-
8/13/2019 Congenital Lung Malformations
1/115
History case
A boy of 7 years the last 2 years was repeatedly treated for
right
inferior lobe bronchopneumonia.
On the plain chest X-ray, there is a well defined opacity at the
level
of the inferior lobe of the right lung. The shadow adjoins to
the
mediastinum.
-
8/13/2019 Congenital Lung Malformations
2/115
Suspected diagnosis???
Pulmonary hypoplasia,
Congenital lobar emphysema,
Pulmonary sequestration, Congenital pulmonary airway
malformation,
Bronchogenic cyst.
-
8/13/2019 Congenital Lung Malformations
3/115
Congenital lung malformations
Jalba Alexandru,
MD, PhD,
associate professor
Chisinau 2013
N. Testemitanu State University of Medicine and Pharmacy
Department of Pediatric Surgery, Orthopedics and
Anesthesiology
-
8/13/2019 Congenital Lung Malformations
4/115
Background
o The aim of this lecture is to provide a concise approach to
congenital lung
malformations.
o Discussed issues:
o bronchogenic cyst,
o pulmonary agenesis and hypoplasia,
o polyalveolar lobe,
o alveolocapillary dysplasia,
o sequestration including arteriovenous malformation (AVM)
and
o scimitar syndrome,
o pulmonary lymphangiectasis,
o congenital lobar emphysema (CLE), and
o congenital cystic adenomatoid malformation (CCAM) (sin.
congenital pulmonary airway malformation(CPAM)) and other
lung
cysts.
-
8/13/2019 Congenital Lung Malformations
5/115
Background
o Although they secrete the amniotic fluid, the lungs are
unnecessary as
organs of respiration in fetal life.
o However, their development must occur so that air exchange may
take
place at birth.
o The lungs go through
o embryonic,
o pseudoglandular,
o canalicular,
o saccular, ando alveolar phases (Fig. 1).
-
8/13/2019 Congenital Lung Malformations
6/115
Background
Fig. 1. Lungs development.
-
8/13/2019 Congenital Lung Malformations
7/115
History of the procedure
o Surgery for congenital lung malformation was made possible
relatively
recently.
o Early 20th century thoracic surgery consisted of mainly
thoracoplasty to
collapse a tuberculoid lung or to drain an empyema.
o Only with the regular use of endotracheal intubation and
mechanical
ventilation in the 1950s did intrathoracic procedures become
routine.
o These techniques were not widely applied to newborns until the
1950s.
o Although Evarts Graham performed pneumonectomy with mass
ligature
of the hilum, Churchill was the first to regularly perform
lobectomy
with hilar dissection.
o Gross and Lewis successfully treated a patient with congenital
lobar
emphysema with lobectomy in 1943.
-
8/13/2019 Congenital Lung Malformations
8/115
History of the procedure
o Bronchogenic cysts are increasingly excised
thoracoscopically.
o Rodgers vigorously promoted endoscopic surgery, which has
become
prevalent with the plethora of new instrumentation available and
with
the expansion of minimally invasive laparoscopy and
thoracoscopy.
o Most thoracic surgical procedures, such as resection of
masses
(neurogenic tumors, bronchogenic cysts) and pulmonary lobectomy,
are
now accomplished with minimally invasive surgery, although
the
benefits of this approach for cystic adenomatoid malformations
are
unclear.
-
8/13/2019 Congenital Lung Malformations
9/115
History of the procedure
o Fetal surgery has been advocated for
cystic adenomatoid malformation with
hydrops, although it has been abandoned
for congenital diaphragmatic hernia
(CDH).
o The extrauterine intrapartum (EXIT)
procedure involves delivery of the baby
in which the umbilical circulation is left
intact if the baby has a congenital high
airway obstruction. This procedureallows relief of the
obstruction while
providing gas exchange across the
placenta (Fig. 2).
Fig. 2.EXIT procedure.
-
8/13/2019 Congenital Lung Malformations
10/115
Classification by site of origin
Trachea and Bronchi Pulmonary parenchyma Vascular
Agenesis
Congenital pulmonary airway
malformations (preciously
congenital cystic adenomatoid
malformation)
Hemangioma
Atresia, stenosisBronchopulmonary
sequestration
Arteriovenosus
malformation
Tracheal bronchus Congenital lobar emphysema Scimitar
syndrome
Esophageal bronchus/lung
(communicating
bronchopulmonary malformation)
Agenesis Congenital pulmonary
lymphangiectasia
Bronchogenic cyst Aplasia Lymphangioma
Enteric duplication cyst Hypoplasia Congenital chylotorax
Neuroenteric cystBronchiolar cysts (cystic
bronchiectasismultiple)
Bronchial cysts (peripheral) Lobulation abnormalities
-
8/13/2019 Congenital Lung Malformations
11/115
Epidemiology
o Frequency: Congenital lung malformations represent 5-18.7% of
all
congenital anomalies. This range may be an underestimate because
of
the high frequency of undetected or asymptomatic lesions.
-
8/13/2019 Congenital Lung Malformations
12/115
Generalities
o Although congenital lung malformations are rare, they are
important
disorders because they may lead to considerable morbidity and
mortality
(eg, infection, hemorrhage, respiratory failure).
o Prognosis depends on the size of the lesion, and the degree of
functional
impairment.
o Small lesions may remain asymptomatic.
o Failure to recognize a malformation may lead to
inappropriate
intervention.
o For example, placement of a chest tube to manage suspected
tension
pneumothorax in a patient with congenital lobar emphysema may
lead
to lung contusion and ventilation through the chest tube instead
of into
the remaining healthy lung.
-
8/13/2019 Congenital Lung Malformations
13/115
Generalities
o Healthy lung is composed of an orderly system of tubes
(airways) and sacs
(airspaces or alveoli) in a strict relationship to pulmonary
blood vessels
(arterial from the right ventricle and venous return to the left
atrium) (Fig.3).
Fig. 3.Lung vasculature
-
8/13/2019 Congenital Lung Malformations
14/115
Generalities
o Also present is a systemic blood supply (aorta to superior
vena cava) and
lymphatic drainage (Fig. 5).
o Congenital lung malformations arise whenever one or more of
these
structures are abnormal or when their relationships are
altered.
Fig. 5.Pulmonary and systemic blood supply of the lungs
-
8/13/2019 Congenital Lung Malformations
15/115
CERTAIN LUNG
MALFORMATIONS
-
8/13/2019 Congenital Lung Malformations
16/115
Bronchogenic cysts
o Bronchogenic cysts are also known as foregut duplication.
o They arise from an abnormal budding of the ventral
foregut.
o Approximately 85% are mediastinal, and 15% are intrapulmonary
(Fig. 6).
Fig. 6.Bronchogenic cysts.
