Embed Size (px)
Citation preview

Congenital ThoracicVascular Anomalies:Evaluation withState-of-the-Art MRImaging and MDCT
Jeffrey C. Hellinger, MDa,*, Melissa Daubert, MDb,Edward Y. Lee, MD, MPHc,d, Monica Epelman, MDeKEYWORDS
� Aortic arch anomalies � Pulmonary artery anomalies� Thoracic systemic venous anomalies� Pulmonary venous anomalies � CT angiography� MR imaging � MR angiography
Congenital thoracic vascular anomalies occurin the thoracic aorta and branch arteries, pulmo-nary arteries, thoracic systemic veins, and thepulmonary veins (Table 1). Technological innova-tions in magnetic resonance (MR) imaging andmultidetector-row computed tomography (MDCT)have greatly advanced the noninvasive diagnosisof these anomalies in pediatric patients in recentyears. From the neonate to the adolescent, high-resolution two-dimensional (2D) and three-dimen-sional (3D) MR imaging (MRI), noncontrast MRangiography (MRA), 3D contrast-enhanced MRA,and 3DMDCT angiography (CTA) datasets providecomprehensive multiprojectional, anatomic dis-plays for interactive interpretation, treatment plan-ning, and postoperative and postendovascularevaluation.
Effective use and interpretation of MRI-MRA(Fig. 1) and CTA (Fig. 2) for the evaluation of
a Advanced Cardiovascular Imaging, Advanced ImagingChildren’s Hospital, Stony Brook University School of Meb Stony Brook University School of Medicine, Stony Brooc Division of Thoracic Imaging, Department of RadioloSchool, Boston, MA, USAd Pulmonary Division, Department of Medicine, ChildrBoston, MA, USAe Neonatal Imaging, The Children’s Hospital of PhiladelPhiladelphia, PA, USA* Corresponding author.E-mail address: [email protected]
Radiol Clin N Am 49 (2011) 969–996doi:10.1016/j.rcl.2011.06.0130033-8389/11/$ – see front matter � 2011 Elsevier Inc. All
congenital thoracic vascular anomalies in pediatricpatients require fundamental understandings ofimaging techniques, anatomic embryology andcharacteristics, and underlying clinical pathophys-iology. Imagers should have knowledge of strate-gies to optimize protocols to deliver accurateand safe cardiovascular imaging based on thesuspected lesion(s) and the clinical stability ofthe patient. Equally important is the ability toadeptly use advanced postprocessing visualiza-tion techniques for image display, interpretation,and clinical management. This article assists thereader in these objectives. Imaging strategiesand MR imaging-MR angiography/CTA tech-niques are reviewed, followed by a discussion onthe commonly encountered thoracic congenitalvascular anomalies, with emphasis on embry-ology, clinical manifestations, and characteristicimaging findings.
and Informatics Laboratory, Stony Brook Long Islanddicine, Stony Brook, NY, USAk, NY, USAgy, Children’s Hospital Boston and Harvard Medical
en’s Hospital Boston and Harvard Medical School,
phia, University of Pennsylvania School of Medicine,
rights reserved. radiologic.th
eclinics.com

Table 1Congenital thoracic vascular anomaly
Arterial Venous
Thoracic Aorta Pulmonary Artery Systemic Veins Pulmonary Veins
Obstructive aortic arch lesions Pulmonary sling Persistent LSVC PAPVR
Tubular hypoplasia Hypoplasia With an RSVC TAPVR
Interruption of theaortic arch
Agenesis Mirror image drainage Type I
Aortic coarctation Stenosis Retroaortic left BCV Type II
Aortic arch anomalies Type III
Left aortic arch Mixed
Aberrant RSCA
Circumflex right DsAo
Double aortic arch
Right aortic arch
Aberrant LSCA/BCA
Mirror image branching
Circumflex left DsAo
Cervical aortic arch
Innominate arterycompression
Abbreviations: BCA, brachiocephalic artery; BCV, brachiocephalic vein; DsAo, descending aorta; LSVC, left superior venacava; PAPVR, partial anomalous pulmonary venous return; RSCA, right subclavian artery; RSVC, right superior vena cava;TAPVR, total anomalous pulmonary venous return.
Hellinger et al970
IMAGING STRATEGIES
Chest radiography, echocardiography, vascularultrasound, esophagography, MRI-MRA, CTA,catheter angiography, or a combination thereofmay be performed for diagnostic evaluation ofcongenital thoracic vascular anomalies. In thepast, catheter angiography was regarded as thestandard for angiographic evaluation of thesedisorders but, in the past decade, MR angiographyand CTA have gradually replaced catheter angiog-raphy for diagnostic purposes. Currently, catheter-based angiography is reserved for endovascularinterventions and obtaining direct hemodynamicmeasurements.In most pediatric patients presenting with a sus-
pected congenital thoracic vascular anomaly,a frontal (and preferably also a lateral) chest radio-graph is the initial imaging modality. The chestradiograph is a fast and inexpensive means to ob-tain initial direct or indirect evidence for a congenitalvascular lesion. Although the chest radiographmaynot always yield the specific diagnosis, it is usefulto exclude other potential causes, guide initialmanagement, and direct selection of subsequentimaging for confirmation and characterization.If cardiovascular symptoms predominate (eg,
congestive heart failure, systemic hypoperfusion,
cyanosis) transthoracic echocardiography (TTE)is usually obtained next. TTE, which requires noradiation, is readily performed and can assessmorphology and function (eg, flow dynamics,pressure gradients). However, TTE is limited bythe acoustic window (inversely related to patientage and size), acoustic impedance (air), operatorskill, and the ability to visualize peripheral vascularsegments (eg, pulmonary arteries, pulmonaryveins, and supra-aortic branch arteries).MR imaging-MR angiography or CTA are indi-
cated based on the TTE findings and performance.State-of-the-art MRI-MRA with parallel imagingshould be considered before CTA in pediatricpatients, because it does not require radiation oriodinated contrast medium and can evaluatevascular hemodynamics as well as vascularmorphology with high-resolution anatomic detail.MDCT angiography is indicated when MRimaging-MR angiography is not available, is con-traindicated, is nondiagnostic, or has a highpretest probability for being nondiagnostic. CTAshould be considered in the patient at high riskwith sedation or anesthesia and when airway,lung parenchyma, and other noncardiovascularstructures require more detailed imaging.If respiratory symptomspredominate (eg, stridor,
exercise intolerance, apnea, cyanosis, recurrent

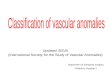
Fig. 1. Innominate artery compression on the trachea. A young child with a history of stridor underwent MRimaging-MR angiography for assessment of a possible vascular ring. (A) Sagittal 3D volume rendered image ofthe MR angiography shows a left aortic arch with normal 3 vessel branches and slightly horizontal course (arrow)of the innominate artery (IA). (B) Oblique MPR projection from a single-shot fast spin echo dark blood acquisitionshows the relationship of the IA (long arrow) to the trachea (short arrows). (C–F) Transverse dark blood imagesshow slightly more than 50% extrinsic compression on the trachea (arrow) by the IA (arrowhead), as the IAcourses from left to right. LSCA, left subclavian artery; MPR, multiplanar reconstruction; RSCA, right subclavianartery.
Congenital Thoracic Vascular Anomalies 971
upper and lower respiratory infections), MRimaging-MR angiography or CTA is performedfollowing chest radiography per the guidelines dis-cussed earlier. Echocardiography is indicated aftera positive MR imaging-MR angiography or CTAto further evaluate cardiac morphology, assess
function, and exclude other congenital cardio-vascular lesions. In this clinical setting, CTA is ad-vantageous to assess for tracheobronchomalacia,tracheal rings, and extrinsic tracheal compression.Paired inspiration-expiration MDCT angiographictechniques with controlled ventilation have proved

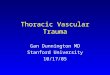
Fig. 2. Tubular hypoplasia of the aortic arch. A neonate with congenital aortic stenosis underwent MDCT angi-ography to further define aortic arch anatomy. (A–C) 3D volume rendered images show moderate to severetubular hypoplasia of the aortic arch (A, arrow) with a small patent ductus arteriosus (B, C; arrow).
Hellinger et al972
to be a reliable means to diagnose clinically signif-icant tracheomalacia and innominate arterycompression on the trachea in pediatric patients.1
If gastrointestinal symptoms predominate (eg,feeding intolerance, failure to thrive, dysphagia,aspiration), an esophagram may be obtainedfollowing chest radiography. MRI-MRA or CTA isperformed if the esophagram is positive, basedon the guidelines discussed earlier. If symptomspersist following a negative esophagram and thereremains a high index of suspicion for a thoracicvascular anomaly, consideration should be givento either MR imaging-MR angiography or CTA.Following a positive MRI-MRA or CTA, if not previ-ously obtained, TTEmay be indicated to assess forcongenital heart structural abnormalities.
IMAGING TECHNIQUESMR Imaging and MDCT Protocols
MR imaging and MDCT angiographic protocolsare designed to accurately evaluate cardiac andvascular morphology, and to provide detailedassessments of the central airway and its relation-ship to cardiac chambers and vascular structures.To minimize the examination duration, only essen-tial scan acquisitions should be used, becausepatients may become hemodynamically unstableor may develop respiratory distress. Beforeimaging, it is recommended to review the patient’sclinical presentation, prior medical history, priorimaging studies, current management, and otherrelevant clinical data. Such information helps inthe selection of the most appropriate imagingmodality and optimal acquisition and contrastinjection protocols. Clinical review also helps todetermine the most appropriate location and size
for an intravenous catheter (eg, CEMRA, CTA)and whether sedation or anesthesia is required.
MR imaging-MR angiographyA standard MRI-MRA protocol for evaluation ofpediatric thoracic vascular anomalies includeselectrocardiogram-gated black-blood and bright-blood sequences in conjunction with an angio-graphic sequence. Black-blood and bright-bloodMR imaging sequences provide comprehensiveanatomic detail, in particular vessel course,caliber, and arterial branching or venous drainagepattern. Black-blood imaging is also applied toevaluate the central airway. Techniques forblack-blood MR imaging typically include eithersingle-shot fast spin echo with double inversionrecovery or half-Fourier, single-shot fast spinecho with double inversion recovery. Bright-blood imaging in most current practices isachieved with 2D or 3D balanced steady-statefree precession. Phase contrast (PC) MR imagingis an optional sequence that is used to evaluateflow direction and velocity, and assess vascularphysiology.Angiographic techniques include time of flight
(TOF) MR angiography, PC-MR angiography, andmultiphase (arterial and venous) 3D T1-weightedCEMRA. CEMRA is most frequently performed,whereas TOF-MR angiography and PC-MR angi-ography are reserved for when gadolinium is con-traindicated. To maximize 3D displays, CEMRAslice thickness should not be greater than 1.5mm. When parallel imaging techniques are appliedwith CEMRA, isotropic, submillimeter datasetscan be obtained, yielding the highest possiblespatial resolution and robust 3D structural displayson par with those from an MDCT angiogram.

