Embed Size (px)
Citation preview

8/4/2019 Congenital Hypothyroidism From Medscape
http://slidepdf.com/reader/full/congenital-hypothyroidism-from-medscape 1/11
Congenital hypothyroidism is inadequate thyroid hormone production in newborn infants.
This can occur because of an anatomic defect in the gland, an inborn error of thyroid
metabolism, or iodine deficiency.
The term endemic cretinism is used to describe clusters of infants with goiter and
hypothyroidism in a defined geographic area. Such areas were discovered to be low in iodine,and the cause of endemic cretinism was determined to be iodine deficiency. In the 1920s,
adequate dietary intake of iodine was found to prevent endemic goiter and cretinism.[1]
Endemic goiter and cretinism are still observed in some areas, such as regions of Bangladesh,
Chad, China, Indonesia, Nepal, Peru, and Zaire.
The term sporadic cretinism was initially used to describe the random occurrence of cretinism
in nonendemic areas. The cause of these abnormalities was identified as nonfunctioning or
absent thyroid glands. This led to replacement of the descriptive term sporadic cretinism with
the etiologic term congenital hypothyroidism. Treatment with thyroid replacement therapy
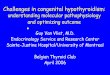
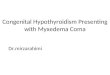
was found to elicit some improvement in these infants (see the images below), although many
remained impaired.
An infant shown a few months after starting thyroid hormone
replacement. Infant a few months after starting thyroid hormone
replacement.
The morbidity from congenital hypothyroidism can be reduced to a minimum by early
diagnosis and treatment.[2]
Although initial preliminary studies were performed using thyroid-
stimulating hormone (TSH) levels in cord blood,[3, 4]
mass screening was made feasible by the
development of radioimmunoassay for TSH and thyroxine (T4) from blood spots on filter
paper, obtained for neonatal screening tests.[5, 6]
Pathophysiology
The thyroid gland develops from the buccopharyngeal cavity between 4 and 10 weeks'
gestation. The thyroid arises from the fourth branchial pouches and ultimately ends up as a
bilobed organ in the neck. Errors in the formation or migration of thyroid tissue can result inthyroid aplasia, dysplasia, or ectopy. By 10-11 weeks' gestation, the fetal thyroid is capable

8/4/2019 Congenital Hypothyroidism From Medscape
http://slidepdf.com/reader/full/congenital-hypothyroidism-from-medscape 2/11
of producing thyroid hormone. By 18-20 weeks' gestation, blood levels of T4 have reached
term levels. The fetal pituitary-thyroid axis is believed to function independently of the
maternal pituitary-thyroid axis.
The thyroid gland uses tyrosine and iodine to manufacture T4 and triiodothyronine (T3).
Iodide is taken into the thyroid follicular cells by an active transport system and then oxidizedto iodine by thyroid peroxidase. Organification occurs when iodine is attached to tyrosine
molecules attached to thyroglobulin, forming monoiodotyrosine (MIT) and diiodotyrosine
(DIT). The coupling of 2 molecules of DIT forms tetraiodothyronine (ie, T4). The coupling
of one molecule of MIT and one molecule of DIT forms T3. Thyroglobulin, with T4 and T3
attached, is stored in the follicular lumen. TSH activates the enzymes needed to cleave T4
and T3 from thyroglobulin. In most situations, T4 is the primary hormone produced by and
released from the thyroid gland.
Inborn errors of thyroid metabolism can result in congenital hypothyroidism in children with
anatomically normal thyroid glands.
T4 is the primary thyronine produced by the thyroid gland. Only 10-40% of circulating T3 is
released from the thyroid gland. The remainder is produced by monodeiodination of T4 in
peripheral tissues. T3 is the primary mediator of the biologic effects of thyroid hormone and
does so by interacting with a specific nuclear receptor. Receptor abnormalities can result in
thyroid hormone resistance.
The major carrier proteins for circulating thyroid hormones are thyroid-binding globulin
(TBG), thyroid-binding prealbumin (TBPA), and albumin. Unbound, or free, T4 accounts for
only about 0.03% of circulating T4 and is the portion that is metabolically active. Infants
born with low levels of TBG, as in congenital TBG deficiency, have low total T4 levels but
are physiologically normal. Familial congenital TBG deficiency can occur as an X-linked
recessive or autosomal recessive condition.
The contributions of maternal thyroid hormone levels to the fetus are thought to be minimal,
but maternal thyroid disease can have a substantial influence on fetal and neonatal thyroid
function. Immunoglobulin G (IgG) autoantibodies, as observed in autoimmune thyroiditis,
can cross the placenta and inhibit thyroid function. Thioamides used to treat maternal
hyperthyroidism can also block fetal thyroid hormone synthesis. Most of these effects are
transient. Radioactive iodine administered to a pregnant woman can ablate the fetus's thyroid
gland permanently.
The importance of thyroid hormone to brain growth and development is demonstrated by
comparing treated and untreated children with congenital hypothyroidism. Thyroid hormone
is necessary for normal brain growth and myelination and for normal neuronal connections.
The most critical period for the effect of thyroid hormone on brain development is the first
few months of life.[2]
Epidemiology

