Embed Size (px)
Citation preview

Confidential: For Review O
nly
Diabetes treatments and risk of heart failure, cardiovascular
disease and all-cause mortality: cohort study in primary
care.
Journal: BMJ
Manuscript ID BMJ.2015.030247
Article Type: Research
BMJ Journal: BMJ
Date Submitted by the Author: 05-Nov-2015
Complete List of Authors: Hippisley-Cox, Julia; Nottingham University, General Practice Coupland, Carol; University of Nottingham, Division of Primary Care
Keywords: diabetes, heart failure, cardiovascular disease, glitazones, gliptins, QResearch, primary care, drug safety
https://mc.manuscriptcentral.com/bmj
BMJ

Confidential: For Review O
nly
Diabetes treatments and risk of heart failure, cardiovascular disease and all-
cause mortality: cohort study in primary care.
Presenting Original Research
Authors
Julia Hippisley-Cox Professor of Clinical Epidemiology & General Practice
Carol Coupland Associate Professor in Medical Statistics
Institution
1Division of Primary Care, 13
th floor, Tower Building, University Park, Nottingham, NG2 7RD,
UK
Author for correspondence
Julia Hippisley-Cox
Email: [email protected]
Telephone: +44 (0)115 8466915
Fax: +44 (0)115 8466904
Word count: 5,250 words
Page 1 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
1 Abstract
Objective
To assess associations between risks of cardiovascular disease, heart failure, and all-cause
mortality and different diabetes drugs in patients with type 2 diabetes, particularly newer
agents including gliptins or thiazolidinediones.
Design
Open cohort study.
Setting
1243 general practices contributing data to the QResearch database in England.
Participants
469,688 patients with type 2 diabetes aged 25-84 years between 01.04.2007 and
31.01.2015.
Exposures
Hypoglycaemic agents (thiazolidinediones; gliptins; metformin; sulphonylureas; insulin;
other) alone and in combination.
Main outcome measure
First recorded diagnoses of cardiovascular disease, heart failure and all-cause mortality
recorded on the patients primary care, mortality or hospital record. Cox proportional
hazards models were used to estimate hazard ratios for diabetes treatments adjusting for
potential confounders.
Results
In total 21,308 patients (4.5%) received prescriptions for thiazolidinediones and 32,533
(6.9%) received prescriptions for gliptins during follow-up.
Compared with non-use, gliptins were significantly associated with an 18% decreased risk of
all-cause mortality; a 14% decreased risk of heart failure and no significant change in risk of
cardiovascular disease; glitazones were significantly associated with a 23% decreased risk of
Page 2 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
all-cause mortality; a 26% decreased risk of heart failure and a 25% decreased risk of
cardiovascular disease.
Compared with no current treatment, there were no significant associations between
monotherapy with gliptins and risk of any complications. Dual therapy with gliptins and
metformin was associated with a decreased risk of all three outcomes (with reductions of
38% for heart failure; 33% for cardiovascular disease and 48% for all-cause mortality). Triple
therapy with metformin, sulphonylureas and gliptins was associated with a decreased risk of
all three outcomes (with reductions of 40% for heart failure; 30% for cardiovascular disease
and 51% for all-cause mortality).
Compared with no current treatment, thiazolidinediones monotherapy was associated with
a 50% decreased risk of heart failure; dual therapy with thiazolidinediones and metformin
was associated with a decreased risk of all three outcomes (with reductions of 50% for heart
failure; 54% for cardiovascular disease and 45% for all-cause mortality); dual therapy with
thiazolidinediones and sulphonylureas was associated with risk reductions of 35% for heart
failure and 25% for cardiovascular disease; triple therapy with metformin, sulphonylureas
and thiazolidinediones was associated with decreased risks of all three outcomes (with
reductions of 46% for heart failure; 41% for cardiovascular disease and 56% for all-cause
mortality).
Conclusions
We have found clinically important differences in risk of cardiovascular disease, heart failure
and all-cause mortality between different diabetes drugs alone and in combination. Overall,
use of gliptins or thiazolidinediones was associated with decreased risks of heart failure,
cardiovascular disease and all-cause mortality compared with non-use of these drugs. These
results, whilst subject to residual confounding, may have implications for prescribing of
hypoglycaemic drugs.
Page 3 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
2 Introduction
Cardiovascular disease and heart failure are major causes of morbidity and mortality in
patients with type 2 diabetes1 2
. Once heart failure is present in patients with diabetes,
there is a 10-fold increase in mortality and a 5 year survival of only 12.5%, a prognosis worse
than metastatic breast cancer2. A number of hypoglycaemic drugs have been associated
with an unexpected increased risk of heart failure both during clinical trials3 and post-
marketing surveillance raising concerns about the overall risks and benefits for patients4 5
.
Following its launch in 20006, rosiglitazone, the first drug in the ‘insulin sensitising’
thiazolidinedione class, was associated with an increased rate of heart failure5. This resulted
in its withdrawal from Europe, India, New Zealand and South Africa in 2010/2011.
Rosiglitazone, however, is still prescribed in the US - a controversial decision7 informed by
the open label ‘non-inferiority’ RECORD trial funded by the manufacturers of rosiglitazone4.
The RECORD study compared cardiovascular outcomes in 2220 people prescribed
rosiglitazone in combination with either metformin or sulphonylureas compared with 2227
prescribed both metformin and sulphonylureas between 2001 and 2008. Although the
numbers of events were low, the trial reported an increased risk of heart failure with
rosiglitazone and was unable to rule out an increased risk of myocardial infarction4. The
design, results and interpretation of this trial have been heavily criticised8.
Pioglitazone is another thiazolidinedione which decreases blood glucose levels. The placebo-
controlled PROactive trial of pioglitazone9 was also controversial in its design and
interpretation, largely because of the choice of composite endpoints10
. Whilst it failed to
clearly demonstrate improved cardiovascular outcomes for patients, it reported increased
hospital admissions for heart failure as an adverse effect9 as did a subsequent meta-analysis
of 8554 patients prescribed pioglitazone11
. Meanwhile, a Canadian cohort study comparing
pioglitazone and rosiglitazone between 2002-2008 reported a lower risk of heart failure and
death in pioglitazone users compared with rosiglitazone12
. Similarly a US cohort study
reported a lower risk of stroke, heart failure and all-cause mortality among patients
prescribed pioglitazone compared with rosiglitazone13
. Pioglitazone continues to be
Page 4 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
prescribed in the UK and the US although it has been withdrawn elsewhere due to concerns
regarding increased risk of bladder cancer14
.
Dipeptidyl peptidase 4 inhibitors (DPP-4), also known as gliptins, are a relatively new class of
hypoglycaemic drug which are included in international guidelines15
as second line agents
after metformin although data regarding long term clinical benefits and safety are
inconclusive16
. Saxagliptin, was associated with an unexpected increase in hospitalisation
due to heart failure during a placebo controlled clinical trial3. Sitagliptin was associated with
an increased risk of heart failure in a cohort study of 8,288 Taiwanese patients exposed to
sitagliptin over 1.5 years17
. Conversely a US cohort study of 8,032 sitagliptin users showed
no excess risk of hospital admission or death compared with other glucose lowering
agents18
. Whilst heart failure was included within the composite endpoint, it was not
evaluated separately. A meta-analysis of 25 trials of 7,726 patients receiving sitagliptin or a
comparator agent for between 12 weeks and 2 years was undertaken by the manufacturers
of sitagliptin19
. Whilst the composite study end points included major adverse
cardiovascular events (defined as ischaemic events or cardiovascular deaths), it did not
specifically evaluate risk of heart failure.
Uncertainty remains over the longer term comparative risks among patients prescribed
hypoglycaemics, particularly gliptins and glitazones alone and in combination with other
treatments20 21
. Regulatory agencies have responded to this uncertainty by requiring
evidence that new hypoglycaemic agencies are not associated with harmful increases in
cardiovascular events rather than the more stringent requirement that the drugs result in
evidence of clinical benefit22 23
.
Concerns have also been raised regarding the safety of an older class of oral hypoglycaemic
(sulphonylureas) since these have been linked with increased adverse cardiovascular events
in some5 but not all studies
24. The lifelong nature of diabetes, the marked increase in its,
incidence and prevalence, and prescribing recommendations in guidelines15
, mean that the
number of patients prescribed hypoglycaemic drugs is likely to increase. Given the
impracticability and ethical difficulties of a head-to-head trial comparing different agents,
there is a need to quantify risks of clinical outcomes in large representative populations of
Page 5 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
patients prescribed these drugs over longer periods of time. This information can
complement information from meta-analyses of clinical trials which, whilst valuable, tend to
suffer from publication bias, lack sufficient detail, duration of follow-up or sufficient power
to make relevant comparisons for unintended effects19 21
.
We therefore carried out a cohort study using a large UK primary care database with linked
GP, mortality and hospital admissions data to investigate the associations between different
classes of hypoglycaemic drugs and the risks of heart failure, cardiovascular disease and all-
cause mortality for patients with type 2 diabetes. We were particularly interested in the
risks associated with the newer agents including glitazones and gliptins. In a companion
paper25
, we report on a similar analysis examining risks of microvascular complications
(severe kidney disease, blindness, amputation), hyperglycaemic and hypoglycaemic coma
between different classes of diabetes drugs in patient with type 2 diabetes.
3 Methods (1250)
3.1 Setting and data source
We did a population based open cohort study of patients in England aged 25-84 years with a
diagnosis of type 2 diabetes.
3.2 Data source
We used a large population of primary care patients derived from version 40 of the
QResearch database (www.qresearch.org). QResearch is a continually updated patient level
pseudonymised database with event level data extending back to 1989. QResearch currently
includes clinical and demographic data from over 1243 general practices in England and two
practices in Scotland covering a population of over 24 million patients, collected in the
course of routine healthcare by general practitioners and associated staff. The primary care
data includes demographic information, diagnoses, prescriptions, referrals, laboratory
results and clinical values. Diagnoses are recorded using the Read code classification26
.
QResearch has been used for a wide range of clinical research including the assessment of
unintended effects of commonly prescribed medicines27-32
. The primary care data is linked
Page 6 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
at individual patient level to Hospital Episode Statistics (HES), and mortality records from
the Office for National Statistics (ONS). HES provides details of all National Health Service
(NHS) inpatient admissions since 1997 including primary and secondary causes coded using
the ICD-10 classifications and OPCS-4 codes for operations and interventions. ONS provides
details of all deaths in England with primary and underlying causes, also coded using the
ICD-10 classification. Patient records are linked using a project specific pseudonymised NHS
number which is valid and complete for 99.8% of primary care patients, 99.9% for ONS
mortality records and 98% for hospital admissions records1.
3.3 Inclusion and exclusion criteria
We included all QResearch practices in England who had been using their Egton Medical
Information Systems (EMIS) computer system for at least a year. We initially identified an
open cohort of patients aged 25-84 years registered with eligible practices between 01 April
2007 and 31st
January 2015. We chose this study period since both pioglitazone and gliptins
were available in the UK for the full study period. We then selected patients with diabetes if
they had a Read code for diabetes or more than one prescription for a hypoglycaemic drug.
We excluded patients as having type 1 diabetes if they had been diagnosed under the age of
35 and prescribed insulin33
. We also excluded patients without a postcode related
deprivation score. We determined an entry date to the cohort for each patient, which was
the latest of the following dates: date of diagnosis of diabetes; 25th
birthday; date of
registration with the practice plus one year; date on which the practice computer system
was installed plus one year; and the beginning of the study period. We used an incident user
design for patients prescribed glitazones, gliptins (our main exposures of interest) or insulin
to reduce bias34
. We defined incident users as patients without a prescription for these
drugs in the 12 months before the study entry date as in other studies18
and we excluded
people who had received any of these drugs in the previous 12 months. We included
prevalent users of metformin or sulphonylureas in the study cohort as if we had excluded
them this would have substantially reduced the numbers of new users of glitazones and
gliptins which were our main exposures of interest, since these are usually prescribed
following monotherapy with metformin or sulphonylureas. We also excluded patients with
Page 7 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
an existing diagnosis of an outcome of interest at the study entry date from the analysis of
that outcome. Patients were censored at the earliest date of the first recorded diagnosis of
the outcome of interest, death, deregistration with the practice, last upload of
computerised data or the study end date (31st
January 2015).
3.4 Outcome
Our primary outcomes were incident heart failure, cardiovascular disease, and all-cause
mortality recorded either in the patient’s primary care record, their linked hospital record or
mortality record.
3.4.1 Definition of outcomes
We used Read codes to identify recorded diagnoses of heart failure from the primary care
records (G58%, G5yy9, G5yyA, 662f, 662g, 662h and 662i). We used ICD-10 clinical codes
(I110, I130, I42 and I50) to identify incident cases of heart failure from hospital and
mortality records. We used the earliest recorded date of heart failure on any of the three
data sources as the index date for the diagnosis of heart failure.
Our definition of cardiovascular disease included coronary heart disease (angina and
myocardial infarction), stroke, or transient ischaemic attacks but not peripheral vascular
disease. The Read codes used for case identification on the primary care record are found in
the appendix. The ICD-10 codes used for case identification on the ONS death certificate or
hospital admission records were: angina pectoris(I20); acute myocardial infarction (I22);
complications following acute myocardial infarction (I23); other acute ischaemic heart
disease (I24); chronic ischaemic heart disease (I25); and ischaemic stroke (I63,I64) or
transient ischaemic attack (G45), We used the earliest recorded date of cardiovascular
disease on any of the three data sources as the index date for the diagnosis of
cardiovascular disease.
All-cause mortality was defined by the status of death recorded in the GP systems linked to
the date and cause of death as recorded on the ONS mortality record.
Page 8 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
3.5 Exposure data
Our primary exposures of interest were new use of gliptins and new use of glitazones during
the study period. We extracted details of all individual prescriptions for all types of
hypoglycaemics for each patient including the prescription date and the type. We
partitioned the follow-up time into different treatment periods, where each period
corresponded to treatment with a particular type or combination of hypoglycaemic drugs,
or could be a period of no treatment with any hypoglycaemic drugs. If the patient changed
to a different type of treatment or to a different combination of treatments we classified
that as a separate treatment period. For example, if the patient was prescribed metformin
alone on entry to the cohort for 12 months and then was prescribed both glitazones and
metformin for a further 24 months and then had a treatment free period for 6 months until
they were censored, the patient would have three treatment periods (metformin only for 12
months, metformin and glitazones for 24 months and no treatment for 6 months).