Congenital Thoracic Vascular Anomalies 973
Acquisitions may be in the coronal or sagittalplane, depending on the required anatomiccoverage and breath-hold duration.
MDCT angiographyBecause of its inherent dependence on radiationfor generating images, low-dose helical and volu-metric pediatric MDCT angiography protocolsstrive for only 1 core series, namely a single-phase angiographic scan. This single scan isacquired with a slice thickness of 0.5 to 1.5 mmand is synchronized with the arrival of contrast togenerate arterial, venous, or equilibrium phase da-tasets. A noncontrast acquisition is a considerationin the postsurgical or endovascular patient toassess the presence, location, and integrity ofhigh-density material that may degrade vascularinterpretation or may be obscured by the contrast(eg, metallic stents, surgical clips, embolizationcoils). Additional vascular phases should only beconsidered if image quality is suboptimal. Ultralowradiation dose volumetric, time-resolved, dynamicCTA with intermittent 2-second to 3-second dataacquisitions in 10 to 15 seconds is a promisingnew technique that can be performed on a 320-channel MDCT scanner; similar to CEMRA, iso-lated arterial and venous phases can be acquired,providing temporal flow information and moredirect imaging of vascular physiology withMDCT. With all pediatric CTA protocols, radiationdose reduction strategies should be used toachieve the lowest possible radiation exposurethat will render an interpretable examination forthe reader. These radiation dose reduction strate-gies include using the lowest possible voltage(eg, 80 kVp), the lowest possible amperage (eg,weight-based milliampere seconds), the minimumamount of coverage (with shielding of nontargetregions), and the shortest possible scan time(eg, fastest scan rotation, high-pitch helical,
Table 2Interpretive review: congenital thoracic arterial anom
Aorta Aortic Arch
AsAo DsAo Transversesegment
Isthmus Brancharterie
Location Location Location Caliber Number
Course Course Number Contour Order
Caliber Caliber Sidedness Coarctation CourseCaliber Preductal Caliber
JuxtaductalPostductal
Abbreviations: AsAo, ascending aorta; DsAo, descending aort
wide-collimation helical, and volumetric MDCTtechniques).2
Interpretation and Advanced Visualization
MR imaging-MR angiography and CTA interpreta-tion address vascular morphology and physiology,as detailed in Tables 2 and 3. Evaluation for asso-ciated cardiovascular and noncardiovascularabnormalities is imperative. Postoperative and en-dovascular evaluations should assess luminalpatency and exclude aneurysms, pseudoaneur-ysms, and iatrogenic injury. For patients whohave undergone stent placement, stent migration,fatigue, and disruption should be excluded.
Display and interpretation of thoracic MRA andCTA datasets are most effective when applyingadvanced workstation visualization techniques(Table 4). Techniques are selected in a comple-mentary manner according to their strengths,using adjustable angiographic window and levelsettings, including a wide window setting toaccount for noise and high vascular contrast.Datasets are interrogated in real time with user-defined interaction of the techniques and relatedworkstation tool functions. Alternatively, protocol-driven static postprocessed single and batch-serial images are generated for review along withthe source images. The spatial detail of angio-graphic anatomy is best displayed using 3Dvolume rendering (VR) and 2D maximum intensityprojection (MIP). Both require sliding thin slabs orprerendering editing to remove bone and otheranatomic structures that may obscure vascularvisualization. However, structural detail is as-sessed with the highest accuracy using 2D multi-planar reformations (MPR) and curved planarreformations (CPR). Although minimum intensityprojection (MinIP) and ray sum (thick MPR) havelimited applications in MR and CT angiographyMinIP is useful with CTA datasets to show cardiac
alies
Ductus Pulmonary Arteries Vascular
sArteriosus Central Peripheral Physiology
Patent Presence Course Gradient
Closed Location Caliber Collaterals
Diverticulum CourseDimple Caliber
a.

Table 3Interpretive review: congenital thoracic venous anomalies
SVC IVCInnominateVein
CoronarySinus
PulmonaryVeins
CardiacChambers
PulmonaryArteries Airways Lungs
Sidedness Sidedness Sidedness Presence Number Connections Caliber Lobar Anatomy Lobar Anatomy
Right Right Right Caliber Course Size Central Hypoplasia Hypoplasia
Left Left Left Caliber Atria Peripheral Partial agenesis Partial agenesis
Course Course Course Insertion Ventricles Patency Mosaicattenuation
Caliber Caliber Flow direction Patency Septae
Insertion Insertion DefectsFlattening
Abbreviations: IVC, inferior vena cava; SVC, superior vena cava.
Hellin
geretal
974

Table 4Cardiovascular advanced visualization techniques
Display Principal Use Advantages Disadvantages
MPR 2D Structural detailQuantitative analysis
Slice through dataset incoronal, sagittal, andoblique projections
Real-time multiplanarinterrogation
Simplify imageinterpretation
Limited spatial perception
CPR 2D Structural detailCenterline displaySimplify MPR
Single anatomic displayLongitudinal cross-sectionalanatomic display
Operator dependent
Ray sum 2D Structural overview Slice through dataset inaxial, coronal, sagittal, andoblique projections
Real-time multiplanarinterrogation
Radiograph-like display
Loss of structural detail withincreased slab thickness
MIP 2D Structural overviewAngiographic display
Slice through dataset inaxial, coronal, sagittal, andoblique projections
Real-time multiplanarinterrogation
Improved depictionSmall-caliber vesselsPoorly enhanced vessels
Communicate findings
Anatomic overlap (vessels,bone, viscera) withincreased slab thickness
Visualization degraded byhigh-density structures (ie,bone, calcium, stents, coils)
Loss of structural detail withincreased slab thickness
Limited grading of stentlumens
MinIP 2D Structural overviewAirwayAir trapping in lungSoft tissue air
Slice through dataset inaxial, coronal, sagittal, andoblique projections
Real-time multiplanarinterrogation
Depict low-density structuresCommunicate findings
Anatomic overlapLoss of structural detail withincreased slab thickness
VR 3D Structural overviewAngiographic display
Slice through dataset inaxial, coronal, sagittal, andoblique projections
Real-time multiplanarinterrogation
Depict structuralrelationships
Accurate spatial perceptionCommunicate findings
Dependent upon opacity-transfer function
Anatomic overlapLoss of structural detail withincreased slab thickness
Abbreviations: CPR, curved planar reformation; MinIP, minimum intensity projection; MIP, maximum intensity projection;MPR, multiplanar reformation; VR, volume rendered.
From Hellinger JC, Pena A, Poon M, et al. Pediatric computed tomographic angiography: imaging the cardiovascularsystem gently. Radiol Clin North Am 2010;48:457; with permission.
Congenital Thoracic Vascular Anomalies 975
valves (eg, bicuspid aortic valve), airways, air trap-ping, and abnormal nonpulmonary air collections.Ray sum may be applied with MR angiographyand CTA datasets to generate radiograph-likeimages for structural overview.
SPECTRUM OF THORACIC CONGENITALVASCULAR ANOMALIESArterial Systems
The primitive circulatory system is initially func-tional by the end of the third week of fetal

Hellinger et al976
development; blood passes from the primitiveheart to paired dorsal aorta. Subsequent develop-ment of the thoracic aorta, aortic arch brancharteries, pulmonary arteries, and ductus arteriosusoccurs during the fourth to eighth weeks of life,beginning with the growth of 6 paired pharyngealaortic arches (PAA), which bridge the aortic sacto the dorsal aortae through the pharyngealpouches. Normal development leads to a left-sided aortic arch (LAA) and descending aorta;aortic arch branching (in order) consists of the bra-chiocephalic artery, the left common carotid artery(LCCA), and the left subclavian artery (LSCA) (seeFig. 1). The ductus arteriosus is left sided, extend-ing from the proximal left pulmonary artery (LPA) tothe aortic isthmus, the segment that is betweenthe LSCA and the proximal descending aorta. Toachieve this morphology, the aortic arches alongwith the dorsal aortae and the seventh interseg-mental arteries, undergo selective involution anddifferential growth of persisting structures, asdetailed in Table 5.3
THORACIC AORTAObstructive Aortic Arch Lesions
Tubular hypoplasiaTubular hypoplasia of the aortic arch (THAA) isa congenital anomaly in which the transverse aortais reduced in caliber in a short segment such thatantegrade flow is reduced. Borders of the aorta inTHAA are smooth, without focal narrowing (seeFig. 2). Obstructive physiology may be present in
Table 5Embryologic origins and development of the left ao
Structure Outcome
Pharyngeal aortic arches First Near compleSecond Near compleThird Bilateral perFourth Left: domina
Right: partiaFifth Never formsSixth Left: domina
Right: partia
Seventh segmental artery Bilateral per
Dorsal aortae Left: dominaRight: involu
Abbreviations: BCA, brachiocephalic artery; CCA, common ccarotid artery; PA, pulmonary artery.
affected patients depending on the length of hypo-plasia and the pressure gradient (Fig. 3). It canoccur in isolation or be associated with otherleft-sided obstructive lesions (LSOLs), includingcongenital mitral stenosis (MS), mitral atresia(MA), hypoplastic left heart syndrome (HLHS),aortic stenosis (AS), aortic atresia (AA), interruptedaortic arch (IAA), and coarctation of the aorta(COA).The hemodynamic theory can explain the path-
ogenesis of aortic arch hypoplasia and its associ-ation with concomitant congenital heart defect(CHD) lesions. Normal development and size ofthe aortic arch is dependent on flow dynamics.In normal fetal circulation, half of the combinedventricular blood volume flows from the right ven-tricle to the main pulmonary artery, whereas theother half flows from the left ventricle to the as-cending aorta. Most the pulmonary blood volumeflows across the ductus arteriosus to the des-cending aorta. Themajority of the ascending aorticblood volume flows to the coronary circulation andthe supra-aortic arteries, resulting in approxi-mately 15% of blood volume flowing across theisthmus and a fetal isthmus that measures up to70% to 75% the size of the ascending aortacaliber.4–6 Any event or lesion that results indecreased antegrade blood flow will lead to lessvascular stimulation for growth of the fourth aorticarches and smaller than expected size of the aorticarch and isthmus.MR imaging-MR angiography and CTA findings
of THAA include diffuse smooth narrowing of the
rtic arch
Vascular Derivatives
te involution Ipsilateral ECAte involution Ipsilateral ECAsistence Ipsilateral CCA and ICAnt persistence Left: midaortic archl persistence Right: BCA, RSCAor involutes Nonent persistence Leftl persistence Ventral: ipsilateral central PA
Dorsal: ductus arteriosusRightVentral: Ipsilateral central PADorsal: ductal involution
sistence Left: LSCARight: LSCA
nt persistence Left: distal aortic archtes Right: none
arotid artery; ECA, external carotid artery; ICA, internal

