Embed Size (px)
Citation preview

A
tca(lasrs©
K
1
bstHb(fs[aatr
D
0d
Pathophysiology 16 (2009) 19–29
Computational molecular docking assessment of hormone receptoradjuvant drugs: Breast cancer as an example
Sayan Mukherjee, Durjoy Majumder ∗Bioinformatics, School of Information Technology, Faculty of Engineering & Technology, Bengal Engineering & Science University,
Shibpur, Botanic Garden, Howrah 711 103, West Bengal, India
Received 14 May 2008; received in revised form 29 November 2008; accepted 7 December 2008
bstract
For the maintenance therapy of breast cancer, drugs which act as antagonists/partial agonists of hormone receptors against the breastissue are used in the conventional clinical practices. However, during the course of treatment the patients may encounter systems relatedomplications. Drugs like tamoxifen, which block the action of estrogens at its receptors in mammary gland; and the recently designedntiestrogens and selective estrogen receptor modulators (SERM) like raloxifene, toremifene and the progesterone antagonist mifepristoneRU-486) are used in the treatment for estrogen and/or progesterone receptor positive breast tumors. These drugs show, however, both acute andong-term toxicity like endometrial hyperplasia and cancer, menopausal symptoms, edema, thromboembolic events like pulmonary embolismnd so on. Using molecular docking method, we studied the binding of these drugs at an array of receptors present within the physiological
ystem. In addition, the molecular basis of the antiglucocorticoid and antiandrogenic side effects of mifepristone have also been studied. Ouresults show weak to moderate binding of these drugs at various receptors of the body. This may explain the toxicity and pathophysiologicalhifting by these drugs during the long term use of these drugs.2008 Elsevier Ireland Ltd. All rights reserved.
logical
miacistt
tst[
eywords: Breast cancer; Antagonist; Agonist; Molecular docking; Physio
. Introduction
Steroidal hormones, like estrogen and progesterone haveeen shown to be the potent mitogens in a number of target tis-ues including the mammary gland. They play a pivotal role inhe development and progression of mammary carcinoma [1].istopathological evidences suggest that in a number of casesreast adenocarcinoma cells are either estrogen receptorER) or progesterone receptor (PR) or both positive. There-ore, the goal of the adjuvant therapy of breast cancer is totarve the hormone sensitive cells from hormonal stimulation2]. Hence, in the line of maintenance and supportive ther-py, patients are treated with drugs, which inhibit hormone
ction at its receptors in cancer cells (antagonists). Towardshis goal several estrogen blocking drugs namely tamoxifen,aloxifene, toremifene and the progesterone blocking drug∗ Corresponding author. Tel.: +91 33 2668 9312; fax: +91 33 2668 9313.E-mail addresses: [email protected],
[email protected] (D. Majumder).
(cMwedt
928-4680/$ – see front matter © 2008 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.pathophys.2008.12.001
alteration; Toxicity; Homeostasis
ifepristone (earlier known as RU-486) is suggested accord-ng to the hormone sensitivity of the cancer cells. To get
clinically effective result, these drugs have a long timeourse—of three to five years of treatment. However, dur-ng the long-term therapeutic schedule patients may developeveral complications and a range of chronic toxicity symp-oms including osteoporosis, menopausal symptoms, edema,hromboembolic events and endometrial hyperplasia [3].
Of the above mentioned drugs, tamoxifen is an oral selec-ive estrogen receptor modulator (SERM). Generally it isuggested for the treatment of early and advanced ER posi-ive breast cancer in both pre- and post-menopausal women4]. It is also approved by the Food and Drug AdministrationFDA, USA) for the reduction of the incidence of breast can-er in women who are at high risk of developing the disease.echanism of action of the drug is that tamoxifen competes
ith estrogen for ERs in breast tissue so that transcription ofstrogen-responsive genes is inhibited. Side effects may beue to the fact that, even though it is an antagonist in breastissue it acts as a partial agonist on the endometrium and

2 / Pathop
hTitr(tapvotoeegviec(itCt
eimmgfldipbhdCtb
oattoremta6cot
itmg4pbcp
sagotDaapetrMa4oflhodhaichsaesm
ttumw
2
2
0 S. Mukherjee, D. Majumder
as been linked to endometrial cancer in some women [5].amoxifen’s effect on estrogen beta receptors (ER-�) present
n bone gives rise to a complex side effect profile of the skele-al system. Tamoxifen treatment and menopausal status cor-elated significantly with the changes in bone mineral densityBMD) of lumbar spine. A significant BMD loss was noted inhose tamoxifen-treated patients who continued to menstru-te after chemotherapy. At 3 years of follow-up, menstruatingatients on tamoxifen had lost 4.6% of their baseline BMDalues (in presence of estrogen the drug acted as an antag-nist). On the contrary, tamoxifen decreased BMD loss inhose women who developed chemotherapy-induced amen-rrhea by acting as an estrogen agonist in this case [6]. Otherffects may be attributed to the fact that though it acts as anstrogen antagonist in breast cancer cells, it acts like an estro-en agonist in the uterus, liver, pituitary and cells of the bloodasculature, thus increasing patients’ risk of getting uter-ne cancer or a life-threatening blood clots (thromboembolicvents) [7]. Hot flashes occur due to blockage of physiologi-al actions of estrogen to the anterior nuclei of hypothalamusthe vasomotor effect of antiestrogens) [8]. Tamoxifens metabolized to 4-hydroxy tamoxifen and N-desmethylamoxifen by cytochrome P450 enzymes especially byYP2D6 [9]. Tamoxifen and its metabolites N-desmethyl
amoxifen have a half-life of approximately 14 days [10].Toremifene, another oral SERM opposes the actions of
strogen in the mammary tumors. Generally it is usedn advanced (metastatic) breast cancer. Side effects are
ore common in pre-menopausal women who may developenopausal side effects because of a reduced level of estro-
en. The most common side effects are nausea and hotashes. Studies have shown that women who take highoses of toremifene over a long period may have a slightlyncreased risk of developing endometrial cancer [11]. Thelasma concentration time profile of toremifene declinesi-exponentially after absorption with a mean distributionalf-life of about 4 h and an elimination half-life of about 5ays. Toremifene is extensively metabolized, principally byYP3A4 (cytochrome P450, family 3, subfamily A, polypep-
ide 4) to N-demethyltoremifene, which is also antiestrogenicut with a weak in vivo antitumor potency [12].
