Embed Size (px)
Citation preview
European Eating Disorders ReviewEur. Eat. Disorders Rev. 11, 210–221 (2003)Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/erv.516
Paper
Computers, E-mail and Therapy in EatingDisorders
Paul Robinson*1 and Marc Serfaty21Royal Free Eating Disorders Service, Royal Free Hospital, London, UK2Department of Psychiatry and Behavioural Sciences, Royal Free andUniversity College London Medical School, London, UK
Many ethical and practical questions have been asked in relation to the deliveryof therapy via e-mail including: is therapy delivered via e-mail acceptable toclients? Are people recruited into treatment via an e-mailed advertisementsimilar to a clinical sample? Is such therapy effective? Is there a therapeuticrelationship which involves expression of emotion, therapist empathy, and otherfeatures of the face-to-face therapeutic interaction? Is such therapy safe? Thispaper attempts to answer these questions based on findings from ongoingstudies on the use of cognitive behavioural treatment (CBT) delivered via e-mailto individuals with bulimic disorders. Copyright # 2003 John Wiley & Sons,
Ltd and Eating Disorders Association.
INTRODUCTION
The use of computers in the treatment of mental disorders is beingsuggested as an alternative to face-to-face treatment with a therapist. Inthe area of depression and anxiety, several studies have shown thatcomputerized CBT packages may be as effective and indeed preferredby patients (National Institute of Clinical Excellence, 2002). Severalmethods have been used with increasing sophistication, includingtelephone computerized packages such as BT Steps for obsessive–compulsive disorder (Nakagawa et al., 2000), COPE (Osgood-Hyneset al., 1998) and palmtop computer programs for generalized anxietydisorder (Newman, Consoli, & Talyor, 1999), or ‘Beating the Blues’
European Eating Disorders ReviewCopyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 11(3), 210–221 (2003)
*Correspondence to: Dr P. Robinson, Royal Free Eating Disorders Service, Royal Free Hospital,London NW3 2QG, UK. E-mail: [email protected]

(http://www:ultrasis:com) for depression. With the development of theinternet, it has been suggested that computerized CBT packages couldbe delivered ‘on-line’ (Ginger, Horan, Tompkins-Bjorkman, Kovalski, &Hackett, 2000) without the use of a therapist. Such approaches have beencriticized for the lack of interpersonal contact which is advocated as anessential part of the therapeutic relationship. However, while efficaciousfor many patients, being treated with a standardized approach may beless effective than tailor made treatments.
Computerized treatments, as described above, range between thosewhich completely avoid the intervention of a therapist and those, suchas e-mail or telephone therapy, in which the therapist sits at a distancefrom the individual requesting help.
E-mail therapy may be a way of delivering treatments where peoplewish to receive individual therapy in a more anonymous setting.Although the internet may merely be a new electronic means ofperforming an old activity, therapy (Skinner, 2001), this new modeof delivery may have many advantages over conventional methods oftreatment delivery, in particular by increasing client empowerment,accountability, affordability, convenience and privacy (Fingeld, 1999).Such treatment may be useful where geographical distance limits accessto treatment, or where the patient wishes to remain anonymous. Forexample, the Samaritans have for many years, offered an anonymousservice to people who may be suicidal, and in recent years have offeredan internet service providing a completely anonymous contact with acounsellor via e-mail (www.samaritans.org).
People who have difficulty in accessing services because of the natureof their psychological or physical symptoms, e.g. agoraphobia, mobilityproblems or body image disturbance may also benefit from thisapproach. Robinson and Serfaty (2001) found that the internet may bea useful way to recruit and treat those in whom engagement is aparticular problem. The authors conducted a pilot study on 23 peoplediagnosed with bulimia nervosa (BN) or related disorders. A number ofpatients in this trial commented that the use of e-mail enabled them tocontact services when normally they would not have done so.
EFFICACY, PRACTICAL AND ETHICAL ISSUES
A large number of websites devoted to provision of therapy for paymenton-line for a variety of problems has accumulated. These can be foundeasily using the search words ‘internetþ therapy’. In response to thisburgeoning activity, which has taken place mostly in the US, theInternational Society for Mental Health Online (www:ismho:org) has
Eur. Eat. Disorders Rev. 11, 210–221 (2003) Therapy Using Computers
Copyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 211

emerged, and their web-site includes clinical descriptions, webdiscussion and a scientific and research element. Actual outcomeresearch on e-mail and internet therapy is still very much in its infancy,with only a few case studies and small randomized controlled trialsdescribing the use of this treatment (Lange, van de Ven, Schrieken, &Emmelkamp, 2001; Murdoch & Connor-Green, 2000; Stroem, Pettersson,& Andersson, 2000; Wilson & Lester, 1998; Zabinski et al., 2001). Thus,there is little evidence to guide practice.