-
8/13/2019 Congenital Lung Malformations
17/115
Bronchogenic cysts
o The peripheral cysts are multiple and appear late in
gestation.
o They may be filled with air or fluid, or they may have
air-fluid levels.
o The cysts can be central or peripheral.
Fig. 6.Bronchogenic cysts.
-
8/13/2019 Congenital Lung Malformations
18/115
Bronchogenic cysts
o Many are asymptomatic, but incidental findings may be observed
on
chest radiography (Fig. 7, 8).
Fig. 7. Bronchogenic cyst of the mediastinum
-
8/13/2019 Congenital Lung Malformations
19/115
Bronchogenic cysts
o Many are asymptomatic, but incidental findings may be observed
on
chest radiography and (Fig. 7, 8).
Fig. 8. Bronchogenic cyst. CT scan demonstrates a thin-walled
cyst in the right upper lobe.
-
8/13/2019 Congenital Lung Malformations
20/115
Bronchogenic cysts
o Infection, hemorrhage, and, in rare cases, malignancy can
occur.
o Respiratory distress may result in a stridor or wheeze.
o Airtrapping may lead to emphysema, atelectasis, or both.
o Dysphagia, chest pain, and epigastric discomfort can
occur.
-
8/13/2019 Congenital Lung Malformations
21/115
Pulmonary agenesis and hypoplasia
o In lung agenesis, the entire lung and bronchial tree may be
absent on one
side.
o The bronchial tree may form without development of the
alveoli.
o Pulmonary hypertension complicates lung agenesis because of
a
combination of factors: normal blood volume passing through
reduced
lung tissue, hypoxemia leading to pulmonary vasoconstriction,
and any
associated left-to-right shunting cardiac lesion.
-
8/13/2019 Congenital Lung Malformations
22/115
Pulmonary agenesis and hypoplasia
o Intrathoracic or extrathoracic lesions can cause pulmonary
hypoplasia.
o Therefore, prolonged rupture of membranes, renal
dysplasia,
neuromuscular diseases, and congenital diaphragmatic hernia can
lead to
lung hypoplasia.
o Reduced urine volume during fetal life may retard lung
growth.
o Secondary pulmonary causes include cystic adenomatoid
malformation
and sequestrations.
o Secondary extrapulmonary, intrathoracic causes include
congenital
diaphragmatic hernia, hydrothorax, pleural effusions, and
tetralogy of
Fallot (due to poor lung blood flow).
-
8/13/2019 Congenital Lung Malformations
23/115
Pulmonary agenesis and hypoplasia
o Extrathoracic causes include renal dysplasia and neuromuscular
disorders(ie, poor breathing).
o Bilateral renal agenesis leads to oligohydramnios and poor
development
of the terminal airways secondary to decreased swallowing of
the
amniotic fluid.
o The urinary proline aids in the formation of collagen by the
fetal lung.
o Thyroid transcription factors also regulate lung
development.
o The lung hypoplasia in congenital diaphragmatic hernia is
complicated by
pulmonary hypertension.
o Pulmonary aplasia leads to respiratory distress, which may
vary
according to the degree of alveolar involvement. Pulmonary
hypoplasia
may be primary when the entire lung or when one lobe is reduced
in size.
-
8/13/2019 Congenital Lung Malformations
24/115
Pulmonary agenesis and hypoplasia
o Both pulmonary agenesis andhypoplasia may be accompanied
by renal anomalies, which are
usually apparent soon after birth
and associated with respiratory
distress. Cardiac defects occur in
50% of patients.
o Pulmonary agenesis is
differentiated from lung aplasia
by the absence of the carina in
the latter (Fig. 9).Fig. 9. A.Normal lungs.
B.Pulmonary aplasia, with complete absence of both bronchial
andalveolar tissue.
C. Pulmonary agenesis with a bronchus reminiscence and
D, Pulmonary dysplasia. Some bronchial elements are present,
butthere are no alveoli.
-
8/13/2019 Congenital Lung Malformations
25/115
Pulmonary agenesis and hypoplasia
o Lung agenesis is less common than aplasia, about 75% of cases
affect
the left side, and it is lethal in half of all patients.
o It may be associated with other manifestations of the syndrome
of
abnormalities of the Vertebrae, Anus, Cardiovascular tree,
Trachea,
Esophagus, Renal system, and Limb buds (VACTERLsyndrome).
o The survival rate is better with left-sided lung agenesis than
with right-
sided agenesis because the right lung is the larger of the
two.
-
8/13/2019 Congenital Lung Malformations
26/115
Pulmonary agenesis and hypoplasia
o In pulmonary hypoplasia,
development of the distal lung
tissue is incomplete (Fig. 10).
o The earlier the delivery of a
child, the higher the incidence of
lung hypoplasia.
o In babies delivered before 28
weeks' gestation, the incidence
approaches 20%.Fig. 10. A to C. Pulmonary hypoplasia. Three
conditions of differentembryogenesis that all result in a smaller
than normal lung.
A,Alveolar tissue not functional.
B,Reduced size of one lung.
C,Hypoplasia resulting from lobar dysplasia.
D to F.Pulmonary ectoplasia. Part or all of one lung is attached
to theesophagus and usually is supplied by a systemicartery. D,
Bronchoesophageal fistula. E, Sequestration of right lowerlobe.
F,Sequestration of lower lobe and dysplasia of upper lobe.
-
8/13/2019 Congenital Lung Malformations
27/115
Pulmonary agenesis and hypoplasia
o Pulmonary hypoplasia resultsfrom conditions that restrict
lung
growth, such as
oligohydramnios, Potter
syndrome (with bilateral renal
agenesis or dysplasia),
abnormalities of the thoracic
cage, Scimitar syndrome (right-
sided pulmonary hypoplasia),
and diaphragmatic hernia
(usually left-sided hypoplasia).Fig. 10. A to C. Pulmonary
hypoplasia. Three conditions of differentembryogenesis that all
result in a smaller than normal lung.
A,Alveolar tissue not functional.
B,Reduced size of one lung.
C,Hypoplasia resulting from lobar dysplasia.
D to F.Pulmonary ectoplasia. Part or all of one lung is attached
to theesophagus and usually is supplied by a systemicartery. D,
Bronchoesophageal fistula. E, Sequestration of right lowerlobe.
F,Sequestration of lower lobe and dysplasia of upper lobe.
-
8/13/2019 Congenital Lung Malformations
28/115
Pulmonary agenesis and hypoplasia
o More than 50% of patients have associated cardiac, gut, or
skeletal
malformations.
o They may have a small thoracic cage, decreased breath sounds
on the
affected side, and a mediastinal shift to the side of the lesion
(Fig. 11,
12).
o Therefore, aplasia of the right lung can be confused with
dextrocardia.
o Patients may present with lung infections, dyspnea upon
exertion,
and/or scoliosis.