Raloxifene is also an oral SERM used in the preventionf osteoporosis in post-menopausal women by its actions asn agonist on the bone. However, raloxifene is as effective asamoxifen in reducing the incidence of breast cancer in cer-ain high risk groups of females, though with a reduced riskf thromboembolic events and cataracts in patients takingaloxifene vs. those taking tamoxifen [8]. Common adversevents considered drug-related hot flashes, leg cramps andore serious side effects include blood clots, deep vein
hrombosis and pulmonary embolism [13]. Raloxifene isbsorbed rapidly after oral administration. Approximately
0% of an oral dose is absorbed, but presystemic glucuronideonjugation is extensive making absolute bioavailabilityf raloxifene is 2.0%. Despite this, the drug is knowno have a long biological half-life of 27 h [14]. Ralox-ad
hysiology 16 (2009) 19–29
fene and the monoglucuronide conjugates are highly boundo plasma proteins. It also undergoes extensive first-passetabolism to the glucuronide conjugates: raloxifene-4′-
lucuronide, raloxifene-6′-glucuronide, and raloxifene-6′,′-diglucuronide. No other metabolites have been detected,roviding strong evidence that raloxifene is not metabolizedy cytochrome P450 pathways [15]. Unconjugated raloxifeneomprises less than 1% of the total radio labeled material inlasma [16].
The progesterone antagonist mifepristone is a syntheticteroid compound and it acts as a competitive progesteronentagonist in both A and B forms of the PR [8]. Because pro-estin antagonists are relatively new compounds, and becausef the controversy related to abortion, their efficacy in thereatment of breast cancer is just beginning to be evaluated.uring early trials, it was known as RU-486, its designation
t the Roussel Uclaf Company, which designed the drug. Thentiproliferative action of RU-486 in several models of PRositive breast cancer supports it as a logical treatment strat-gy in metastatic PR positive breast cancer. It is suggestedhat the antiproliferative efficacy of the antiprogestins iselated to their ability to induce terminal differentiation [17].
ifepristone is an orally active compound with nearly 70%bsorption rate but its bioavailability is reduced to around0% because of the first-pass effect. The drug had a half-lifef 20–30 h in most of the subjects studied [18]. Clearancerom the body occurs mainly through feces (83%). Bio-ogically active mono-demethylated, di-demethylated andydroxylated metabolites are found in plasma soon afterral administration of mifepristone. RU-486 and its mono-emethylated metabolite bind to progesterone receptors withigh affinity. Mifepristone is also a potent glucocorticoidntagonist and this antiglucocorticoid property is the mainmpediment in the use of this drug for long-term breast can-er. Acute side effects include nausea, vomiting, diarrhoea,eadache and dizziness, when used in abortion due to expul-ion of uterine contents. Long-term antiglucocorticoid andntiandrogenic properties may result in adrenal failure, exac-rbation of asthma and cardiovascular side effects [8]. Table 1hows a summary of drugs showing their structure, half-life,etabolism and side effects.The present work investigates the molecular portrayals of
hese side effects caused by different drugs used as adjuvantherapy for breast cancer at the systems level by the long-termses. To explain this we used molecular docking interactionethod for these drugs with an array of receptors presentithin the physiological system.
. Materials and methods
.1. Softwares and data sources
All softwares used for this analysis are freely available forcademic use. Table 2 provides the source of availability ofata used for the study.

S. Mukherjee, D. Majumder / Pathophysiology 16 (2009) 19–29 21
Table 1A summary of model drugs used showing structure, half-life, metabolism and side effects.
Drug Structure shown inFigure number
Half-life Metabolism Side effects
Tamoxifen Fig. 2A 14 days by the enzyme CYP2D6 BMD loss, vasomotor effect, thromboembolic event,amenorrhoea, endometrial hyperplasia, lactation failure
Toremifene Fig. 2B 5 days by the enzyme CYP3A4 Pulmonary embolism, hot flash, endometriosis,endometrial cancer, lactation failure
Raloxifene Fig. 2C 27 h by the enzyme CYP-P450 Pulmonary embolism, hot flash, depression, deep veinthrombosis, lactation failure
M oxylates
wbhPs
dcccpdd6almdd
wP
TSt
P
EEPTGPA
DETTRPTTN
cts
uRAtfds3rlpw
sT
ifepristone Fig. 2D 20–30 h Methylated and hydrcleared through fece
The Protein Data Bank (PDB) (www.rcsb.org) is a world-ide repository for the processing and distribution of 3Diological macromolecular structure data [19]. Presently itas over 20,000 structures determined by X-ray diffraction.rotein structures may be downloaded from the site withpecific keywords or a PDB alphanumeric filename.