A number of ethical and practical concerns have been raised inrelation to the delivery of therapy via e-mail (Childress & Asamen, 1998;Manhal-Baugus, 2001; Oravec, 2000; Rothchild, 1997; Sampson, 2000).These include concern about loss of face-to-face contact, elitism, delayedon-site services and confidentiality (Fingeld, 1999). For example, therehas been some debate about whether or not warmth, caring andcompassion, which are integral to the development of a therapeuticrelationship, can be delivered by text (Murphy & Mitchell, 1998).
There have also been concerns about the safety of such treatment andit has been suggested that e-mail therapy is inappropriate for anyonewho is suicidal or has violent thoughts (Landau, 2001). The UK GeneralMedical Council has issued guidelines suggesting that therapeutic useof e-mail may be appropriate, but e-mail therapy is not recommended‘where standards of care may be seriously compromised if the patient is notpreviously known to the doctor, no examination can be provided, or there islittle or no provision for appropriate monitoring of the patient or follow-up care’(GMC, 2003). This issue is further complicated by a lack of licensing andregulation of people who may deliver treatments on line.
In order to address some of these concerns, a voluntary ethical codehas been adopted by three professional organizations in the USA(American Counseling Association, National Board of Certified Coun-selors and the International Society for Mental Health on-line; Manhal-Bergus, 2001). In the UK guidelines have yet to be developed.Furthermore, a number of legal issues remain unresolved, because ofthe problems of different laws across borders (Love, 2000).
A CONSIDERATION OF ISSUES RAISED
As outlined above a number of ethical and practical questions have beenasked about the delivery of therapy via e-mail including:
(1) Is therapy delivered via e-mail acceptable to clients?(2) Are people recruited into treatment via an e-mailed advertisement
similar to a clinical sample?(3) Is such therapy effective?
P. Robinson and M. Serfaty Eur. Eat. Disorders Rev. 11, 210–221 (2003)
Copyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 212
(4) Is there a therapeutic relationship which involves expression ofemotion, therapist empathy, and other features of the face-to-facetherapeutic interaction?
(5) Is such therapy safe?
In an attempt to address some of these questions we have analysedthe data from our 2001 study and from an ongoing study.
PARTICIPANTS AND METHODS
Data from two studies were used to answer the questions outlinedabove.
Study 1
An open study of CBT delivered via e-mail to 23 participants withbulimia nervosa or EDNOS recruited via an e-mail to the entire studentand staff population of a single multi-faculty London college of theUniversity of London. This study has been reported in Robinson andSerfaty (2001).
Study 2
This is an ongoing randomized controlled trial of CBT delivered viae-mail to another population derived from the same student and staffbase as Study 1. In what follows, data from the initial assessments of thefirst 29 participants of that study have been included.
Outcomes were evaluated using two self-report measures, namely theBulimic Investigatory Test, Edinburgh (BITE; Henderson & Freeman,1987) and Beck Depression Inventory (BDI); and patients were alsoasked to give qualitative comments on their treatment.
RESULTS
Acceptability of e-mail therapy
Quantitative information
None of the 23 participants in Study 1 and only two of the 29participants in Study 2 were currently receiving treatment for theireating disorder (total 2/52, 4 per cent). In the past, nine participants inStudy 1 and six in Study 2 (total 15/52, 29 per cent) had receivedtreatment for their eating disorder.
Asked, at the end of therapy, whether they would accept either face-to-face or e-mail therapy, of 19/23 participants in Study 1 who replied to
Eur. Eat. Disorders Rev. 11, 210–221 (2003) Therapy Using Computers
Copyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 213
this question, 10 (53 per cent) indicated they would be willing to acceptface-to-face therapy, and 5 (26 per cent) further on-line therapy.
Participants in Study 1 were asked to comment on their treatment and14/23 (61 per cent) did so.
