Embed Size (px)
Citation preview

BRAIN AND COGNITION 19, 172-182 (19%)
Confabulation in Alzheimer’s Disease
ROBERT S. KERN,* WILFRED G. VAN GORP,~ JEFFREY L. CUMMING~,$ WARREN S. BROWN,§ AND SHERYL S. OSATOJJ
*Fuller Graduate School of Psychology; TPsychology Service, VA Medical Center West Los Angeles, and Department of Psychiatry and Biobehavioral Sciences, UCLA School
of Medicine; SNeurobehavior Unit, VA Medical Center West Los Angeles, Departments of Neurology and Psychiatry and Biobehavioral Sciences,
UCLA School of Medicine; BDepartment of Psychiatry and BiobehavioralSciences, Fuller Graduate School of Psychology, UCLA School of Medicine; and IjPsychology Service, VA Medical Center West
LOS Angeles, UCLA School of Medicine
Confabulation is present when memory is disturbed, but does it occur in Alz- heimer’s disease (AD) where memory abnormalities are often severe? In this study, confabulation was assessed prospectively in 26 AD patients and 15 normal elderly (NE) controls using a neuropsychological battery specifically designed to assess different types of memory errors. The results indicated that the AD group made significantly more verbal intrusions than the NE group. These findings provide evidence for the feasibility of eliciting confabulatory-type behavior during clinical assessment and support previous reports which have documented verbal intrusions as a common accompaniment of the memory impairment manifested by AD patients. 0 1992 Academic Press, Inc.
INTRODUCTION Confabulation is a prominent clinical feature in several neurological
disorders that involve memory impairment, most notably in the Wernicke- Korsakoff syndrome (Talland, 1961). Several investigators have suggested that frontal systems dysfunction may also be etiologically implicated in confabulatory behavior (Geschwind, 1974; Joseph, 1986; Kapur & Cough- lan, 1980; Kopelman, 1987; Mercer, Wapner, Gardner, & Benson, 1977; Weinstein & Lyerly, 1968). In Alzheimer’s disease (AD), the clinical
This study was supported in part by the Department of Veteran’s Affairs Medical Research Service, and was a requirement in partial fulfillment for the doctor of philosophy degree at Fuller Graduate School of Psychology. We express our gratitude to the Pasadena Com- munity Adult Psychological Services program and the UCLA-Neuropsychiatric Institute and Hospital for their assistance in this project.
172
0278-2626192 $5.00 Copyright 0 1992 by Academic Press, Inc. All rights of reproduction in any form reserved.

CONFABULATION 173
syndrome is typified by a dramatic memory impairment and frequently involves frontal systems disturbances as well (Cummings & Benson, 1992; Kazniak, 1986). Although a number of investigators have anecdotally noted the presence of confabulation in AD (Polatin, Hoch, Horwitz, & Roizin, 1948; Sourander & Sjogren, 1970; Uyematsu, 1923), few studies have systematically investigated the degree to which confabulation is pres- ent in AD using a prospective experimental design.
Confabulatory behavior is typically transient in nature (Weinstein, Mar- vin, & Keller, 1962). Hence, evidence supporting the presence of con- fabulation in specific syndromes has been largely determined by anecdotal clinical case studies. Confabulation may be elicited during the clinical examination, or it may be systematically assessed by examining patients’ verbal responses on formal memory tests. An advantage to the latter is that patients’ verbal responses can be measured both qualitatively and quantitatively for comparison with other clinical samples.
Although confabulation has been studied primarily in the verbal do- main, one might hypothesize that nonverbal forms may be just as common. To our knowledge only one previous study has investigated verbal vs. nonverbal forms of confabulatory-type behavior. If confabulation is re- lated to inadequate synthesizing of incoming material, amnesia, and poor impulse control (Geschwind, 1965; Joseph, 1986; Mercer et al., 1977), then confabulators may be expected to produce more line embellishments on drawings produced during free recall than nonconfabulators. Joslyn, Grundvig, and Chamberlain (1978) reported that embellishment errors on recall of abstract geometrical drawings were associated with confab- ulation. The “confabulators,” identified on the basis of their behavior on the inpatient unit, made nearly twice as many drawing elaborations as the group identified as “nonconfabulators.”
