Embed Size (px)
Citation preview

1357
CONFERENCE
Clinical oncologyMolecular oncology was the hallmarkof ECCO 7, the seventh EuropeanConference on Clinical Oncologyand Cancer Nursing, in Jerusalem(Nov 13-18), mainly because ofthe ever-increasing importance ofbasic science. Indeed, in welcome,Umberto Veronesi (Milan), presidentof the organisers FECS (Federationof European Cancer Societies), won-dered aloud whether it was time todrop the "clinical" descriptor.Understanding of the factors thatlead to loss of growth control in thecell and how to regain that controlremain the goals for genetic, immun-ological, and virological research andtherapies.
Bert Vogelstein (Baltimore), usingthe example of familial adenomatouspolyposis (FAP) en route to coloncarcinoma, described a genetic bal-ance of oncogenes, tumour suppres-sor genes, and mutator genes; the lastremain hypothetical but may acceler-ate mutations in the other two. Wild-
type (wt) p53 gene expression isassociated with tumour suppressionwhile mutant p53 leads to loss ofgrowth control and hence prolifera-tion. He and his colleagues have nowidentified a wt-p53 activated frag-ment (WAF i) that mediates wt-p53tumour suppression but is not
expressed by mutant p53 (see Cell :
1993, vol 75, for a paper from theBaltimore group and similar findingsindependently reported from the Bay-lor College of Medicine; their gene iscalled CIPl). Therapeutic manipula-tion, for example by mimicry of
WAF 1, would circumvent the diffi- j
:ulties of gene-therapy delivery. j"Infections are by far the most
,gnored risk factor for cancer", said ,
Harald zur Hausen (Heidelberg).The E6 and E7 regions of the human 1papillomavirus (HPV) genome act as 1true oncogenes. E6 binds to p53 andprevents G1 repair arrest after DNA 1damage, while E7 binds to the sup- 1pressor Rb and causes mutations inthe host-cell DNA. The combinedeffect is accumulation of mutations,and E6/E7 are more activelyexpressed in high-grade than in low-grade HPV lesions. Leo Sachs (Rehovot) emphasised 1
that malignant cells are not immortal, 1and they can undergo cell death 1(apoptosis). The same viability fac-tors that prevent apoptosis in normalcells also maintain malignant cells,which explains why the scheduling oftreatment with growth factors is cru-cial, and it is only beginning to beunderstood. Evolution has led to
growth factors acting as safeguardsamong a network of proteins. jClaude Helene (Paris) said that the
best way to control nucleic acids is touse nucleic acids, and he classified 1potential treatments with oligonu-cleotides into four strategies: anti-
sense, antigene, sense, and ribozyme.In the sense approach, oligonu- 1cleotides trap proteases, while specialantisense nucleic acids cleave their
target mRNA in the ribozymeapproach, whch is especially impor-tant in potential anti-HIV treatments.In the antisense or antigene strate-
gies, the oligonucleotide binds to
mRNA or to DNA, respectively. 1To improve binding to the triplex
formed by antigene blocking, anti-
... and cancer nursingA popular concept is that cancer nursing is especially stressful. Nurses surveyed at the Institut Gustave-Roussy, Villejuif, were statistically more stressed than those in a gen- jeral hospital, but the investigators, C Rodary and colleagues, did not think this "sub- stantial". Dr Susie Wilkinson (Liverpool) found that stress among cancer nurses is jmore myth than reality. Cancer nurses were no more prone to general anxiety than 1other working women. Cancer nurses chose their specialty, which may strongly influ- ence their ability to cope. Many now see chemotherapy nursing as rewarding, largely jbecause of the huge improvements in emetic control. However, hospitals with restric- jtions on staffing and use of the new anti-emetics are a continuing worry. Stress factors jand support outside work are often neglected, and provide ground for further study. jBernadette Wouters (Brussels) insisted on the patient’s right to palliative care j
which, she says, is not a treatment of second-choice in the "anteroom of death". In jterminal illness, the nurse is confronted by the symptoms of a patient who is often by jthis stage disempowered and exhausted by repeated therapeutic failures. The reality of palliative care, especially in general units, is often far from the public’s perception 1of the "five- star" hospice. Palliation specialists have much work to do in educating 1their colleagues and managements. j
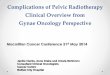
Figure: Antisense and antigeneoligonucleotide targets
cancer drugs can be attached as
intercalators at the end of the thirdstrand. The first clinical trials withantisense oligonucleotides, in effect
gene pharmacology, have begun inchronic myelocytic leukaemia, inacute myeloblastic leukaemia, withHPV (cervical cancer), and with
HIV.
So, what is the state of health ofEuropean oncology? John Smyth(Edinburgh), retiring president ofESMO (European Society for Med-ical Oncology), pleaded strongly forrecognition of medical oncology as aspecialty, which may sound simplebut is blocked from within the med-ical profession. Amateurism
abounds, he added, with patientsdenied appropriate treatment or giv-en the wrong treatment. ESMO’scertificate in medical oncology is
recognised in all but four EC coun-tries.
In view of its high cure (not remis-sion) rate, radiotherapy is both cost-effective, costing about 5% of
spending on cancer therapy and
leading to around 30% of the cures,and neglected, with the limelightalways on chemotherapy. Europeanradiotherapists are leaders in audit.Quality control may no longer betaboo, but it remains voluntary. Oneparticipating centre found, within afortnight, a software complicationthat remained undetected in a non-audit UK hospital for a decade.Emmanuel van der Schueren,
president of the European Organiza-tion for Research and Treatment of
Cancer, said that treating all patientsto the same high standard wouldmake an enormous difference to out-
come, because standards are verydifferent between European regions.But, he added, "we can do morethan society is willing to pay" andthe availability of treatment is "partpolitical and part educational".
David McNamee