Embed Size (px)
Citation preview
Current Cases & Concepts
Computed Tomographic Documentation of a NowEnhancing Posterior Fossa Medulloblastoma: An Uncommon Presentation
Paul K. Woodrow, M.D. Jatin Gajarawala, M.D. Robert L. Pinck, M.D.
Department of Radiology, The Long Island College Hospital, Brooklyn, New York
Computed tomography (CT) is now well recognized as the procedure of choice in the diagnosis of medulloblastoma. It is also extremely useful in monitoring the patient’s response to surgical and/or radiation therapy (1). A review of CT literature reveals reference to only two cases that did not show enhancement following the intravenous injection of a contrast material during the patient’s initial workup (2).
CASE REPORT
A 13-year-old male was seen in the emergency room because of an occipital headache that had begun 5 days earlier and had been increasing in severity. For the 2 days prior to the admission, the patient also ex- perienced projectile vomiting. Neurological examina- tion revealed moderate nuchal rigidity, mild papille- dema, and a positive Kernig’s sign. Temperature was 103”.
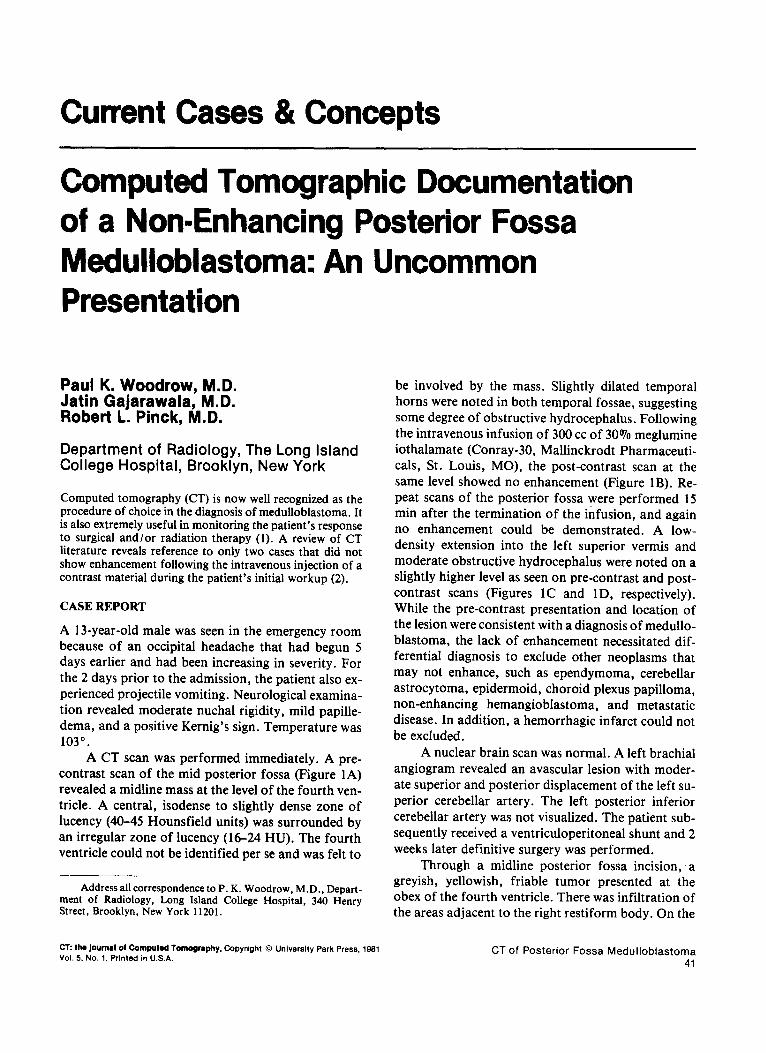
A CT scan was performed immediately. A pre- contrast scan of the mid posterior fossa (Figure 1A) revealed a midline mass at the level of the fourth ven- tricle. A central, isodense to slightly dense zone of lucency (40-45 Hounsfield units) was surrounded by an irregular zone of lucency (16-24 HU). The fourth ventricle could not be identified per se and was felt to -
Address all correspondence to P. K. Woodrow, M.D., Depart- ment of Radiology, Long Island College Hospital, 340 Henry Street, Brooklyn, New York 11201.
