Embed Size (px)
Citation preview

Compuferixd Rudiol. Vol. IO, No. 6, pp. 31 l-318, 1986 0730-4862/86 $3.00 + 0.00 Printed in the U S.A. All rights reserved Pergamon Journals Ltd
COMPUTERIZED TOMOGRAPHY FINDINGS IN POSTERIOR FOSSA LESIONS
IRITH REIDER-GROSWASSER,’ AMIRAM CATZ** and IAIR Luz3 ‘Departments of Radiology and ‘Neurosurgery, Tel-Aviv Medical Center, and Loewenstein Rehabilitation
Hospital Ra’anana and ‘Tel-Aviv University Sackler School of Medicine, Tel-Aviv, Israel
(Received 2 I February 1986; in revised form IO June 1986; received ,fijr publication 4 July 1986)
Abstract-In 190 of 7000 brain CT studies performed between April 1978 and September 1984, abnormalities of the posterior fossa were found. Of these, 51.5% were primary tumors, 15.3% metastases, 12. I % vascular lesions and 5.8% congenital or developmental lesions. Frequencies, age and sex distribution and radiologic characteristics of the various posterior fossa pathologies are reviewed and discussed.
Posterior fossa lesions Computerized tomography
INTRODUCTION
The difficulties in the radiological diagnosis of posterior fossa (PF) lesions have been largely overcome since the use of computerized tomography (CT). The various pathologies occurring in the PF have been annotated by several authors [l-6]. In the present study, abnormal findings in PF CT of 190 patients are reviewed, analysed and compared with data obtained from the literature.
MATERIALS AND METHODS
About 7000 hospitalized and ambulatory patients were referred for CT study of the brain during the period April 1978 to September 1984. One hundred and ninety of them, who presented abnormalities of the PF, were selected for this study. Among them, 57% were females and 43% were males. Their ages ranged from 6 days to 80 years. 43 patients were under 15 years of age, and 147 were above this age. In 88 cases histologic diagnosis was obtained. Of the 98 primary tumors, of which 12 were recurrent, histology was obtained in 81 cases. The other 17 primary tumors were acoustic neurinomas. This diagnosis was based on the clinical features i.e. hearing loss, abnormal brainstem evoked potentials and typical radiological findings including widening of internal acoustic canal, extra-axial location in cerebella-pontine angle, sharp borders and homogenous contrast enhancement. Histology was obtained in 4 patients with single metastases and unknown primary tumor. In the other 25 cases the diagnosis was based on known primary tumors and demonstration of multiple enhanced lesions. In the vascular group histological diagnosis was made in a patient with acute cerebellar infarction. In the patients with an aneurysm of posterior inferior cerebellar artery and arterio-venous malformation, the diagnosis was made by angiography. The diagnosis of the remaining vascular cases was based on clinical findings, follow-up and the characteristic CT features of acute hemorrhage or infarct. Histologic confirmation was obtained in two arachnoid cysts. In the other 9 congenital lesions the diagnosis was based on clinical data and radiological findings. In 13 cases of atrophy the diagnosis was based on CT findings. In the case of empyema there was surgical verification. In the other miscellaneous lesions, the diagnosis was based on clinical, laboratory and CT findings. In 11 patients the diagnosis could not be made on the basis of the available data (“unclassified”).
All CT studies were performed on an Elscint 710 Scanner. Contrast material was injected in most of the cases. In three patients an air canaliculogram was performed in addition to contrast enhanced CT studies. Routine cuts of 12 mm width and 10 mm distance were taken 15-25” to Reid’s baseline. In some of the patients 8 mm width slices and coronal cuts were obtained as well. Measurements were made by a transparent ruler on radiographic films. These were used to determine the maximal
* Present address: Loewenstein Rehabilitation Hospital, P.O. Box 3, Ra’anana 43100, Israel.
311
312 IRITH REIDER-GROSWASSER et al.
diameter of lesions and the bifrontal cerebra-ventricular index (CVI-1) calculated according to the method described by Hahn and Rim [7]. Other radiological features were evaluated qualitatively.
RESULTS
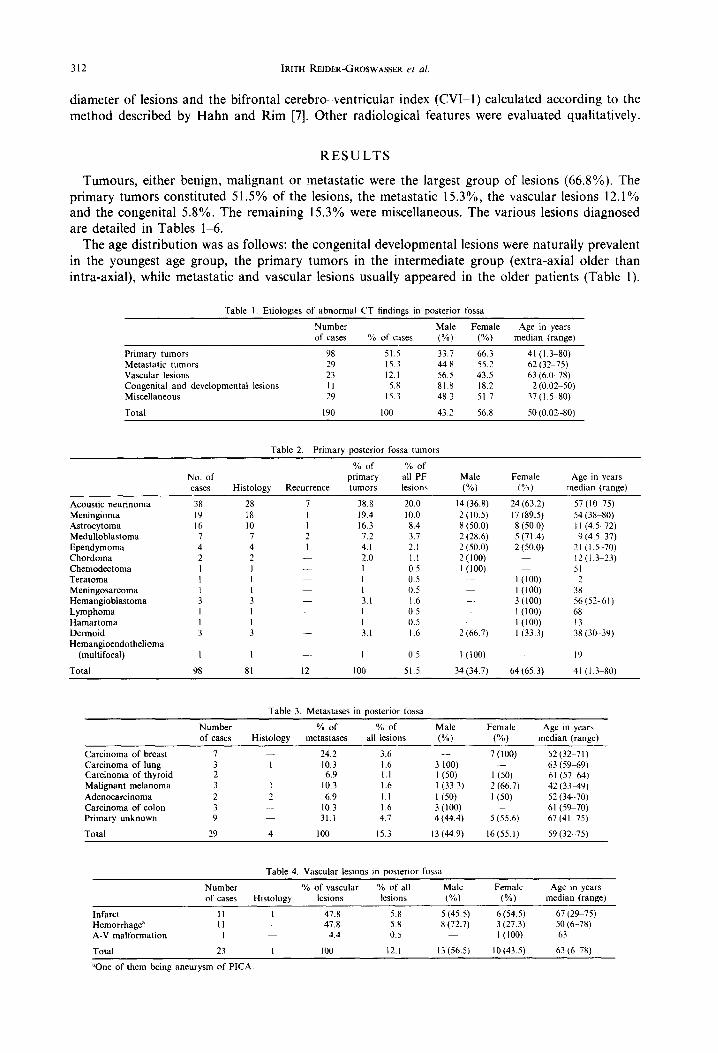
Tumours, either benign, malignant or metastatic were the largest group of lesions (66.8%). The primary tumors constituted 51.5% of the lesions, the metastatic 15.3%, the vascular lesions 12.1% and the congenital 5.8%. The remaining 15.3% were miscellaneous. The various lesions diagnosed are detailed in Tables l-6.