The Drug Bank (http://redpoll.pharmacy.ualberta.ca/rugbank/) database [20] is a unique bioinformatics andheminformatics resource that combines detailed drug (i.e.,hemical, pharmacological and pharmaceutical) data withomprehensive drug target (i.e., sequence, structure, andathway) information. The database contains nearly 4300rug entries including >1000 FDA-approved small moleculerugs, 113 FDA-approved biotech (protein/peptide) drugs,2 nutraceuticals and >3000 experimental drugs. Addition-lly, more than 6000 protein (i.e., drug target) sequences areinked to these drug entries. Each Drug Card entry contains
ore than 80 data fields with half of the information beingevoted to drug/chemical data and the other half devoted to
rug target or protein data.PyMol (version 0.99) is a Python-based visualization soft-are (Delano Scientific, 2006; www.pymol.org) [21]. TheDB files of the proteins obtained from the Protein Data Bank
able 2ources of data used. PDB denotes protein data bank and the selected recep-
ors (R) are of human origin (Homo sapiens).
rotein or drug data Source
strogen receptor (ER) alpha PDB ID 1X7Estrogen receptor (ER) beta PDB ID 1NDErogesterone receptor (PR) PDB ID 20VMhyroid Receptor (TR) PDB ID 2H6Wlucocorticoid receptor (GR) PDB ID 1NHZrolactin Receptor (PLR) PDB ID 1BP3ndrogen receptor (ligandbinding domain) (AR)
PDB ID 2AMA
examethasone THE DRUG BANK(APRD00674)stradiol THE DRUG BANK(APRD00311)amoxifen THE DRUG BANK(APRD00123)oremifene THE DRUG BANK(APRD00391)aloxifene THE DRUG BANK(APRD00400)rogesterone THE DRUG BANK(APRD00700)hyroxine T4 THE DRUG BANK(APRD00235)hyroxine T3 PDB ID 2H6Wandrolone THE DRUG BANK(APRD00134)
(a
2
op
1
d product Nausea, vomiting, diarrhoea, headache, dizziness,asthma, hypotension, loss of hair growth, loss of libido,failure in lactation
an be visualized using PyMol. It has tools for measuring dis-ances as well as identifying different atoms. PyMol has beenelected for the analysis of the docking results.
AutoDock: The docking experiments were performedsing the docking software AutoDock 3.0 (The Scrippsesearch Institute, www.scripps.edu) [22–24], with the helputoDockTools (ADT)—an accessory program that allows
he user to interact with AutoDock from a Graphic User Inter-ace (GUI). AutoDock is a suite of automated docking toolsesigned to predict how small molecules/ligands such as sub-trates or drug candidates, bind to a receptor/protein of knownD structure. AutoDock (version 3.0) consists of three sepa-ate programs: AutoDock which performs the docking of theigand to a set of grids describing the target protein; AutoGridre-calculates these grids; and AutoTors sets up which bondsill be treated as rotatable in the ligand.Nucleotide/protein sequence: Nucleotide/protein
equence of the receptors (ER-�, ER-�, PR, GR, AR,R and PRL) has been retrieved from PDB data bank
Table 2). These sequences were used for homology andligning the sequences.
.2. Molecular docking
For getting the drug-receptor binding energy proceduresf molecular docking were followed. The detailing of therocedure is as follows.
. Preparing the ligand and macromolecule files forAutoDock: The PDB files obtained from the World WideWeb repository are often far from perfect for dockingstudy and present with potential problems like missinghydrogen atoms, multiple molecules, added waters andrelated problems. Using the GUI (graphic user interface)of ADT, we prepared the files as follows:(a) The Macromolecule file: The downloaded PDB files
were first read in ADT, added waters removed andpolar hydrogens were added. ADT then checked if themolecule had charges, if not ADT checked whether
the molecule was a peptide (by checking whether allof its residues’ names appear in the standard set of 20commonly occurring amino acids). If the moleculewas found to be a peptide Kollman charges were
2 / Pathop
2
3
4
2 S. Mukherjee, D. Majumder
added, else Gasteiger charges were added. Finally sol-vation parameters were added and the files saved with.pdbqs extension (where ‘q’ and ‘s’ represent chargeand solvation, respectively).
(b) The Ligand file: In a similar procedure, the ligandfiles were read in ADT, all hydrogens added, chargesadded and non-polar hydrogens merged and savedwith .pdbqs extension. ADT then automatically deter-mined the best root. The root is defined as the fixedportion of the ligand from which rotatable branchessprout. Next, we defined rotatable bonds in the lig-and, making all amide bonds non-rotatable and set thenumber of active torsions to fewest atoms. The ligandfile was then saved with ligand.out.pdbq extension (qrepresenting charge).
. Preparing the grid parameter file: For the calculation of
docking interaction energy, a three-dimensional box (grid)was created in which the protein molecule is enclosed.The grid volume was large enough to allow the ligandto rotate freely, even with its most fully extended con-Fig. 1. Schematic flow chart for the use of A
hysiology 16 (2009) 19–29
formation. The parameters required to create such a gridwere stored in the Grid Parameter File with molecule.gpfextension.