We determined the duration of each treatment period by calculating the number of days
between the earliest issue date and the latest issue date plus 90 days for the type of
treatment prescribed, or if another treatment was added before the initial treatment was
stopped then we calculated the duration of the treatment period on the initial treatment
alone to be the number of days between the earliest issue date for the initial treatment and
the earliest issue date for the next treatment. We added 90 days to the last prescription
date as an estimate of the date on which the patient stopped treatment (the “stop date”),
we made this assumption in order to allow for events which occur during a withdrawal
period to be attributed to the medication rather than counting as unexposed time. For the
analysis, for each treatment period we had six binary exposure variables to indicate
treatment with any of the diabetes drugs grouped into 6 drug classes – glitazones (including
rosiglitazone and pioglitazone) ; gliptins; metformin; sulphonylureas; insulin; other oral
hypoglycaemic agents (including α-glucosidase inhibitors, glinides, SGLT2 inhibitors, glinides,
guar). This allowed for patients to be on different combinations of these treatments drugs
during a treatment period. In order to further assess associations for different specific
treatment combinations (such as dual therapy with metformin and glitazones) we also
categorised treatments during each treatment period into one categorical variable with 21
Page 9 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
mutually exclusive treatment categories including a ‘no current treatment group’ and 20
categories for mono, dual and triple combinations of drugs.
3.6 Confounding variables
We considered confounding variables that were likely to be associated with the risk of the
diabetes complications35
18 36-38
or with the likelihood of receiving treatment for different
hypoglycaemic agents. These included: age at study entry; sex; number of years since
diagnosis of diabetes (categorised as <1 year; 1-3; 4-6; 7-10; ≥ 11 years)38
; calendar year;
smoking status (non-smoker; ex-smoker; light smoker: 1–9 cigarettes/day; moderate
smoker: 10–19 cigarettes/day; heavy smoker: ≥20 cigarettes/day; not recorded); ethnic
group (categorised as white/not recorded, Indian, Pakistani, Bangladeshi, other Asian, black
African, black Caribbean, Chinese, other including mixed)35
; Townsend deprivation score;
prior complications (severe kidney failure38
, one or more episodes of hyperglycaemia; one
or more episodes of hypoglycaemia; amputation; blindness); comorbidities (cardiovascular
disease38
(other than when cardiovascular disease was the outcome of interest), heart
failure (other than when heart failure was the outcome of interest), peripheral vascular
disease, valvular heart disease, chronic kidney disease, atrial fibrillation35
, hypertension35
,
rheumatoid arthritis35
), prescription drugs (statins, aspirin, anticoagulants, thiazides, ACE
inhibitors/angiotensin blockers, beta blockers, calcium channel blockers) and clinical values
(body mass index kg/m2
38, cholesterol/HDL ratio
35, systolic blood pressure
35, serum
creatinine, glycosylated haemoglobin HBA1C mmol/mol38 39
). We evaluated confounders at
the start of each treatment period for co-morbidities, other complications, other prescribed
medications, smoking status and clinical values. For co-morbidities and other complications
we identified whether patients had a diagnosis recorded prior to the relevant treatment
period. For prescribed medications, we defined patients as treated at the start of the
relevant diabetes drug treatment period if they had at least 2 prescriptions for the other
type of drug including one in the 28 days prior to treatment period and one after the start
date. For smoking status and continuous variables (systolic blood pressure, body mass
index, creatinine, cholesterol/HDL ratio and HBA1C), we used the most recent recorded
value immediately before the relevant treatment period.
Page 10 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
3.7 Analysis
We used Cox proportional hazards models to assess the associations between the six
different classes of hypoglycaemic drugs and risk of each of our three outcomes adjusting
for potential confounding variables. We used the Cox model for analysis rather than a
competing risks analysis as it is considered more appropriate for aetiological analyses such
as this study whereas competing risks analyses tend to be most useful for prediction
modelling or estimating absolute risks40-42
. To account for patients starting and stopping
different treatments and changing between treatments, we treated hypoglycaemic
exposures as time varying exposures. In the analysis we calculated unadjusted and adjusted
hazard ratios for the six different diabetes drug classes (each as a binary variable indicating
use or no use) with adjustment for the confounding variables and the other classes of
hypoglycaemic drugs. We also calculated unadjusted and adjusted hazard ratios for the
mutually exclusive treatment combinations comparing each treatment category with “no
current treatment”. To determine whether significant differences existed between classes
or individual drugs, we carried out Wald’s tests. We tested for interactions between the six
different drug classes and age, sex, HBA1C and body mass index. We used multiple
imputation with chained equations to replace missing values for continuous values and
smoking status and used these values in our main analyses43-45
. We did this for each of the
study outcomes and included the censoring indicator for the outcome, the log of survival
time, all the confounding variables and the diabetes drug treatment variables in the
imputation model. We log transformed body mass index, HbA1c, creatinine, cholesterol,
and high density lipoprotein cholesterol before imputation, as they had skewed
distributions. We carried out 5 imputations and combined results using Rubin’s rules.
To evaluate the robustness of our results and assess the impact of confounding variables we
added the confounding variables to our model in blocks and compared the adjusted hazard
ratios. The models we assessed were:
• Model A: diabetes drug classes adjusted for age, sex, ethnicity, deprivation, calendar
year, duration of diabetes plus other diabetes drugs
Page 11 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
• Model B: model A + comorbidities (hypertension; cardiovascular disease; heart
failure; atrial fibrillation; chronic kidney disease; rheumatoid arthritis; valvular heart
disease; peripheral vascular disease) + existing complications (history of
hypoglycaemia; hyperglycaemia; amputation; severe kidney failure; blindness) + use
of other drugs (statins, aspirin, anticoagulants, thiazides, ACE inhibitors/angiotensin
blockers, beta blockers, calcium channel blockers) Model C (primary analysis model):
model B + clinical values (body mass index, cholesterol/HDL ratio, systolic blood
pressure, serum creatinine, glycosylated haemoglobin)
• Model D: model C + interaction terms
• Model E: treatment combinations categorical variable plus confounders in model C.
We have presented this model with hazard ratios for each category compared with
no treatment in the main text of the paper and compared with metformin
monotherapy in supplementary table 3.
We also carried out a sensitivity analysis where we excluded prevalent users of
sulphonylureas from the study cohort so that the hazard ratios for sulphonylureas are based
on incident users, and we fitted the following models:
• Model F: model C having excluded prevalent users of sulphonylureas.
• Model G: model E having excluded prevalent users of sulphonylureas.
We used all the available data in the database to maximise the power and also
generalisability of the results. We used a P value of less than 0.01 (two tailed) to determine
statistical significance. We considered a hazard ratio of >= 1.10 or <=0.90 as clinically
important. We used STATA (version 13.1) for all analyses.
4 Results
4.1 Overall study population
Overall, 1243 QResearch®
practices in England met the inclusion criteria. As shown in figure
Page 12 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
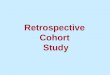
1, we identified a cohort of 601,405 patients aged 25-84 years with diabetes. We
sequentially excluded 31,224 patients with type 1 diabetes (5.1%), 748 patients (0.1%)
without a Townsend deprivation score and 99,745 patients prescribed glitazones or gliptins
or insulin in the 12 months prior to the study entry date leaving 469,688 patients with type
2 diabetes in the study cohort. Figure 1 also shows the numbers of patients with each
outcome at baseline who were excluded from the analysis of that outcome as well as the
numbers of incident outcomes observed during follow up.
4.2 Baseline characteristics
In total 274,324 (58.4%) of the patients in the study cohort received prescriptions for one or
more diabetes drugs during follow-up, with 21,308 (4.5%) receiving prescriptions for
glitazones, 32,533 (6.9%) receiving prescriptions for gliptins, 256,024 (54.5%) receiving
prescriptions for metformin, 134,570 (28.7%) receiving prescriptions for sulphonylureas,
19,791 (4.2%) receiving prescriptions for insulin, and 12,062 (2.6%) receiving prescriptions
for other oral hypoglycaemic agents.
Table 1 shows the characteristics of patients who started each of the 6 classes of diabetes
medication during follow up based on the last recorded value before the medication was
first prescribed (or at study entry for patients already prescribed sulphonylureas, metformin
or other hypoglycaemics at baseline). The groups were similar for most characteristics
except for higher levels of comorbidities other than hypertension in patients prescribed
insulin and lower levels of prescriptions for statins and aspirin in patients prescribed
metformin compared with the other drugs.
Table 2 shows levels of recording and mean values for HBA1C, body mass index,
cholesterol/HDL ratio, systolic blood pressure and serum creatinine prior to starting
medication. Highest levels of recording were for HBA1C which were in excess of 97% for all
six drug groups. Lowest levels of recording were for cholesterol/HDL ratios which were
above 84% for all drug groups. Overall, at least 82% of patients had complete data for each
clinical value across all drug groups. Apart from higher mean levels of HBA1C in patients
prior to exposure to insulin and the ‘other’ hypoglycaemic groups, and higher levels of
creatinine among those prescribed sulphonylureas or insulin, the mean values were similar
across the six groups. Supplementary table 1 shows mean values prior to starting the 20
Page 13 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
different treatment combinations. The mean values for HBA1C tended to be higher for
patients starting triple therapy (as high values of HBA1C will tend to trigger changes in
therapy).
4.3 Risks associated with use of each group of medication
Table 3 shows the number of incident cases of each outcome for patients during periods of
exposure to each of the six treatment classes during follow-up. It is important to note that
the treatment classes in Table 3 are not mutually exclusive – for example the row for
glitazones includes any use of glitazones, whether as monotherapy, dual therapy or triple
therapy. Similarly, the adjusted hazard ratios for model C shown in Table 3 give an overall
risk for the use of each drug group compared with non-use of that drug group, having
adjusted for use of other diabetes drugs and the potential confounders listed in the
footnote.
For our main exposures of interest we found:
• Compared with non-use, glitazones were significantly associated with a 23%
decreased risk of all-cause mortality; a 26% decreased risk of heart failure and a 25%
decreased risk of cardiovascular disease.
• Compared with non-use, gliptins were significantly associated with an 18%
decreased risk of all-cause mortality; a 14% decreased risk of heart failure and no
significant association with risk of cardiovascular disease.
In addition for the other diabetes drug groups we found that:
• Compared with non-use, metformin was associated with a significantly decreased
risk of all three outcomes – 41% decreased risk of all-cause mortality; a 30%
decreased risk of heart failure and a 24% decreased risk of cardiovascular disease.
• Compared with non-use, sulphonylureas were significantly associated with a 10%
increased risk of all-cause mortality.
• Compared with non-use, insulin was associated with a 47% increased risk of all-cause
mortality; a 32% increased risk of heart failure and a 23% increased risk of
cardiovascular disease.
Page 14 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
• Compared with non-use, the other hypoglycaemic group was significantly associated
with an 18% decreased risk of all-cause mortality.
For all-cause mortality, we found significant interactions between glitazones and both age
and HBA1C (Supplementary table 2; Model D) where the reduced risk of all-cause mortality
associated with glitazone use became less marked both with increasing age and with
increasing levels of HBA1C. Similarly, for cardiovascular disease, there were significant
interactions between glitazones and HBA1C, where the reduced risk of cardiovascular
disease associated with glitazone use became less marked with increasing levels of HBA1C.
We found similar interactions, both in magnitude and direction, for gliptins and both age
and HBA1C for all-cause mortality and between gliptins and HBA1C for cardiovascular
disease.
Supplementary table 2 also shows the results from analyses adding confounders in separate
blocks (models A and B). Generally, including comorbidities and existing complications in the
model (model B) tended to result in similar hazard ratios for gliptins and glitazones
(compared with model A). Further inclusion of clinical values (Table 3: model C) only
resulted in small changes to the hazard ratios. The sensitivity analysis excluding prevalent
users of sulphonylureas at study entry showed increases in adjusted hazard ratios for all-
cause mortality and cardiovascular disease for insulin (Supplementary table 2: model E
compared with model C) but similar hazard ratios for the other diabetes drugs for all three
outcomes.
Page 15 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
4.4 Risks associated with different treatment combinations
Table 4 shows a more detailed breakdown of 21 mutually exclusive treatment categories
including a ‘no current treatment group’ which included 0.7 million person years free of any
hypoglycaemic medication. The table shows the number of events for each clinical outcome
for each of the treatment categories.
Table 5 shows the corresponding adjusted hazard ratios for each treatment group category
compared with no current treatment. The key significant findings are (all compared with
periods of no hypoglycaemic treatment):
• There were no significant associations between monotherapy with gliptins and risk
of any complications. Dual therapy with gliptins and metformin was associated with
a decreased risk of all three outcomes (with reductions of 38% for heart failure; 33%
for cardiovascular disease and 48% for all-cause mortality). Triple therapy with
metformin, sulphonylureas and gliptins was associated with a decreased risk of all
three outcomes (with reductions of 40% for heart failure; 30% for cardiovascular
disease and 51% for all-cause mortality).
• Monotherapy with glitazones was associated with a 50% decreased risk of heart
failure. Dual therapy with glitazones and metformin was associated with a decreased
risk of all three outcomes (with reductions of 50% for heart failure; 54% for
cardiovascular disease and 45% for all-cause mortality). Dual therapy with
sulphonylureas and glitazones was associated with a decreased risk of two outcomes
(with reductions of 35% for heart failure and 25% for cardiovascular disease). Triple
therapy with metformin, sulphonylureas and glitazones was associated with a
decreased risk of all three outcomes (with reductions of 46% for heart failure; 41%
for cardiovascular disease and 56% for all-cause mortality).
Supplementary table 3 shows the results for the different treatment combinations
compared with metformin monotherapy alone (rather than compared with periods of no
treatment as above). The key findings for our two exposures of interest are:
Page 16 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
• Monotherapy with gliptins was associated with a 50% increased risk of
cardiovascular disease and an 86% increased risk of all-cause mortality; dual therapy
with gliptins and metformin was associated with a decreased risk of two outcomes
(with reductions of 13% for cardiovascular disease and 20% for all-cause mortality);
dual therapy with sulphonylureas and gliptins was associated with a 44% increased
risk of all-cause mortality and a borderline 27% increased risk of cardiovascular
disease; triple therapy with metformin, sulphonylureas and gliptins was associated
with a 24% decreased risk of all-cause mortality compared with metformin
monotherapy.
• Monotherapy with glitazones was not associated with an increased or decreased risk
of any outcome compared with metformin monotherapy; dual therapy with
glitazones and metformin was associated with a decreased risk of two outcomes
(with reductions of 26% for heart failure and 40% for cardiovascular disease) and a
borderline 14% decreased risk in all-cause mortality; dual therapy with
sulphonylureas and glitazones was associated with a 50% increased risk of all-cause
mortality; triple therapy with metformin, sulphonylureas and glitazones was
associated with a decreased risk of all three outcomes (with reductions of 21% for
heart failure; 22% for cardiovascular disease and 32% for all-cause mortality)
compared with metformin monotherapy.
