Embed Size (px)
Citation preview

Computerized Cognitive Rehabilitation in ICU Survivors: RETURN-CCR Pilot Investigation
Jo Ellen Wilson MD MPH1, Erin M. Collar MPH
2, Amy L. Kiehl MA
2, Hyunkyu Lee PhD
3, Michael
Merzenich PhD3, E. Wesley Ely MD MPH
4,5 and James Jackson PsyD
2 for the Returning to
Everyday Tasks Using Rehabilitation Networks - Computerized Cognitive Rehabilitation
(RETURN-CCR) Investigators
1Department of Psychiatry and Behavioral Sciences, Vanderbilt University School of Medicine,
Nashville, TN
2Department of Medicine, Vanderbilt University School of Medicine, Nashville, TN
3Posit Science, San Francisco, CA
4Veteran’s Affairs TN Valley, Geriatrics Research, Education and Clinical Center (GRECC)
5Department of Medicine, Division of Pulmonary and Critical Care, and the Center for Health
Services Research, Vanderbilt University Medical Center, Nashville, TN
Corresponding Author:
Jo Ellen Wilson, MD MPH
The Vanderbilt Psychiatric Hospital
1601 23rd
Avenue South
Nashville, TN 37212
Phone: (615)-719-0464
Fax: (615)-322-4856
Email: [email protected]
Web: www.icudelirium.org
Author Contributions: All authors listed above have contributed substantially to the conception
or design of the work; or the acquisition, analysis, or interpretation of data for the work and
have participated in drafting the work or revising it critically for important intellectual content.
Additionally, each author has given their approval to the final version of the manuscript and has
agreed to be accountable for all aspects of the work in ensuring that questions related to the
accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflicts of Interest and Source of Funding: Dr. Wilson would like to acknowledge salary
support from the Vanderbilt Faculty Research Scholars Program (KL2). Drs. Ely and Jackson as
well as Mrs. Collar and Kiehl all receive funding for their time working on this investigation from
AG035117 and HL111111. Dr. Ely would additionally like to acknowledge salary support from
the Tennessee Valley Healthcare System Geriatric Research Education and Clinical Center
(GRECC). Dr. Ely will also disclose additional funding for his time from AG027472 and having
received honoraria from Orion and Hospira for CME activity; he does not hold stock or
consultant relationships with those companies. None of the Vanderbilt investigators received
any consulting fees, stocks, or other financial support from Posit Science, the company that
provided Brain-HQ, the computer program used in this investigation. Dr. Lee would like to
disclose salary support from the Posit Science and that she is a research scientist and employee
of Posit Science. Dr. Merzenich would like to disclose being a developer of the technology used
Page 1 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

in the computerized rehabilitation Brain HQ used in this investigation and that he is a founder
and employee of Posit Science.
Running Head: Computerized Cognitive Rehabilitation in ICU Survivors
Subject Category: 4.4 Clinical Trials in Critical Care Medicine
MeSH Key Words: cognitive neuroscience, training, delirium, cognitive impairment
Word Count: 1710
Page 2 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

Utilization and cost of critical care medicine have risen steadily since 2000 (1, 2). Nearly one-
third of patients who survive their critical illness will suffer from newly acquired or accelerated
post-ICU cognitive impairment (3). One-third to one-half of all survivors of critical illness are
newly unemployed at 12 months, likely attributable to newfound cognitive deficits (4-6). This
public health problem is growing, poorly addressed, and requires innovation to reduce suffering
and help patients return to normal functioning. By monitoring delirium (7, 8), we have shown
that delirium duration (3, 9) is associated with white matter disruption after a critical illness
(10). While therapeutic approaches are emerging in the context of critical care delivery to
reduce delirium and enhance patient safety by reducing the duration of delirium and coma (11),
few therapeutic approaches have been tested in this population to regain acquired cognitive
deficits. What remains unknown is whether we can help patients recover cognitive abilities
once lost.
A need exists to develop cognitive rehabilitation approaches for patients with critical
illnesses who despite our best care go on to acquire post-ICU cognitive impairment even
without prior stroke or head injury. While cognitive rehabilitation has historically been
employed with predominantly brain-injured populations (TBI, stroke), it has only recently been
trialed in primary medical populations such as individuals with “chemo-fog”, HIV-associated
neurologic dysfunction and only minimally among those with post-intensive care syndrome
(12). Computerized Cognitive Rehabilitation (CCR) is a novel approach of traditional cognitive
rehab through the use of computerized “brain exercises”. A recent systematic review of 16
computerized cognitive training trials found moderate effect sizes in improvement of attention,
executive function and memory, in individuals with cognitive impairment, which persisted at
Page 3 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

