Embed Size (px)
Citation preview

Congenital CMV
PD Dr Klara Pósfay Barbe
Pediatric Infectious Diseases Unit
Hôpital des Enfants
Genève

Baby boy, born 21.8.2013
Normal pregnancy, except prenatal hyperechogenicity of small bowel (CF screen negative)C‐section birth @36 5/7BW 1715 g; BH 41 cm; HC 31 cm (P<10 for all) Hypoglycemia: early feedingDD small for gest. age:
Genetic (parents consanguineous)Congenital infection (mother: Toxo, syph, HIV neg; CMV, rubella pos )Other ( e.g. calcified placenta found)

Work‐up
Clinical status otherwise normal at birthPlatelets 123’000, CBC normal otherwise
AST 39 U/L ALT 15 U/L GGT 1282 U/L Bilirubin 181 umol/l
Urinary CMV +Reactivation of maternal CMV with transplacental infection of the fetus
CMV viremia: 718 UI/mLHead US: intraventricular membrane + hyperechogenicity of thalamostriate blood vessels

Hypoplasia left cerebellum
Intraventricular membrane in occipital horn
Hearing screening NEye exam N
MRI

Why is it a problem?
CMV is the most frequent cause of congenital infections (0.2 to 2.2% of live births)
Congenital CMV (cCMV) can lead to stillbirth
In Europe, cCMV is the most important cause of neurological problems in children (25% of hearing loss (!), vision impairment, neuro‐developmental delay)
Important health costs and healthcare use
Screening of women currently not recommendedDemmler G Rev Infect Dis 1991Paixão P Eurosurveillance 2009

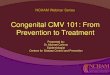
CMV seroprevalence rate
in women (12 yo‐49 yo) + in children Manickal S CMR 2013

Cytomegalovirus (CMV)
Large double‐stranded, enveloped DNA virus, part of the β‐herpes virusesMany genes coding for products used to escape the immune system or interact with inflammatory molecules: avoids immune destruction: life‐longlatencyPrevalence 60‐70% in US; ~100% in parts of AfricaPrimary infection:
Fever > 2 weeks, fatigue, headache, pharyngitis, adenopathies, hepatosplenomegaly, arthralgia (= mono‐like syndrome) Often no perceived disease

1 month
salivaurine
Vaginal secretions
spermblood
Antibody production
Entry through contact with mucosa
Viremia for several weeks/monthsCMV in biological fluids for months/years
Transmission

CMV latency, reactivation, reinfection
CMV persists in host for life (latency in hematopoietic cells, endothelial cells, etc.)
Can reactivate et cause viremia [inflammation, immune deficiency (disease or drug‐induced), pregnancy, breastfeeding]
> 90% women who breastfeed have detectable CMV by PCR in their milk
Possible to be infected with a new strain of CMVRole in cCMV possible (?)
Schleiss MR Curr Opin Pediatr 2006Boppana SB NEJM 2001

Epidemiology: pregnancySeroconversion during pregnancy: 1% ‐ 8%
Risk factors: working in daycare, in hospital (pediatric), have young children in household, sexually active teenagers
Infection during 1st trimester associated with increased risk of CNS disease Risk of cCMV
Seroconversion >> reactivation/reinfection
Risk of morbidities Seroconversion >> reactivation/reinfection
Ludwig A Eurosurveillance 2009Fowlers KB JAMA 2003Kenneson A Rev Med Virol 2007

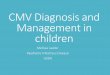
90% asymptomaticat birth
Approx. 10% of asymptomaticwill develop late sequelae
Ludwig A
, Eurosurveillance2009
CMV

10%90%
Kimberlin DW JID 2008Lombardi G J Clin Virol 2010If symptomatic at birth: risk of death ~5%

Diagnostic tests in women
Antibody measurement IgG + indicates old infection
IgM + indicates recent infection (< 2 mo to 6‐9 mo); in addition, IgM sometimes detectable during pregnancy
Avidity testsShows the strength of the link between antigen and antibody
Avidity increases over time

Diagnostic tests in women
CMV detection in blood or other biological fluids in pregnant women not used because detection of CMV possible even if infection not recent
Differential diagnosis between re‐infection or reactivation impossible

Diagnostic tests in fetus
Can be suggested when: Seroconversion in mother proven or
Prenatal US suggests cCMV
Discuss risk/benefit of amniotic fluid testing
Detection of virus in amniotic fluid is the best test to prove infection before birth
Viral culture= PCR regarding
sensitivity, but PCR faster

Diagnostic tests in fetus
Fetus excretes CMV in urine: must have a functional renal function (> 10 weeks of GA)
Transmission of virus not always right at the time of primo‐infection of mother
Amniocentesis in general around weeks 20‐21 and ~6‐8 weeks after presumed infection
Prenatal US recommended…..but up to 47% cCMV have a normal US
ECCI 2007

Antenatal imaging studies
US: Periventricular lesions, Ca++, microcephaly, cysts…
Ventricular enlargement (red flag)
Fetal MRI: Cortex analysis, white matter, cerebellum
Useful if anomaly on US, around 31 weeks GA
NB :Normal MRI ≠ no hearing loss or ≠ no developmental delay

Diagnostic tests in newborn
Diagnosis confirmed if detection of CMV in biological fluids during first 3 weeks of life (PCR or viral culture)
Urines or saliva preferred
> 3 weeks: intra‐partum infection, post‐partum possible (milk?)