Supplementary table 4 shows the results for the different treatment combinations
compared with periods of no treatment having dropped prevalent users of sulphonylureas
at study entry (model G). Overall the adjusted hazard ratios for glitazones and gliptins were
similar to those in Table 5 except confidence intervals were wider and there was no longer a
significant decrease inheart failure risk and cardiovascular disease among patients
prescribed dual therapy with sulphonylureas and glitazones.
Page 17 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
5 Discussion
5.1 Key findings
We have conducted a large cohort study of risks of cardiovascular disease, heart failure and
all-cause mortality associated with different diabetes drugs in patients with type 2 diabetes
attending for routine clinical care in the UK. Our companion paper25
presents the
corresponding analysis of other diabetes complications including blindness, amputation,
severe kidney failure, hyperglycaemia and hypoglycaemia. The approach we have taken
allows assessment of the relative benefits and hazards of diabetes drugs in a “real world”
clinical setting for a range of clinically important outcomes. It enables analysis of treatment
periods which are substantially longer than those reported in clinical trials9 including more
events than previous similar observational studies5 12
.
We have found clinically relevant differences between different diabetes drugs (alone and in
combination) in the risk of three key outcomes – heart failure, cardiovascular disease and
death – in patients with type 2 diabetes. Compared with non-use, glitazones were
significantly associated with decreased risk of all three 3 outcomes (all-cause mortality;
heart failure and cardiovascular disease), whilst use of gliptins were significantly associated
with a decreased risk of two outcomes (all-cause mortality; and heart failure) but no
significant change in risk of cardiovascular disease. Compared with periods of no treatment,
dual therapy (i.e. metformin + gliptins or metformin + glitazones) was associated with a
decreased risk of all three outcomes as was triple therapy with metformin, sulphonylureas
and either gliptins or glitazones.
However, since the use of gliptins and glitazones is usually recommended as a second line
treatment in combination with other agents such as metformin, the clinical question is
whether addition of gliptins or glitazones to metformin monotherapy is associated with net
benefit or net harm. Compared with metformin monotherapy, dual therapy (metformin +
glitazones) and triple therapy (metformin + sulphonylureas + glitazones) was associated
with decreased risk of all three outcomes (Supplementary Table 3). Dual therapy (metformin
+ gliptins) was associated with a decreased risk of cardiovascular disease and all-cause
Page 18 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
mortality compared with metformin monotherapy. Triple therapy ( metformin +
sulphonylureas + gliptins) was associated with a 24% increased risk of all-cause mortality
(Supplementary Table 3).
5.2 Gliptins
Our study included over 70,000 person years of exposure to gliptins from over 32,500
patients which represents one of the largest studies to date with over 4 times more gliptin
users than the previous observational study by Eurich et al18
. Our results differ from those
reported by Eurich et al, since we found that use of gliptins was associated with a reduction
in all-cause mortality compared with non-use of gliptins. We also found that dual treatment
(metformin + gliptins) and triple therapy (metformin + sulphonylureas + gliptins) appears to
be associated with lower risk of all-cause mortality compared with monotherapy with
metformin alone. The median duration of exposure to gliptins in our study was 5.7 years
compared with 2.5 years in the Eurich study18
and the mean age of our cohort was 63 years
compared with 52 years18
. We also had more events and more statistical power - there were
996 deaths during 71,524 person years of exposure to gliptins in our study compared with
32 deaths during 11,307 person years in the Eurich study18
.
Our results are broadly consistent with recent non-inferiority trials46
and meta-analyses of
randomized controlled trials reporting that various gliptins (alogliptin, dutogliptin,
linagliptin, saxagliptin, sitagliptin, and vildagliptin) are associated with statistically significant
30-60% reductions in major adverse cardiac events and non-significant 33% and 48%
reductions in all-cause and cardiovascular death compared with other active drugs or
placebo treatment47 48
. However Monami et al urge caution in interpreting the results since
the events were not the principle endpoints, the trial duration was short and the
characteristics of patients could be different from routine clinical practice48
.
The predominant gliptin prescribed in our dataset was sitagliptin which was prescribed to
80% of the gliptin users. There are currently too few patients prescribed linagliptin,
saxagliptin and vildagliptin to support separate analyses by individual drug which is a
limitation of the study since there may be differences between individual gliptins and their
Page 19 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
effect on HBA1C49
. However the numbers of patients on different types of gliptin is likely to
increase over time and further analyses can be undertaken once more data has accrued.
5.3 Glitazones
Our study included over 55,000 person years of exposure to glitazones arising from 21,308
patients. The predominant glitazone was pioglitazone which was prescribed to 90% of
glitazone users and hence our results most closely reflect associations for pioglitazone
rather than rosiglitazone (withdrawn in the UK in 2010). Our study is substantially larger
than a previous UK study of 92,000 patients with diabetes which finished in 20054 and
includes newer drugs available over the last decade. It supplements information from the
Canadian study12
which compared three outcomes (heart failure, myocardial infarction and
death) among 16,951 elderly users of pioglitazone compared with 22785 users of
rosiglitazone between 2002 and 2008. Our study is more recent and includes more patients
prescribed pioglitazone over a longer duration (mean exposure of 4.5 years in our study
compared with 294 days). It also includes more events – the Canadian study12
included 461
cases of heart failure, 273 of myocardial infarction and 377 deaths.
We have found significant reductions in two outcomes - cardiovascular disease and all-cause
mortality - among patients prescribed glitazones compared with non-use (Table 3). This
reduction is similar in magnitude to that reported in clinical trials and meta-analyses of
pioglitazone9 11
. In 2007, Lincoff et al reported a meta-analysis of 19 trials of pioglitazone
with a treatment duration ranging from 4 months to 3.5 years11
. The results showed an 18%
decreased risk of their composite primary outcome (risk of death, myocardial infarction or
stroke). However, we have reported a decreased risk of heart failure among patents
prescribed glitazones compared with non-use of glitazones. This contrasts with the increase
in heart failure which occurred in other studies without an associated increase in mortality9
11. The authors of the PROactive study partially attributed this finding to a diagnostic bias
due to the increase of oedema in the pioglitazone group9. Our observational study differs
from the clinical trial not only in design, size and setting, but also in the calendar time during
which it was conducted and in the selection of participants. For example, the PROactive
study9 selectively recruited high risk patients with pre-existing macrovascular disease
Page 20 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
whereas our study included a more representative population of patients from primary
care. Two thirds of patients In the PROactive study9
had evidence of myocardial infarction or
stroke compared with 14% in our study. It is also possible that patients in our study with
symptoms or signs suggestive of early heart failure (such as breathlessness or oedema) may
not have been prescribed pioglitazone or may have switched to another diabetes drug given
the growing concerns and subsequent withdrawal of rosiglitazone.
5.4 Strengths and limitations
5.4.1 Generalisability
To our knowledge this is the largest such study to date based on an ethnically diverse
contemporaneous, representative population of patients with type 2 diabetes during an 8
year study period. We included all eligible patients in order to minimise selection bias.
Hence we think the results are likely to be generalizable to similar populations of patients
with type 2 diabetes. Whilst our observational study has limitations inherent in its design
(see below) it also has advantages over meta-analyses of clinical trials since these tend to be
limited by ascertainment and reporting of events, short follow-up, lack of time to event data
and insufficient power to report on rare cardiovascular events21
.
5.4.2 Clinical outcomes
Strengths of our analysis are the inclusion of ‘hard’ clinical end points of cardiovascular
disease, heart failure and death based on clinical diagnoses recorded on at least one of
three linked electronic data sources. Use of all three linked data sources was designed to
minimise under-ascertainment of outcomes which would otherwise lead to under-
estimation of absolute risks. The CVD and heart failure outcomes are based on clinical
diagnoses made by the treating clinician rather than formally adjudicated events as would
occur in a clinical trial. Whilst it is possible therefore that some patients were recorded as
having heart failure or cardiovascular disease who did not have this condition, such
misclassification will not have affected the mortality outcome. UK general practices have
good levels of accuracy and completeness in recording clinical diagnoses and prescribed
medications50
. Also the diagnostic validity of such diagnoses in general practice has been
shown to be high51
. Possible ascertainment bias of outcomes is unlikely to vary according to
the type of hypoglycaemic prescribed so would not explain the associations we have found.
Page 21 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
5.4.3 Exposure to medication
We had detailed exposure information on hypoglycaemic agents prescribed throughout the
follow-up period enabling us to develop a detailed categorisation of drug exposure time into
21 different treatment groups including combinations of treatments. Recording of
prescriptions issued in UK general practices has very high levels of completeness52
. We
ascertained patient characteristics, concurrent medications, clinical values and diagnoses at
the beginning of each treatment period. This enabled us to account for switching between
different treatments or treatment combinations making adjustments for a large number of
potential confounders. We undertook a time varying analysis which analysed different types
of monotherapy, dual and triple therapy over the study period. This reflects ‘real world’
prescribing patterns over a long duration of time allowing multiple comparisons, not only
between drugs, but also between different combinations of drugs compared with untreated
periods of time (diet only treatment). Our study analysed prescribed medication rather
than the medication actually taken by the patients, although renewal of prescriptions is
likely to indicate drug use as patients need to initiate repeat prescriptions. This could result
in misclassification of exposure if patients were prescribed medication which they didn’t
actually take and could underestimate associations between diabetes drug use and clinical
outcomes. Unlike previous studies, we have included comparisons of risk against periods of
no treatment5 which is important since approximately 40% of patients with type 2 diabetes
are managed without hypoglycaemics treatments throughout follow-up.
5.4.4 Assessment of other types of bias
Other types of bias which can affect observational studies include recall bias, indication bias
and channelling bias. Recall bias will not have occurred since data on prescriptions for
hypoglycaemia and confounding variables was recorded prior to the clinical outcomes. We
restricted the study population to patients with type 2 diabetes in order to limit indication
bias (i.e. bias which occurs when patients are prescribed drugs for a condition which is itself
associated with the risk of the adverse event under consideration). We used an incident
user design to reduce confounding and biases that can otherwise arise from adjustment for
Page 22 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
intermediate characteristics in the causal path34
. There were some differences at baseline
between patients prescribed different treatment groups (Tables 1 & 2) though these were
predominantly increased levels of comorbidities for insulin and lower levels of concurrent
use of medication (such as statins and aspirin) for metformin. To reduce channelling bias
(where the choice of a particular drug is influenced by patient characteristics), we adjusted
for a wide range of potential confounding variables. This included demographic
characteristics (age, sex, ethnicity, and deprivation), different co-morbidities, clinical values
(including HBA1C, body mass index, blood pressure, and creatinine and cholesterol/HDL
ratio) and concurrent medication. However we are unable to exclude the possibility of
residual confounding since there may be other unmeasured patient characteristics which
affected selection of hypoglycaemic agents.
As in other similar studies18
, we excluded prevalent users of insulin at baseline but left
patients subsequently prescribed insulin in for the rest of the analysis as it is part of the
treatment ladder and some of these patients will also have had other medications of
interest during follow up. Whilst insulin was not the primary exposure of interest, we note
that patients prescribed insulin had higher risks of all three complications (Tables 3 and 5)
despite adjustment for higher levels of co-morbidity. It is unlikely that this is a direct result
of treatment with insulin. It could be because of residual confounding and ‘reverse causality’
i.e. the insulin-treated group is at much higher risk of complications than the groups treated
with diet or oral medication, and it is this that results in their apparently worse outcomes
and not their treatment with insulin. For example, in Table 2, the insulin-treated group has
the highest HBA1c and creatinine values prior to treatment, although both of these factors
were adjusted for in the analyses.
Although randomised controlled trials of hypoglycaemics are not influenced by residual
confounding, they tend to be small, of short duration, and may not report on relevant
clinical outcomes. An alternative design would be an observational study of a cohort of
patients specifically assembled for the purpose rather than routinely collected data as in our
study. Studies using routinely collected data are susceptible to missing data although in our
study, over 99% of patients had smoking status recorded, 87% had ethnic group recorded
and over 82% had of patients had complete data for all five clinical values (table 2). We also
used multiple imputation to impute missing data. Other problems with routine data include
Page 23 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
coding errors and variable timing between measurements of risk factors in patients because
of differences in when patients present to their GP. Advantages of using routinely collected
data rather than a purposeful cohort include size, efficiency, better generalisability and less
susceptibility to selection bias or attrition bias.
We fitted several different models and carried out sensitivity analyses which showed some
heterogeneity of results. The results are therefore sensitive to the assumptions made in the
study design and modelling and have uncertainty; however our findings were generally
consistent across the different analyses for glitazones and gliptins.
6 Conclusions
We have found clinically important differences in risk of CVD, heart failure and all-cause
mortality between different diabetes drugs alone and in combination compared with no
drug treatment. Overall, use of gliptins or glitazones was associated with decreased risk of
heart failure, cardiovascular disease or all-cause mortality compared with non-use of these
drugs. These results, whilst subject to residual confounding, may have implications for
prescribing of diabetes drugs.
7 Other information
7.1.1 Acknowledgements
We acknowledge the contribution of EMIS practices who contribute to the QResearch® and
EMIS and the University of Nottingham for expertise in establishing, developing and
supporting the database.
7.1.2 Approvals:
The project was reviewed in accordance with the QResearch® agreement with Trent Multi-
Centre Ethics Committee [reference 03/4/021].
Page 24 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
7.1.3 Contributorship
JHC initiated the study, undertook the literature review, data extraction, data manipulation
and primary data analysis and wrote the first draft of the paper. CC contributed to the
design, analysis, data manipulation, interpretation and drafting of the paper. Both authors
had access to all the data for this project.
7.1.4 Funding
There was no external funding for this project.
7.1.5 Competing Interests
All authors have completed the Unified Competing Interest form at
www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and
declare: JHC is professor of clinical epidemiology at the University of Nottingham and co-
director of QResearch® – a not-for-profit organisation which is a joint partnership between
the University of Nottingham and Egton Medical Information Systems (leading commercial
supplier of IT for 60% of general practices in the UK). JHC is also a paid director of ClinRisk
Ltd which produces open and closed source software to ensure the reliable and updatable
implementation of clinical risk algorithms within clinical computer systems to help improve
patient care. CC is associate professor of Medical Statistics at the University of Nottingham
and a paid consultant statistician for ClinRisk Ltd. This work and any views expressed within
it are solely those of the co-authors and not of any affiliated bodies or organisations.
7.1.6 Copyright
The Corresponding Author has the right to grant on behalf of all authors and does grant on
behalf of all authors, an exclusive licence (or non-exclusive for government employees) on a
worldwide basis to the BMJ Publishing Group Ltd, and its Licensees to permit this article (if
accepted) to be published in BMJ editions and any other BMJPGL products and to exploit all
subsidiary rights, as set out in our licence (bmj.com/advice/copyright.shtml).