Fig. 3. Tubular hypoplasia of the aortic arch with endovascular stent placement. An adolescent with asymmetricupper extremity hypertension underwent MDCT angiography. (A–C) Initial diagnostic 3D volume renderedimages showmild tubular hypoplasia of a mildly elongated transverse aortic arch (A, B; long arrow) with compen-satory LSCA enlargement (B, C short arrows) for collateral flow. Catheter angiography confirmed a significantpressure gradient that subsequently led to endovascular stent placement. (D–F) 3D volume rendered CTA imagesafter stent placement show overlapping uncovered stent placement (long arrow) extending from the LCCA to justpast the LSCA. Note the persistent residual LSCA enlargement (short arrow). LCCA, left common carotid artery.
Congenital Thoracic Vascular Anomalies 977
transverse aorta. Narrowing may involve the entireaortic arch or only a portion (typically midaorticarch to distal aortic arch). Search should bemade for associated left-sided obstructivelesions. If MR imaging-MR angiography is per-formed, phase contrast imaging is essential to
document the presence of a gradient. Treatmentis only indicated when there is a hemodynamicallysignificant gradient (eg, >15–20 mm Hg). If diag-nosis is made by CTA, echocardiography cansubsequently be performed to determine thegradient.

Hellinger et al978
Interruption of the aortic archInterruption of the aortic arch is a rare, hemody-namically critical left-sided obstructive conotrun-cal anomaly in which there is discontinuity of theaortic arch, resulting in systemic perfusion that isdependent on the ductal and/or aortic branchartery. IAA accounts for 0.4% to 1.3% of CHDlesions7,8 and 7% of CHD lesions presenting withsignificant physiologic compromise.9 Arch inter-ruption may occur at 1 of 3 levels with variablefrequency: (1) type A, distal to the LSCA origin(26%); (2) type B, between the origins of theLCCA and LSCA (72%); and (3) type C, proximalto the LCCA, between the origins of the innominateand left common carotid arteries (2%).7,10–16
Associated CHD lesions include patent ductusarteriosus (PDA), ventricular septal defect (VSD;isolated and multiple), atrial septal defect (ASD),left ventricular outflow tract obstruction (LVOTO,such as hypoplasia and subaortic, valvular, andsupravalvular aortic stenosis), aortopulmonarywindow, truncus arteriosus, transposition of thegreat arteries (TGA), double outlet right ventricle,and aortic arch anomalies.7,10–17 Evidence indi-cates that type A IAA occurs secondary todecreased antegrade hemodynamics from anunderlying CHD lesion (eg, LVOTO lesions, left toright shunts), with presumed left fourth aorticarch involution.17,18 By distinction, type B IAAresults from genetically altered neural crest em-bryogenesis. In patients affected with type B IAA,approximately 50% to 82%18–23 have a 22q11.2deletion (most commonly Tbx1 haploinsufficiency)in which abnormal neural crest development andmigration lead to an impaired epithelial remodelingof the fourth pharyngeal arch and derivatives ofthe third and fourth pharyngeal pouches. Thiscondition accounts for the variably associatedconcomitant cardiovascular (eg, other conotruncalCHD lesions) and noncardiovascular phenotypeexpression (eg, DiGeorge syndrome, Velo-Cardio-Facial syndrome, conotruncal anomaly facesyndrome).24,25 IAA is also associated withCHARGE syndrome, in which CHD7 gene muta-tion (8q12.1 chromosome) contributes to abnor-mal neural crest and fourth PAA epithelialmorphogenesis.24,25
Affected patients usually present clinically withinthe first few days of life and typically not more than2 weeks of age. As with other critical LSOLs, theneonate with IAA may appear normal at birthand with no clinical cyanosis. However, as theductus closes, systemic blood flow decreasesand pulmonary venous pressure rises; congestiveheart failure, respiratory distress, systemic hypo-perfusion, pallor, and decreased organ functionmay ensue. Prompt hemodynamic stabilization,
diagnosis, and surgical revision are mandatoryfor survival. Radiographically, IAA (and otherLSOLs) shows pulmonary venous congestion,with the heart size ranging from normal to mark-edly increased. If a septal defect is present withleft to right shunting, there may be a componentof increased pulmonary vascularity. A narrowmediastinum in these patients indicates thymicaplasia (eg, DiGeorge syndrome). Echocardiog-raphy can usually define IAA with reliable accu-racy. MR imaging-MR angiography or CTA maybe indicated to further define the level of interrup-tion, aortic branch arteries, and/or associatedanomalies, which is key information for preopera-tive planning.
Coarctation of the aortaCoarctation of the thoracic aorta is defined asa focal, eccentric, obstructive narrowing involvingthe aortic isthmus (Fig. 4). It accounts for 1.8%to 9.8% of CHD, with most studies showing anincidence of 5% to 6%.8,26–29 COA has a slightmale predominance (1.2–2.3:1).30–37 Most casesoccur sporadically, but both environmental factorsand genetic causes may contribute. COA is char-acterized as preductal, juxtaductal, or postductal,based on its anatomic relationship to the ductusarteriosus. Preductal COA predominates in chil-dren less than 1 year of age, whereas the postduc-tal type is more common in children greater than 1year and in adults.The narrowing in COA results from abnormal fi-
bromuscular ductal tissue encircling the aorta.The ductal theory hypothesizes that, as the LSCAmigrates cephalad through differential growth ofthe dorsal aorta, the ductal ostium from the sixtharch is pulled into the aorta, forming the circumfer-ential sling. Obstruction at the isthmus developswhen there is postnatal constriction of the ductusarteriosus. The hemodynamic theory facilitatesa greater understanding of the pathogenesis andlends an explanation to the occurrence of COAwith associated cardiovascular lesions. Congen-ital lesions with decreased antegrade flow in theascending aorta (eg, LSOLs, left to right shunts),result in reversal of blood flow across the fetalisthmus, altering the branch point angulation,and accentuating LSCA cephalad migration,increasing the possibility for developing COA. Incontrast, right-sided obstructive cardiac lesions(eg, right ventricular outflow tract obstruction,pulmonary stenosis, and pulmonary atresia) pro-tect against coarctation, because there is domi-nant antegrade isthmus flow.4–6,38–40
The primary physiologic sequelae of coarctationis increased left ventricular afterload and de-creased systemic perfusion with activation of the

Fig. 4. COA. A young child with upper extremity hypertension underwent CTA examination following echocar-diographic diagnosis of COA. (A, B) 3D volume rendered images show severe narrowing involving the isthmicportion of the aorta (arrow). (C, D) 3D volume rendered images show well-developed collateral pathways,including internal mammary (C, long arrows), thoracodorsal (C, short arrows), superficial paraspinal (D, longarrows), and parascapular (D, short arrows) pathways. (E, F) 3D volume rendered images show intercostal (arrow-head) and mediastinal paraspinal (arrows) collateral arteries.
Congenital Thoracic Vascular Anomalies 979
sympathetic and renin-angiotensin systems, re-sulting in increased blood pressure. In neonatesand infants with COA (similar to IAA), systemicperfusion is dependent on maintaining patency of
the ductus arteriosus. Prostaglandins are initiatedearly in the clinical course to maintain this patency.Once the ductus closes, the inability to rapidlydevelop collateral blood flow and counter the

