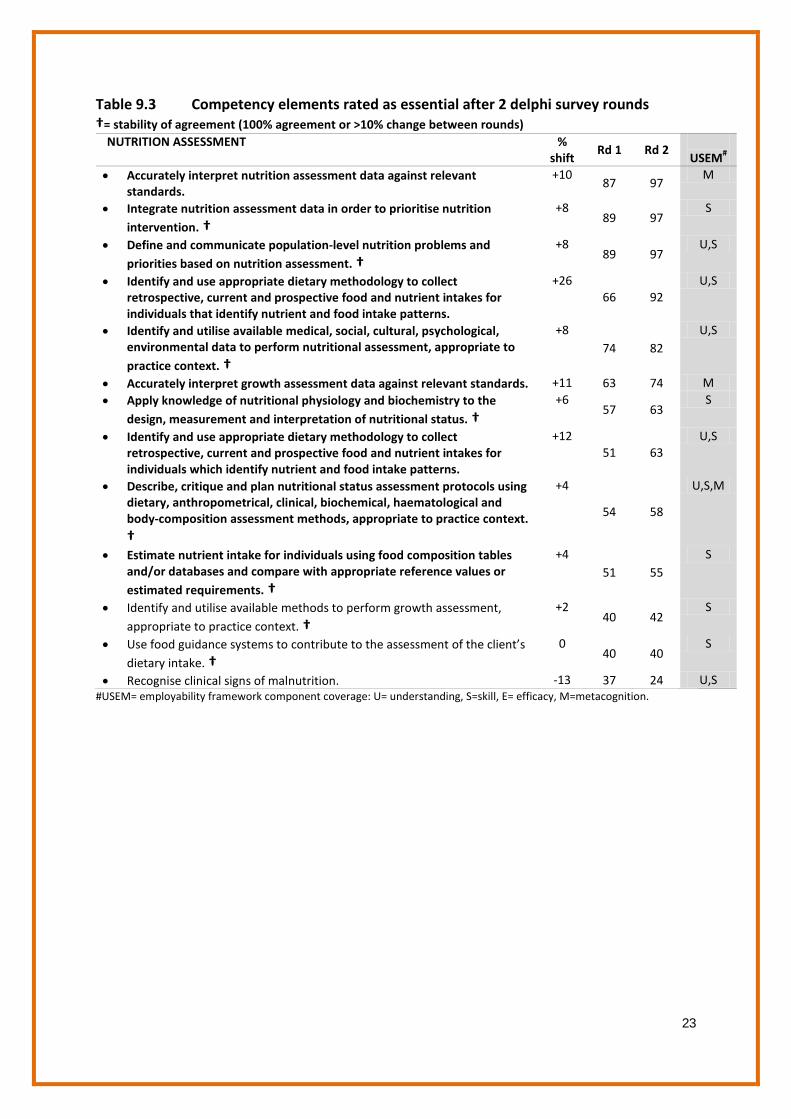
Table 9.3 Competency elements rated as essential after 2 delphi survey rounds †= stability of agreement (100% agreement or >10% change between rounds)
NUTRITION ASSESSMENT
% shift
Rd 1 Rd 2
USEM# • Accurately interpret nutrition assessment data against relevant
standards. +10
87 97 M
• Integrate nutrition assessment data in order to prioritise nutrition intervention. †
+8 89 97
S
• Define and communicate population-level nutrition problems and priorities based on nutrition assessment. †
+8 89 97
U,S
• Identify and use appropriate dietary methodology to collect retrospective, current and prospective food and nutrient intakes for individuals that identify nutrient and food intake patterns.
+26 66 92
U,S
• Identify and utilise available medical, social, cultural, psychological, environmental data to perform nutritional assessment, appropriate to practice context. †
+8 74 82
U,S
• Accurately interpret growth assessment data against relevant standards. +11 63 74 M • Apply knowledge of nutritional physiology and biochemistry to the
design, measurement and interpretation of nutritional status. †
+6 57 63
S
• Identify and use appropriate dietary methodology to collect retrospective, current and prospective food and nutrient intakes for individuals which identify nutrient and food intake patterns.