7.1.7 Data Sharing
The patient level data from the QResearch are specifically licensed according to its
governance framework. See www.qresearch.org for further details.
Page 25 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
8 References
1. Health and Social Care Information Centre. National Diabetes Audit 2012-2013 Report 2 Complications and Mortality, 2014:37.
2. Khan SS, Butler J, Gheorghiade M. Management of comorbid diabetes mellitus and worsening heart failure. JAMA 2014;311(23):2379-80.
3. Scirica BM, Bhatt DL, Braunwald E, et al. Saxagliptin and Cardiovascular Outcomes in Patients with Type 2 Diabetes Mellitus. New England Journal of Medicine 2013;369(14):1317-26.
4. Home PD, Pocock SJ, Beck-Nielsen H, et al. Rosiglitazone evaluated for cardiovascular outcomes in oral agent combination therapy for type 2 diabetes (RECORD): a multicentre, randomised, open-label trial. Lancet 2009;373(9681):2125-35.
5. Tzoulaki I, Molokhia M, Curcin V, et al. Risk of cardiovascular disease and all cause mortality among patients with type 2 diabetes prescribed oral antidiabetes drugs: retrospective cohort study using UK general practice research database. 2009;339:4731.
6. NICE. Guidance on rosiglitazone for type 2 diabetes mellitus. London: National Institute for Clinical Excellence, 2000.
7. Cohen D. Insiders criticise FDA’s decision not to withdraw rosiglitazone, 2010. 8. Psaty BM, Furberg CD. The record on rosiglitazone and the risk of myocardial infarction.
N Engl J Med 2007;357(1):67-9. 9. Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondary prevention of macrovascular
events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised controlled trial. Lancet 2005;366(9493):1279-89.
10. Scheen AJ. Outcomes and lessons from the PROactive study. Diabetes Research and Clinical Practice 2012;98(2):175-86.
11. Lincoff AM, Wolski K, Nicholls SJ, et al. Pioglitazone and Risk of Cardiovascular Events in Patients With Type 2 Diabetes Mellitus: A Meta-analysis of Randomized Trials. JAMA 2007;298(10):1180-88.
12. Juurlink DN, Gomes T, Lipscombe LL, et al. Adverse cardiovascular events during treatment with pioglitazone and rosiglitazone: population based cohort study. 2009;339.
13. Graham DJ, Ouellet-Hellstrom R, MaCurdy TE, et al. RIsk of acute myocardial infarction, stroke, heart failure, and death in elderly medicare patients treated with rosiglitazone or pioglitazone. JAMA 2010;304(4):411-18.
14. Lewis JD, Ferrara A, Peng T, et al. Risk of Bladder Cancer Among Diabetic Patients Treated With Pioglitazone. Diabetes Care 2011;34(4):916-22.
15. Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2012;55(6):1577-96.
16. Karagiannis T, Boura P, Tsapas A. Safety of dipeptidyl peptidase 4 inhibitors: a perspective review. Therapeutic advances in drug safety 2014;5(3):138-46.
17. Wang KL, Liu CJ, Chao TF, et al. Sitagliptin and the risk of hospitalization for heart failure: a population-based study. Int J Cardiol 2014;177(1):86-90.
18. Eurich DT, Simpson S, Senthilselvan A, et al. Comparative safety and effectiveness of sitagliptin in patients with type 2 diabetes: retrospective population based cohort study. 2013;346.
19. Engel SS, Golm GT, Shapiro D, et al. Cardiovascular safety of sitagliptin in patients with type 2 diabetes mellitus: a pooled analysis. Cardiovascular diabetology 2013;12:3.
Page 26 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
20. Diamond GA, Bax L, Kaul S. Uncertain Effects of Rosiglitazone on the Risk for Myocardial Infarction and Cardiovascular Death. Ann Intern Med 2007:0000605-200710160-00182.
21. Hernandez AV, Walker E, Ioannidis JP, et al. Challenges in meta-analysis of randomized clinical trials for rare harmful cardiovascular events: the case of rosiglitazone. Am Heart J 2008;156(1):23-30.
22. Department of Health and Human Services FaDA, Center for Drug Evaluation and Research. Guidance for industry: diabetes mellitus— evaluating cardiovascular risk in new antidiabetic therapies to treat type 2 diabetes, 2008.
23. European Medicine Agency CfMPfHU. Guideline on clinical investigation of medicinal products in the treatment of diabetes mellitus, 2010.
24. Bell DS. Do sulfonylurea drugs increase the risk of cardiac events? CMAJ 2006;174(2):185-6.
25. Hippisley-Cox J, Coupland C. Diabetes treatments and risk of blindness, amputation, kidney failure, hypoglycaemia and hyperglycaemia : cohort study in primary care. BMJ (submitted) 2015.
26. Wikipedia. Readcodes. Secondary Readcodes 2015. http://en.wikipedia.org/wiki/Read_code.
27. Hippisley-Cox J, Coupland C. Risk of myocardial infarction in patients on Cox 2 inhibitors or conventional non-steroidal anti-inflammatory drugs: population based nested case control analysis. BMJ 2005;330:1366-74.
28. Hippisley-Cox J, Coupland C, Logan R. Risk of adverse gastrointestinal outcomes in patients taking cyclo-oxygenase-2 inhibitors or conventional non-steroidal anti-inflammatory drugs: population based nested case-control analysis. BMJ 2005;331(7528):1310-6.
29. Hippisley-Cox J, Coupland C. Unintended effects of statins in men and women in England and Wales: population based cohort study using the QResearch database. BMJ 2010;340:c2197.
30. Parker C, Coupland C, Hippisley-Cox J. Antipsychotic drugs and risk of venous thromboembolism: nested case-control study. BMJ 2010;341:c4245.
31. Vinogradova Y, Coupland C, Hippisley-Cox J. Exposure to bisphosphonates and risk of gastrointestinal cancers: series of nested case-control studies with QResearch and CPRD data. BMJ 2013;346:f114.
32. Coupland C, Hill T, Morriss R, et al. Antidepressant use and risk of suicide and attempted suicide or self harm in people aged 20 to 64: cohort study using a primary care database. BMJ 2015;350:h517.
33. Hippisley-Cox J, Pringle M. Prevalence, Care and Outcomes for patients with diet controlled diabetes in general practice: cross sectional survey. Lancet 2004;364:423-28.
34. Johnson ES, Bartman BA, Briesacher BA, et al. The incident user design in comparative effectiveness research. Pharmacoepidemiol Drug Saf 2013;22(1):1-6.
35. Hippisley-Cox J, Coupland C, Vinogradova Y, et al. Predicting cardiovascular risk in England and Wales: prospective derivation and validation of QRISK2. BMJ 2008:bmj.39609.449676.25.
36. Clarke PM, Gray AM, Briggs A, et al. A model to estimate the lifetime health outcomes of patients with type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS) Outcomes Model (UKPDS no. 68). Diabetologia 2004;47(10):1747-59.
37. Davis TME, Coleman RL, Holman RR, et al. Ethnicity and long-term vascular outcomes in Type 2 diabetes: a prospective observational study (UKPDS 83). Diabetic Medicine 2014;31(2):200-07.
38. Nichols GA, Gullion CM, Koro CE, et al. The Incidence of Congestive Heart Failure in Type 2 Diabetes: An update. Diabetes Care 2004;27(8):1879-84.
39. Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321(7258):405-12.
Page 27 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
40. Andersen PK, Geskus RB, de Witte T, et al. Competing risks in epidemiology: possibilities and pitfalls. International Journal of Epidemiology 2012;41(3):861-70.
41. Lau B, Cole SR, Gange SJ. Competing Risk Regression Models for Epidemiologic Data. American Journal of Epidemiology 2009.
42. Pintilie M. Analysing and interpreting competing risk data. Stat Med 2007;26(6):1360-7. 43. Steyerberg EW, van Veen M. Imputation is beneficial for handling missing data in
predictive models. J Epidemiol Community Health 2007;60:979. 44. Moons KGM, Donders RART, Stijnen T, et al. Using the outcome for imputation of
missing predictor values was preferred. J Epidemiol Community Health 2006;59:1092.
45. Schafer J, Graham J. Missing data: our view of the state of the art. Psychological Methods 2002;7:147 - 77.
46. Green JB, Bethel MA, Armstrong PW, et al. Effect of Sitagliptin on Cardiovascular Outcomes in Type 2 Diabetes. New England Journal of Medicine 2015;0(0):null.
47. Patil HR, Al Badarin FJ, Al Shami HA, et al. Meta-analysis of effect of dipeptidyl peptidase-4 inhibitors on cardiovascular risk in type 2 diabetes mellitus. Am J Cardiol 2012;110(6):826-33.
48. Monami M, Dicembrini I, Martelli D, et al. Safety of dipeptidyl peptidase-4 inhibitors: a meta-analysis of randomized clinical trials. Curr Med Res Opin 2011;27 Suppl 3:57-64.
49. Esposito K, Chiodini P, Maiorino MI, et al. A nomogram to estimate the HbA1c response to different DPP-4 inhibitors in type 2 diabetes: a systematic review and meta-analysis of 98 trials with 24 163 patients. BMJ Open 2015;5(2):e005892.
50. Majeed A. Sources, uses, strengths and limitations of data collected in primary care in England. Health Statistics Quarterly 2004(21):5-14.
51. Meier CR, Derby LE, Jick SS, et al. Antibiotics and risk of subsequent first-time acute myocardial infarction. JAMA 1999;281(5):427-31.
52. Majeed A. Sources, uses, strengths and limitations of data collected in primary care in England. HSQ 2004;21.
Page 28 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
Page 29 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
Patients aged 25-84 with
diabetes registered
1998-2015
N=601,405
Baseline cases of CVD
excluded N=93,224
Incident cases of CVD
N=26,434
Type 2 diabetes
(excluding prevalent
insulin/gliptins/glitazones
users)
N=469,688
Type 2 diabetes with
Townsend score recorded
N=569,433
Type 2 diabetes
N=570,181
Type 1 diabetes excluded
N=31,224
Type 2 diabetes prevalent
users of gliptins or
glitazones or insulin
excluded N=99,745
Deaths
N=52,476
Baseline cases heart
failure excluded
N=15,573
Incident cases of heart
failure
N=13,806
Type 2 diabetes without
Townsend score excluded
748
Page 30 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Table 1 Characteristics of patients with type 2 diabetes shown as numbers (percentages) unless stated otherwise. Values represent those recorded
prior to starting medication or at study entry for prevalent users. Treatment groups not mutually exclusive.
glitazones gliptins metformin sulphonylureas insulin Other
hypoglycaemics
total patients exposed 21308 32533 256024 134570 19791 12062
Median years exposed 4.5 5.7 4.8 4.9 5.9 4.9
mean age at study entry (SD) 63.0 (11.9) 63.3 (12.1) 64.6 (13.1) 66.2 (12.9) 64.5 (12.7) 60.0 (11.9)
Mean Townsend score (SD) 0.4 (3.5) 0.5 (3.5) 0.6 (3.6) 0.6 (3.6) 0.5 (3.6) 0.8 (3.6)
Male 12658 (59.4) 18871 (58.0) 146690 (57.3) 79284 (58.9) 11499 (58.1) 6509 (54.0)
Ethnicity recorded 19130 (89.8) 29396 (90.4) 228962 (89.4) 119507 (88.8) 17264 (87.2) 10947 (90.8)
White or not recorded 17112 (80.3) 26104 (80.2) 204915 (80.0) 107537 (79.9) 17001 (85.9) 10135 (84.0)
Indian 997 (4.7) 1662 (5.1) 11732 (4.6) 5978 (4.4) 476 (2.4) 420 (3.5)
Pakistani 811 (3.8) 1132 (3.5) 7425 (2.9) 3972 (3.0) 389 (2.0) 290 (2.4)
Bangladeshi 586 (2.8) 713 (2.2) 7282 (2.8) 3980 (3.0) 370 (1.9) 374 (3.1)
Other Asian 476 (2.2) 720 (2.2) 5873 (2.3) 2947 (2.2) 234 (1.2) 164 (1.4)
Caribbean 473 (2.2) 795 (2.4) 6376 (2.5) 3700 (2.7) 549 (2.8) 278 (2.3)
Black African 392 (1.8) 676 (2.1) 5715 (2.2) 2977 (2.2) 350 (1.8) 161 (1.3)
Chinese 84 (0.4) 95 (0.3) 983 (0.4) 513 (0.4) 36 (0.2) 34 (0.3)
Other 377 (1.8) 636 (2.0) 5723 (2.2) 2966 (2.2) 386 (2.0) 206 (1.7)
Smoking status recorded 21215 (99.6) 32399 (99.6) 255186 (99.7) 134080 (99.6) 19569 (98.9) 12003 (99.5)
non smoker 11374 (53.4) 17116 (52.6) 132634 (51.8) 69849 (51.9) 9393 (47.5) 6126 (50.8)
Ex-smoker 6252 (29.3) 9725 (29.9) 78935 (30.8) 41438 (30.8) 6142 (31.0) 3726 (30.9)
light smoker 2170 (10.2) 3358 (10.3) 25678 (10.0) 13846 (10.3) 2413 (12.2) 1252 (10.4)
moderate smoker 730 (3.4) 1121 (3.4) 9395 (3.7) 4661 (3.5) 832 (4.2) 441 (3.7)
heavy smoker 689 (3.2) 1079 (3.3) 8544 (3.3) 4286 (3.2) 789 (4.0) 458 (3.8)
Comorbidities
Page 31 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only Page 2
cardiovascular disease 2962 (13.9) 5325 (16.4) 48066 (18.8) 28895 (21.5) 4596 (23.2) 1992 (16.5)
heart failure 302 (1.4) 737 (2.3) 6943 (2.7) 5069 (3.8) 960 (4.9) 374 (3.1)
peripheral vascular disease 1008 (4.7) 1576 (4.8) 12458 (4.9) 8467 (6.3) 1519 (7.7) 544 (4.5)
valvular heart disease 379 (1.8) 914 (2.8) 7378 (2.9) 4606 (3.4) 765 (3.9) 292 (2.4)
hypertension 12520 (58.8) 19293 (59.3) 150219 (58.7) 80776 (60.0) 11117 (56.2) 7310 (60.6)
atrial fibrillation 929 (4.4) 1980 (6.1) 17327 (6.8) 10574 (7.9) 1890 (9.5) 657 (5.4)
chronic kidney disease 388 (1.8) 593 (1.8) 3067 (1.2) 4183 (3.1) 1165 (5.9) 224 (1.9)
rheumatoid arthritis 719 (3.4) 1237 (3.8) 9718 (3.8) 5382 (4.0) 842 (4.3) 460 (3.8)
Prior complications
Existing severe kidney disease 54 (0.3) 74 (0.2) 509 (0.2) 825 (0.6) 213 (1.1) 36 (0.3)
Existing blindness 260 (1.2) 383 (1.2) 3715 (1.5) 2404 (1.8) 360 (1.8) 170 (1.4)
existing amputation 85 (0.4) 125 (0.4) 1239 (0.5) 894 (0.7) 161 (0.8) 65 (0.5)
1+ prior episode of hypoglycaemia 288 (1.4) 286 (0.9) 2247 (0.9) 1946 (1.4) 337 (1.7) 215 (1.8)
1+ prior episode of hyperglycaemia 7921 (37.2) 10054 (30.9) 68839 (26.9) 46341 (34.4) 7279 (36.8) 3914 (32.4)
Other medications
anticoagulation 642 (3.0) 1419 (4.4) 9409 (3.7) 5989 (4.5) 1344 (6.8) 540 (4.5)
thiazides 3444 (16.2) 4346 (13.4) 31291 (12.2) 16972 (12.6) 2386 (12.1) 1844 (15.3)
ACE inhibitors 9318 (43.7) 12939 (39.8) 83847 (32.7) 48960 (36.4) 7750 (39.2) 5362 (44.5)
Angiotension 2 blockers 3399 (16.0) 4895 (15.0) 28629 (11.2) 16976 (12.6) 2633 (13.3) 2088 (17.3)
calcium channel blockers 5613 (26.3) 8105 (24.9) 55674 (21.7) 32141 (23.9) 5034 (25.4) 3328 (27.6)
statins 15512 (72.8) 21383 (65.7) 137574 (53.7) 77865 (57.9) 12640 (63.9) 8451 (70.1)
aspirin 7890 (37.0) 9684 (29.8) 68013 (26.6) 41647 (30.9) 7057 (35.7) 4096 (34.0)
Page 32 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only Page 3
Table 2 Recorded clinical values prior to starting medication or at study entry for prevalent users. Treatment groups not mutually exclusive.
