Embed Size (px)
Citation preview
MNT in a Patient with Congestive
Heart FailureMegan Smith
UMD Dietetic InternMay 6, 2015
El Corazon
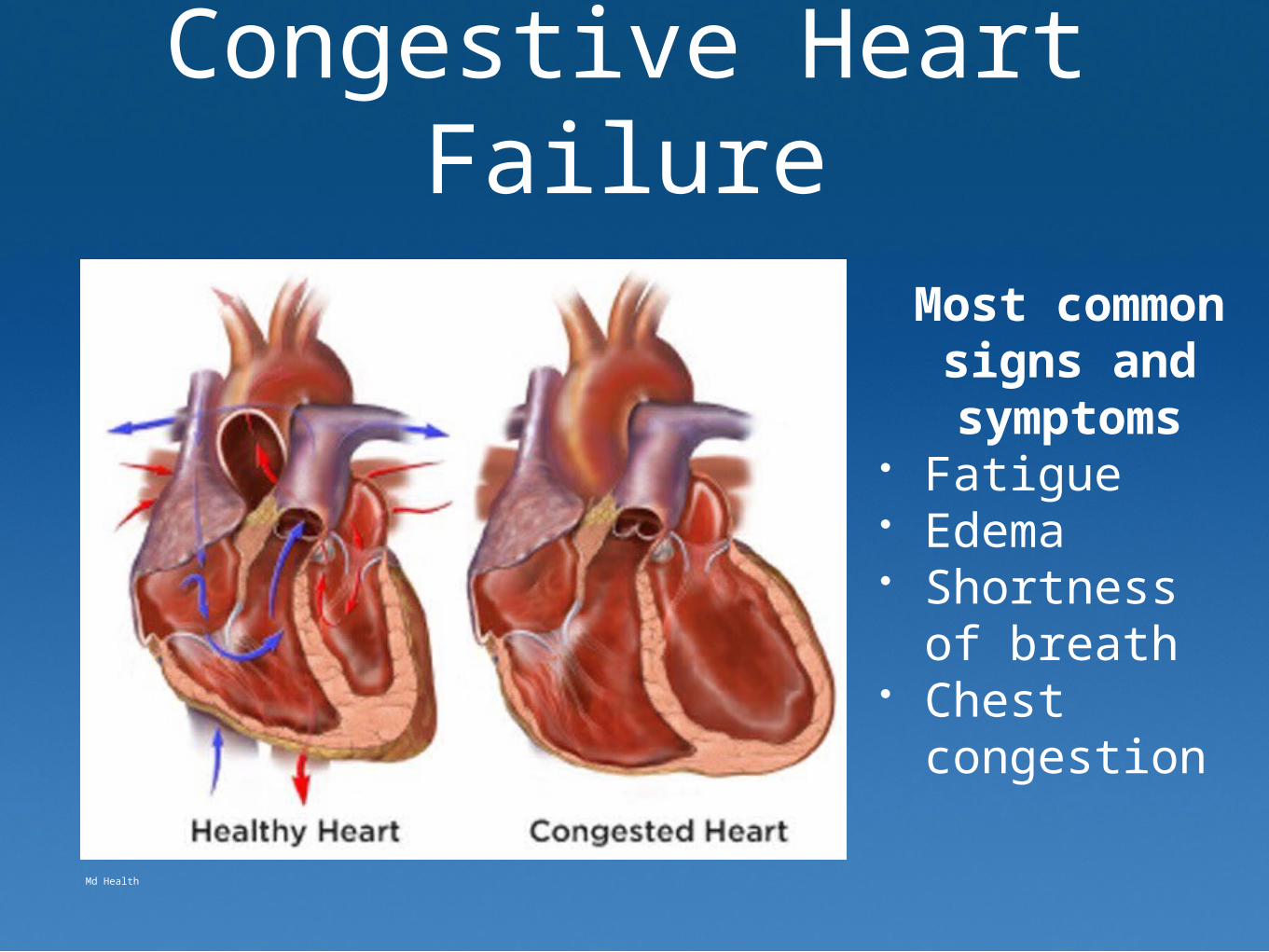
Congestive Heart Failure
Most common signs and symptoms
