Embed Size (px)
Citation preview

HAL Id: hal-00173388https://hal.archives-ouvertes.fr/hal-00173388
Submitted on 19 Sep 2007
HAL is a multi-disciplinary open accessarchive for the deposit and dissemination of sci-entific research documents, whether they are pub-lished or not. The documents may come fromteaching and research institutions in France orabroad, or from public or private research centers.
L’archive ouverte pluridisciplinaire HAL, estdestinée au dépôt et à la diffusion de documentsscientifiques de niveau recherche, publiés ou non,émanant des établissements d’enseignement et derecherche français ou étrangers, des laboratoirespublics ou privés.
Computer aided planning and navigation fororbito-zygomatic reconstruction.
Christophe Marecaux, Matthieu Chabanas, Yohan Payan, Franck Boutault
To cite this version:Christophe Marecaux, Matthieu Chabanas, Yohan Payan, Franck Boutault. Computer aided plan-ning and navigation for orbito-zygomatic reconstruction.. Surgetica’2007: Computer-Aided MedicalInterventions: tools and applications., 2007, France. pp.271-281. �hal-00173388�
3D Navigation Systems (3DNS) wereintroduced in the late 80s in neurosur-gery and no later described in maxillo-facial surgery. Concomitant develop-ment of computed imaging techniquesoffered exciting horizons for surgicalplanning and simulation and principlesof Computer Aided Surgery (CAS) couldbe formulated for a consistent use inCranio-maxillofacial surgery. To date ithas been widely developed and increa-sing fields of indications were reported.However, no 3DNS specifically designedfor maxillofacial surgery or one patholo-gy dedicated planning software plat-form are yet commercially available.
We suggest a full protocol of CAS aspreviously recommended in literatureaddressing the challenging task of pri-mary or secondary reconstruction ofOZMC dislocation. First, on a specifi-cally developed planning software, thebest zygoma reduction and orbitalboundaries reconstruction to achieveskeletal symmetry are determined. Thistreatment plan is then transferred to
the 3DNS within the operating room.After patient’s anatomy registration tohis preoperative CT scan data, the navi-gation system allows zygomatic gui-ding to its planned reduced locationand bone orbital volume restorationcontrol. The feasibility of this tech-nique was checked in 3 patients withmajor OZMC deformities. Preliminaryclinical results are presented.
MATERIALS ANDMETHODS
Preoperative planning
Planning method for primary or secon-dary surgical treatment of OZMC waspreviously widely described [2]. Mainsteps are reminded.
3D models generation
The planning workstation providesfrom a regular CT scan dataset axial
1
COMPUTER AIDED PLANNING AND NAVIGATION FOR ORBITO-ZYGOMATIC RECONSTRUCTION
CH. MARECAUX*,**, M. CHABANAS*, Y. PAYAN*, F. BOUTAULT***
* TIMC/GMCAO Laboratory, In3S - Université Joseph Fourier, Faculté de Médecine - 38706 La Tronche cedex.** Clinic Cours Dillon – 1, rue Peyrolade - 31300 Toulouse.
*** Department of maxillofacial and facial plastic surgery, Hopital Purpan, TSA 40031 - 31059 Toulouse cedex 9.
11.3 Marecaux 9/07/07 14:35 Page 1
and reconstructed coronal and sagittalviews, as well as 3D reconstructed sur-face soft-tissue and skeletal.Practitioner can interactively browsethrough the different series, manipula-te the 3D models or select anatomicalpoints or Regions Of Interest (ROI).