8/4/2019 Congenital Hypothyroidism From Medscape
http://slidepdf.com/reader/full/congenital-hypothyroidism-from-medscape 3/11
Frequency
United States
The incidence of congenital hypothyroidism, as detected through newborn screening, is
approximately 1 per 4000 births.[7]
An increase in the diagnosis of primary congenitalhypothyroidism has been reported in New York .
[8]This trend has also been observed in some
other states,[9]
although not all. Possible explanations include changing demographics of the
birth population, including changes in race, ethnicity, and the incidence of low birth weight.[9]
Changes in laboratory and screening methodology may also play a role in this reported rise in
incidence.[10]
Some infants identified as having primary congenital hypothyroidism may have
transient disease and not permanent congenital hypothyroidism.[11]
Twins
An increased incidence of congenital hypothyroidism is observed in twins.[12, 13, 14]
Twin
births are approximately 12 times as likely to have congenital hypothyroidism assingletons.
[15]Usually, only one twin is hypothyroid, but a common in-utero exposure can
cause hypothyroidism in both.[16]
International
In central Africa, where iodine deficiency occurs along with excess dietary cyanate from
cassava (Manihot esculenta),[17]
as many as 10% of newborns may have both low cord blood
T4 concentration and TSH concentrations over 100 mU/L.[18]
Data from most countries with well-established newborn screening programs indicate an
incidence of congenital hypothyroidism of about 1 per 3000-4000.[19, 20]
Some of the highest
incidences (1 in 1400 to 1 in 2000) have been reported from various locations in the Middle
East.[21]
Although percentages of specific etiologies vary from country to country, ranges are as
follows:
Ectopic thyroid - 25-50%
Thyroid agenesis - 20-50%
Dyshormonogenesis - 4-15%
Hypothalamic-pituitary dysfunction - 10-15%
Mortality/Morbidity
Profound mental retardation is the most serious effect of untreated congenital
hypothyroidism. Severe impairment of linear growth and bone maturation also occurs.
Affected infants whose treatment is delayed can have neurologic problems such as spasticity
and gait abnormalities, dysarthria or mutism, and autistic behavior.

