Embed Size (px)
Citation preview

Concussion Management:
A Team Approach
Bill Condon, PT, MPT
Maria Davenport, MPT
Jamie L Johnson, MA L/CCC-SLP, BCS-S
Claude Lamoureux, PT, DPT, NCS1

2
• https://www.youtube.com/watch?v=Sno_0Jd8GuA
• https://www.youtube.com/watch?v=_55YmblG9YM

Objectives:
• Develop a better understanding of Concussion and Post-Concussion Syndrome
• Develop a better understanding of evidence-based assessment and intervention by Speech Therapy following Concussion
• Develop a better understanding of evidence-based assessment and intervention for Concussion Management/Vestibular Therapy by trained Physical Therapist,
• Further understand impact on balance following a concussion
• Knowing when to refer to other disciplines (SLP, OT, NeuroOptometry, NeuroPsychology)
3

Concussion
4

What is a concussion?• CDC 2010
• A type of TBI, caused by a bump, blow, or jolt to the head that can change the way your brain normally works.
• Concussions can also occur from a fall or blow to the body that causes the head and brain to move rapidly back and forth.
• Even what seems to be a mild bump to the head can be serious.
5

Concussion symptoms generally last less than 24
hours, and usually recovery is within 2-3 weeks
By 3 months 75% of patients will be
symptom-free (Anderson, et al. .2006)
PCS seek therapy 3-6 months after injury
Children and adolescents are among those at
greatest risk for concussion.
6

7
• The potential for a concussion is greatest during
activities where collisions can occur, such as
during physical education (PE) class, playground
time, or school-based sports activities.

8
Most concussions occur
WITHOUT
loss of consciousness.

Concussion
Signs and Symptoms
• Confusion
• Dazed or stunned
• Answers questions slowly
• Concentration or memory
problems
• Forgets plays
• Unsure of game, score or
opponent
• Can’t recall events prior to
or following incident
• HA or pressure
• Balance problems or
dizziness
• Light and/or noise sensitivity
• LOC
• Double or blurry vision
• Clumsiness
• Behavior or personality
changes
• Sleep disturbances
9

Adolescent Brain
– Prolonged brain swelling
– Slower recovery
– Greater potential for lingering problems with
LEARNING
MEMORY
JUDGEMENT
SOCIAL BEHAVIORS**KEY!!!!**
10

Adult brain connections at 18-
24 years
Disordered patterns become
permanent with long-term
consequences.
11

Danger Signs:
• Adults:
– Headache that worsens
– Weakness, numbness or decreased coordination
– Repeated vomiting or nausea
– Slurred speech
– Sleeping and Unable to awaken
– One pupil larger
– Convulsions or seizures
– Can’t recognize people or places
– More confused, restless or agitated
– Unusual behaviors
– LOC12

Danger signs:
• Additional signs in Children:
– Won’t stop crying
– Won’t eat/drink
13

Gender
• Girls are twice as likely to sustain a concussion
• More likely to report sleep disturbances and HA
• More likely to have PCS at one, three and six mos
post injury
• Less likely to be in school one year after injury
14

15
Proper Recognition and Response
Prevent further injury Help with recovery

Factors Influencing Risk and Recovery from
Sport-Related Concussion: Reviewing the
Evidence
• Primary Risk Factors:
• Sport Type and Setting -Football, Ice hockey, lacrosse, women’s soccer and Cheerleading.
• Sex –Female
• Age/Level of Competition – College>HS
• Genetics –APOE e4 and G-219T
• History of Concussion -3x more likely
• Equipment
Elgin, et al 2015
16

Four primary categories:
• Physical
• Thinking
• Emotional/Mood
• Sleep
17

Physical:
•Headache or “pressure” in head
•Nausea or vomiting
•Balance problems or dizziness
•Fatigue or feeling tired
•Blurry or double vision
•Sensitivity to light or noise
•Numbness or tingling
•Does not “feel right”
18

Thinking/Remembering:
• Difficulty thinking clearly
• Difficulty concentrating or remembering
• Feeling more slowed down
• Feeling sluggish, hazy, foggy, or groggy
• Difficulty finding the "right" word; difficulty
expressing words or thoughts; changes in speech.19

Emotional:
• Irritable
• Sad
• More emotional than usual
• Nervous *ANXIETY
20

Sleep:
• Drowsy
• Sleeps less than usual
• Sleeps more than usual
• Has trouble falling asleep
21

Signs observed by others:
Appears dazed or stunned
Is confused about events
Answers questions slowly
Repeats questions
Can’t recall events prior to/after the hit, bump, or fall
Loses consciousness (even briefly)
Shows behavior or personality changes
Forgets class schedule or assignments
22

Work place presentation…
23

Recovery• Varies
• Look Fine
• Don’t understand symptoms
• Days, weeks or longer
• Slower for older adults,
young children and teens
• IF Previous concussion-
longer to recover
24

• Symptomatic students may require active supports
and accommodations in school, which may be
gradually decreased as their functioning improves.
• Inform the student’s teacher(s), the school nurse,
psychologist/counselor, and administrator of the
student’s injury, symptoms, and cognitive deficits.
25