• Fatigue• Edema• Shortness of
breath• Chest
congestion
Md Health
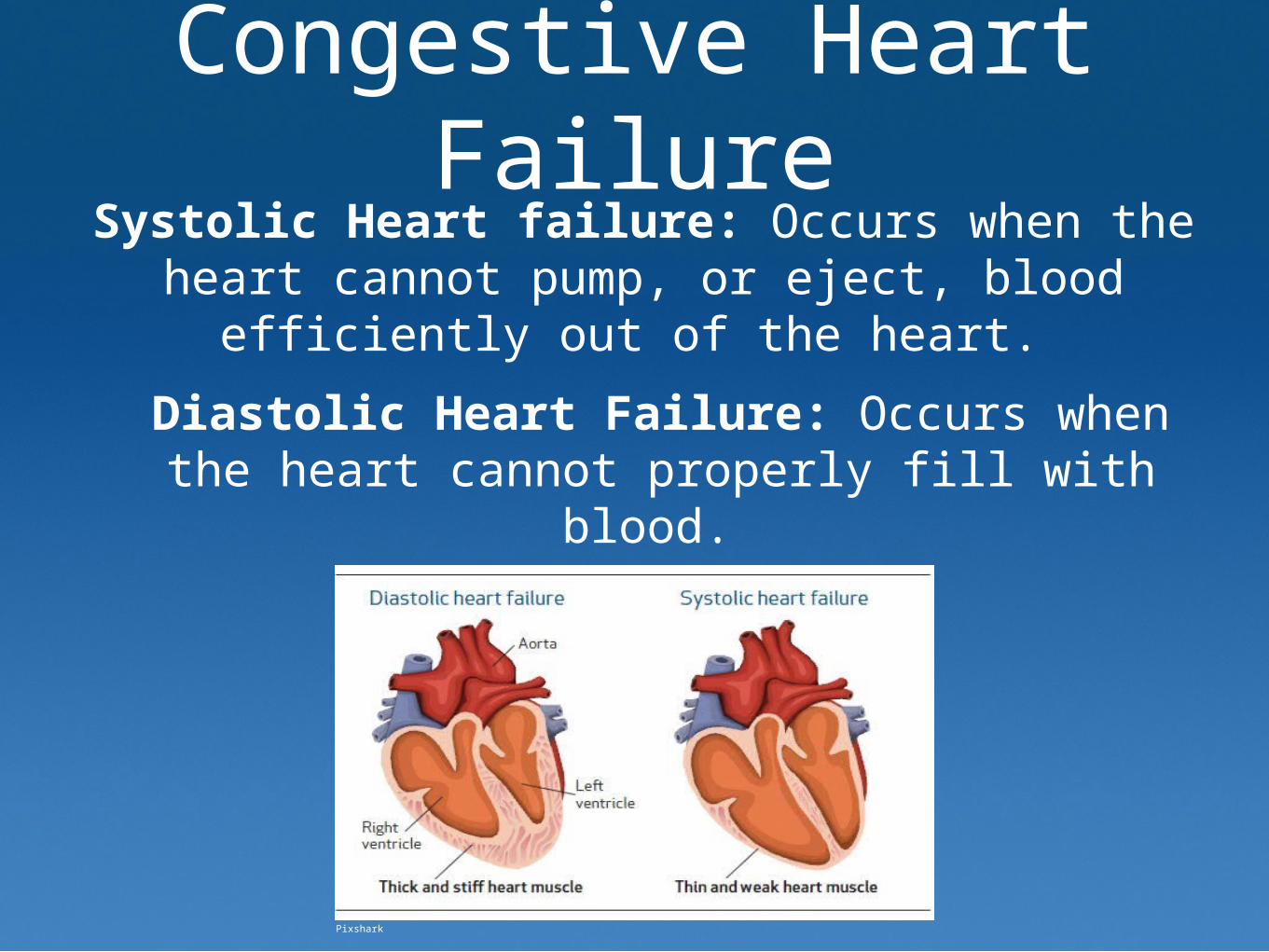
Congestive Heart Failure
Systolic Heart failure: Occurs when the heart cannot pump, or eject, blood efficiently out of
the heart.