8/4/2019 Congenital Hypothyroidism From Medscape
http://slidepdf.com/reader/full/congenital-hypothyroidism-from-medscape 4/11
Race
Congenital hypothyroidism is observed in all populations. The prevalence at birth is
increased in Hispanics, particularly in Hispanic females, who have a birth prevalence of 1 in
1886 births.[22]
Black infants have about one third the prevalence rate of white infants.
Sex
Most studies of congenital hypothyroidism suggest a female-to-male ratio of a 2:1. Devos et
al showed that much of the discrepancy is accounted for by infants with thyroid ectopy.[23]
The sex ratio for Hispanics is more striking, with a 3:1 female-to-male ratio. The ratio is
lower among Black infants.
Age
By definition, congenital hypothyroidism is present at, or before, birth. Children who develop
primary hypothyroidism when aged 2 years or older have poor growth and slow mentation
but generally do not exhibit the profound and incompletely reversible neurologic
abnormalities observed in untreated congenital hypothyroidism.
History
In regions of iodide deficiency and a known prevalence of endemic cretinism, the diagnosis
may be straightforward.
Infants with congenital hypothyroidism are usually born at term or after term.
Symptoms and signs include the following:
Decreased activity
Large anterior fontanelle
Poor feeding and weight gain
Small stature or poor growth
Jaundice
Decreased stooling or constipation
Hypotonia
Hoarse cry
Often, they are described as "good babies" because they rarely cry and sleep most of the time.
Family history should be carefully reviewed for information about similarly affected infants
or family members with unexplained mental retardation.
Maternal history of a thyroid disorder and mode of treatment, whether before or during
pregnancy, can occasionally provide the etiology of the infant's problem.
Congenital hypothyroidism is more common in infants with birthweights less than 2,000 g or
more than 4,500 g.[24, 13]

8/4/2019 Congenital Hypothyroidism From Medscape
http://slidepdf.com/reader/full/congenital-hypothyroidism-from-medscape 5/11
Congenital hypothyroidism is more common in multiple births, with a low concordance
rate.[1
Physical
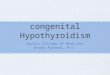
The physical findings of hypothyroidism may or may not be present at birth (see the image
below).
An infant with cretinism. Note the hypotonic posture, coarse
facial features, and umbilical hernia.
Signs include the following:
Coarse facial features
Macroglossia (See the image below.) Note the macroglossia.
Large fontanelles
Umbilical hernia Mottled, cool, and dry skin
Developmental delay
Pallor
Myxedema
Goiter
A small but significant number (3-7%) of infants with congenital hypothyroidism have other
birth defects, mainly atrial and ventricular septal defects.[25]
Newborn screening involves the following:
Infants with congenital hypothyroidism are usually identified within the first 2-3
weeks of life.
These infants should be carefully examined for signs of hypothyroidism, and the
diagnosis should be confirmed by repeat testing.

8/4/2019 Congenital Hypothyroidism From Medscape
http://slidepdf.com/reader/full/congenital-hypothyroidism-from-medscape 6/11
Infants with obvious findings of hypothyroidism (eg, macroglossia, enlarged
fontanelle, hypotonia) at the time of diagnosis have intelligence quotients (IQs) 10-20
points lower than infants without such findings.
Anemia may occur, due to decreased oxygen carrying requirement.
Causes
Endemic cretinism is caused by iodine deficiency, and is occasionally exacerbated by
naturally occurring goitrogens.[26]
Dysgenesis of the thyroid gland, including agenesis (ie, complete absence of thyroid gland)
and ectopy (lingual or sublingual thyroid gland) may be a cause.
Inborn errors of thyroid hormone metabolism include dyshormonogenesis. Most cases are
familial and inherited as autosomal recessive conditions. These may also include thefollowing:
Thyroid-stimulating hormone (TSH) unresponsiveness (ie, TSH receptor
abnormalities)[27]
Impaired ability to uptake iodide
Peroxidase, or organification, defect (ie, inability to convert iodide to iodine)
Pendred syndrome, a familial organification defect associated with congenital
deafness
Thyroglobulin defect (ie, inability to form or degrade thyroglobulin)
Deiodinase defect
Thyroid hormone resistance (ie, thyroid hormone receptor abnormalities) may also be a
cause.[27]
In maternal autoimmune disease, transplacental passage of antibodies cause transient or
permanent hypothyroidism.[28, 29]
Radioactive iodine therapy of pregnant women may cause permanent congenital
hypothyroidism. Iodine in contrast agents or skin disinfectants can cause hypothyroidism or
hyperthyrotropinemia in premature neonates.[30]
TSH or thyrotropin-releasing hormone (TRH) deficiencies are also noted. Hypothyroidismcan also occur in TSH or TRH deficiencies, either as an isolated problem or in conjunction
with other pituitary deficiencies (eg, hypopituitarism). If present with these deficiencies,
hypothyroidism is usually milder and is not associated with the significant neurologic
morbidity observed in primary hypothyroidism.
Diagnostic Considerations
Neonatal hypothyroxinemia
Premature and sick infants have lower levels of thyroid hormone than term infants but usuallydo not have elevated thyroid-stimulating hormone (TSH) levels.
[31, 32]Reference ranges