Target determination
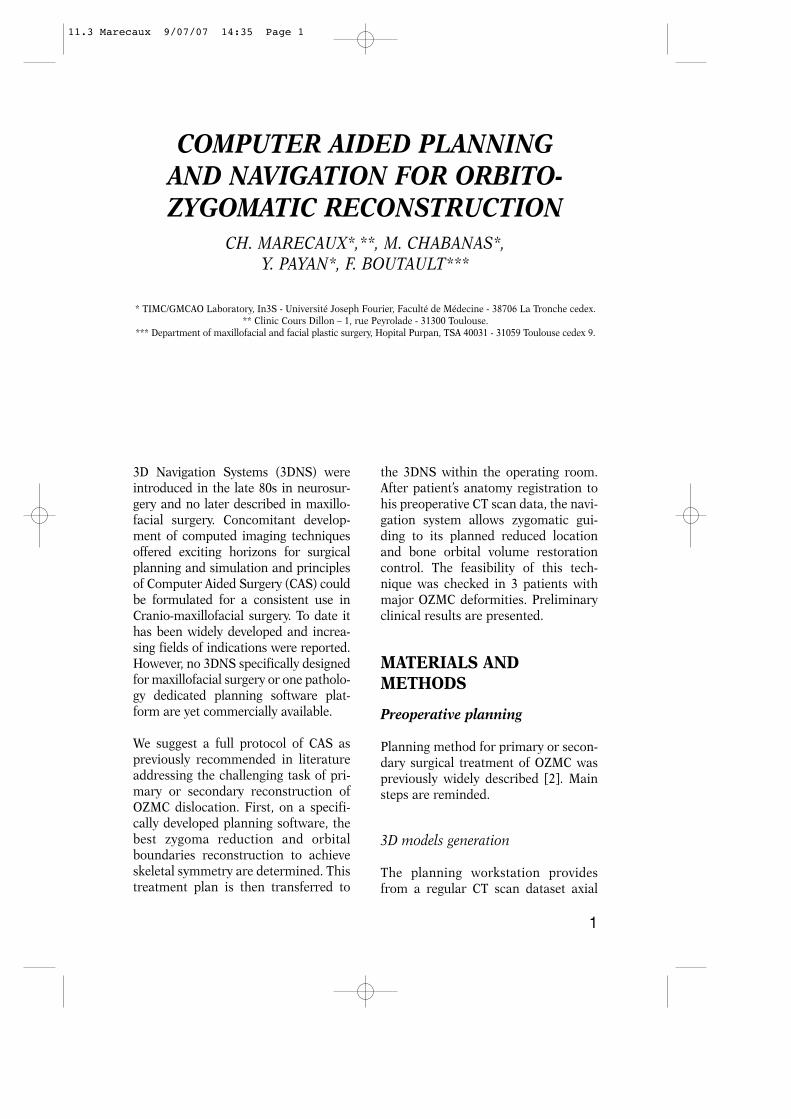
Whereas the target location for thefractured bone segment is defined sym-metrically to the healthy side, a theore-tical symmetric skull is computedaround a midsagittal plane (fig. 1). Thisplane is defined by 3 included andmanually selected anatomical land-marks.
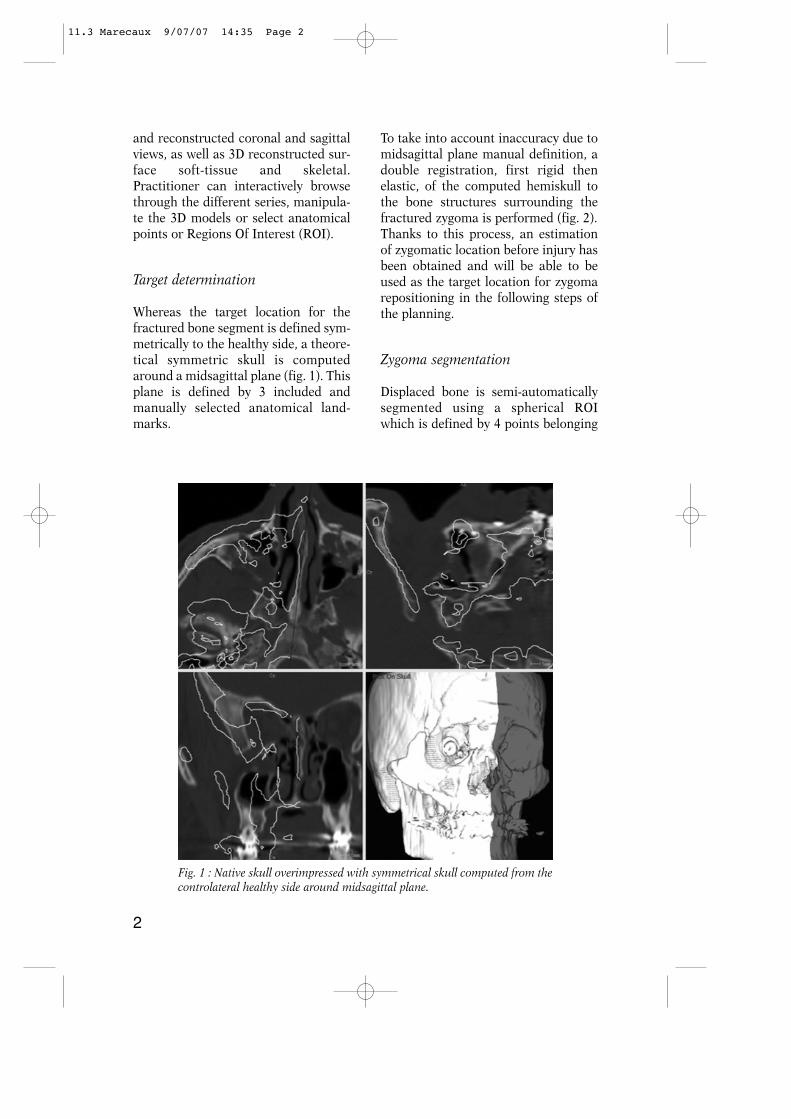
To take into account inaccuracy due tomidsagittal plane manual definition, adouble registration, first rigid thenelastic, of the computed hemiskull tothe bone structures surrounding thefractured zygoma is performed (fig. 2).Thanks to this process, an estimationof zygomatic location before injury hasbeen obtained and will be able to beused as the target location for zygomarepositioning in the following steps ofthe planning.
Zygoma segmentation
Displaced bone is semi-automaticallysegmented using a spherical ROIwhich is defined by 4 points belonging