Hellinger et al980
rising afterload may lead to left heart dysfunctionwith chamber enlargement and congestive heartfailure. Pulmonary hypertension (with right heartdysfunction), renal insufficiency, and systemicshock may also develop. With isolated COA,when sufficient compensatory collateral flowdevelops to supply blood distal to the obstruction,clinical presentation is delayed until later in life.Primary collateral pathways include the sub-clavian, internal mammary, intercostal, cervical,scapular, and thoracodorsal arteries (see Fig. 4).The presence of collateral arteries and a pressuregradient are the distinguishing features betweencoarctation and pseudocoarctation (Fig. 5). Incases of pseudocoarctation, there is absence ofa pressure gradient and collateral arteries.Associated congenital cardiovascular abnor-
malities may occur in 44% to 84% of patientswith COA; most of these patients present by 2
Fig. 5. Pseudocoarctation. A neonate underwent contrastlying complex congenital heart disease. (A, B) 3D volumethe aortic arch, with uplifting of the aortic arch and kiarteries.
years of age.30,32,41 Commonly associated abnor-malities include PDA, bicuspid aortic valve, left toright shunts (eg, ASD, VSD), LSOLs, and TGA.Syndromes and genetic disorders associatedwith COA include Shone complex, PHACEsyndrome, Williams syndrome, Noonan syndrome,Turner syndrome (45 XO karyotype), trisomy 13,and trisomy 18.Early diagnosis and intervention are essential to
minimizing morbidity and mortality in pediatricpatients with COA. Untreated COA in neonatesand infants has a poor prognosis (50% mortality)without urgent surgical intervention.42 Milder formsof COA may take years or decades to becomesymptomatic. However, the long-term effects ofsystemic hypertension from aortic coarctationmay lead to late cardiovascular complications,reducing life expectancy compared with thegeneral population. Chronically increased blood
-enhanced MR angiography for evaluation of under-rendered images show pseudocoarctation (arrow) of
nking at the isthmus. Note the absence of collateral

Congenital Thoracic Vascular Anomalies 981
pressure results in left ventricular hypertrophy withcongestive heart failure in early to midadulthood.The increased blood pressure can lead to anincreased incidence of premature coronary arterydisease, ischemic heart disease, cerebral vascularaccidents (eg, ischemia, hemorrhage), aorticvalvular disease (eg, stenosis or insufficiencyrelated to a bicuspid aortic valve), aortic root dila-tation, aortic aneurysms (eg, proximal to a coarcta-tion), acute aortic disease (eg, dissection, rupture),and bacterial endocarditis.
Definitive management of COA requiressurgical (eg, resection with interposition graft) orendovascular (eg, angioplasty with stent place-ment) repair. Age at the time of coarctation repairhas a predictive value for operative mortality (2%–41%, highest in infants <1 year old),30,32,41–46
recoarctation (4%–26%, highest in infants <1year old),30,32,41,44–47 and residual hypertension(12.5%–21%, lowest when operated between 1and 5 years old).32,33,44,47 To optimize surgicaloutcome and minimize potential future cardiovas-cular risk, elective repair is recommended in earlychildhood (1–5 years of age) and should not bedelayed past 10 years of age. Hypertension atthe first postoperative evaluation and the devel-opment of postoperative paradoxic hypertensionare risk factors for chronic hypertension (residualor recurrent) and acquired cardiovascular dis-ease. Patients should be followed closely afterrepair for possible recurrent coarctation, progres-sion of associated cardiac defects, and develop-ment of acquired cardiovascular disease.33,48,49
Chest radiography has a low to moderate sensi-tivity for detection of COA, dependent on the ageof the patient, the degree of narrowing, and thepresence of associated cardiac defects. In theneonate and infant, the heart is typically enlargedand pulmonary venous congestion is present. Inthe older child to young adult with isolated COA,typical imaging findings include a prominent aorticarch and proximal descending aorta silhouettewith a figure-of-3 contour, inferior rib scallopingand/or sclerosis, and a normal or mildly enlargedheart size. Confirmatory diagnosis of COA inneonates and infants is most often made withTTE, which has a sensitivity of 94% to 98%50,51
and a positive predictive value as high as 98%and 100% for neonates and infant, respectively.51
In older children to young adults, CEMRA (sensi-tivity 98%, specificity 99%) is superior to TTE fordepicting COA and the complete thoracic arterialsystem.52 PC-MR imaging is applied to measurethe gradient across the obstructive narrowingand quantify collateral flow. MDCT angiographyis a highly sensitive imagingmodality with an accu-racy as high as 100%.53 As with MRA, collateral
pathways should be described in detail becausetheir number and extent directly correlate withthe severity of disease.
Aortic Arch Anomalies
Aortic arch anomalies (AAA) are congenitalvascular abnormalities involving development ofthe primitive aortic arches and their derivatives,accounting for 0.5% to 1.6% of CHD lesions.28,54
Men have a slightly greater prevalence thanwomen(1.2:1).55–63 Four percent of patients with theseanomalies may have 22q11.2 deletion, whereas35% of those with 22q11.2 deletion may have anisolated aortic arch anomaly.63,64 Common AAAin pediatric patients include vascular rings, pulmo-nary artery slings (PAS), and innominate arterycompression (IAC). The most common symptom-atic AAA are a double aortic arch (49%, range36%–72%) and right aortic archwith a left ligamen-tum/ductus arteriosum (28%, range 8%–49%), fol-lowed by IAC (10%, range 3.3%–27%), left aorticarch with an aberrant right subclavian artery (8%,range 1.7%–20%), and pulmonary sling (5%, range1.8%–12.5%).55–61,63,65,66 AssociatedCHD lesionsoccur in 18% (range 12%–32%) of patients withAAA,55,57,59–62,65 including VSD, ASD, PDA, right-sided obstructive lesions, and COA.
The unifying characteristic of these disorders issecondary vascular compression on the centralairway, the esophagus, or both. Depending onthe type of lesion, severity of compression, andthe presence of comorbid cardiovascular andnoncardiovascular congenital disease, affectedpatients present with variable degrees of respira-tory and gastrointestinal symptoms during theneonatal period, infancy, childhood, or youngadulthood. Respiratory symptoms are more prev-alent among infants and young children, whereasesophageal symptoms are more common amongolder children, adolescents, and adults. In additionto extrinsic compression of the central airway,concomitant intrinsic tracheomalacia may occurin up to 53% of pediatric patients with AAA,affecting the presentation and clinical manage-ment of respiratory symptoms.1
Vascular ringsA vascular ring occurs when the trachea and/oresophagus are surrounded and compressed byvessels (eg, aortic arch or arches, aortic archbranch arteries, pulmonary branch arteries) andthe ductus or ligamentum arteriosum. A vascularring may be complete or incomplete. Vascularrings result from abnormal persistence and involu-tion of primitive brachial arch segments, mostcommonly the third, fourth, and sixth arches.They may occur with a normal left-sided arch,

Hellinger et al982
a double aortic arch (DAA), a right-sided aorticarch (RAA), and a cervical aortic arch (CAA). Clas-sification of vascular rings is based on Edwards’67
hypothetical embryologic double aortic archmodel.
Left aortic arch The normal LAA, left-sided de-scending aorta, and left-sided ligamentum arterio-sum are formed by regression of the right andpersistence of the left fourth arches, eighth dorsalaorta segments, and sixth dorsal arches, respec-tively. Two main anomalous patterns may occur.The first is an aberrant right subclavian artery(Fig. 6), which results when right fourth archregression occurs between the right commoncarotid and right subclavian arteries, rather thandistal to the right subclavian artery. The aorta givesrise to the right common carotid, the left commoncarotid, the left subclavian, and the right subcla-vian arteries. The right subclavian artery coursesretroesophageal. Two subdivisions are possible,namely a left-sided or right-sided ligamentum arte-riosum. If there is a left-sided ligament, no vascularring occurs; the aberrant right subclavian arteryhas smooth caliber throughout its course.However, a rare right-sided ligament completesa true vascular ring; it forms by persistence ofthe right dorsal sixth arch and passes from theright pulmonary artery (RPA) to the descendingaorta, via the proximal right subclavian artery,potentially leading to fusiform dilatation of the ret-roesophageal aberrant segment (eg, diverticulumof Kommerell). Beyond the diverticulum, thesubclavian artery is normal in caliber.The second anomalous pattern with a LAA is
a circumflex right descending aorta. With thisentity, distal aortic arch and proximal descending
Fig. 6. Left aortic arch with an aberrant right subclavianpulmonary embolism. (A, B) 3D volume rendered images shartery (RSCA; arrow). The RSCA arises from the aorta as thcarotid artery (RCCA), LCCA, and LSCA.
aorta course posterior to the esophagus andtrachea. It may occur with normal arch branchingor an aberrant right subclavian artery.The vascular ring is completed by the ligament
passing between the RPA and the descendingaorta after the retroesophageal segment.
Double aortic arch A double aortic arch (Fig. 7)results from persistence of both the right and leftfourth arches and the dorsal aorta, forminga complete vascular ring. Right dominance occursin 66% (range 37%–81%), left dominance in 16%(range 10%–20%), and codominance in 17%(range 3%–53%).55,60–63,66 The left archmay be at-retic with a fibrous segment distal to the take-off of1 or both of the left arch branch arteries. Rarely, theright arch may be atretic. The right arch typicallysupplies the right common carotid and brachioce-phalic arteries, whereas the left supplies the leftcommon carotid and brachiocephalic arteries.The descending aorta is often on the left but theproximal descending aorta can be on the right ormidline. The ligament is usually left sided. Lesscommonly, it can be right sided or bilateral. Pulmo-nary arteries are typically normal.
Right aortic arch A right aortic arch occurs frompersistence of the right, and regression of theleft, fourth arches and eighth dorsal aortasegments, respectively. A vascular ring may occurdepending on the level of the left fourth archresorption, the origins and course of the ligamen-tum arteriosum and the descending aorta, ora combination thereof. Three possible patterns ofa RAA may occur. The first is an aberrant LSCA/brachiocephalic artery. In this case, left fourtharch regression occurs between the left carotid
artery. A young child underwent CTA for suspectedow a left aortic arch with an aberrant right subclaviane fourth aortic branch artery, after the right common