The age distribution was as follows: the congenital developmental lesions were naturally prevalent in the youngest age group, the primary tumors in the intermediate group (extra-axial older than intra-axial), while metastatic and vascular lesions usually appeared in the older patients (Table 1).
Table 1. Etioloeies of abnormal CT findines m oosterior fossa
Number of cases % of cases
Male Female Age in years (%) (%) median (range)
Primary tumors 98 51.5 33.7 66.3 41 (I .3S80) Metastatic tumors 29 15.3 44.8 55.2 62 (32-75) Vascular lesions 23 12.1 56.5 43.5 63 (6.0-78) Congenital and developmental lesmns II 5.8 81.8 18.2 2 (0.02-50) Miscellaneous 29 15.3 48.3 51.7 37(1.5-80)
Total 190 100 43.2 56.X 50 (0.02 -801
Table 2. Primary posterior fossa tumors
No. of cases
% of % of primary all PF Male Female Age in years
Histology Recurrence tumors lesions (%) (%I median (range)
Acoustic neurinoma Meningioma Astrocytoma Medulloblastoma Ependymoma Chordoma Chemodectoma Teratoma Meningosarcoma Hemangioblastoma Lymphoma Hamartoma Dermoid Hemangioendothelioma
(multifocal)
Total
38 28 19 18 16 IO 7 7 4 4 2 2 I I I I I I 3 3 I I I I 3 3
I I 98 81
7 38.8 I 19.4 I 16.3 2 7.2 I 4.1
2.0 I I I 3.1 I I 3.1
I 12 100
20.0 10.0 8.4 3.7 2.1 1.1 0.5 0.5 0.5 I.6 0.5 0.5 I.6
0.5
51.5
I4 (36.8) 2 (10.5) 8 (50.0) 2 (28.6) 2 (50.0) 2 (100) l(lO0)
._
2 (66.7)
I(100) 34 (34.7)
24 (63.2) 17 (89.5) 8 (50.0) 5 (71.4) 2 (50.0)
l(lO0) I (loo) 3 (100) l(lO0) I(lO0) I (33.3)
64 (65.3)
Table 3. Metastdses in oosterior fossd
57 (l&75) 54 (3X-80) I I (4.5.-72) 9 (4.5S37)
2 I (I .5-70) 12(1.3-23) 51 2
38 56(52-61) 68 I3 38 (30 39)
1’)
41 I I .3SXOI
Number of cases Histology
% of % of Male Female Age in years metastases all lesions (%) (“A) median (range)
Carcinoma of breast 7 24.2 3.6 Carcinoma of lung 3 I 10.3 1.6 Carcinoma of thyroid 2 6.9 I.1 Malignant melanoma 3 I 10.3 1.6 Adenocarcinoma 2 2 6.9 I.1 Carcinoma of colon 3 10.3 1.6 Primary unknown 9 31.1 4.7
29 4 100 15.3
7(lOO) 52 (32-71) 3 100) - 63 (59-69) I (50) I (50) 61 (57-64) I(33.3) 2 (66.7) 42 (3349) I Pa I (50) 52 (34 70) 3(100) 61 (59-70) 4 (44.4) 5 (55.6) 67 (41-75)
I3 (44.9) 16c55.1) 59(32 75)
Table 4. Vascular lesions m posterior fossa
Infarct Hemorrhage"
A-V malformation