. Then AutoGrid3 job was run; autogrid3 creates onemap for every type of atom in the ligand. For examplea molecule having C, N, O, H, maps will be createdas molecule.C.map, molecule.N.map, molecule.O.map,molecule.H.map. These are grid maps in ASCII formatfor readability by AutoDock. AutoGrid also generatescorresponding output of the macromolecular file with theextension molecule.glg.
. Preparing the docking parameter file: The docking param-eter file, which instructs AutoDock about the ligand tomove, the map files to use, and other properties definedfor the ligand was created. AutoDock’s search meth-ods include the Monte Carlo simulated annealing (SA)
method, the Genetic Algorithm (GA), local search (LS)and the hybrid genetic algorithm with local search (GA-LS). The latter is also referred to as the Lamarckian geneticalgorithm (LGA) because offsprings are allowed to inheritutoDock for protein–ligand docking.

/ Pathophysiology 16 (2009) 19–29 23
5
2
FEAP(af
3
arTrt(
Fm
ae
TD
R
EA
EB
G
T
Tfi
S. Mukherjee, D. Majumder
the local search adaptations of their parents and this wasthe chosen algorithm for our analysis.
. Finally, the AutoDock job was run from the GUI (graph-ical user interface) of ADT and the docked ligand files(.dlg extension) were used for study. The dlg files wereread in ADT as well as in PyMol to calculate the bind-ing energies in the docked ligand–protein complexes. Theentire procedure is schematically shown in Fig. 1.
.3. Homology search
A BLAST homology search between 2 sequences inASTA format was done between ER-�, ER-� and PR;R-�, ER-� and GR; PR and GR; ER-�, ER-� andR; AR and PR; and ER-�, ER-�, PR, GR, AR andRL. The blast program is available at the NCBI websitehttp://www.ncbi.nlm.nih.gov/blast/bl2seq/). bl2seq is a vari-nt of the blast program in which two sequences in FASTAormat are aligned and mismatches highlighted.
. Results
To assess the cross-reactivity of various drugs used asn adjuvant therapy for breast cancer to different hormonaleceptors rigorous docking experiments had been performed.
he drugs, the receptors and the corresponding dockingesults are listed in Table 3. Corresponding figures men-ioned in Table 3 demonstrates the receptor ligand interactionFigs. 3–9).
Tiea
able 3ocking results of various drugs at an array of hormone receptors.
eceptor Drug �G (kcal/mol) Figure number R
strogenlpha
Tamoxifen −6.68 3A PToremifene −6.88 3BRaloxifene −7.77 3CEstradiol −10.0 3DMifepristone −5.89 3EProgesterone −5.75 3F
strogeneta
Tamoxifen −5.11 4A PToremifene −5.49 4BRaloxifene −6.83 4CEstradiol −9.21 4DMifepristone −5.80 4EProgesterone −5.74 4F
lucocorticoid Tamoxifen −1.82 5A AToremifene −3.89 5BRaloxifene −4.77 5CEstradiol −8.44 5DMifepristone −8.50 5EProgesterone −8.59 5FDexamethasone −7.49 5G
hyroid Tamoxifen −1.78 9A TToremifene −4.95 9BRaloxifene −7.10 9CEstradiol −5.60 9D
able showing minimum Gibbs’ Free Energy (�G) of receptor vs. drug binding.gure are tabulated only.
ig. 2. Structure of drugs tamoxifen (A), toremifene (B), raloxifene (C) andifepristone (D).
The docked conformation of various drugs on the ER-lpha (ER-�) showed that the natural endogenous ligandstradiol had the highest affinity for the receptor (Table 3).
he SERM raloxifene had the next highest binding affin-ty (most negative Gibbs free energy) among the drugs, thusxplaining its efficacy in chemoprevention and antiprolifer-tive effects even at a low bioavailability. Tamoxifen and
eceptor Drug �G (kcal/mol) Figure number
rogesterone Tamoxifen −2.94 6AToremifene −3.92 6BRaloxifene −5.95 6CEstradiol −5.75 6DMifepristone −8.19 6EProgesterone −9.10 6F
rolactin Tamoxifen −3.17 7AToremifene −4.83 7BRaloxifene −4.74 7CEstradiol −5.03 7DMifepristone −5.90 7EProgesterone −5.43 7F
ndrogen Tamoxifen −3.41 8AToremifene −4.77 8BRaloxifene −5.08 8CEstradiol −7.81 8DMifepristone −8.06 8EProgesterone −7.19 8FNandrolone −7.79 8G
hyroid Mifepristone −7.74 9EProgesterone −6.00 9FThyroxine (T4) −8.40 9GThyroxine (T3) −13.1 9H
�G minimal conformation out of 20 docking runs and the corresponding

24 S. Mukherjee, D. Majumder / Pathophysiology 16 (2009) 19–29
F ristone (i ge. (Forr
t−ttrp�B
(5
d
Fir
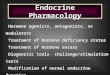
ig. 3. Tamoxifen (A), toremifene (B), raloxifene (C), estradiol (D), mifepn its lowest energy docked conformation. Drug molecule is shown in oraneferred to the web version of the article.)
oremifene had binding energies in the range of −6.6 to6.9 kcal/mol demonstrating efficacy of these drugs in the
reatment of ER-� positive metastatic breast cancer. Proges-erone and mifepristone showed less affinity towards ER-�,
eceptor homology between ER and PR may explain whyrogesterone showed some affinity for binding to the ER-(Table 4). To test this we used the bl2seq variant of theLAST program of NCBI to align two FASTA sequences
hr�T
ig. 4. Tamoxifen (A), toremifene (B), raloxifene (C), estradiol (D), mifepristone (n its lowest energy docked conformation. Drug molecule is shown in orange. (Foreferred to the web version of the article.)