+12 51 63
U,S
• Describe, critique and plan nutritional status assessment protocols using dietary, anthropometrical, clinical, biochemical, haematological and body-composition assessment methods, appropriate to practice context. †
+4
54 58
U,S,M
• Estimate nutrient intake for individuals using food composition tables and/or databases and compare with appropriate reference values or estimated requirements. †
+4 51 55
S
• Identify and utilise available methods to perform growth assessment, appropriate to practice context. †
+2 40 42
S
• Use food guidance systems to contribute to the assessment of the client’s dietary intake. †
0 40 40
S
• Recognise clinical signs of malnutrition. -13 37 24 U,S #USEM= employability framework component coverage: U= understanding, S=skill, E= efficacy, M=metacognition.
24
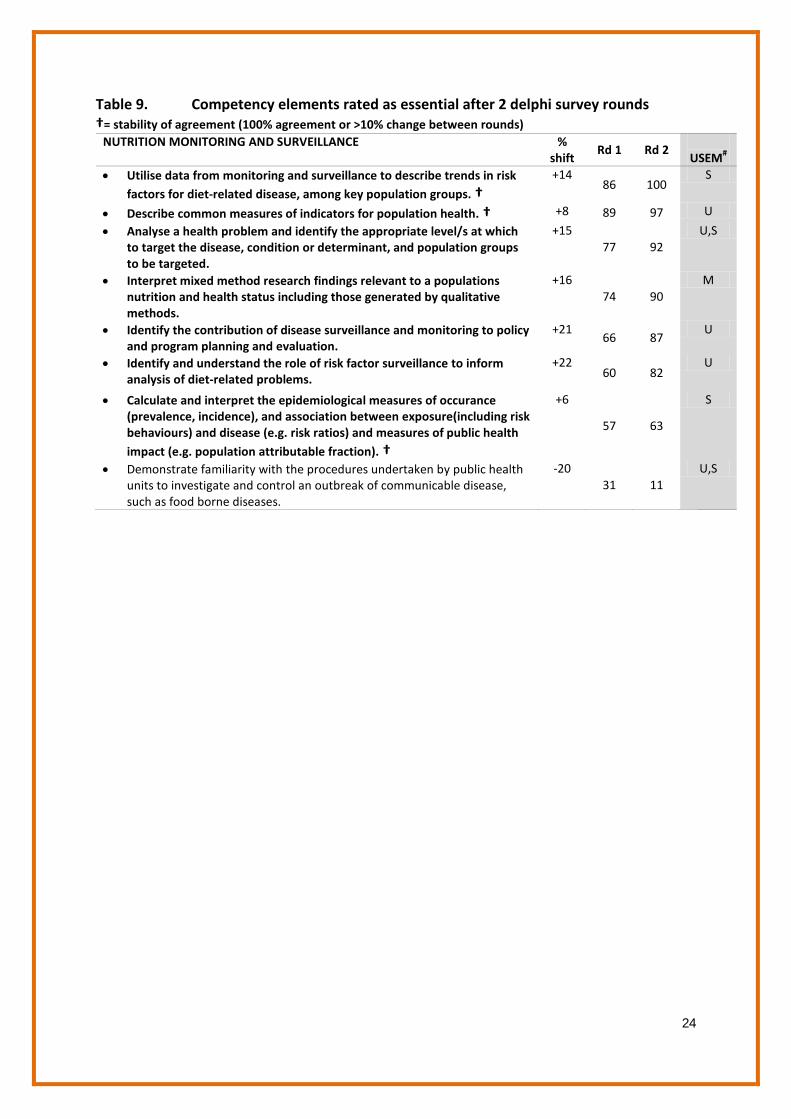
Table 9. Competency elements rated as essential after 2 delphi survey rounds †= stability of agreement (100% agreement or >10% change between rounds)
NUTRITION MONITORING AND SURVEILLANCE
% shift
Rd 1 Rd 2
USEM# • Utilise data from monitoring and surveillance to describe trends in risk
factors for diet-related disease, among key population groups. †
+14 86 100
S
• Describe common measures of indicators for population health. † +8 89 97 U
• Analyse a health problem and identify the appropriate level/s at which to target the disease, condition or determinant, and population groups to be targeted.