follow-up (13). Despite early promising results, many in the scientific community have
questioned whether computerized cognitive exercises have any real impact (14, 15). To the
contrary, others suggest that CCR holds the promise of accelerating recovery by harnessing
neuroplasticity (16-18). We hypothesized that application of CCR would improve key cognitive
abilities in ICU survivors even years after the original brain injury.
Methods
The Returning to Everyday Tasks Using Rehabilitation Networks – Computerized Cognitive
Rehabilitation (RETURN-CCR) pilot investigation was designed by Posit Science, to test feasibility
and proof of principle of specially designed computer exercises in addressing cognitive
impairment in ICU survivors (19). IRB-approval was obtained, and patients from the BRAIN-ICU
observational cohort study (3) as well as our group’s ongoing studies were enrolled after we
obtained their informed consent. These patients had survived ICU treatment with mechanical
ventilation or vasopressors in the context of severe critical illness and had since shown
persistent long-term cognitive impairment. A convenience sample (N=33) of patients was
recruited to participate in RETURN-CCR. In general, if patients had completed their
participation in one of the above studies and were alive and felt to be able to participate in this
trial (i.e., had previously followed up with former study assessments) they were approached for
participation in RETURN-CCR.
Patients received the CCR program, which was comprised of adaptive exercises focused
on optimizing speed and memory accuracy and auditory verbal processing (16, 17). Patients
completed 7 cognitive exercises daily (~42 minutes), 5 days a week, over the 12-week trial
Page 4 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

period, with core therapeutic tasks built into a game-like experience. Use of the program was
tracked from Posit Science BrainHQ’s experimental portal, where the experimenter can easily
track progress of each participant, number of training days, and overall performance.
During a session, patients performed trials, with auditory and visual feedback and
rewards to indicate if the trial was performed correctly or incorrectly. After each session, the
difficulty of the next session was titrated to ensure appropriate difficulty based on immediate
preceding performance. That is, patients excelling experienced progressively more challenging
tasks whereas patients performing poorly engaged in tasks that were easier.
The brain-training program included 18 computerized training exercises. Core training
targets include visual and auditory processing accuracy, speed, and sequencing; phasic,
sustained, and divided attention; memory and memory association; and executive control
abilities. For each session, participants were given 7 computer exercises and each game lasted
about 6 minutes. During the 6-minute time window, participants played a certain level of game
multiple times (usually between 2-4 times, varying based on participants’ response speed and
number of trials). Baseline was set by the performance of very first attempt. On repetition, the
initial difficulty was set by the previous trial’s best performance to promote performance
improvement. As each session progresses, improvements in processing speed and/or
performance accuracy and in their controlled, higher-order performance operations are
challenged at progressively more cognitively demanding task levels, to maintain ~75-85%
accuracy. By this adaptive training strategy, virtually all trainees, regardless of learning rate,
were continuously challenged at an appropriate difficulty level as their abilities improved.
We compared the baseline (Pre-CCR) scores versus post-CCR scores to assess
Page 5 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