E) and progesterone (F) docked onto the estrogen receptor � (ER-�, blue)interpretation of the references to color in this figure legend, the reader is
like ER and PR) and results showed high positive value of5% and identities 29%.
At the ER-beta (ER-�) docked conformation of variousrugs showed that the natural endogenous ligand estradiol
as the highest affinity for the receptor (Table 3). The SERMaloxifene had the next highest binding affinity with ER-(Table 3) explaining its positive effects on the bone.oremifene and tamoxifen had binding energies in the range
E) and progesterone (F) docked onto the estrogen receptor � (ER-�, blue)interpretation of the references to color in this figure legend, the reader is

S. Mukherjee, D. Majumder / Pathophysiology 16 (2009) 19–29 25
F stone (Er ule is shl
optimip
nh
Fir
ig. 5. Tamoxifen (A), toremifene (B), raloxifene (C), estradiol (D), mifeprieceptor (GR, blue) in its lowest energy docked conformation. Drug molecegend, the reader is referred to the web version of the article.)
f −5.5 and −5.1 kcal/mol, respectively, explaining theirositive binding and the probable side effects. Similarly tohe ER-�, progesterone and mifepristone show some affin-
ty towards ER-�, receptor homology between ER-� and PRay explain why progesterone shows some affinity for bind-ng to the ER. The blast scores showed identities = 29% andositives = 52% (Table 4).
4Smo
ig. 6. Tamoxifen (A), toremifene (B), raloxifene (C), estradiol (D), mifepristonen its lowest energy docked conformation. Drug molecule is shown in orange. (Foreferred to the web version of the article.)
), progesterone (F) and dexamethasone (G) docked onto the glucocorticoidown in orange. (For interpretation of the references to color in this figure
The situation at the PR was remarkably similar with theatural endogenous ligand progesterone binding with veryigh affinity followed by the progesterone antagonist RU-
86 or mifepristone as expected (Table 3). As expected theERM drugs specifically tamoxifen and toremifene bounduch weakly to the PR with the binding energies in the rangef −2.9 and −3.9 kcal/mol, respectively.
(E) and progesterone (F) docked onto the progesterone receptor (PR, blue)interpretation of the references to color in this figure legend, the reader is

26 S. Mukherjee, D. Majumder / Pathophysiology 16 (2009) 19–29
F stone (El r interpt
titMmit
etP
a(adiMsd
F(r
ig. 7. Tamoxifen (A), toremifene (B), raloxifene (C), estradiol (D), mifepriowest energy docked conformation. Drug molecule is shown in orange. (Foo the web version of the article.)
At the thyroid receptor (TR), the endogenous ligandhyroxine-T3 bound with the highest affinity followed byts other natural ligand thyroxine-T4 (Table 3) comparedo all other ligands interactions investigated in this study.
ifepristone, raloxifene, progesterone and estradiol showedoderately strong binding with a decreasing order. Tamox-
fen showed negligible affinity for the receptor, whereasoremifene showed weak to moderate affinity for the TR.
At the glucocorticoid receptor (GR), progesterone andstradiol showed high affinity for docking, possibly dueo homology between the receptors. Between GR andR blast scores were identities = 52% and positives = 71%
t
dM
ig. 8. Tamoxifen (A), toremifene (B), raloxifene (C), estradiol (D), mifepristone (EAR, blue) in its lowest energy docked conformation. Drug molecule is shown in oreader is referred to the web version of the article.)
) and progesterone (F) docked onto the prolactin receptor (PLR, blue) in itsretation of the references to color in this figure legend, the reader is referred
nd, between ER and GR identities = 29%, positives = 55%Table 4). The synthetic ligand dexamethasone was used asstandard as coordinates of cortisol were not found in the
atabase search. Dexamethasone showed high binding affin-ty for the glucocorticoid receptor as expected (Table 3).
ifepristone displayed its antiglucocorticoid property with atrongly negative binding energy (Table 3). The three SERMrugs raloxifene, toremifene and tamoxifen showed moderate
o weak affinity.At the prolactin receptor (PLR), progesterone and estra-iol showed moderate affinity for binding to the receptor.ifepristone had moderate affinity and the three SERM drugs
), progesterone (F) and nandrolone (G) docked onto the androgen receptorange. (For interpretation of the references to color in this figure legend, the

S. Mukherjee, D. Majumder / Pathophysiology 16 (2009) 19–29 27
F ristonet rug mot
rbtai
tr(sTwaEita
TH
R
EEEEEEEEPPPPP
4
rdtAwbtaotr
ig. 9. Tamoxifen (A), toremifene (B), raloxifene (C), estradiol (D), mifephe thyroid receptor (TR, blue) in its lowest energy docked conformation. Dhis figure legend, the reader is referred to the web version of the article.)
aloxifene, toremifene and tamoxifen had moderate to weakinding affinity in the range of −4.8 to −3.2 kcal/mol inhe order of toremifene and raloxifene having nearly similarffinity (toremifene had slightly greater affinity) and tamox-fen showing the poorest binding energy.