Returning to Daily
Home/Community Activities
• Increased rest and limited exertion are important to facilitate the patient’s recovery.
• Physicians should be cautious about allowing patients to return to driving, especially if the patient has problems with attention, processing speed, or reaction time.
• Patients should also be advised to get adequate sleep at night and to take daytime naps or rest breaks when significant fatigue is experienced.
• Symptoms typically worsen or re-emerge with exertion.
• Let any return of a patient’s symptoms be the guide to the level of exertion or activity that is safe.
26

Post Concussion Syndrome (PCS)
• Symptoms occur in 30-80% of mild brain injury
– May appear immediately or after injury
– May persist 3-6 months
– Subjective problems after test scores return to NL
– Evidence of altered brain metabolism and blood flow > 3 years
– Delayed or persistent symptoms seldom attribute to the injury
Memory problem, behavioral changes too much/little sleep, HA, fatigue
Mistaken for sinus inflammation, allergies, stress, “typical teenager” behaviors
27

Identify the Team
Schools:
Teachers
School psychologist and/or school counselor
Speech-Language Pathologists
Monitor/Identify concussed students withdifficulty in the classroom
Services may include: Testing, Classroom strategies or Modifications
School Principal or other school administrator
28

Identify the Team
Hospital:
KU Concussion Center
Neurologist
Physical Therapist
Speech-Language Pathologists
Neuro Optometrist/Opthamologist
Neuro-Psychologist
29

Anatomy and Physiology –
Vestibular System
30

Signs and Symptoms
• Dizziness/lightheadedness
• Blurred vision
• Vision deficits
• Nystagmus
• Tinnitus/hearing loss
• Vertigo
• Balance impairments, especially in the dark
• Falls
• Motion discomfort/motion sensitivity
• Sweating/nausea/vomiting episodes
• Height and busy environment avoidance31

32

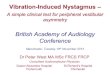
MotionInput
Intended Movement
VestibularProprioception
Visual
Vestibular NuclearComplex
Eye movement(VOR)
Motor Neurons
Body movement(VSR)
Adapted from Vestibular Rehabilitation, Herdman and Clendaniel33
Cerebellum

Peripheral Vestibular System
Functions:
• Stabilization of visual images on the fovea of the
retina during head movement to allow clear vision
• Maintain postural stability especially during
movement of the head
• Provide information used for spatial orientation
Involves the vestibular apparatus in the inner ear:
• Semicircular canals (SCC)
• Utricle
• Saccule
• CN VIII: Vestibulocochlear nerve 34

Labyrinth
• Bony structure- contains the three semicircular
canals, cochlea and vestibule. The canals are
filled with perilymphatic (similar to cerebrospinal
fluid). This fluid moves freely within the canal in
response to direction head motion.
• Membranous- is contained within the bony
structure and includes the three semicircular canal
as well as the utricle and saccule (otoliths).
Contains endolymphatic fluid surrounding the
structures, which has density slightly higher than
water.35

Anatomy
36

Orientation of Canals
• The three semicircular canals - anterior, horizontal,
and posterior-respond to angular acceleration and are
at right angles in respect to each other
• The horizontal (or lateral) canals form a coplanar pair,
inclined approximately 30 degrees upward from
horizontal plane
• The posterior (inferior) and anterior (superior) canals
are inclined approximately 90 deg from plane; the
posterior and contralateral anterior SCCs form pairs
( i.e. R posterior and L anterior; L posterior and R
anterior with Dix-Hallpike testing)37

Inertial Navigation: Inner Ear
• Semicircular Canals (3) are angular rate sensors--*anterior, horizontal, posterior
• Otoliths (utricle and saccule) are linear accelerometers
• Utricle excitation during horizontal; saccule excites with vertical accelerations 38

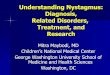
How Does This Work?
Each canal enlarges
at one end to form
the AMPULLA-
(shape of a
lightbulb). Within
the ampulla lies a
CUPULA, which
contains many hair
cells. Through head
movements, the
cupula transmits
signals via the
Vestibular Nerve to
the Brain.
The ratio of eye to
head movement
should be 1:1.
Abnormal gain can
cause symptoms of
blurry vision/vertigo
39

Central Vestibular System
– Vestibular reflexes are controlled by processes
primarily in the brainstem
– Connections between the vestibular nuclei,
reticular formation, thalamus & cerebellum are
seen
– SCC (angular) & otolith (linear) input is sent to
the vestibular nuclei
40

Central Vestibular System(cont.)
– Information travels to the ocular motor nuclei
(III, IV , VI) for mediation of the VOR
– Information travels further to the thalamus &
cortex for arousal & conscious awareness of
the head & body in space
– Maintenance of postural control – peripheral
vestibular input is sent distally as the medial &
lateral vestibulospinal tracts
41

42

Motor Outputs
• VOR (Vestibular Ocular Reflex): generates eye
movements, which enables clear vision while head
is in motion
• VSR (Vestibular Spinal Reflex): generates
compensatory body movement in order to maintain
head and postural stability, thereby preventing falls
• VCR (Vestibular Collic Reflex): stabilizes the
head in space
43

