Embed Size (px)
Citation preview

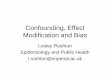
Confounding

A plot of the population of Oldenburg at the end of each year against the number of storks observed in that year, 1930-1936.
Ornitholigische Monatsberichte 1936;44(2)

Mortality rate in six countries in the Americas, 1986
Country Mortality rate(per 1000)
Costa RicaVenezuelaMexicoCubaCanadaUS
3.84.44.96.77.38.7
Question:Are people living in Costa Rica or Venezuela at lower risk of mortality than people in Canada or the US?
Yes
No
(assuming vital statistics are correct)

Mortality rate in six countries in the Americas, 1986
Country Mortality rate(per 1000)
Costa RicaVenezuelaMexicoCubaCanadaUS
3.84.44.96.77.38.7
Next question:Is the observed association causal in nature, i.e., is there something about living in Costa Rica or Venezuela that makes the population have lower risk of death than the population of Canada or the US?
Yes
No

Mortality
Country
?Agedistribution

N=14,054 middle age adults from 4 US communities
Comparing risk profile according to known CVD risk factors:
Low Risk individuals (n=623):- Never smokers- Total cholesterol <200 mg/dL- HDL cholesterol >65mg/dL- LDL cholesterol <100 mg/dL- Triglycerides <170 mg/dL- Glycemia <140 mg/dL- BP<140/90 mm Hg, no Rx- No Hx of CVD, htn, diabetes, high cholesterol
Rest (n=13,431): at least one of the above.

Low risk Rest
Number 623 13431
Age (years) Male (%) Education <12 years (%) Family history CHD (%)
51.6 19.7 12.9 39.4
54.3 46.1 23.6 44.6
BMI (kg/m2) Subscapular skinfold Triceps skinfold
26.1 22.0 26.6
27.8 24.9 25.0
Fibrinogen (mg/dL) Apolipoprotein B (mg/dL) Apolipoprotein AI (mg/dL)
280.0 147.2 61.2
303.5 132.3 95.0

Low risk Rest
Number 623 13431
Age (years) Male (%) Education <12 years (%) Family history CHD (%)
51.6 19.7 12.9 39.4
54.3 46.1 23.6 44.6
BMI (kg/m2) Subscapular skinfold Triceps skinfold
26.1 22.0 26.6
27.8 24.9 25.0
Fibrinogen (mg/dL) Apolipoprotein B (mg/dL) Apolipoprotein AI (mg/dL)
280.0 147.2 61.2
303.5 132.3 95.0
!?

Low risk Rest
Number 623 13431
Age (years) Male (%) Education <12 years (%) Family history CHD (%)
51.6 19.7 12.9 39.4
54.3 46.1 23.6 44.6
BMI (kg/m2) Subscapular skinfold Triceps skinfold
26.1 22.0 26.6
27.8 24.9 25.0
Fibrinogen (mg/dL) Apolipoprotein B (mg/dL) Apolipoprotein AI (mg/dL)
280.0 147.2 61.2
303.5 132.3 95.0
LR Rest
F 29.0 30.1
M 16.8 19.1

Low risk Rest
Number 623 13431
Age (years) Male (%) Education <12 years (%) Family history CHD (%)
51.6 19.7 12.9 39.4
54.3 46.1 23.6 44.6
BMI (kg/m2) Subscapular skinfold Triceps skinfold
26.1 22.0 26.6
27.8 24.9 25.0
Fibrinogen (mg/dL) Apolipoprotein B (mg/dL) Apolipoprotein AI (mg/dL)
280.0 147.2 61.2
303.5 132.3 95.0
LR Rest
F 29.0 30.1
M 16.8 19.1

DiseaseOutcome
Exposure
?Confounder
Common feature of previous examples

A variable can be a confounder if all the following conditions are met:
• It is associated with the exposure of interest (causally or not).
• It is causally related to the outcome.
• AND ... It is not part of the exposure outcome causal pathway

Ways to assess if confounding is present:
1) Does the variable meet the criteria to be a confounder (relation with exposure and outcome)?
2) If the effect of that variable (on exposure and outcome) is controlled for (e.g., by stratification or adjustment) does the association change?