+15 77 92
U,S
• Interpret mixed method research findings relevant to a populations nutrition and health status including those generated by qualitative methods.
+16 74 90
M
• Identify the contribution of disease surveillance and monitoring to policy and program planning and evaluation.
+21 66 87
U
• Identify and understand the role of risk factor surveillance to inform analysis of diet-related problems.
+22 60 82
U
• Calculate and interpret the epidemiological measures of occurance (prevalence, incidence), and association between exposure(including risk behaviours) and disease (e.g. risk ratios) and measures of public health impact (e.g. population attributable fraction). †
+6
57 63
S
• Demonstrate familiarity with the procedures undertaken by public health units to investigate and control an outbreak of communicable disease, such as food borne diseases.
-20 31 11
U,S
25
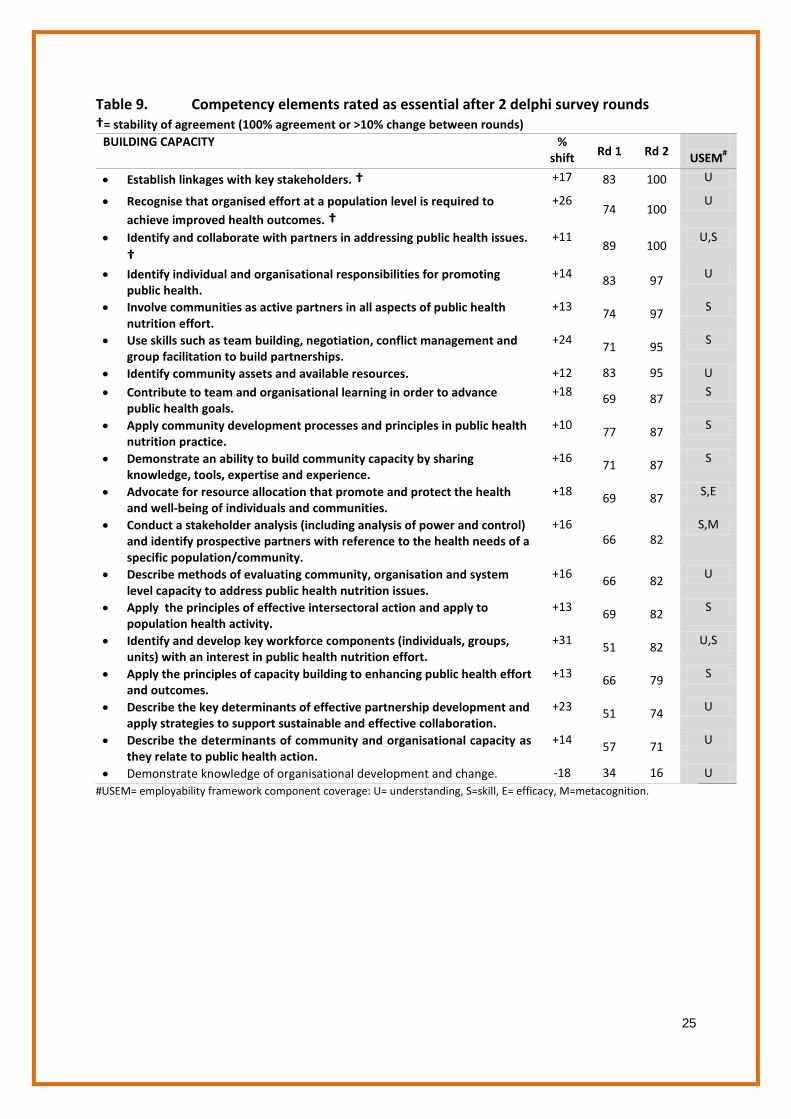
Table 9. Competency elements rated as essential after 2 delphi survey rounds †= stability of agreement (100% agreement or >10% change between rounds)
BUILDING CAPACITY
% shift Rd 1 Rd 2
USEM#
• Establish linkages with key stakeholders. † +17 83 100 U
• Recognise that organised effort at a population level is required to achieve improved health outcomes. †
+26 74 100
U
• Identify and collaborate with partners in addressing public health issues. †
+11 89 100
U,S
• Identify individual and organisational responsibilities for promoting public health.