Fig. 7. Double aortic arch. A neonate with respiratory distress underwent CTA for evaluation of a vascular ring.(A, B) 3D volume rendered (A) and MIP (B) images show the typical vascular morphology of a double aortic arch(arrows) with a left descending aorta. In this instance, the right (long arrow) and left (short arrow) arches haverelative codominance, forming a complete ring. (From Hellinger JC, Pena A, Poon M, et al. Pediatric computedtomographic angiography: imaging the cardiovascular system gently. Radiol Clin North Am 2010;48:462; withpermission.)
Congenital Thoracic Vascular Anomalies 983
and subclavian arteries. The aorta gives rise to theleft common carotid, the right common carotid,the right subclavian, and the left subclavianarteries; the LSCA courses retroesophageal(Fig. 8). Regression before the LCCA results inan anomalous left brachiocephalic artery. The rightcarotid artery becomes the first branch followedby the right subclavian artery and the left brachio-cephalic artery. The left brachiocephalic arterycourses retroesophageal with subsequent branch-ing into the left common carotid and subclavianarteries. In both types, when the ligament is rightsided, no vascular ring is present. The left subcla-vian or brachiocephalic artery has a regular caliberthroughout its course. When the ligament is leftsided, a complete vascular ring is present; the liga-ment courses between the LPA and the proximaldescending aorta, via the aberrant LSCA or bra-chiocephalic artery (Fig. 9). The retroesophagealsegment of the left subclavian or brachiocephalicartery is dilated with a diverticulum of Kommerellin 15% to 21% of cases.60,62
The second pattern with a RAA is mirror imagebranching. In this condition, left fourth arch regres-sion occurs distal to the LSCA and the aorta givesrise to the left brachiocephalic, the right commoncarotid, and the right subclavian arteries. In mostinstances, no vascular ring is present becausethe descending aorta and ductus/ligamentum ar-teriosum are ipsilateral. The right ligament passesbetween the right descending aorta and the RPA.
Less commonly, the ductus is contralateral. Inthis instance, the ligamentum usually passesbetween the brachiocephalic artery and the LPAwithout formation of a vascular ring. Rarely,however, the ligamentum arises from the proximaldescending aorta and takes a retroesophagealcourse to the LPA, creating a vascular ring.Although the ligament may not be visualized,a small leftward-facing dimple may be present onthe proximal descending aorta, at the take-off ofthe ligament, indicating the anomalous ligament.
The third pattern with a RAA is circumflex left de-scending aorta. With this entity, the descendingaorta courses posterior to the esophagus and thendescends on the left side, analogous to a left aorticarch with a right descending aorta. A circumflex leftdescending aorta can occur with an anomalousLSCA, an anomalous left brachiocephalic artery,and mirror image branching. A vascular ring iscompletedbya left ligamentumarteriosumcoursingbetween the descending aorta and the LPA.
Cervical aortic arch A CAA occurs when the aorticarch is positioned above the thoracic inlet. Thiscondition results when the third arch is the basisfor aortic arch development, rather than the fourth.CAAmay occurwith both right and left third arches,leading to the potential formation of left-sided,right-sided, and double AAA. Most commonly, itoccurs on the right side with a persistent right thirdaortic arch and right dorsal aorta.68

Fig. 8. Right aortic arch with an aberrant LSCA. A young child with recurrent aspiration and respiratory distressunderwent MR angiography for evaluation of a vascular ring. (A–C) 3D volume rendered images show a rightaortic arch with an aberrant LSCA (short arrow), a diverticulum of Kommerell (long arrow), and a left ligamentusarteriosum resulting in a complete vascular ring. (D, E) Transverse dark blood images show an approximate 50%tracheal compression (asterisk) by the retroesophageal LSCA (arrow).
Hellinger et al984
Pulmonary artery slingPAS is a condition in which the LPA typically arisesfrom the RPA and courses between the tracheaand esophagus toward the left lung (Fig. 10).PAS develops as a result of proximal left sixtharch involution. Although right and left ligamentsare possible, only a left ligament leads to acomplete vascular ring. In this instance, the leftligament connects between the main or RPAand the left descending aorta. PAS is often associ-ated with concomitant central airway anomaliesand acquired abnormalities, including trachealrings, right upper lobe tracheal bronchus,
and tracheomalacia. Relief of symptoms re-quires transposing the LPA and correction ofpotential central airway anomalies or acquiredabnormalities.
Innominate artery compressionIAC on the trachea occurs when the anteriorcrossing innominate artery extrinsically com-presses the upper to midanterior trachea, oftenin an oblique manner (see Fig. 1). Although IACdoes not constitute a traditional vascular ring, itcan cause significant respiratory symptoms, parti-cularly in infants and young children, as discussed

Fig. 9. Right aortic arch with an aberrant LSCA. A young child with respiratory distress underwent CTA for eval-uation of a vascular ring. (A–C) 3D volume rendered (A) and MIP (B, C) images show a right aortic arch with anaberrant LSCA and a diverticulum of Kommerell (A, long arrow). A left ductus arteriosum (B, C; arrow) is patent,directly confirming the presence of a complete vascular ring.
Congenital Thoracic Vascular Anomalies 985
in an article by Lee and colleagues elsewhere inthis issue. IAC often results when there is accentu-ated horizontal angulation of the ascending aortaand compensatory angulation of the aortic archand branch arteries. MRI-MRA or CTA can directlydepict the innominate artery caliber and course aswell as the degree of tracheal narrowing, whichmay vary from a shallow asymmetric indentationto marked anterior-posterior compression ofgreater than 50%. IAC has a high associationwith intrinsic tracheomalacia, which should beconsidered when choosing the imaging modality,selecting the MRI-MRA or CTA protocol, and inter-preting the examination.1
Fig. 10. Pulmonary artery sling. A neonate with complexdistress who underwent CTA for evaluation of a vasculaLPA (arrow) arising from the RPA.
Pulmonary Arterial Anomalies
In addition to PAS, congenital pulmonary arterialanomalies include hypoplasia, agenesis (Fig. 11),and stenosis. These anomalies most often occurin associationwith complex conotruncal congenitalheart lesions, such as pulmonary valve stenosis,pulmonary valve atresia, tetralogy of Fallot, andTGA.69 Isolated pulmonary arterial hypo-plasia and agenesis, in the absence of complexCHD, are often associated with pulmonary hypo-plasia and hypogenetic lung syndrome (Fig. 12).Isolated pulmonary arterial stenosis (PASt) israre. Such stenoses most commonly involve thecentral main and branch pulmonary arteries, but
congenital heart disease and unexplained respiratoryr ring. (A, B) 3D volume rendered images show the

Fig. 11. Pulmonary artery agenesis. A neonate with mild respiratory distress underwent CTA following anabnormal chest radiograph. (A) Frontal chest radiograph shows dextroposition of the heart and mild rightlung oligemia with asymmetric left greater than right pulmonary vascularity. (B) 3D volume rendered imageshows RPA agenesis. Pulmonary blood flow (PBF) is thus from the main pulmonary artery (MPA) to the LPA.(C) Coronal MIP image shows right pulmonary arterial reconstitution at the lobar level from systemic to pulmo-nary collateral arteries (arrows).
Fig. 12. Hypogenetic lung syndrome with partial pulmonary venous return to the IVC (scimitar syndrome). Anadolescent with respiratory exercise intolerance underwent MDCT angiography. (A) Frontal chest radiographshows increased left pulmonary vascularity and an enlarged heart with either dextrocardia or dextropositionof the heart. (B) 3D volume rendered image confirms dextroposition of the heart. (C) Coronal inverse MinIPimage shows hypoplasia of the right lung with absence of the right upper lobe bronchus. (D) Coronal MIP imageshows hypoplasia of the RPA (long arrow) and partial anomalous pulmonary venous return of most of the rightlung into the IVC via 2 venous channels (short arrows). (E) Oblique thin-slab MIP image shows the hypoplastic RPAwith compensatory LPA enlargement related to dominant PBF. (F, G) Cardiac 4-chamber (F) and short-axis (G) mul-tiplanar reformations show an enlarged right atrium (RA) and right ventricle (RV) related to the right heartvolume overload. LA, left atrium; LV, left ventricle. (H, I) 3D volume rendered images show the anomalous rightlung venous drainage (short arrows) into the IVC. A small native right middle lobe vein (long arrow) drainsdirectly into the LA.
Hellinger et al986

Fig. 12. (continued)
Congenital Thoracic Vascular Anomalies 987
may occur in peripheral segments (eg, lobar andsegmental divisions). Lesions may be diffuse withlong segments of disease, resembling hypoplasia,or may be focal or multifocal with poststenotic dila-tation. Possible underlying causes for PASt includecongenital rubella, Williams syndrome, Noonansyndrome, Alagile syndrome, Ehlers-Danlossyndrome, and cutis laxa. The common pathologicfinding is abnormal development of the elastictissue of the media and increased collagen andfibrous tissue. Secondary intimal proliferationoccurs with the risk of localized thrombosis.Progressive and long-standing PASt increasesright ventricular afterload (pressure), leading toright ventricular hypertrophy, strain on the tricuspidvalvular apparatus, and potentially tricuspid insuffi-ciency and right heart failure.
VENOUS SYSTEMSSystemic Venous Anomalies
Normal thoracic systemic venous anatomyconsists of bilateral subclavian (SCV) and brachio-cephalic (BCV) veins, draining to the right superiorvena cava (RSVC) and then into the sinus venosusportion of the right atrium. Embryologically, theseveins develop from the paired anterior cardinaland common cardinal veins. A communicatingvein forms from the superior transverse capillaryplexuses and directs blood from the left to rightanterior cardinal vein. The entire right anteriorcardinal vein normally persists, forming the rightSCV (RSCV) and right BCV (RBCV) as well as theright internal jugular vein. The right SVC (RSVC)develops from the right anterior cardinal and