-
8/13/2019 Congenital Lung Malformations
29/115
Pulmonary agenesis and hypoplasia
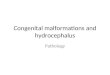
Fig. 11. Pulmonary hypoplasia. (a) Schematic illustrates
pulmonaryhypoplasia. (b)Anteroposterior chest radiograph of a
7-month-old infant shows opacityof the left hemithorax and small
left lung (arrows) with ipsilateral displacement of themediastinum,
secondary to repaired Bochdaleck hernia.
a b
-
8/13/2019 Congenital Lung Malformations
30/115
Pulmonary agenesis and hypoplasia
a b
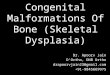
Fig. 12. Pulmonary hypoplasia. (a)Anteroposterior radiograph
shows opacity of the right hemithorax anda shift of the mediastinal
structures to the right, due to pulmonary hypoplasia secondary to
rightdiaphragmatic agenesis. (b) Angiographic MR image of a
10-year-old boy shows a hypoplastic rightpulmonary artery
(arrows).
-
8/13/2019 Congenital Lung Malformations
31/115
Pulmonary isomerism
o Pulmonary isomerism is an anomaly of the number of lung
lobes.
o In the common variety of pulmonary isomerism, the right lung
has 2
lobes, whereas the left has 3.
o This anomaly may be associated with situs inversus,
asplenia,
polysplenia, and/or anomalous pulmonary drainage.
-
8/13/2019 Congenital Lung Malformations
32/115
Azygous lobe
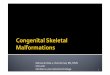
o An azygous lobe is a
malformation of the right
upper lobe caused by an
aberrant azygous vein
suspended by a pleural
mesentery.
o An azygous lobe is a
radiographic curiosity
without clinical
significance that occurs
in 0.5% of the general
population.
Fig. 13. A. A 15-year-old boy receiving chemotherapy for
osteogenic
sarcoma of the left femur. The chest radiograph showed an
azygous lobeof the lung with a thin fissure (arrows) separating it
from the rest of theright upper lobe. Computed tomography (Panels B
and C) revealed thefissure (Panel B, white arrows and Panel C,
asterisk) and a small nodulein the posterior right upper lobe, 1 cm
in diameter (Panel B, blackarrow). Evaluation of a specimen from a
thoracoscopic lung biopsy(Panel D) showed that the membranous
fissure (asterisk) contained theazygos vein (arrowheads) and
divided the apex of the right hemithorax.The lung nodule was found
to contain metastatic osteosarcoma.
-
8/13/2019 Congenital Lung Malformations
33/115
Pulmonary sequestration
o If an accessory lung bud forms early enough, it leads to the
formation of
sequestration in the normal lung tissue.
o Development late in gestation leads to extrapulmonic
sequestration.
o Both types obtain their blood supply from the aorta or its
branches.
o Patients may present with exercise intolerance due to these
vascularshunts.
o Sequestrations may also be connected to the GI tract.
-
8/13/2019 Congenital Lung Malformations
34/115
Pulmonary sequestration
o Pulmonary sequestration
accounts for 6% of all
congenital lung malformations
and mostly occurs in the lower
lobes.
o A sequestration is a
bronchopulmonary mass without
a normal bronchial
communication and with normal
or anomalous vascular supply
from the systemic circulation.
o Sequestered lung may be
intralobar or extralobar.
AORTA
INTRALOBAR EXTRALOBAR
Fig. 14. Pulmonary sequestration
-
8/13/2019 Congenital Lung Malformations
35/115
Pulmonary sequestration
o Children present with recurrent respiratory problems in the
same
anatomic location.
o Associated anomalies include diaphragmatic hernia and
eventration.
o Patients may have exercise intolerance if they have large
systemic
arterial venous shunts.
o The extrathoracic variety can be associated with hydrops
fetalis or
increased lymphatic transudate in the thorax.
-
8/13/2019 Congenital Lung Malformations
36/115
Pulmonary sequestration
o About 50% of pulmonary sequestration cases are intralobar, and
60% of
intralobar cases occur in the left lower lobe with equal sex
distributions.
o Patients with intralobar sequestration usually present
late.
o They may have a chronic cough, recurrent pneumonias, or poor
exercise
performance.
o Systemic arterial flow may produce a murmur, and shunts may
lead to
congestive cardiac failure.
o Squamous cell carcinoma, adenocarcinoma, and
rhabdomyosarcoma
may arise in the sequestration.
-
8/13/2019 Congenital Lung Malformations
37/115
Pulmonary sequestration
o Approximately 95% of extrapulmonary cases are left sided.
o Most extrapulmonary cases are detected in infancy, with boys
affected 4
times more than girls.
o Infants usually present with a chronic cough and recurrent
chest
infections.
o Radiographs may reveal signs of consolidation.
o If communication with the gut is present, children may present
with
vomiting, failure to thrive due to poor oral intake, and
abdominal pain.
-
8/13/2019 Congenital Lung Malformations
38/115
Scimitar syndrome
o The constant feature of this
syndrome is partial or total
anomalous pulmonary venous
return to the inferior vena cava.
o This abnormal vein on the chest
radiography creates a gentle
curve bulging into the right
chest from the mediastinum that
some believe resembles the
Turkish sword called a scimitar.Fig. 15.Scimitar syndrome.
-
8/13/2019 Congenital Lung Malformations
39/115
Scimitar syndrome
o Other features of the syndrome are variable and may
include
dextrocardia, hypoplasia of the right lung and/or pulmonary
artery,malformation of the bronchi, and systemic arterial supply to
the right
lung.
o The clinical features vary according to age. Infants almost
always
present with congestive heart failure and severe pulmonary
hypertension. Adults are generally asymptomatic.
Fig. 16. Chest x-ray of a five-year-old girl with Scimitar
syndrome. The heart (blue outline) is shiftedinto the right half of
the chest, and the anomalous pulmonary venous return (red) has a
shape reminiscentof a Scimitar.
-
8/13/2019 Congenital Lung Malformations
40/115
Scimitar syndrome
Fig. 17. Scimitar syndrome (MRI).
-
8/13/2019 Congenital Lung Malformations
41/115
Lung hamartoma
o Hamartomas are lung nodules contain cartilage, respiratory
epithelium,
and collagen.
o They may be in the lung tissue or the bronchial lumen.
AA BA
Fig. 18. Pulmonary hamartoma. (A)Chest CT scan shows a
heterogeneous, sharply marginated lesionwith small focal areas of
calcification and fat. These findings are typical features of
hamartoma. (B)The chest radiograph shows a solitary pulmonary
nodule in the left lung apex. Close inspection of thisnodule shows
small foci of increased attenuation within the nodule, consistent
with calcium. Thesefindings are typical features of hamartoma.