Qualitative information
Comments about e-mail therapy specifically were:
Typing is just as hard as talking.I would never admit to my problem face to face.E-mail therapy is easier to ignore.I would never have responded in the first place without the anonymity ofe-mail therapy.You miss the personal touch without face-to-face contact.The anonymity afforded by this medium makes me feel I’m ready to seek help(face-to-face).E-mail gives you more time to think about your response than face-to-face.E-mail therapy can be a bit cold.Easier to misunderstand what is being communicated with e-mail.I made a lot of progress and want further e-mail therapy.I stopped laxative abuse, but couldn’t make the other changes.During the e-therapy I felt trapped, but a month after stopping I realize Idon’t have the problem any more.Although the problem has been approached I still need to look for its cause.
Most respondents felt they had been helped, either to reduce theirbulimia or to accept the idea of referral for treatment in a clinic. TheRoyal Free Eating Disorders Unit accepts referrals from the UniversityHealth Centre at the college studied, and in the year following Study 1,four of the 23 participants were referred for therapy, in addition to oneperson who had been turned down for the study due to low weight.
In summary, there was a balance of opinion about the positive andnegative aspects of e-mail therapy, and a large proportion felt it couldlead them to seeking treatment although, in the event, a rather smallnumber seemed to do so. The referral rate excludes participants whomay have been referred privately, or who were referred to NHS servicesother than the Royal Free, or who were referred abroad.
Clinical characteristics of the sample treated
Qualitative information
Many studies of eating disorders, particularly in the United States, areperformed on participants recruited via advertisement, and the questionis sometimes, rightly, raised, ‘Is this group similar to people I see in the
P. Robinson and M. Serfaty Eur. Eat. Disorders Rev. 11, 210–221 (2003)
Copyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 214
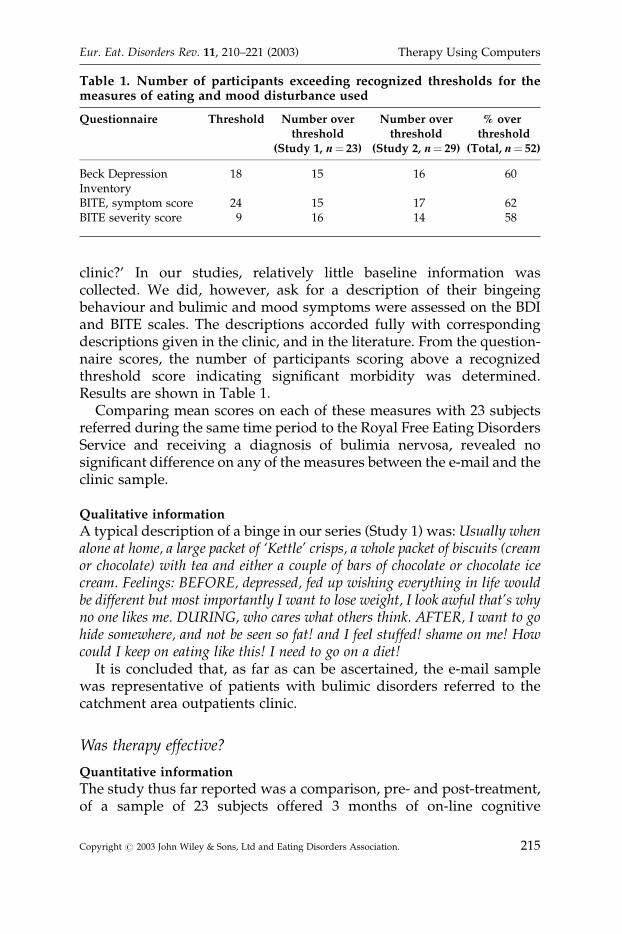
clinic?’ In our studies, relatively little baseline information wascollected. We did, however, ask for a description of their bingeingbehaviour and bulimic and mood symptoms were assessed on the BDIand BITE scales. The descriptions accorded fully with correspondingdescriptions given in the clinic, and in the literature. From the question-naire scores, the number of participants scoring above a recognizedthreshold score indicating significant morbidity was determined.Results are shown in Table 1.
Comparing mean scores on each of these measures with 23 subjectsreferred during the same time period to the Royal Free Eating DisordersService and receiving a diagnosis of bulimia nervosa, revealed nosignificant difference on any of the measures between the e-mail and theclinic sample.