Hellinger et al988
common cardinal veins, which enter the sinus ve-nosus. In distinction, the left anterior cardinal veinundergoes near complete atrophy below the levelof the communicating vein, forming the ligament ofthe left vena cava. A residual central venoussegment forms the left superior intercostal vein,which drains the second and third intercostalspaces. The remainder of left anterior cardinalvein persists to form the left SCV and internaljugular vein. The communicating vein becomesthe left BCV (LBCV) and enlarges to accommodateincreased left to right flow. The LBCV coursesobliquely downward superior to the aortic archand anterior to the supra-aortic branch arteries,joining with the RBCV to form the RSVC. The leftcommon cardinal vein is incorporated into thecoronary venous anatomy, becoming the obliquevein of the left atrium (vein of Marshall), draininginto the coronary sinus of the right atrium.3
Anomalies of these systemic veins are rare.Systemic venous anomalies may occur in isolationor may be associated with cardiac disease, inparticular CHD and arrhythmias. Three of themore common systemic venous anomalies are(1) a persistent left SVC (LSVC) with a nativeRSVC; (2) a LSVC with mirror image venousdrainage (Fig. 13); and (3) a retroaortic left BCV(RA-LBCV, Fig. 14). Clear understanding of thesesystemic venous anomalies can facilitate planningand placement of central venous catheters, hemo-dynamic monitoring devices, and cardiac pace-maker and cardioverter-defibrillator leads, as wellas assessment of their respective positioning onchest radiographs following placement. Recogni-tion of a LSVC on echocardiography, MRI-MRA,or CTA is important for cardiac preoperativeplanning and surgical management, including
Fig. 13. Persistent left SVC with mirror systemic venous drMDCT angiography after abnormal chest radiograph. (A) Fmediastinal shadow (arrows). (B) Coronal MIP from a direcinto the coronary sinus (CS). (C) Coronal 3D volume rendshows mirror image systemic venous drainage with a rigThe LSVC is again noted to drain to the CS.
cardiopulmonary bypass and procedures forCHD (eg, cavopulmonary shunts).
Persistent left superior vena cavaA persistent left superior vena cava (LSVC) hasa prevalence of 0.1% to 0.5% in the generalpopulation.70,71 It occurs more frequently inpatients with CHD, with a reported prevalence of1.3% to 5%.72–74 Commonly associated CHDanomalies include septal defects (ventricular,atrial, and atrioventricular), tetralogy of Fallot, pul-monary atresia, bicuspid aortic valve, AS, aorticcoarctation, PDA, and anomalous pulmonaryvenous return.72,74 Extracardiac congenital anom-alies may be found in 60% of pediatric patientswith a persistent LSVC. Commonly associateddisorders include VACTERL (vertebral anomalies,anal atresia, cardiovascular anomalies, tracheoe-sophageal fistula, esophageal atresia, renal(kidney) and/or radial anomalies, limb defects),trisomy 21, 22q11 deletion, CHARGE (colobomaof the eye, central nervous system anomalies,heart defects, atresia of the choanae, retardationof growth and/or development, genital and/orurinary defects, ear anomalies and/or deafness)syndrome, and Turner syndrome.74 Embryologi-cally, a persistent LSVC results from persistenceof the left anterior cardinal vein. Concurrent persis-tence of the right anterior and common cardinalveins yields bilateral SVCs with or without acommunicating brachiocephalic vein (ie, bridgingvein).
Left superior vena cava with mirror imagevenous drainageInvolution of the right common cardinal vein andthe central anterior cardinal vein, along with
ainage. A young child with a known ASD underwentrontal chest radiograph shows a prominent left para-t CT venogram (CTV) shows a persistent LSVC drainingered image obtained during the delayed CTV phaseht brachiocephalic vein (RBCV) draining to the LSVC.

Fig. 14. Retroaortic left brachiocephalic vein. CTA was performed in a young adolescent who previously under-went tetralogy of Fallot surgical repair. (A–D) 3D volume rendered images (A, C, D) and MIP image (B) illustratethe course of a retroaortic left brachiocephalic vein (LBCV, arrows) that contains a traversing central venous cath-eter. The LBCV courses under the aortic arch, anterior to the central pulmonary arteries and then posterior to theascending aorta (AO) to join the right SVC.
Congenital Thoracic Vascular Anomalies 989
persistence of the communicating vein and the leftanterior cardinal vein, results in mirror imagethoracic systemic venous drainage (ie, right BCVand an LSVC). In most instances, the LSVC drainsinto the coronary sinus and the coronary sinusenlarges to accommodate flow.74 Coronary sinusdilatation may potentially lead to left atrioventric-ular valve inflow obstruction, which in turn maylead to cardiac arrhythmias and/or sudden death.In addition, abnormal cardiac impulse formationand conduction may arise from abnormal mor-phologic development of the sinoatrial node,atrioventricular node, and bundle of His (eg,lengthening).70 Rarely, the LSVC drains into theleft atrium (ie, complete unroofing of the coronarysinus), leading to interatrial communication, rightto left shunting, and cyanosis.74
Retroaortic left brachiocephalic veinThe retroaortic LBCV is found in 0.5% to 0.6% ofpatients with CHD75,76 and in only 0.02% ofpatients who do not have CHD.76 It courses poste-rior to the ascending aorta, underneath the aorticarch, and anterior to the central main and rightpulmonary arteries, to join the RSVC at or belowthe ostial confluence of the azygous vein. Althoughit results in neither physiologic nor hemodynamicsequelae, a retroaortic left brachiocephalic veinis associated with congenital heart disease,including right side obstructive lesions (tetralogy
of Fallot, pulmonary atresia), truncus arteriosus,and AAA (eg, IAA, RAA, CAA). Embryologically, itoccurs when the developing communicating veinanastomoses with the right inferior transversecapillary plexus.75
Pulmonary Venous Anomalies
The lung buds, developing from the foregut,initially drain via a venous plexus into the cardinalvenous system.3 A common pulmonary vein (CPV)arises from the dorsum of the left atrium and anas-tomoses with the venous plexus. Connections tothe cardinal venous system involute with subse-quent direct pulmonary venous drainage into theleft atrium. CPV absorption into the wall of theleft atrium results in variable pulmonary vein ostiaand branching patterns, with a standard of single,bilateral superior and inferior pulmonary veintrunks.
Abnormal development of the CPV (eg, incom-plete resorption) and its anastomosis with theprimitive venous plexus, along with persistentconnections to the systemic cardinal veins, giverise to partial anomalous pulmonary venous return(PAPVR) or total anomalous pulmonary venous re-turn (TAPVR; 0.7%–3.2% of CHD).8,26–28 BothPAPVR and TAPVR result in a left to right shuntwith partial (PAPVR) or complete (TAPVR) admix-ture of deoxygenated and oxygenated blood.PAPVR and TAPVR may be associated with other

Hellinger et al990
congenital heart diseases, including heterotaxy;atrial, ventricular, and atrioventricular septaldefects; tetralogy of Fallot; and COA.77 Anoma-lous pulmonary venous return should be distin-guished from pulmonary veins, which haveanomalous peripheral connections and/or anaberrant course (eg, aberrant meandering vein)within the lungs, before normal drainage into theleft atrium.78 In most instances, echocardiographywith gray scale and Doppler interrogation depictsthe number, location, and course of pulmonaryveins; detects the direction of venous blood flow;and excludes flow obstruction. MRI-MRA or CTAmay be required when echocardiography cannotidentify all veins or when more comprehensiveevaluation is required following the diagnosis ofPAPVR or TAPVR. MR imaging offers the advan-tage of quantifying the shunt ratio (eg, Qp/Qs)using phase contrast imaging. CTA is advanta-geous for its superior visualization of the centralairway and lung in the evaluation of associatedpulmonary developmental anomalies.
Partial anomalous pulmonary venous returnIn PAPVR, 1 or more (but not all) of the pulmonaryveins (segmental, lobar, or main central trunk)drain directly into systemic veins (eg, SVC, inferiorvena cava [IVC], SCV, BCV, azygous vein), rightatrium, or coronary sinus. Hemodynamic sequelaereflect the degree (eg, number and size of anoma-lous veins) and duration of shunting. When theshunt is significant, flow across the right heartand pulmonary circulation is increased (eg,increased pulmonary blood flow [PBF]). The rightcardiac chambers and pulmonary vasculature(arteries and veins) are enlarged because ofvolume overload. Pulmonary hypertension andright heart failure may subsequently develop.Increased left atrial pressure may lead to pul-monary venous congestion; initially acyanotic,patients may become cyanotic. The right pulmo-nary veins are anomalous twice as often as theleft. Right upper lobe venous drainage into theSVC is the most common type of PAPVR(Fig. 15) and may be associated with a sinus veno-sus defect (Fig. 16). The second most frequenttype of PAPVR is left pulmonary venous drainageto the LBCV. The third most common form isanomalous drainage from the right lung to theIVC with an intact atrial septum. This conditionmay be associated with more complex pulmonarydevelopmental anomalies in the spectrum ofcongenital pulmonary venolobar syndrome,including bronchopulmonary sequestration (BPS),scimitar syndrome (see Fig. 12), and horseshoelung. Most associated BPS are extralobar withvenous drainage into azygous or hemiazygous
veins. In scimitar syndrome, also known as hypo-genetic lung syndrome, an anomalous CPV (scim-itar vein) drains a portion or the entire lung into theIVC either above or below the diaphragm. Alterna-tively, drainage may occur into hepatic veins,portal veins, azygous vein, coronary sinus, or rightatrium. The right lung is almost exclusivelyinvolved and has variable hypoplasia versus partialagenesis, associated with dextroposition of theheart and ipsilateral decreased pulmonary perfu-sion relative to the left. Additional associatedanomalies include bronchogenic cyst, BPS, horse-shoe lung, accessory diaphragm, and congenitaldiaphragmatic hernia. Pulmonary arteries to theaffected lung may have variable hypoplasia oragenesis, with or without systemic arterial supplyin the absence of an associated sequestration.
Total anomalous pulmonary venous returnIn TAPVR, all pulmonary veins have anomalousdrainage. Affected patients typically present inthe neonatal period. An obligatory ASD or patentforamen ovale is often present, leading to a rightto left shunt and cyanosis. Veins may drain viaa common vein into systemic veins or the rightatrium (via the coronary sinus). Alternatively, veinsmay first drain into a venous confluence and thento a common draining vein. Depending on the levelof anomalous connections, TAPVR drainage maybe categorized as supracardiac (type I, Fig. 17),intracardiac (type II), infracardiac (type III), ormixed (Figs. 18 and 19). In the common form oftype I TAPVR, the pulmonary veins are mostcommonly drained by a left ascending verticalvein to the LBCV and then the SVC, resulting inincreased PBF, cardiomegaly, and a wide medias-tinum radiographically. Other sites of supracardiacsystemic connection are the SVC (right or left, seeFig. 17) and azygous vein. In type 2 TAPVR, theanomalous pulmonary veins drain into the coro-nary sinus (see Fig. 18B–D), leading to increasedPBF, cardiomegaly, and a narrow mediastinumradiographically. Venous flow in types I and IITAPVR is unobstructed. Affected neonates oftendevelop right heart volume overload, pulmonaryhypertension, and right heart failure. In type 3TAPVR (see Fig. 19B, C), anomalous veins drainvia a descending vertical vein into the portal,hepatic, or mesenteric venous systems, with flowobstruction at or below the diaphragm, pulmonaryvenous congestion, a normal to small heart size,and a narrow mediastinum radiographically. Thistype constitutes a neonatal cardiopulmonaryemergency because there is diminished cardiacoutput, poor systemic perfusion, and even greatercyanosis. The mixed type consists of combina-tions of types I to III TAPVR.