Total
Number % Of VaSCUhr % of all Male Female Age in years of cases Histology lesions lesions (%) (%) median (range)
II I 47.8 5.x 5 (45.5) 6 (54.5) 67 (29-75) II 47.8 5.X 8 (72.7) 3 (27.3) 50 (6.-78)
I 4.4 0.5 I(lO0) 63
23 I 100 12.1 13 (56.5) IO (43.5) 63 (IS 78)
“One of them being aneurysm of PICA
CT findings in posterior fossa lesions 313
Table 5. Congenital lesions in posterior fossa
Number % of congenital % of all Male Female Age in years of cases Histoloev lesions lesions wo) (0~1 median Iranne~
Arachnoid cyst 8 2 12.1 4.2 8 (100) 2.2 (0.240) Dandy-Walker variant 2 18.2 I.1 1 (50) 1 (50) 0.04 (0.02~ 0.07) Supra-pineal cyst I 9.1 0.5 I(lO0) 50
Total II 2 100 5.8 9 181.8) 2 (IS.21 2 (0.02- 50)
Table 6. Miscellaneous lesions in posterior fossa
Atrophy Cerebritis Subdural empyema Leukemia Sarcoidosis Calcifications Unclassified
Total
Number % of miscellaneous % of all Male Female Age m years of cases Histology lesions lesions (%) (%) median (range)
I3 44.9 6.9 8 (61.5) 5 (38.5) 14(1.5 54) I 3.4 0.5 I(lO0) -. 6 I 3.4 0.5 I(lO0) ?I I 3.4 0.5 I(lO0) 6 I 3.4 0.5 I(lO0) 72 I 3.4 0.5 I 60, 54
II 38.0 5.8 3 (27.3) 8 (72.7) 52 J-80) (I
29 100 15.3 I4 (48.2) 15(51.8) 38(1.5 80)
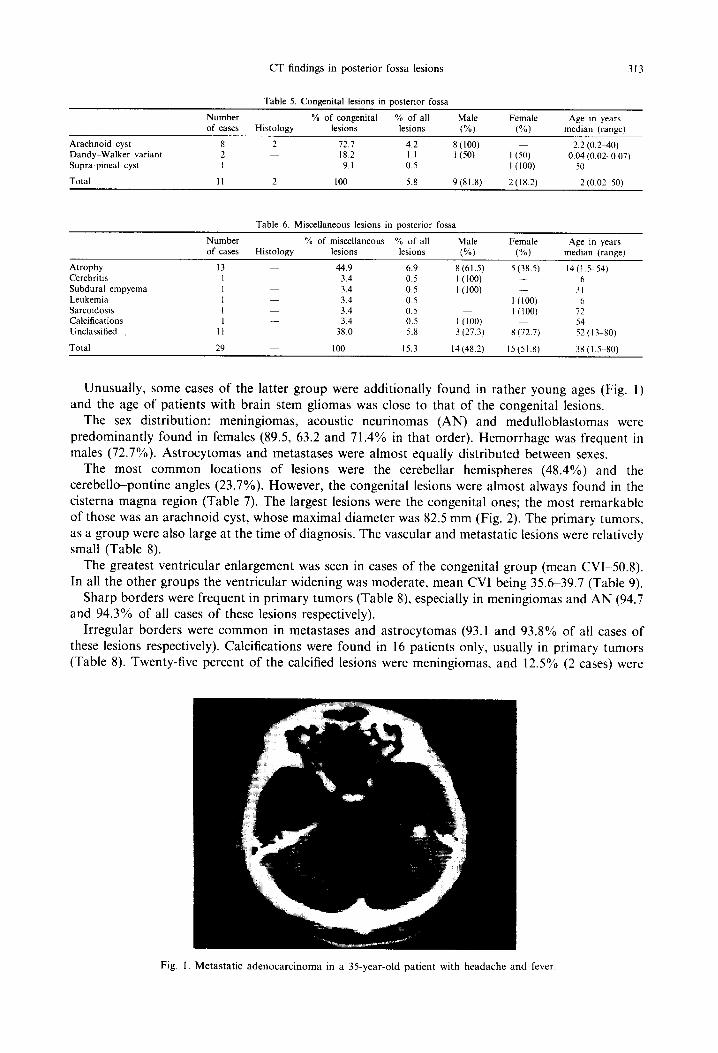
Unusually, some cases of the latter group were additionally found in rather young ages (Fig. 1) and the age of patients with brain stem gliomas was close to that of the congenital lesions.
The sex distribution: meningiomas, acoustic neurinomas (AN) and medulloblastomas were predominantly found in females (89.5, 63.2 and 71.4% in that order). Hemorrhage was frequent in males (72.7%). Astrocytomas and metastases were almost equally distributed between sexes.
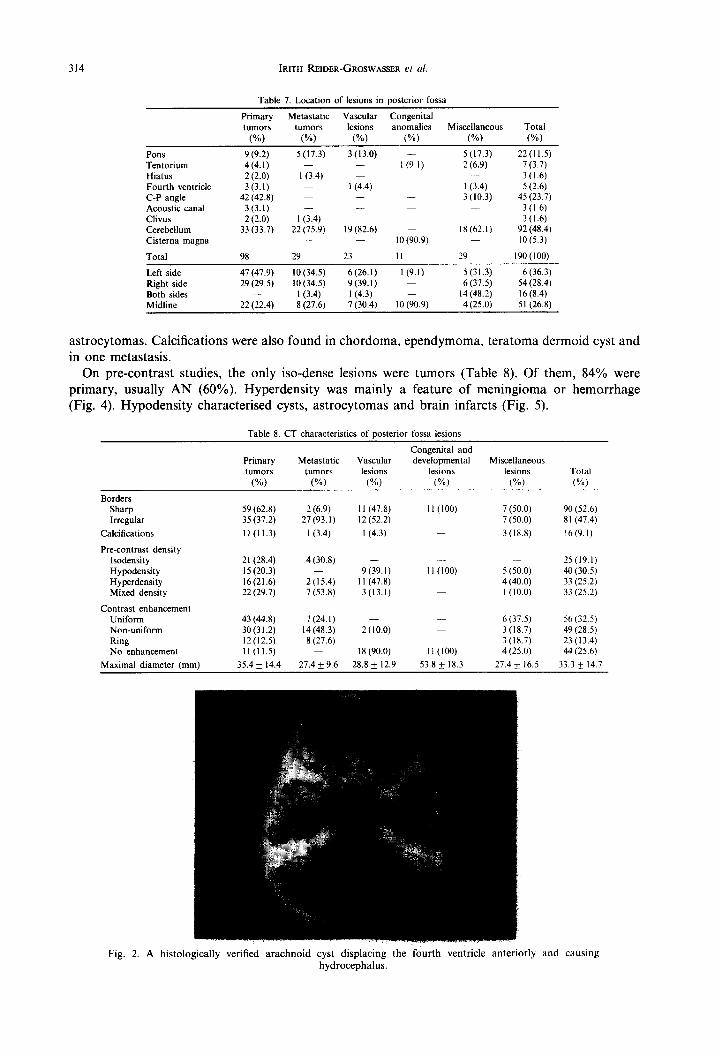
The most common locations of lesions were the cerebellar hemispheres (48.4%) and the cerebella-pontine angles (23.7%). However, the congenital lesions were almost always found in the cisterna magna region (Table 7). The largest lesions were the congenital ones; the most remarkable of those was an arachnoid cyst, whose maximal diameter was 82.5 mm (Fig. 2). The primary tumors, as a group were also large at the time of diagnosis. The vascular and metastatic lesions were relatively small (Table 8).