+14 83 97 U
• Involve communities as active partners in all aspects of public health nutrition effort.
+13 74 97 S
• Use skills such as team building, negotiation, conflict management and group facilitation to build partnerships.
+24 71 95 S
• Identify community assets and available resources. +12 83 95 U
• Contribute to team and organisational learning in order to advance public health goals.
+18 69 87 S
• Apply community development processes and principles in public health nutrition practice.
+10 77 87 S
• Demonstrate an ability to build community capacity by sharing knowledge, tools, expertise and experience.
+16 71 87 S
• Advocate for resource allocation that promote and protect the health and well-being of individuals and communities.
+18 69 87 S,E
• Conduct a stakeholder analysis (including analysis of power and control) and identify prospective partners with reference to the health needs of a specific population/community.
+16 66 82
S,M
• Describe methods of evaluating community, organisation and system level capacity to address public health nutrition issues.
+16 66 82 U
• Apply the principles of effective intersectoral action and apply to population health activity.
+13 69 82 S
• Identify and develop key workforce components (individuals, groups, units) with an interest in public health nutrition effort.
+31 51 82 U,S
• Apply the principles of capacity building to enhancing public health effort and outcomes.
+13 66 79 S
• Describe the key determinants of effective partnership development and apply strategies to support sustainable and effective collaboration.
+23 51 74 U
• Describe the determinants of community and organisational capacity as they relate to public health action.
+14 57 71 U
• Demonstrate knowledge of organisational development and change. -18 34 16 U #USEM= employability framework component coverage: U= understanding, S=skill, E= efficacy, M=metacognition.
26
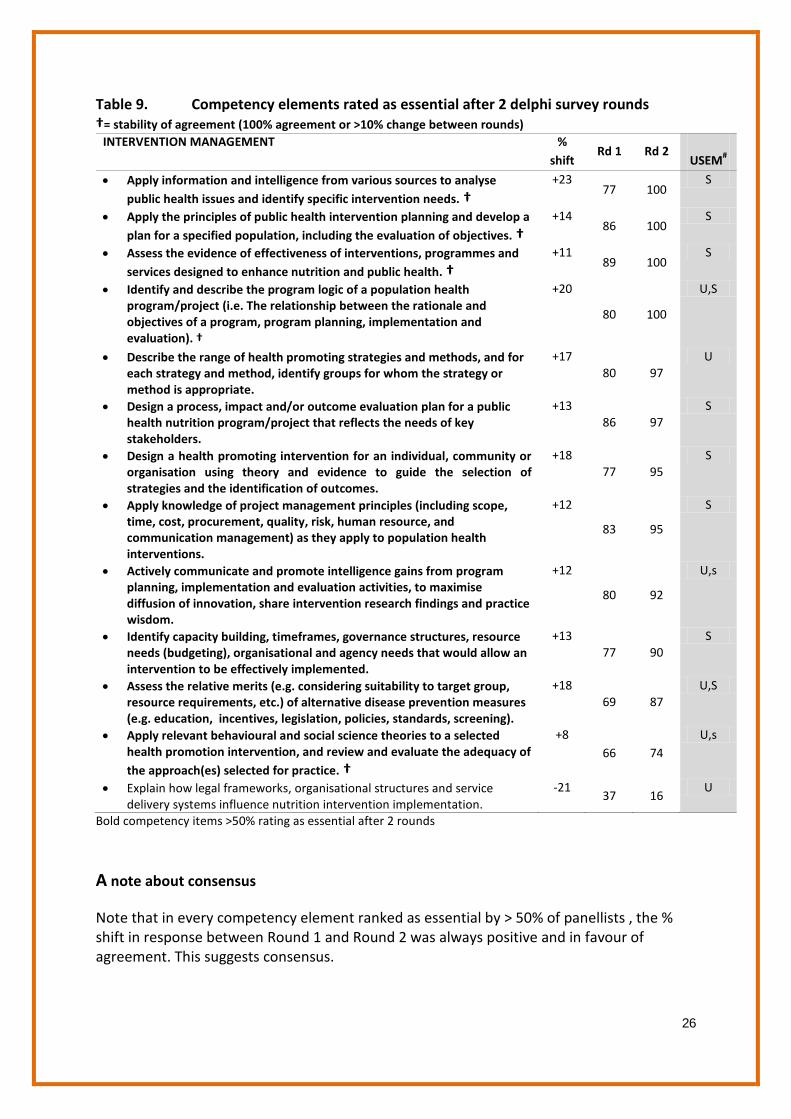
Table 9. Competency elements rated as essential after 2 delphi survey rounds †= stability of agreement (100% agreement or >10% change between rounds)
INTERVENTION MANAGEMENT
% shift
Rd 1 Rd 2
USEM#
• Apply information and intelligence from various sources to analyse public health issues and identify specific intervention needs. †
+23 77 100
S
• Apply the principles of public health intervention planning and develop a plan for a specified population, including the evaluation of objectives. †
+14 86 100
S
• Assess the evidence of effectiveness of interventions, programmes and services designed to enhance nutrition and public health. †
+11 89 100
S
• Identify and describe the program logic of a population health program/project (i.e. The relationship between the rationale and objectives of a program, program planning, implementation and evaluation). †
+20
80 100
U,S
• Describe the range of health promoting strategies and methods, and for each strategy and method, identify groups for whom the strategy or method is appropriate.
+17 80 97
U
• Design a process, impact and/or outcome evaluation plan for a public health nutrition program/project that reflects the needs of key stakeholders.
+13 86 97