Diastolic Heart Failure: Occurs when the heart cannot properly fill with blood.
Pixshark

Congestive Heart FailureEtiology most commonly includes:• Coronary Artery Disease• Myocardial Infarction• Uncontrolled Hypertension• Arrythmias, valve problems, drugs,and
alcohol can also contribute
Leading Predictors• Coronary artery disease• Poorly controlled blood pressure• Elevated B natriuretic peptides
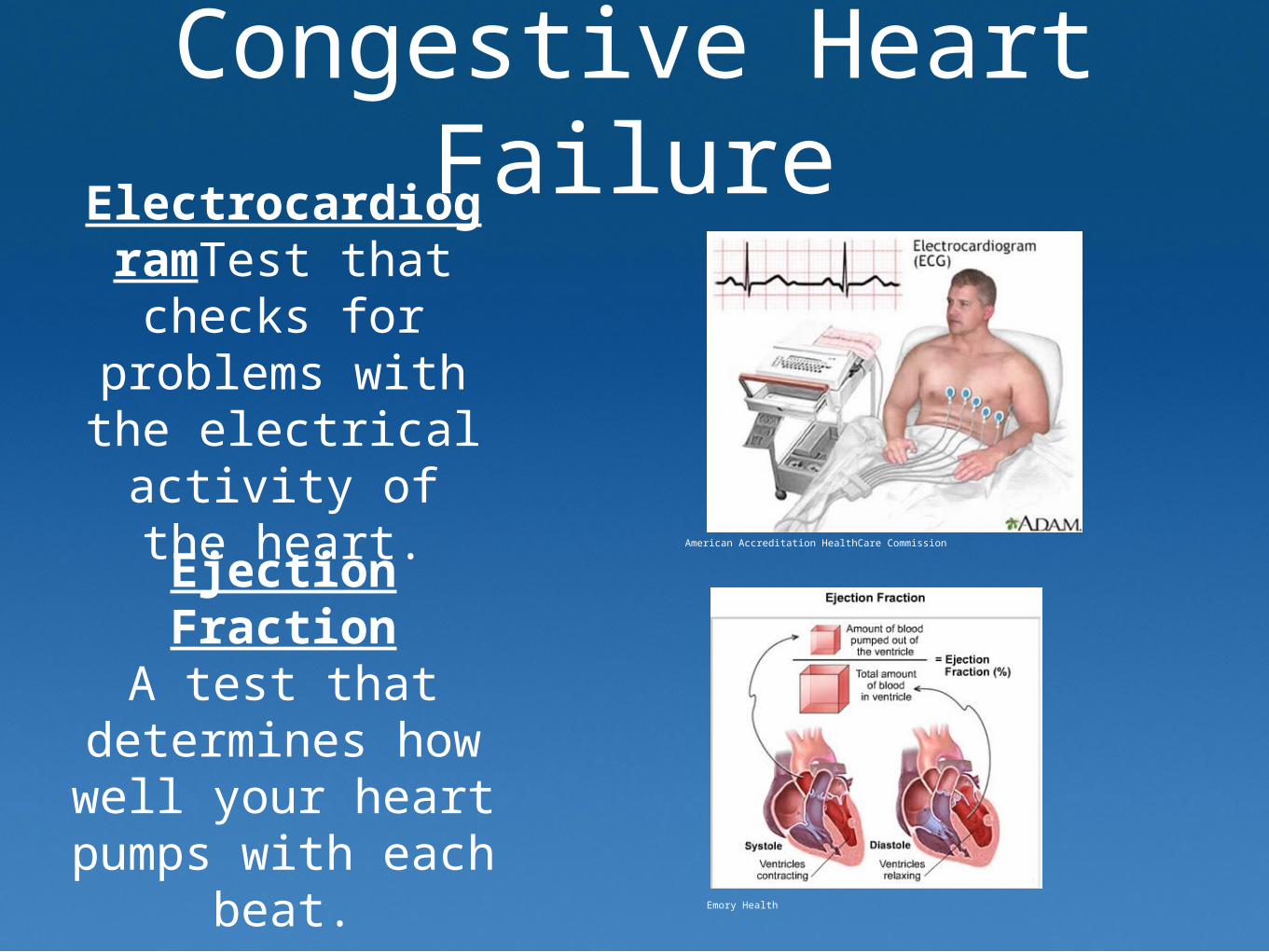
Congestive Heart Failure
ElectrocardiogramTest that checks
for problems with the electrical activity of the
heart.
