Embed Size (px)
DESCRIPTION
pdf file
Citation preview

Indian Journal of Pediatrics, Volume 76—January, 2009 57
Correspondence and Reprint requests : Dr. P. SyamasundarRao, Professor of Pediatrics, Director, Division of PediatricCardiology, UT-Houston Medical School, 6431 Fannin, MSB3.132, Houston, TX 77030, USA. Phone: 713-500-5738; Fax: 713-500-5751[Received December 15, 2008 ; Accepted December 15, 2008]
Symposium on Advances in Cardiology - I
Diagnosis and Management of Cyanotic CongenitalHeart Disease: Part I
P. Syamasundar Rao
Division of Pediatric Cardiology, Department of Pediatrics University of Texas-Houston Medical School/Children’s Memorial Hermann Hospital, Houston, Texas, USA
ABSTRACT
Most commonly encountered cyanotic cardiac lesions in children, namely, tetralogy of Fallot, transposition of the greatarteries and tricuspid atresia are reviewed. Pathology, pathophysiology, clinical features, non-invasive and invasivelaboratory studies and management are discussed. The clinical and non-invasive laboratory features are sufficientlycharacteristic for making the diagnosis and invasive cardiac catheterization and angiographic studies are not routinelyrequired and are needed either to define features, not clearly defined by non-invasive studies or as a part of catheter-basedintervention. Surgical correction or effective palliation can be undertaken with relatively low risk. However, residual defects,some requiring repeat catheter or surgical intervention, are present in a significant percentage of patients and therefore,continued follow-up after surgery is mandatory. [Indian J Pediatr 2009; 76(1) : 57-70] E-mail: [email protected]
Key words : Cyanotic cardiac lesions; Diagnosis; Invasive cardiac catheterization; Surgical intervention
Congenital heart defect (CHD) may be defined as ananatomic malformation of the heart or great vesselswhich occurs during intrauterine development,irrespective of the age at presentation. Congenital heartdefects may be classified into acyanotic and cyanoticdepending upon whether the patients clinically exhibitcyanosis. The acyanotic defects (obstructive and left-to-right shunt lesions) were discussed in a previousPediatric Cardiology Symposium in this Journal1,2 andwill not be reviewed here. In cyanotic congenital heartdefects systemic venous blood bypasses the pulmonarycirculation and gets shunted across into the left side ofthe heart. Thus, there is systemic arterial desaturation.By definition, cyanotic CHD does not include cyanosisdue to intrapulmonary right-to-left shunting andpulmonary venous desaturation secondary tocongestive heart failure. There are usually multipledefects of the heart causing right-to-left shunt.Obstruction to pulmonary blood flow (for exampletetralogy of Fallot), complete admixture of pulmonaryand systemic venous returns (for example, totalanomalous pulmonary venous return and double-inletleft ventricle) and parallel rather than in-series
circulation (transposition of the great arteries) are thecauses of right-to-left shunts and cyanosis.
The most important of the cyanotic CHDs are whatare called “5 Ts” and are listed in table 1. This reviewconsists of two parts; in the first part the objective is todescribe the important findings in history, physicalexamination and laboratory studies of the mostcommon cyanotic lesions, namely tetralogy of Fallot,transposition of the great arteries and tricuspid atresiaand to discuss the available options in themanagement of these defects. In the second part a briefdiscussion of the other cyanotic CHD will be included.
TABLE 1. Common Cyanotic Congenital Heart Defects (5 Ts)
1. Tetralogy of Fallot2. Transposition of the great arteries3. Tricuspid atresia4. Total anomalous pulmonary venous connection5. Truncus arteriosus
TETRALOGY OF FALLOT
Tetralogy of Fallot (TOF) is the most common cause ofcyanosis beyond one year of age and constitutes 10% ofall congenital heart defects.3 Fallot defined it as aconstellation of four abnormalities to include aventricular septal defect (VSD), pulmonary stenosis(PS), right ventricular hypertrophy and dextropositionof the aorta. The ventricular defect is always large and

P. Syamasundar Rao
58 Indian Journal of Pediatrics, Volume 76—January, 2009
non-restrictive and is located in the membranousseptum in the subaortic region. Pulmonary stenosis isvariable in severity and nature of obstruction. The rightventricular outflow obstruction may be mild resultingin initial left-to-right shunt at ventricular level or it maybe severe causing severe cyanosis even in the neonatalperiod. It may be completely obstructed (pulmonaryatresia) so that there is no forward flow from the rightventricle into the pulmonary artery, thus ductaldependent. The obstruction may be infundibular,valvar or supravalvar in nature or may involve branchpulmonary arteries. The stenotic component may be ata single site or may involve multiple sites. Infundibularobstruction is the most common obstruction in TOF andis due to malposition of the crista supraventricularis.The valvar stenosis may be due to valve leaflet fusionand/or due to valve ring hypoplasia. Right ventricularhypertrophy of severe degree is present in all cases.Dextroposition or over-riding of aorta over theventricular septum is a variable phenomenon. Theaorta is large and is thought to be due to adevelopmental anomaly rather than the result ofphysiologic abnormality of TOF. Right aortic arch ispresent in 25% of TOF cases.
Atrial septal defects may be present in 15% ofpatients with TOF in which case it may be calledpentology of Fallot. Coronary artery anomalies arepresent in a small but significant number of cases.Origin of the left anterior descending coronary arteryfrom the right coronary artery is the most commoncoronary anomaly in TOF and sometime the course ofthe coronary artery may be intramyocardial.
Because the VSD is large, the systolic pressures inboth ventricles are equal and for practical purposesboth ventricles act as one functional chamber. Thequantity of blood flow into to the systemic andpulmonary circuits depends upon their respectiveresistances. The level of systemic vascular resistanceand the resistance offered by the right ventricularoutflow tract stenosis determine the flows. The moresevere the PS, the less is the pulmonary flow. In theaverage case of tetralogy of Fallot, the resistance offeredby PS is more than that of the systemic vascular tonewith consequent right-to-left shunt across the VSD. Theresultant cyanosis and hypoxemia stimulate bonemarrow (via kidney and erythropoietin) and producepolycythemia.4 While the polycythemia is helpful inincreasing oxygen carrying capacity, it becomescounter-productive when the hematocrit is excessive (>60 to 70%).
Symptoms
The clinical presentation depends upon the degree ofPS. With milder degrees of PS, symptoms may not bepresent until late childhood while with severe PS, thepresentation may be in the early infancy. Typically the
infant may be pink (not cyanotic) as a neonate anddevelops cyanosis between 2 to 6 months of age. Mostusual modes of presentation are asymptomatic murmurdiscovered on routine auscultation, bluish color(cyanosis) observed by the parent or primary physician,hypercyanotic spells, and decreased exercise tolerance.
