Embed Size (px)
Citation preview

R
C
Cdo
SQ1
La
b
c
d
a
ARRA
KCHRS
i
B
(
h0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
ARTICLE IN PRESSG ModelESUS 5989 1–5
Resuscitation xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Resuscitation
j ourna l h o me pa g e : www.elsev ier .com/ locate / resusc i ta t ion
linical paper
ompressions during defibrillator charging shortens shock pauseuration and improves chest compression fraction during shockableut of hospital cardiac arrest�
heldon Cheskesa,b,c,∗, Matthew R. Commonc,d, P. Adam Byersc, Cathy Zhanc,aurie J. Morrisonb,c
Sunnybrook Centre for Prehospital Medicine, Toronto, ON, CanadaUniversity of Toronto, Division of Emergency Medicine, Toronto, ON, CanadaRescu Li Ka Shing Knowledge Institute, St. Michaels Hospital, Toronto, ON, CanadaInstitute of Medical Science, University of Toronto, Toronto, ON, Canada
r t i c l e i n f o
rticle history:eceived 16 January 2014eceived in revised form 8 March 2014ccepted 1 May 2014
eywords:ardiopulmonary resuscitationeart arrestesuscitationurvival
a b s t r a c t
Background: Previous studies have demonstrated significant relationships between shock pause durationand survival to hospital discharge from shockable out-of hospital (OHCA) cardiac arrest. Compressionsduring defibrillator charging (CDC) has been proposed as a technique to shorten shock pause duration.Objective: We sought to determine the impact of CDC on shock pause duration and CPR quality measuresin shockable OHCA.Methods: We performed a retrospective review of all treated adult OHCA occurring over a 1 year periodbeginning August 1, 2011 after training EMS agencies in CDC. We included OHCA patients with an initialshockable rhythm, available CPR process data and shock pause data for up to the first three shocks ofthe resuscitation. CDC by EMS personnel was confirmed by review of impedance channel measures. Weevaluated the relationship between CDC and shock pause duration as the primary outcome measure.Secondary outcome measures investigated the association between CDC and CPR quality measures.Results: Among 747 treated OHCA 149 (23.4%) presented in a shockable rhythm of which 129 (81.6%)met study inclusion criteria. Seventy (54.2%) received CDC. There was no significant difference betweenthe CDC and no CDC group with respect to Utstein variables. Median pre-shock pause (15.0 vs. 3.5 s; �11.5; 95% CI: 6.81, 16.19), post-shock pause (4.0 vs. 3.0 s; � 1.0; 95% CI: −2.57, 4.57), and peri-shockpause (21.0 vs. 9.0 s; � 12.0; 95% CI: 5.03, 18.97) were all lower for those who received CDC. Mean chestcompression fraction was significantly greater (0.77 vs. 0.70, � 0.07; 95% CI: 0.03, 0.11) with CDC. Nosignificant difference was noted in compression rate or depth with CDC. Clinical outcomes did not differbetween the two approaches (return of spontaneous circulation 62.7% vs. 62.9% p = 0.98, survival 25.4%
vs. 27.1% p = 0.82), although the study was not powered to detect clinical outcome differences.Conclusions: Compressions during defibrillator charging may shorten shock pause duration and improveschest compression fraction in shockable OHCA. Given the impact on shock pause duration, further studywith a larger sample size is required to determine the impact of this technique on clinical outcomes fromshockable OHCA.© 2014 Published by Elsevier Ireland Ltd.
Please cite this article in press as: Cheskes S, et al. Compreduration and improves chest compression fraction during shochttp://dx.doi.org/10.1016/j.resuscitation.2014.05.001
� A Spanish translated version of the abstract of this article appears as Appendixn the final online version at http://dx.doi.org/10.1016/j.resuscitation.2014.05.001.∗ Corresponding author at: Sunnybrook Centre for Pre-Hospital Medicine, 77rown’s Line, Suite 100 Toronto, ON, Canada M8W 3S2.
E-mail addresses: [email protected], [email protected]. Cheskes).
ttp://dx.doi.org/10.1016/j.resuscitation.2014.05.001300-9572/© 2014 Published by Elsevier Ireland Ltd.