Qualitative information
A typical description of a binge in our series (Study 1) was: Usually whenalone at home, a large packet of ‘Kettle’ crisps, a whole packet of biscuits (creamor chocolate) with tea and either a couple of bars of chocolate or chocolate icecream. Feelings: BEFORE, depressed, fed up wishing everything in life wouldbe different but most importantly I want to lose weight, I look awful that’s whyno one likes me. DURING, who cares what others think. AFTER, I want to gohide somewhere, and not be seen so fat! and I feel stuffed! shame on me! Howcould I keep on eating like this! I need to go on a diet!
It is concluded that, as far as can be ascertained, the e-mail samplewas representative of patients with bulimic disorders referred to thecatchment area outpatients clinic.
Was therapy effective?
Quantitative information
The study thus far reported was a comparison, pre- and post-treatment,of a sample of 23 subjects offered 3 months of on-line cognitive
Table 1. Number of participants exceeding recognized thresholds for themeasures of eating and mood disturbance used
Questionnaire Threshold Number over Number over % overthreshold threshold threshold
(Study 1, n¼ 23) (Study 2, n¼ 29) (Total, n¼ 52)
Beck Depression 18 15 16 60InventoryBITE, symptom score 24 15 17 62BITE severity score 9 16 14 58
Eur. Eat. Disorders Rev. 11, 210–221 (2003) Therapy Using Computers
Copyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 215
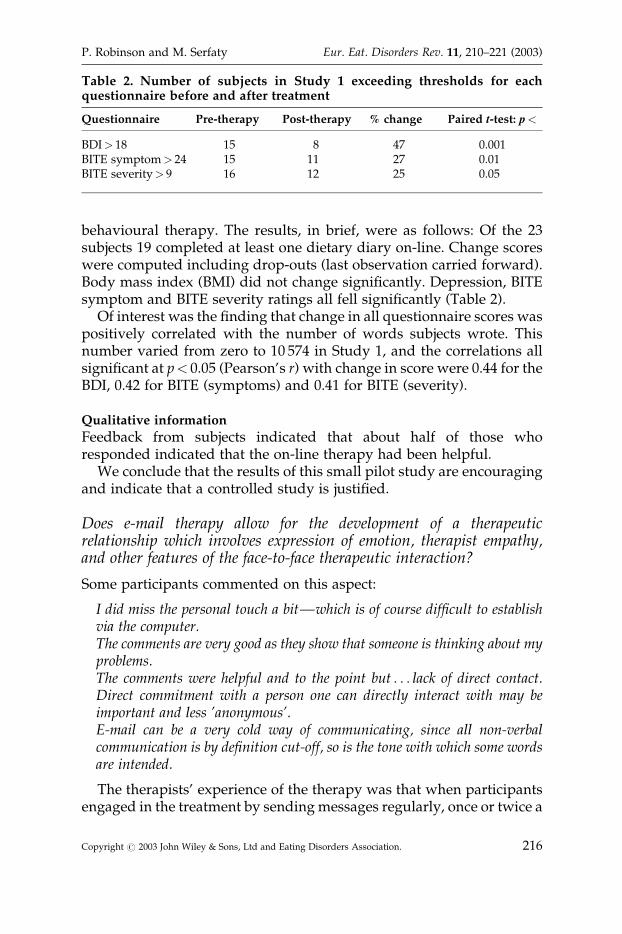
behavioural therapy. The results, in brief, were as follows: Of the 23subjects 19 completed at least one dietary diary on-line. Change scoreswere computed including drop-outs (last observation carried forward).Body mass index (BMI) did not change significantly. Depression, BITEsymptom and BITE severity ratings all fell significantly (Table 2).
Of interest was the finding that change in all questionnaire scores waspositively correlated with the number of words subjects wrote. Thisnumber varied from zero to 10 574 in Study 1, and the correlations allsignificant at p< 0.05 (Pearson’s r) with change in score were 0.44 for theBDI, 0.42 for BITE (symptoms) and 0.41 for BITE (severity).
Qualitative information
Feedback from subjects indicated that about half of those whoresponded indicated that the on-line therapy had been helpful.
We conclude that the results of this small pilot study are encouragingand indicate that a controlled study is justified.
Does e-mail therapy allow for the development of a therapeuticrelationship which involves expression of emotion, therapist empathy,and other features of the face-to-face therapeutic interaction?