Vestibular Ocular Reflex
• Stabilizes eye in space
• Necessary to see while head is in motion
• Has 2 components, angular and linear VOR
• VOR is primarily responsible for gaze stabilization
44

Vestibular Spinal Reflex
• Stabilizes body
• Helps maintain desired orientation to environment
45

Function of Vestibular System
Vestibular Ocular Reflex (VOR) Vestibular Spinal Reflex (VSR)
Stabilizes Vision When
Head Moves
Balance Control
46

Anatomy and Physiology –
Vision Overview
47

Oculomotor System
48

Oculomotor System• Purpose: to produce eye movements to direct the fovea
toward the target of interest
• 6 extraocular muscles rotate the eye
– Divided into 3 pairs with complementary actions
• 3 cranial nerves control the eye movement
– CNIII (oculomotor): Medial rectus,
superior rectus, inferior rectus and
inferior oblique
– CN IV (Trochlear): Superior oblique
– CN VI (Abducens): Lateral rectus
49

50

Physical Therapy Management of
Concussion
51

Evaluation
• Balance
• Outcome Measures
• Oculomotor
• Cervical
• Exertion
• Reaction time and Divided attention52

Balance
53

Balance
• There is two “type” of balance: static and dynamic
• Balance is composed of three main systems:
– Visual
– Proprioception
– Vestibular
54

Balance
• mCTSIB
– Traditional versus computerized
• Bertec Cobalt
– Assessment of balance with Head Shaking and Visual
Motion Sensitivity
• Performed on a force plate which measures sway with
and without compliant surface
• Functional Gait Assessment
55

Balance
• BESS test
• Sharpened Romberg
– Eyes open and eyes closed
• Single leg stance
– Eyes open and eyes closed
56

Outcome Measures
57

Outcome Measures
• Dizziness – Dizziness Handicap Inventory (DHI)
• Adult
• Youth
• Pediatric
• Patients answer 25 questions, subgrouped into functional, emotional, and physical components
• Headache– HIT-6
– Headache Disability Index (HDI)
• Cervical– Neck Disability Index (NDI)
58

Outcome Measures
• Anxiety
– Hospital Anxiety and Depression Scale (HADS)
– Generalized Anxiety Disorder 7(GAD-7) Scale
• Vision
– Developmental Eye Movement ( Adult –ADEM)
– King Devick
• Migraine
– Migraine Disability Assessment (MIDAS)
59

Oculomotor
60

Major Oculomotor Gaze Systems
• Eye movement controlled by 4 major system
– Saccadic eye movement: for rapid eye movements to bring new objects being viewed on to the fovea
– Smooth Pursuit: for eye movements to keep a moving image centered on fovea
• CN III. Oculomotor: eye movement (dilation of pupils, follow target)
• CN IV. Trochlear: eye movement (look down)
• VI. Abducens: eye movement (look lateral)
– Vestibulo-ocular reflex: keeps image steady on fovea during head movements
– Vergence: keeps image on fovea predominately when the viewed object is moved closer
61

Spontaneous/ Fixed Nystagmus
• Spontaneous
– Simple test! Patient holds head still while looking
at you. Will not see unless acute event has
occurred!
– Observe for nystagmus
• Fixed Gaze Nystagmus
– Hold patient’s head stationary
– Use your finger or pen and take patient to 30
degrees left, right, up and down from center and
hold gaze
– Observe for any nystagmus at 30 degrees angle
– DO NOT TAKE TO END RANGE!!! 62

Smooth Pursuits
• Holds images of a moving target on the retina
• Keep target between 18” from patient
• 60 degree total arc to avoid end range nystagmus
• Do not move pen/finger too fast
• Positive findings: Saccadic intrusion
63

64

Smooth Pursuit
• practice
65

66

Saccades
• Rapid conjugate movements of the eyes to place the object of interest on the fovea
• Have patient look between 2 targets approximately 15 degrees apart
• Nose, pen, nose, pen in left right and up and down
• Looking for the eyes to reach each target in one smooth movement
• Positive findings: hypometric and hypermetric (cerebellar) or inability to increase speed
67

68

Saccades
• Practice
69

70

VOR
• Tilt patient’s head down 30 degrees
• Start slowly moving head side to side while they
focus on your nose, gradually increasing speed
• Repeat in vertical plane
• Pace:120 bpm
• Positive finding: Patient unable to stabilize
gaze on nose71

72

VOR
• practice
73

VOR Cancellation
• Hold patient’s head and tilt forward 30 degrees
(HC is in horizontal plane)
• Have patient look at your nose while you and the
patient move side to side
• Repeat in vertical plane
• Pace: 60 bpm
• Positive findings: saccadic intrusion
74

75

VOR Cancellation
• Practice
76

Convergence
• Hold patient’s head stable with pen or optotype 2 feet away from their nose
• Ask patient to focus on pen or optotype while you move it towards their nose
• You should be able to observe convergence of the eyes
• Ask patient when they see double. If patient sees blurry before double, they may need reader glasses to facilitate testing.
• Patient should be able to converge from 6 to 10 cm measured from the forehead
• Positive findings: Greater than 10 cm
77