2
Fig. 1 : Native skull overimpressed with symmetrical skull computed from thecontrolateral healthy side around midsagittal plane.
11.3 Marecaux 9/07/07 14:35 Page 2
to its limit and rather corresponding tothe fractured buttresses. This sphereincludes the body of zygomatic bonewhich is the most significant skeletalpart for facial symmetry restoration.
Surgical planning for zygomareduction
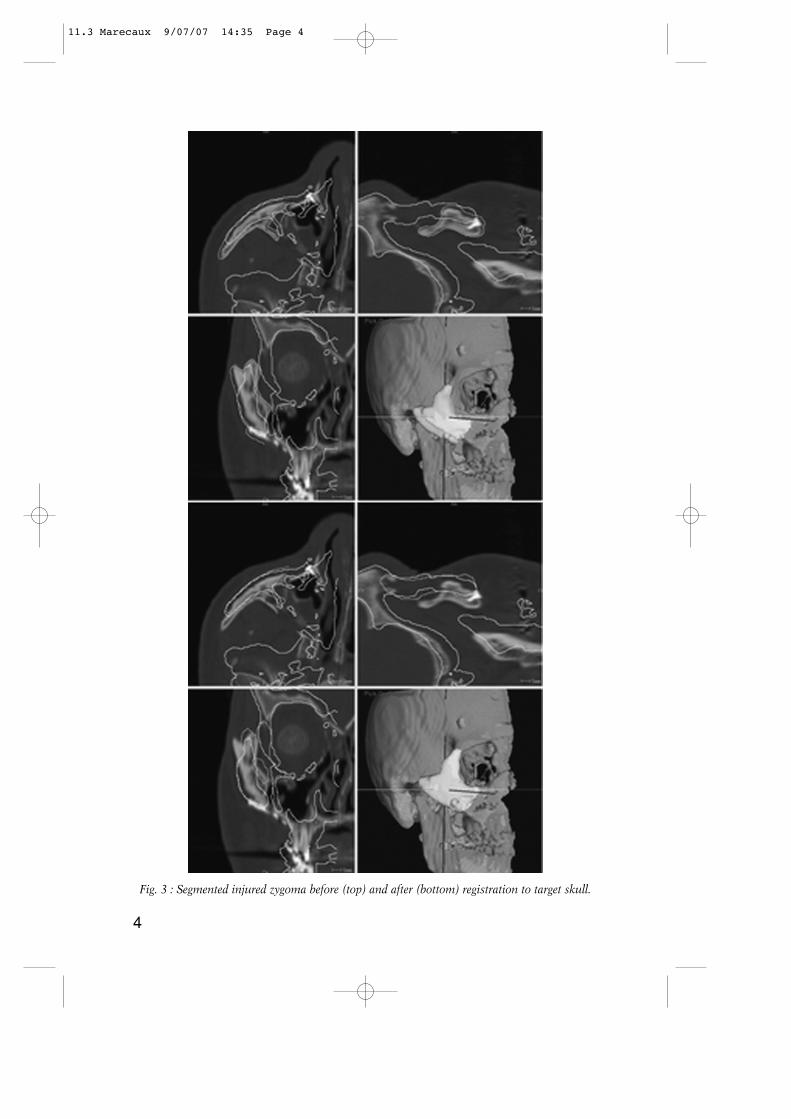
Finally, an automatic rigid registrationof the previously segmented fracturedbone to the target skull computed instep 2 is performed to determine thebest zygomatic bone repositioning toachieve skeletal symmetry (fig. 3).Since matching provides all the better
result that initial position of both sur-faces is close, a prior point-to-pointregistration can be required in case oflarge displacement.