Fig. 16. Partial pulmonary venous return with sinus venosus defect. Cardiac MR imaging was performed ina young child with exertional shortness of breath and mild hypoxia. (A, B) Bright-blood MR angiography MIPimages show right upper lobe anomalous pulmonary venous return into the SVC, above (arrows) or at the cav-oatrial junction (arrowhead). A septal defect is present along the sinus venosus portion of the interatrial septum(asterisk), leading to communication between the RA and LA.
Fig. 15. Partial pulmonary venous return with intact atrial septum. An adolescent with exertional chest pressureand mild hypoxia underwent MDCT angiography. (A) Frontal chest radiograph shows moderate cardiomegalywith prominent central pulmonary vascularity. (B) Four-chamber multiplanar reformation shows an enlargedRA and RV with flattening of the interatrial and interventricular septae, related to the right heart volume over-load. (C, D) 3D volume rendered images show right upper lobe segmental pulmonary veins (arrows) draining tothe SVC (asterisk) with all other pulmonary veins draining into the LA.
Congenital Thoracic Vascular Anomalies 991

Fig. 18. TAPVR (mixed type I and II). A neonate with anomalous pulmonary veins diagnosed by echocardiographyunderwent low-dose MDCT angiography. (A–D) Variable thick, MIP images show that the left upper pulmonaryveins drain into the LBCV (A, short arrow), whereas the left lower (B, D; arrowheads) and all right lung pulmonaryveins (B, C; long arrows) drain to a retrocardiac confluence (B, asterisk). From the common confluence, blooddrains (C, D, asterisks) into the CS.
Fig. 17. TAPVR (Supracardiac Type I). A neonate with complex congenital heart disease underwent MDCT angi-ography. (A, B) 3D volume rendered images show bilateral anomalous drainage of all pulmonary veins (arrows)into a left SVC (LSVC). Blood then flows to the CS.
Hellinger et al992

Fig. 19. TAPVR (mixed type I and III). A neonate in severe cardiopulmonary distress at 2 days of life underwentMDCT angiography. (A) Frontal chest radiograph shows moderate diffuse pulmonary venous congestion witha normal cardiac silhouette. (B, C) Coronal MIP (B) and 3D volume rendered (C) images show right pulmonaryvenous drainage via a common draining vein (short arrows). The common vein courses below the diaphragmand feeds into the confluence of the mesenteric and splenic veins (asterisk). Blood then drains into the portalvenous (PV) system. Note the moderate obstructive stenosis (long arrow) in the common draining vein just aboveits distal outflow. Left pulmonary venous drainage was into the LBCV (not shown).
Congenital Thoracic Vascular Anomalies 993
SUMMARY
Diagnostic imaging is crucial in the evaluation ofthoracic congenital arterial and venous anomaliesin pediatric patients. Although clinical assessmentmay provide insight into the possible diagnosis,imaging is usually necessary to confirm the diag-nosis. Initial imaging algorithms using noninvasivemodalities often begin with chest radiographyfollowed by echocardiography. State-of-the-artMRI-MRA and MDCT angiography with advanced3D visualization are essential in these algorithmsnot only for diagnosis but also treatment planningand postoperative and postendovascular evalua-tion. Selection betweenMRI-MRA and CTA shouldbe based on their respective advantages,balanced by the suspected or known congenitalvascular anomaly and patient’s clinical presenta-tion and hemodynamic stability. Understandingthe embryologic basis and anatomic characteris-tics of thoracic congenital vascular anomaliesassists in their recognition with MRI-MRA andMDCT angiography in pediatric patients.
REFERENCES
1. Lee EY, Zurakowski D, Waltz DA, et al. MDCT evalu-
ation of the prevalence of tracheomalacia in children
with mediastinal aortic vascular anomalies. J Thorac
Imaging 2008;23:258–65.
2. Hellinger JC, Pena A, Poon M, et al. Pediatric
computed tomographic angiography: imaging the
cardiovascular system gently. Radiol Clin North Am
2010;48:439–67, x.
3. Moore KL. The cardiovascular system. In: The devel-
oping human: clinically oriented embryology. 8th
edition.Philadelphia:WBSaunders; 2008.p. 286–337.
4. Rudolph AM, Heymann MA, Spitznas U. Hemody-
namic considerations in the development of narrow-
ing of the aorta. Am J Cardiol 1972;30:514–25.
5. Shinebourne EA, Elseed AM. Relation between fetal
flow patterns, coarctation of the aorta, and pulmo-
nary blood flow. Br Heart J 1974;36:492–8.
6. Rosenberg HS. Coarctation as a deformation. Pe-
diatr Pathol 1990;10:103–15.
7. Collins-Nakai RL, Dick M, Parisi-Buckley L, et al. In-
terrupted aortic arch in infancy. J Pediatr 1976;88:
959–62.
8. Samanek M, Voriskova M. Congenital heart disease
among 815,569 children born between 1980 and
1990 and their 15-year survival: a prospective
Bohemia survival study. Pediatr Cardiol 1999;20:
411–7.
9. Schultz AH, Localio AR, Clark BJ, et al. Epidemio-
logic features of the presentation of critical congen-
ital heart disease: implications for screening.
Pediatrics 2008;121:751–7.
10. Norwood WI, Lang P, Castaneda AR, et al. Repara-
tive operations for interrupted aortic arch with
ventricular septal defect. J Thorac Cardiovasc
Surg 1983;86:832–7.
11. Vouhe PR, Mace L, Vernant F, et al. Primary definitive
repair of interrupted aortic arch with ventricular
septal defect. Eur J Cardiothorac Surg 1990;4:
365–70.

Hellinger et al994
12. Jonas RA, Quaegebeur JM, Kirklin JW, et al.
Outcomes in patients with interrupted aortic arch
andventricular septal defect.Amultiinstitutional study.
Congenital Heart Surgeons Society. J Thorac Cardio-
vascSurg1994;107:1099–109 [discussion: 1109–13].
13. Serraf A, Lacour-Gayet F, Robotin M, et al. Repair of
interrupted aortic arch: a ten-year experience.
J Thorac Cardiovasc Surg 1996;112:1150–60.
14. Tlaskal T, Hucin B, Hruda J, et al. Results of primary
and two-stage repair of interrupted aortic arch. Eur J
Cardiothorac Surg 1998;14:235–42.
15. Brown JW, Ruzmetov M, Okada Y, et al. Outcomes in
patients with interrupted aortic arch and associated
anomalies: a 20-year experience. Eur J Cardiothorac
Surg 2006;29:666–73 [discussion: 673–4].
16. Flint JD, Gentles TL, MacCormick J, et al. Outcomes
using predominantly single-stage approach to inter-
rupted aortic arch and associated defects. Ann
Thorac Surg 2010;89:564–9.
17. Van Mierop LH, Kutsche LM. Interruption of the
aortic arch and coarctation of the aorta: pathoge-
netic relations. Am J Cardiol 1984;54:829–34.
18. Marino B, Digilio MC, Persiani M, et al. Deletion
22q11 in patients with interrupted aortic arch. Am
J Cardiol 1999;84:360–1, A369.
19. Van Mierop LH, Kutsche LM. Cardiovascular anoma-
lies in DiGeorge syndrome and importance of neural
crest as a possible pathogenetic factor. Am J Cardiol
1986;58:133–7.
20. Lewin MB, Lindsay EA, Jurecic V, et al. A genetic
etiology for interruption of the aortic arch type B.
Am J Cardiol 1997;80:493–7.
21. Goldmuntz E, Clark BJ, Mitchell LE, et al. Frequency
of 22q11 deletions in patients with conotruncal
defects. J Am Coll Cardiol 1998;32:492–8.
22. Rauch A, Hofbeck M, Leipold G, et al. Incidence
and significance of 22q11.2 hemizygosity in patients
with interrupted aortic arch. Am J Med Genet 1998;
78:322–31.
23. Momma K, Ando M, Matsuoka R, et al. Interruption
of the aortic arch associated with deletion of chro-
mosome 22q11 is associated with a subarterial
and doubly committed ventricular septal defect in
Japanese patients. Cardiol Young 1999;9:463–7.
24. Randall V, McCue K, Roberts C, et al. Great vessel
development requires biallelic expression of Chd7
and Tbx1 in pharyngeal ectoderm in mice. J Clin
Invest 2009;119:3301–10.
25. Jyonouchi S, McDonald-McGinn DM, Bale S, et al.
CHARGE (coloboma, heart defect, atresia choanae,
retarded growth and development, genital hypo-
plasia, ear anomalies/deafness) syndrome and
chromosome 22q11.2 deletion syndrome: a compar-
ison of immunologic and nonimmunologic pheno-
typic features. Pediatrics 2009;123:e871–7.
26. Report of the New England Regional Infant Cardiac
Program. Pediatrics 1980;65:375–461.
27. Goetzova J, Benesova D. Congenital heart diseases
at autopsy of still-born and deceased children in
the central Bohemian region. Cor Vasa 1981;23:8–13.
28. Samanek M, Slavik Z, Zborilova B, et al. Prevalence,
treatment, and outcome of heart disease in live-born
children: a prospective analysis of 91,823 live-born
children. Pediatr Cardiol 1989;10:205–11.
29. Bolisetty S, Daftary A, EwaldD, et al. Congenital heart
defects in central Australia. Med J Aust 2004;180:
614–7.
30. Tawes RL Jr, Aberdeen E, Waterston DJ, et al.
Coarctation of the aorta in infants and children. A
review of 333 operative cases, including 179 infants.
Circulation 1969;39:I173–84.
31. Miettinen OS, Reiner ML, Nadas AS. Seasonal inci-
dence of coarctation of the aorta. Br Heart J 1970;
32:103–7.
32. Cheatham JE Jr, Williams GR, Thompson WM, et al.
Coarctation: a review of 80 children and adoles-
cents. Am J Surg 1979;138:889–93.
33. Liberthson RR, Pennington DG, Jacobs ML, et al.
Coarctation of the aorta: review of 234 patients
and clarification of management problems. Am J
Cardiol 1979;43:835–40.
34. Kish GF, Tenekjian VK, Tarnay TJ, et al. Coarctation
of the thoracic aorta: an 18-year experience. Am
Surg 1981;47:26–30.
35. Bobby JJ, Emami JM, Farmer RD, et al. Operative
survival and 40 year follow up of surgical repair of
aortic coarctation. Br Heart J 1991;65:271–6.
36. Ou P, Celermajer DS, Mousseaux E, et al. Vascular
remodeling after “successful” repair of coarctation:
impact of aortic arch geometry. J Am Coll Cardiol
2007;49:883–90.
37. Koller M, Rothlin M, Senning A. Coarctation of the
aorta: review of 362 operated patients. Long-term
follow-up and assessment of prognostic variables.
Eur Heart J 1987;8:670–9.
38. Krediet P. An hypothesis of the development of
coarctation in man. Acta Morphol Neerl Scand 1965;
6:207–12.
39. Hutchins GM. Coarctation of the aorta explained as
a branch-point of the ductus arteriosus. Am J Pathol
1971;63:203–14.
40. Momma K, Takao A, Ando M. Angiocardiographic
study of coarctation of the aorta–morphology and
morphogenesis. Jpn Circ J 1982;46:174–83.
41. Kappetein AP, Zwinderman AH, Bogers AJ, et al.
More than thirty-five years of coarctation repair. An
unexpected high relapse rate. J Thorac Cardiovasc
Surg 1994;107:87–95.
42. Glass IH, Mustard WT, Keith JD. Coarctation of the
aorta in infants. A review of twelve years’ experi-
ence. Pediatrics 1960;26:109–21.
43. Williams WG, Shindo G, Trusler GA, et al. Results of
repair of coarctation of the aorta during infancy.
J Thorac Cardiovasc Surg 1980;79:603–8.