Strategy #1: Does the variable meet the criteria to be a confounder?
Hypothetical case-control study of risk factors for malaria. 150 cases, 150 controls; gender distribution.
Cases Controls
Males 88 68
Females 62 82150 150
Question:Is male gender causally related to the risk of malaria?
Yes
No
Further study is needed
OR= [88 x 82] ÷ [68 x 62] = 1.71

Malaria
Malegender
?
Confounder for a male gender-malaria association?
?

Malaria
Malegender
?
Confounder for a male gender-malaria association?
Outdooroccupation

Malaria
Malegender
?Outdooroccupation
?
First criterion: Is the putative confounder associated with exposure?

.
Males Females N (%) N (%)
Outdoor 68 (43.5) 13 (9.0) Indoor 88 131
156 (100) 144 (100)
Question:Is outdoor occupation associated with male gender?
Yes
No
OR=7.8
First criterion: Is the putative confounder associated with exposure?

Malaria
Malegender
?Outdooroccupation
?
Second criterion: Is the putative confounder associated with the outcome
(case-control status)?

.
Cases Controls N (%) N (%)
Outdoor 63 (42.0) 18 (12.0) Indoor 87 132
150 (100) 150 (100)
Question:Is outdoor occupation (or something for which this variable is a marker of --e.g., exposure to mosquitoes) causally related to malaria?
Yes
No
OR=5.3
Malaria
Second criterion: Is the putative confounder associated with case-control
status?

Third criterion: Is the putative confounder in the causal pathway exposure outcome?
.
Malaria
Malegender
?Outdoor
occupation
?
Yes, it could be
Probably not
Note: Judgment and knowledge about the socio-cultural context are critical to answer this question

Question: Provided that:• Crude association between male gender and malaria: OR=1.71
and
• ... Outdoor occupation is more frequent among males, and• ... Outdoor occupation is associated with greater risk of malaria …
What would be the expected magnitude of the association between male gender and malaria after controlling for occupation (i.e., assuming the same degree of outdoor occupation in males and females)?
The (adjusted) association estimate will be smaller than 1.71
The (adjusted) association estimate will =1.71
The (adjusted) association estimate will greater than 1.71

Strategy #2: Does controlling for the putative confounder change the magnitude
of the exposure-outcome association?
Cases ControlsMales 88 68
Females 62 82150 150
OR=1.71
OR=1.06 OR=1.00
Cases ControlsMales 53 15
Females 10 363 18
Cases ControlsMales 35 53
Females 52 7987 132
Outdooroccupation
Indooroccupation
Malaria

Ways to control for confounding
• During the design phase of the study:– Randomized trial– Matching– Restriction
• During the analysis phase of the study:– Stratification– Adjustment

Low risk Rest
Triceps skinfold 26.6 25.019.116.8M
30.129.0F
RestLR
Examples of stratification
Cases ControlsMales 88 68
Females 62 82150 150
OR=1.71
Cases ControlsMales 53 15
Females 10 363 18
OR=1.06
Cases ControlsMales 35 53
Females 52 7987 132
OR=1.00
Outdooroccupation
Indooroccupation
Malaria

Note that confounding is present when:
• RR/ORpooled different from RR/ORstratified
and
• RR/OR1 = RR/OR2 = …= RR/ORz

Examples of adjustmentCases Controls
Males 88 68Females 62 82
150 150OR=1.71
OR=1.06 OR=1.00Outdoor
occupationIndoor
occupation
Adjusted OR*=1.01
*Using the Mantel-Haenszel method, to be discussed.
Country Crude Mortality rate(per 1000)
Age-adjusted* Mortality rate(per 1000)
Costa RicaVenezuelaMexicoCubaCanadaUS
3.84.44.96.77.38.7
3.74.65.04.03.23.6
*Adjusted by direct method using the 1960 population of Latin America as the standard population.
Malaria

Further issues for discussion
• Types of confounding• Confounding is not an “all or none”
phenomenon• Residual confounding• Confounder might be a “constellation” of
variables or characteristics• Considering an intermediary variable as a
“confounder” for examining pathways• Confounding: a type of bias?• Statistical significance and confounding

Types of confounding
• Positive confoundingWhen the confounding effect results in an
overestimation of the effect (i.e., the crude estimate is further away from 1.0 than it would be if confounding were not present).
• Negative confoundingWhen the confounding effect results in an
underestimation of the effect (i.e., the crude estimate is closer to 1.0 than it would be if confounding were not present).

