Embed Size (px)
Citation preview

The Problem
◼ Cardiovascular prevention trials are large, long and expensive
• 10,000+ patients
• Years of patient follow-up
• € 100,000,000+ development cost
◼ Many patient groups-data from one group may not be relevant to others
How can MR help design the clinical program to maximize revenue and minimize development time and cost?

Opportunity for MR
◼ MR traditionally develops target product profile
◼ High cost of CV clinical development leads to a new MR opportunity
• ID patient populations• Trade off revenue and cost

The Approach
How do cardiologists think about CV risk?
30 Key Opinion Leader Interviews
How will MDs extrapolate data?
Web survey: 200 cardiologists & PCPs
How to trade off revenue and costs?
Patient Rx versus clinical cost and time

Objectives
◼ Quantify the revenue impact of:• Registration studies (baseline)
• Four different patient populations
◼ Incremental impact of:• Biomarker studies
• Surrogate endpoint studies
15 scenarios in all

Peripheral
Arterial Disease
(PAD or PVD)
Cerebrovascular
Disease
(CEVD)
Coronary
Artery
Disease
(CAD)
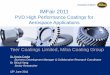
CV Risk Stratification
BMI > 30
Abdominal Fat
> 140 systolic
or
> 90 diastolic
LDL > 160 mg/dL
HDL < 40 mg/dL
Obesity Dyslipidemia Hypertension SmokingType II
DiabetesAge
Age:
M > 65, 55, 45
F >75, 65, 55
PTCA
CABG
ACS
Post MI
Unstable
Angina
Single
Risk
Factors
Stroke
Carotid
Disease
Documented
Carotid
Narrowing
Intermittent
ClaudicationPrevious
Event
Multiple Risk Factors including
“Metabolic Syndrome”
Inc
rea
sin
g R
isk
of
CV
Eve
nt
or
De
ath

Type II
Diabetes
Coronary
Artery Disease
(CAD)
Cerebrovascular
Disease
(CEVD)
Peripheral
Arterial Disease
(PAD or PVD)
CV Risk Stratification - Qualitative Risk
Model Schematic
or or
CAD or CEVD or PVD w/ DM
Secondary
PreventionPost-Primary
Event
Primary
PreventionPre-Primary
Event
Inc
rea
sin
g R
isk
of
CV
Eve
nt
or
De
ath
BMI > 30
Abdominal Fat
> 140 systolic
or
> 90 diastolic
LDL > 160 mg/dL
HDL < 40 mg/dL
Obesity Dyslipidemia Hypertension SmokingType II
DiabetesAge
Age:
M > 65, 55, 45
F >75, 65, 55
PTCA
CABG
ACS
Post MI
Unstable
Angina
Metabolic
Syndrome
Risk
Factors
Stroke
Carotid
Disease
Documented
Carotid
Narrowing
Intermittent
Claudication
Hypertension
Plus One Other
Risk Factoror
or

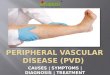
Eligible US patients slightly outnumber
those in Europe
Patients Eligible for Treatment (MM)
1.0
2.0
3.0
4.0
5.0
6.0
CV+DM DM CAD CEVD PVD HBP+1 Met. Syn. HBP
Millio
ns o
f P
ati
en
ts
U.S.
Europe

◼ A leading pharmaceutical company will offer an alternative
add-on therapy for CV patients who have documented CV
disease or are at risk for CV disease and currently receiving
standard clinical therapy.
◼ The product has the following characteristics:
• Novel mechanism
• Oral, once daily in tablet form
• Reduces events/revascularization procedures by 25%
• No increase in adverse drug events
• No additional side effects or monitoring
• No clinically significant drug-drug interactions with
commonly co-prescribed medications
• Price comparable to Lipitor
Product Profile

Physician Comments on Product Profile
◼ First in class-cardiologists had little basisfor comparison with alternatives
◼ Interviewees expect mortality data inaddition to “events”
◼ Cardiologists need good safety data

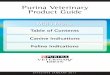
Type II Diabetes32%
CerebrovascularDisease (CEVD)
58%
Coronary Artery Disease (CAD)
42%
US Halo Effect
Peripheral Arterial Disease (PAD or PVD)
35%
Metabolic Syndrome27%
Hypertension plus one risk factor
30%
Hypertension26%
CAD or CEVD or PVDw/ Type II Diabetes
45%
Regulatory approval
6.7 MM total patients
45%
32%
45%
28%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
CV + DM DM CADCEVD/PAD
PrimaryPrevention
Pe
rce
nt
of
Pa
tie
nts
0.7
1.0
2.42.6
0.5
1.0
1.5
2.0
2.5
CV + DM DM
Pa
tie
nts
(M
M)
CADCEVD/PAD
PrimaryPrevention