Clinical and biological evaluation at birthPrevalence (%)
Jaundice 70
Thrombocytopenia 70
Microcephaly 50
Intracranial calcifications 50
Hepatomegaly 50
Splenomegaly 40
Abnormal liver function tests 40
Cortical dysplasia 35
Purpuric rash 30
Chorioretinitis 10
Bale JF Semin Pediatr Neurol 2012

Work‐up at birth when cCMV confirmed or suspected
Full clinical exam + head circumference
Urinary CMV (early Ag )
CMV in oropharynx (swab) by PCR (+/‐ viral culture)
Complete blood count
Liver function tests

cCMV work‐up
As soon as possible
Head ultrasound
Hearing test of both ears
@ 2 weeks of life: if neurological exam abnormal or small head: MRI
During first weeks of life
Complete eye exam

Neurologic physiopathology
Teratogenic action on fetus?Modulation of genomic expression?Direct chromosomal injury?
Anti‐apoptotic action and destruction of nearby neurons Neuroinflammatory process?“Preferential” infection of subventricular neural stem cells and glial cells?Placental insufficiency?…
Developmental susceptibility to CMV (< GA: > lesions)
Cheeran MCJ Clin Microbiol Rev 2009

Imaging studies: useful?
US: useful for early screening and follow‐upPeriventricular hyperechogenicity, lenticulostriate vasculopathy, calcifications, ventriculomegaly, white matter abnormalities…
CT‐scan: calcifications, often periventricular
MRI: polymicrogyria, schizencephaly, lissencephaly, cortical dysplasia, cerebellum hypoplasia, white matter abnormalities…

Imaging studies cCMV
Ca ++ 34 to 70 %Ventriculomegaly 45 % White matter abnormalities 22 %Problem with neuronal migration 10 % Microcephaly 27 %
Ventricular adhesionLenticulostriate vasculopathy
What are we looking for?
Amir, Arch Dis Child 2011
Best exam
CT
US
MRI
MRI
Clinical
MRI
MRI

US abnormalities…
Ca++ : Periventricular and basal gangliaLarge ventricles
White matter abnormalities
CMV

What else?Consult with pediatric infectious diseases specialist + follow‐up depending on results
Other imaging studies to be discussed
Hearing tests (acoustic oto‐emissions or evoked auditive potentials : @birth, 3 mo, 6 mo, 9 mo, 12 mo, 18 mo, 24 mo, 30 & 36 mo, then @ 4 & 5 years
Eye exam: around birth, then every mo until 6 mo, @ 1 year, 3 year, 5 year (+ according to ophthalmologist)
Psychomotor development exam every 3 mo
The patient should be announced to the AI/IV (code 493)

Retinitis
7 / 31 of retinitis appear > 1 year of life or progress slowly over time (23% ; 3‐11 yo)
No relationship with systemic symptoms or viremia
Hearing loss
CMV‐induced hearing loss is believed to be caused by virus‐induced labyrinthitis = damage to vestibular endolymphatic system, vestibular organs, collapse of the saccular membrane; sometimes involvement of the cochlea
No clear relationship with systemic symptoms or viremia
cCMV
Boppana PIDJ 1994

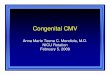
cCMV‐retinitis
cCMV, congenital immunodeficiency (HUG 2006); picture courtesy of Dr R. de Haller

CMV retinitis
Spontaneous evolution: auto-limited in immunocompetent
Often lesions with scarring already at birth
Can appear several weeks after birth
Rarely reactivations or new lesions later
PictureHUG 2012 Boppana & al. Ped Infect Dis J 1994 - Barampouti & al. BJO 2001, Slide courtesy of Dr R. de Haller

Detachment of the retina(1/3 of cases of retinitis)
Congenital or acquired cataract
Optic nerve atrophia
Coloboma of optic nerve
Keratitis
Anophtalmia
cCMV: other eye problems
Coats & al. JAAPOS 2000

Long‐term: not necessary
Follow‐up of urinary CMV useless, because excretion possible > 4 years!Repeated serologies unnecessary, unless diagnosis unclearFollow‐up viremia useless, because correlation between disease and viremia not studied/few studies in children with cCMV
CMV detection on Guthrie card possible if late diagnosis

Prevention & treatment

Screening
CDC does not recommend routine screening during pregnancyIn CH, screening of syphilis, CMV, VZV & parvovirus B19 is recommended to « at‐risk women »Screening via Guthrie ?
Sensitivity 93%; specificity 100% NPV 99%; PPV 100%
Screening via PCR in liquid or dry saliva Sensitivity 97.4%; specificity 99.9%NPV 99.9%; PPV 90.2%
Barbi M Rev Med Virol 2006Boppana JAMA 2010 & NEJM 2011

Prevention of cCMV
No available vaccine (… yet: phase II)
Screening before/after beginning of pregnancy of seronegative women, after encouragement to perform careful hand hygiene if seronegative (…!)