Non-injured orbit segmentation
The same as for zygomatic reconstruc-tion planning, orbital boundaries resto-ration is planned symmetrically fromthe healthy side. Orbital volume issemi-automatically segmented with acone-shaped growing ROI defined byits main axis corresponding to theneuro-optic axis and a closing anteriorplane (fig. 4).
3
Fig. 2 : Result from the double registration of symmetrical skull to native skullaccording to selected surrounding ROI (spheres).
11.3 Marecaux 9/07/07 14:35 Page 3
4
Fig. 3 : Segmented injured zygoma before (top) and after (bottom) registration to target skull.
11.3 Marecaux 9/07/07 14:35 Page 4

Surgical planning for orbital boun-daries reconstruction
A virtual orbit is then computed fromthe previously segmented orbit symme-trically around the midsagittal plane.Its boundaries are superimposed onthe different axial, coronal and sagittalseries and will be used as a guiding foraccurate orbital walls reconstruction(fig. 5).
Intraoperative navigation andguiding
The Surgetics™ navigation system andthe Craniologics™ software (Praxim-Medivision, La Tronche, France) were
fitted and used for intraoperative navi-gation. This navigation system uses apassive and infrared light based opticaltechnology. Novelty of theCraniologics™ software is a doublepoint-surface registration of patient’sanatomy to preoperatively acquired CTscan data set, first cutaneous, secondskeletal after surgical exposure toimprove navigation accuracy aroundthe ROI. Then, location of calibratedsurgical instruments in relation to itsactual location in the surgical field canbe presented in the different series or3D models and in real time updated.
Software adaptation consists of anadditional zygomatic navigation step.First, a Rigid Body is rigidly fixated to
5
Fig. 4 : Segmentation of the healthy orbit with a cone-shaped growing ROIdefined by the neuro-optic axis and an average closing anterior plane.
11.3 Marecaux 9/07/07 14:35 Page 5

zygomatic body by a 2 pins transcuta-neous fixation (Digital ZygomaticFrame, DZF) (fig. 6). Next, a point-to-surface registration between zygomaand its model transferred with theplanning data set is performed. Thus,zygoma can be guided to the plannedbest repositioning. Relative positionbetween actual zygomatic location andtarget location is in real time updatedand presented by a distance map bet-ween both surfaces and by boundariesof both elements superimposition onaxial, sagittal and coronal series (fig. 7).
Navigation interface also provides ove-rimpression of planned orbital recons-tructed boundaries on axial, coronaland sagittal series. Accuracy of orbitalwalls reconstruction or implant place-
ment according to planning is checkedby scanning reconstructed orbital wallssurface with the calibrated pointer.
6
Fig. 5 : Planning for orbital reconstruction defined by symmetrical orbit fromthe healthy one around midsagittal plane.
Fig. 6 : 3DNS setting. DRF : Digital ReferenceFrame for registering patient’s anatomy to itsCT scan data set. DZF : Digital ZygomaticFrame for navigating bone fragment.
11.3 Marecaux 9/07/07 14:35 Page 6

Problem raised by our method was toknow if the point-to-surface zygomaticregistration according to the smallbone surface exposed through the limi-ted surgical approach is enough accu-rate for Zygoma repositioning. This hasbeen evaluated on a one piece dry skullpreviously CT scan acquired. 3DNSwas set up as previously presented.Mean and max distances of zygomaticsurface in DZF referential to the samesurface in DRF referential was compu-ted in 10 successive manipulations.