Type II Diabetes25%
CerebrovascularDisease (CEVD)
55%
Coronary Artery Disease (CAD)
32%
European Halo Effect
Peripheral Arterial Disease (PAD or PVD)
26%
Metabolic Syndrome23%
Hypertension plus one risk factor
25%
Hypertension22%
CAD or CEVD or PVDw/ Type II Diabetes
42%
5.5 MM total patients
42%
25%
38%
23%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
CV + DM DM CADCEVD/PAD
PrimaryPrevention
Pe
rce
nt
of
Pa
tie
nts
0.90.6
2.2
1.8
0.5
1.0
1.5
2.0
2.5
CV + DM DM
Pa
tie
nts
(M
M)
CADCEVD/PAD
PrimaryPrevention
Regulatory approval

Biomarker Effect
Type II Diabetes41% (36%)
CerebrovascularDisease (CEVD)
47% (38%)
Coronary Artery Disease (CAD)66% (65%)
Peripheral Arterial Disease (PAD or PVD)
47% (38%)
Metabolic Syndrome37% (29%)
Hypertension plus one risk factor
38% (32%)
Hypertension34% (28%)
CAD or CEVD or PVDw/ Type II Diabetes
54% (50%)
Regulatory approval
Epidemiological study: shown elevated disease biomarker
7.7MM to 8.7 MM total patients
0.71.1
3.02.8
0.5
1.0
1.5
2.0
2.5
Pa
tie
nts
(M
M)
0.8
1.3
3.23.43.0
CV + DM DM CAD/CEVD/PAD Primary Prev.
50%
36%
47%
30%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
CV + DM DM CAD/CEVD/PAD Primary Prev.
Pe
rce
nt
of
Pa
tie
nts 54%
41%
53%
36%
55%
CAD App & Epi
CAD App + Epi

Surrogate Effect
Type II Diabetes37% (36%)
CerebrovascularDisease (CEVD)
46% (44%)
Coronary Artery Disease (CAD)71% (68%)
Peripheral Arterial Disease (PAD or PVD)
42% (39%)
Metabolic Syndrome33% (31%)
Hypertension plus one risk factor
36% (34%)
Hypertension30% (29%)
CAD or CEVD or PVDw/ Type II Diabetes
61% (54%)
Regulatory approval
Epidemiological study: shown elevated disease biomarker
Study has shown improvement in surrogate endpoint
7.9MM to 8.4 MM total patients
54%
36%
50%
31%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
CV + DM DM CAD/CEVD/PAD Primary Prev.
Pe
rce
nt
of
Pa
tie
nts 61%
37%
53%
33%
55%
CAD App + Epi
CAD App + Epi + Surr in CV+DM
1.20.9
3.4
2.4
0.5
1.0
1.5
2.0
2.5
Pa
tie
nts
(M
M)
1.3
3.6
2.5
3.0
CV + DM DM CAD/CEVD/PAD Primary Prev.
0.9

Primary Hypertension Treatment#
Type II Diabetes
US 56% (53%)EU 45% (50%)
CerebrovascularDisease (CEVD)
US 64% (53%)EU 53% (50%)
Coronary Artery Disease (CAD)
US 79% (53%)EU 75% (50%)
Survey Responses
Client Estimate*
* Prescribing for secondary prevention patients with elevated BP is much higher (e.g., 85% for CAD patients with elevated BP in the U.S.).
# Physician responses for secondary prevention patients are weighted 2:1 cardiologist to PCP; for primary prevention, patients weighted 1:5 cardiologist to PCP.
Peripheral Arterial Disease (PAD or PVD)
US 63% (53%)EU 51% (50%)
Metabolic Syndrome
US 53% (69%)EU 51% (43%)
Hypertension plus one risk factor
US 66% (69%)EU 62% (43%)
Hypertension
US 62% (69%)EU 57% (43%)
CAD or CEVD or PVDw/ Type II Diabetes
US 82% (53%)EU 81% (50%)

Halo Effect Summary
A B C D E F G H I J K L M N O
Scenario
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
Pati
en
ts (
MM
)
Indication Halo Biomarker Surrogate

Revenue Present Value versus Clinical Cost
Scenario A
Scenario B
Scenario C
Scenario D
Scenario E
Scenario F
Scenario G
Scenario H
Scenario I
Scenario J
Scenario K
Scenario L
Scenario M
Scenario N
Scenario O
Cost versus Revenue PV Index
50
60
70
80
90
100
$150 $200 $250 $300 $350
Clinical Development Cost
Re
ve
nu
e P
V I
nd
ex
(0
-1
00
)

Outcome◼ Phase IIB program to support the “Blue”
registration plan, which maximizes revenues and saves:• $80 million
• 1 year to market
◼ Technique recently expanded to marketed products-predicting impact of new(Phase IV) clinical trials• Client sponsored
• Competitor sponsored

Conclusions◼ MR spending early in development can
save $ and time
◼ “Rocket science” is understanding clinical trial trade offs, not MR tools
◼ Web enables more complex research• Faster and better, not
• Faster and cheaper