-
8/13/2019 Congenital Lung Malformations
42/115
-
8/13/2019 Congenital Lung Malformations
43/115
Fig. 19. MRI angiography using MIP (Maximum IntensityProjection)
reconstruction shows the presence of multiple,bilateral
arteriovenous malformations of pulmonary vessels
Fig. 19. MRI angiography using MIP (Maximum IntensityProjection)
reconstruction shows the presence of multiple,bilateral
arteriovenous malformations of pulmonary vessels
Pulmonary arteriovenous malformation
o Pulmonary arteriovenous
malformations are abnormal
communications between the
pulmonary arterial and
venous systems without
interposed capillaries (Fig.
19).
Fig. 19. MRI angiography using MIP (Maximum IntensityProjection)
reconstruction shows the presence of multiple,bilateral
arteriovenous malformations of pulmonary vessels
Fig. 19. MRI angiography using MIP (Maximum IntensityProjection)
reconstruction shows the presence of multiple,bilateral
arteriovenous malformations of pulmonary vessels.
-
8/13/2019 Congenital Lung Malformations
44/115
Pulmonary arteriovenous malformation
o Arteriovenous malformations with a systemic arterial supply
are
unusual in the lung.
o As with arteriovenous malformations elsewhere, they can lead
to high-
output cardiac failure.
o Symptoms are unusual in childhood.
o However, by adulthood, 50% of patients have at least
exertional
dyspnea.
o Hemoptysis is most common in patients who also have
cutaneous
telangiectasis.
o A continuous bruit is often heard over the lesion.
-
8/13/2019 Congenital Lung Malformations
45/115
Pulmonary arteriovenous malformation
o The fistulas are usually seen as
well-defined opacities on chest
radiography, and are multiple in
as many as 50% of patients (Fig.
20) and bilateral in 10%.
Fig. 20. Chest X-ray. Pulmonary arteriovenousmalformation.
-
8/13/2019 Congenital Lung Malformations
46/115
Pulmonary arteriovenous malformation
o Most of the fistulas are subpleural, and more often occur in
the lower
lobes.
o CT findings are usually diagnostic (Fig. 21).
Fig. 21. Right intrahilar pulmonary
arteriovenousmalformation.
-
8/13/2019 Congenital Lung Malformations
47/115
Pulmonary arteriovenous malformation
o Complications include bleeding, infection, and embolus.
o Patients with cutaneous telangiectasis are likely to have
Rendu-Osler-
Weber disease (also known as hereditary hemorrhagic
telangiectasia a
genetic disorder that leads to abnormal blood vessel formation
in
the skin, mucous membranes, and often in organs such asthe
lungs, liver, and brain).
o They are likely to have multiple pulmonary arteriovenous
malformations and progressive symptoms.
-
8/13/2019 Congenital Lung Malformations
48/115
Pulmonary arteriovenous malformation
o Treatment is resection.
o If this is not possible, the lesions can be embolized (Movie
1).
Movie 1. Right pulmonary arteriovenousembolization.
-
8/13/2019 Congenital Lung Malformations
49/115
Fig. 22. Alveolar capillary dysplasia: characteristic histologic
features of ACD/MPV: thickened alveolarseptae with scarce dilated
pulmonary capillaries located away from the alveolar epithelium,
with absence ofthe usual alveolar-capillary barrier ( ); medial
hypertrophy of small pulmonary arteries and muscularization
of distal arterioles (); congested pulmonary veins
malpositioned, adjacent to pulmonary arteries in the
sameadventitial sheath (*); lymphangiectasis not present.
Fig. 22. Alveolar capillary dysplasia: characteristic histologic
features of ACD/MPV: thickened alveolarseptae with scarce dilated
pulmonary capillaries located away from the alveolar epithelium,
with absence ofthe usual alveolar-capillary barrier ( ); medial
hypertrophy of small pulmonary arteries and muscularization
of distal arterioles (); congested pulmonary veins
malpositioned, adjacent to pulmonary arteries in the
sameadventitial sheath (*); lymphangiectasis not present.
Alveolar capillary dysplasia
o In alveolar capillary dysplasia, a fatal condition, the distal
arteriolar
blood supply is reduced, the pulmonary veins are misaligned, and
the
connective tissue between the alveolar epithelium and the
capillary
endothelium is increased (Fig. 22).
A B
Fig. 22. Alveolar capillary dysplasia: characteristic histologic
features of ACD/MPV: thickened alveolarseptae with scarce dilated
pulmonary capillaries located away from the alveolar epithelium,
with absence ofthe usual alveolar-capillary barrier ( ); medial
hypertrophy of small pulmonary arteries and muscularization
of distal arterioles (); congested pulmonary veins
malpositioned, adjacent to pulmonary arteries in the
sameadventitial sheath (*); lymphangiectasis not present.
Fig. 22. Alveolar capillary dysplasia: characteristic histologic
features of ACD/MPV: thickened alveolarseptae with scarce dilated
pulmonary capillaries located away from the alveolar epithelium,
with absence ofthe usual alveolar-capillary barrier ( ); medial
hypertrophy of small pulmonary arteries and muscularization
of distal arterioles (); congested pulmonary veins
malpositioned, adjacent to pulmonary arteries in the
sameadventitial sheath (*); lymphangiectasis not present.
Fig. 22. Alveolar capillary dysplasia: characteristic histologic
features of ACD/MPV: thickened alveolarseptae with scarce dilated
pulmonary capillaries located away from the alveolar epithelium,
with absence ofthe usual alveolar-capillary barrier ( ); medial
hypertrophy of small pulmonary arteries and muscularization
of distal arterioles (); congested pulmonary veins
malpositioned, adjacent to pulmonary arteries in the
sameadventitial sheath (*); lymphangiectasis not present.
Fig. 22. Alveolar capillary dysplasia: characteristic histologic
features of ACD/MPV: thickened alveolarseptae with scarce dilated
pulmonary capillaries located away from the alveolar epithelium,
with absence ofthe usual alveolar-capillary barrier ( ); medial
hypertrophy of small pulmonary arteries and muscularization
of distal arterioles (); congested pulmonary veins
malpositioned, adjacent to pulmonary arteries in the
sameadventitial sheath (*); lymphangiectasis not present.
-
8/13/2019 Congenital Lung Malformations
50/115
Alveolar capillary dysplasia
o The alveolar circulation is impaired, and the response to
nitric oxide is
poor.
o Affected babies do well with venoarterial extracorporeal
membrane
oxygenation (ECMO), but they cannot be weaned from it.
o The clinical presentation of alveolar capillary dysplasia is
that ofpersistent pulmonary hypertension of the newborn.
o Hypoxemia leads to arteriolar muscular hypertrophy.
o Patients may have associated anomalies in the heart or urinary
system.
o Open lung biopsy and cardiac catheterization are suggested
as
diagnostic tools to look for or exclude pulmonary capillary
blush.