CT: tlm journal of Computed Tomography. Copyright 0 University Park Press. 1981
Vol. 5. No. 1, Printed in U.S.A.
be involved by the mass. Slightly dilated temporal horns were noted in both temporal fossae, suggesting some degree of obstructive hydrocephalus. Following the intravenous infusion of 300 cc of 30% meglumine iothalamate (Conray-30, Mallinckrodt Pharmaceuti- cals, St. Louis, MO), the post-contrast scan at the same level showed no enhancement (Figure 1B). Re- peat scans of the posterior fossa were performed 15 min after the termination of the infusion, and again no enhancement could be demonstrated. A low- density extension into the left superior vermis and moderate obstructive hydrocephalus were noted on a slightly higher level as seen on pre-contrast and post- contrast scans (Figures 1C and lD, respectively). While the pre-contrast presentation and location of the lesion were consistent with a diagnosis of medullo- blastoma, the lack of enhancement necessitated dif- ferential diagnosis to exclude other neoplasms that may not enhance, such as ependymoma, cerebellar astrocytoma, epidermoid, choroid plexus papilloma, non-enhancing hemangioblastoma, and metastatic disease. In addition, a hemorrhagic infarct could not be excluded.
A nuclear brain scan was normal. A left brachial angiogram revealed an avascular lesion with moder- ate superior and posterior displacement of the left su- perior cerebellar artery. The left posterior inferior cerebellar artery was not visualized. The patient sub- sequently received a ventriculoperitoneal shunt and 2 weeks later definitive surgery was performed.
Through a midline posterior fossa incision, a greyish, yellowish, friable tumor presented at the obex of the fourth ventricle. There was infiltration of the areas adjacent to the right restiform body. On the
CT of Posterior Fossa Medulloblastoma 41
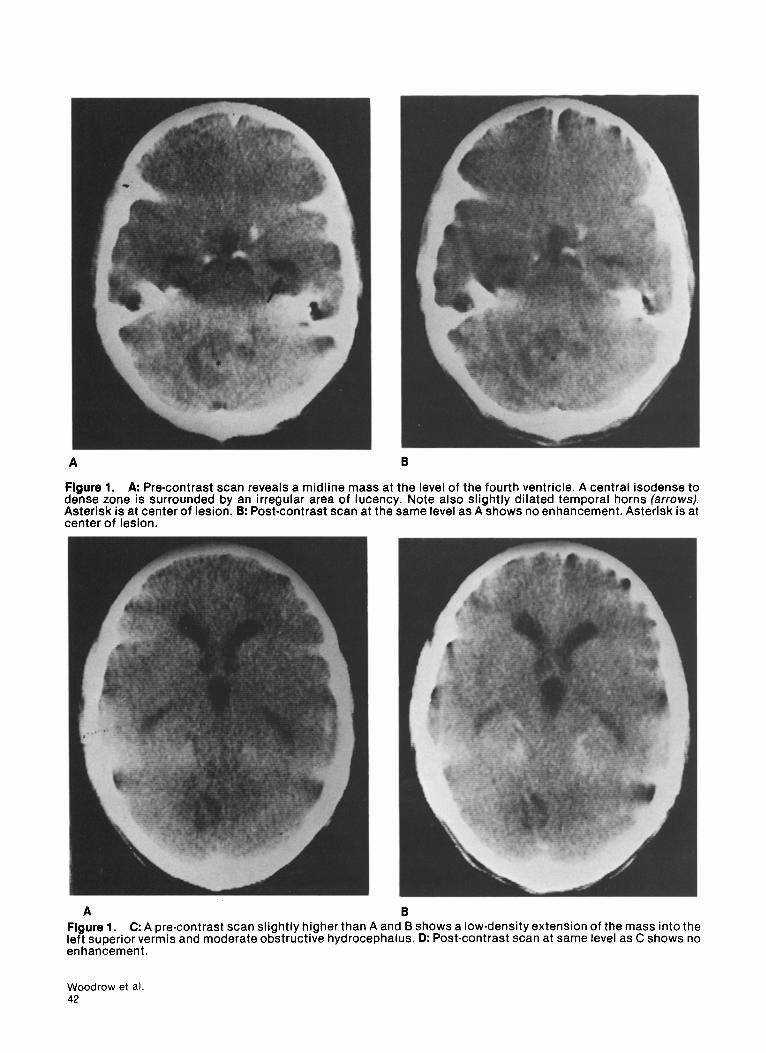
Figure 1. A: Pre-contrast scan reveals a midline mass at the level of the fourth ventricle. A central isodense to dense zone is surrounded by an irregular area of lucency. Note also slightly dilated temporal horns (arrows). Asterisk is at center of lesion. B: Post-contrast scan at the same level as A shows no enhancement. Asterisk is at center of lesion.
A B Figure 1. C: A pre-contrast scan slightly higher than A and B shows a low-density extension of the mass into the left superior vermis and moderate obstructive hydrocephalus. D: Post-contrast scan at same level as C shows no enhancement.