glitazones gliptins metformin sulphonylureas insulin Other hypo
Total patients exposed 21308 32533 256024 134570 19791 12062
values recorded (%)
HBA1C 21251 (99.7) 32474 (99.8) 253219 (98.9) 133170 (99.0) 19255 (97.3) 12022 (99.7)
BMI 21120 (99.1) 32224 (99.1) 252290 (98.5) 132477 (98.4) 19436 (98.2) 11749 (97.4)
cholesterol/HDL 18264 (85.7) 29307 (90.1) 224504 (87.7) 115991 (86.2) 16723 (84.5) 10619 (88.0)
systolic blood pressure 21306 (100.0) 32529 (100.0) 255892 (99.9) 134487 (99.9) 19765 (99.9) 12057 (100.0)
creatinine 21288 (99.9) 32509 (99.9) 255381 (99.7) 134244 (99.8) 19655 (99.3) 12044 (99.9)
all above values recorded 18097 (84.9) 29010 (89.2) 220119 (86.0) 113843 (84.6) 16270 (82.2) 10340 (85.7)
mean values (SD)
HBA1C mmol/mol 66.8 (18.9) 68.4 (18.4) 61.4 (18.7) 64.9 (19.9) 75.4 (22.7) 70.9 (19.6)
BMI kg/m2 31.7 (6.0) 31.7 (5.9) 30.6 (5.9) 30.1 (5.8) 30.2 (6.1) 34.1 (6.6)
cholesterol/HDL ratio 3.8 (1.3) 3.9 (1.3) 3.8 (1.3) 3.8 (1.3) 4.0 (1.4) 4.0 (1.3)
SBP mmHg 133.1 (14.8) 132.3 (14.7) 132.5 (15.3) 132.8 (15.9) 131.7 (16.9) 132.5 (14.9)
creatinine 87.1 (33.7) 84.9 (33.3) 84.8 (30.1) 92.1 (47.7) 99.3 (62.0) 83.5 (34.6)
Page 33 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyTable 3 Adjusted hazard ratio with 95% confidence intervals for each outcome by use of diabetes
drug.
cases pyrs rate per
10,000
Adjusted HR (95% CI)
model C ±
All-cause mortality glitazones§ 597 55,916 106.8 0.77 (0.71 to 0.84 )
gliptins§ 996 71,524 139.3 0.82 (0.77 to 0.88 )
metformin§ 17,109 1,066,516 160.4 0.59 (0.58 to 0.60 )
sulphonylureas§ 12,717 506,719 251.0 1.10 (1.07 to 1.12 )
insulin§ 2,529 57,875 437.0 1.47 (1.41 to 1.53 )
other hypoglycaemic§ 350 28,293 123.7 0.82 (0.73 to 0.91 )
Heart failure glitazones§ 308 55,051 56.0 0.74 (0.66 to 0.83 )
gliptins§ 421 68,724 61.3 0.86 (0.78 to 0.95 )
metformin§ 6,785 1,029,331 65.9 0.70 (0.68 to 0.73 )
sulphonylureas§ 4,415 481,339 91.7 1.04 (1.00 to 1.08 )
insulin§ 686 52,634 130.3 1.32 (1.22 to 1.43 )
other hypoglycaemic 192 26,950 71.2 0.92 (0.79 to 1.06 )
Cardiovascular disease glitazones§ 699 47,374 147.6 0.75 (0.69 to 0.81 )
gliptins§ 912 56,414 161.7 0.94 (0.88 to 1.00 )
metformin§ 14,218 834,914 170.3 0.76 (0.74 to 0.78 )
sulphonylureas§ 7,999 378,816 211.2 1.00 (0.97 to 1.03 )
insulin§ 985 39,870 247.1 1.23 (1.15 to 1.31 )
other hypoglycaemic§ 396 22,152 178.8 0.95 (0.86 to 1.05 )
Notes significantly increased HR shown in red; significantly decreased HR shown in green; non-significant results are shown in
black. ±Model C Hazard ratios adjusted for the following: sex; age; calendar year; duration since diagnosis of diabetes (5 levels);
ethnicity (9 levels) Townsend deprivation score; smoking status (5 levels); use of other diabetes drugs; use of anticoagulants,
thiazide, ace, angiotensin 2 blockers; calcium channel blockers; statins; aspirin; existing complications (blindness,
hyperglycaemia; hypoglycaemia; amputation; severe kidney failure); hypertension; cardiovascular disease; atrial fibrillation;
chronic renal disease; rheumatoid arthritis; valvular heart disease; peripheral vascular disease; body mass index; systolic
blood pressure; HBA1C; serum creatinine; cholesterol/HDL ratio
Page 34 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyTable 4 number of incident events for each outcome & person-years exposure to mutually
exclusive treatment groups
Heart failure Cardiovascular
disease
All-cause mortality
cases pyrs cases pyrs cases pyrs
Periods with no treatment 5,317 675,598 9,769 541,445 27,367 707,183
Monotherapy
Metformin alone 3,334 570,230 7,376 464,698 9,815 589,353
Sulphonylureas alone 1,211 82,466 1,752 59,918 5,654 90,846
Insulin alone 220 14,802 290 11,408 1,349 16,859
Glitazones alone 9 1,671 24 1,352 48 1,704
Gliptins alone 23 2,361 43 1,874 112 2,560
Other diabetes treatments alone 18 1,474 31 1,168 72 1,618
Dual therapy
Metformin & sulphonylureas 2,439 304,023 4,772 242,136 5,350 316,576
Metformin & insulin 189 17,328 262 13,153 399 18,540
Metformin & glitazones 75 17,825 160 15,742 163 18,024
Metformin & gliptins 114 23,530 263 19,898 257 24,218
Metformin & other hypo 60 9,009 119 7,479 85 9,375
Triple therapy
Sulphonylureas & insulin 94 3,756 100 2,558 369 4,593
Sulphonylureas & glitazones 37 3,444 59 2,691 114 3,564
Sulphonylureas & gliptins 47 4,068 71 2,988 164 4,451
Sulphonylureas & other hypo 21 973 22 765 46 1,096
Metformin, sulphonylureas & insulin 123 10,893 212 8,209 283 11,593
Metformin, sulphonylureas & glitazones 133 24,790 344 21,295 209 25,168
Metformin, sulphonylureas & gliptins 181 30,617 412 24,885 355 31,762
Metformin, sulphonylureas & other 60 9,636 127 7,902 87 10,070
All other drug combinations 101 13,519 226 11,160 178 14,127
Total 13,806 1,822,013 26,434 1,462,724 52,476 1,903,280
Page 35 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyTable 5 Adjusted hazard ratio with 95% confidence intervals for each outcome (model F).
Heart failure† Cardiovascular
disease †
All-cause mortality†
Adjusted HR Adjusted HR Adjusted HR
No current treatment 1.00 1.00 1.00
Monotherapy
Metformin alone± 0.68 (0.65 to 0.71 ) 0.76 (0.74 to 0.79 ) 0.64 (0.63 to 0.66 )
Sulphonylureas alone± 1.00 (0.94 to 1.07 ) 1.00 (0.95 to 1.05 ) 1.24 (1.20 to 1.28 )
Insulin alone± 1.26 (1.10 to 1.44 ) 1.22 (1.08 to 1.37 ) 1.64 (1.55 to 1.74 )
Glitazones alone± 0.50 (0.26 to 0.97 ) 0.79 (0.53 to 1.18 ) 0.89 (0.67 to 1.18 )
Gliptins alone± 0.87 (0.58 to 1.31 ) 1.14 (0.85 to 1.54 ) 1.20 (1.00 to 1.44 )
Other drugs alone± 0.92 (0.58 to 1.46 ) 1.12 (0.79 to 1.59 ) 1.06 (0.84 to 1.33 )
Dual therapy
Metformin & sulphonylureas± 0.74 (0.70 to 0.78 ) 0.75 (0.73 to 0.78 ) 0.62 (0.60 to 0.64 )
Metformin & insulin± 1.08 (0.93 to 1.25 ) 0.89 (0.78 to 1.01 ) 0.76 (0.69 to 0.84 )
Metformin and glitazones± 0.50 (0.40 to 0.63 ) 0.46 (0.39 to 0.54 ) 0.55 (0.47 to 0.64 )
Metformin and gliptins± 0.62 (0.52 to 0.75 ) 0.67 (0.59 to 0.75 ) 0.52 (0.46 to 0.59 )
Metformin and other hypo± 0.74 (0.57 to 0.95 ) 0.73 (0.61 to 0.88 ) 0.46 (0.37 to 0.57 )
Sulphonylureas and insulin± 1.18 (0.96 to 1.45 ) 1.18 (0.96 to 1.44 ) 1.49 (1.35 to 1.66 )
Sulphonylureas and glitazones± 0.65 (0.47 to 0.89 ) 0.75 (0.58 to 0.98 ) 0.96 (0.80 to 1.16 )
Sulphonylureas and gliptins± 0.88 (0.66 to 1.17 ) 0.97 (0.76 to 1.22 ) 0.92 (0.79 to 1.08 )
Sulphonylureas and other hypo± 1.46 (0.95 to 2.24 ) 1.02 (0.67 to 1.55 ) 1.33 (1.00 to 1.78 )
Triple therapy
Metformin, sulphonylureas and insulin± 0.91 (0.76 to 1.09 ) 0.95 (0.82 to 1.09 ) 0.98 (0.87 to 1.10 )
Metformin, sulphonylureas and glitazones± 0.54 (0.45 to 0.64 ) 0.59 (0.53 to 0.66 ) 0.44 (0.38 to 0.50 )
Metformin, sulphonylureas and gliptins± 0.60 (0.52 to 0.70 ) 0.70 (0.63 to 0.78 ) 0.49 (0.44 to 0.55 )
Metformin, sulphonylureas and other hypo± 0.60 (0.46 to 0.77 ) 0.62 (0.52 to 0.74 ) 0.46 (0.37 to 0.57 )
All other drug combinations± 0.72 (0.59 to 0.88 ) 0.82 (0.72 to 0.94 ) 0.68 (0.58 to 0.79 )
± compared with periods not on any treatment.
Notes: significantly increased HR shown in red; significantly decreased HR shown in green; non-significant results shown in
black.