Hypercyanotic spells are variously described asanoxic spells, hypoxic spells, blue spells, paroxysmaldyspnea, paroxysmal hyperpnea and so on. The spellscharacteristically occur in tetralogy although they canbe present in other lesions with similar physiology.They can occur any time between 1 month and 12 yearsof age but the peak incidence is 2 to 3 months. They canoccur at any time of the day but most commonly seenafter awakening from sleep; crying, defecation andfeeding are the common precipitating factors. Spells arecharacterized by increasing rate and depth ofrespiration (hyperpnea) with increasing cyanosis,progressing to limpness and syncope, occasionallyterminating in convolutions, cerebrovascular accidentor death. Spells may occur in tetralogy with mildarterial desaturation and conversely may not be presentin patients with severe cyanosis. The cause or mecha-nism of onset of spells is not clear. Right ventricularinfundibular spasm, precipitated by acute increase inendogenous catecholamines has been proposed as amechanism. Prevention of these spells by beta-adrenergic blockade may further support thishypothesis. Since the spells have also been observed inpatients with VSD and pulmonary atresia in whominfundibular spasm is singularly irrelevant, it isunlikely that the infundibular spasm is the cause in allcases. Another mechanism proposed is paroxysmalhyperpnea.5 During sleep oxygen consumption isreduced and there is a normal acid base balance. Whenthe infant awakens the O2 consumption increases andthere is a slight acid base imbalance. There areadjustments made by the respiratory center to bring theimbalance back to normal. But, if there is a suddenincrease in activity and consequent increase in oxygen
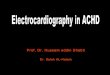
Fig. 1. The mechanism of hypercyanotic spells as proposed byGuntheroth.5 See the txt for details.

Diagnosis and Management of Cyanotic Congenital Heart Disease: Part I
Indian Journal of Pediatrics, Volume 76—January, 2009 59
consumption before the above described adjustmentsoccur, decrease in PO2 and pH and increase in PCO2
take place triggering a hyperpnea response from therespiratory center and enter a vicious cycle (Fig. 1).Hyperpnea reduces mean intrathoracic pressure, whichdecreases systemic and pulmonary resistances.Decreased systemic resistance is not matched withincreased pulmonary flow because of dominant rightventricular outflow tract obstruction. Thus, there is evengreater right-to-left shunt, further decreasing the PO2
and pH and thus a vicious cycle.4,5 Most workers believethat this is the most likely mechanism for thedevelopment of spells.
Physical Examination
Central cyanosis is observed in most cases of’ tetralogyof Fallot. However, it should be noted that mild arterialdesaturation may not cause clinically detectablecyanosis. Clubbing of fingers and toes is observedbeyond the first few months of life. There are usually nosigns of congestive heart failure. Prominent rightventricular impulse or heave may be present. A systolicthrill may be present at the left upper sternal border.The first heart sound may be normal or slightlyincreased. The second heart sound is single without anaudible pulmonary component. A grade III-IV, long,ejection, systolic murmur, caused by blood flowthrough the right ventricular outflow tract, is usuallyheard at the left upper sternal border. In contrast to PSwith intact ventricular septum, the murmur of tetralogybecomes shorter and less intense with increasingseverity of PS. During hypercyanotic spell the murmurdisappears or becomes very soft. A holosystolicmurmur of VSD may be heard at the left lower sternalborder in some children especially in less severe andacyanotic forms of tetralogy of Fallot. Early diastolicmurmurs do not occur with TOF; the exception is TOFwith absent pulmonary valve. Continuous murmur ofassociated PDA is rarely heard. Older children mayhave an audible continuous murmur of bronchialcollateral flow into the lungs, usually heard on the back.
Noninvasive evaluation
On a chest roentgenogram the heart size is usuallynormal to minimally increased. An uplifted apex,thought to indicate right ventricular hypertrophy maybe present and is described by some as “boot-shaped”heart. Concavity in the region of pulmonary conus,reflecting hypoplasia of the pulmonary outflow tractmay be present. Pulmonary vascular markings areusually diminished. A right sided aortic arch may bepresent. While a right aortic arch is expected to bepresent in 25% of TOF patients, the presence of a rightaortic arch along with concave pulmonary conus anddecreased pulmonary vascular markings in a chest x-ray makes the diagnosis of TOF virtually certain.
Electrocardiogram shows signs of right ventricularhypertrophy. Right atrial enlargement is less commonlyseen.
Hemoglobin and hematocrit along with red bloodcell indices should be monitored periodically in allchildren with cyanotic congenital heart defectsincluding TOF. The degree and duration of hypoxemiadetermine the level of hemoglobin. In the absence ofadequate iron intake, relative anemia with hypochromiaand microcytosis may develop. Because this is a riskfactor for developing cerebrovascular accidents, therelative anemia should be treated with oralsupplemental iron.4
Echocardiogram is very helpful in confirming thediagnosis and in evaluating several of the issuesrelated to TOF (Fig. 2). Enlargement of the rightventricle, large VSD, aortic over-ride and rightventricular outflow tract obstruction can be imaged.Shunting across the VSD and increased Doppler flowvelocity across the right ventricular outflow tract can bedemonstrated. Size of the main and proximal branchpulmonary arteries can be evaluated although the distalpulmonary arteries cannot easily be seen byechocardiogram.
CT and MRI. These noninvasive studies, including
Fig. 2. Selected echocardiographic and Doppler recordings froma patient with tetralogy of Fallot, demonstrating a largeaorta (Ao) overriding the interventricular septum (A),narrowed right ventricular outflow tract (RVOT) (B),large aorta and a small left atrium (LA) (C) and highDoppler flow velocity (D) across the RVOT. PA,pulmonary artery.
three-dimensional reconstruction, are useful in definingissues that could not be addressed by conventionalechocardiography. But, the expertise in performing andinterpreting such studies are not readily available in all institutions.

P. Syamasundar Rao
60 Indian Journal of Pediatrics, Volume 76—January, 2009
Cardiac catheterization and angiography :Catheterization is not routinely required, but may beperformed if all the data required for making decisionfor surgical correction can not be obtained by non-invasive studies with reasonable certainty.
Oxygen saturation data reveal systemic venous andarterial desaturation, usually proportional to the degreeof right ventricular outflow obstruction. There areusually no left-to-right shunts demonstrated.Pulmonary venous and left atrial saturations areusually normal. The left ventricular and aorticsaturations are diminished because of right-to-left shuntacross the VSD. Aortic saturation is a better (than leftventricular) indicator of the degree of desaturationbecause of better mixing distally. The peak systolicpressures in both ventricles are equal because of a largenon-restrictive VSD. The top of the right ventricularpressure curve is flat when compared to that of patientswith PS with intact ventricular septum in which it istriangular. The pulmonary arterial pressures are lowto normal with demonstrable peak systolic gradientsacross the pulmonary valve and infundibulum.However, multiple gradients may not be demonstrablein all patients either because of technical (multipleholes in the catheter or rapid withdrawal) orphysiologic reasons. Angiographic data should beused to supplement pressure information forassessment of degree and level of right ventricularoutflow obstruction. The left ventricular and aorticpressures are normal without any gradient across theaortic valve.
Angiography is an integral part of cardiaccatheterization. Selective left ventricular angiographyin a left axial oblique view to demonstrate the size andfunction of the left ventricle and the size and location ofthe VSD, particularly to exclude muscular VSD isimportant. Similarly selective right ventricularangiography to study its architecture, size and functionand to evaluate right ventricular outflow obstruction isrecommended. Pulmonary arteriogram in a sitting upview (150 LAO and 350 cranial) to visualize the size ofthe main and branch pulmonary arteries and toexclude branch pulmonary artery stenosis should beobtained. Aortic root angiography is also necessary tovisualize coronary artery anatomy, especially toexclude coronary arteries crossing the right ventricularinfundibulum. Origin of the left anterior descendingcoronary artery from the right coronary artery occurs ina significant number of cases of TOF and should beexcluded, if need be by selective coronary angiography.Some of the above angiographic features are illustratedin fig. 3.
Management
The goal of management of TOF patients is to allowtotal surgical correction with minimal mortality and
morbidity and to prevent or treat complicationsinherent to cyanotic heart defects in general and TOF inparticular. Protection against subacute bacterialendocarditis, prevention and/or prompt treatment ofdehydration, and periodic monitoring for relativeanemia secondary to iron deficiency and prompttreatment when found should be undertaken.Palliative or corrective surgical procedures should beperformed prior to development of significantpolycythemia. Exercise, as tolerated should bepermitted unless symptoms develop with activity.