Previous studies have failed to provide a consensually agreed upon definition of confabulation. Hence, for the purpose of the present study we opted for an experimental definition limited to the precise elements which comprise confabulatory behavior. A confabulatory element was defined as any response (verbal or nonverbal) on a memory/learning task which is novel and not synonymous with the original material, representing a clear departure from the to-be-remembered material. Defined in this manner, confabulatory elements may be compared neuropathologically to other forms of memory failure: (a) near misses, e.g., the inaccurate recall of a story or event; (b) acknowledged recall failures; and (c) per- severations of previously presented material.
We undertook the current study to investigate confabulation in AD by (a) using standardized neuropsychological measures to assess confabula- tion; (b) examining the relationship between frontal systems dysfunction and confabulation; and (c) examining qualitative and quantitative aspects of confabulation.

174 KERN ET AL.
METHODS
Subjects
Two groups were studied: 26 subjects meeting the criteria for Probable AD as defined by the work group of the National Institute for Neurological and Communicative Disorders and Stroke-Alzheimer’s Disease and Re- lated Disorders Association (McKhann, Drachman, Folstein, Katzman, Price, & Stadlan, 1984) and 15 normal, independently living, older adult volunteer subjects recruited from the neighboring community. All of the AD patients had recently received a full neurological and physical ex- amination, including laboratory studies (serum folate and B12 levels, thy- roid functions, VDRL), and EEG and neuroimaging tests (either CT or MRI) .
The subjects comprising the AD group were recruited from an out- patient clinical service. Inclusionary criteria for AD and normal elderly (NE) subjects included (a) a minimum of 6 years of education, (b) age at testing greater than or equal to 50 years, and (c) a Mini-Mental State score (Folstein, Folstein, & McHugh, 1975) of 8 or above. Exclusionary criteria for all subjects included (a) previous history of psychiatric illness (before diagnosis of AD for the dementia group), (b) history of alcohol or substance abuse, (c) history of previous neurological disorder (e.g., cerebral vascular accident), and (d) presence of a delirium or confusional state.
Procedure
A neuropsychological test battery was selected to formally assess the presence and type of confabulatory response. The battery was comprised of eight measures:
1. Mini-Mental Status Exam (MMSE) (Folstein et al., 1975) was ad- ministered to assess cognitive impairment.
2. Vocabulary subtest from the Wechsler Adult Intelligence Scale- Revised (WAIS-R) (Wechsler, 1981) was administered to assess vocab- ulary integrity.
3. Block Design subtest from the WAIS-R (Wechsler, 1981) was ad- ministered to assess visuospatial ability.
4. Boston Naming Test (BNT) (Kaplan, Goodglass, & Weintraub, 1978) was administered to assess confrontation naming ability.
5. Frontal systems tests, including the hand alternation and response inhibition measures from the Luria-Nebraska Neuropsychological Battery (LNNB) (G o Id en, Hammeke, & Purisch, 1980), a modified form of the Continuous Performance Test (“A” test) (Rosvold, Mirsky, Sarason, Bransome, & Beck, 1956), and the verbal fluency section from the Fuld Object-Memory Evaluation (FOME) (Fuld, 1977) were administered to assess a range of frontal systems abilities.

CONFABULATION 175
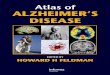
Design 3 Embellishment error FIG. 1. Illustrative example of an embellishment error on the Memory-for-Designs test.
6. Logical Prose subtest with 30-min delay from the Wechsler Memory Scale-Revised (WMS-R) (Wechsler, 1987) was administered to assess confabulation in the context of recall for prose-type material.