25
26
27
28
1. Introduction
Survival from out-of-hospital cardiac arrest (OHCA) continuesto challenge Emergency Medical Services (EMS) systems.1–3 Withthe advent of the 2010 American Heart Association-International
ssions during defibrillator charging shortens shock pausekable out of hospital cardiac arrest. Resuscitation (2014),
Liaison Committee on Resuscitation (AHA-ILCOR) guidelines forCardiopulmonary Resuscitation (CPR), interest has focused onimproving survival through improvements in CPR.4,5 Chest com-pression fraction (CCF), compression rate and depth, peri-shock
29
30
31
32

ING ModelR
2 citatio
pbOsnosfApcdscvpNbposC
2
2
t2EP((mtpdCpipoisnZew
cqAHa
3
ardota
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
ARTICLEESUS 5989 1–5
S. Cheskes et al. / Resus
ause duration and chest compression release velocity have alleen associated with improved survival to hospital discharge fromHCA.6–9 Shorter peri-shock pause duration and in particular pre-
hock pause duration have as well been associated with improvedeurological outcome from OHCA.10 Defibrillator mode (automaticr manual mode) is known to have a significant impact on pre-hock pause duration as a result of the mandatory time requiredor both defibrillator analysis and charging in automatic mode.10,11
variety of techniques have been shown to decrease pre-shockause duration when employed by providers in a simulated resus-itation environment.12 Chest compressions performed during theefibrillator charging phase (CDC) is one technique that has beenuggested in an attempt to mitigate the impact of defibrillatorharging time on pre-shock pause duration. Edelson et al.13 pre-iously have demonstrated significant improvements in pre-shockause duration by employing CDC in the inhospital environment.o previous studies have examined the impact of CDC performedy paramedics during OHCA. If CDC consistently shortens pre-shockause duration, it may have significant impact on both terminationf ventricular fibrillation and survival from OHCA. We thereforeought to explore the impact of CDC on shock pause duration andPR quality metrics during shockable OHCA.
. Methods
.1. Setting and design
The study took place in the Regions of Peel and Halton inhe province of Ontario, Canada. The regions cover an area of040 km2 and have a combined population of 1.6 million people.MS responds to a volume of 100,000 emergency calls per year.rehospital medical care is provided by advanced care paramedicsfull advanced life support skills) and primary care paramedicsbasic life support skills with the addition of a small number of
edications and manual defibrillation). Both agencies are part ofhe Resuscitation Outcomes Consortium (ROC), Toronto site, andarticipate in both ROC Epistry14,15 as well as all ROC cardiac ran-omized controlled trials. Since 2006, both agencies have collectedPR process data (chest compression rate, depth, CCF and shockause duration). Training in the technique of CDC occurred dur-
ng both EMS services’ continuing medical education immediatelyrior to the study start date of August 1, 2011. Training consistedf both didactic classroom instruction on the importance of min-mizing peri-shock pause duration and practical manikin-basedcenario training where paramedics learned to apply the CDC tech-ique during each shock delivered in a cardiac arrest resuscitation.oll E series defibrillators (Zoll Medical, Chelmsford, MA, USA) weremployed during the study period with no change in either hard-are or software configuration.
This study consisted of a retrospective review of prospectivelyollected data on the impact of CDC on shock pause duration, CPRuality metrics and clinical outcomes for a 1 year period beginningugust 1, 2011. The protocol was approved by the St. Michael’sospital Research Ethics Board (REB) as an amendment to eachgency’s pre-existing ROC REB approval.
. Study population
Patients eligible for this study included those 18 years of agend older who sustained non-traumatic OHCA with a first EMShythm of ventricular fibrillation or pulseless ventricular tachycar-
Please cite this article in press as: Cheskes S, et al. Comprduration and improves chest compression fraction during shochttp://dx.doi.org/10.1016/j.resuscitation.2014.05.001
ia (VF/VT) for which CPR process data for at least one shock wasbtained. The initial rhythm was determined to be VF/VT if the ini-ial rhythm was interpreted as VF/VT by the initial EMS providernd a shock was provided. Patients were excluded if they received
PRESSn xxx (2014) xxx–xxx
public access defibrillation before EMS arrival, or if their arrest waswitnessed by EMS.
4. Measurement
CPR process data from all eligible resuscitations were reviewedand assessed for duration of pre- and post-shock pauses, CCF, com-pression rate and compression depth up to and including onlythe third shock, to minimize confounding by other resuscitationinterventions (intubation, intravenous epinephrine or intravenousantiarrythmics). Pre-shock pause was defined as the time inter-val between chest compression cessation (as detected in theimpedance channel waveform) and shock delivery. Post-shockpause was defined as the time between shock delivery and chestcompression resumption (as detected in the impedance channelwaveform). Peri-shock pause was defined as the total of the pre-and post-shock pause time. CCF was defined as the proportionof time spent performing chest compressions during which thepatient was without spontaneous circulation.
All resuscitations were assessed for the presence or absenceof CDC. If chest compressions were clearly noted during the defi-brillator charging phase then the individual shock was noted tohave CDC. Resuscitations were either classified as CDC, if >50%of shocks delivered during a resuscitation demonstrated CDC, ornon-CDC if they did not. All resuscitations were assessed by twoinvestigators to ensure uniform classification with respect to thepresence or absence of CDC. The primary outcome measure wasthe relationship between CDC and shock pause duration. Secondaryoutcome measures investigated the association between CDC andCPR quality metrics (CCF, compression rate, compression depth).The relationship between CDC and clinical outcomes of return ofspontaneous circulation (ROSC) and survival to hospital dischargewere also examined.