The greatest ventricular enlargement was seen in cases of the congenital group (mean CVl-50.8). In all the other groups the ventricular widening was moderate, mean CVI being 35.639.7 (Table 9).
Sharp borders were frequent in primary tumors (Table 8), especially in meningiomas and AN (94.7 and 94.3% of all cases of these lesions respectively).
Irregular borders were common in metastases and astrocytomas (93.1 and 93.8% of all cases of these lesions respectively). Calcifications were found in 16 patients only, usually in primary tumors (Table 8). Twenty-five percent of the calcified lesions were meningiomas, and 12.5% (2 cases) were
Fig. 1. Metastatic adenocarcinoma in a 35-year-old patient with headache and fever
314 IRITH REIDER-GR~SWASER et al.
Table 7. Location of lesions in posterior fossa
Primary Metastatic Vascular Congenital tumors tumors lesions anomalies Miscellaneous Total
(%) (“/) (X) W) W) W)
Pons Tentorium Hiatus Fourth ventricle C-P angle Acoustic canal Clivus Cerebellum Cisterna magna
9 (9.2) 4(4.1) 2 (2.0) 3 (3.1)
42 (42.8) 3 (3.1) 2 (2.0)
33 (33.7)
Total 98
5 (17.3) 3(13.0) - 5 (17.3) I (9. I) 2 (6.9)
I (3.4) 1 (4.4) I (3.4)
3 (10.3) _
I (3.4) _
22 (75.9) I9 (82.6) I8 (62.1) IO (90.9) -
29 23 II 29
22(11.5) l(3.7) 3(1.6) 5 (2.6)
45 (23.7) 3 (I 6) 3(1.6)
92 (48.4) lO(5.3)
190(100)
Left side Right side Both sides Midline
47 (47.9) 10 (34.5) 6 (26.1) l(9.1) 5(31.3) 6 (36.3) 29 (29.5) 10 (34.5) 9 (39.1) 6 (37.5) 54 (28.4)
I (3.4) I (4.3) I4 (48.2) 16 (8.4) 22 (22.4) 8 (27.6) 7 (30.4) IO (90.9) 4 (25.0) 51 (26.8)
astrocytomas. Calcifications were also found in chordoma, ependymoma, teratoma dermoid cyst and in one metastasis.
On pre-contrast studies, the only iso-dense lesions were tumors (Table 8). Of them, 84% were primary, usually AN (60%). Hyperdensity was mainly a feature of meningioma or hemorrhage (Fig. 4). Hypodensity characterised cysts, astrocytomas and brain infarcts (Fig. 5).
Table 8. CT characteristics of posterior fossa lesions
Borders Sharp Irregular
Calcifications
Pre-contrast density Isodensity Hypodensity Hyperdensity Mixed density
Contrast enhancement Uniform Non-uniform Ring No enhancement
Maximal diameter (mm)
Congenital and Primary Metastatic Vascular developmental Miscellaneous tumors tumors lesions lesions lesions Total
W) W) (“/) W) W) W)
59 (62.8) 2 (6.9) I I (47.8) II (100) 7 (50.0) 90 (52.6) 35 (37.2) 27(93.l) 12 (52.2) l(50.0) 81 (47.4)
11 (11.3) I (3.4) I (4.3) _ 3(18.X) 16(9.l)
21 (28.4) 4 (30.8) _. 25(19.1) I5 (20.3) 9(39.1) I I (100) 5 (50.0) 40 (30.5) 16(21.6) 2(15.4) I I (47.8) 4 (40.0) 33 (25.2) 22 (29.7) 7 (53.8) 3(13.1) I(lO.0) 33 (25.2)
43 (44.8) 7 (24.1) 6(37.5) 56 (32.5) 30 (3 I .2) 14148.3) 2(10.0) 3 (18.7) 49 (28.5) 12(12.5) 8 (27.6) 3 (18.7) 23(13.4) II (11.5) I8 (90.0) II (100) 4 (25.0) 44 (25.6)
35.4 * 14.4 27.4 f 9.6 28.8 f 12.9 53.8 + 18.3 27.4 & 16.5 33.3 * 14.7
Fig. 2. A histologically verified arachnoid cyst displacing the fourth ventricle anteriorly and causing hydrocephalus.