Some participants commented on this aspect:
I did miss the personal touch a bit—which is of course difficult to establishvia the computer.The comments are very good as they show that someone is thinking about myproblems.The comments were helpful and to the point but . . . lack of direct contact.Direct commitment with a person one can directly interact with may beimportant and less ’anonymous’.E-mail can be a very cold way of communicating, since all non-verbalcommunication is by definition cut-off, so is the tone with which some wordsare intended.
The therapists’ experience of the therapy was that when participantsengaged in the treatment by sending messages regularly, once or twice a
Table 2. Number of subjects in Study 1 exceeding thresholds for eachquestionnaire before and after treatment
Questionnaire Pre-therapy Post-therapy % change Paired t-test: p<
BDI> 18 15 8 47 0.001BITE symptom> 24 15 11 27 0.01BITE severity> 9 16 12 25 0.05
P. Robinson and M. Serfaty Eur. Eat. Disorders Rev. 11, 210–221 (2003)
Copyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 216
week, and when a substantial amount was written, there were signs thata therapeutic relationship was developing. Participants would useinformal language, calling the therapist ‘doc’ or ‘e-doc’, and emotionwas certainly strongly expressed at times. In one case, in Study 2, asubject wrote a furious e-mail in Spanish, indicating how angry she waswith the therapist for neglecting her. In fact, her previous e-mail hadgone astray, and the therapist was waiting for further contact.Subsequent therapy in that case (in English) was quite productive anduseful. Sometimes comments that might be made face to face were not souseful via e-mail. In one case, in Study 1, a subject related how hermother insisted on sending her boxes of cakes and chocolates althoughshe was fully aware of her daughter’s bulimia. The therapist began toexplore the mother–daughter relationship and this was met with arather affronted ‘There’s nothing wrong with our relationship, it’sabsolutely fine’. It seemed that the nuances of expression, tone, andposture absent in e-mail therapy, made sensitive exploration moredifficult using that medium, and finding other sources of communica-tion within the e-mail messages became an important task.
Is such therapy safe?
The Research Ethics Committee of the hospital at which this work wascarried out spent an unusually long time discussing the project, longer,in fact, than any other project for several years. The issues raised relatedto the fact that treatment was to be provided without the clinician everseeing the ‘patient’. Concern was raised that participants might becomeill either physically or mentally, perhaps as a result of disclosingdistressing material during treatment, and that there was limited abilityto intervene, for example by making a risk assessment and deciding onthe appropriate course of action, as occurs in face to face clinical practice.Secondly, it was argued that some people might pretend they had eatingdisorders in order to obtain treatment on-line. The first issue raised was,to the authors, the most important one. It was argued that someorganizations, such as the Samaritans, already have an anonymoustelephone and web-based support system for people in distress.Secondly, any subject revealing worrying information such as suicidalthoughts, or frequent vomiting requiring a blood test to excludehypokalaemia, was advised to visit the University Health Centre. Ifconcern continued, the Health Centre would be informed and makecontact with the individual herself. The therapy was not, therefore,anonymous, in that we had all the participants’ e-mail addresses andnames. The protocol was, therefore, accepted, and in the two studies,totalling 52 participants, no major concern about the safety of an
Eur. Eat. Disorders Rev. 11, 210–221 (2003) Therapy Using Computers
Copyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 217

individual has arisen. Some were asked to visit their doctors, to have apotassium check or to discuss depression or possible referral for eatingdisorders therapy, and, so far, five of the participants in Study 1 havebeen referred to the Royal Free Eating Disorders Service.
DISCUSSION
From our work and that of others there are indications that for certainindividuals, e-mail might represent an acceptable medium for ther-apeutic work. There is some evidence that it may produce a benefit andno evidence of harm when it is provided by skilled clinicians. Moreover,in our studies in patients with bulimia nervosa, advertising theavailability of treatment electronically seems to have helped to engageindividuals in treatment who would otherwise have been unlikely to askfor help through more traditional routes. At present, the vast majority ofcases of bulimia nervosa in the community are unknown to their generalpractitioners (van Hoeken, Lucas, & Hoek, 1998) and receive notreatment (Fairburn et al., 1996) even though they frequently consulttheir general practitioners for other reasons (Ogg, Millar, Pusztai, &Thom, 1997). Thus, e-mail therapy has the potential to overcomemajor barriers to help-seeking.