8/4/2019 Congenital Hypothyroidism From Medscape
http://slidepdf.com/reader/full/congenital-hypothyroidism-from-medscape 7/11
appropriate to the infant's gestational age should be used to avoid confusing this with
hypothyroidism. A meta-analysis suggests that treatment of these neonates with thyroxine is
futile.[33]
Transient neonatal hypothyroidism and hyperthyrotropinemia
Ingestion of excessive amounts of iodine,[34]
or of goitrogens such as lithium,[35]
thioamides,[36, 16]
or amiodarone,[37, 38]
can cause a temporary hypothyroid state. Maternal
antibodies to the TSH receptor can also cause temporary hypothyroidism.[28, 29, 39]
This may
require treatment with levothyroxine for a period of days to months. The etiology of transient
hypothyroidism is often unclear.[40, 11]
Differentials
Beckwith-Wiedemann Syndrome
Goiter Hypopituitarism
Iodine Deficiency
Panhypopituitarism
Thyroxine-Binding Globulin Deficiency
Laboratory Studies
Diagnosis of primary hypothyroidism is confirmed by demonstrating decreased levels of
serum thyroid hormone (total or free T4) and elevated levels of thyroid-stimulating hormone
(TSH).
If maternal antibody – mediated hypothyroidism is suspected, maternal and neonatal
antithyroid antibodies may confirm the diagnosis.[28]
Such antibodies are an uncommon cause
of congenital hypothyroidism.[39]
Low or low-normal serum total T4 levels in the setting of a serum TSH within the reference
range suggests TBG deficiency. This congenital disorder causes no pathologic consequence;
however, it should be recognized to avoid unnecessary thyroid hormone administration.
Thyroid-binding globulin (TBG) deficiency affects 1 individual per 3000 population;
therefore, occurrence is nearly as frequent as that in congenital hypothyroidism. TBG
deficiency results in low serum total T4 levels; however, serum TSH and serum-free T4concentrations are normal. Assessment of the serum TBG concentration, preferably with
simultaneous serum free and serum total T4 concentrations, confirms the diagnosis.
TBG levels can be measured in infants with suspected TBG deficiency. This condition does
not require treatment, but appropriate diagnosis and parental counseling can avoid later
confusion and misdiagnosis.
Routine laboratory testing in patients with TBG deficiency shows a low total T4 level and a
TSH level within the reference range. Free T4 and T3 levels are within the reference range.
Congenital nephrotic syndrome is a rare cause of TBG deficiency or congenital
hypothyroidism.[41, 42]