Finally we checked the antiandrogenic effect of mifepris-one and found that the drug strongly bound to the androgeneceptor’s (AR) ligand binding domain with high affinityTable 3). The synthetic ligand nandrolone had been cho-en as it had very high affinity for the receptor (Table 3).here was significant receptor homology between AR and ERith identities = 25% and positives = 50% and, between AR
nd PR with identities = 55% and positives = 78% (Table 4).stradiol and progesterone showed moderately high affin-
ty for the receptor. The SERM drugs bound in the order ofamoxifen being the poorest binder followed by toremifenend raloxifene (Table 3).
able 4omology search data between the array of receptors.
eceptors Similarity (identity% and positives%)
R Alpha vs. PR Identity = 29%; positives = 55%R Alpha vs. ER Beta Identity = 59%; positives = 82%R Beta vs. PR Identity = 29%; positives = 52%R Alpha and beta vs. PRL No significant similarityR Alpha vs. GR Identity = 52%; positives = 71%R Beta vs. GR Identity = 32%; positives = 56%R Alpha vs. AR Identity = 25%; positives = 50%R Beta vs. AR Identity = 30%; positives = 55%R vs. GR Identity = 52%; positives = 71%R vs. AR Identity = 55%; positives = 78%RL vs. PR No significant similarityRL vs. GR No significant similarityRL vs. AR No significant similarity
ttroa(ots
imAcamfsl
(E), progesterone (F), thyroxine (T4) (G) and thyroxine (T3) docked ontolecule is shown in orange. (For interpretation of the references to color in
. Discussion
To make a comparison between drugs to their targeteceptors estradiol, progesterone, thyroxine, nandrolone andexamethasone were taken as endogenous ligand controls tohe corresponding receptors, i.e., to the receptors ER, PR, TR,R and GR, respectively. For PLR, its endogenous ligandas not tested as prolactin was too large ligand to be handledy the autotors program of AutoDock software. The generalrend of protein–ligand docking showed that tamoxifen beingSERM bound strongly only to the ER and most poorly atther receptors. Toremifene had a similar trend, but it boundo non-ERs with slightly higher affinity than tamoxifen andaloxifene bound to non-ERs with slightly higher affinity thanoremifene. Estradiol and progesterone bound to most recep-ors in our study, though they were not their endogenouseceptors, with considerable affinity possibly due to homol-gy in receptor shape. We had found that ER-� and ER-�s well as PR and GR exhibited a high degree of homologyTable 4). They had high identities and positives and lowr no gap percentages as visible from the bl2seq variant ofhe BLAST homology search that aligns two peptide/proteinequences.
The antiestrogenic effects of the SERM drugs tamox-fen, toremifene and raloxifene on the ovary would induce
enopausal symptoms, primary and secondary amenorrhea.gonism of estrogen on uterine receptors could increase
hances of uterine cancer. Similarly actions on the cells ofrteries increase risk of thromboembolic events like a pul-
onary embolism. In pulmonary thromboembolism, a clotorms and tries to pass through the capillaries, till the pas-age is too narrow for the clot thus blocking circulation in theungs. Estrogen like actions on the endometrium could cause

2 / Pathop
eo
pnIioiwmttgp
s(sapctscatpu
ruoiatprraatllatdwn[iamtil
sobiwetwiohtmi
iiautpcc
A
IvDne
R
8 S. Mukherjee, D. Majumder
ndometrial hyperplasia, the long-term toxicity possible mayccur with this chemotherapy.
Tamoxifen group of drugs through their actions on theituitary hypothalamic axis can cause acute hot flashes atight and up-regulate estrogen receptors in undesired places.n pre-menopausal women, binding of an SERM like tamox-fen as an antagonist to ER-� may correlate with loweringf BMD, though raloxifene acts more of an agonist hav-ng beneficial effect on BMD in postmenopausal womenhere the presence of estrogen is decreased. Chemotherapyakes pregnancy almost impossible to succeed and of course
he abortion pill mifepristone in PR positive breast cancerreatment would cause immediate abortion through antipro-esterone actions on the uterus causing the detachment of thelacenta.
Mifepristone was also bound to most receptors in ourtudy with highest affinities with GR (−8.5 kcal/mol), PR−8.19 kcal/mol) and AR (−8.1 kcal/mol). Mifepristone’side effects are more severe owing to its antiglucocorticoidctions in the brain and the adrenal glands where the increasedressure by negative feedback loop on the adrenals mightause acute adrenal failure and chronically reduced glucocor-icoid levels may lead to exacerbation of asthma and hypoten-ion. Antiandrogenic properties of the drug would causehanges in hair growth pattern and libido. In males the effectsre far more severe and gynomasticia can occur. Binding ofhese drugs to PLR may lead to a disturbance in the lactationrocess, total failure of lactation have been reported in womenndergoing SERM or mifepristone chemotherapy [25].