improvement in performance. Each computerized cognitive exercise has multiple levels,
presented to participants in fixed order (i.e., from easy to more complex levels). Participants set
the baseline or “pre” cognitive training score from their individual performance on the initial
trial and their “post” score representing their individual best performance within the trial
period. Pre and post-scores for each exercise were calculated by averaging the normed pre and
post-scores of all levels. Normed pre and post scores from each exercise were averaged to
produce a composite score for each cognitive domain. Mixed-effects linear regression was
performed for each cognitive domain separately with time (pre and post performance) as a
factor. Mixed linear regression models were used to assess the effect of user group (super,
high, normal) on improvement (pre- and post-) of untrained neuropsychological tests (including
Digit Span, Spatial Span and Trail Making A and B). To assess for group effect we then used a
one-way ANOVA with group as a factor to assess for differences between groups. All statistical
analyses were run in Python (version 3.5.3).
Results
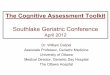
Between April 2015 and April 2016, 113 former study participants were approached for
participation in RETURN-CCR (Figure 1). Thirty-three patients were initially enrolled, however of
these, three participants were excluded at enrollment as they declined to participate in the full
program (Figure 1). Ultimately, 24 of the 30 (80%), who engaged in the program, completed
both a baseline and post-training assessment at 12 weeks after initiation of the trial.
Page 6 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

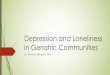
At the time of their original critical illness, patients who remained in the pilot at the 12
week mark, had a median (IQR) age of 60 (52-70), 96% Caucasian, 52% male, with 16 years (12-
16) of education, were not cognitively impaired, spent a median (IQR) of 15 days (7-21) in the
hospital and 6 days (3-15) in the ICU (Table 1). Amongst those who completed the 12 week
assessment, 75% had experienced at least one day of delirium and 58% experienced at least 1
day of coma and all but one patient required mechanical ventilation for at least 1 day during
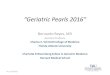
their original critical illness. Patients (N=24) completed a median of 517.5 levels of
rehabilitation (IQR 240, 862) (each daily rehabilitation session was comprised of a number of
“levels”) and showed a significant (p<0.01) improvement comparing baseline Pre-CCR vs. Post-
CCR composite z-score performances in 4 key domains of cognitive functioning: attention,
processing speed, memory and executive function (Figure 2a).
Next, the improvement of untrained cognitive exercises (i.e., a carryover effect of
training) was measured by comparing baseline (prior to use of computerized cognitive
exercises) and post-training cognitive assessment measures (such as the: Digit Span, Spatial
Span and Trail Making A and B). At protocol completion, ICU-survivors demonstrated
improvement on some of the measures of cognitive abilities (Digit Span: t = -1.91; p =.06;
Spatial Span: t = -1.39; p >.05; Trail Making A: t = - 2.26; p < .05; Trail Making B: t = -0.78; p >.05;
Trails B-A (cost): t = 0.62; p>.05).
In a linear regression model, the amount of improvement was positively correlated with
the number of training hours, suggesting that benefits from training will transfer to general
untrained cognitive abilities (F(1,22) = 3.0, p = .097, see Figure 2b). Super users (or those who
played at least 1000 levels) had a significantly higher mean z-score on untrained
Page 7 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

neuropsychological tasks than normal users (less than 500 levels) after participating in the 12-
week trial (p-value = 0.046). When we analyzed the improvement in the untrained
neuropsychological tests by user group (super, high, normal) in a one-way ANOVA model, with
group as a factor, the group effect was significant at p = 0.03. This effect was mainly driven by
the difference between the super and normal groups. In an ANOVA with group (super and
normal) as a factor, the group difference was significant (p=0.005). There was no significant
difference between "super and high" (high users = <1000 and >500 levels played) and "high and
normal" user groups.
Discussion
In this limited proof of concept pilot study we showed that survivors of critical illness with
cognitive impairment had significant improvement in important neuropsychological domains
and that improvement in untrained cognitive abilities was positively correlated with the
amount of levels played. This investigation is the first to our knowledge to evaluate feasibility of
a computer gaming approach of cognitive rehabilitation in survivors of non-neuro/non-trauma
critical illness. Such an approach is appealing as it is more scalable than traditional cognitive
rehabilitation interventions that require intensive face-to-face interaction between patients
and clinical professionals.
Although we did not reach statistical significance on the individual untrained
neuropsychological assessments before and after the 12 week trial, we were underpowered to
do so. In order to answer questions of efficacy, a randomized clinical trial would be required.
We did however find a statistically significant effect of user group (super, high and normal) on
Page 8 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

untrained neuropsychological assessments, suggesting that the most “robust” improvement in
higher order cognitive tasks occurs in the super user group.
These pilot data were designed to help generate hypotheses to shape appropriately
designed randomized trials. Future work should consider a time point more proximal to ICU
stay for maximal impact and clinical outcomes data inclusive of “real world” evaluations such as
handling money, driving simulators, work place capacity, and social interactions (14).
Additionally, future work should explore the impact of CCR on other important outcomes from
critical illness, including depression, PTSD, frailty, life space and quality of life.
Page 9 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