-
8/13/2019 Congenital Lung Malformations
51/115
Pulmonary lymphangiectasis
o Pulmonary lymphangiectasis is a rare disorder in which the
normal
pulmonary lymphatics are dilated.
o It may be associated with congenital heart disease in which
the
pulmonary venous pressure is elevated.
o Pulmonary lymphangiectasis can also be observed
withlymphangiomatosis, in which proliferation of the lymphatic
tissue and
channels occurs.
o The disease can also be part of a syndrome of lymphangiomas in
many
organs; it is sometimes associated with vanishing bones
(Gorhams
disease).
o Pulmonary lymphangiectasis is congenital, but symptoms of
respiratory
insufficiency usually do not appear until adulthood.
Pulmonary lymphangiectasis
-
8/13/2019 Congenital Lung Malformations
52/115
Pulmonary lymphangiectasis
(History case)
o A female infant was born at 40 weeks and 3 days of gestation,
weighing
2970 g.
o The Apgar scores were 8, 10, and 10 at 1, 5, and 10
minutes,
respectively.
o Within one hour after birth, severe respiratory distress with
profoundcyanosis developed while the infant was breathing room air,
and
intubation and mechanical ventilation were required.
Pulmonary lymphangiectasis
-
8/13/2019 Congenital Lung Malformations
53/115
Pulmonary lymphangiectasis
(History case)
o An initial chest radiograph showed normal lung volumes with
diffuse,
bilateral nodular changes, and a subsequent chest radiograph
obtained
on the 17th day of life showed that these changes had become
more
prominent (Fig. 23).
Fig. 23. Chest X-ray - pulmonary lymphangiectasia
Pulmonary lymphangiectasis
-
8/13/2019 Congenital Lung Malformations
54/115
Pulmonary lymphangiectasis
(History case)
o Surfactant and antibiotics were administered.
o Lung compliance remained poor, and high-frequency
oscillatory
ventilation was begun.
o Congenital heart disease was ruled out, and cultures of blood
and
tracheal aspirates were unrevealing.
o After surfactant protein B deficiency was ruled out, an
open-lung biopsy
was performed, on the 18th day of life.
Pulmonary lymphangiectasis
-
8/13/2019 Congenital Lung Malformations
55/115
Pulmonary lymphangiectasis
(History case)
o On gross examination, the lung had an irregular surface with
scattered
nodular changes (Fig. 24).
Fig. 24. Pulmonary lymphangiectasis. Intraoperative view.
Pulmonary lymphangiectasis
-
8/13/2019 Congenital Lung Malformations
56/115
Pulmonary lymphangiectasis
(History case)
o On microscopical examination, there was subpleural and septal
cystic
lymphangiectasia (L, Fig. 25; hematoxylin and eosin, 150). A
denotes artery. These findings are consistent with a diagnosis
of
congenital pulmonary lymphangiectasia, which is a uniformly
fatal
disease when it manifests in the newborn period. The infant died
on the
20th day of life.
Fig. 25. Pulmonary lymphangiectasis.Hematoxylin and eosin,
150.
-
8/13/2019 Congenital Lung Malformations
57/115
Congenital lobar emphysema
o Massive overinflation of one or more lung lobes occurs
postnatally in
congenital lobar emphysema (Fig. 26).
Fig. 26. Congenital lobar emphysema
-
8/13/2019 Congenital Lung Malformations
58/115
Congenital lobar emphysema
o Causes are obscure in 50%. Other causes include intrinsic
absence or
abnormality (bronchomalacia) of cartilaginous rings or
external
compression by a large pulmonary artery. (Compression of the
cartilage
usually leads to malacia.)
o Hyperexpansion of a pulmonary lobe is present after birth
when, with
negative inspiratory pressure, air can enter the lung.
o However, the air cannot exit easily because positive pressure
causes the
softened airway to collapse.
o The remaining normal lung is then compressed.
-
8/13/2019 Congenital Lung Malformations
59/115
Congenital lobar emphysema
o Congenital lobar emphysema primarily involves the upper
lobes.
o The left upper lobe is involved in 41% of patients; the right
middle lobe,
in 34%; and the right upper lobe, in 21%.
o Involvement of the lower lobes is rare, occurring in fewer
than 5% of
patients.
o Congenital cardiac anomalies may be present in as many as 10%
of
patients.
o Lesions most commonly occur in whites, in male individuals
(male-to-
female ratio, 3:1), and in young infants.
-
8/13/2019 Congenital Lung Malformations
60/115
Congenital lobar emphysema
o Most patients with congenital lobar emphysema present before 6
months
of life.
o Neonates may present with mild-to-moderate respiratory
distress.
o Mediastinal shift may be present, with hyperresonance and
decreased
breath sounds on the involved side.
o Infants present with cough, wheezing, respiratory distress,
and cyanosis.
o Older children may present with recurrent chest
infections.
o On images obtained in neonates, the affected lobe may be
slightly
opacified, rather than lucent, because it is still filled with
fluid.
o Associated cardiac anomalies occur in as many as 10% of
patients. See
the images below.
-
8/13/2019 Congenital Lung Malformations
61/115
Congenital lobar emphysema
Fig. 27. Chest X-ray. (front and lateral views) Congenital lobar
emphysema on the right side of the chest in aneonate. Film shows
marked lucency and hyperexpansion in the middle lobe of the right
lung; this finding isconsistent with lobar emphysema. The
possibility of tension pneumothorax is unlikely because lung
markingsare seen in this region, with splaying of the pulmonary
vessels. Compressive atelectasis is present in the leftupper and
right lower areas of the lungs. The mediastinum and heart are
shifted to the left. The osseousstructures are intact.
-
8/13/2019 Congenital Lung Malformations
62/115
Congenital lobar emphysema
Fig. 28. Same patient as in the previous 2 images. After
surgery, the left lungis expanded. A thoracotomy tube is on the
right, with a small right-sidedpneumothorax.
-
8/13/2019 Congenital Lung Malformations
63/115
Congenital cystic adenomatoid malformation
o Congenital cystic adenomatoid malformation (CCAM) or
congenital
pulmonary airway malformation (CPAM) lately is a defect in
thedevelopment of the terminal bronchioles.
o A hamartomatous proliferation of cysts occurs and
resembles
bronchioles (airways without cartilage).
Fig. 29. CCAM on chest radiograph in a newborn.Large cystic
changes in the left lung, leading to amediastinal shift to the
right due to their mass effect.