Present study is theoretical and based on docking algo-ithm. The general trend is that the docking methods aresed during the course of drug discovery for the screeningf true ligand from false one [26]. For this approach a targets docked against an array of drug molecules. Here attemptsre made to find-out the cross-reactivity of a drug moleculeowards its off-targets. Homology analysis between differentrotein receptors is used to support the rationality of cross-eactivity of drugs with its off-targets. Selected drugs areoutinely used in clinic for the patients of breast cancer andre suggested for long-term use. However, there is no reli-ble experimental procedure at present which can predict theoxicity of any drug at the systems level particularly for theong drawn out therapeutic procedure. At the experimentalevel the toxicity testing of drug relies on the linear approachnd of course, of short duration and that may not sufficient inhe understanding of drug-related toxicity in long-term proce-ure [27]. Similar sort of evidences also found in the literaturehere systems level adverse effect of low dose calcium isoted in the long term for the treatment of hypocalcemia28]. This issue, particularly in cancer, has been addressedn some recent works and reinforces the need of theoreticals well as simulation study [29–33]. As breast cancer treat-
ent involves long-drawn out therapeutic procedure and dueo absence of clinical data regarding the onset of toxicolog-cal symptoms we depend on scanty reports present in theiterature for choosing the off-targets.
hysiology 16 (2009) 19–29
With respect to drug discovery docking methods are con-idered to have a modest predictive power as the performancef the algorithms are of stochastic in nature, however, areased on the chemical principles of the ligands/bio-moleculesnteractions. However, the proper utilisation of this techniqueith respect to the toxicological assessment has not been
xploited. With the availability of data related to the onsetoxicological symptoms, a correlation study between the twoould then be beneficial in future particularly for the cal-
bration of duration of drug application. Hence, generationf database about the onset of toxicological symptoms inumans (for different drugs) is needed. Towards this aspecthis study has of significance. However, if any in vitro experi-ental data corresponds to the theoretical data in future, then
t would definitely strengthen the theoretical study.Comparative analysis of interaction between a drug with
ts ideal receptor and to its off-targets may indicate a weaknteraction of drug to its off-targets. Though the interactionsre weak, however, the docking algorithm and computer sim-lation may provide the molecular rationale of toxicity withinhe physiological system and the probable cause of patho-hysiological alteration due to long-term use of differenthemotherapeutic drugs used as the adjuvant therapy of breastancer.
cknowledgement
S.M. is an honorary research fellow at the School ofnformation Technology, Bengal Engineering & Science Uni-ersity, Shibpur. Authors are thankful to Prof. S. Barat,irector, School of Information Technology, Bengal Engi-eering & Science University, Shibpur for his constantncouragement for doing this work.
eferences
[1] K.C. Osborne, Steroid hormone receptors in breast cancer management,Breast Cancer Res. Treat. 51 (1998) 227–238.
[2] G. Shyamala, Y.C. Chou, S.G. Louie, R.C. Guzman, G.H. Smith, S.Nandi, Cellular expression of estrogen and progesterone receptors inmammary glands: regulation by hormones, development and aging, J.Steroid Biochem. Mol. Biol. 80 (2002) 137–148.
[3] E. Chu, A.C. Sartorelli, Cancer chemotherapy, ch. 55, Section VIII, in:B.G. Katzung (Ed.), Basic and Clinical Pharmacology, 9th edn., McGraw Hill, New York, 2004, pp. 878–907.
[4] V.T. De Vita, S. Hellman, S.A. Rosenberg, Tamoxifen and breast can-cer, in: Cancer: Principles and Practice of Oncology, ch. 32, 7th edn.,Lippincott Williams & Wilkins, Philadelphia, USA, 2004, pp. 1399–1487.
[5] P.J. Taskinen, T. Laatikainen, Endometrial changes in postmenopausalwomen receiving tamoxifen, Obstet. Ggynecol. 81 (1993) 660–664.
[6] V. Leena, E. Inkeri, B. Carl, S. Tiina, Tamoxifen treatment after adju-vant chemotherapy has opposite effects on bone mineral density in
premenopausal patients depending on menstrual status, J. Clin. Oncol.24 (2006) 675–680.[7] B. Fischer, J. Costantino, D. Wickerham, C. Redmond, M. Kavanah,W. Cronin, V. Vogel, A. Robidoux, N. Dimitrov, J. Atkins, M. Daly, S.Wieland, E. Tan-chiu, L. Ford, N. Wolmark, Tamoxifen for the preven-

/ Pathop
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
S. Mukherjee, D. Majumder
tion of breast cancer. Project P-1 study, J. Natl. Cancer Inst. 90 (1998)1371–1388.
[8] D. Loose-Mitchell, G.M. Stancel, Hormones and hormone antagonists,in: J.G. Hardman, E. Limbard (Eds.) [A.G. Gilman (Consult. Ed.)], ThePharmacological Basis of Therapeutics; ch. 58, Section XII, 10th edn.,McGraw Hill, New York, San Francisco, Singapore, Sydney, 2001, pp.1597–1634.
[9] H.K. Crewe, L.M. Notley, R.M. Wunsch, M.S. Lennard, E.M. Gillam,Metabolism of tamoxifen by recombinant human cytochrome P450enzymes: formation of the 4-hydroxy, 4′-hydroxy and N-desmethylmetabolites and isomerization of trans-4-hydroxytamoxifen, DrugMetab. Dispos. 30 (2002) 869–874.
10] D. De Vos, P.H. Slee, D. Stevenson, R.J. Briggs, Serum eliminationhalf-life of tamoxifen and its metabolites in patients with advancedbreast cancer, Cancer Chemother. Pharmacol. 31 (1992) 76–78.
11] R.M. O’Regan, A. Cisneros, G.M. England, J.I. MacGregor, H.D.Muenzner, V.J. Assikis, M.M. Bilimoria, M. Piette, Y.P. Dragan, H.C.Pitot, R. Chatterton, V.C. Jordan, Effects of the antiestrogens tamox-ifen, toremifene, and ICI 182,780 on endometrial cancer growth, J.Natl. Cancer Inst. 90 (1998) 1552–1558.