10.1 10Relative risk
3.0
5.0
3.0
2.0
0.4
0.3
0.4
0.7
0.7
3.0
Type of confounding:Positive Negative
UNCONFOUNDED
OBSERVED, CRUDE
?“Qualitativeconfounding”

Example of positive confounding
Cases ControlsMales 88 68
Females 62 82150 150
OR=1.71
Cases ControlsMales 53 15
Females 10 363 18
OR=1.06
Cases ControlsMales 35 53
Females 52 7987 132
OR=1.00
Outdooroccupation
Indooroccupation
Adjusted OR=1.01
Malaria

Example of negative confounding
An occupational study in which workers exposed to a certain carcinogen are younger than those not exposed.
If the risk of cancer increases with age, the crude association between exposure and cancer will underestimate the unconfounded (adjusted) association.
Age: negative confounder.

Low risk Rest
Triceps skinfold 26.6 25.019.116.8M
30.129.0F
RestLR
Examples of qualitative confounding
Country Crude Mortality rate(per 1000)
Age-adjusted* Mortality rate(per 1000)
Costa RicaVenezuelaMexicoCubaCanadaUS
3.84.44.96.77.38.7
3.74.65.04.03.23.6
*Adjusted by direct method using the 1960 population of Latin America as the standard population.
Rate ratioUS/Mex= 1.78 0.72

• Confounding is not an “all or none” phenomenonA confounding variable may explain the whole or just part of the observed
association between a given exposure and a given outcome.• Crude OR=3.0 … Adjusted OR=1.0• Crude OR=3.0 … Adjusted OR=2.0
• Residual confoundingControlling for one of several confounding variables does not guarantee
that confounding is completely removed. Residual confounding may be present when:
- the variable that is controlled for is an imperfect surrogate of the true confounder,
- other confounders are ignored,- the units of the variable used for adjustment/stratification are too broad
• The confounding variable may reflect a “constellation” of variables/characteristics– E.g., Occupation (SES, physical activity, exposure to environmental risk
factors)– Healthy life style (diet, physical activity)


Low CHD
ERT(adjusted)*
?Otherfactors?
*Adjusted for family history, type of menopause, smoking, hypertension, diabetes, OC use, high cholesterol, age, obesity.

(Matthews KA et al. Prior to use of estrogen replacement therapy, are users healthier than nonusers? Am J Epidemiol 1996;143:971-978)

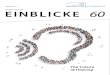
JAMA 1998;280:605-13.
Estrogen-Progestin
Placebo
Kaplan-Meier estimates of the cumulative incidence of primary coronary heart disease events.

Circulation 1996;94:922-7.

• Treating an intermediary variable as a confounder (i.e., ignoring “the 3rd rule”)Under certain circumstances, it might be of interest to
treat an hypothesized intermediary variable acting as a mechanism for the [risk factor outcome] association as if it were a confounder (for example, adjusting for it) in order to explore the possible existence of additional mechanisms/pathways. This is done by comparing the adjusted with the unadjusted values.

EXAMPLE:It has been argued that obesity is not a risk factor of mortality. The observed association between obesity and mortality in many studies might just be the product of the confounding effect of hypertension.
Mortality
Obesity
?Hypertension

HOWEVER,Hypertension is probably not a real confounder but rather a mechanism whereby obesity causes hypertension.*
Mortality
Obesity
Hypertension
*Manson JE et al: JAMA 1987;257:353-8.

EVEN IF HYPERTENSION IS A MECHANISM LINKING OBESITY TO MORTALITY, it may be of interest to conduct analyses that control for hypertension, to assess whether alternative mechanisms may causally link obesity and mortality.
Mortality
Obesity
Hypertension
alternativ
e mechanism(s)?
Block by adjustment

EXAMPLE:Is maternal smoking a risk factor of perinatal death?Is the association confounded by low birth weight?
Perinatal mortality
Maternal smoking
?Low birth
weight

OR RATHER:Is low birth weight the reason why maternal smoking is associated to higher risk of perinatal death?
Perinatal mortality
Maternal smoking
Low birthweight

