Embed Size (px)
Citation preview

CONGENITAL MALFORMATION OF HEART.
By ARTHUR WYNNE FOOT, 3I.D., F.K.Q.C.P.;Physician to the Meath Hospital ; Professor of Medicine, Royal College of
Surgeons.
[Read in the Pathological Section, February 11, 1887.]
DR. FOOT exhibited the heart of a young man, aged twenty-one,which presented a perforation of the inter-ventricular septum.The communication was formed by a passage about the width of agoose-quill passing downwards and to the right. Its left end com-menced immediately underneath the posterior segment of the aorticvalve ; its right end debouched in the right ventricle underneath astrong moderator band, and in front of the attachment of thepostero-internal segment of the tricuspid valve, just below themouth of the pulmonary artery ; the arterial (left) end of thepassage was funnel-shaped and smoothly lined by a tough ring ofthickened endocardium. The foramen ovale was closed. Thecoronary arteries were anomalous, inasmuch as both rose above theposterior aortic valve, and these were very unequal in size; theconus arteriosus bulged prominently forwards towards the lumenof the right ventricle.
This lad was in hospital with an attack of rheumatism, theresult of a wetting. The day after admission a loud single murmur,systolic in time, was discovered, most audible over the face of theright ventricle, not conveyed along the vessels, unattended withthrill, and distinctly transverse in direction. Five days afteradmission his temperature rose suddenly, and he became delirious,and he died on the tenth day after admission. It is likely that themurmur, in the absence of valvular lesion, was connected with thisinter-ventricular opening. The depression bulging towards the right'ventricle would suggest that blood passed from the left to the right
Congenital Malformation of Heart. 271
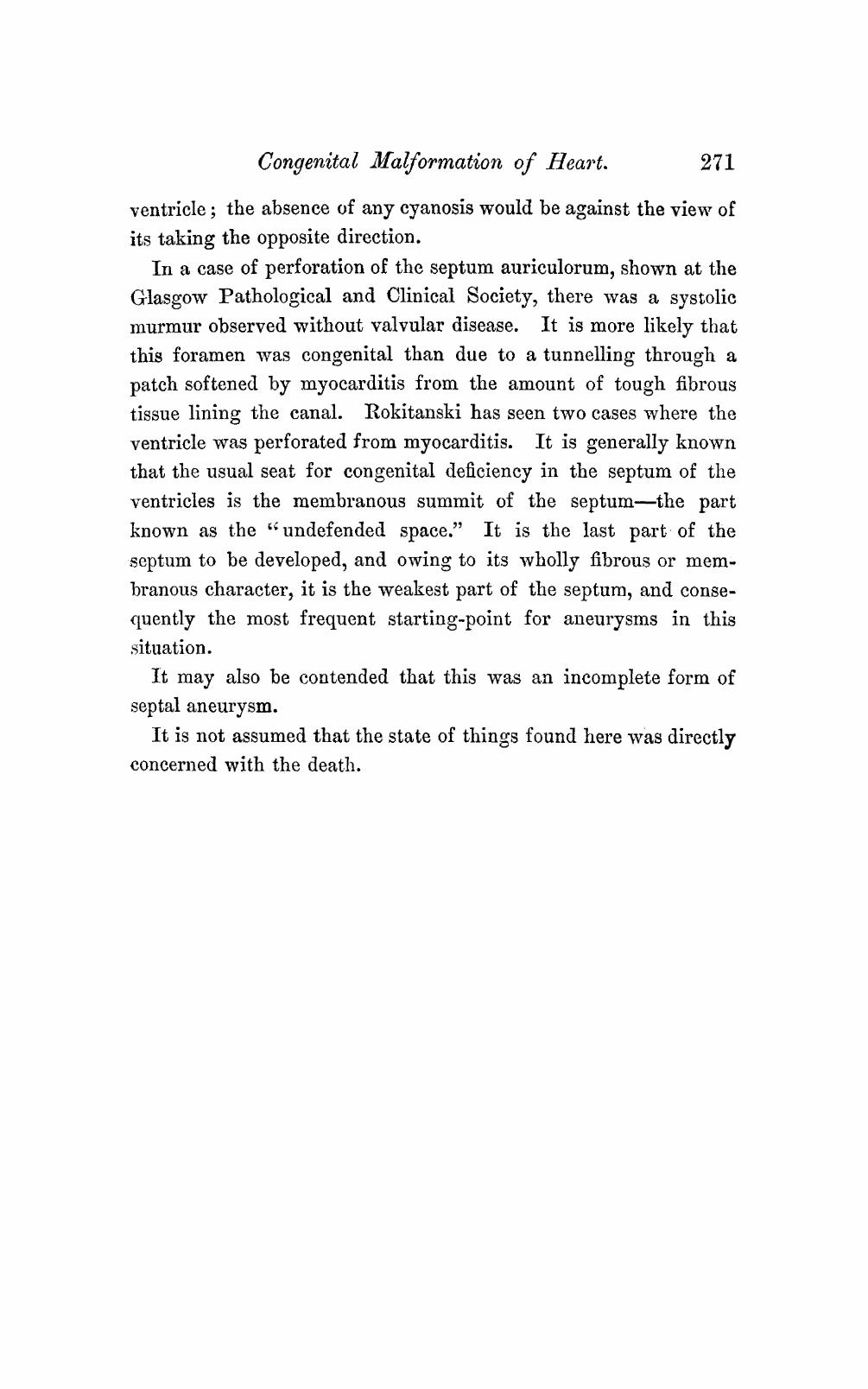
ventricle; the absence of any cyanosis would be against the view ofits taking the opposite direction.
In a case of perforation of the septum auriculorum, shown at theGlasgow Pathological and Clinical. Society, there was a systolicmurmur observed without valvular disease. It is more likely thatthis foramen was congenital than due to a tunnelling through apatch softened by myocarditis from the amount of tough fibroustissue lining the canal. Rokitanski has seen two cases where theventricle was perforated from myocarditis. It is generally knownthat the usual seat for congenital deficiency in the septum of theventricles is the membranous summit of the septum the partknown as the " undefended space." It is the last part - of theseptum to be developed, and owing to its wholly fibrous or membranous character, it is the weakest part of the septum, and conse-quently the most frequent starting-point for aneurysms in thissituation.
It may also be contended that this was an incomplete form ofseptal aneurysm.
It is not assumed that the state of things found here was directlyconcerned with the death.




![Rx161 Arnold-Chiari Malformationfinalcopy0048502.netsolhost.com/.../pdfs/RXforms/Arnold_Chiari_Malformation.pdfArnold-Chiari malformation [Chiari malformation (CM)] is a congenital](https://img.pdfslide.us/doc/110x75/5ab9a8f17f8b9ac60e8e5491/rx161-arnold-chiari-malforma-malformation-chiari-malformation-cm-is-a-congenital.jpg)