Ejection FractionA test that
determines how well your heart
pumps with each beat.
American Accreditation HealthCare Commission
Emory Health

Meet the Patient
• XX is a 59 year-old Caucasian male• Married with two daughters• Lives at home with wife• Employed as a physician by a local
Baltimore Hospital
Medical Considerations
Diagnosis: Acute left systolic heart failure with aortic insufficiency. Broadly referred to
as CHF.
PMH: hypertension
Echocardiogram: Ejection Fraction was 20-25%
Signs/Symptoms: Fatigue, loss of appetite, SOB
Nutrition AssessmentFood/Nutrient Related History
•Decreased appetite one month PTA•Eating approx. 50% of meals PTA•MD expressed basic understanding of nutrition and wanted to maximize caloric intake prior to surgery.
•MD is a physician so he understood his disease state
• MD is on feet all day; in training for a marathon.
Nutrition Assessment
•Height=168 cm Weight=194 lbs (88.2 kg) BMI=31
•UBW=210 lbs;16 pound wt loss, 7% weight change in past month
Anthropometric Measurements
Nutrition AssessmentClient History•PMH: hypertension, dyslipidemia,
hypercholesteremia•No surgical history (hx) •Employed as a physician as Chief of Orthopedics
•Denies family psychiatric hx, alcohol, and drug use
Nutrition AssessmentNutrition Focused Physical Findings
•No edema present on admission•Vital signs stable on admission•Signs & Symptoms on admission: 3 weeks SOB, orthopnea, upper back discomfort, fatigued, lower energy levels during normal work activities, loss of appetite, weight loss
Nutrition AssessmentBiochemical
BNP levels normal upon admissionBUN slightly elevated: 26 mg/dL on 12/11
XX Labs were not nutritionally significant throughout his stay in the hospital
DiagnosisNI-1.2: Inadequate oral intake related to decreased desire to
consume sufficient energy 2/2 to CHF symptoms of shortness of
breath and fatigue as evidenced by patient report of poor po intake (50% of meals) over last month.
NC-3.2: Unintended weight loss related to decreased appetite 2/2 inadequate oral intake caused by
CHF symptoms as evidenced by 15 pound weight loss in past month
(7% weight change).