†Hazard raCos adjusted for the following: sex; age; calendar year; duraCon since diagnosis of diabetes (5 levels); ethnicity (9
levels) Townsend deprivation score, smoking status (5 levels); use of other diabetes drugs; use of anticoagulant thiazide ace
angiotensin 2 blockers; calcium channel blockers; statins; aspirin; existing complications (blindness, hyperglycaemic coma;
hypoglycaemia; amputation; severe kidney failure); hypertension; cardiovascular disease; atrial fibrillation; chronic renal
disease; rheumatoid arthritis; valvular heart disease; peripheral vascular disease; body mass index; systolic blood pressure;
HBA1C; serum creatinine; cholesterol/HDL ratio
Page 36 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Supplementary table 1 Mean values prior to starting different medication combinations
age Townsend
score
HBA1C
mmol/mol
BMI kg/m2 Cholester
ol/HDL
ratio
SBP
mmHg
Creatinine
mol/l
No treatment 64.6 0.4 57.6 30.5 3.9 132.7 87.9
Monotherapy
Metformin alone 64.1 0.5 60.0 30.8 3.8 132.3 83.2
Sulphonylureas alone 70.5 0.4 63.1 28.8 3.8 132.2 110.8
Insulin alone 66.4 0.3 66.6 29.6 3.9 130.2 118.5
Glitazones alone 66.8 -0.2 59.3 32.0 3.8 133.3 101.4
Gliptins alone 67.8 0.1 63.5 31.2 3.9 131.5 98.3
Other diabetes treatments alone 63.7 0.7 63.2 32.3 4.0 132.3 100.6
Dual therapy
Metformin and sulphonylureas 65.5 0.7 65.3 30.3 3.8 132.9 87.7
Metformin and insulin 63.5 0.6 69.4 31.1 3.9 131.7 87.4
Metformin and glitazones 61.2 0.1 63.0 32.6 3.8 132.8 82.5
Metformin and gliptins 61.8 0.3 65.2 32.2 3.8 131.7 80.4
Metformin and other hypo 59.3 0.7 66.1 34.1 3.9 131.6 79.6
Sulphonylureas and insulin 70.7 0.3 74.4 29.2 4.0 131.2 134.2
Sulphonylureas and glitazones 70.2 0.1 65.9 31.0 3.8 133.4 112.8
Sulphonylureas and gliptins 70.0 0.2 70.2 30.7 3.9 132.5 105.9
Sulphonylureas and other hypo 66.0 0.4 70.6 32.8 4.1 131.4 106.7
Triple therapy
Metformin, sulphonylureas and insulin 65.0 0.6 76.2 30.3 3.9 132.2 90.8
Metformin, sulphonylureas and glitazones 63.3 0.5 68.2 31.3 3.8 133.3 86.5
Metformin, sulphonylureas and gliptins 63.5 0.7 70.4 31.3 3.8 132.4 83.6
Metformin, sulphonylureas and other hypo 60.4 0.8 72.7 33.8 4.0 132.5 81.8
All other drug combinations 61.6 0.5 73.2 32.5 3.9 132.5 86.5
Page 37 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only Page 2
Supplementary Table 2. Adjusted hazard ratio (95% CI) for each outcome (models A, B, D and E)
Adjusted HR
model A ±
Adjusted HR
model B ±
Adjusted HR
model D †
Adjusted HR
model E±
All-cause mortality Glitazones 0.57 (0.53 to 0.62 ) 0.73 (0.67 to 0.79 ) 0.68 (0.61 to 0.77 ) 0.76 (0.67 to 0.86 )
Gliptins 0.73 (0.69 to 0.78 ) 0.81 (0.76 to 0.86 ) 0.71 (0.65 to 0.78 ) 0.80 (0.73 to 0.87 )
Metformin 0.43 (0.42 to 0.44 ) 0.57 (0.56 to 0.58 ) 0.48 (0.47 to 0.50 ) 0.62 (0.61 to 0.64 )
Sulphonylureas 0.95 (0.93 to 0.97 ) 1.09 (1.07 to 1.12 ) 1.31 (1.27 to 1.36 ) 1.21 (1.17 to 1.25 )
Insulin 1.45 (1.39 to 1.51 ) 1.44 (1.38 to 1.50 ) 1.57 (1.49 to 1.66 ) 2.16 (2.04 to 2.30 )
other hypo 0.67 (0.61 to 0.75 ) 0.77 (0.69 to 0.86 ) 0.82 (0.73 to 0.91 ) 0.80 (0.69 to 0.93 )
Gliptins*age 1.016 (1.010 to 1.022 )
Gliptins*HBA1C 1.008 (1.004 to 1.011 )
Glitazones*age 1.016 (1.007 to 1.024 )
Glitazones*HBA1C 1.007 (1.003 to 1.012 )
Insulin*age 0.991 (0.987 to 0.994 )
Insulin*HBA1C 1.010 (1.008 to 1.012 )
Metformin*age 1.018 (1.016 to 1.020 )
Metformin*BMI 1.017 (1.013 to 1.020 )
Metformin*HBA1C 0.996 (0.995 to 0.997 )
Sulphonylureas*age 0.987 (0.985 to 0.989 )
Heart failure Glitazones 0.80 (0.71 to 0.90 ) 0.79 (0.71 to 0.89 ) 0.74 (0.66 to 0.83 ) 0.66 (0.55 to 0.79 )
Gliptins 0.92 (0.83 to 1.01 ) 0.85 (0.77 to 0.93 ) 0.86 (0.78 to 0.95 ) 0.86 (0.75 to 0.98 )
Metformin 0.76 (0.73 to 0.79 ) 0.69 (0.67 to 0.72 ) 0.63 (0.59 to 0.66 ) 0.70 (0.67 to 0.73 )
Sulphonylureas 1.20 (1.16 to 1.25 ) 1.00 (0.96 to 1.04 ) 1.14 (1.07 to 1.20 ) 1.08 (1.01 to 1.15 )
Insulin 1.68 (1.55 to 1.82 ) 1.31 (1.21 to 1.42 ) 1.33 (1.22 to 1.44 ) 1.56 (1.37 to 1.78 )
Other hypo 1.09 (0.94 to 1.26 ) 0.94 (0.81 to 1.08 ) 0.91 (0.79 to 1.05 ) 0.91 (0.74 to 1.12 )
Metformin*age 1.010 (1.007 to 1.014 )
Page 38 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only Page 3
Metformin*BMI 1.013 (1.007 to 1.019 )
Sulphonylureas*age 0.993 (0.989 to 0.996 )
cardiovascular
disease
Glitazones 0.81 (0.75 to 0.87 ) 0.72 (0.66 to 0.77 ) 0.75 (0.69 to 0.81 ) 0.69 (0.61 to 0.77 )
Gliptins 0.99 (0.93 to 1.06 ) 0.91 (0.85 to 0.98 ) 0.92 (0.86 to 0.99 ) 0.90 (0.82 to 0.98 )
Metformin 0.86 (0.84 to 0.89 ) 0.73 (0.71 to 0.75 ) 0.75 (0.72 to 0.77 ) 0.76 (0.74 to 0.79 )
Sulphonylureas 1.15 (1.12 to 1.19 ) 1.00 (0.97 to 1.03 ) 1.00 (0.98 to 1.04 ) 1.05 (1.01 to 1.10 )
Insulin 1.39 (1.31 to 1.48 ) 1.21 (1.13 to 1.29 ) 1.09 (1.02 to 1.18 ) 1.23 (1.11 to 1.37 )
Other hypo 1.06 (0.96 to 1.17 ) 0.91 (0.82 to 1.00 ) 0.94 (0.85 to 1.04 ) 0.99 (0.86 to 1.13 )
Gliptins*HBA1C 1.008 (1.004 to 1.011 )
Glitazones*HBA1C 1.007 (1.003 to 1.012 )
Insulin*HBA1C 1.018 (1.015 to 1.021 )
Metformin*HBA1C 0.997 (0.996 to 0.999 )
Model A: adjusted for age, sex, ethnicity, deprivation, calendar year, duration of diabetes plus other diabetes drugs
Model B: model A + comorbidities (hypertension; cardiovascular disease; atrial fibrillation; chronic renal disease; rheumatoid arthritis; valvular heart disease;
peripheral vascular disease) + existing complications (history of hypoglycaemia; hyperglycaemia; amputation; severe kidney disease; blindness) + use of other drugs
(statins, aspirin, anticoagulants, diuretics, ACE inhibitors/angiotensin blockers, beta blockers, calcium channel blockers)
Model C (main paper): model B + clinical values (body mass index, cholesterol/HDL ratio, systolic blood pressure, serum creatinine, glycosylated haemoglobin)
Model D: model C + interaction terms shown in the table
Model E model C having excluded prevalent users of sulphonylureas
Page 39 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlySupplementary table 3 Adjusted hazard ratio with 95% confidence intervals for each outcome
(model F) except compared to monotherapy with metformin.
Heart failure† Cardiovascular
disease †
All-cause mortality†
Adjusted HR Adjusted HR Adjusted HR
Monotherapy or no medication
Metformin alone± 1.00 (1.00 to 1.00 ) 1.00 (1.00 to 1.00 ) 1.00 (1.00 to 1.00 )
No current treatment 1.47 (1.40 to 1.53 ) 1.31 (1.27 to 1.35 ) 1.55 (1.52 to 1.59 )
Sulphonylureas alone± 1.47 (1.37 to 1.57 ) 1.31 (1.24 to 1.38 ) 1.93 (1.87 to 2.00 )
Insulin alone± 1.85 (1.61 to 2.12 ) 1.59 (1.41 to 1.80 ) 2.55 (2.41 to 2.71 )
Glitazones alone± 0.74 (0.38 to 1.42 ) 1.03 (0.69 to 1.54 ) 1.38 (1.04 to 1.83 )
Gliptins alone± 1.28 (0.85 to 1.92 ) 1.50 (1.11 to 2.02 ) 1.86 (1.55 to 2.25 )
Other drugs alone± 1.35 (0.85 to 2.14 ) 1.47 (1.03 to 2.09 ) 1.65 (1.31 to 2.08 )
Dual therapy
Metformin & sulphonylureas± 1.09 (1.03 to 1.15 ) 0.99 (0.95 to 1.03 ) 0.96 (0.93 to 0.99 )
Metformin & insulin± 1.58 (1.36 to 1.83 ) 1.16 (1.03 to 1.32 ) 1.18 (1.07 to 1.31 )
Metformin and glitazones± 0.74 (0.58 to 0.93 ) 0.60 (0.51 to 0.70 ) 0.86 (0.74 to 1.00 )
Metformin and gliptins± 0.91 (0.76 to 1.10 ) 0.87 (0.77 to 0.99 ) 0.80 (0.71 to 0.91 )
Metformin and other hypo± 1.08 (0.84 to 1.40 ) 0.96 (0.80 to 1.15 ) 0.72 (0.58 to 0.89 )
Sulphonylureas and insulin± 1.73 (1.41 to 2.13 ) 1.54 (1.26 to 1.88 ) 2.32 (2.09 to 2.58 )
Sulphonylureas and glitazones± 0.95 (0.68 to 1.31 ) 0.99 (0.76 to 1.28 ) 1.50 (1.24 to 1.80 )
Sulphonylureas and gliptins± 1.29 (0.96 to 1.72 ) 1.27 (1.00 to 1.60 ) 1.44 (1.23 to 1.68 )
Sulphonylureas and other hypo± 2.13 (1.39 to 3.28 ) 1.33 (0.87 to 2.03 ) 2.07 (1.55 to 2.77 )
Triple therapy
Metformin, sulphonylureas and insulin± 1.34 (1.11 to 1.60 ) 1.24 (1.08 to 1.42 ) 1.53 (1.35 to 1.72 )
Metformin, sulphonylureas and glitazones± 0.79 (0.66 to 0.93 ) 0.78 (0.70 to 0.87 ) 0.68 (0.59 to 0.78 )
Metformin, sulphonylureas and gliptins± 0.89 (0.76 to 1.03 ) 0.92 (0.83 to 1.02 ) 0.76 (0.69 to 0.85 )
Metformin, sulphonylureas and other hypo± 0.87 (0.68 to 1.13 ) 0.81 (0.68 to 0.97 ) 0.71 (0.58 to 0.88 )
All other drug combinations± 1.06 (0.86 to 1.29 ) 1.07 (0.94 to 1.23 ) 1.05 (0.91 to 1.22 )
± compared with periods not on any treatment.
Notes: significantly increased HR shown in red; significantly decreased HR shown in green; non-significant results shown in
black.
†Hazard ra@os adjusted for the following: sex; age; calendar year; dura@on since diagnosis of diabetes (5 levels); ethnicity (9
levels) Townsend deprivation score, smoking status (5 levels); use of other diabetes drugs; use of anticoagulant thiazide ace
angiotensin 2 blockers; calcium channel blockers; statins; aspirin; existing complications (blindness, hyperglycaemic coma;
hypoglycaemia; amputation; severe kidney failure); hypertension; cardiovascular disease; atrial fibrillation; chronic renal
disease; rheumatoid arthritis; valvular heart disease; peripheral vascular disease; body mass index; systolic blood pressure;
HBA1C; serum creatinine; cholesterol/HDL ratio
Page 40 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
Supplementary table 4 Adjusted hazard ratio with 95% confidence intervals for each outcome
having prevalent users of sulphonylureas (model G). Treatment categories are mutually exclusive.
Adjusted HR
heart failure†
Adjusted HR
Cardiovascular
disease †
Adjusted HR
all-cause mortality†
No treatment 1.00 1.00 1.00
monotherapy
Metformin alone± 0.70 (0.67 to 0.73 ) 0.77 (0.75 to 0.80 ) 0.65 (0.64 to 0.67 )
Sulphonylureas alone± 1.16 (1.04 to 1.29 ) 1.12 (1.02 to 1.23 ) 1.50 (1.43 to 1.58 )
Insulin alone± 1.45 (1.18 to 1.78 ) 1.07 (0.90 to 1.27 ) 2.27 (2.10 to 2.45 )
Glitazones alone± 0.34 (0.14 to 0.81 ) 0.66 (0.42 to 1.05 ) 0.77 (0.54 to 1.09 )
Gliptins alone± 0.79 (0.49 to 1.28 ) 1.17 (0.84 to 1.63 ) 0.99 (0.78 to 1.26 )
Other drugs alone± 0.88 (0.50 to 1.55 ) 1.00 (0.66 to 1.51 ) 1.02 (0.78 to 1.34 )
Dual therapy
Metformin & sulphonylureas± 0.75 (0.69 to 0.82 ) 0.78 (0.74 to 0.83 ) 0.65 (0.62 to 0.69 )
Metformin & insulin± 1.25 (0.99 to 1.58 ) 0.89 (0.73 to 1.09 ) 1.18 (1.02 to 1.37 )
Metformin and glitazones± 0.49 (0.38 to 0.63 ) 0.47 (0.40 to 0.55 ) 0.58 (0.49 to 0.68 )
Metformin and gliptins± 0.68 (0.56 to 0.83 ) 0.69 (0.61 to 0.79 ) 0.54 (0.47 to 0.62 )
Metformin and other hypo± 0.80 (0.61 to 1.05 ) 0.73 (0.60 to 0.90 ) 0.54 (0.43 to 0.68 )
Sulphonylureas and insulin± 1.02 (0.59 to 1.76 ) 1.73 (1.21 to 2.47 ) 2.71 (2.25 to 3.27 )
Sulphonylureas and glitazones± 0.83 (0.46 to 1.50 ) 0.82 (0.51 to 1.32 ) 0.80 (0.53 to 1.21 )
Sulphonylureas and gliptins± 0.68 (0.40 to 1.14 ) 0.79 (0.53 to 1.18 ) 0.85 (0.65 to 1.11 )
Sulphonylureas and other hypo± 0.34 (0.05 to 2.38 ) 1.66 (0.83 to 3.33 ) 1.41 (0.76 to 2.62 )
Triple therapy
Metformin, sulphonylureas and insulin± 1.42 (1.00 to 2.01 ) 1.13 (0.84 to 1.50 ) 1.87 (1.52 to 2.30 )
Metformin, sulphonylureas and glitazones± 0.54 (0.37 to 0.79 ) 0.66 (0.53 to 0.82 ) 0.46 (0.34 to 0.62 )
Metformin, sulphonylureas and gliptins± 0.60 (0.46 to 0.79 ) 0.65 (0.55 to 0.77 ) 0.54 (0.45 to 0.65 )
Metformin, sulphonylureas and other hypo± 0.47 (0.26 to 0.85 ) 0.63 (0.43 to 0.90 ) 0.39 (0.23 to 0.64 )
All other drug combinations± 0.63 (0.44 to 0.88 ) 0.85 (0.69 to 1.04 ) 0.73 (0.58 to 0.92 )
± compared with periods not on any treatment.