S
• Design a health promoting intervention for an individual, community or organisation using theory and evidence to guide the selection of strategies and the identification of outcomes.
+18 77 95
S
• Apply knowledge of project management principles (including scope, time, cost, procurement, quality, risk, human resource, and communication management) as they apply to population health interventions.
+12
83 95
S
• Actively communicate and promote intelligence gains from program planning, implementation and evaluation activities, to maximise diffusion of innovation, share intervention research findings and practice wisdom.
+12
80 92
U,s
• Identify capacity building, timeframes, governance structures, resource needs (budgeting), organisational and agency needs that would allow an intervention to be effectively implemented.
+13 77 90
S
• Assess the relative merits (e.g. considering suitability to target group, resource requirements, etc.) of alternative disease prevention measures (e.g. education, incentives, legislation, policies, standards, screening).
+18 69 87
U,S
• Apply relevant behavioural and social science theories to a selected health promotion intervention, and review and evaluate the adequacy of the approach(es) selected for practice. †
+8 66 74
U,s
• Explain how legal frameworks, organisational structures and service delivery systems influence nutrition intervention implementation.
-21 37 16
U
Bold competency items >50% rating as essential after 2 rounds
A note about consensus
Note that in every competency element ranked as essential by > 50% of panellists , the % shift in response between Round 1 and Round 2 was always positive and in favour of agreement. This suggests consensus.
27
SUMMATIVE DISCUSSION
To what extent was the panel an expert panel?
This Delphi study included a cohort of 44 public health nutrition academics and practitioners completing 3 full survey rounds. The attributes of panellists indicate that they were highly qualified (63% with PhDs) and with over 75% self rating as having considerable or extensive experience in public health nutrition education and training. Given the sampling technique of targeted invitations based on professional network knowledge and the attribute data reported, it is reasonable to conclude that this Delphi panel was indeed an expert panel in this context.
Current workforce effectiveness and workforce development priorities
The Delphi panellists prioritised workforce preparation that targeted education and training to enable competent practice in public health nutrition intervention management (designing, implementing and evaluating interventions). This was consistent with the high ratings of existing workforce preparedness in these function categories. This probably reflects the reality of public health nutrition workforce activity in which practitioners are primarily engaged in developing programmatic interventions at a community level. Assessment of the effectiveness of the current public health nutrition workforce (as a proxy for workforce preparedness) suggests that workforce effectiveness in analytical and evaluative functions are however suboptimal.