7. FOME (Fuld, 1977) was administered to assess intrusive responding during serial learning.
8. Memory-for-Designs Test (Graham & Kendall, 1960). Five drawings (Nos. 3, 6, 9, 12, and 15) were administered to assess nonverbal forms of confabulation. Embellishment errors on the Memory-for-Designs test were scored according to criteria described by Taylor (1961).
Measures 1-5 (evaluating cognitive impairment, language, visuospatial functioning, and frontal systems functioning) were used to categorize sub- ject differences in cognitive performance, while measures 6-8 (memory tests) were used to assess confabulation. All patients were administered individual tests from the battery in the same order to control for possible confounding effects from order of administration.
The dependent variables of interest were as follows: 1. Memory-for-Designs test (MFD). Novel embellishments: any sin-
gular element (e.g., line, loop, flag, box) added to the original figure. Novel embellishments are distinguished from (a) distortions-where the preservation of the original figure is lost, and (b) perseverations-a re- production or partial reproduction of any previous figure (Taylor, 1961). An example of a novel embellishment error on the Memory-for-Designs test is illustrated in Fig. 1.
2. Fuld Object-Memory Evaluation. Intrusions: any response describing an item or object which is not among the ten objects from the FOME bag.
3. Wechsler Memory Scale-Revised. (a) Recall inaccuracies: a response that is categorically correct with respect to subject content, but is inac- curate in detail (e.g., “Anna Thomas,” instead of “Anna Thompson,” or “She was from South Chicago,” instead of “South Boston”). (b) Novel intrusions: a response which describes a story element not included in the original passage (e.g., “the woman was shot and killed”).
The confabulation score drawn from the MFD was the sum of novel embellishments. On the FOME, the confabulation score was the number of extra-list intrusions, and on the WMS-R, the confabulation score was

176 KERN ET AL.
TABLE 1 DEMOGRAPHIC CHARACTERISTICS OF THE ALZ-
HEIMER’S DISEASE (AD) AND NORMAL ELDERLY (NE) GROUPS
Age Mean (SD)
Education Mean (SD)
Ethnicity Caucasian Black Other
Sex Male Female
Handedness Right Left
AD
70.58 (8.74)
13.58 (2.72)
81% 15% 4%
62% 38%
92% 8%
NE
67.87 (8.W
15.00 (2.25)
80% 7%
13%
60% 40%
93% 7%
the number of novel intrusions. This provided a robust measure of con- fabulation.
RESULTS
Efforts were made during subject selection to minimize group differ- ences on the demographic variables of age, education, ethnicity, sex, and handedness. Table 1 shows the means, standard deviations, and frequency distributions of the demographic characteristics for the two groups. The AD group did not significantly differ from the NE group on any of the demographic variables.
Table 2 presents the means and standard deviations of the measures used to define cognitive differences between the two groups.
Group Differences on Confabulation Measures
Table 3 presents the means and standard deviations of the confabulation measures for the two groups. Performances for the AD and NE groups on the confabulation indices were initially analyzed using a multivariate analysis of variance (MANOVA), with one independent variable (diag- nostic group) and three dependent variables (confabulation scores from the MFD, FOME, and WMS-R). A significant effect was found for di- agnostic group (F (3, 37) = 5.14, p < .Ol). To examine group differences on the individual measures of confabulation, one-way analyses of variance (ANOVA) were performed. As shown in Table 3, these analyses yielded

CONFABULATION 177
TABLE 2 NEUROPSYCHOLOGICAL TEST RESULTS FOR THE ALZHEIMER’S DISEASE (AD) AND NORMAL
ELDERLY (NE) GROUPS
AD NE
Mean SD Mean SD
MMSE Vocabulary Block design Boston naming test Frontal systems tests
Verbal fluency CPTa (Errors) Memory-for-Designs
(Error score-5 figures) Fuld Object-Memory Evaluation
(total retrieval) WMS-R: Logical prose
(immediate recall) WMS-R: Logical prose
(30 min delayed recall)
18.38 5.39 28.40 1.08** 9.46 3.73 12.07 3.21* 6.21 3.16 11.93 2.57+*
32.85 17.98 54.93 2.72**
20.13 10.60 42.00 5.61** 1.73 4.15 0.47 0.96 6.96 2.77 0.93 1.39**
15.42
5.54
1.00
12.50
3.96
1.98
41.87
22.00
17.00
5.25**
7.21**
8.00**
Note: aCFT = Continuous performance test. *p < .05; **p < ,001.