†Hazard ratios adjusted for the following: sex; age; calendar year, duration since diagnosis of diabetes (5 levels);
ethnicity (9 levels) Townsend deprivation score smoking status (5 levels) use of anticoagulant thiazide ace
angiotensin 2 blockers; calcium channel blockers; statins; aspirin; existing complications (blindness,
hyperglycaemic coma; hypoglycaemia; amputation; severe kidney failure); hypertension; cardiovascular disease;
atrial fibrillation; chronic renal disease; rheumatoid arthritis; valvular heart disease; peripheral vascular disease;
body mass index; systolic blood pressure; HBA1C; serum creatinine; cholesterol/HDL ratio.
Page 41 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015.
BMJ.2015.028426 entitled "Diabetes treatments and risk of heart failure, cardiovascular
disease and all-cause mortality: cohort study in primary care."
Thank you for sending us your paper. We read it with interest but I regret to say that we
have decided not to publish it in the BMJ. The comments of the reviewers did not convince
us we could take these manuscripts further. You will notice that one reviewer looked at the
two companion papers you submitted. I thought this was necessary because the papers
reference each other. One our statistical consultants also reviewed the paper and echoed
many of the concerns raised by the reviewers and found that substantial re-analyses of the
data were needed to address the concerns of the reviewers. In addition, he wondered if you
see any chance to address confounding by indication on the individual drug selection,
compared to another one, and if there model is robust against introducing bias in a
counterfactual sense (so in contrast to marginal structural models). This is a very complex
data analyses and I echo that many concerns raised by the reviewers. I find it very difficult in
this setting to "pick" on the lowest associated risk with adverse outcomes. For all treatment
the confounder set is the same although the main question is why one drug is used over the
other. The Cox model may be appropriate but in a time-varying setting, I am concerned
about introducing bias in this setting. Of course the topic is of importance and the
observational setting is good. Nevertheless, I believe that the authors need to conduct a
very large amount of re-analyses to address the concerns of the reviewers. From my side, I
would like to ask the authors if they see any chance to address confounding by indication on
the individual drug selection, compared to another one and if there model is robust against
introducing This question may also be addressed by thinking of potential interaction
between confounders (so, for example, age and gender).
Authors’ response: Thank you for these comments and for considering an appeal. We have
undertaken substantial re-analyses of the data to address the issues raised by the reviewers
and statistical editor. We have answered each of the reviewers’ comments point by point
below but have summarized the key changes here for ease of reference.
In particular,
1. We have selected an open cohort of patients between 2007 and 2015 rather than the
original 18 year period of 1998-2015. This represents a period when gliptins and
pioglitazone were available for the full study period.
2. We have excluded prevalent users of insulin at baseline (in addition to having already
excluded prevalent users of gliptins and glitazones as in the original analysis).
3. We have adjusted for calendar year in the model. This, together with the shorter time
period for the study, reduces confounding by calendar year/differences in recording of
risk factors/changing patterns of drug use/ trends in outcomes.
4. We have adjusted hazard ratios for each of the 3 outcomes (heart failure,
cardiovascular disease, all-cause mortality) for the presence of other complications
(hypoglycaemia, hyperglycaemia, severe renal failure, amputation and blindness) to the
start of each treatment period to reduce confounding by indication on individual drug
selection. Also the hazard ratio for heart failure is adjusted for cardiovascular disease
and vice versa. This is in addition to the adjustment for a large list of confounders in our
original analyses (which were largely based on those in the paper by Eurich et al1
Page 42 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015. Page 2
examining comparative safety and effectiveness of sitagliptin published in the BMJ in
2013)
5. We have tested for interactions between drug exposure and confounders including age,
sex, HBA1C and BMI. We found several significant interactions with age and HBA1C
which we have described in the results section. We have included these significant
interactions in the supplementary tables (supplementary Table 2, model D).
6. We have presented additional analyses having excluded prevalent users of
sulphonylureas at baseline (so that the hazard ratios for sulphonylureas are based on
new users). We didn’t exclude prevalent users of sulphonylureas from our main
analyses as this would have substantially reduced the numbers of new users of
glitazones and gliptins which were our main exposures of interest, since they are mainly
prescribed as second line treatment.
7. We have added supplementary tables with the mean clinical values for each treatment
combination prior to starting it. There are some differences in these values - for
example, the mean values for HBA1C tend to be higher for patients starting triple
therapy (as high values of HBA1C will tend to trigger changes in therapy) – which
justifies our inclusion of these values in the models.
8. We have amended our main conclusions, abstract and key messages to reflect the
primary focus of the paper on gliptins and glitazones and offered more cautious
comments regarding associations found for sulphonylureas and insulin.
9. We have provided more detail in the methodology, justifying decisions made on the
approach taken
10. We have provided more detailed consideration of the limitations of the approaches
used in the Discussion as suggested by Fumiaki Imamura
Reviewer: 1 Timothy Davis, Professor of Medicine, University of Western Australia
The main issue with retrospective administrative database analyses such as this one is
prescription bias introduced by perceived or actual adverse effects of therapies,
convenience of administration, and efficacy. This can give rise to paradoxical results - in this
case a lower incidence of heart failure in pioglitazone-treated patients which is contrary to
both the biological effect of the drug (increased sodium resorption from the renal tubule)
and robust clinical (including trial) data. In addition, metformin use as first line therapy will
bias against bad outcomes given that the patients are relatively early in their disease -
duration of diabetes is included in the Cox models but the reliability of this estimate in
primary care may well be questionable as some GPs may document the date of first
attendance at the practice as the start of diabetes. By contrast, insulin (mostly because it is
injected therapy) is introduced relatively late when complications may well be established
although not yet clinically evident. Gliptins could be viewed as relatively weak blood
glucose-lowering agents in comparison with other second line drugs and thus not
considered for patients with poor glycaemic control and thus a greater risk of complications.
As a result, the clinical implications of the data are questionable at best. The size of the
database is impressive but it would be useful to know whether there has been any
validation of the accuracy of the variables (such as duration). Some idea of medication
adherence would also be valuable but this may not be available.
Page 43 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015. Page 3
The last concern relates to important within-class differences. Recent evidence from the
TECOS trial suggests that sitagliptin is less likely to cause heart failure than saxagliptin within
the DPP4 inhibitor class of drugs, while gliclazide is likely to be safer than the longer acting
sulphonylureas which have renally excreted active metabolites (such as glibenclamide and
glimepiride).The differences between drugs, although highly statistically significant because
of the numbers, appear mostly relatively modest and influenced by factors which were
beyond the range of confounders used in the multivariate analyses. Inconsistencies in the
results relative to a range of other data, including mechanistic studies, erode the credibility
of the analyses.
Authors’ response:
We have no reason to believe that the date of diagnosis of diabetes or duration since
diagnosis is inaccurate. Since 2004, UK general practitioners have been required to keep
accurate diabetes registers based on computer recorded clinical codes as part of the
National Quality and Outcomes framework. The registers rely on clinical coding of diabetes
and the associated date to identify patients with diabetes rather than issued prescriptions
especially since only 60% of patients with a diagnosis of diabetes are prescribed diabetes
drugs. As stated in the methods (section 3.3) patients were eligible for inclusion in the
cohort after they had been registered with the practice for at least 12 months making it
unlikely that the date of diagnosis would be the date of first attendance at the practice or
the first date of prescription for diabetes drugs. Even if there were some inaccuracies in the
recording of the date of first recorded diagnosis, there is no reason to think this would be
differential between different types of diabetes medication.
We agree that insulin may be used among patients with more severe disease. For this
reason, we excluded prevalent users of insulin from the study. We have also included a
discussion of the potential biases, confounding by indication and reverse causality in the
discussion (section 5.4.3).
We have also included additional tables of the characteristics of patients starting each type
of medication (Table 1, 2 and supplementary table 2) with these variables included as
potential confounders in the analysis and also undertaken new analysis to test for
interactions between clinical values and age and sex. We have presented these in
Supplementary table 2, model D. We agree with reviewer 2 that we have taken account of
the major confounders. However since all observational studies are subject to residual
confounding, we have highlighted this in the abstract, results, discussion and conclusion
Our main exposures of interest in this study were gliptins and glitazone and we have
updated the introduction, methods, results and discussion to highlight the focus of our
study. We have clarified in the discussion (section 5) that during this study period, 80% of
gliptin prescriptions were for sitagliptin and 90% of glitazone prescriptions were for
pioglitazone which limited the analyses we could undertake by individual drug. We have
included reference to the TECOS trial in the discussion.
In our original analysis, we reported that rosiglitazone was associated with a 9-13%
increased risk of heart failure whereas pioglitazone was associated with an 18% decreased
Page 44 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015. Page 4
risk of heart failure. This is consistent with observational studies comparing pioglitazone
with rosiglitazone2 3
. In our revised analysis, we have reported on a later period (2007-2015)
during which pioglitazone accounted for approximately 90% of glitazone prescriptions since
rosiglitazone was withdrawn in 2010. Hence there is insufficient data to make a comparison
between the two. While both rosiglitazone and pioglitazone have been associated with
heart failure4
5, the extent to which this is a class effect remains unclear
3. Juurlink et al
summarised a number of reasons why the risk of heart failure with rosiglitazone may be
higher than that reported for rosiglitazone3: Pioglitazone has more favourable effects on
serum lipids ; may impart anti-inflammatory and anti-atherogenic effects; it is less likely to
cause glitazone-induced salt and water retention. There are also differences between the
patients included in our study and the much higher risk patients included in the pioglitazone
trials – we have added a discussion of this to section 5.3.
Reviewer: 2 Richard Lehman
This is a study which should change practice in a domain which currently accounts for over
10% of the NHS budget. It is an article of major global importance.
Authors’ response: Thank you for these comments
As the authors repeatedly state, observational outcome data of this kind cannot prove
causality but constitute the best evidence currently available to inform practice in this area.
They have carried out a very large study from a database which although imperfect is not
likely to be systematically biased in its recording of the outcomes in question. Data about
prescribing are likely to be highly accurate.
Authors’ response: Thank you for these comments.
This complex analysis appears to have been undertaken thoroughly and appropriately by a
highly regarded team. Reporting is clear, and as well as giving a well-structured account of
the findings, the article provides a very comprehensive review of the issues and of
comparable studies.
Authors’ response: Thank you for these comments
Randomised controlled trials of single and combined treatments for type 2 diabetes are
extremely problematic because of the necessary duration and the effect of other
concomitant treatments, so this paper is likely to be a major determinant of prescribing
policy in the UK and the world over coming years. Because of its importance for several
hundred million people, it will come under close scrutiny but I believe that its methods and
findings are sound. In particular, I think that there has been comprehensive consideration of
all important confounders. Ideally there will be replication studies using other comparable
databases both in the UK and elsewhere, but even taken singly, this study is an important
step forward in understanding the effect of glucose-lowering treatment as part of the
management of this condition.
Authors’ response: We agree with these comments as mentioned above. In particular, we
believe we have made comprehensive considerations of all important confounders.
An accompanying editorial should explore its strengths and limitations, and attempt to place
glucose-lowering treatment in the wider context of risk reduction in people labelled as
Page 45 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015. Page 5
having type 2 diabetes. My only concern about this excellent study is that it will confirm
clinicians in their glucocentric view of what is meant by the treatment of type 2 diabetes.
Authors’ response: Thank you for these comments
Reviewer: 3. Fumiaki Imamura
Job Title: Senior investigator scientist. MRC Epidemiology Unit, University of Cambridge
I appreciate the opportunity of reviewing the important manuscript. The topic is clinically
important, stimulating further research and helping understand what is going on in clinical
practice. Thorough considerations of underlying limitations would be helpful:
1. The sample size reduces errors in estimation, but that is independent of potential
bias. Huge sample size with bias would give wrong clinical implications, and thus description
of potential bias should be much more emphasized. The followings may deserve thorough
consideration.
Authors’ response: We have expanded the section on potential biases in the discussion on
strengths and limitations.
i) The authors failed to interpret potential heterogeneity of the associations of interest.
For example, while the use of sulphonylurea was positively associated with higher incidence
of cardiovascular diseases, inverse association was seen when the authors excluded those
adults treated with any hypoglycaemic drugs (Suppl Table 1). HR (95% confidence interval)
for all-cause mortality in all person-years was 1.07 (1.06-1.08); in person-years without
exposure to any hypoglycaemic drugs, 0.78 (0.77-0.78). Sulphonylureas also showed
heterogeneity by time. HR (95% CI) for CVD was 1.13 (1.12 to 1.14) over 2000-2010. But, HR
during 2007-2015 was 1.00 (0.99 to 1.01). The latter indicates no harm of using
sulphonylureas for CVD in recent years.
Authors’ response: We have re-run the analyses based on an open cohort of patients
between 2007 and 2015 rather than the original 18 year period of 1998-2015. This
represents a period when gliptins and pioglitazone were available for the full study period.
There was a less of a difference in hazard ratios in the new analysis when the study period is
shorter and the results are adjusted for calendar year and other factors as described above.
We have added text to the discussion (section 5.3.4) to ensure readers understand that the
results are sensitive to modelling and have uncertainty.
As indicated above, we have presented additional analyses having excluded prevalent users
of sulphonylureas at baseline (so that the hazard ratios for sulphonylureas are based on new
users). We didn’t exclude prevalent users of sulphonylureas from our main analyses as this
would have substantially reduced the numbers of new users of glitazones and gliptins which
were our main exposures of interest, since they are mainly prescribed as second line
treatment.
The authors argued, “The results are broadly comparable with those in Table 3” on Page 13
of 44. This statement is invalid. The authors must highlight results that appeared not to be
robust.
Page 46 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015. Page 6
Authors’ response: We have updated the text of the results with the new analyses and also
highlighted the heterogeneity of the results as suggested (section 5.3.4. of Discussion):
Some of the lack of robustness or heterogeneity are clearly important for clinical
implications. For example, if the associations varied by time, findings in recent years were
more relevant to the current clinical practice, than those in earlier period of time. The
authors must reconsider and provide proper interpretation, rather than just saying “broadly
similar”.
Authors’ response: We agree that there may be confounding due to calendar time, and our
original analyses may not have fully accounted for changes over time. We have now
restricted the main analysis to the more recent time period 2007-2015 rather than the
original 18 year time period starting in 1998. We have also adjusted for calendar year in the
model. This reduces confounding by calendar year/differences in recording of risk
factors/trends in outcomes and is also then based on a period when gliptins were available
for the full study period.
The abstract and the main text do not discuss these findings. The lack of robustness of some
of the findings should be informed in the abstract, the results and the discussion, including
the last paragraph.
Author response: we have highlighted these findings as suggested in the abstract, results
and discussion.