CT findings in posterior fossa lesions 315
Table 9. Tumor associated CT tindinns
Primary turnours
(%)
Metastatic turnours
I%)
Vascular lesions
(%)
Conpnital and developmental
ICSiOllS
I%)
Miscellaneous lesions
(%) Total (%)
Edema
Bone erosion
Fourth ventricle Compressed Normal Enlarged
Cisternal deformity
Cerebra-ventricular index (CVI I)
35 (38.0) 26 (89.7) 11 (50.0) 4 (28.6) 76 (45.2)
38 (39.2) 2(6.9) - 4 (36.4) I (6.7) 45 (25.7)
70 (72.1) 23 (79.3) 12 (52.2) 3 (27.2) 9 (33.3) I17 (62.6) I8 (18.6) 6 (20.7) 7 (30.4) 4 (36.4) 3(1l.l) 38 (20.3) 9( 9.3) 4(17.4) 4 (36.4) I5 (55.6) 32(17.1)
66 (68.8) 23 (79.3) 10 (43.5) 5 (45.5) 8 (53.3) I I2 (64.4)
39.3 f 7.5 35.6 + 7.4 36.1 + 5.7 50.8 f 20.9 39.7 f 11.6 39.0 * 9.5
Contrast enhancement was noted in three quarters of the studied cases. Over three quarters (76.8%) of lesions with uniform enhancement were primary tumors of the PF. The main tumors presenting this pattern were AN and PF meningioma. A nonuniform pattern was found in both primary and metastatic tumors, in the later more frequently than the uniform. Ring enhancement was found in 23 patients, of whom 34.8% had metastases, 17.4% astrocytomas, and 13% AN. Lack of contrast enhancement was noted in congenital lesions, vascular lesions and primary tumors-mainly gliomas (Table 8).
(a)
(b)
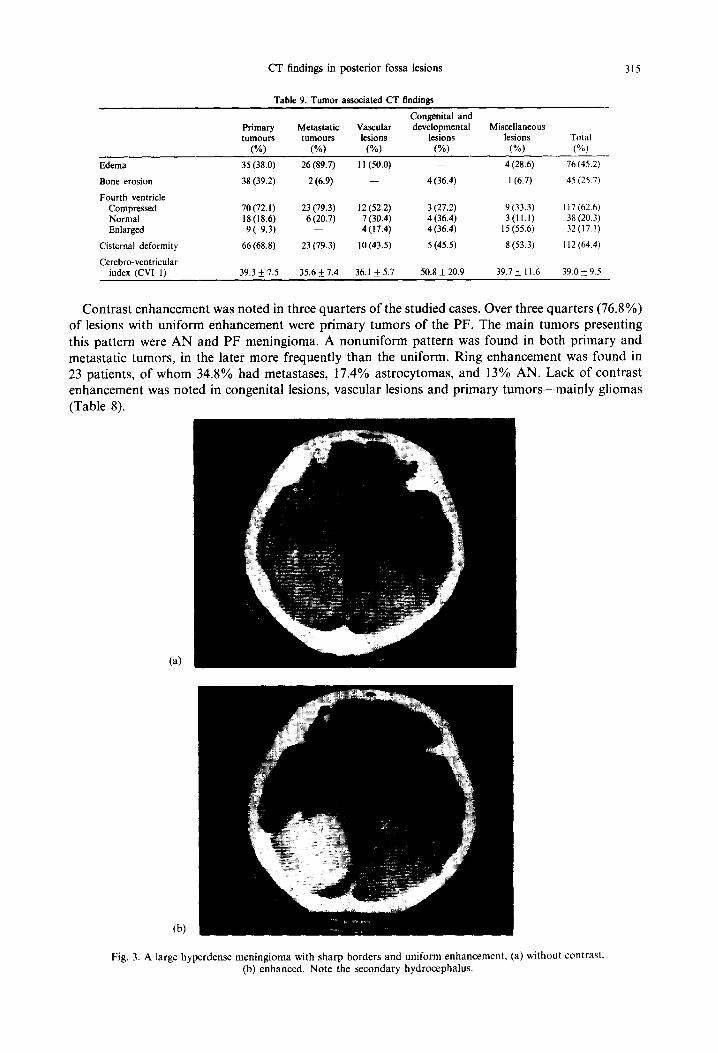
Fig. 3. A large hypcrdense meningioma with sharp borders and uniform enhancement, (a) without contrast. (b) enhanced. Note the secondary hydrocephalus.