Fig. 30. Contrast enhanced computerizedtomography of the chest
of the patient withcongenital cystic adenomatoid
malformation(CCAM)
-
8/13/2019 Congenital Lung Malformations
64/115
Congenital cystic adenomatoid malformation
o Adenomatoid malformation results when the terminal
bronchiolar
component of the advancing endodermal lung bud
proliferateshaphazardly because of disruption of humoral factors
from the
surrounding mesenchyme.
o Apoptosis in the advancing lung bud is decreased.
o Glial cellderived neurotrophic factor is a growth factor that
isabnormally expressed in the epithelial cells of the cystic
adenomatoid
malformation.
o Cystic adenomatoid malformations usually appear before 7
weeks'
gestation but can occur in the mid stage of lung development.o
The growth is thought to plateau at 28 weeks' gestation.
C i i i f i
-
8/13/2019 Congenital Lung Malformations
65/115
Congenital cystic adenomatoid malformation
o Communication with the normal airways can lead to
overinflation and
compression of the surrounding lung tissue.
o The larger the sonographic volume of cystic adenomatoid
malformation
in relation to head circumference, the greater the chance for
developing
hydrops because of more severe central venous compression.
-
8/13/2019 Congenital Lung Malformations
66/115
-
8/13/2019 Congenital Lung Malformations
67/115
C it l ti d t id lf ti
-
8/13/2019 Congenital Lung Malformations
68/115
Congenital cystic adenomatoid malformation
o Polyhydramnios may be present if the cystic adenomatoid
malformation
presses on the esophagus.
o Pressure on the heart and large vessels may lead to hydrops
fetalis.
o In approximately 60% of patients, cystic adenomatoid
malformation
manifests soon after the neonatal period.
o It results in recurrent infections because the mucociliary
clearance is
poor.
o Malignancy can occur in the cystic adenomatoid
malformation
(pulmonary blastoma, rhabdomyosarcoma, and bronchoalveolar
carcinoma). See the images below.
C it l ti d t id lf ti
-
8/13/2019 Congenital Lung Malformations
69/115
Congenital cystic adenomatoid malformation
Fig. 31. Cystic adenomatoid malformation.
C it l ti d t id lf ti
-
8/13/2019 Congenital Lung Malformations
70/115
Congenital cystic adenomatoid malformation
Fig. 32. Initial radiograph in a patient with congenital
cysticadenomatoid malformation on the first day of life with opaque
lungsand a suggestion that the right lung is slightly more
voluminous than
the left lung.
C it l ti d t id lf ti
-
8/13/2019 Congenital Lung Malformations
71/115
Congenital cystic adenomatoid malformation
Fig. 33. Radiograph obtained in the same patient as in the
previous image onthe second day of life shows that the physiologic
fluid is resorbed andreplaced with an air-containing cystic area
occupying the right upper lung.
Fig. 33. Radiograph obtained in the same patient as in the
previous image onthe second day of life shows that the physiologic
fluid is resorbed andreplaced with an air-containing cystic area
occupying the right upper lung.
P l l l l b
-
8/13/2019 Congenital Lung Malformations
72/115
Polyalveolar lobe
o In a polyalveolar lobe, the number of alveoli increased to
more than 3
times normal.
o The alveoli are counted microscopically in random lung
sections.
o When extra lung fluid is retained, respiratory distress may
occur in the
first days of life.o This generally benign anomaly may be
associated with some cases of
congenital lobar emphysema.
-
8/13/2019 Congenital Lung Malformations
73/115
INDICATIONS
Bronchogenic cyst
-
8/13/2019 Congenital Lung Malformations
74/115
Bronchogenic cyst
o Resection is recommended because of the potential for
infection,
hemorrhage, and respiratory compromise.
o Resection is especially important in the peripheral lesions,
which are
usually multiple.
o These can frequently be excised thoracoscopically because they
seldomhave a major blood supply.
Pulmonary agenesis and pulmonary hypoplasia
-
8/13/2019 Congenital Lung Malformations
75/115
Pulmonary agenesis and pulmonary hypoplasia
o Patients with pulmonary agenesis and pulmonary hypoplasia seem
to
have one of 3 presentations.
o The first group consists of patients with insufficient lung
tissuewho
may have received mechanical ventilation for some time.
o However, ventilator-induced lung injury results in slow
decompensationand death.
o The second group of patients is identified serendipitously
when chest
radiography is obtained to assess a minor complaint.
o These patients require no intervention.
Pulmonary agenesis and pulmonary hypoplasia
-
8/13/2019 Congenital Lung Malformations
76/115
Pulmonary agenesis and pulmonary hypoplasia
o The third group does not have respiratory distress requiring
mechanical
ventilation, but they have respiratory limitations to activity
or kinking of
the airway with shift of the lung to the contralateral side of
the chest.
o In addition to the aplasia or hypoplasia, congenital narrowing
of the
upper airway also affects many patients.
Pulmonary sequestration
-
8/13/2019 Congenital Lung Malformations
77/115
Pulmonary sequestration
o Resection is recommended, even in asymptomatic patients, to
prevent
infection, hemorrhage, shunting from arteriovenous anastomoses,
or
compression of normal lung mass leading to respiratory
distress.
o Lobectomy can usually be performed.
o For patients with intralobar sequestration, segmentectomy may
suffice.o Segmentectomy is relatively difficult, but preserves
additional
functioning lung tissue.
Pulmonary sequestration
-
8/13/2019 Congenital Lung Malformations
78/115
Pulmonary sequestration
o Resection is recommended, even in asymptomatic patients, to
prevent
infection, hemorrhage, shunting from arteriovenous anastomoses,
or
compression of normal lung mass leading to respiratory
distress.
o Lobectomy can usually be performed.
o For patients with intralobar sequestration, segmentectomy may
suffice.o Segmentectomy is relatively difficult, but preserves
additional
functioning lung tissue.
Scimitar syndrome
-
8/13/2019 Congenital Lung Malformations
79/115
Scimitar syndrome
o When symptoms of scimitar syndrome are related to
anomalous
pulmonary venous return, this return can be redirected
surgically.
o Symptoms are often related to the bronchial abnormalities and
chronic
infection.
o In these cases, pneumonectomy is indicated.
Hamartoma and
-
8/13/2019 Congenital Lung Malformations
80/115
pulmonary arteriovenous malformation
o Resection is usually performed for diagnosis when a lesion is
noted on
chest radiography.
o Symptoms of airway obstruction or high cardiac output are
occasionally
indications for surgery as well.
Congenital lobar emphysema
-
8/13/2019 Congenital Lung Malformations
81/115
Congenital lobar emphysema
o Progressive airtrapping leads to respiratory and circulatory
compromise
in infancy.
o Emergency lobectomy may be required.