Spells. Treatment of an infant with cyanotic spellmay be summarized5,6 as follows:
• The infant should be placed in a knee-chestposition. The reason for its effectiveness appears to berelated to its effect in increasing the systemic vascularresistance and thus decreasing the right-to-left shuntand improving the pulmonary flow.
• Humidified oxygen via a facemask should beadministered. Since the major defect in the spellsyndrome is pulmonary oligemia rather than alveolarhypoxia, oxygen administration has limited usefulness.If the infant is unduly disturbed by the facemask,oxygen therapy may be discontinued.
• Morphine sulfate, 0.1 mg/kg subcutaneously, maybe effective in aborting the spell. The mechanism ofaction is not clearly delineated, but its depressive effecton the central nervous system respiratory drive (thusreducing hyperpnea) and sedation of the infant may beimportant.
• Once the physical examination is completed (andthe limited but important laboratory studies areobtained) the infant should be left undisturbed andallowed to rest; this in itself may improve the infant’scondition.
Fig. 3. A. Selected right ventricular (RV) cineangiographic framedemonstrating enlarged and trabeculated RV opacifyingthe aorta (Ao) through a ventricular septal defect (notshown) and severe infundibular stenosis (IS). Note thatthe AO descends on the right side of the spine. B.Selected RV outflow tract cineangiographic framedemonstrating markedly narrowed pulmonary valve(VPS) with doming. The main (PA) and branchpulmonary arteries are well visualized. C, catheter.

Diagnosis and Management of Cyanotic Congenital Heart Disease: Part I
Indian Journal of Pediatrics, Volume 76—January, 2009 61
• Correction of metabolic acidosis (with sodiumbicarbonate), anemia (by blood transfusion), anddehydration (by appropriate fluids), if present, is veryimportant at this stage.
• If the spell continues, vasopressors to increase thesystemic vascular resistance and thus increase thepulmonary blood flow may be tried. In our experience,methoxamine (Vasoxyl) an alpha agonist has been mosthelpful. It is a pure peripheral vascular stimulatorwithout any direct action on the heart. Methoxamine20-40 mg in 250 ml of 5% dextrose in water may beadministered intravenously; the rate of infusion shouldbe adjusted to increase the systolic blood pressure by 15to 20% of the control value. Alternatively, phenyle-phrine may be given to increase systemic vascularresistance.
• Another option, propranolol, 0.1 mg/kg bodyweight, diluted in 50 ml of 5% dextrose in water, may beslowly administered intravenously while monitoringthe heart rate (by ECG if possible). Should there bemarked bradycardia, propranolol should be stopped.Once it is found to be effective, the infant may beswitched to oral propranolol 1-4 mg/kg/day in threeand four divided doses. The mechanism of action ofpropranolol is not clearly understood, but may includenegative inotropic effect on the right ventricularinfundibular myocardium, prevention of decrease insystemic vascular resistance and/or prevention ofventilatory response (hyperpnea) to hypoxia, allthrough beta adrenergic blockade. Esmolol, a rapidacting beta blocker, may also be used. Therecommended loading dose of Esmolol is 500 mcg/kgfollowed by 50-100 mcg/kg/min.
• Infrequently, general anesthesia may be necessaryto break the spell.
• If the infant does not improve with any of theaforementioned measures, an emergency systemic-to-pulmonary artery shunt (modified Blalock-Taussiganastomosis) should be performed. Occasionally, totalcorrection, if the anatomy is adequate, may heperformed on an emergency basis. The importantprinciple is that the infant requires more pulmonaryblood flow.
• If the infant improves with the managementoutlined above, total surgical correction of the cardiacdefects, if anatomically feasible, or a systemic-to-pulmonary artery shunt to improve pulmonary bloodflow on an elective basis within the next day or so maybe performed. More recently, we have used balloonpulmonary valvuloplasty as an alternative to Blalock-Taussig shunt, especially if valvar obstruction is asignificant component of right ventricular outflowobstruction.7-10 An alternative to surgery is oralpropranolol (dosage as above) which may help
postpone surgery by several months.
Surgery. Total surgical correction to include closureof VSD in such a manner as to direct left ventricularoutput into the aorta and resection of the infundibulumand/or relief of pulmonary valvar obstruction can beperformed almost at any age. Enlargement of the rightventricular outflow tract with a pericardial patch (orother prosthetic material) may be necessary in somecases. Sometimes total corrective procedures are notfeasible with “respectable” mortality either because ofpulmonary arterial (and/or annular) hypoplasia,“smallish” left ventricle, and/or anomalous course of amajor coronary artery in the right ventricularinfundibulum. Size and age of the patients also enterinto such decision making. If it is deemed that a givenpatient is not suitable for total surgical correction,palliative surgery may be utilized to augmentpulmonary blood flow and to allow the patients to growinto an age, size and anatomy that are more likelysuitable for complete correction. Classic or modifiedBlalock-Taussig shunt11,12 are options most surgeonsprefer modified Blalock-Taussig shunt using aninterposition Gore-Tex graft between right or leftsubclavian arteries to the ipsilateral pulmonary artery.We have used balloon pulmonary valvuloplasty7-10 inTOF patients to augment pulmonary blood flow and toallow for growth and development of the pulmonaryarterial system and left ventricle so that a total surgicalcorrective procedure could be performed at a later timewith a greater chance for success.7-1 0
Follow-up of all patients after surgery is important toaddress issues related to residual defects. On long-termfollow-up many patients seem to require replacement ofpulmonary valves for the management of pulmonaryvalve insufficiency.
TRANSPOSITION OF THE GREAT ARTERIES
Transposition of the great arteries (TGA) is the mostcommon cyanotic congenital heart defect presenting inthe newborn period. It constitutes 5% of all CHD and10% of all neonatal cyanotic CHD. There are multipledefinitions used to describe TGA. Perhaps, the mostaccurate description is “a condition in which the aortaarises from the morphologic right ventricle and thepulmonary artery from the morphologic left ventricle”.In the most common form, usually referred to ascomplete transposition, the atria are normal in position(situs solitus of the atria), there is atrioventricularconcordance (right atrium connected to the rightventricle and the left atrium to the left ventricle), d loopof the ventricles (right ventricle on the right and leftventricle on the left), ventriculo-arterial discordance(aorta arising from the right ventricle and thepulmonary artery from the ventricle) and the aortic

P. Syamasundar Rao
62 Indian Journal of Pediatrics, Volume 76—January, 2009
valve is located to the right of pulmonary valve (d-TGA). The systemic venous blood from the vena cavaeenters the right atrium and right ventricle and fromthere the aorta while the pulmonary venous bloodenters the left atrium and left ventricle and from therethe pulmonary artery (Fig. 4). Thus, the circulation isparallel instead of normal in-series circulation.Because of this reason, the systemic venous blood doesnot get oxygenated and the pulmonary venous blooddoes not get delivered to the body. The infants will notsurvive unless there are inter-circulatory shunts such asatrial or ventricular septal defect or patent ductusarteriosus.
Symptoms
Clinical features depend upon the anatomic type,namely Group I, TGA with intact ventricular septum;
otherwise be asymptomatic. However, they will, withtime, become tachypnoeic and develop respiratorydistress. If they are not appropriately treated, theybecome acidotic and go on to become lethargic withoutlack of spontaneous movement, and eventually die.