316 IRITH REIDER-GROSWASSER et al.
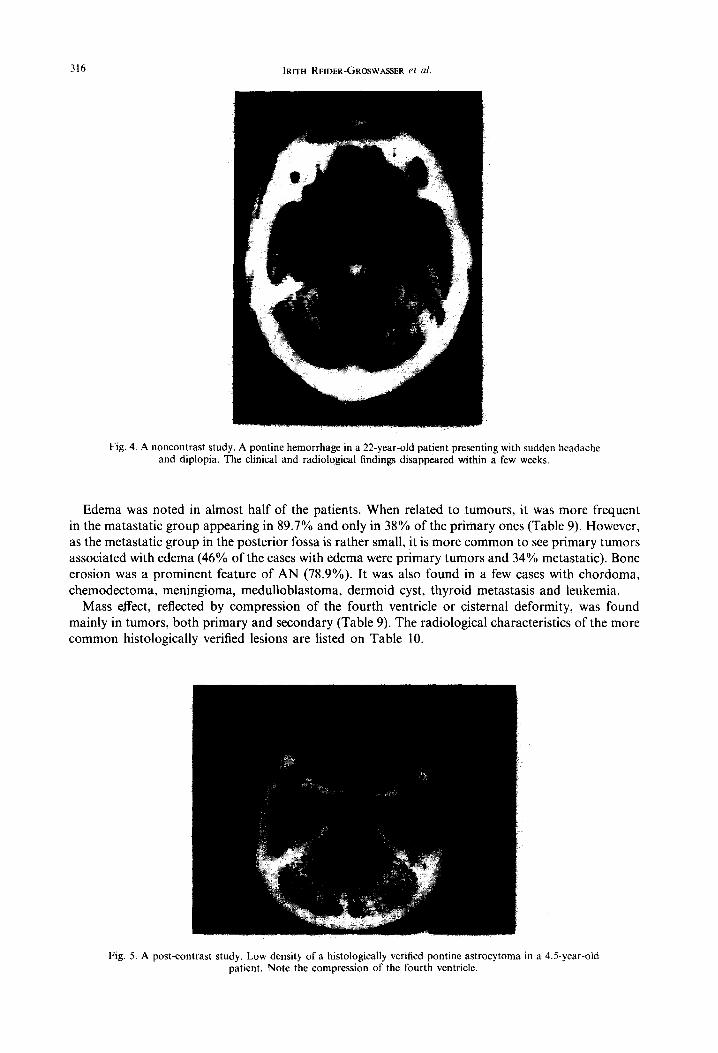
Fig. 4. A noncontrast study. A pontine hemorrhage in a 22-year-old patient presenting with sudden headache and diplopia. The clinical and radiological findings disappeared within a few weeks.
Edema was noted in almost half of the patients. When related to tumours, it was more frequent in the matastatic group appearing in 89.7% and only in 38% of the primary ones (Table 9). However, as the metastatic group in the posterior fossa is rather small, it is more common to see primary tumors associated with edema (46% of the cases with edema were primary tumors and 34% metastatic). Bone erosion was a prominent feature of AN (78.9%). It was also found in a few cases with chordoma, chemodectoma, meningioma, medulloblastoma, dermoid cyst, thyroid metastasis and leukemia.
Mass effect, reflected by compression of the fourth ventricle or cisternal deformity, was found mainly in tumors, both primary and secondary (Table 9). The radiological characteristics of the more common histologically verified lesions are listed on Table 10.
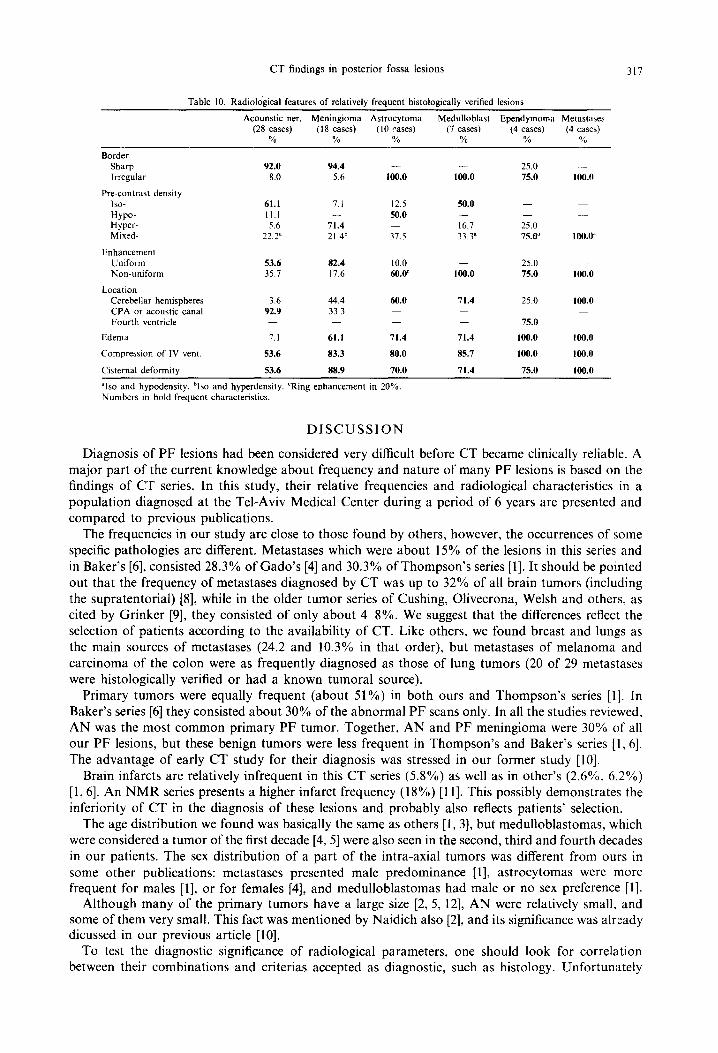
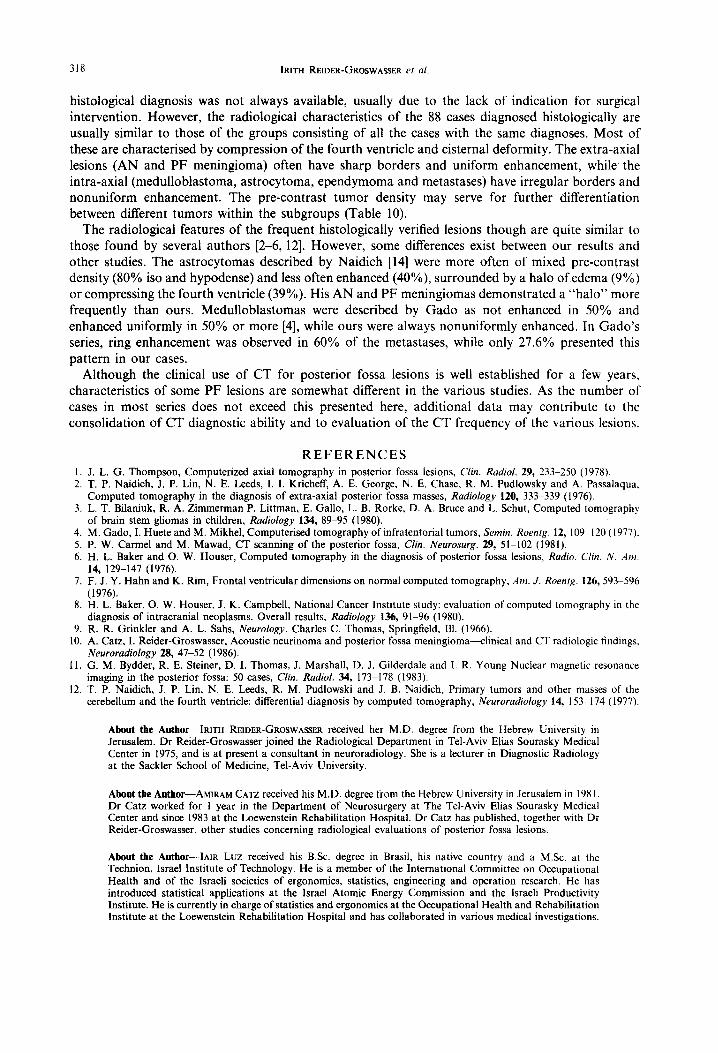
Fig. 5. A post-contrast study. Low density of a histologically verified pontine astrocytoma in a 4.5-year-old patient. Note the compression of the fourth ventricle.
CT findings in posterior fossa lesions 317
Table 10. Radiological features of relatively frequent histologically verified lesions
Acounstic ner. Meningioma Astrocytoma Medulloblast Ependymoma Metastases (28 cases) (I 8 cases) (IO cases) (7 cases) (4 cases) (4 cases)
% % % % % %
Border Sharp Irregular
Pre-contrast density ISO-
HYPO- Hyper- Mixed-
Enhancement Uniform Non-uniform
92.0 94.4 - - 25.0 - 8.0 5.6 100.0 100.0 75.0 100.0
61.1 7.1 12.5 50.0 - 11.1 50.0 - 5.6 71.4 16.7 25.0
22.2” 21.4h 37.5 33.3” 75.0” 100.0
53.6 82.4 10.0 25.0 35.7 17.6 6o.OC 100.0 75.0 100.0
Location Cerebellar hemispheres CPA or acoustic canal Fourth ventricle
3.6 44.4 60.0 71.4 25.0 100.0 92.9 33.3
75.0
Edema 7.1 61.1 71.4 71.4 100.0 100.0
Compression of IV vent. 53.6 83.3 80.0 85.7 100.0 100.0
Cisternal deformity 53.6 88.9 70.0 71.4 75.0 100.0
“Iso and hypodensity. bIso and hyperdensity. ‘Ring enhancement m 20% Numbers in bold-frequent characteristics.
DISCUSSION
Diagnosis of PF lesions had been considered very difficult before CT became clinically reliable. A major part of the current knowledge about frequency and nature of many PF lesions is based on the findings of CT series. In this study, their relative frequencies and radiological characteristics in a population diagnosed at the Tel-Aviv Medical Center during a period of 6 years are presented and compared to previous publications.