Further clarity on the core work of public health nutritionists
The ratings and prioritisation of core functions for the public health nutrition workforce by level of practice in the health system serve to help delineate the contextual nuances of practice, and the related competency expectations by function and level of practice. Results suggest that as practitioners take on roles with broader population coverage (e.g. district to state), the expectations on competency attainment/requirement increase. This prioritisation of core functions (work) amy be of assistance in the development of human resource management and recruitment instruments such as position descriptions/duty statements.
Competencies
The data on essential competency requirements provides a comprehensive smorgasbord of statements relating to knowledge/understanding, skills, attitudes/ways of thinking (metacognition) and practitioner efficacy. This data can be used to inform the development of competency standards and frameworks to inform curriculum design and renewal, assessment and to focus learning and teaching strategy design.

28
Acknowledgements
The following panellists who completed all 3 rounds and gave permission to be acknowledged include : Steve Pratt, Susan Torres, Roscoe Taylor, Tini Gruner, Sharleen O'Reilly, John Coveney, Tony Worsley, Danielle Gallegos, Wendy Foley, Rex Milligan, Heather Yeatman, Rebecca Golley, Pamela Murch, Sandra Murray, Jane Scott, Claire Palermo, Andrea Begley, Lesley Patton, Julie Woods, Julie Parkinson, Mark Lawrence, Elizabeth Stephens, Fiona McKenzie-Lewis, Holley Jones, Geoff Marks, Veronica Graham, Sharon Laurence, Lisa Schubert, Rafat Hussain, Lauren Williams, Roger Hughes, Pattanee Winichagoon, Ann Fox, Barrie Margetts, Elisabetta Recine, Idrus Jus'at, Jennifer Davies, Christina Black, Betsy Haughton, Nasrin Omidvar, Irja Haapala, Geraldine McNeill. Their contribution as expert panellists is appreciated and acknowledged. Similar acknowledgement and appreciation is extended to the panellist (n=1) who elected not to be publicly acknowledged.
References
1. Jonsdottir, S., et al., Consensus on the competencies required for public health nutrition workforce development in Europe - The JobNut project. Public Health Nutrition, 2010. Accepted Jan 2010.(In print).
2. Hughes, R., Competencies for effective public health nutrition practice: a developing consensus. Public Health Nutr, 2004. 7(5): p. 683-91.
3. Murphy, M., et al., Consensus development methods, and their use in clinical guideline development. Health Technology Assessment, 1998. 2(3).
4. Rowe, G. and G. Wright, The Delphi techniqueas a forecasting tool: issues and analysis. International Journal of Forecasting, 1999. 15: p. 353-375.
5. Powell, C., The Delphi technique: myths and realities. Journal of Advanced Nursing. , 2003. 41: p. 376-382.
6. Keeney S, H.F. and, and M. H, Consulting the oracle: ten lessons from using the Delphi technique in nursing research. Journal of Advanced Nursing. , 2006. 53 p. 205-212.
7. Hughes, R., A competency framework for public health nutrition workforce development. 2005, Australian public Health nutrition Academic Collaboration: www.aphnac.com.
8. Hughes, R., A competency framework for public health nutrition: Position paper for the Australian Public Health Nutrition Academic Collaboration. . 2005, Australian Public Health Nutrition Academic Colllaboration: Southport.
9. Hughes, R., et al., Towards a competency framework for global public health nutrition workforce development. World Nutrition, 2011. [In press].
10. Duffield, C., The Delphi technique: a comparison of results obtained using two expert panels. Int. J. Nurs. Stud., 1993. 30(3): p. 227-237.
11. Hughes, R., A conceptual framework for intelligence-based public health nutrition workforce development. Public Health Nutrition, 2003. 6(6): p. 599-605.
12. Hughes, R., Introduction to Public Health Nutrition Practice, in Public Health Nutrition: From principles to practice, M.L.T. Worsley, Editor. 2007, Allen & Unwin: Crows Nest.
13. Hughes, R., Practices Overview, in Public Health Nutrition: From principles to practice., M.W. Lawrence, A. , Editor. 2007, Allen & Unwin: Crows Nest. p. 265-272.
14. Hughes, R. and B. Margetts, Practical Public Health Nutrition. 2011, Chichester: Wiley Blackwell.