It seems to us that the medium of e-mail therapy lends itself very wellto the study of treatment outcome and process and the assessmentof therapist competency and further work is needed. For example,whilst it had been suggested (Murphy & Mitchell, 1998) that non-specific factors such as warmth and empathy cannot be communicatedusing a written medium, there is no reason why it would not be possibleto evaluate the quality and warmth of a therapeutic interaction usingtextual analysis.
Regarding therapist competency, we argue that e-therapy provides apotentially useful way to monitor general competency and adherence toa specific therapeutic model. In e-mail therapy, a therapist can sendcopies to a supervisor who can annotate them and return them to thetherapist. Adherence to, for example, a cognitive behavioural approach,can be monitored using Beck’s (Beck, Rush, Shaw, & Emory, 1979; Valliset al., 1986) Competency Checklist for cognitive therapy in which anumber of factors, regarded as important in using cognitive behaviouralinterventions, are rated. A particular strength of e-mail therapy is theuse of specific cognitive behavioural techniques which focus on keythoughts using, for example, the triple column and other techniques.There do however, need to be some adaptations to the scale, which inpart relies on non-verbal cues, such as therapists’ dress and demeanour,
P. Robinson and M. Serfaty Eur. Eat. Disorders Rev. 11, 210–221 (2003)
Copyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 218

which cannot be assessed in e-mail therapy. Nevertheless, the use of on-line supervision by trained individuals, can be used to improve the skillsof therapists doing this work.
The nature of e-mail makes it accessible worldwide, although varyingregulations in different countries and states might restrict practitionerswithin countries with less permissive legislation. E-mail is notparticularly secure, and, if internet therapy is to continue to develop,the use of secure websites to hold messages may become morewidespread, allowing a confidential, personal therapeutic service,without the need to see the therapist face to face. The problem raisedby our Research Ethics committee, that people might become distressedduring therapy, remains, and therapists and participants will need toaccept that there will be little opportunity, apart from messages via theweb, to intervene. This is, of course, one example of the shift in powerbalance towards the subject that is a characteristic of e-mail and webtherapy, and could be seen on balance as an advantage.
It is likely that therapy delivered via e-mail will take its place amongother therapeutic media, including those involving face to face, writtenand telephone contact and that contact by e-mail when a client, usuallyseen face to face, is away from home, may become increasingly a part ofnormal clinical practice. Preliminary findings suggest a possible clinicalbenefit from therapy for bulimic disorders delivered via e-mail.Whether for a proportion of participants e-mail can ever replace face-to-face therapeutic contact is a question for further study.
REFERENCES
Beck, A. T., Rush, A. J., Shaw, B. F., & Emory G. (1979), The cognitive therapy ofdepression. New York: Guilford Press.
Childress, C. A., & Asamen, J. K. (1998). The emerging relationship ofpsychology and the internet: Proposed guidelines for conductinginternet intervention research. Ethics and Behavior, 8, 19–35.
Fairburn, C. G., Welch, S. L., Norman, P. A., O’Connor, M. E., Doll, H. A. (1996).Bias and bulimia nervosa: How typical are clinic cases? AmericanJournal of Psychiatry, 153, 386–391.
Fingeld, D. L. (1999). Psychotherapy in cyberspace. Journal of the AmericanPsychiatric Nursing Association, 5, 105–110.
General Medical Council (2003). Providing advice and medical services on-lineor by telephone. http://www.gmc-uk.org
Ginger, C., Horan, J., Tompkins-Bjorkman, A., Kovalski, T., & Hackett, G.(2000). Interactive career counseling on the internet. Journal of CareerAssessment, 8, 85–93.
Eur. Eat. Disorders Rev. 11, 210–221 (2003) Therapy Using Computers
Copyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 219
Henderson, M., & Freeman, C. P. (1987). A self-rating scale for bulimia: TheBITE. British Journal of Psychiatry, 150, 18–24.
Lange, A., van de Ven, J. P., Schrieken, B., & Emmelkamp, P. M. (2001).Interapy, treatment of posttraumatic stress through the Internet: Acontrolled trial. Journal of Behaviour Therapy and Experimental Psychiatry,32, 73–90.
Landau, B. M. (2001). Psychotherapy online in 2001: For psychotherapists newto the Internet. Journal of Mental Imagery, 25, 65–82.