78
Convergence

79

80

Convergence
• Practice
81

Accommodation
• A reflex action of the eye, response of focusing on
a near object, then looking at a distant object
• Ask the patient to close one eye to check for
accommodation monocular vision
• Start close to the eye then patient move the target
out until just able to read and measure the
distance from target to cheek in inches
• The reflex is dependent on CN II (optic) and CN III
for changes in the shape of the lens; assisting with
focus on vision
• Positive findings: Age group normative data82

83

Visual Acuity
• Visual acuity (VA) is acuteness or clearness of
vision, which is dependent on the sharpness of the
retinal focus within the eye and the sensitivity of
the interpretative faculty of the brain.
84

Dynamic Visual Acuity
• Using a ETDRS eye chart asked the patient to
read the chart until the lowest line or until the
lowest line is recognizable or until they are unable
to identify all the letters on a given line
• Hold patient’s head and tilt at 20 degrees of flexion
• Rotate their head yaw at 120 bpm
• While maintaining the rotation, ask the patient to
read the eye chart as described above
• Note how many lines above the baseline they are
able to read
• Repeat in the pitch plane
85

Dynamic Visual Acuity
• Positive findings: Greater then 2 lines
difference both vertically and horizontally
86

87

Optokinetic Reflex
• Optokinetic reflex (response) allows the eyes to
follow objects in motion while the head is
stationary. It is a combination of slow-phase and
fast-phase eye movements
• Patient is sitting looking at a ribbon with a
repeating vertical pattern at eye level
• While the patient keeps on looking at the ribbon
the examining therapist quickly moves the ribbon
horizontally to the right for 5 repetitions. Repeat to
the left, up and down
• Positive findings: Decreased “nystagmus"88

89

90

Visual Motion Sensitivity
• Clinical technique to measure motion-provoked
dizziness in patients with vestibular disturbances
• In standing , patient turns head, eyes, and trunk 80
degrees to the right and left at 50 bpm- 5
repetitions
• Positive findings: Reproduction of symptoms
91

92

Vestibular/Ocular-Motor Screening
(VOMS)
• The VOMS was developed to assess vestibular
and ocular motor impairments
• Evaluates 5 domains:
– Smooth pursuit
– Horizontal and vertical saccades
– Near point convergence
– Horizontal and Vertical VOR
– Visual and Motion Sensitivity
93

VOMS
• Patients rate and compare their levels with their
pre-assessments levels
– Headache
– Dizziness
– Nausea
– Fogginess
• It has demonstrated a high sensitivity in
identifying athletes who experienced a sport
related concussion
• Provides information to guide clinical management94

95
Yorke et al (2017) Sports Health

Cervical Spine
96

Cervical Spine –
Anatomy and Physiology
97

Why do we look at the Cervical Spine?
• For whiplash patients, did the patient also sustain
a concussion during the injury?
• For concussion patients, did the patient also
sustain a whiplash affecting the cervical region?
• Forces to cause mild traumatic injuries
(concussions) are between 60 to 160 g on the
other hand as little as 4.5 g, can cause mild strain
injury to the tissues of the cervical spine
98

Signs and Symptoms
• Unilateral headaches, often developing at the
occiput and extending around the temporal region
to the forehead (“ram’s horn”)
• Localized pain to occipital region, cervical
paraspinals, upper trapezius
• Stiffness with movement
99

Signs and Symptoms
• Reduced cervical motion
• “Bobble head motion” – feeling unstable
• Numbness or tingling in arm or hand
100

Signs and Symptoms
ConcussionHeadache
Pressure in head
Neck pain
Nausea/vomiting
Dizziness
Blurred vision
Balance problems
Sensitivity to light
Sensitivity to noise
Feeling slowed down
Feeling like in a “fog”
“Don’t feel right”
Difficulty concentrating
Difficulty remembering
Fatigue or low energy
Confusion
Drowsiness
Trouble falling asleep
More emotional
Irritable
Sadness
Nervous or anxious
Whiplash Associated Disorder
Neck/shoulder pain
Reduced/painful neck movement
Headache
Reduced/painful jaw movements
Numbness, tingling arm and hand
Numbness, tingling leg and foot
Dizziness/unsteadiness
Nausea/vomiting
Difficulty swallowing
Ringing in ears
Memory problems
Problems concentrating
Vision problems
Lower back pain
101

Structural Anatomy
102

Cervical Ligaments
103

Blood Supply- Cervical Spine
• Vertebral Artery:– Branch of the first part of
subclavian artery
– Passes through foramen
transverse of the upper six
cervical
– Enters skull through
foramen magnum
– At the lower border of the
pons, it joins the vessel of
the opposite side to form
the basilar artery
104

Supporting Musculature - Posterior
105

Supporting Musculature
106

Deep Cervical Flexor Muscles
107

Physiology of the cervical Spine
• Sensorimotor process
• Proprioception
• Sensory
108