8/4/2019 Congenital Hypothyroidism From Medscape
http://slidepdf.com/reader/full/congenital-hypothyroidism-from-medscape 8/11
Laboratory results similar to infants with TBG deficiency can be found in infants who have
hypopituitarism or hypothalamic disease, but these children have normal TBG levels.
Imaging Studies
Thyroid scanning (using technetium-99m or iodine-123) may be useful in defining the cause
of hypothyroidism and may aid in genetic counseling. It can aid in distinguishing congenital
hypothyroidism from transient hyperthyrotropinemia.[43, 11]
The absence of radionuclide
uptake suggests sporadic athyreotic hypothyroidism but can also be seen when uptake is
blocked by excess iodide or thyroid receptor blocking antibodies. If no uptake is found on
isotope scanning, thyroid ultrasonography may demonstrate thyroid tissue in these patients.[11,
44]One study of 210 scanned infants stated a preference for using iodine-123 over
pertechnetate.[45]
Thyroid scans can also demonstrate the presence of an ectopic thyroid, such as a lingual or
sublingual gland, which is also sporadic. The presence of a bilobed thyroid in the appropriateposition or a goiter would suggest either an inborn error of thyroid hormone production or
transient hypothyroidism or transient hyperthyrotropinemia. Thyroid scanning is not required
to make or confirm the diagnosis of congenital hypothyroidism, but can provide important
information about the etiology.
Ultrasonography may be a reasonable alternative or addition to scintigraphy but may fail to
reveal some ectopic glands.[46]
A lateral radiograph of the knee may be obtained to look for the distal femoral epiphysis.
This ossification center appears at about 36 weeks' gestation. Its absence in a term or
postterm infant indicates prenatal effects of hypothyroidism, and prior to the introduction of hormone measurements, was used as a diagnostic test for congenital hypothyroidism.
[47]
Early studies of outcome suggested that infants without a distal femoral epiphysis did less
well than those with one, although both groups had results in the normal range.[48]
The author
of this study was later unable to demonstrate an effect of bone age at diagnosis on
outcome.[49]
Another study was unable to demonstrate any difference in outcome in infants
with or without a distal femoral epiphysis.[50]
Other Tests
Neonatal hypothyroidism screening, using TSH levels, has proven helpful in countries with
mild to no iodine deficiency. It has not been found useful in countries with moderate-to-
severe levels of iodine deficiency disorders (IDD) because resources are insufficient to deal
with the problem, and efforts here should be made to supply sufficient iodine to the
population as a whole.
In infants with suspected dyshormonogenesis, radioactive iodine uptake (iodine-123) and
perchlorate flush testing (KCIO2) can be performed to determine the presence of an iodide
uptake or organification defect.
Medical Care

8/4/2019 Congenital Hypothyroidism From Medscape
http://slidepdf.com/reader/full/congenital-hypothyroidism-from-medscape 9/11
The mainstay in the treatment of congenital hypothyroidism is early diagnosis and thyroid
hormone replacement. One study suggested that optimal care includes diagnosis before age
13 days and normalization of thyroid hormone blood levels by age 3 weeks.[51]
Consultations
The treatment of hypothyroidism is straightforward. However, because of the potential for
serious morbidity with inadequate treatment or overtreatment, primary physicians should
consult a pediatric endocrinologist. Appropriate psychological, developmental, and
educational evaluations should also be considered.
Diet
Dietary iodide supplementation in iodine-deficient areas can prevent endemic cretinism but
does not have a major effect on sporadic congenital hypothyroidism. Dietary iodine
deficiency is the most common preventable cause of brain damage worldwide.[52]
Soy-based formulas may decrease the absorption of levothyroxine.[53]
This is not a
contraindication to their use, even in infants with congenital hypothyroidism. Switching an
infant from a milk-based formula to a soy-based formula may increase the dose of thyroid
hormone needed to maintain a euthyroid status.[54]
Activity
Activity should be encouraged in children with congenital hypothyroidism, because activity
should be encouraged in all children.
Medication Summary
Only levothyroxine is recommended for treatment.[55]
It has been established as safe,
effective, inexpensive, easily administered, and easily monitored. No liquid preparations are
commercially available in the United States, but they are licensed elsewhere.[56]
Pharmacies
should be discouraged from dispensing suspensions prepared in-house by crushing tablets
and mixing with various agents. The T4 in these preparations is very difficult to keep in
suspension, and the delivery of drug is inconsistent.
Parents should be provided the hormone in pill form and taught proper administration. The
pills can be crushed in a spoon; dissolved with a small amount of breast milk, water, or other
liquid immediately before administration, and administered to the child with a syringe or
dropper. The pills should not be mixed in a full bottle of formula. Toddlers readily chew the
tablets without problems or complaints.
Optimum dosage regimens and follow-up laboratory monitoring have not yet been
determined.[57, 58, 59]
Initial dosages of 10-15 mcg/kg/d, equivalent to a starting dose of 50 mcg
in many newborns, have been recommended.[60]
Equally good developmental results, but with
higher thyroid-stimulating hormone (TSH) levels, have been reported with half this starting
dose (25 mcg/d).[61]