Love, J. S. (2000). Cybercounselors v. Cyberpolice. In J. W. Bloom, & G. R. Walz(Eds.), Cybercounseling and cyberlearning: Strategies and resources for themillennium (pp. 339–360). Alexandria, VA, US: American CounselingAssociation.
Manhal-Baugus, M. (2001). E-therapy: Practical, ethical, and legal issues.Cyberpsychology and Behaviour, 4, 551–563.
Murdoch, J., & Connor-Greene, P. (2000). Enhancing therapeutic impact andtherapeutic alliance through electronic mail homework assignments.Journal of Psychotherapy Practice and Research, 9, 237–242.
Murphy, L. J., & Mitchell, D. L. (1998). When writing helps to heal: E-mail as atherapy. British Journal of Guidance Counselling, 26, 21–32.
Oravec, J. A. (2000). Online counselling and the internet: Persepectives for themental health care supervision and education. Journal of Mental Health(UK), 9, 121–135.
Osgood-Hynes, D. J., Greist, J.H., Marks, I. M., Baer, L., Heneman, S. W.,Wenzel, K. W., Manzo, P. A., Parkin, J. R., Spierings, C. J., Dottl, S. L., &Vitse, H. M. (1998). Self-administered psychotherapy for depressionusing a telephone-accessed computer system plus booklets: An openUS–UK study. Journal of Clinical Psychiatry, 59, 358–365.
Nakagawa, A., Marks, I. M., Park, J. M., Bachofen, M., Baer, L., Dottl, S. L., &Greist, J. H. (2000). Self-treatment of obsessive–compulsive disorderguided by manual and computer-conducted telephone interview.Journal of Telemedicine & Telecare, 6, 22–26.
National Institute of Clinical Excellence. (2002). Guidance on the use ofcomputerised cognitive behavioural therapy for anxiety and depres-sion. Technology Appraisal Guidance, No. 51.
Newman, M. G., Consoli, A. J., & Talyor, C. B. (1999). A palmtop computerprogram for the treatment of generalised anxiety disorder. BehaviourModification, 23, 597–619.
Ogg, E. C., Millar, H. R., Pusztai, E. E., & Thom, A. S. (1997). General practiceconsultation patterns preceding diagnosis of eating disorders. Interna-tional Journal of Eating Disorders, 22, 89–93.
Robinson, P. H., & Serfaty, M. A. (2001). The use of e-mail in the identificationof bulimia nervosa and its treatment. European Eating Disorders Review,9, 182–193.
Rothchild, E. (1997). E-mail therapy. American Journal of Psychiatry, 154, 1476–1477.
P. Robinson and M. Serfaty Eur. Eat. Disorders Rev. 11, 210–221 (2003)
Copyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 220
Sampson, J. P. (2000). Using the internet to enhance testing in counseling.Journal of Counseling & Development, 78, 348–356.
Skinner, A. (2001). Online therapy: A cause for concern. Psycholoogist, 14, 248.Stroem, L., Pettersson, R., & Andersson, G. (2000). A controlled trial of self-help
treatment of recurrent headache conducted via the internet. AmericanJournal of Consulting and Clinical Psychology, 68, 722–727.
Vallis, T. M., Shaw, B. F., & Dobson, K. D. (1986). The Cognitive Therapy Scale:Psychometric properties. Journal of Consulting and Clinical Psychology,54, 381–385.
van Hoeken, D., Lucas, A. R., & Hoek, H. W. (1998). Epidemiology. In H. W.Hoek, J. L. Treasure, & M. A. Katzman (Eds.), Neurobiology in thetreatment of eating disorders. Chichester: John Wiley & Sons.
Wilson, G., & Lester, D. (1998). Suicide prevention by e-mail. Crisis Intervention& Time-Limited Treatment, 4, 81–87. www:gbhap-us:com
Zabinski, M., Wilfley, D. E., Puung, M. A., Winzelberg, A. J., Eldredge, K., &Barr, T. C. (2001). An interactive internet-based intervention for womenat risk of eating disorders: A pilot study. International Journal of EatingDisorders, 20, 129–137.
Eur. Eat. Disorders Rev. 11, 210–221 (2003) Therapy Using Computers
Copyright # 2003 John Wiley & Sons, Ltd and Eating Disorders Association. 221