Intervention
Nutrition Prescription
Energy Needs: 1870-2066 kcal (Mifflin St. Jeor)Protein Needs: 65-78 grams (1-1.2 gram/kg)
Fluids: 1760-2200 mL
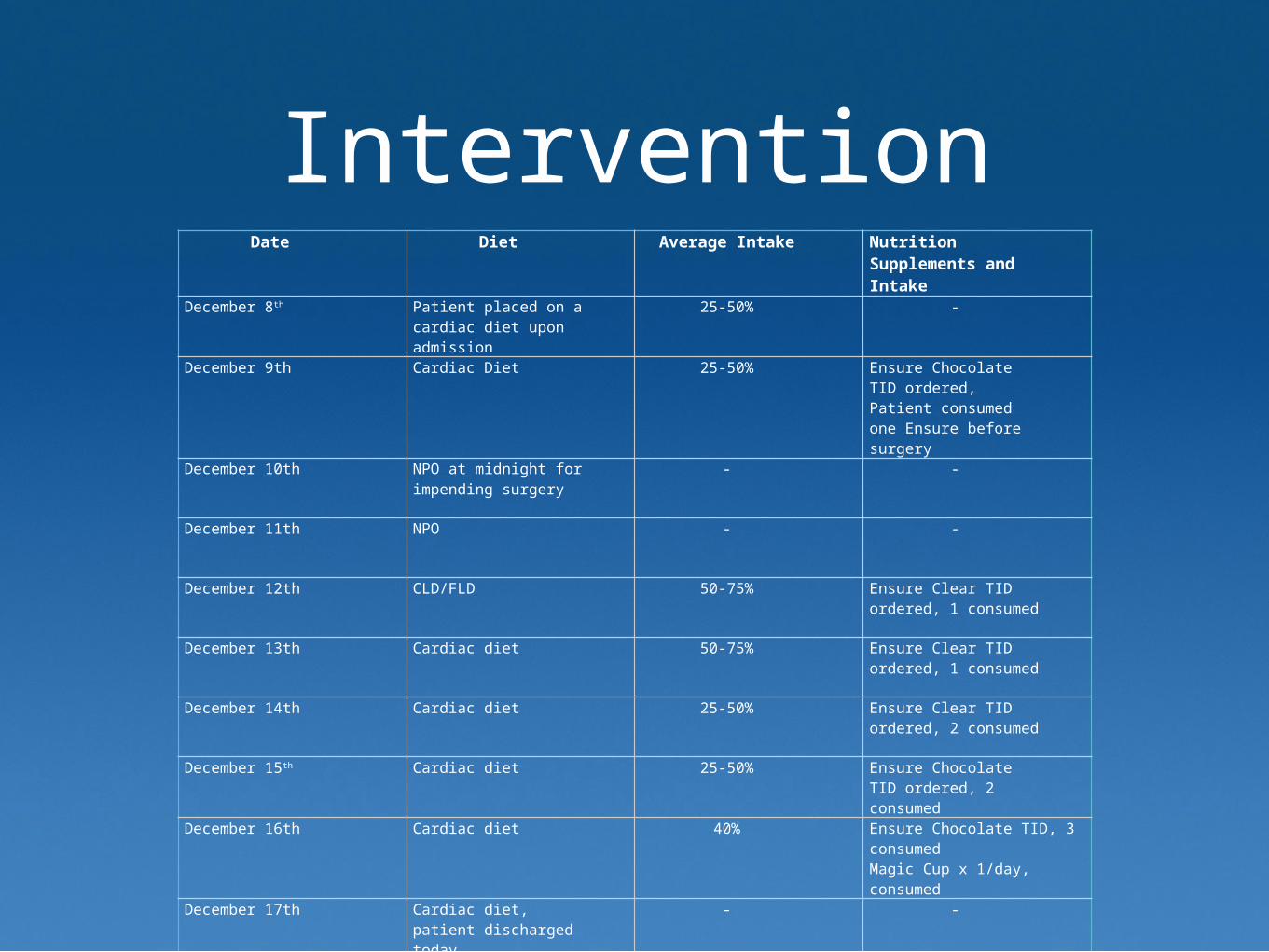
InterventionDate Diet Average Intake Nutrition
Supplements and Intake
December 8th Patient placed on a cardiac diet upon admission
25-50% -
December 9th Cardiac Diet 25-50% Ensure Chocolate TID ordered, Patient consumed one Ensure before surgery
December 10th NPO at midnight for impending surgery
- -
December 11th NPO - -
December 12th CLD/FLD 50-75% Ensure Clear TID ordered, 1 consumed
December 13th Cardiac diet 50-75% Ensure Clear TID ordered, 1 consumed
December 14th Cardiac diet 25-50% Ensure Clear TID ordered, 2 consumed
December 15th Cardiac diet 25-50% Ensure Chocolate TID ordered, 2 consumed
December 16th Cardiac diet 40% Ensure Chocolate TID, 3 consumedMagic Cup x 1/day, consumed
December 17th Cardiac diet, patient discharged today
- -
InterventionRC 1.3 Coordination with other providers: Recommend low sodium, cardiac Diet.