In Table 3, the authors should clarify which HR was not constant over time: asterisk or
dagger, for instance.
ii) The authors raised an issue of residual confounding. The question is how big the
issue is. The authors must indicate it. In Table 3, HR based on different models should be
presented, not only the single adjusted model. Two or more HRs can tell readers how
estimated HRs could change by adjusting for different covariates. That is one indication of
robustness of the study results. Crude HR, estimated by using N of cases and person-years
(Table 4), could be estimated and indicated that some confounding was remarkable. For
example, for all-cause mortality, crude HR was 0.83 (0.82 to 0.84) while adjusted HR=1.07
(1.06 to 1.08). For CVD and heart failure, adjustment substantially attenuated the
associations by 25% to 50%. These differences indicate substantial degrees of confounding,
although the authors’ adjustment was not sufficient (residual confounding due to lack of
information on some unmeasured confounders such as compliance / general lifestyle /
other factors). The authors should present this kind of difference, so that readers can
recognise how variable results could be by including different variables.
Author’s response: Please see above. Also we have added further analyses showing models
adjusted for different subsets of confounding variables. We have also tested for interactions
between diabetes medications and potential confounders such as age and sex, HBA1C and
BMI and have included significant interaction terms in the final models.
These are:
• Model A: diabetes drug classes adjusted for age, sex, ethnicity, deprivation, calendar
year, duration of diabetes plus other diabetes drugs
Page 47 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015. Page 7
• Model B: model A + comorbidities (hypertension; cardiovascular disease; heart
failure; atrial fibrillation; chronic renal disease; rheumatoid arthritis; valvular heart
disease; peripheral vascular disease) + existing complications (history of
hypoglycaemia; hyperglycaemia; amputation; severe kidney disease; blindness) + use
of other drugs (statins, aspirin, anticoagulants, diuretics, ACE inhibitors/angiotensin
blockers, beta blockers, calcium channel blockers)
• Model C: model B + clinical values (body mass index, cholesterol/HDL ratio, systolic
blood pressure, serum creatinine, glycosylated haemoglobin)
• Model D: model C + interaction terms
• Model E: treatment combinations categorical variable plus confounders in model C.
Model F: model C having excluded prevalent users of sulphonylureas.
• Model G: model E having excluded prevalent users of sulphonylureas.
Models C and E are presented in the main paper. Models A, B, D, F and G are all presented
in the supplementary tables alongside one another for ease of reference. We have also
presented model E with hazard ratios for each category compared with metformin
monotherapy rather than no treatment in supplementary table 3
iii) The authors argued strength of repeated measures of drug use and covariates. Yet,
the authors made arbitrary decisions. The decisions might be justifiable, but it remains
unclear if the decisions were the best. The decisions include:
a. The authors assumed 90-day treatment period for any drugs if the follow-up
clinical visit indicated a stop of the treatment (Page 9). The decision made for the
person-years exposed is not clear and not justified.
Authors’ response: In line with similar studies of drug exposure using GP
databases6-8
, we made this assumption in order to allow for events which occur
during a withdrawal period to be attributed to the medication rather than
counting as unexposed time. We have added this to the methods.
b. The authors assumed that confounders for a treatment at one time point were
variables observed at the same time point or the others (BMI, blood pressure,
creatinine, blood lipids, and HbA1c) observed in a previous clinical record (page
9). Time-varying factors are richer than used. For example, dual therapy is likely
to happen after mono-therapy, but not adjusted for such prior treatment
decisions. Also, a certain outcome may determine future drug use: for instance,
onset of hypoglycaemia may alter drug treatments later and risk of the outcomes
examined. The authors’ decision of multivariable adjustment is likely to be
suboptimal.
Author response: We have updated section 3.6 of the methods to clarify that
confounders were evaluated at the start of each treatment period for co-
morbidities, other complications (including prior diagnoses of CVD, heart failure,
hypoglycemia, hyperglycaemia, amputation, blindness, severe kidney failure),
other prescribed medication, smoking status and clinical values.
c. Different scientists would think of it differently. The authors at least provide
different results that together could convince anyone familiar with different
Page 48 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015. Page 8
issues in observational research. Indeed, those results must be presented as a
part of sensitivity analysis. Sensitivity analysis just for a few stratification is little
helpful.
Authors’ response: Please see reply above - we have presented 7 models with
different blocks of confounders and different selection criteria to address this.
iv)The authors assume that associations of drug use with incidence of diabetes
complications are consistent across subgroups of a patient population. Validity of the
assumption is questionable, given variations of patients’ characteristics. The authors indeed
identified heterogeneity of associations over time or by hypoglycaemic drug.
The authors have very strong advantage of the large sample size, and the authors must
make use of that, by investigating associations across subgroups. For example, strata by
HbA1c (glucose control ok/not ok) or risk strata according to QRISK, generated by the
authors, may be handy and meaningful clinically.
Author response: We believe we have addressed this with the different models presented
as described above which includes adjustment for HBA1C levels at the start of treatment.
We have tested for interactions between the different diabetes drugs and confounders such
as age, sex, body mass index and HBA1C. We have also highlighted the similarities between
the exposure groups for baseline values as shown in Table 1 & 2. We adjusted for the
variables which make up the QRISK2 score in the analysis as potential confounders. We
didn’t stratify the analysis by QRISK strata since the QRISK2 score can only be applied to
patients without pre-existing cardiovascular disease.
v) The authors analysed the data without consistent inclusion criteria for different
drugs. For gliptins and thiazolidinediones, the authors examined only new users, for which
the authors termed ‘an incident user design’, arguing analysis of prevalent users would
cause bias (ref 33). Without the design, the authors introduced bias to the analyses of the
other drugs with ‘a prevalent user design’. The inconsistency of the design across the drugs
is not clear. It seems straightforward to do analyses based on an incident user design only or
based on two types separately. More importantly, the bias for analyses with prevalent user
design is concerning. Because of these concerns, the overall results seem to be too crude
and may not be optimised for readership of a medical journal. If these issues are not
minimized or proven to be negligible, the authors must give conclusions accounting for the
uncertainty of the associations. The information should guide readers to understand
underlying issues, needs for additional research and interest in future evidence. Giving
caution or concerns about ongoing clinical practice should be rephrased carefully. At least,
they should not stand alone. Just a note about possible residual confounding is not enough,
in the abstract particularly.
Authors’ response: We used a new user design for gliptins and glitazones since the use of
these two drug groups reflect the main research questions of interest. We considered
restricting the main analysis to exclude prevalent users of other drugs such as metformin
and sulphonylureas. However since gliptins and glitazones are recommended as second line
agents, excluding prevalent users of metformin and sulphonylureas would result in the loss
of too many patients exposed to gliptins or glitazones. It would also result in a population
Page 49 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015. Page 9
which is not representative of new users of glitazones or gliptin. This is likely to make the
findings less generalizable to everyday clinical practice. However, we have now excluded
prevalent users of insulin and have also included an additional analysis (in the
supplementary tables) where we excluded prevalent users of sulphonylureas. We have
made this clear in section 3.3 of the methods.
Additionally, we also carried out a sensitivity analysis where we excluded prevalent users of
sulphonylureas from the study cohort so that the hazard ratios for sulphonylureas are based
on incident users, and we fitted the following models:
• Model F: model C having excluded prevalent users of sulphonylureas.
• Model G: model E having excluded prevalent users of sulphonylureas.
We have also expanded the section on strengths and limitations in the discussion (section
5.6) to address the points made.
2. The authors conclude this work with remark on sulphonylureas. The authors should
account for and strongly highlight available evidence for different types of sulphonylureas.
Simpson et al. summarised available evidence for sulphonylureas and reported that use of
certain types of sulphonylureas was associated with lower all-cause mortality and
cardiovascular mortality (Simpson et al Lancet Diabetes Endocrinol, 2015;3(1):43-51). The
authors of this submitted work aggregated different types of sulphonylureas, and this might
be huge limitation.
Gliptins may also cause the same question (Clar et al., BMJ Open, 2012;2:e001007). The
authors are aware of the variations (page 17 of 40). The authors said “The predominant
gliptin prescribed in our dataset was sitagliptin which was prescribed to 80% of the gliptin
users.” This indicates availability of specific data on different types of a single class of drugs
(as evaluated for thiazolidinediones). This should be informed for all classes of anti-diabetic
drugs in the method section, rather than the discussion section. If reasonable to do, the
authors should separate different types of sulphonylureas and gliptins, probably with a
certain criterion for a sample size.
The use of sulphonylureas was not the main focus of the study so we haven’t looked at
different types in our analysis.
We have added a sentence to the discussion to refer to the paper by Esposito et al9 to
highlight there may be differences between individual gliptins and their effect on HBA1C.
We have limited power to look at different types of gliptins at this stage since they are
relatively new drugs so have presented the results for the group overall.
3. The authors derived NNT and NNH, probably accounting for the generalisability of
the results. However, NNT and NNH are assumed to have causal association, although this
study does not demonstrate causal associations. In addition, the authors evaluated the
outcomes that can be or have been evaluated in clinical trials. The authors should
acknowledge that evidence from trials may be available. For any results with substantial
uncertainty, presentation of NNH/NNT is concerning. Treatments showing heterogeneity by
a certain factor (eg calendar years) are of concern. For them, the NNH/NNT based on the
overall estimate seems not helpful. The authors should formally examine quality of evidence
to translate the findings to clinical message, for example by using GRADE system. Then, only
Page 50 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015. Page 10
if evidence is moderately strong, the authors might want to present NNT or NNH. Without
at least moderate evidence, presented results of NNT and NNH seem not be meaningful or
even misleading. The authors may want to highlight that participants in a trial tend to be
selectively recruited, and NNT/NNH based on a trial tend to have an issue of external
validity.
Authors’ response: We think it is important for readers that we present measures of
absolute risk as well as relative risks, however we have now removed the NNH/NNT values
but included rates of the outcomes in Table 3 to given an indication of absolute risks.
Minor comments:
1.Table 4 indicates that person-years for the three main outcomes were the same. But
according to the method description (section 3.3), the authors excluded baseline CVD
patients in analysis of CVD and baseline heart failure patients in analysis of heart failure.
Person-years in Table 4 should not be interpreted mistakenly. So, person-years used for
each outcome should be described appropriately.
Author response: We have added the person years for each outcome separately.
2.The findings would be biased partly by competing risk. The issue would be small, as CVD
would be the leading cause of deaths in the UK population. However, people would be
censored earlier by deaths due to non-CVD causes. If the non-CVD mortality was associated
with drug use, the authors might have bias due to competing risk. In addition to the
considerations regarding the comments above, the authors should describe the issue of
competing risks so that readers can at least recognise it.
Authors’ response: We have addressed this by undertaking a time varying analysis and have
updated confounders prior to the start of each treatment period. We have also adjusted for
existing complications (see above). We reviewed some of the literature on competing
risks10-12
, and the consensus seems to be that competing risk methods are most useful for
prediction modelling/estimating absolute risks whereas for more aetiological research such
as this diabetes study then Cox methods are better - for ease of interpretation (as long as
these censor when a competing risk occurs - as we've done in our analysis by censoring at
death). We have added this to the methods (section 3.7).
3.Heart failure is one of cardiovascular diseases. Parallel description of CVD and heart failure
is confusing. The method description is clear (page 8). The description in the abstract
should be revised, falsely indicating that heart failure is included in cardiovascular diseases.
Authors’ response: the main outcomes in the abstract list cardiovascular disease, heart
failure and all-cause mortality. Heart failure is not included in the cardiovascular disease
outcome.
4.Missing imputation was done seemingly appropriately. However, the missing data on
certain risk factors for cvd are concerning. For example, lipid profiles are only available for
60% of the total population. Validity of the imputation and the uncertainty based on the
Page 51 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015. Page 11
missing information should be described. Also, the authors should describe what variables
were taken into consideration for imputation.
Author response: restricting the analyses to the later time period 2007-2015 means that the
completeness of the risk factors is higher – for example 85% or more patients have lipid
profiles available. We had added additional comments in the text of the results (section 4.2)
on the completeness of the data. We have added further information on the multiple
imputation procedure we used to the Methods (section 3.7).
5. Please note that cardiovascular disease patients were excluded in certain analyses.
Author response: we have clarified in the methods (section 3.3) that patients with an
existing diagnosis of an outcome of interest at the study date were excluded from the
analysis of that outcome.
6. Suppl Table 1.
The header of the last column does not make sense. This column was interpreted as the
results for the sensitivity analysis regarding use of any hypoglycaemic drugs.
Author response: we have updated the tables.
References
1. Eurich DT, Simpson S, Senthilselvan A, et al. Comparative safety and effectiveness of
sitagliptin in patients with type 2 diabetes: retrospective population based cohort
study. 2013;346.
2. Graham DJ, Ouellet-Hellstrom R, MaCurdy TE, et al. RIsk of acute myocardial infarction,
stroke, heart failure, and death in elderly medicare patients treated with
rosiglitazone or pioglitazone. JAMA 2010;304(4):411-18.
3. Juurlink DN, Gomes T, Lipscombe LL, et al. Adverse cardiovascular events during
treatment with pioglitazone and rosiglitazone: population based cohort study.
2009;339.
4. Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondary prevention of macrovascular
events in patients with type 2 diabetes in the PROactive Study (PROspective
pioglitAzone Clinical Trial In macroVascular Events): a randomised controlled trial.
Lancet 2005;366(9493):1279-89.
5. Lincoff AM, Wolski K, Nicholls SJ, et al. Pioglitazone and Risk of Cardiovascular Events in
Patients With Type 2 Diabetes Mellitus: A Meta-analysis of Randomized Trials. JAMA
2007;298(10):1180-88.
6. Coupland C, Hill T, Morriss R, et al. Antidepressant use and risk of suicide and attempted
suicide or self harm in people aged 20 to 64: cohort study using a primary care
database. BMJ 2015;350:h517.
7. Hippisley-Cox J, Coupland C. Unintended effects of statins in men and women in England
and Wales: population based cohort study using the QResearch database. BMJ
2010;340:c2197.
8. Coupland C, Dhiman P, Morriss R, et al. Antidepressant use and risk of adverse outcomes
in older people: population based cohort study. BMJ 2011;343(aug02 1):d4551-d51.
Page 52 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
©Julia Hipisley-Cox, 2015. Page 12
9. Esposito K, Chiodini P, Maiorino MI, et al. A nomogram to estimate the HbA1c response to
different DPP-4 inhibitors in type 2 diabetes: a systematic review and meta-analysis
of 98 trials with 24 163 patients. BMJ Open 2015;5(2):e005892.
10. Andersen PK, Geskus RB, de Witte T, et al. Competing risks in epidemiology: possibilities
and pitfalls. International Journal of Epidemiology 2012;41(3):861-70.
11. Lau B, Cole SR, Gange SJ. Competing Risk Regression Models for Epidemiologic Data.
American Journal of Epidemiology 2009.
12. Pintilie M. Analysing and interpreting competing risk data. Stat Med 2007;26(6):1360-7.
Page 53 of 53
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960