The frequencies in our study are close to those found by others, however, the occurrences of some specific pathologies are different. Metastases which were about 15% of the lesions in this series and in Baker’s [6], consisted 28.3% of Gado’s [4] and 30.3% of Thompson’s series [l]. It should be pointed out that the frequency of metastases diagnosed by CT was up to 32% of all brain tumors (including the supratentorial) [8], while in the older tumor series of Cushing, Olivecrona, Welsh and others, as cited by Grinker [9], they consisted of only about 448%. We suggest that the differences reflect the selection of patients according to the availability of CT. Like others, we found breast and lungs as the main sources of metastases (24.2 and 10.3% in that order), but metastases of melanoma and carcinoma of the colon were as frequently diagnosed as those of lung tumors (20 of 29 metastases were histologically verified or had a known tumoral source).
Primary tumors were equally frequent (about 51%) in both ours and Thompson’s series [l]. In Baker’s series [6] they consisted about 30% of the abnormal PF scans only. In all the studies reviewed, AN was the most common primary PF tumor. Together, AN and PF meningioma were 30% of all our PF lesions, but these benign tumors were less frequent in Thompson’s and Baker’s series [ 1, 61. The advantage of early CT study for their diagnosis was stressed in our former study [lo].
Brain infarcts are relatively infrequent in this CT series (5.8%) as well as in other’s (2.6%. 6.2%) [ 1,6]. An NMR series presents a higher infarct frequency (18%) [ 1 I]. This possibly demonstrates the inferiority of CT in the diagnosis of these lesions and probably also reflects patients’ selection.
The age distribution we found was basically the same as others [l, 31, but medulloblastomas, which were considered a tumor of the first decade [4, 51 were also seen in the second, third and fourth decades in our patients. The sex distribution of a part of the intra-axial tumors was different from ours in some other publications: metastases presented male predominance [ 11, astrocytomas were more frequent for males [l], or for females [4], and medulloblastomas had male or no sex preference [l].
Although many of the primary tumors have a large size [2, 5, 121, AN were relatively small, and some of them very small. This fact was mentioned by Naidich also [2], and its significance was alteady dicussed in our previous article [lo].