Group II TGA patients with VSD present withsymptoms of congestive heart failure (tachypnea,tachycardia, sweating, and poor feeding) between 4 to 8weeks of life, but the cyanosis is minimal.
Group III patients (TGA with VSD and PS) havevariable presentation, depending upon the severity ofPS. If there is poor mixing, they may present early inlife and mimic TGA with intact septum. If the PS issevere, the presentation is essentially similar to thatdescribed in the TOF section. With moderate PS thepresentation is late with longer survival. With mild PS,congestive heart failure signs may be present, similar togroup II patients.
Physical examination
The group I patients with intact septum are usuallyseverely cyanotic but are without distress until severehypoxemia and acidosis develop. Clubbing is notpresent in the newborn period and may not developuntil 3 to 6 months. The right ventricular impulse isincreased and the second heart sound is single. Eitherno murmur or a grade I-II/VI nonspecific ejectionsystolic murmur may be auscultated. In group IIpatients, tachypnea, tachycardia, minimal cyanosis,hepatomegaly, increased right and left ventricularimpulses, single second sound, a grade III-IV/VIholosystolic murmur at the left lower sternal border anda mid-diastolic flow rumble (murmur) at the apex maybe present. In group III patients, the findings are similarto TGA with intact septum, TGA with VSD, or TOFdepending upon the degree of mixing and severity ofPS.
Noninvasive Evaluation
Chest X-ray in the intact septum group is benign withnormal to minimal cardiomegaly and normal to slightlyincreased pulmonary vascular marking. The thymicshadow may rapidly involute and a narrow pedicle(superior mediastinum) may be seen. A combination ofthe above signs may sometimes assume “egg-shaped”appearance on a postero-anterior chest roentgenogram.In group II patients with VSD, moderate to severecardiomegaly and increased pulmonary vascularmarkings are usually seen. In group III patients, mild toat worst moderate cardiomegaly may be observed. Thepulmonary vascular marking may be increased, normalor decreased, dependent upon the severity of PS.
The electrocardiogram in a neonate with TGA andintact septum (Group I) may be normal with the usualright ventricular preponderance seen during this age.
Fig. 4. Box diagram of the heart showing parallel circulations intransposition of the great arteries. Note that rightventricle pumps into the aorta (Ao) (because oftransposition) which goes to the body and returns intoright atrium and back into the body. Similarly leftventricular output goes to the pulmonary artery (PA)and lungs and returns back to the left atrium and leftventricle to be pumped back into the lungs. Unless thereare inter-circulatory communications via either a patentforamen ovale or patent ductus arteriosus, the infantcannot survive. Mixing across a ventricular septal defect(VSD) if such is present (not shown in the diagram)would also prevent progressive hypoxemia and death.
Group II, TGA with VSD, and Group III, TGA with VSDand PS.
In group I with intact septum, the infants usuallypresent with cyanosis within the first week of life(sometimes within hours to days of life). They may

Diagnosis and Management of Cyanotic Congenital Heart Disease: Part I
Indian Journal of Pediatrics, Volume 76—January, 2009 63
In older infants clear-cut right ventricular hypertrophyis seen and in addition right atrial enlargement may beobserved. In group II patients, biventricularhypertrophy and left atrial enlargement are usual. Ingroup III, right ventricular or biventricular enlargementis seen.
Echocardiogram is usually helpful in the diagnosisand assessment. Demonstration of transposition of thegreat arteries is somewhat difficult in view of the factthat atrial and ventricular anatomy is normal and theaortic and pulmonary valves look similar onechocardiographic study. If one can follow the greatvessel arising from the left ventricle and demonstrate itsbifurcation (Fig. 5), identifying it as a pulmonary artery,the diagnosis is easy. One of the helpful indirect signsis somewhat a posterior course the great vessel off of theleft ventricle in a precordial long axis view, indicatingpulmonary artery in contradistinction to anteriorlycoursing ascending aorta (Fig. 6). On-end visualizationof both the aorta and pulmonary artery simultaneouslyon a precordial short axis view of the heart is alsohelpful in suggesting TGA. The presence of aninteratrial communication and patent ductusarteriosus and shunt across them by color and pulsedDoppler can also be evaluated. In addition to these,demonstration of VSD and PS will place the patientsinto the respective groups.
Blood gas values are useful in demonstrating thedegree of hypoxemia and ventilatory status.
With the increased accuracy of echocardiographicdiagnosis, invasive studies are not necessary fordiagnosing TGA. Need for rapid relief hypoxemia andacidosis by balloon atrial septostomy and the need for agreater definition of coronary artery anatomy prior toarterial switch procedure may necessitatecatheterization and angiography.
In group I patients, vena caval, right atrial, rightventricular and aortic saturations are moderately toseverely diminished unless atrial, ventricular or ductalshunting is present. Similarly, the pulmonary venous,left atrial, left ventricular and pulmonary arterialsaturations are high with minimal, if any right-to-leftshunt. In TGA, the pulmonary artery saturations arehigher than those in the aorta.
The left atrial pressure is usually high with apressure gradient across the atrial septum. The rightventricular pressure is at systemic level without anygradient across the aortic valve. In TGA with intactseptum the left ventricular and pulmonary arterypressures are normal without any gradient across thepulmonary valve. However, in the early neonatalperiod, prior to involution of the pulmonaryvasculature, these pressures are elevated, compared to
Fig. 5. Selected video frames from a 2-dimensionalechocardiographic views of an infant with transpositionof the great arteries. In a, note the great vessel coming offof the left ventricle (LV) courses posteriorly andbifurcates into left (LPA) and right (RPA) pulmonaryarteries. In b. posterior vessel is similarly seen tobifurcate. The anterior vessel is aorta (Ao). LA, leftatrium; RV, right ventricle.
Hemoglobin and hematocrit are particularly useful inthe follow-up of older children.
Cardiac catheterization and angiography
Fig. 6. Precordial long axis views of two neonates, first (top, A& B) with normally related great arteries and the second(bottom, C) with transposition of the great arteries. A.Note that the posterior vessel arising from the leftventricle (LV) courses somewhat anteriorly, indicatingthat it is likely to be the aorta. In B, the anterior vesselcoming of off the right ventricle (RV) divides into rightand left pulmonary arteries, suggesting that his vessel ismain pulmonary artery (MPA). In C, the posterior vesselis coursing backward (posteriorly) after its origin fromthe LV and is likely to be the MPA, suggestingtransposition of the great arteries. Ao, aorta; Asc,ascending aorta; AV, aortic valve; LA, left atrium; mv,mitral valve; PV, pulmonary valve; PW, posterior wall ofLV; RVO, right ventricular outflow tract; VS, ventricularseptum.

P. Syamasundar Rao
64 Indian Journal of Pediatrics, Volume 76—January, 2009
normal. In the presence of significant VSD and/or PS,the left ventricular pressure is elevated and this isusually proportional to the size of VSD and severity ofPS. The pulmonary artery pressure is usually increasedwith associated VSD while with PS, it may be low tonormal.
Selective right ventricular angiography (Fig. 7)reveals a morphologically right ventricle withopacification of an anteriorly and superiorly displacedaorta. The aortic valve is located to the right of thepulmonary valve (d-TGA). The aorta ascends in anormal fashion and usually descends on the left side ofthe spine. The size and function of the right ventricleand presence of tricuspid insufficiency should beevaluated. If a VSD is present, it may be visualized. Alaid-back view of the aortic root angiography alongwith a lateral view may be useful in demonstratingcoronary artery anatomy. Aortography may, inaddition, be useful in demonstrating PDA andcoarctation of the aorta. Left ventricular cineangiogram(Fig. 7) reveals a morphologic left ventricle with promptopacification of the pulmonary artery. The pulmonaryvalve is located posterior, inferior and to the left of theaortic valve. Left ventricular angiography should bescrutinized for subvalvar and valvar PS. A VSD may
be visualized, if present.