8/4/2019 Congenital Hypothyroidism From Medscape
http://slidepdf.com/reader/full/congenital-hypothyroidism-from-medscape 10/11
Thyroid Hormones
Class Summary
These agents are administered to supplement thyroid hormone in patients withhypothyroidism. Levothyroxine is the preferred form of thyroid hormone replacement in all
patients with hypothyroidism.[62]
Desiccated thyroid is an obsolete medication made from
pooled animal tissue. Desiccated thyroid should not be used.
View full drug information
Levothyroxine (Levothroid, Levoxyl, Synthroid)
Also known as L-thyroxine, T4, and thyroxine. A thyroid hormone with proven record of
safety, efficacy, and ease of use. In active form, influences growth and maturation of tissues.Involved in normal growth, metabolism, and development.
Further Outpatient Care
Children with congenital hypothyroidism should be monitored clinically and biochemically.
Clinical parameters should include linear growth, weight gain, developmental progression,
and overall well-being.
Laboratory measurements of T4 (total or free T4) and TSH should be repeated 4-6 weeks
after initiation of therapy, then every 1-3 months during the first year of life and every 2-4months during the second and third years. In children aged 3 years and older, the time
interval between measurements may be increased, depending on the reliability of the patient's
caretakers. As dosage changes are made, testing should be more frequent.
Formal developmental and psychoneurological evaluations should be considered in all infants
with congenital hypothyroidism. Such evaluations are especially important in children whose
treatment was delayed or inadequate. As mentioned above, infants diagnosed early who have
detectable signs of hypothyroidism at the time of diagnosis are also at increased risk of
developmental problems. As with any child, school progression should be monitored and
parents encouraged to seek early evaluations and interventions as soon as problems are
recognized.[63]
Unless an anatomic defect of the thyroid was found at diagnosis, reevaluation after
withdrawing treatment should be considered at about age 3 years.[64]
If the child remains
hypothyroid at age 3 years, thyroid hormone replacement and medical monitoring are usually
required for life.
Deterrence/Prevention
Dietary iodide supplementation can prevent endemic goiter and cretinism, but not sporadic
congenital hypothyroidism. Iodization of salt is the usual method, but cooking oil, flour, anddrinking water have also been iodinated for this purpose. Long-acting intramuscular

8/4/2019 Congenital Hypothyroidism From Medscape
http://slidepdf.com/reader/full/congenital-hypothyroidism-from-medscape 11/11
injections of iodized oil (Lipiodol) have been used in some areas, and oral lipiodol[65, 66]
can
also be effective.
Properly administered newborn screening programs have made diagnosis of infants with
congenital hypothyroidism possible within the first 3 weeks of life. With early and adequate
treatment, the sequelae can be eliminated in most and minimized in the rest.
Methods of prenatal diagnosis and treatment are being evaluated.
Prognosis
Early diagnosis and treatment of congenital hypothyroidism prevents severe mental
retardation and other neurologic complications.[67]
Even with early treatment, some children
demonstrate mild delays in areas such as reading comprehension and arithmetic in third
grade. Some of these delays improve by sixth grade. Despite treatment, individuals diagnosed
by newborn screening as a group do not do as well as their euthyroid peers.[68]
As might be expected, infants with delayed bone age at diagnosis or a longer time to
normalize thyroid hormone levels have poorer outcomes. Although continued improvement
in IQ has been documented in treated patients through adolescence, some cognitive problems
may persist. These may include problems in visuospatial, language, and fine motor function.
Defects in memory and attention may also be present.
Patient Education
Parents should be educated regarding their child's disorder, the potential problems associated
with no treatment or inadequate treatment, and the benefits of early and appropriate
treatment. This should include instructions on the proper administration of the medication
and how and when to follow up with the physician. Because learning problems are possible,
even with early diagnosis and treatment, parents should be advised when to seek
psychomotor and educational evaluations and interventions. Early childhood intervention
programs, if available, should be encouraged.
When inborn errors of thyroid hormone production are suspected, genetic counseling should
be provided.
For excellent patient education resources, visit eMedicine's Endocrine System Center. Also,see eMedicine's patient education article Thyroid Problems.