Proprioception
• Proprioception is important to maintain the stability
and control of head movement
• Proprioceptors of the cervical spine have
anatomical connections with the vestibular and the
visual system
109

Proprioception Deficits
• Deficits in the cervical proprioception may results
in:
• Cervicogenic dizziness
• Oculomotor deficits
110

Sensory
• Sensory- afferents from ganglion root C2-C3 end
on the same nerve roots as the trigeminal nerve.
Referred pain from upper cervical structures, C0-
to at least C3, may radiate symptoms to the upper
cranium/ forehead region
111

Reflexes
• Both the cervicocollic and cervico-ocular reflexes
work in tangent with the VOR reflex to stabilize the
head and trunk during head/neck motions and to
assist in gaze stabilization
• Cervicospinal reflex (CSR)- changes in limb
position driven by neck afferent activity. Can
assist or interfere with the Vestibulospinal Reflex
(VSR)
• Disturbances in these reflexes can cause balance
disturbances and oculomotor dysfunction112

Research
• Vuillerme and Pinsault- 16 healthy males
experienced balance disturbances in which
experimental electrical stimulation was placed on
the bilateral trapezius with patients standing on a
force platform (eyes closed). The students were
asked to stand as still as possible on the platform
in two conditions: no pain and pain in the neck
muscles elicited by painful electrical stimulation.
Postural control and performance was assessed.
Results showed that experimental electrical
current significantly impaired standing balance.
113

Research
• Treleaven, et al- 12 post concussion subjects with
post concussion headache were compared to
normal subjects. PCH group presented with
painful upper cervical segmental joints, less
endurance in neck flexor muscles with testing, and
higher incidence of tightness in neck.
114

Cervical Spine
• Assess if
– Unilateral headaches
– Whiplash
– Pain
– Complain of Stiffness
115

Cervical Assessment
• Vertebral Artery
– administer in sitting (cervical spine in extension)
– turn head to the right count backward from 10 to 0 and
repeat on the left
– looking for 5 D’s: drop attack, diplopia, dysphagia,
dizziness, dysarthria; 3 N’s: Nausea, Nystagmus,
Numbness
116

Cervical Assessment
• Sharp Purser (Transverse ligament)
– with head in slight cervical flexion, anterior translation on
C2 and posterior translation with hand on forehead
– Positive if head slides backward, may hear a clunk
117

Cervical Assessment
• Alar Ligament
– Pinch grip on C2 spinous process
– Rotate head to the right, you should feel spinous process
move to the left
– Repeat on the left
– Same test should be done with side bending to the right
and left
– Absence of spinous process moving in the opposite
direction indicates a positive
118

Cervical Assessment
• Cervical Range of motion
• Upper cervical rotation test
– Performed in supine
– Bring the cervical spine in full flexion in an
attempt to isolate movement to C1-C2
– Rotate head to the right and the left
– Normal range of motion should be between 40
to 45 degrees
– Positive finding is a reduction in rotation of
more than 15 degrees
119

Cervical Assessment
• Passive mobilization
– Sitting (Mulligan Concept) and/or prone
(Maitland)
– Assessment of symptoms: headache and/or
dizziness
120

Cervical Assessment
• Deep neck flexor endurance test
– Assess deep cervical flexors endurance
– Test perform in either supine or hook lying
– Patient asked to tuck chin in and lift off the
table approximately 1” avoiding substitution by
SCM or platysma muscle
– Norms : men 38.9 sec, women: 29.4 sec
121

Cervicogenic Dizziness
• Assessment
– Head-Neck differentiation test
– Joint position error test
– Smooth Pursuit neck torsion test
123

Head Neck Differentiation Test
• Patient seated on a swivel chair
– The clinician rotates the chair while stabilizing
the patient head (cervical)
– The clinician rotates the chair without
stabilizing the head (vestibular)
• Reproduction of symptoms
124

Joint Position Error Test
• Assess cervicocephalic proprioception and neck
reposition sense
– Patient is seated 90 cm in front of target
– Patient in neutral head position (target adjusted
accordingly) using a laser light
– Patient instructed to perform active head
rotation to one side with eyes closed and return
to starting position- 3 repetitions
– Greater than 4.5 degrees indicates abnormal
cervical proprioception
125

Smooth Pursuit Neck Torsion Test
• Patient seated with cervical spine in neutral
– Perform smooth pursuit test and observe for
saccadic intrusion
• Patient seated with body rotated to one side 45
degrees while head remains in neutral position to
create cervical torsion
– Repeat the smooth pursuit test
– Tested in right and left side
• Positive findings: saccadic intrusion with
cervical torsion
126

Exertion
127

Exertion
• Following a concussion there is:
– Decreased in cerebral autoregulation capacity
– Potential in decreased in cerebral blood flow
• Preliminary evidence supports
– Symptom limited aerobic exercise programs for
individuals with persistent post concussion symptoms
– Protracted recovery associated
• Autonomic instability
• Physical deconditioning
128