Management
The initial management of TGA and other cyanoticneonates is similar. Monitoring the infant’s temperatureand maintenance of neutral thermal environment isextremely important. In hypoxemic infants, ambientoxygen should be administered. In cyanotic CHDpatients, no more than 0.4 FIO2 is necessary. Metabolicacidosis (pH < 7.25), if any, should be corrected withsodium bicarbonate (usually 1-2 mEq/kg diluted halfand half with 5% or 10% dextrose solution)immediately. Respiratory acidosis should be cared forby appropriate suctioning, intubation and assistedventilation. Hypoglycemia may be a significantproblem; therefore, the infant’s serum glucose shouldbe monitored and the neonates should routinelyreceive 10% dextrose in water intravenously. Ifhypoglycemia (<30 mg/100ml) occurs, 15% to 20%dextrose solution should be administered. Similarlyhypocalcemia should be monitored for and treated, iffound.
Untreated, TGA with intact septum carries a poorprognosis. If an infant is getting progressivelyhypoxemic, it is likely that the inter-circulatorypathways (patent foramen ovale and patent ductusarteriosus) are closing. Prostaglandin El (PGEI ) (0.05 to0.1 mcg/kg/min) intravenously may help open theductus, thus improve oxygenation. Balloon atrialseptostomy13,14 (Fig. 8) may be necessary to improvehypoxemia even after PGE1. Total surgical correction byarterial switch procedure (Jatene)15 is the treatment ofchoice in these neonates and will be discussed here-
Fig. 7. A & B. Left ventricular (LV) cineangiogram in postero-anterior (A) and lateral (B) views demonstrating a finelytrabeculated, morphologic left ventricle with promptopacification of the pulmonary artery (PA). The PA isinferior and posterior to its usual position. C & D. Rightventricular (RV) cineangiogram in postero-anterior (C)and lateral (D) views showing a coarsely trabeculatedventricle with opacification of the aorta (Ao). Note thatthe aortic valve is superior and anterior (D) to its usualposition.
Fig. 8. Selected cinfluroscopic frames of the Rashkind’s balloonseptostomy procedure. Note the position of the inflatedballoon in the left atrium (A) and in right atrium andinferior vena cava in successive frames, as it is rapidlyand forcefully withdrawn across the atrial septum (B,C,& D). After it reaches the inferior vena cava (D), it israpidly advanced into the right atrium (E & F) in ordernot to inadvertently occlude the inferior vena cava in caseof failure to deflate the balloon (which is quite rare).

Diagnosis and Management of Cyanotic Congenital Heart Disease: Part I
Indian Journal of Pediatrics, Volume 76—January, 2009 65
under.
TGA patients with VSD usually present with heartfailure and aggressive anticongestive measures areindeed needed. Balloon atrial septostomy may helprelieve pulmonary venous congestion and improveoxygenation. These patients will require Jateneprocedure with closure of VSD.
TGA patients with VSD and PS may have varyingtypes of presentation. If the reason for hypoxemia is poormixing, balloon atrial septostomy is the treatment ofchoice. If the hypoxemia is secondary to decreasedpulmonary flow, a Blalock-Taussig type of shunt may beneeded. Sometimes both balloon septostomy and balloondilatation of pulmonary valve may be performed viacatheters in some of these children. Eventually thesepatients require a Rastelli type of repair.
Surgical correction. Mustard procedure, which wasoriginally described in 1964 was the most commonlyused operation for TGA in the past. In this operation,hemodynamic correction of the defect is achieved by re-directing the systemic and pulmonary venous returnsby means of an intraatrial baffle. Better understandingof the conduction system and its blood supply coupledwith the use of a pericardial baffle (instead of Dacronbaffle) has significantly reduced post-operativecomplications such as arrhythmia and baffleobstruction. Other types of atrial switch operations,originally described by Senning and by Shumackerhave also been used in several centers. When venousswitch procedure is opted for, Mustard and Senningprocedures appear to be selected with equal frequency,depending upon the institution/surgeon. In 1975,Jatene described anatomical corrections for TGA byarterial switch with relocation of the coronary arteries.Initially this procedure was performed for TGA withnon-restrictive VSD and subsequently was adapted toTGA with intact septum. The arterial switch procedurehas several advantages over the venous switchprocedure in that the arrhythmias are less frequent, andthe left ventricle rather than the right ventricle serves asa pump to the systemic circuit. Arterial switchprocedure, however, must be performed in the earlyneonate prior to deconditioning the left (pulmonary)ventricle in TGA patients with intact septum. Althoughthere are no extensive long term follow-up resultsavailable, the short term and medium-term follow-upresults are very encouraging and, at this time, thearterial switch procedure with or without LeComptemaneuver is considered the preferable operation forpatients with TGA. Again, follow-up after surgery ismandatory to manage residual defects.
TRICUSPID ATRESIA
Tricuspid atresia (TA) is a cyanotic, congenital cardiacanomaly and has been commonly defined as congenital
absence or agenesis of the morphologic tricuspid valve.It is the third most common cyanotic CHD and is themost common cause of cyanosis with left ventricularhypertrophy. Most issues related to this disease entitywere extensively reviewed elsewhere;16-20 the interestedreader is referred to these publication for additionaldetails. Tricuspid atresia accounts for 1.4% of subjectswith CHD. The most common type of TA, muscularvariety, is characterized by a dimple or a localizedfibrous thickening in the floor of the right atrium at theexpected site of the tricuspid valve. The right atrium isusually enlarged and its wall thickened andhypertrophied. An interatrial communication, which isnecessary for survival, is usually a stretched patentforamen ovale. The left atrium is enlarged and may bemore so if the pulmonary blood flow is increased. Themitral valve is morphologically a mitral valve, usuallybicuspid but its orifice is large and rarely incompetent.The left ventricle is clearly a morphologic left ventriclewith only occasional abnormality; however, it isenlarged and hypertrophied. The VSD may be large,small or non-existent (intact ventricular septum) ormultiple VSDs may be present. While a variety of VSDsare seen in TA hearts, muscular defects are mostcommon. Also, most of these VSDs are restrictive andproduce subpulmonary stenosis in patients withnormally related great arteries and subaortic stenosis inpatients with transposed great arteries. The rightventricle is small and hypoplastic; its size, by and large,is determined by the anatomic type. The relativeposition of the great vessels is quite variable and hasbeen the basis for classification of’ this anomaly: Type I,normally related great arteries; Type II, d-transpositionof the great arteries; Type III, transposition of the greatarteries other than d-transposition; and Type IV,Truncus arteriosus (Table 2).21 Pulmonary outflow tractobstruction may be either subvalvar or valvar inpatients with transposition while in patients withnormally related great arteries, it is often at the VSDlevel although, in a few cases, subvalvar pulmonarystenosis, narrow tract of the hypoplastic right ventricleand, rarely, valvar PS may also be responsible forpulmonary outflow tract obstruction. The pulmonaryartery may be atretic and in such cases a PDA or aorto-pulmonary collateral vessels may be present.Association with aortic coarctation is rare with type Ipatients and is more common in patients withtransposition of the great arteries.