To test the diagnostic significance of radiological parameters, one should look for correlation between their combinations and criterias accepted as diagnostic, such as histology. Unfortunately
318 IRITH REIDER-GROSWASSER et al.
histological diagnosis was not always available, usually due to the lack of indication for surgical intervention. However, the radiological characteristics of the 88 cases diagnosed histologically are usually similar to those of the groups consisting of all the cases with the same diagnoses. Most of these are characterised by compression of the fourth ventricle and cisternal deformity. The extra-axial lesions (AN and PF meningioma) often have sharp borders and uniform enhancement, while the intra-axial (medulloblastoma, astrocytoma, ependymoma and metastases) have irregular borders and nonuniform enhancement. The pre-contrast tumor density may serve for further differentiation between different tumors within the subgroups (Table 10).
The radiological features of the frequent histologically verified lesions though are quite similar to those found by several authors [2-6, 121. However, some differences exist between our results and other studies. The astrocytomas described by Naidich [14] were more often of mixed pre-contrast density (80% iso and hypodense) and less often enhanced (40%) surrounded by a halo of edema (9”/0) or compressing the fourth ventricle (39%). His AN and PF meningiomas demonstrated a “halo” more frequently than ours. Medulloblastomas were described by Gado as not enhanced in 50% and enhanced uniformly in 50% or more [4], while ours were always nonuniformly enhanced. In Gado’s series, ring enhancement was observed in 60% of the metastases, while only 27.6% presented this pattern in our cases.
Although the clinical use of CT for posterior fossa lesions is well established for a few years, characteristics of some PF lesions are somewhat different in the various studies. As the number of cases in most series does not exceed this presented here, additional data may contribute to the consolidation of CT diagnostic ability and to evaluation of the CT frequency of the various lesions.
REFERENCES 1. J. L. G. Thompson, Computerized axial tomography in posterior fossa lesions, Clin. Radiol. 29, 233-250 (197X). 2. T. P. Naidich, J. P. Lin, N. E. Leeds, I. I. Kricheff, A. E. George, N. E. Chase, R. M. Pudlowsky and A. Passalaqua,
Computed tomography in the diagnosis of extra-axial posterior fossa masses, Rudio/ogy 120, 333-339 (1976). 3. L. T. Bilaniuk, R. A. Zimmerman P. Littman, E. Gallo, L. B. Rorke, D. A. Bruce and L. Schut, Computed tomography
of brain stem gliomas in children, Radiology 134, 89-95 (1980). 4. M. Gado, I. Huete and M. Mikhel, Computerised tomography of infratentorial tumors, Semin. Roenrg. 12, 1099120 (1977). 5. P. W. Carmel and M. Mawad, CT scanning of the posterior fossa, Clin. Neurosurg. 29, 51-102 (1981). 6. H. L. Baker and 0. W. Houser, Computed tomography in the diagnosis of posterior fossa lesions, Radio. C/in. N. .4m.
14, 129-147 (1976). 7. F. J. Y. Hahn and K. Rim, Frontal ventricular dimensions on normal computed tomography, Am. J. Roenlg. 126,593-596
(1976). 8. H. L. Baker, 0. W. Houser, J. K. Campbell, National Cancer Institute study: evaluation of computed tomography in the
diagnosis of intracranial neoplasms. Overall results, Radiology 136, 91-96 (1980). 9. R. R. Grinkler and A. L. Sahs, Neurology. Charles C. Thomas, Springfield, 111. (1966).
10. A. Catz, I. Reider-Groswasser, Acoustic neurinoma and posterior fossa meningioma-linical and CT radiologic findings. Neuroradiology 28, 47-52 (1986).
11. G. M. Bydder, R. E. Steiner, D. I. Thomas, J. Marshall, D. J. Gilderdale and I. R. Young Nuclear magnetic resonance imaging in the posterior fossa: 50 cases, Clin. Radiol. 34, 173-178 (1983).
12. T. P. Naidich, J. P. Lin, N. E. Leeds, R. M. Pudlowski and J. B. Naidich, Primary tumors and other masses of the cerebellum and the fourth ventricle: differential diagnosis by computed tomography, Neuroradiology 14, 153-I 74 (1977).
About the Author-IRITH REIDER-GROSWASER received her M.D. degree from the Hebrew University in Jerusalem. Dr Reider-Groswasser joined the Radiological Department in Tel-Aviv Elias Sourasky Medical Center in 1975, and is at present a consultant in neuroradiology. She is a lecturer in Diagnostic Radiology at the Sackler School of Medicine, Tel-Aviv University.
About the Author-AMIRAM CATZ received his M.D. degree from the Hebrew University in Jerusalem in 198 I. Dr Catz worked for 1 year in the Department of Neurosurgery at The Tel-Aviv Elias Sourasky Medical Center and since 1983 at the Loewenstein Rehabilitation Hospital. Dr Catz has published, together with Dr Reider-Groswasser. other studies concerning radiological evaluations of posterior fossa lesions.
About the Author-IAIR Luz received his BSc. degree in Bras& his native country and a M.Sc. at the Technion, Israel Institute of Technology. He is a member of the International Committee on Occupational Health and of the Israeli societies of ergonomics, statistics, engineering and operation research. He has introduced statistical applications at the Israel Atomic Energy Commission and the Israeli Productivity Institute. He is currently in charge of statistics and ergonomics at the Occupational Health and Rehabilitation Institute at the Loewenstein Rehabilitation Hospital and has collaborated in various medical investigations.