Congenital lobar emphysema
-
8/13/2019 Congenital Lung Malformations
82/115
Congenital lobar emphysema
o A patient with respiratory distress whose chest radiograph
reveals a
hyperlucency on one side and mediastinal shift usually has a
tension
pneumothorax. However, one must consider congenital lobar
emphysema (CLE), especially in the newborn.
Fig. 34. Bilateral pneumotorax in anewborn.
Fig. 35. Congenital lobar emphysema in a newborn.
Congenital lobar emphysema
-
8/13/2019 Congenital Lung Malformations
83/115
Congenital lobar emphysema
o The diagnosis can usually be determined by looking at the
edges of the
hyperlucent area. In pneumothorax, the edges are convex and
outline the
chest wall, whereas in congenital lobar emphysema, they are
concave
and outline the cystic structure of an overexpanded lobe.
Fig. 34. Bilateral pneumotorax in anewborn.
Fig. 35. Congenital lobar emphysema in a newborn.
Congenital lobar emphysema
-
8/13/2019 Congenital Lung Malformations
84/115
Congenital lobar emphysema
Fig. 36.Bilateral pneumotorax. Fig. 37.Congenital lobar
emphysema of the upperlobe of the left lung.
Congenital lobar emphysema
-
8/13/2019 Congenital Lung Malformations
85/115
Congenital lobar emphysema
Fig. 39.Right sided pneumotorax.Fig. 38.Congenital lobar
emphysema of the upper lobeof the left lung.
Cystic adenomatoid malformation
-
8/13/2019 Congenital Lung Malformations
86/115
Cystic adenomatoid malformation
o In congenital cystic adenomatoid malformation (CAM), resection
of
even asymptomatic masses is recommended because of the risk
for
infection, hemorrhage, acute respiratory compromise (which may
occur
anytime), and neoplastic transformation.
o This disease is usually segmental; however, as noted for
sequestration,
lobectomy may reduce morbidity.
-
8/13/2019 Congenital Lung Malformations
87/115
WORKUP
Laboratory Studies
-
8/13/2019 Congenital Lung Malformations
88/115
Laboratory Studies
o Hemoglobin testing is always valuable in respiratory illness
because the
result is an important factor in oxygen delivery and in planning
surgery,
which often involves major vessels.
Renal function tests to measure BUN (Blood Urea Nitrogen),
serum
creatinine, and electrolyte levels are important because of the
frequent
association of renal anomalies with pulmonary anomalies
(usually
pulmonary hypoplasia).
Imaging Studies
-
8/13/2019 Congenital Lung Malformations
89/115
(Chest radiography)
Bronchogenic cysts: Bronchogenic
cysts are usually fluid-filled lesions
and are well circumscribed in the
mediastinum.
Solid masses may be difficult to
differentiate from fluid.
Intrapulmonic cysts appear as solitary
nodules unless they contain air.
Large cysts may be difficult to
differentiate from macrocystic cystic
adenomatoid malformation (CAM).
Fig. 40. Mediastinal bronchogenic cyst.
Imaging Studies
-
8/13/2019 Congenital Lung Malformations
90/115
(Chest radiography)
Pulmonary hypoplasia: In pulmonary
hypoplasia, a mediastinal shift to the
side of a homogenous density may be
depicted, with compensatory
herniation of the uninvolved lung.
The associated anomalies (cardiac,
skeletal, gut) may be seen.
Fig. 41. Chest radiograph shows diffuse haziness ofthe right
hemithorax (arrow), slight deviation of thetrachea and heart to the
right, and poor differentiationof the right heart border.
Imaging Studies
(
-
8/13/2019 Congenital Lung Malformations
91/115
(Chest radiography)
o Pulmonary sequestration: In pulmonary sequestration, an opaque
or
cystic lesion is seen, depending on the presence of
infection.
Fig. 42. Chest radiograph. The PA view demonstrates a left
sidedtriangular density of the medial left lung base. On the
lateral view, thetriangular density is seen posteriorly over the
left lung base.
Imaging Studies
(
-
8/13/2019 Congenital Lung Malformations
92/115
(Chest radiography)
o Congenital lobar emphysema (CLE):In congenital lobar
emphysema,
the involved lobe crossing the midline and the compressed normal
lung
can be seen.
Fig. 43. Congenital lobar emphysema.
Imaging Studies
(
-
8/13/2019 Congenital Lung Malformations
93/115
(Chest radiography)
o This appearance does not change during expiration or in the
decubitus
position.
o Vascularity of the involved site is attenuated.
Fig. 43. Congenital lobar emphysema.
Imaging Studies
(
-
8/13/2019 Congenital Lung Malformations
94/115
(Chest radiography)
o The intercostal spaces in the involved site appear widened,
and the
hemidiaphragm is flattened. Lucent, anteriorly herniated lung
pushes the
lung posteriorly, as seen on the lateral view.
Fig. 43. Congenital lobar emphysema.
Imaging Studies
(C i )
-
8/13/2019 Congenital Lung Malformations
95/115
(Chest radiography)
o The lesion must be differentiated from contralateral lung
hypoplasia and
ipsilateral pneumothorax.
Fig. 43. Congenital lobar emphysema.
Imaging Studies
(Ch di h )
-
8/13/2019 Congenital Lung Malformations
96/115
(Chest radiography)
o The lesion must be differentiated from contralateral lung
hypoplasia and
ipsilateral pneumothorax.
Fig. 44. Left lung hypoplasia. Fig. 45. Left sided
pneumothorax.
-
8/13/2019 Congenital Lung Malformations
97/115
Imaging Studies
(Ch t di h )
-
8/13/2019 Congenital Lung Malformations
98/115
(Chest radiography)
o In a newborn, the lung fluid may not have been absorbed, and
the mass may
appear fluid filled and homogenous.
Fig. 46. Congenital pulmonary airway malformation.
Imaging Studies
(Ch t di h )
-
8/13/2019 Congenital Lung Malformations
99/115
(Chest radiography)
o In an older child, pneumatoceles may be confused with cystic
adenomatoid
malformation.
o Pneumatoceles are postinfectious pulmonary cysts.
Fig. 46. Congenital pulmonary airwaymalformation.
Fig. 47. Chest X-ray with large, expanding,multicystic
pneumatocele associated with
Respiratory Syncytial Virus infection.
Imaging Studies
(Ch t di h )
-
8/13/2019 Congenital Lung Malformations
100/115
(Chest radiography)
o They occur after Staphylococcus aureus infection.
o However, they are unlikely to recur in the same area of the
lung as where
cystic adenomatoid malformation occurs.
Fig. 46. Congenital pulmonary airwaymalformation.
Fig. 47. Chest X-ray with large, expanding,multicystic
pneumatocele associated with
Respiratory Syncytial Virus infection.