An obligatory right-to-left shunt occurs it the atriallevel in most types and subtypes of TA. Thus, thesystemic and coronary venous blood mixes withpulmonary venous return in the left atrium and exitsinto the left ventricle. In type I (normally related greatarteries) patients with a VSD, left-to-right ventricularshunt occurs, thus perfusing the lungs. In the absenceof a VSD (i.e., intact ventricular septum), the pulmonary

P. Syamasundar Rao
66 Indian Journal of Pediatrics, Volume 76—January, 2009
circulation is derived either via a PDA or through aorto-pulmonary collateral vessels. The presence of either aVSD or other means of blood supply to the lungs isessential for the patient’s survival. The aortic bloodflow is derived directly from the left ventricle. In type II(with d-transposition of the great arteries), thepulmonary blood flow is directly divided from the leftventricle. The systemic blood flow is via the VSD andright ventricle.
Symptoms
Approximately one-half of the patients with TA presentwith symptoms on the first day of life and 80% wouldhave had symptoms by the end of the first month oflife.17,19,20 The magnitude of pulmonary blood flowdetermines the timing of and type of clinicalpresentation. Two modes of presentation arerecognized; those with decreased pulmonary bloodflow and those with increased pulmonary blood flow.
Infants with pulmonary oligemia present withsymptoms of cyanosis within the first few days of life;the more severe the pulmonary oligemia, the earlier isthe clinical presentation. These hypoxemic infantsmay have hyperpnea and acidosis if the pulmonaryblood flow is markedly diminished. The majority of theinfants belong to type Ib (no transposition andpulmonary hypoplasia with a small VSD). Patientswith pulmonary atresia (subgroup a of all types)irrespective of great vessel relationship will also presentwith early cyanosis, especially when the ductus beginsto close. Hypoxic spells are not common in the neonatealthough the spells can occur later in infancy.
Infants with pulmonary plethora usually presentwith signs of heart failure within the first few weeks oflife although an occasional infant may present withinthe first few days of life. They are only minimallycyanotic, but present with symptoms of dyspnea,fatigue, difficulty to feed, and perspiration. Recurrentrespiratory tract infections and failure to thrive are othermodes of presentation. The majority of these patientsbelong to type II (transposition with a large VSD)although a small number of patients may be of type Ic(no transposition but a large VSD). The association of
aortic coarctation with type II patients is well known22
and coarctation, when present, makes them vulnerableto early cardiac failure.
Physical Findings
In infants (and children) with pulmonary oligemia,physical examination reveals central cyanosis,clubbing (in older infants and children), tachypnea orhyperpnea, normal pulses, prominent “a” wave in thejugular venous pulse (if there is interatrial obstruction),and no hepatic enlargement. Quiet precordium, andabsence of thrills are usual. The second heart sound isusually single. A holosystolic murmur suggestive ofVSD may be heard at the left lower or mid sternalborder. No diastolic murmurs are heard. In patientswith associated pulmonary atresia, no murmurs areusually heard, although in an occasional patient acontinuous murmur of PDA may be heard. Signs ofclinical congestive heart failure are notably absent.
In the group with pulmonary plethora, examinationreveals tachypnea, tachycardia, decreased femoralpulses (if associated with coarctation of the aorta),minimal cyanosis and hepatomegaly. Prominent “a”waves in the jugular veins and/or presystolic hepaticpulsations may be observed with associated interatrialobstruction. The second heart sound may be single orsplit. A holosystolic murmur of VSD is usually heardat the left lower sternal border. An apical mid-diastolicflow murmur may be heard. Clear-cut signs ofcongestive heart failure are usually present.
Non-invasive evaluation
Chest X-ray appearance is, by and large, dependentupon the total pulmonary blood flow. In patients withdiminished pulmonary blood flow (the majority ofinfants fall into this group), the heart size is eithernormal or minimally enlarged. Several patterns ofcardiac configuration have been described but in theauthor’s experience and that of others, there is noconsistent pattern that would be diagnostic of TA.There may be concavity in the region of pulmonaryartery segment in patients with pulmonary oligemiaand small pulmonary artery. The right atrial shadow
TABLE 2. Unified Classification of Tricuspid Atresia
Type I Normally related great arteries Each Type and Subtype are dividedType II D-transposition of the great arteries Subgroup a. Pulmonary atresiaType III Malpositions of the great arteries other than
D-transposition Subgroup b. Pulmonary stenosis or hypoplasiaSubtype 1. L-transposition of the great arteriesSubtype 2. Double outlet right ventricle Subgroup c. Normal pulmonary arteries (noSubtype 3. Double outlet left ventricle pulmonary stenosis)Subtype 4. D-malposition of the great arteries
(anatomically corrected malposition)Subtype 5. L-malposition of the great arteries
(anatomically corrected malposition)Type IV. Persistent truncus arteriosus

Diagnosis and Management of Cyanotic Congenital Heart Disease: Part I
Indian Journal of Pediatrics, Volume 76—January, 2009 67
may be prominent. In patients with increasedpulmonary blood flow, cardiomegaly and prominentpulmonary vasculature are seen.
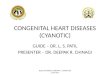
The electrocardiogram (Fig. 9) can be virtuallydiagnostic of tricuspid atresia in an infant with cyanoticCHD. The characteristic features include right atrialenlargement, an abnormal, superiorly oriented majorQRS vector (so called left axis deviation) in the frontalplane, left ventricular hypertrophy and diminishedright ventricular forces. Abnormally superior vector (leftaxis deviation) is present in excess of 80% of patientswith type I (normally related great vessels) anatomywhile only less than 50% of patients with type II(transposition) anatomy show such a typicalelectrocardiographic pattern.
will help decide whether there is associatedtransposition of the great arteries. Measurement ofpeak Doppler flow velocities across the VSD and rightventricular outflow tract will not only reveal obstructionif present at these sites but will also allow estimation ofpulmonary artery pressures. Suprasternal notchimaging will be of use in demonstrating aorticcoarctation, which is often seen in type II(transposition) patients. Contrast echocardiographywith two-dimensional imaging will clearly demonstratesequential opacification of the right atrium, left atrium,left ventricle and then the right ventricle. However,such a study is not always necessary for diagnosis.
Cardiac catheterization and selective cineangiography
The diagnosis of TA based on clinical, electro-cardiographic, and echocardiographic features isrelatively simple, and cardiac catheterization andselective cineangiography, rarely, if ever, are essentialfor arriving at the diagnosis. However, these proceduresare useful and should be undertaken to resolve issuesnot clarified by non-invasive studies and to evaluatemultiple physiologic and anatomic features prior toplanned Fontan-Kreutzer operation.23
Oxygen saturation data reveal diminished systemicvenous saturation; the extent of decrease is related to thesystemic arterial desaturation and the severity ofcongestive heart failure. The pulmonary venoussaturation is usually in the normal range. A significantdecrease in left atrial saturation is expected because ofobligatory right-to-left shunting across the patent
Fig. 9. A 12-lead electrocardiogram of a child with tricuspidatresia, demonstrating a mean frontal plane vector (axis)of -450. Also, note tall R waves in the left chest leads anddeep S waves in the right chest leads indicative of leftventricular hypertrophy and tiny, if any r waves in rightchest leads, suggestive of small right ventricle, all typicalfeatures tricuspid atresia.