References
1. Halpern NA, Pastores SM. Critical care medicine beds, use, occupancy, and costs in the
united states: A methodological review. Crit Care Med 2015;43(11):2452-2459.
2. Halpern NA, Goldman DA, Tan KS, Pastores SM. Trends in critical care beds and use among
population groups and medicare and medicaid beneficiaries in the united states: 2000-
2010. Crit Care Med 2016;44(8):1490-1499.
3. Pandharipande PP, Girard TD, Jackson JC et al. Long-term cognitive impairment after critical
illness. N Engl J Med 2013;369(14):1306-1316.
4. Norman BC, Jackson JC, Graves JA et al. Employment outcomes after critical illness: An
analysis of the bringing to light the risk factors and incidence of neuropsychological
dysfunction in icu survivors cohort. Crit Care Med 2016;44(11):2003-2009.
5. Kamdar BB, Huang M, Dinglas VD et al. Joblessness and lost earnings after acute respiratory
distress syndrome in a 1-year national multicenter study. Am J Respir Crit Care Med
2017;196(8):1012-1020.
6. Kamdar BB, Sepulveda KA, Chong A et al. Return to work and lost earnings after acute
respiratory distress syndrome: A 5-year prospective, longitudinal study of long-term
survivors. Thorax 2018;73(2):125-133.
7. Ely EW, Inouye SK, Bernard GR et al. Delirium in mechanically ventilated patients: Validity
and reliability of the confusion assessment method for the intensive care unit (cam-icu).
JAMA 2001;286(21):2703-2710.
8. Ely EW, Truman B, Shintani A et al. Monitoring sedation status over time in icu patients:
Reliability and validity of the richmond agitation-sedation scale (rass). JAMA
2003;289(22):2983-2991.
9. Girard TD, Jackson JC, Pandharipande PP et al. Delirium as a predictor of long-term cognitive
impairment in survivors of critical illness. Crit Care Med 2010;38(7):1513-1520.
10. Morandi A, Rogers BP, Gunther ML et al. The relationship between delirium duration, white
matter integrity, and cognitive impairment in intensive care unit survivors as determined by
diffusion tensor imaging: The visions prospective cohort magnetic resonance imaging study.
Crit Care Med 2012;40(7):2182-2189.
11. Pandharipande PP, Pun BT, Herr DL et al. Effect of sedation with dexmedetomidine vs
lorazepam on acute brain dysfunction in mechanically ventilated patients: The mends
randomized controlled trial. JAMA 2007;298(22):2644-2653.
12. Needham DM, Davidson J, Cohen H et al. Improving long-term outcomes after discharge
from intensive care unit: Report from a stakeholders' conference. Crit Care Med
2012;40(2):502-509.
Page 10 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

13. Coyle H, Traynor V, Solowij N. Computerized and virtual reality cognitive training for
individuals at high risk of cognitive decline: Systematic review of the literature. Am J Geriatr
Psychiatry 2015;23(4):335-359.
14. Simons DJ, Boot WR, Charness N et al. Do “brain-training” programs work? Psychological
Science in the Public Interest 2016;17(3):103-186.
15. 2014 A consensus on the brain training industry from the scientific community. Available at
http://longevity.stanford.edu/a-consensus-on-the-brain-training-industry-from-the-
scientific-community-2/. Last Accessed: 9/22/2017.
16. Ball K, Berch DB, Helmers KF et al. Effects of cognitive training interventions with older
adults: A randomized controlled trial. JAMA 2002;288(18):2271-2281.
17. Rosen AC, Sugiura L, Kramer JH, Whitfield-Gabrieli S, Gabrieli JD. Cognitive training changes
hippocampal function in mild cognitive impairment: A pilot study. J Alzheimers Dis 2011;26
Suppl 3:349-357.
18. 2014 Cognitive training data response letter. Available at
https://www.cognitivetrainingdata.org/the-controversy-does-brain-training-
work/response-letter/. Last Accessed: 9/22/2017.
19. Jackson JC, Ely EW, Morey MC et al. Cognitive and physical rehabilitation of intensive care
unit survivors: Results of the return randomized controlled pilot investigation. Crit Care Med
2012;40(4):1088-1097.
Page 11 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