Patients
A pilot study of a non-comparative,non-randomized series of 3 patients
(table 1) was carried out to checkmethod feasibility. Advisory Comity forPeople Protection Consenting toClinical Research approval was obtai-ned through the Toulouse UniversityHospital, France. Informed consentforms were provided to patients, signedby both sides and collected by investi-gators.
2 patients had post traumatic malarasymmetry with associated enophthal-mos. One of them (patient 1) could nothave received primary surgical treat-ment because of initial neurosurgicalinjury and the second (patient 2) wasfirst operated 6 months before in ano-ther center. Patient 2 underwent bilate-ral OZMC fracture and left side was
7
Fig. 7 : 3DNS interface. Navigated zygoma location is in real time updated and tracked throughits boundaries overimpression on axial, coronal and sagittal views in comparison to target loca-tion or a distance map between actual and target locations.
11.3 Marecaux 9/07/07 14:35 Page 7

considered as the reference side forcontrolateral symmetrization. Patient 1initially lost vision by optic nerve inju-ry and patient 2 by eyeball dilacerationwhich required prosthetic rehabilita-tion. The last patient (patient 3) had anacute largely displaced zygomatic frac-ture with severe comminutive fractureof zygomatico-maxillary buttress andorbital rim. No ophthalmologic com-plication was associated.
Surgical approaches and number ofminiplates for zygomatic fixation wereindividualized according to the patien-t’s fracture. Intraoral upper sulcus andtransconjunctival incisions were usedin all patients. In secondary treatment,a temporal or coronal approach pre-viously used in a neurosurgical treat-ment was associated to control zygo-matic arch.
RESULTS
Accuracy of the point-to-surfacezygomatic registration
The computed mean distance betweenthe same zygomatic registered in DRFreferential and DZF referential was0,44 mm in mean and 0,91mm in maxi-mum (Table 1).
Pilot study
Computer aided planning and naviga-tion procedures were successfully car-ried out for all 3 clinical cases. Surgicalprocedures and postoperative courseswere uneventful.
Preoperative planning was completedin 7 to 10 minutes and was judgedquite convenient by practitioners.Virtual repositioning alone was usefulto conceptualize 3D displacement ofzygomatic bone. Navigation and gui-ding device and specially DZF did notstop performing surgical treatment.Surgical time increase due to 3DNSinstallation was about 20 minutes.Whereas no anatomical landmarksallowed intraoperatively to check sym-metry achievement, zygoma repositio-ning was done as indicated by intrao-perative guiding whatever practitionerthought.
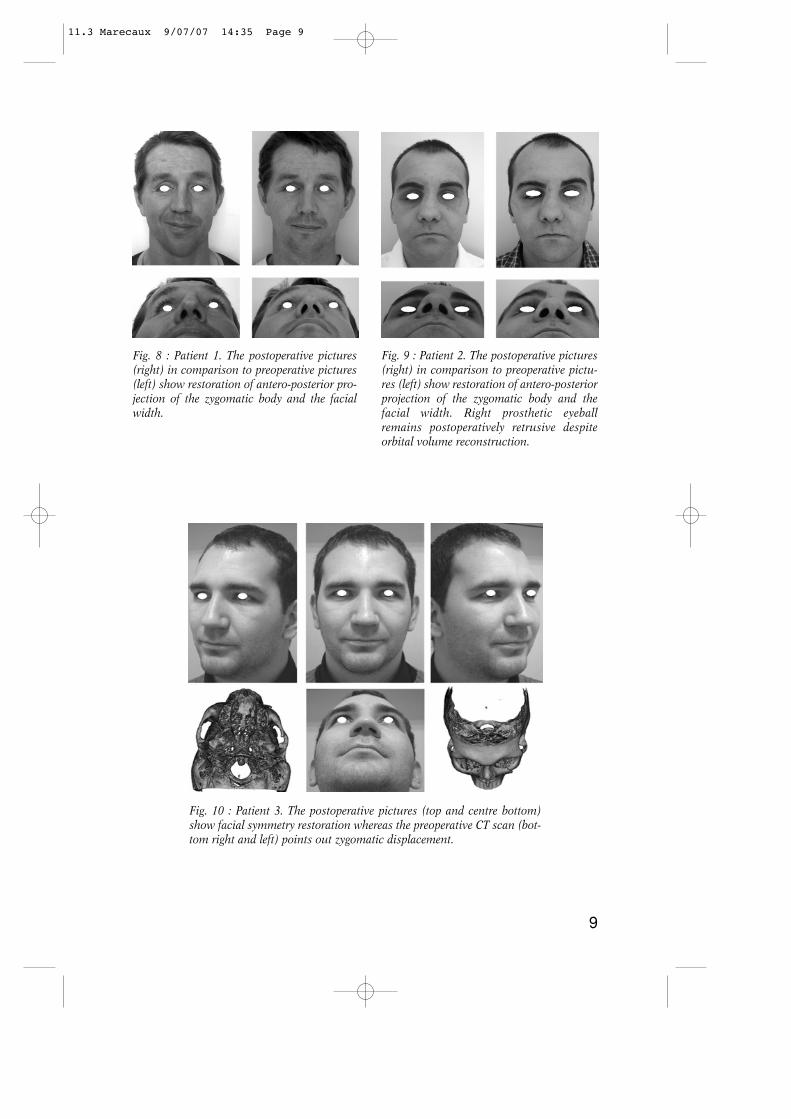
Surgical outcomes are presented(fig. 8, 9, 10). They have been conside-red as satisfying by both patient andsurgeon in all 3 cases. Patient 2 whohad initially bilateral OZMC fracturehas not been back on his pretraumaticappearance but on a slightly enlargedfacial width. However, he was totallysatisfied with facial symmetrization.None of the 3 patients complained ofthe cheek scare.
8
Determination Mean Max (mm) (mm)
1 0,41 0,932 0,45 0,973 0,32 0,904 0,46 0,895 0,61 1,116 0,28 0,717 0,48 0,878 0,43 0,999 0,52 1,0010 0,41 0,68