12] L. Kangas, Review of the pharmacological properties of toremifene, J.Steroid. Biochem. 36 (1990) 191–195.
13] S. Cummings, S. Eckert, K. Krueger, D. Grady, T. Powles, J. Cauley,L. Norton, T. Nickelsen, N. Bjarnason, M. Morrow, M. Lippman, D.Black, J. Glusman, A. Costa, V.C. Jordan, The effect of raloxifene onrisk of breast cancer in postmenopausal women: results from the MORErandomized trial. Multiple outcomes of raloxifene evaluation, JAMA281 (1999) 2189–2190.
14] V.C. Jordan, Beyond raloxifene for the prevention of osteoporosis andbreast cancer, Br. J. Pharmacol. 150 (2007) 3–4.
15] K.R. Synder, N. Sparano, J.M. Malinowski, Raloxifene hydrochloride,Am. J. Health Syst. Pharm. 57 (2000) 1669–1675.
16] P. Reddy, M.S. Chow, Safety and efficacy of antiestrogens for preven-tion of breast cancer, Am. J. Health Syst. Pharm. 57 (2000) 1315–2132.
17] K.B. Horwitz, Clinical Applications of Mifepristone (RU486) and otherAntiprogestins: Assessing the Science and Recommending a ResearchAgenda, in: M.S. Donaldson, L. Dorflinger, S.S. Brown, and L.Z. Benet,(Eds.), ch. B9, The National Academies Press, 1993, pp. 210–228[website: http://www.nap.edu/catalog.php?record id=2203#toc].
18] N.N. Sarkar, Mifepristone: bioavailability, pharmacokinetics and use-
effectiveness, Eur. J. Obstet. Gynecol. Reprod. Biol. 101 (2002)113–120.19] H.M. Berman, J. Westbrook, Z. Feng, G. Gilliland, T.N. Bhat, H. Weis-sig, I.N. Shindyalov, P.E. Bourne, The Protein Data Bank, NucleicAcids Res. 28 (2000) 235–242.
[
hysiology 16 (2009) 19–29 29
20] D.S. Wishart, C. Knox, A.C. Guo, S. Shrivastava, M. Hassanali, P.Stothard, Z. Chang, J. Woolsey, Drug Bank: a comprehensive resourcefor in silico drug discovery and exploration, Nucleic Acids Res. 1 (2006)34–36.
21] W.L. Delano, The PyMol Molecular Graphics System, Delano Scien-tific, San Carlos, CA, USA, 2004 (website: http://www.pymol.org).
22] G.M. Morris, D.S. Goodsell, R.S. Halliday, R. Huey, W.E. Hart, R.Belew, J.K. Olson, Automated docking using a Lamarckian geneticalgorithm and an empirical binding free energy function, J. Comput.Chem. 19 (1998) 1639–1662.
23] G.M. Morris, D.S. Goodsell, R. Huey, W.E. Hart, S. Holliday, R. Belew,A.J. Olson, User’s guide AutoDock—Automated Docking of Flexi-ble Ligands to Receptors, The Scripps Research Institute, MolecularGraphics Laboratory, 2001, pp. 1–86 [website: http://autodock.scripps.edu/faqs-help/manual/autodock-3-user-s-guide].
24] R. Huey, G.M. Morris, Using AutoDock with AutoDockTools: A Tuto-rial, The Scripps Research Institute, Molecular Graphics Laboratory,USA, 2006, pp. 1–51.
25] I. Romieu, M. Hernandez-Avila, E. Lazcano, L. Lopez, R. Romero-Jaine, Breast cancer and lactation history in Mexican women, Am. JEpidemiol. 143 (1996) 543–552.
26] D.B. Kitchen, H. Decornez, J.R. Furr, J. Bajorath, Docking and scor-ing in virtual screening for drug discovery: methods and applications,Nature Rev. Drug Discov. 3 (2004) 935–949.
27] S. Banerjee, M. Dowsett, A. Ashworth, L.-A. Martin, Mechanisms ofdisease: angiogenesis and the management of breast cancer, NatureClin. Pract. Oncol. 4 (2007) 536–550.
28] A.C. Ahn, M. Tewari, C.S. Poon, R.S. Phillips, The limits of reduc-tionism in medicine: could systems biology offer an alternative? PLoSMed. 3 (2006) e208.
29] D. Majumder, A. Mukherjee, Pathophysiologically based logistics forthe treatment of cancer, J. Biol. Syst. 14 (2006) 631–650.
30] D. Majumder, A. Mukherjee, Simulation of drug administration delayin metronomic chemotherapy of cancer due to pathophysiological con-straints, Proc. 1st Int. Conf. Comp. Syst. Biol., Shanghai, China, 2006,pp. 68–73 [presentation details available in the web site: http://life.fudan.edu.cn/ICCSB/pdf/7.22-1050-Abhik%20Mukherjee.pdf].
31] D. Majumder, A. Mukherjee, Mathematical modelling of toxicity-related trade-offs in metronomic chemotherapy, IET Syst. Biol. 1 (2007)298–305.
32] O. Wolkenhauer, Defining systems biology: an engineering perspective,
IET Syst. Biol. 1 (2007) 204–206.33] A. Mukherjee, D. Majumder, Mathematical modelling for the assess-ment of the effect of drug application delays in metronomicchemotherapy of cancer due to physiological constraints, BioSystems91 (2008) 108–116.