Exertion
• Exertion protocol
– The Buffalo Treadmill concussion test
– Bike protocol to decrease motion sensitivity
(work in progress)
129

Reaction Time
130

Reaction time
• Computerized
131

Treatment
132

Intervention after Concussion
• From the Consensus statement on concussion in sport -2016
“ The Berlin expert consensus is that the use of the term “persistent symptoms” following sport related concussion should reflect failure of normal clinical recovery- that is, symptoms that persist beyond expected time frames (i.e. > 10-14 days in adults and > 4 weeks in children)”
• Preliminary evidence supporting– Individualized symptom-limited aerobic exercise
– Targeted physical therapy program for cervical or vestibular dysfunction
– Cognitive behavioral therapy for mood and behavioral issues
133

Intervention after Concussion
• There as been a change in the “rest “ formula for
concussion patient, from complete rest to
relative/active rest
• Evidence exist that sub-symptom-threshold and
submaximal exercise have been shown to be safe
and may benefit in facilitating recovery.
134

Intervention after Concussion
• Reneker et al. advocates for early intervention to
shorten recovery in Sport Related Concussion
• Interventions included vestibular therapy, oculomotor,
neuro-motor retraining and manual therapy
• Intervention was as early as 10 days
• Recovery time was shorten. The median time for
medical release was 10.5 shorter than the control
group
135

Treatment! Treatment! Treatment!
•Adaptation –Refers to the ability of the Vestibulo-ocular
Reflex to undergo changes through exercises involving
vision and head motion
•Substitution –other strategies to replace lost/impaired
function (strength, ROM, proprioception, assistive
device, activity modification, visual tracking) Improve
Postural Stability through vision
•Habituation–“based on the concept that repeated
exposure to provocative stimulus will result in a reduction
in the pathological response to that treatment”
(Herdman & Clendaniel, 2014, p.399)
136

Treatment Strategies• Treat positive findings (including symptom reproducing tests)• Frequent symptoms check as an assessment for
progression of therapy • Always try to challenge the vestibular spinal reflex
– Decreased base of support• Feet together • Semi-tandem• Tandem
– Progress onto compliant surface• Close cell foam (airex)• Open cell foam• Rocker board• Bosu ball
– Ambulation• Forward/backward
137

Treatment Strategies
• dual task – include a cognitive task
simultaneously while performing a vestibular
activity
– Examples:
• Playing music
• Naming animals or states
• Numbers
138

Example of treatment progression
• Smooth Pursuit– Tracking target
• Progression :
– Increasing repetition or time
– Increasing speed up to 60 degrees per second
– Changing target
• Plain letter on a card
• Busy background
• Marsden ball
• Target on mirror
– www.eyecanlearn.com
139

Example of treatment progression
• Saccades
– Eye movement
• Eye movement only
• Eye/head movement
– Time and Speed
• Increased the speed and the duration of the exercise
– Complexity
• 4 panel saccade
• Hart chart
– www.eyecanlearn.com
140

Example of treatment progression
• Gaze stability
– Speed
• Progress to 120 bpm for general population
• Progress to up to 150 bpm for athlete/high level
patient
– Target
• Plain
• Increasingly busy background
– Complexity
• Viewing X1
• Viewing X2
141

Example of treatment progression
• VOR cancellation
– Speed
• goal 60 bpm
– Target
• Plain
• Increasingly busy background
142

Example of treatment progression
• Motion sensitivity/Optokinetic– Repeating pattern ribbon
– Motion sensitivity test as a treatment
– Optokinetic video https://www.youtube.com/watch?v=kAPtu1WTHYc
– Disco ball
– YouTube videos
– Riding escalator
143

Convergence Exercises
• Pencil Push Ups
• Brock String
• Dot Card
• Convergence fusion pictures
144

Accommodation
• Binocular/monocular
– Poems
– Hart Chart
– Brock Bead with far target
145

Cervicogenic Dizziness Treatment
• Cervical deep flexor strengthening and motor
control
• Cervical manual therapy
• Cervical joint proprioception
• Scapular and cervical stabilization and postural
retraining
146

Exertion Treatment
• Submaximal symptom exacerbation threshold is
identified
– Aerobic exercise 20 minutes/day
– Intensity of 80% of the threshold heart rate
achieved during testing (90% in elite athletes)
– 5 to 6 day per week using a heat rate monitor
– Terminate exercise at first sign of symptom
exacerbation or 20 minutes whichever comes
first
147

Speech Therapy Management of
Concussion
148

Coming Out of the DarkASHA Leader December 2015
• Kathryn Hardin
– Changes 2009- to present
– Turning point:
2013 Journal of Head Trauma Rehabilitation
• Too much inactivity slows down the total recovery time and can make symptoms more severe.
• After acute period of neurotoxicity has passed the brain must begin functional activity to encourage recovery. 149

Before
SLP Role
150

The Rest Trap
• Brain gets better at what it is asked to do.
• Ongoing Dysfunction “steals” energy that would
enable quick bounce back.
• Sacrifice “fun” activities with negative effects.
• Tech restriction-social outlet
• Physical rest and Cognitive rest similar effects-
energy outlet
• Students who most need academic rigor may
prolong the break from it- head off “convenience”
151