BUT THERE COULD BE AN ADDITIONAL QUESTION:Does maternal smoking cause perinatal death by mechanisms other than low birth weight?
Perinatal mortality
Maternal smoking
Low birthweight
Direct toxic effect?
Block by adjustment

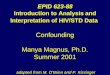
• Statistical significance should not be used to assess confounding effects
44
46
48
50
52
54
56
58
60
Age (years) 55 56
Odds Ratio [age 56/age 55] = 60/40 ÷ 50/50 = 1.5

44
46
48
50
52
54
56
58
60
Controls Cases
% p
os
t-m
en
op
au
sal
Age (years) 55 56
Odds Ratio [cases/controls] = 60/40 ÷ 50/50 = 1.5
• Statistical significance should not be used to assess confounding effects

• Statistical significance should not be used to assess confounding effects
The main strategy must be to evaluate whether the difference in the confounder is large enough to explain the association.

Control of Confounding Variables
• Randomization
• Matching
• Adjustment– Direct– Indirect– Mantel-Haenszel
• Multiple Regression– Linear– Logistic– Poisson– Cox
Stratified methods

Control of Confounding Variables
• Randomization
• Matching
• Adjustment– Direct– Indirect– Mantel-Haenszel
• Multiple Regression– Linear– Logistic– Poisson– Cox
Stratified methods

Mantel-Haenszel Technique for Adjustment of the Odds Ratios and Rate Ratios
• Nathan Mantel and William Haenszel were two very productive statisticians:
– Test for homogeneity of stratified OR’s (see Schlesselman, pp. 193-6, or Kahn & Sempos, pp. 115-6): for the assessment of multiplicative interaction
– Mantel-Haenszel test for trend
MHad bc Nn n m m
22
1 2 1 2
1 ( ) ( )

Mantel-Haenszel Technique for Adjustment of Odds Ratios-- Example (Israeli Study, see Kahn & Sempos, pp. 105)
MI Case Control
140 29 711 SBP (mmHg)
< 140 27 1244
OR= 1.88
• Is the association causal? •Is it due to a third (confounding) variable (e.g., age)?
BP MI?
Age
A variable is onlya confounder if dualassociation is present

Age Vs SBP 140 <140
60 124 79Age
< 60 616 1192
OR= 3.0
Age Vs MI MI Controls
60 15 188Age
< 60 41 1767
OR= 3.4
Does age meet the criteria to be a confounder? Yes

Age
Increased odds of systolic hypertension (“exposure”)
Increased odds of myocardial infarction (“outcome”)

Blood Pressure MI Risk
Age SBP MI CONT 60 140 9 115
<140 6 73 OR=
<60 140 20 596
<140 21 1171 OR=
0.9
1.9
• Is it appropriate to calculate an adjusted ORMH? NO
Odds Ratios not homogeneous
These findings fail to meet Mantel-Haenszel adjustment approach’s main assumption: that odds ratios are
homogeneous (no multiplicative interaction).

Mantel-Haenszel Formula for Calculation of Adjusted Odds Ratios
OR
a dNb cN
MHi
i i
i
i i
ii
Exposure Cases Controls
Yes ai bi
No ci di
Ni
=
b cN
a db c
b cN
w OR
w
i i
i
i i
i ii
i i
ii
i ii
ii
Thus, the ORMHis a weighted average of stratum-specific ORs(ORi), with weights equal to each stratum’s:
=
b cb c
a dN
b cN
i i
i i
i i
ii
i i
ii
wb cNii i
i

CHD No CHDPost-
menopausal118 3606
Pre-menopausal 17 2361ORPOOLED= 4.5
Post 3 171Stratum 1Age 45-49 Pre 10 1428
1612
Post 14 684Stratum 2Age 50-54 Pre 6 757
1461Post 37 1408Stratum 3
Age 54-59 Pre 1 153
1599
Post 64 1343Stratum 4Age 60-64 Pre 0 23
1430
OR1= 2.5
OR2= 2.6
OR3= 4.0
OR4=1.2*
(*adding 1.0 to each cell)

OR MH
3 1 4 2 81 6 1 2
1 4 7 5 71 4 6 1
3 7 1 5 31 5 9 9
6 4 2 31 4 3 0
1 7 1 1 01 6 1 2
6 8 4 61 4 6 1
1 4 0 8 11 5 9 9
1 3 4 3 01 4 3 0
3 0 4.
Ages 45-64

Stratum-specific odds ratios: 2.5, 2.6, 4.0, 1.2
Average= 3.04
?