significant group differences for intrusions on the FOME (F(1, 39) = 12.35, p < .005), but not for novel embellishments on the MFD or novel intrusions on the WMS-R.
Group Differences x Type of Memory Error
The AD and NE groups were further examined to compare the type of memory errors produced. On the WMS-R, recall inaccuracies were compared with novel intrusions. Analysis of group differences for type
TABLE 3 CONFABULATION TEST RESULTS FOR THE ALZHEIMER’S DISEASE (AD) AND NORMAL
ELDERLY (NE) GROUPS
AD NE
Mean SD Mean SD
Memory-for-Designs: Novel embellishments Fuld Object-Memory Evaluation: Intrusions Wechsler Memory Scale-Revised (logical prose):
Novel intrusions
* p < .Ol
0.62 0.96 0.20 0.40 6.19 6.42 0.20 0.75*
5.31 6.69 3.67 2.09

178 KERNETAL.
of memory error on the WMS-R yielded significant group differences for recall inaccuracies (F(1, 39) = 18.21, p < .OOl), but not for novel intru- sions. The NE group made significantly more recall inaccuracies than the AD group; the AD group demonstrated a nonsignificant trend to make more novel intrusions. These results may be misleading at face value. It is important to note that the AD group did not recall as much material as the NE group, and in general, produced fewer verbal responses during recall assessment. Therefore, in order to adequately address the relative frequency of these two types of memory errors with respect to total recall in our AD and NE groups a further analysis was necessary. The raw memory error scores (number of novel intrusions and recall inaccuracies) were converted to provide an index of the relationship between memory error and recall ability. The conversion yielded the following indexes: (1) recall inaccuracy index = No. of recall inaccuracies/WMS-R total recall; (2) novel intrusion index = No. of novel intrusions/WMS-R total recall. A MANOVA was performed with one independent variable (diagnostic group) and two dependent variables (recall inaccuracy index and novel intrusion index). Significant group effects were found for both the recall inaccuracy index (F(1,39) = 4.60, p < .04) and the novel intrusion index (F(1, 39) = 4.32, p < .04). Thus, when analyzed in the context of recall performance, the AD group showed a greater proportion of both types of memory errors compared to the NE group. In other words, the AD group’s recall of the short stories was dominated by more recall inaccur- acies and novel intrusions than the NE group.
Confabulation and Frontal Systems Functioning
Measures of frontal systems functioning were analyzed to assess their association with confabulation. More traditional measures of frontal sys- tems functioning (e.g., Wisconsin Card Sorting Test) were intentionally omitted from this battery because of the predicted likelihood of floor effects in a sample of dementia patients. Instead, two measures were devised: (a) a frontal severity index and (b) a verbal fluency score. The frontal severity index was drawn from the hand alternation and response inhibition measures of the LNNB and the modified Continuous Perfor- mance Test (CPT). Cutoff criteria were developed for the purposes of analyses, providing an index of frontal systems functioning. Those AD subjects who showed significant impairment on (a) the hand alternation task (i.e., eight or less hand sequences in 10 set; (b) the response inhibition test (i.e., one or more errors); or (c) the modified Continuous Performance Test (i.e., one or more errors of commission) were classified as a Low Frontal Systems Functioning group (Low FSF; N = 12). The remainder of the AD subjects were classified as a High Frontal Systems Functioning group (High FSF; N = 14).