CDC recommendationsWash hands during 15‐20 seconds after
Changing diapersFeeding young childCleaning mouth or nose of childTouching toys
Do not share food, drinks, silverware, toothbrush with childDo not put pacifier in mouthAvoid contact with saliva of childWash toys, surfaces in contact with urine or saliva of child
Adler SP J Pediatr 2004; Velloup‐Fellous C J Clin Virol 2009

ECCI Recommandations (European Congenital CMV Initiative)Education
1. Women in childbearing age should be informed on CMV and risk of infection during pregnancy 2. Women should be informed of
Hygiene measures to prevent acquisition of CMV during pregnancyBenefits and limits of antenatal /neonatal screening

Prevention of cCMV : intrauterine treatments
Immunoglobulines: hyperimmunes CMV immunoglobulines during pregnancy
Encouraging results, but finished studies have biases. New studies ongoing (NCT 01376778)
► Insufficient data available to recommend CMV-IG
AntiviralsValacyclovir given @ 28 weeks GA reaches therapeutic levels in amniotic fluid, but no change in outcomeGanciclovir: more efficient against CMV. No randomized studies
► Insufficient data available to recommend antiviral during pregnancy

TREATMENT OPTIONS FOR THE CHILD

Antiviral: i.v. ganciclovir
Antiviral used for > 20 years, mostly in immunocompromised children (transplant)RCT symptomatic neonates: 6 weeks of treatment @ 6 mg/kg 2x/d
Better hearing @ 6 mo (84% vs 59% [better or N])Impaired hearing @ 1 year (21% vs 65%)
Doesn’t cure but decreases progression of diseaseBetter neuro‐developpemental outcome (Denver)Efficacy on asymptomatic baby? If other than CNS impairment?
Problems: IV line; medullar toxicity (up to 2/3 neutropenia) Kimberlin DW J Pediatr 2003
Oliver SE J Clin Virol 2009

Antiviral: oral valganciclovir
Pro‐drug of ganciclovir, metabolized in gutAvailable > 10 years; often used in transplant population
Possibility to obtain same blood levels as with ganciclovir16 mg/kg orally = 6 mg/kg iv ganciclovir23 children 6 weeks iv, followed by 6 weeks orally: safe and efficient (audition, viremia)CASG study 6 weeks vs 6 mo presented at IDSA
Problems: medullar toxicity; more g‐i troubles than with ganciclovir; oncogenicity?, suspension to produce Amir J Eur J Pediatr 2010
Kimberlin DW JID 2008

Valganciclovir
Has to be discussed individually (outside study, off‐label): valganciclovir orally 16 mg/kg 2x/day for 6‐12 moResults seem encouraging
Decrease in viral replicationDirect effect of CMV mostly during first year: decrease in replication = decrease in morbidity?
Conclusion: “6 months of oral VGCV treatment of infants with symptomatic congenital CMV disease improves audiologic and neurodevelopmental outcomes to at least 2 years of age. Less neutropenia is seen during the first 6 weeks of treatment with VGCV (19.3%) than was seen in an earlier CASG study of IV GCV (63%), and there is no excess neutropenia with continuation of VGCV treatment from 6 weeks to 6 months compared with placebo. “ Kimberlin IDSA Oct. 2013

Other antivirals
Foscarnet (selectively inhibits the pyrophosphate binding site on viral DNA polymerases)
Cidofovir (selective inhibition of viral DNA polymerase)
Maribavir (inhibition of a protein kinase UL97)Letermovir (quinazoline, inhibits CMV viral terminase)
Problems of toxicity (kidney, bone, teeth, …)
Vaccines: candidates in the pipeline…

General problems of CMV studies
Heterogeneity of Clinical presentationDiagnostic timeWork‐upTreatmentLength of follow‐up
Less severe cases less studies: impact of treatments?Long studiesMulticenter studies necessary….

In summaryCMV is the cause of a relatively frequent congenital infectionRisk of transmission to fetus ≈ 1/3Infected babies: 90% = asymptomatic @ birth, among which 10% will however have long‐term sequelaePossibly severe consequences of seroconversion during pregnancy: prevention should be encouragedMultidisciplinary approach necessary to detect sequelae et add auxiliary supportTreatment (yes/no, type, duration) of baby to discuss with experts, and with parentsNew studies hopefully published early 2014