Current
SLP Role
152

Evidence-based Practice
• 2 Days Cognitive and physical rest following
concussion
• Some more prone to concussion:
– History of previous TBI, LD, ADHS,
Neuro/psycho-emotional diagnosis
– Person or family history of HA
– Gender-Females
• Neck circumference
• Hormonal fluctuations153

Recovery:
• Cellular level changes even in those with functional recovery
• SLP support is crucial
• Visual-vestibular evaluation-reading
• Mechanism of Injury: TBI Trauma vs. Sports
• Education Setting: Parent, Student and Staff education
• *Work setting: Boss/ manager, Co-Workers
154

EVALUATION
155

EVALUATION
• Symptom Checklist
156

Evaluation-Adults
• Montreal Cognitive Assessment –MoCA
screening
• Wechsler Memory Scale III -Auditory, Working
and Verbal Memory
• Attention Processing Test -Attention
• Cognitive Linguistic Quick Test
• RIPA-2/RIPA G-2
• Assessment of Language-Related Functional
Activities (ALFA) -Functional ADLs
157

Quest for Cognitive Treatment Coverage
• Elaine Ledwon-Robinson, MS, CCC-SLP
• The ASHA Leader, June 2016, Vol 21, 20-
21.doi:101044/leader.GR.21062016.20
• The ASHA Leader, June 2016
158

Memory
159

Working Memory Facts
• May be referred to as Short-term Memory
• Core executive function that closely correlates to both IQ and attention stamina.
• Working memory can impact long-term learning outcomes
• Working memory is essential for comprehension, learning and reasoning that draws from several parts of the brain
– Frontal cortex
– Parietal cortex
160

Working Memory Facts
• Gender balance fairly even with slightly greater
proportion of males than females
• Fluctuates throughout the day and from day to day
• Slow to learn in the areas of reading math and
science
• Unable to meet memory demands of structured
learning activities
• Information is lost through overload or distraction
161

• Need to re-read text
• Difficulty following multi-step directions
• Difficulty attending during class
• Test anxiety
• Need for more time and repetition
• Inconsistent performance
• Lack of focus and attention deficits disorders
• Unable to hold material in mind and manipulate
the material
• Limited in capacity
162
Working Memory deficit checklist:

Struggle to Learn
• Learning is a step-by-step process
• Fail in classroom as working memory loads are too
demanding
• Working memory failure leads to inattentive
behaviors-forget what they are doing!
163

Evaluation
• Standardized Tests include two measures of working memory:
– Forward and backward digit span
436
371
2876
3987
32097
67482
Also consider…..
Auditory Memory
Visual Memory164

ATTENTION
165

Attention
166

Types of Attention
167
• Sustained Attention
• Focus on ONE specific task for a continuous
amount of time without distraction

Types of Attention
168
• Selective Attention
• Ability to select from many factors or stimuli and
focus on only the one you want while filtering out
other distractions

Types of Attention
169
• Alternating Attention
• Ability to switch your focus back and forth between
tasks that require different cognitive demands

Types of Attention
170
• Divided Attention
• Ability to process two or more responses or react
to two more different demands simultaneously.
• Multi-tasking!

TREATMENT
171

172

Classroom/Workplace/Home
Support
• Ways to avoid working memory overload in classroom
– Recognize working memory failures
– Monitor child
– Evaluate working memory load and reduce
– Simplify the load-chunk
– Use of memory guides such as wall charts, posters, memory cards
– Develop personal strategies such as note taking, place-keeping and organizational strategies.
173

Strategies for Cognitive Deficits
Concentrate first on general cognitive skills, such as flexible thinking and organization, rather than academic content.
Focus on what the student does well and expand the curriculum to more challenging content as concussion symptoms subside.
Adjust the schedule as needed to avoid fatigue: shorten day, time most challenging classes with time when student is most alert, allow for rest breaks, reduced course load.
Adjust the learning environment to reduce identified distractions or protect the student from irritations such as too-bright light or loud noises.
Use self-paced, computer-assisted, or audio learning systems for the student having reading comprehension problem
174

GAMES
Memory
Crazy 8
Magazines to circle
words, cut out
pictures
License plates
Card sort
Blink!
175

• Encourage active reading
– Take notes
– Use a highlighter
– Talk about it out loud and ask questions
176

• Chunk information into smaller bites
– Ex. Phone numbers, SS#
– Write down instructions step by step
177

• Make it multi-sensory
– Write down tasks
– Say them out loud
– Say them while completing a task
178

Walk and Talk
179

180

Additional Suggestions• One thing at a time
• To Do List
• One monitor
• Proof read email
• Lighting
• Set a timer for breaks
• Shopping off hours
181

Summary
182

183

Contact Numbers
• Bill Condon, PT, MPT
• Maria Davenport, MPT
• Jamie L Johnson, MA L/CCC-SLP BCS-S
• Claude Lamoureux, PT, DPT, NCS