Figure 1. Flow diagram of patients through RETURN-CCR from recruitment through the 12-
week pilot trial
Page 12 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

Figure 2. 2a.) Cognitive Performance Over Time (Pre vs. Post Computerized Cognitive Rehabilitation (CCR) by Neuropsychological Domain: Change from baseline “Pre-CCR” performance (displayed as a composite z-score) to “Post-CCR” score for each cognitive domain after the 3-month trial period (N=24). Error bars indicate standard error. For all 4 cognitive domains, a statistically significant improvement (p<0.01) in performance was demonstrated as compared to baseline performance. F2b.) Improvement of cognitive assessment by user group (Super >1000 levels played, High <1000 and >500 levels played, and Normal <500 levels played. Error bars and bands are standard errors.
2a.)
2b.)
Page 13 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

Table 1. Demographic and Baseline Characteristics
a Median values (interquartile range).
b The Short Informant Questionnaire on Cognitive Decline in the Elderly ranges from 1 to 5, with
a score of 3 indicating no change in cognition over the past 10 yr, a score < 3 indicating
improvement, and a score > 3 indicating decline in cognition, as compared with 10 yr before. A
score of ≥ 3.6 indicates preexisting cognitive impairment. c Sepsis or Septic shock diagnosis includes individuals with Acute Respiratory Distress Syndrome
(ARDS) with Infection d Scores on the Sequential Organ Failure Assessment (SOFA) range from 0 to 24 (from 0 to 4 for
Variable
median (IQR)a
Entire RETURN-
CCR Cohort
(N=30)
Participation
Cohort (N=24)
Age at Enrollment 60 (50 – 67) 60 (52 – 70)
Gender (%)
Male
Female
53
47
50
50
Race (%)
Caucasian / White
African American / Black
97
3
96
4
Years of Education at Enrollment 15 (12 – 16) 16 (12-16)
IQCODE at Enrollmentb 3 (3 - 3.063) 3 (3 - 3.063)
Days in the Hospital 17 (8 – 21) 15 (7 -21)
Days in the ICU 6 (3 – 13) 6 (3 -15)
Admission Diagnosis (%)
Sepsis or Septic Shockc
Hepatobiliary / Pancreatic surgery
Airway Protection / Upper Airway Obstruction
Acute Myocardial Infarction
Gastric Surgery
Acute Lung Injury / ARDS without infection
CHF / Cardiogenic Shock
Orthopedic Surgery
Vascular Surgery
GI Bleed
40
13
13
10
7
3
3
3
3
3
42
13
17
13
4
4
4
4
0
0
Mean SOFA score at Enrollmentd 8 (6 – 10) 9 (6 – 10)
Mean Charlson score at Enrollmente 2 (0 – 3) 2 (0 - 3)
Percent with at least 1 day of Delirium in the ICU (%) 73 75
Percent with at least 1 day of Coma in the ICU (%) 53 58
Days spent in the ICU 6 (3 – 13) 6 (3 – 15)
Days spent in the Hospital 17 (8 – 21) 15 (7 – 21)
Ventilator Support (%)
Mechanical Ventilation (at least 1 day)
Non-Invasive Positive Pressure Ventilation
97
3
96
4
Page 14 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society

each of six organ systems), with higher scores indicating more severe organ dysfunction. We
used a modified SOFA score, which excluded the Glasgow Coma Scale components, since coma
was included separately in our models. e Scores on the Charlson comorbidity index range from 0 to 33, with higher scores indicating a
greater burden of illness.
Page 15 of 15 ANNALSATS Articles in Press. Published on 18-June-2018 as 10.1513/AnnalsATS.201709-744RL
Copyright © 2018 by the American Thoracic Society