Congenital Thoracic Vascular Anomalies 995
44. Sorland SJ, Rostad H, Forfang K, et al. Coarctation
of the aorta. A follow-up study after surgical treat-
ment in infancy and childhood. Acta Paediatr Scand
1980;69:113–8.
45. Rostad H, Abdelnoor M, Sorland S, et al. Coarctation
of the aorta, early and late results of various surgical
techniques. J Cardiovasc Surg (Torino) 1989;30:
885–90.
46. Van Son JA, Falk V, Schneider P, et al. Repair of
coarctation of the aorta in neonates and young
infants. J Card Surg 1997;12:139–46.
47. Nanton MA, Olley PM. Residual hypertension after
coarctectomy in children. Am J Cardiol 1976;37:
769–72.
48. Cohen M, Fuster V, Steele PM, et al. Coarctation of
the aorta. Long-term follow-up and prediction of
outcome after surgical correction. Circulation 1989;
80:840–5.
49. Toro-Salazar OH, Steinberger J, Thomas W, et al.
Long-term follow-up of patients after coarctation of
the aorta repair. Am J Cardiol 2002;89:541–7.
50. Smallhorn JF, Huhta JC, Adams PA, et al. Cross-
sectional echocardiographic assessment of coarc-
tation in the sick neonate and infant. Br Heart J
1983;50:349–61.
51. Dodge-Khatami A, Ott S, Di Bernardo S, et al.
Carotid-subclavian artery index: new echocardio-
graphic index to detect coarctation in neonates
and infants. Ann Thorac Surg 2005;80:1652–7.
52. Ming Z, Yumin Z, Yuhua L, et al. Diagnosis of
congenital obstructive aortic arch anomalies in
Chinese children by contrast-enhanced magnetic
resonance angiography. J Cardiovasc Magn Reson
2006;8:747–53.
53. Hu XH, Huang GY, Pa M, et al. Multidetector CT
angiography and 3D reconstruction in young chil-
dren with coarctation of the aorta. Pediatr Cardiol
2008;29:726–31.
54. Dorfman AT, Marino BS, Wernovsky G, et al. Critical
heart disease in the neonate: presentation and
outcome at a tertiary care center. Pediatr Crit Care
Med 2008;9:193–202.
55. Bertolini A, Pelizza A, Panizzon G, et al. Vascular
rings and slings. Diagnosis and surgical treatment
of 49 patients. J Cardiovasc Surg (Torino) 1987;28:
301–12.
56. Hartyanszky IL, Lozsadi K, Marcsek P, et al.
Congenital vascular rings: surgical management
of 111 cases. Eur J Cardiothorac Surg 1989;3:
250–4.
57. Rivilla F, Utrilla JG, Alvarez F. Surgical management
and follow-up of vascular rings. Z Kinderchir 1989;
44:199–202.
58. Chun K, Colombani PM, Dudgeon DL, et al. Diag-
nosis and management of congenital vascular rings:
a 22-year experience. Ann Thorac Surg 1992;53:
597–602 [discussion: 602–3].
59. van Son JA, Julsrud PR, Hagler DJ, et al. Surgical
treatment of vascular rings: the Mayo Clinic experi-
ence. Mayo Clin Proc 1993;68:1056–63.
60. Kocis KC, Midgley FM, Ruckman RN. Aortic arch
complex anomalies: 20-year experience with symp-
toms, diagnosis, associated cardiac defects, and
surgical repair. Pediatr Cardiol 1997;18:127–32.
61. Woods RK, Sharp RJ, Holcomb GW 3rd, et al.
Vascular anomalies and tracheoesophageal com-
pression: a single institution’s 25-year experience.
Ann Thorac Surg 2001;72:434–8 [discussion: 438–9].
62. Backer CL, Mavroudis C, Rigsby CK, et al. Trends in
vascular ring surgery. J Thorac Cardiovasc Surg
2005;129:1339–47.
63. Turner A, Gavel G, Coutts J. Vascular rings–presen-
tation, investigation and outcome. Eur J Pediatr
2005;164:266–70.
64. McElhinney DB, McDonald-McGinn D, Zackai EH,
et al. Cardiovascular anomalies in patients diag-
nosed with a chromosome 22q11 deletion beyond
6 months of age. Pediatrics 2001;108:E104.
65. Anand R, Dooley KJ, Williams WH, et al. Follow-up of
surgical correction of vascular anomalies causing
tracheobronchial compression. Pediatr Cardiol
1994;15:58–61.
66. McLaughlin RB Jr, Wetmore RF, Tavill MA, et al.
Vascular anomalies causing symptomatic tracheo-
bronchial compression. Laryngoscope 1999;109:
312–9.
67. Edwards JE. Anomalies of the derivatives of the aortic
arch system. Med Clin North Am 1948;32:925–49.
68. Davies M, Guest PJ. Developmental abnormalities of
the great vessels of the thorax and their embryolog-
ical basis. Br J Radiol 2003;76:491–502.
69. Ziolkowska L, Kawalec W, Turska-Kmiec A, et al.
Chromosome 22q11.2 microdeletion in children with
conotruncal heart defects: frequency, associated
cardiovascular anomalies, and outcome following
cardiac surgery. Eur J Pediatr 2008;167:1135–40.
70. Biffi M, Boriani G, Frabetti L, et al. Left superior vena
cava persistence in patients undergoing pacemaker
or cardioverter-defibrillator implantation: a 10-year
experience. Chest 2001;120:139–44.
71. Gonzalez-Juanatey C, Testa A, Vidan J, et al. Persis-
tent left superior vena cava draining into the coro-
nary sinus: report of 10 cases and literature review.
Clin Cardiol 2004;27:515–8.
72. Bjerregaard P, Laursen HB. Persistent left superior
vena cava. Incidence, associated congenital heart
defects and frontal plane P-wave axis in a paediatric
population with congenital heart disease. Acta Pae-
diatr Scand 1980;69:105–8.
73. Parikh SR, Prasad K, Iyer RN, et al. Prospective
angiographic study of the abnormalities of systemic
venous connections in congenital and acquired
heart disease. Cathet Cardiovasc Diagn 1996;38:
379–86.

Hellinger et al996
74. Postema PG, Rammeloo LA, van Litsenburg R, et al.
Left superior vena cava in pediatric cardiology asso-
ciated with extra-cardiac anomalies. Int J Cardiol
2008;123:302–6.
75. Curtil A, Tronc F, Champsaur G, et al. The left retro-
aortic brachiocephalic vein: morphologic data and
diagnostic ultrasound in 27 cases. Surg Radiol
Anat 1999;21:251–4.
76. Nagashima M, Shikata F, Okamura T, et al. Anoma-
lous subaortic left brachiocephalic vein in surgical
cases and literature review. Clin Anat 2010;23:
950–5.
77. Seale AN, Uemura H, Webber SA, et al. Total anom-
alous pulmonary venous connection: morphology
and outcome from an international population-
based study. Circulation 2010;122:2718–26.
78. Sato M, Tanaka D, Nakajo M. Meandering pulmonary
veins with a common inferior trunk: an anomalous left
inferior pulmonary vein entering an anomalous right
inferior pulmonary vein. Radiat Med 2007;25:426–9.