Mean 0,44 0,91
Table 1 : Distances computed of zygomaticsurface registered in DZF referential to thesame surface registered in DRF referential.
11.3 Marecaux 9/07/07 14:35 Page 8
9
Fig. 8 : Patient 1. The postoperative pictures(right) in comparison to preoperative pictures(left) show restoration of antero-posterior pro-jection of the zygomatic body and the facialwidth.
Fig. 9 : Patient 2. The postoperative pictures(right) in comparison to preoperative pictu-res (left) show restoration of antero-posteriorprojection of the zygomatic body and thefacial width. Right prosthetic eyeballremains postoperatively retrusive despiteorbital volume reconstruction.
Fig. 10 : Patient 3. The postoperative pictures (top and centre bottom)show facial symmetry restoration whereas the preoperative CT scan (bot-tom right and left) points out zygomatic displacement.
11.3 Marecaux 9/07/07 14:35 Page 9

DISCUSSION
Development of augmented realitytechniques seems to be able to helpsurgical treatment of late or acuteOZMC deformities resulting fromdisplaced or comminuted fractures.Preoperative, 3D multiplanar or surfa-cic reconstruction from CT scan dataset is helpful in evaluating the extentand the way of post traumatic deformi-ties. Then, 3D planning system basedon 3D virtual models allows segmenta-tion of the skeletal region of interestand interactive repositioning in orderto assess different alternatives andretain the best to achieve skeletal sym-metry. Finally, surgical procedure canbe carried out as planned preoperative-ly using 3DNS control and guidance.Thus, several suggestions were madeaddressing whether zygomatic reposi-tioning or orbital reconstruction, plan-ning or operative assistance for surgi-cal treatment [2, 3, 4].
The method we present includes allsteps of a comprehensive computeraided protocol from diagnostic tointraoperative assistance, for bothzygomatic and orbital reconstructionin primary or secondary treatment.Diagnostic, planning and simulationwere automated as much as possible toshorten allocated time and get the pro-cess friendly. All 3D skeletal and softtissue models, fractured zygoma ornon-injured orbit are semi-automati-cally segmented. Zygoma repositioningis automatically planned as the regis-tration of segmented injured zygoma tothe target skull. The correspondingmathematical transformation is equi-valent to the repositioning movementto apply. So far, manual shift with6 degrees of freedom in a virtual envi-ronment was suggested [4] but seemedtime consuming, difficult to achieve in
the same time reduction of all 4 zygo-matic buttresses and inaccurate in caseof dislocated fracture which does notallow visual control of buttresses align-ment. Targets for both zygomatic andorbital reconstruction are defined sym-metrically from the healthy sidearound the midsagittal plane.Landmarks-based definition of thefacial midsagittal plane without anyfurther correction can give rise to ashift in target skull definition. So, incorrection, we suggest to apply a dou-ble registration first rigid second elas-tic between symmetrical hemiskullcomputed from the healthy side andregions of interest of the native skullsurrounding OZMC.