A MANOVA was performed, examining FSF group as the independent

CONFABULATION 179
variable by the three measures of confabulation (MFD, FOME, and WMS- R). The overall effect approached significance (p < .07), with novel embellishment errors on the MFD accounting for most of the variance. The Low FSF group made more novel embellishment errors than the High FSF group. A second MANOVA was performed, using verbal fluency from the distractor trials on the FOME as a frontal systems functioning measure. Using a median split, AD subjects were divided into a High Verbal Fluency group (Mean = 29.2) and a Low Verbal Fluency group (Mean = 12.2). The overall effect was nonsignificant.
DISCUSSION
This study provides new information with respect to the types of memory errors observed in AD patients. In general, the AD patients produced a greater number of confabulatory-type responses than the NE individuals on measures of learning and free recall.
Types of Confabulatory Responding
This study extends previous research on confabulation by examining both verbal and nonverbal forms of confabulation. These results indicate that AD patients make more verbal intrusions than the NE when required to perform list learning tasks. Of the three confabulation measures, the number of intrusions on the FOME was the strongest discriminator be- tween AD and NE groups. Over 80% of the AD subjects made at least one extra-list intrusion, as compared to only 1 of the 15 NE subjects. In fact, over 46% of the AD subjects made five or more intrusions on this measure. These results are similar to those reported by Fuld, Katzman, Davies, & Terry (1982) and Reed, Jagust, & Seab (1988).
Recall of short stories (WMS-R) also yielded decisively different per- formances for the two groups. In general, the recall performance of the AD group was characterized by reduced verbal output, limited amounts of accurate information, and an increased proportion of recall inaccuracies and novel intrusions relative to the amount of accurate recall.
With respect to assessment of nonverbal confabulation, the AD group showed a trend to make more line embellishments on drawings produced during free recall than the NE group. It should be noted, however, that despite these suggestive differences the number of embellished drawings was relatively few in the AD group (occurring in less than 20% of the drawings).
Memory Functioning in the Normal Elderly
Confabulation has conventionally been associated with amnesic syn- dromes (Berlyne, 1972; Mercer et al., 1977; Stuss, Alexander, Lieberman, & Levine, 1978; Weinstein, Kahn, & Malitz, 1956; Weinstein et al., 1962). However, it appears that the NE engage in a type of confabulatory process

180 KERN ET AL.
during free recall where there is an attempt to synthesize bits of infor- mation that have been retrieved. When unable to completely reconstruct the exact details of a short story, it is suggested that NE individuals attempt to “fill in the gaps” by providing material which approximates the missing information or makes sense of those elements that remain. This process of synthesizing remembered elements into a meaningful unit is not path- ological and may be considered a normal strategy used by unimpaired NE.
The NE made more recall inaccuracies than novel intrusions in their recall of the short stories. There are important qualitative distinctions between these two types of recall errors. Recall inaccuracies are the correct recall of semantic category, but not detail. On the other hand, novel intrusions are irrelevant, having no basis in the original story. The former type of responding may actually facilitate recall and be compensatory for changes that occur during normal aging by storing learned information into meaningfully “chunked” units (Loring & Papanicolaou, 1987). Fur- thermore, recall inaccuracies represent a less severe form of memory error than novel intrusions in that the former have an associative basis.
Confabulation in Alzheimer’s Disease: A Neuropathological Perspective
Historically, researchers have been unable to agree on a consensually accepted definition of confabulation (Berlyne, 1972; Shapiro, Alexander, Gardner, & Mercer, 1981; Stuss et al., 1978; Talland, 1961). Differences have also persisted in the conceptualization of the phenomenon from a brain/behavior perspective. However, despite these pitfalls, the move- ment toward a convergent neuropathological understanding appears to be promising.