CHD No CHDPost-
menopausal118 3606
Pre-menopausal 17 2361ORPOOLED= 4.5
Post 3 171Stratum 1Age 45-49 Pre 10 1428
1612
Post 14 684Stratum 2Age 50-54 Pre 6 757
1461Post 37 1408Stratum 3
Age 54-59 Pre 1 153
1599
Post 64 1343Stratum 4Age 60-64 Pre 0 23
1430
OR1= 2.5
OR2= 2.6
OR3= 4.0
OR4=1.2*
(*adding 1.0 to each cell)

Ages 45-59
OR MH
3 1 4 2 81 6 1 2
1 4 7 5 71 4 6 1
3 7 1 5 31 5 9 9
1 7 1 1 01 6 1 2
6 8 4 61 4 6 1
1 4 0 8 11 5 9 9
2 8 3.

Stratum-specific odds ratios: 2.5, 2.6, 4.0
Average= ORMH 2.83

There is an analogous procedure to obtain an adjusted Rate Ratio from stratified data in a
prospective study (see Kahn & Sempos, pp. 219-221)
EventsPersonTime
Stratum i Exposed ai Li
Unexposed bi Li
ni ti
Rate Ra tio
a Ltb Lt
MH
i i
ii
i i
ii

Mortality of Individuals with High and Low Vitamin C/Beta-Carotene Intake Index, by Smoking Status, Western Electric Company Study (Pandey et al, Am J
Epidemiol 1995;142:1269-78)
Vitamin C/Beta Carotene
Index
No. deaths
No. of Person-
years
Stratified Rate Ratio
Non-smokers High 53 5143
RR= 0.77Low 57 4260
Total 9403
Smokers High 111 6233 RR= 0.83
Low 138 6447
Total 12680
Rate Ra tio
a Ltb Lt
MH
i i
ii
i i
ii
5 3 4 2 6 09 4 0 3
11 1 6 4 4 71 2 6 8 0
5 7 5 1 4 39 4 0 3
1 3 8 6 2 3 31 2 6 8 0
0 8 1.

Formulas for calculating confidence intervals for the ORMH are available (Schlesselman, p.
184, Szklo & Nieto, Appendix A.8)

All participants
Strata of potential confounder Z
RF+ Z= 1
RF-
ORPooled
RF+
RF-
ORZ=1
Z= 2
RF+ ORZ=2
RF-
Z=3
RF+ ORZ=3
RF-
Z=…
If ORPooled ~~ (ORZ=1 ~~ ORZ=2 ~~ORZ=3, …) Z is not a confounder:
report crude OR (ORPooled)Z is a confounder:report ORPooled and adjusted OR
If ORPooled (ORZ=1 ~~ ORZ=2 ~~ORZ=3, …)#
If ORZ=1 ORZ=2ORZ=3, …
# # Z is an effect modifier. Do notadjust: report Z-specific ORs

Correspondence between the “matched” odds ratios and the Mantel-Haenszel method
No. pairs Reserpine Case Control (a x d)/N (b x c)/N
+ 1 18
- 0 00 0
2
+ 1 045
- 0 11/2 0
2
+ 0 123
- 1 0 20 1/2
+ 0 0362
- 1 1 20 0
BREAST CANCER CASESYes No
Yes 8 23CONTROLS
No 45 362
(Adapted from Heinone et al, Lancet 2:675, 1974)
OR= 45/23= 1.96
OR??

OR MH
( ) ( ) ( ) ( )
( ) ( ) ( ) ( )
( )
( ).
1 02
81 1
24 5
0 02
2 30 1
23 6 2
1 02
80 0
24 5
1 12
2 30 1
23 6 2
1 12
4 5
1 12
2 3
4 52 3
1 9 6
BREAST CANCER CASESYes No
Yes 8 23CONTROLS
No 45 362OR= 45/23= 1.96
Reserpine Use and Breast Cancer

Stratification Methods• Advantages
– Easy to understand and compute
– Allow simultaneous assessment of interaction
• Disadvantages
– Cannot handle a large number of variables (zero cells are problematic in direct adjustment)
– Each calculation requires a rearrangement of tables