Echocardiogram is reasonably characteristic for TA.Two-dimensional echocardiography, apart fromshowing enlarged right atrium, left atrium, and leftventricle and a small right ventricle, will demonstratethe atretic tricuspid valve directly (Fig. 10). In the mostcommon muscular type, a dense band of echoes is seenat the site where the tricuspid valve should be and theanterior leaflet of the detectable atrioventricular valve isattached to the left side of the interatrial septum. Apicaland subcostal four-chambered views are best todemonstrate the anatomy. Atrial and ventricular septaldefects can also be demonstrated by 2-D echocar-diography and shunting across these defects can bedemonstrated by Doppler echocardiography.Semilunar valves can be identified as pulmonary oraortic by following the great vessel until the bifurcationof the pulmonary artery or arch of the aorta is seen, this
Fig. 10. Apical four chamber two-dimensional echocardiographicviews of a child with tricuspid atresia showing anenlarged left ventricle (LV), a small right ventricle (RV)and a dense band of echoes, representing atretic tricuspidvalve (ATV) at the site where the tricuspid valve echoshould be. Atrial (not labeled) and ventricular (openarrow-head) septal defects are also seen. Note theattachment of the detectable atrioventricular valve to theleft side of the interatrial septum. Frames a and b showopen and closed mitral valve leaflets (closed arrow-heads)respectively. LA, left atrium; RA, right atrium.

P. Syamasundar Rao
68 Indian Journal of Pediatrics, Volume 76—January, 2009
foramen ovale. Falsely high or falsely low saturationsmay be measured in the left atrium because ofstreaming. The left ventricular saturations are usuallywell mixed and are more reliable. The saturations in theleft atrium, left ventricle and aorta as well as those in theright ventricle and pulmonary artery are nearly equal.Systemic arterial (aortic) desaturation is always presentand the extent of desaturation is largely proportional tothe Qp:Qs (has a curvilinear relationship23).
The right atrial pressure may be mildly increased. Ifthe foramen ovale is restrictive the pressure in the rightatrium is markedly elevated; a mean pressure gradientof 5 mmHg across the patent foramen ovale in favor ofthe right atrium and giant “a” waves in the rightatrium are indicative of an obstructive foramen ovale.The left atrial mean and left ventricular end-diastolicpressures are usually normal, but may be elevated ifthere is increased pulmonary blood flow, poor leftventricular function or significant mitral insufficiency.The right ventricular pressure is proportional to thesize of the VSD in type I (normally related great arteries)patients while it is at systemic level in type II(transposition) patients. Systolic pressure gradientacross the VSD may be seen if it is restrictive. Thepulmonary artery pressure may be normal or increaseddepending upon the size of the VSD (and associatedPS) in type I patients and upon the presence or absenceof subvalvar or valvar PS in type II patients. Aorticpressures are usually normal. If aortic coarctation ispresent, systolic hypertension and pressure gradientacross the coarctation may be present.
Of all the calculated values, Qp:Qs and pulmonaryvascular resistance are most useful. The Qp:Qs isdiminished in type I hypoxemic patients with small orno VSD while it is markedly increased in type I patientswith moderate to large VSD and in most patients withtype II anatomy. Pulmonary vascular resistance is animportant factor to be taken into consideration fordeciding to go ahead with Fontan-Kreutzer operation;elevated resistance adversely affects the outcome of theoperation.
Selective right atrial angiography will not onlyconfirm the diagnosis but also gives informationregarding its size and location and shape of the atrialappendage. Following right atrial injection, successiveopacification of the left atrium and left ventricle (Fig. 11)occurs without direct opacification of the right ventricleand this negative shadow of the unopacified rightventricle, the so called right ventricular window isconsidered characteristic for TA. Selective leftventricular angiography is also recommended and isuseful in evaluating its size and function, size and typeof VSD, anatomy and size of the right ventricle,relationship of the great arteries and the source ofpulmonary blood flow. Selective right ventricular and
pulmonary arterial angiograms are possible with thecurrently available catheter/guide wire technology andmay be necessary in some cases for better definitionprior to considering “corrective” surgical procedures.
Management
Physiologically “corrective” operation for TA, namely,Fontan-Kreutzer procedure24,25 and its modifications,have improved the prognosis of patients with tricuspidatresia. Such physiologic correction is usuallyperformed in patients older than 2 years. As statedabove, most patients with TA present with symptoms inthe neonatal period and should be effectively palliatedto enable them to reach the age at which surgicalcorrection could be undertaken. The objective of anymanagement plan, apart from providing symptomaticrelief and increased survival rate, should be to preserve,protect, and restore anatomy (good sized andundistorted pulmonary arteries) and physiology(normal pulmonary artery pressures and preserved leftventricular function) to normal such that a “corrective”procedure could later be performed safely.
Medical management of the neonate, just as for TGApatients, includes maintenance of neutral thermalenvironment, normal acid-base status, normoglycemiaand normocalcemia by appropriate monitoring andcorrection, if needed. No more than 0.4 FI02 is necessaryunless there is associated pulmonary pathology.
In neonates with low arterial PO2 and O2 saturationwith ductal dependent pulmonary blood flow, the
Fig. 11. Selected frame from a postero-anterior view of a rightatrial (RA) angiogram in an infant with tricuspid atresiashowing successive opacification of the left atrium (LA)and left ventricle (LV). There was no direct andimmediate opacification of the right ventricle; thenegative shadow, the so called right ventricular window,is shown with an arrow.

Diagnosis and Management of Cyanotic Congenital Heart Disease: Part I
Indian Journal of Pediatrics, Volume 76—January, 2009 69
ductus should be kept open by intravenous infusion ofPGE1, in doses similar to that described in TOF andTGA sections. Once the infant is stabilized andappropriate diagnostic studies are performed, a Blalock-Taussig type of shunt is performed in the group withpulmonary oligemia.
In neonates and infants with pulmonary plethoraand congestive heart failure, aggressive anticongestivetherapy must be instituted. In type I (normally relatedgreat arteries) patients, the natural history of the VSD issuch that it closes spontaneously26,27 and the infantswill go on to develop pulmonary origemia. Because ofthese reasons, it is recommended that banding of thepulmonary artery not be routinely performed in thisgroup of patients. If optimal anti-congestive therapywith some delay does not produce adequate relief ofsymptoms, pulmonary artery banding should then beconsidered. Perhaps a serious consideration for usingabsorbable band material28-29 should be given. Anabsorbable pulmonary artery band has been used forpalliation in such infants.28 By restricting thepulmonary blood flow, the absorbable polydioxanoneband decreases pulmonary artery pressure initially andhelps abate symptoms of heart failure. As the VSDspontaneously closes, the pulmonary artery band getsresorbed and does not produce the severe pulmonaryoligemia29 that might have been associated with aconventional non-absorbable band. This is an inventiveapproach, although it is likely to be helpful in a limitednumber of patients.29 By contrast, in type II(transposition) patients, banding of the pulmonaryartery should be performed once the infant is stabilizedwith anti-congestive measures. If there is associatedaortic coarctation, it should also be relieved.
In infants with evidence for interatrial obstruction,balloon and/or blade atrial septostomy may benecessary.
Following initial palliation, the children should befollowed under close cardiologic supervision.Currently, preferred procedure is staged total cavo-pulmonary anastomosis.30 Between the ages of 6months to 1 year, bidirectional Glenn (the superior venacava is divided and anastomosed to the rightpulmonary artery, end to side so that the blood form thesuperior vena cava flows into both the right and leftpulmonary arteries) is performed. The bidirectionalGlenn shunt may be performed in patients as young as3 months; however, an increased probability of failureexists at this young age, presumably related topulmonary vascular reactivity and we do not advocatesuch an approach. At the time of bidirectional Glenn,repair of pulmonary artery narrowing, if present,should be undertaken. If the atrial septal defect isrestrictive it should be enlarged. Issues related tosubaortic obstruction and mitral valve regurgitation
should also be addressed. At the age of 2 years or whenthe patient reaches a weight of 15 kg, Fontanconversion is performed. Two types of Fontanconversion are described, namely intra-atrial tunneldiverting the inferior vena caval flow into thepulmonary arteries and an extracardiac conduit, againdiverting the inferior vena caval flow into thepulmonary arteries. Extracardiac Fontan is preferred bymost surgeons. In patients with associatedtransposition of the great arteries, early pulmonaryartery banding, relief of aortic coarctation (if present),and bypassing (by Damus-Kaye-Stansel) or resectingsubaortic obstruction should be incorporated into themanagement plan.