Imaging Studies
(Ch t di h )
-
8/13/2019 Congenital Lung Malformations
101/115
(Chest radiography)
o Bronchogenic cysts are central or mediastinal (relatively
early embryologic
origin) and peripheral or intrapulmonary (late origin).
o The latter are rare (15%) and tend to be multiple.
Fig. 46. Congenital pulmonary airwaymalformation.
Fig. 48. Chest X-ray revealing bronchogeniccyst in the posterior
right middle lobe.
-
8/13/2019 Congenital Lung Malformations
102/115
Imaging Studies
(Ch t CT i )
-
8/13/2019 Congenital Lung Malformations
103/115
(Chest CT scanning)
o Bronchogenic cysts:In patients with bronchogenic cysts, CT
findings are
characteristic.
o The lesions are sharply marginated and nonenhancing. If the
lesions are
seen as soft-tissue attenuation instead of water attenuation,
differentiating
from lymph nodes may be difficult.
Fig. 50.Chest CT scan. Bronchogenic cyst.
Imaging Studies
(Chest CT scanning)
-
8/13/2019 Congenital Lung Malformations
104/115
(Chest CT scanning)
o Pulmonary hypoplasia: In lung hypoplasia, loss of lung volume
and
associated anomalies can be seen.
Fig. 51.Right lung hypoplasia. Chest CT scan showsherniation of
left lung to right side with narrow right main
bronchus and shift of heart to right side.
Imaging Studies
(Chest CT scanning)
-
8/13/2019 Congenital Lung Malformations
105/115
(Chest CT scanning)
Pulmonary sequestration: In
pulmonary sequestration, the
findings may be only an unusual
solid attenuation. Therefore, CT
may have little to add tosonographic and plain
radiographic results unless the
anomalous vascular supply can
be visualized with vascular
contrast enhancement.Fig. 52. CT with IV contrast of the thorax
showing an IntralobarBronchopulmonary Sequestration. The yellow
arrow in framesA and B point to a hyperdense region in the left
lower lobe of thelung with small cystic lesions containing air
within it. The redarrows in frames C and D show a contrast enhanced
vesselarising from the aorta and supplying the area of hyperdensity
in
the lung.
-
8/13/2019 Congenital Lung Malformations
106/115
-
8/13/2019 Congenital Lung Malformations
107/115
Imaging Studies
(MRI)
-
8/13/2019 Congenital Lung Malformations
108/115
(MRI)
o MRI: MRI is particularly useful
when delineation of blood vessels
is important. It is the study of
choice in difficult cases of
bronchogenic cysts.
o The cysts appear bright on T2-
weighted images and do not
enhance after the administration of
gadolinium-based contrast
material.Fig. 55.MRI in the supine (A, B) and right
lateraldecubitus (C, D) positions. Bronchogenic cystmasquerading as
pericarditis.
Imaging Studies
(MRI)
-
8/13/2019 Congenital Lung Malformations
109/115
(MRI)
o Pulmonary sequestration: MRI
and magnetic resonance
angiography (MRA) can be
performed to identify pulmonary
pathology, and aberrant systemicvessels. MRI and MRA have
been
suggested as the diagnostic
procedures of choice for
evaluating sequestration of the
lung.
Fig. 56. MR-Angiography showing an aberrant vesselfrom the
celiac trunk (white arrow) to a lung sequesterin the right lower
lobe.
Imaging Studies
(MRI)
-
8/13/2019 Congenital Lung Malformations
110/115
(MRI)
o Cystic adenomatoid
malformation: In cases of
hydrops fetalis in a fetus with a
prenatal, MRI may be beneficial
for planning surgery. Cysts largerthan 3 mm are depicted as
areas of
increased signal intensity on T2-
weighted images.
Fig. 57. Congenital cystic adenomatoid malformation. Fetus at22
weeks gestation. a, b and c Fetal sagittal, coronal, andaxial
single-shot fast spin-echo MR images of the fetal chestshow a
complex hyperintense lesion with cysts inside in theright lung
(arrows). CT after birth dshows the lesion, which isproportionally
smaller than in the MR images
-
8/13/2019 Congenital Lung Malformations
111/115
Imaging Studies
(Prenatal ultrasonography)
-
8/13/2019 Congenital Lung Malformations
112/115
(Prenatal ultrasonography)
o Pulmonary hypoplasia: In lung hypoplasia, renal
malformations,
oligohydramnios, decreased fetal movements in neuromuscular
disease,
dysmorphisms in trisomies, and skeletal dysplasias may be
identified. The
thoracic-to-abdomen ratio and lung area are useful parameters.
Pulmonary
arterial flow can be measured by using Doppler studies.
Fig. 58. Diaphragmatic Hernia. A. Transverse image through the
chest shows the stomach (S) and a largevolume of small bowel
(straight arrows) occupying the left chest and displacing the heart
(curved arrow) intothe right thorax. No lung is visible, indicating
that severe pulmonary hypoplasiais very likely. B. In anotherfetus,
a moderate volume of lung (L) is visible in the right thorax even
though the heart (long arrow) isdisplaced rightward by the
herniation of bowel (short arrows) and stomach (S) into the left
thorax.
Imaging Studies
(Prenatal ultrasonography)
-
8/13/2019 Congenital Lung Malformations
113/115
(Prenatal ultrasonography)
o Congenital lobar emphysema:In congenital lobar emphysema, a
large fluid-
filled lobe may be seen.
Fig. 59. Sagittal section of the thorax showing enlargement of
the leftlung. The right lung has normal echogenicity.
Imaging Studies
(Prenatal ultrasonography)
-
8/13/2019 Congenital Lung Malformations
114/115
(Prenatal ultrasonography)
o Cystic adenomatoid malformation: In cystic adenomatoid
malformation, a
unilateral cystic mass is seen. However, the patient's postnatal
clinical course
and chest radiographic findings may be normal, and CT, MRI,
and/or MRA
may be indicated.
Fig. 60. 27th week of gestation. Image shows an axial view
through the area of cysticadenomatoid malformation of the left
fetal lung, type I. Large anechogenic, left-sided lesion(arrow)
displaces the heart to the right.
Imaging Studies
(Isotope ventilation scanning)
-
8/13/2019 Congenital Lung Malformations
115/115
(Isotope ventilation scanning)
o Although specific changes occur on isotope ventilation
scanning, this
modality seldom adds clinically useful information.
o In congenital lobar emphysema, decreased ventilation initially
occurs,
followed by isotope retention.
o Attenuated vascularity results in decreased perfusion.o
Sequestration does not fill up at all during the early pulmonary
phase, but it
does during the systemic (late) phase.
o The value of radionuclide imaging is limited because of the
lack of anatomic
details.