Several investigators agree that confabulation is likely the result of dysfunction to both frontal systems and memory processes (Joseph, 1986; Kapur & Coughlan, 1980; Stuss et al., 1978; Weinstein et al., 1956; Weinstein et al., 1962). When the frontal lobes are compromised, there is a failure to monitor and exclude irrelevant and extraneous information. Added significance may be given to minor details due to failure in ap- propriate selection. In AD, although the frontal cortex is less involved than the parietal association cortex, it has a substantial pathological burden (Brtm & Gustafson, 1976). Moreover, positron emission tomography re- search has demonstrated that glucose metabolism in the frontal lobe is moderately to severely affected in AD patients (Duara, Haxby, Sundaram, Cutler, Heston, Moore, Schlageter, Larson, & Rapoport, 1986; Hunter, McCuskie, Wyper, Patterson, Christie, Brooks, McCulloch, Fink, & Goodwin, 1989; McGeer, Kamo, Harrop, Li, Tuokko, McGee!+, Adam, & Ammann, 1986). These observations establish the occurrence of frontal lobe dysfunction in AD, and this particular region could contribute to the observed confabulation. Our data, however, were unable to support

CONFABULATION 181
a prominent role for frontal systems dysfunction in confabulation. The measures included in this study assess function of frontal convexity areas, and involvement of the orbitofrontal cortex with associated disinhibition, impulsiveness, and poor judgement may be more relevant to confabula- tion. Neuroimaging studies may be helpful in providing information on the contribution of specific brain regions, i.e., orbitofrontal areas, to confabulation.
REFERENCES Berlyne, N. 1972. Confabulation. British Journal of Psychiatry, 120, 31-39. Brun, A., & Gustafson, L. 1976. Distribution of cerebral degeneration in Alzheimer’s
disease. Archiv fur Psychiatric und Nervenkrankheiten, 223, 15-23. Cummings, J. L., & Benson, D. F. 1992. Dementia: A clinical approach, (2nd ed.) Stoneham,
MA: Butterworth, Inc. Duara, R., Haxby, J., Sundaram, M., Cutler, N. R., Heston, L., Moore, A., Schlageter,
N., Larson, S., & Rapoport, S. I. 1986. Positron emission tomography in Alzheimer’s disease. Neurology, 36, 879-887.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. 1975. Mini-Mental State. Journal of Psychiatric Research, 12, 189-198.
Fuld, P. A. 1977. Fuld Object-Memory Evaluation. Chicago: Stoelting Instrument. Fuld, P. A., Katzman, R., Davies, P., & Terry, R. D. 1982. Intrusions as a sign of Alzheimer
dementia: Chemical and pathological verification. Annals of Neurology, 11, 155-159. Geschwind, N. 1965. Disconnection syndromes in animals and man. Brain, 88, 237-294,
585-644. Geschwind, N. 1974. In R. S. Cohen & M. W. Wartofsky (Eds.), Selected Papers on language
and the brain. Boston: Reidel. Golden, C. J., Hammeke, T. A., & Purisch, A. D. 1980. Manual for the Luria-Nebraska
Neuropsychological Battery. Los Angeles: Western Psychological Services. Graham, F. K., & Kendall, B. S. 1960. Memory-for-Designs test: Revised general manual.
Perceptual and Motor Skills, (Monograph Supplement No. 2-VIII), 11, 147-188. Hunter, R., McCuskie, R., Wyper, D., Patterson, J., Christie, J. E., Brooks, D. N.,
McCulloch, J., Fink G., & Goodwin, G. M. 1989. The pattern of function-related regional cerebral blood flow investigated by single photon emission tomography with 99 mTc-HMPAO in patients with presenile Alzheimer’s disease and Korsakoff’s psy- chosis. Psychological Medicine, 19(4), 847-855.
Joseph, R. 1986. Confabulation and delusional denial: Frontal lobe and lateralized influences. Journal of Clinical Psychology, 42, 507-520.
Joslyn, D., Grundvig, J. L., & Chamberlain, C. J. 1978. Predicting confabulation from the Graham-Kendall Memory-for-Designs test. Journal of Consulting and Clinical Psy- chology, 46, 181-182.