The planned procedure componentsincluding 3D native skull, target skull,target orbit and zygoma models as wellas mathematical transformation aredirectly transferred to the operatingtheatre. OZMC reconstruction outlinescan be check similar to the plannedones scanning bone surface with thecalibrated pointer, but zygomatic trac-king makes proper repositioning easierand shorter. So far, only surface scan-ning control was performed [4] whatmeans zygomatic osteosynthesis has tobe taken down if repositioning is notchecked correct.
Primary or secondary OZMC recons-truction was addressed by others work-groups, because it synthesizes require-ments and difficulties of computer-assisted preoperative planning andintraoperative assistance in cranio-maxillofacial plastic and reconstructivesurgery. However, none of them dealtwith orbital and zygomatic reconstruc-tion in the same time while they areanatomically and physiopathologicallyclosely linked. Since no pretraumaticimaging data is available, all groups are
10
11.3 Marecaux 9/07/07 14:35 Page 10

agreed to plane reconstruction symme-trically from the healthy side around amidsagittal plane. However, to avoidinaccuracy due to landmarks baseddefinition of the midsagittal plane,either an automatic extraction basedon matching of homologous surfaceareas using an iterative closest pointoptimization can be used [5] or, as wesuggest, a correction by matching thetheoretical symmetrical skull to thenative skull around the region of inter-est. Planning of Zygoma repositioningto the target skull was mainly manualwhat reserves the method for modera-tely displaced zygomatic fracturewithout buttress dislocation whereaslarge displacement, dislocated fractureand secondary treatment are probablythe best indications for computed-assisted OZMC reconstruction. Somegroups ruled out direct bone guiding
fixing DRF onto the segmented bonewhich should be moved, to use as intraoperative assistance the only surfacescanning with a calibrated pointer tocheck reconstruction outline accurate[3]. In our opinion, in selected recons-tructive problems, direct bone gui-ding can be useful to achieve moreeasily repositioning as preoperativelyplanned.
This pilot study on the computer-assis-ted management of post traumaticOZMC deformities show virtual plan-ning for orbital boundaries reconstruc-tion or zygomatic repositioning, as wellas intraoperative guiding and verifica-tion of the surgical procedure in accor-dance with the planned one can be suc-cessfully carried out. First results seempromising specially in difficult case oflate deformities.
11
BIBLIOGRAPHY
[1] MAUBLEU S., MARECAUX C.,CHABANAS M. et al.Computer-aided planning for zygomaticbone reconstruction in maxillofacialtraumatology. Proceedings of the SecondInternational Conference Surgetica’2005:Computer-Aided Medical Interventions:tools and applications.Sauramps Medical Eds., 2005, pp.405-411.
[2] MARMULLA R. NIEDERDELL-MANN H. et al.
Surgical Planning of Computer-Assisted Repositioning Osteotomies.Plast. Reconstr. Surg., 1999: 104: 938-944.
[3] GELLRICH N.C., SCHRAMM A.,HAMMER B. et al.Computer-Assisted Secondary Recons-truction of Unilateral PosttraumaticOrbital Deformity.Plast. Reconstr. Surg. 2002, 110: 1417-1429.
[4] WESTENDORFF C.,GÜLICHER D., DAMMANN F. et al.Computer-Assisted Surgical Treatmentof Orbitozygomatic Fractures.J Craniofac.Surg., 2006, 17: 837-842.
[5] DE MOMI E., CHAPUIS J.,PAPPAS I. et al.Automatic extraction of the mid-facialplane for cranio-maxillofacial surgeryplanning.Int. J. Oral Maxillofac. Surg 2006, 35 :636-642.
11.3 Marecaux 9/07/07 14:35 Page 11