Goal: Implement once medically feasible after surgery.
ND-3.1 Medical food supplements: Initiate Ensure Chocolate TID once medically feasible.
RC 1.3 Coordination with other providers: Recommend Ensure Chocolate TID. Goal: Implement once advanced to Clear Liquid Diet after surgery.
RC 1.3 Collaboration with other providers: Patient will maintain current weight throughout hospital stay.
E-1.1 Purpose of Nutrition Education: Prior to discharge educate patient and patient family on importance of adhering to low sodium, cardiac diet after surgery
and discharge.
E-1.4 Nutrition relationship to health/disease: Prior to discharge help patient recognize and understand importance of adherence to low sodium cardiac diet in
relation to his CHF
Monitor/Evaluate
FH 1.1.1.1 Energy Intake
FH-1.2.1 Fluid/beverage intake
FH 1.6.2 Sodium Intake
FH 4.1.1 Food and Nutrition Knowledge/Skill
FH 4.1.2 Diagnosis specific food and nutrition knowledge

Nutrition Implications•Severity of MD’s CHF was reflected in the medical and nutritional therapy.
•Dietary Approaches to Stop Hypertension (DASH)
• Implemented to help client make better choices after surgery
•2000 mg sodium/day
•Many CHF patients will require a fluid-modified diet (ND-1.2.8)
•XX was not experiencing edema or hypernatremia
Nutrition Implications•Self-monitoring (C-2.3)
•Reading nutrition labels•Choosing salt-free additives

References Academy of Nutrition and Dietetics. International Dietetics and Nutrition Terminology (IDNT) Reference Manual. Chicago, IL: American Dietetic Association;
2013;
Academy of Nutrition and Dietetics. Nutrition Care Manual®. http://www.nutritioncaremanual.org. Accessed several times from December 2014-February 2015. ϖ https://www.nutritioncaremanual.org/topic.cfm?ncm_category_id=1&lv1=5803&lv2=8585&ncm_toc_id=8585&ncm_heading=Nutrition%20Care
Cotugna N, Wolpert S. Sodium Recommendations for Special Populations and the Resulting Implications . Journal of Community Health. 2011; 36: 874-882.
“Ejection Fraction picture” Emory Health http://www.emoryhealthsciblog.com
“Electrocardiogram” American Accreditation HealthCare commission-http://www.medicalwordmeanings.com/what-is-electrocardiogram-the-meaning-and-diagram/
Evidence Analysis Library. Academy of Nutrition and Dietetics Website. https://www.andeal.org. Accessed several times from December-February 2015. https://www.andeal.org/topic.cfm?menu=5289&cat=2815
“Healthy heart vs. Congested Heart” MD Health http://www.md-health.com/Congestive-Heart-Failure.html
“Heart” El Corazon. http://www.efn.uncor.edu/departamentos/divbioeco/anatocom/Biologia/Los%20Sistemas/Circulatorio/Corazon.htm
Lavid CJ, Ventura HO. Analyzing the Weight of Evidence on the Obesity Paradox and Heart Failure—Is there a Limit to the Madness? Congestive Heart Failure. 2013; 19:158-159.
Lennie TA, Moser DK, Biddle MJ, Walsh D. Nutrition Intervention to Decrease Symptoms in Patients with Advanced Heart Failure. Res Nurs Health. 2013; 36(2): 120-145.
Mahan LK. & S. Escott-Stump. 2012. 13th edition of Krause’s Food, Nutrition & Diet Therapy. W.B. Saunders Co.: New York. Medical Reference Guide-Complementary and Alternative Medicine Guide. University of Maryland Medical Center. January 2012.
http://umm.edu/health/medical/altmed/condition/heart-failure Accessed April 2015.
Riegel B, Moser DK, Anker SD, Appel LJ. State of Science. Promoting Self-Care in Persons with Heart Failure-A Scientific Statement From the American Heart Association.
“Systolic/Diastolic HF picture” http://pixshark.com/congestive-heart-failure-prevention.htm