Kaplan, E. F., Goodglass, H., & Weintraub, S. 1978. The Boston naming test. Boston: E. Kaplan & H. Goodglass.
Kapur, N., & Coughlan, A. K. 1980. Confabulation and frontal lobe dysfunction. Journal of Neurology, Neurosurgery, and Psychiatry, 43, 461-463.
Kazniak, A. W. 1986. The neuropsychology of dementia. In I. Grant & K. M. Adams (Eds.), Neuropsychological assessement of neuropsychiatric disorders. New York: Oxford Univ. Press.
Kopelman, M. D. 1987. Two types of confabulation. Journal of Neurology, Neurosurgery, and Psychiatry, 50, 1482-1487.
Loring, D. W., & Papanicolaou, A. C., 1987. Memory assessment in neuropsychology:

182 KERN ET AL.
Theoretical considerations and practical utility. Journal of Clinical and Experimental Neuropsychology, 9(4), 340-358.
McGeer, P. L., Kamo, H., Harrop, R., Li, D. K. B., Tuokko, H., McGeer, E. G., Adam, M. J., & Ammann, W. 1986. Positron emission tomography in patients with clinically diagnosed Alzheimer’s disease. Canadian Medical Association Journal, 134, 597-607.
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., & Stadlan, E. M. 1984. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s disease. Neurology, 34, 939-944.
Mercer, B., Wapner, W., Gardner, H., & Benson, D. F. 1977. A study of confabulation. Archives of Neurology, 34, 429-433.
Polatin, P., Hoch, P. H., Horwitz, W. A., & Roizin, L. 1948. Presenile psychosis. American Journal of Psychiatry, 105, 96-101.
Reed, B. R., Jagust, W. J., & Seab, J. P. 1988, February, Differences in rates of confabulatory responses in Alzheimer’s disease and multi-infarct dementia. Paper presented at the Annual Meeting of the International Neuropsychological Society. New Orleans, LA.
Rosvold, H. E., Musky, A. F., Sarason, I., Bransome, E. D., & Beck, L. H. 1956. A continuous performance test of brain damage. Journal of Consulting Psychology, 20, 343.
Shapiro, B. E., Alexander, M. P., Gardner, H., & Mercer, B. 1981. Mechanisms of con- fabulation. Neurology, 31, 1070-1076.
Sourander, P., & Sjogren, H. 1970. The concept of Alzheimer’s disease and its clinical implications. In G. E. W. Wohtenholme & M. O’Connor (Eds.), Alzheimer’s disease and related conditions. London: Churchill.
Stuss, D. T., Alexander, M. P., Lieberman, A., & Levine, H. 1978. An extraordinary form of confabulation. Neurology, 28, 1166-1172.
Talland, G. A. 1961. Confabulation in the Wernicke-Korsakoff syndrome. The Journal of Nervous and Mental Disease, 132, 361-381.
Taylor, F. R. 1961. A revised scoring system for the Graham-Kendal Memory-for-Designs test. Unpublished master’s thesis, Univ. Utah.
Uyematsu, S. 1923. On the pathology of senile psychosis. Journal of Nervous and Mental Disorders, 57, l-25, 131-156, 237-260.
Wechsler, D. 1981. WA&R manual. New York: The Psychological Corporation. Wechsler, D., 1987 Wechsler Memory Scale-Revised. New York: The Psychological Cor-
poration. Weinstein, E. A., Kahn, R. L., & Malitz, S. 1956. Confabulation as a social process.
Psychiatry, 19, 383-396. Weinstein, E. A., & Lyerly, 0. G. 1968. Confabulation following brain injury. Archives
of General Psychiatry, 18, 348-354. Weinstein, E. A., Marvin, S. L., & Keller, J. A. 1962. Amnesia as a language pattern.
Archives of General Psychiatry, 6(4), 259-270.