Before Fontan conversion, cardiac catheterizationshould be undertaken to ensure normal pulmonaryartery anatomy and pressure as well as normal leftventricular end-diastolic pressure. At the same time,aortopulmonary collaterals should be evaluated bymeans of selective subclavian artery and descendingthoracic aortic angiography. If collateral vessels arepresent, they should be coil occluded. If the patient hasrisk factors for poor outcome (for e.g., elevatedpulmonary pressure/resistance, pulmonary arterydistortion, and left ventricular dysfunction) for thecorrective procedure, a fenestrated Fontan procedureshould be considered. Transcatheter closure of thefenestration may be undertaken at a later date. Two-stage staged surgical-catheter approach has beenadvocated;31 initially a modified hemi-Fontan isperformed that is later completed by transcathetermethodology. This reduces the total number ofoperations required. However, there is only a limitedexperience with this approach.
Periodic follow-up after surgical correction isnecessary for continued medical management, but alsoto address complications that are not uncommon afterFontan surgery.20
CONCLUSION
In this review, tetralogy of Fallot, transposition of thegreat arteries and tricuspid atresia, the three mostcommon cyanotic congenital heart defects in children,are discussed. The clinical presentation, laboratoryfindings and management options are described. Thesedefects have sufficiently distinctive features such thatthey can be diagnosed with relative ease. Upondiagnosis, some require immediate treatment forstabilization and all require subsequent corrective orpalliative surgical therapy. Significant post-operativeresidual abnormalities may be present and some mayrequire catheter interventional procedures and/orrepeat surgery. Consequently periodic follow-up ismandatory.

P. Syamasundar Rao
70 Indian Journal of Pediatrics, Volume 76—January, 2009
REFERENCES
1. Rao PS. Diagnosis and management of acyanotic heartdisease: Part I - obstructive lesions. Indian J Pediatr 2005;72: 496-502.
2. Rao PS. Diagnosis and management of acyanotic heartdisease: Part II - left-to-right shunt lesions. Indian JPediatr 2005; 72 : 503-512.
3. Fyler DC, ed. Nadas’ Pediatric Cardiology. Philadelphia, PA,Hanley & Belfus, Inc., 1992.
4. Rao PS. Pathophysiologic consequences of cyanotic heartdisease. Indian J Pediat 1983; 50: 479-487.
5. Guntheroth WG, Morgan BC, Mullin GL. Physiologicstudies of paroxysmal hyperpnea in cyanotic congenitalheart disease. Circulation 1965; 31: 70-76.
6. Rao PS. Congenital heart disease. In Rakel RE ed. Conn’sCurrent Therapy, Philadelphia, PA; W.B. Saunders. 1989;2010-2013.
7. Rao PS, Brais M. Balloon pulmonary valvuloplasty forcongenital cyanotic heart defects. Am Heart J 1988; 115:1105-1110.
8. Rao PS, Wilson AD, Thapar MK, Brais M. Balloonpulmonary valvuloplasty in the management of cyanoticcongenital heart defects. Cathet Cardiovasc Diagn 1992; 25:16-24.
9. Rao PS. Transcatheter management of cyanotic congenitalheart defects: a review. Clin Cardiol 1992; 15 : 483-496.
10. Rao PS. Pulmonary valve in cyanotic heart defects withpulmonary oligemia. In Sievert H, Qureshi SA, Wilson N,Hijazi Z eds. Percutaneous Interventions in Congenital HeartDisease, Informa Health Care; Oxford, UK, 2007; 197-200.
11. Blalock A, Taussig HB. The surgical treatment ofmalformations of the heart in which there is pulmonarystenosis or pulmonary atresia. J Am Med Assoc 1945;128:189-194.
12. de Leval MR, McKay R, Jones M et al. Modified Blalock-Taussig shunt. Use of subclavian artery orifice as flowregulator in prosthetic systemic-pulmonary artery shunts. JThorac Cardiovasc Surg 1981; 81 : 112-119.
13. Rashkind WJ, Miller WW. Creation of an atrial septal defectwithout thoracotomy. J Am Med Assoc 1966; 196: 991-992.
14. Rao PS. Role of Interventional Cardiology In Neonates: PartI. Non-Surgical Atrial Septostomy. Neonatology Today 2007;2 : 9-14.
15. Jatene AD, Fontes VF, Paulista PP et al. Anatomic correction
of transposition of the great vessels. J Thorac CardiovascSurg 1976; 72: 364-370.
16. Rao PS. Tricuspid Atresia. NY; Mt Kisco, Futura PublishingCo, 1982.
17. Rao PS: Tricuspid atresia. In: Long WA, ed. Fetal andNeonatal Cardiology. Philadelphia; WB Saunders Co, 1990;525-540.
18. Rao PS. Tricuspid Atresia. Mt Kisco, NY: Futura PublishingCo; 1992.
19. Rao PS. Tricuspid Atresia. In Pediatric CardiovascularMedicine. Moller JH, Hoffman JIE eds. New York, NYChurchill Livingstone, 2000; 421-441.
20. Rao PS. Tricuspid Atresia. In e-medicine – Pediatrics http://www.emedicine.com
21. Rao PS. A unified classification for tricuspid atresia. AmHeart J 1980; 99 : 799-804.
22. Rudolph AM. Congenital Disease of the Heart. Year-BookMedical Publishers, Inc., Chicago, IL, 1974.
23. Rao PS. Cardiac catheterization in tricuspid atresia. In: RaoPS, ed. Tricuspid Atresia. 2nd ed. Mt Kisco, NY: FuturaPublishing Co; 1992; 153-178.
24. Fontan F, Baudet E: Surgical repair of tricuspid atresia.Thorax 1971; 26: 240-248.
25. Kreutzer G, Bono H, Galindez E et al. Una operacion para lacorreccion de la atresia tricuspidea. Ninth ArgentineanCongress of Cardiology, Buenos Aires, Argentina, Oct. 31-Nov. 6, 1971.
26. Rao PS. Natural history of the ventricular septal defect intricuspid atresia and its surgical implications. Br Heart J1977; 39: 276-288.
27. Rao PS. Further observations on the spontaneous closure ofphysiologically advantageous ventricular septal defects intricuspid atresia: surgical implications. Ann Thorac Surg1983; 35: 121-131.
28. Bonnet D, Sidi D, Vouhe PR. Absorbable pulmonary arterybanding in tricuspid atresia. Ann Thorac Surg 2001; 71: 360-361.
29. Rao PS. Absorbable pulmonary artery band in tricuspidatresia (editorial). Ann Thorac Surg 2001; 71 : 361-362.
30. deLeval MR, Kilner P, Gewilling M et al. Totalcavopulmonary connection: a logical alternative toatriopulmonary connection for complex Fontan operation. JThorac Cardiovasc Surg 1988; 96 : 682-695.
31. Konertz W, Schneider M, Herwig V et al. Modified hemi-Fontan operation and subsequent nonsurgical Fontancompletion. J Thorac Cardiovasc Surg 1995; 110: 865-867.