Woodrow et al 42

left side there was invasion of the cerebellar hemi- sphere. Rostrally, the tumor involved the vermis, ex- tending up to the anterior medullary velum. The floor of the fourth ventricle was free of tumor. Most of the tumor mass was removed from the fourth ventricle, cerebellar hemisphere, and superior vermis. The path- ological report revealed medulloblastoma. The mi- croscopic sections showed a highly cellular tumor composed of darkly staining cells with hyperchro- matic nuclei and ill-defined cytoplasmic outlines. A moderate number of mitotic figures were noted.
The patient did well post-operatively. Post-oper- ative brain irradiation (5500 rads) and whole spine ir- radiation (3600 rads) were performed. Four months after the completion of radiation therapy, a follow-up CT scan was performed on the patient, who was virtu- ally symptom free. The pre-contrast scan follow-up revealed an irregular low density in the mid posterior fossa. This may represent the fourth ventricle, which showed slight posterior retraction along its left poste- rior border, possibly secondary to post-surgical change. There was no definite evidence of residual or recurrent tumor. The post-contrast image at the same level showed no evidence of contrast enhancement.
DISCUSSION
The CT pre-contrast appearance of the classical med- ulloblastoma is variable. It may present as a lesion of hemogeneously increased density or of mixed density, or as an isodense mass. When the fourth ventricle is involved by the tumor, a lucent halo can often be noted surrounding the lesion. Calcification may be present but is not common. After the intravenous ad- ministration of contrast material, however, nearly all reported medulloblastomas show varying degrees of contrast enhancement. In a series of 24 medulloblas- tomas, Kingsley and Kendall (3) reported enhance- ment in all cases. Zimmerman et al. (4) also reported enhancement in each of their series of 13 proven medulloblastomas. In their series, the average in- crease in density of the tumor following contrast was 16 HU. In a series of 7 medulloblastomas, Nadich et al. (5) reported definite enhancement following con-
trast in all cases. Van Kirk et al. (6) reported enhance- ment in all 4 of their reported medulloblastomas. Pal- acios et al. (7) reported that medulloblastomas enhance an average of 16 HU with contrast infusion. Gado et al. (2), in a series of 4 histologically proven medulloblastomas, noted lack of contrast enhance- ment in 2 of these lesions. From our investigation, we are unable to document any additional cases revealing lack of contrast enhancement in a medulloblastoma.
Medulloblastomas are one of the most common posterior fossa tumors in children. While most of these lesions are found in the midline of the vermis be- hind and above the fourth ventricle, invasion of the fourth ventricle is quite common. In addition, the tumor may arise as far laterally as the cerebellopon- tine angle.
The lack of contrast enhancement in the poste- rior fossa mass does not necessarily exclude medullo- blastoma from the differential diagnostic considera- tions. The non-enhancing medulloblastoma should therefore be added to the differential diagnosis of non-enhancing lesions of the posterior fossa.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
Enzmann VR, Norman D, Levin V, Wilson C, Newton TH: Computed tomography in the follow-up of medul- loblastomas and ependymomas. Radiology 128:57-63, 1978 Gado M, Heute I, Mikhael M: Computerized tomog- raphy of infratentorial tumors. Semin Roentgen01 12: 109-120, 1977 Kingsley DPE, Kendall BE: The CT scanner in posterior fossa tumors of childhood. Brit J Radio1 52:769-776, 1979 Zimmerman RA, Bilaniuk LT, Pahlajani H: Spectrum of medulloblastomas demonstrated by computed to- mography. Radiology 126:137-141, 1978 Naidich TP, Lin JP, Leeds NE, Pudloski RM, Naidich JB: Primary tumors and other masses of the cerebellum and fourth ventricle: Differential diagnosis by com- puted tomography. Neuroradiology 14:153-174, 1977 Van Kirk OC, Cornell SH, Jacoby CC: Posterior fossa intra-axial tumors: A comparison of computed tomog- raphy with other imaging methods. CT 3(1):31-39, 1979 Palacios SE, Shannon M, Fine M: Unusual metastases from a medulloblastoma: Case report. Neuroradiology 17:219-222, 1979
CONTINUING MEDICAL EDUCATION QUESTIONS (COMPUTED TOMOGRAPHIC DOCUMENTATION OF A NON-ENHANCING POSTERIOR FOSSA MEDULLOBLASTOMA: AN UNCOMMON PRESENTATION)
True or False:
1. Calcification is a common finding in medulloblastomas. 2. The great majority of medulloblastomas will show contrast enhancement. 3. The pre-contrast scan of a medulloblastoma almost always shows an isodense mass. 4. Medulloblastomas are rarely located in the posterior fossa midline.
CT of Posterior Fossa Medulloblastoma 43