Reference
• Broglio, S.P., Collins, M.W., Williams, R.M., Mucha, A., Kontos, A. (2015). Current and emerging rehabilitation for concussion: A review of the evidence. Clinical Sports Medicine, 34(2): 213-231.
• Choe M.C. (2016). The pathophysiology of concussion. Current Pain Headache Reports. DOI 10.1007/s11916-016-0573-9
• Cameron M. Marshall, Howard Vernon, John J. Leddy & Bradley A. Baldwin (2015) The role of the cervical spine in post-concussion syndrome, The Physician and Sportsmedicine, 43:3, 274-284.
• Domenech, M.A. et al. (2011). The deep neck flexor endurance test: normative data scores in healthy adults.PM&R 3(2): 105-10
• Hain T. Dizziness and Balance.com. 2015. http://www.dizziness-and-balance.com
• Herdman, S.J., Clendaniel, R.A. (2014). Vestibular rehabilitation. Philadelphia, PA: F.A. Davis Company.
• Kristjansson, E. Treleaven J., 92009). Sensorimotor function and dizziness in neck pain: Implications for Assessment and management. Journal of orthopaedic and sports physical therapy. 39(5): 364-377.
185

Reference
• Leddy, J.J. and Willer, B. (2013) . Use of graded exercise testing in concussion and return to activity management. Current Sports Medicine Reports. 12(6): 370-6.
• Leddy, J.J., Kozlowski, K., Donnelly, J.P., Pendergast, D.R., Epstein, L.H., Willer, B. (2010). A preliminary study of subsymptomthreshold exercise training for refractory post-concussion syndrome. Clinical Journal Sport Medicine, 20(1): 21-7.
• Leddy j.J, Baker J.G., Willer B. (2016). Active Rehabilitation of concussion and post-concussion syndrome. Physical Medicine and Rehabilitation Clinics of North America. 27: 437-454.
• McCrory, P. et al. (2017). Consensus statement on concussion in sport-the 5th international conference on concussion in sport held in Berlin, October 2016. British Journal Sports Medicine, 0:1-10
• Mucha, A., Collins, M.,Elbin, R.G., Furman, J., et al. (2014) A brief vestibular/ocular motor screening(VOMS) assessment to evaluate concussion. American Journal of Sports Medicine. 42(10):2479-2486.
• Neil, J.A., Adams, M.A., Dolan, P.(2015). Sensorimotor function of the cervical spine in healthy volunteers. Clinical Biomechanics, 30(3): 260-268.
186

Reference
• Ogince, M. et al. (2007). The diagnostic validity of the cervicalflexion-rotation test in c1/2-related cervicogenic headache. Manual Therapy, 12(3): 256-62.
• Reneker, J.C., Hassen, A., Phillips, R.S., Moughiman, M.C., Donaldson, M., Moughiman, J. (2017). Feasibility of early physical therapy for dizziness after a sports-related concussion: A randomized clinical trial. Scandinavian Journal of Medicine and Science in Sports, 1-10. doi: 10.1111/sms.12827.
• Sullivan S. Physical Rehabilitation. Vol 6th Ed. Philadelphia: F.A. Davis Company; 2014.
• Strelzik, J., Langdon, R. (2017). The role of active recovery and ‘rest” after concussion. Pediatric Annals 46(4): 139-144.
• Treleaven, J. (2017). Dizziness, unsteadiness, visual disturbances, and sensorimotor control in traumatic neck pain. Journal of orthopaedic and sports physical therapy. 47(7): 492-502.
• Treleaven J, Jull G, Atkinson L.(1994). Cervical musculoskeletal dysfunction in post-concussional headache. Cephalalgia;14:273–57.
• Vuillerme N, Pinsault N. Experimental neck muscle pain impairs standing balance in humans. Exp Brain Res 2008;192:723–9.
• Yorke, A.M., Smith, L., Babcock, M., lsalaheen, B. (2017). Validity and reliability of the vestibular/ocular motor screening and associations with common concussion screening tools. Sports Health, 9(2): 174-180.
187

Speech Pathology References:
Anderson T, Heitger M, Macleod A D. Concussion and
Mild head injury. Practical Neurology 2006; 6:342-357m
Brain Injury in Children and Youth: A Manual for
Educators Colorado Department of Education
cdc.gov/concussion
Canlearnsociety.ca
Elbin, R.J. et al. Factors Influencing Risk and Recovery
from Sport-Related Concussion: Reviewing the Evidence.
Perspectives on Neurophysiology and Neurogenic
Speech and Language Disorders. Vol 25, January 2015.
Hardin, K. The ASHA Leader, December 2015. Vol 20,
18-44 . Doi:10.1044/leader.FTR1.20122015.38.
Understood.org188

• Krug, H., Turkstra, L. Assessment of Cognitive-
Communication Disorders in Adults with Mild
Traumatic Brain Injury. Perspective on
Neurophysiology and Neurogenic Speech and
Language Disorders. Vol 25, January 2015.
ASHA.
• Ledwon-Robinson, Elaine. The ASHA Leader,
June 2016, Vol 21, 20-21. doi:
101044/leader.GR.21062016.20
189