5. Statistical analysis
Descriptive statistics were used to assess whether baselinecharacteristics remained consistent across study cohorts (CDC andnon-CDC). The relationship between CDC and all outcome meas-ures (median shock pause duration, CPR quality metrics, ROSC, andsurvival to hospital discharge) was calculated by univariate regres-sion analysis using a chi-squared test. To ensure our findings wererobust and not cofounded by the limitation of our analysis to thefirst three shocks of each resuscitation, we performed a secondaryper shock analysis on all shocks administered during the studyperiod to assess the association between shock pause duration andCDC. Study data management and storage was accomplished usingMicrosoft SQL Server 2008 (v.10.0.5848.0, Microsoft Corporation,Redmond, WA, USA), while statistical analysis was performed withSAS (v.9.3, SAS, Cary, NC, USA).
6. Results
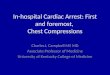
Fig. 1 displays a CONSORT diagram of all cases included in thestudy. Of 747 treated, unwitnessed cardiac arrest resuscitations,20% had an initial arrest rhythm of VF/VT. Of those 149, CPR processdata was missing on 20 cases leaving 129 for analysis. Seventy (54%)of these cases were identified as CDC cases.
Table 1 compares the baseline characteristics of both studycohorts. No significant differences in Utstein variables or resusci-tation duration were noted between the two cohorts. Shocks per
essions during defibrillator charging shortens shock pausekable out of hospital cardiac arrest. Resuscitation (2014),
resuscitation and percent of shocks (first three) receiving CDC weresignificantly greater in the CDC then non CDC group.
Table 2 displays the association between CDC and median shockpause duration at the patient level (patients categorized as CDC or
148
149
150
151
ARTICLE IN PRESSG ModelRESUS 5989 1–5
S. Cheskes et al. / Resuscitation xxx (2014) xxx–xxx 3
Fig. 1. Consort diagram of study cohort.
Table 1Study population baseline characteristics.
No CDC CDC p
n 59 70Age (mean) [year] 63.78 64.47 0.79Male [%] 77.97 74.29 0.63Public Location [%] 30.51 32.86 0.78Bystander witnessed [%] 71.19 70.00 0.89Bystander CPR [%] 50.85 52.86 0.82Response time (median) [min] 5.42 5.20 0.26Resuscitation duration (median) [min] 20.90 23.55 0.29Shocks per resuscitation (mean) 3.14 4.79 0.005First three shocks receiving CDC [%] 0.056 0.78 <0.001
CDC = compressions during charging; min = minutes.
Table 2Patient based univariate analysis of the impact of compressions during defibrillatorcharging on median shock pause duration.
No CDC CDC p value Difference 95% CI
Pre-shock pause (s) 15.0 3.5 <0.001 11.5 (6.81, 16.19)Post-shock pause (s) 4.0 3.0 0.11 1.0 (−2.57, 4.57)Peri-shock pause (s) 21.0 9.0 <0.001 12.0 (5.03, 18.97)
C
nmctSp
psabsts8
Table 3Shock based univariate analysis of the impact of compressions during defibrillatorcharging on median shock pause duration.
Non-CDC CDC p Difference 95% CI
n 314 159Pre-shock pause (s) 16 3 <0.001 13 (10.57, 15.43)Post-shock pause (s) 4 3 0.09 1(−0.68, 2.68)Peri-shock pause (s) 21 7 <0.001 14 (10.49, 17.51)
CDC = compressions during charging; s = seconds.
0
5
10
15
20
25
30
35
40
45
50
0 0.2 0. 4 0.6 0. 8 1
Shoc
k Pa
use
dura
�on
[s]
% of shocks wit h CD C
Pre-Shock
Peri-Sh ock
Post-Shock
on a patient based or shock based analysis. As expected, there
TUh
C
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
DC = compressions during charging; s = seconds.
on CDC). Median values in the table represent the median of theedian individual case shock durations for all CDC and non-CDC
ases. Significant reductions in pre and peri-shock pause dura-ions were noted for CDC cases when compared with non-CDC.pecifically CDC cases demonstrated reductions in pre-, post- anderi-shock pause durations of 77%, 25% and 57% respectively.
Table 3 displays the association between CDC and median shockause duration incorporating all shocks administered during thetudy. In contrast to Table 2 this represents a shock based analysiss opposed to a patient based analysis of CDC. Similar to our patientased analysis, significant reductions were noted in pre- and peri-hock pause durations for shocks in which CDC occurred as opposedo shocks where CDC did not occur. Specifically CDC shocks demon-
Please cite this article in press as: Cheskes S, et al. Compreduration and improves chest compression fraction during shochttp://dx.doi.org/10.1016/j.resuscitation.2014.05.001
trated reductions in pre-, post- and peri-shock pause durations of1%, 25% and 67% when compared to non CDC shocks.
able 4nivariate analysis of impact of compressions during defibrillator charging on CPR qualityospital discharge.
No CDC C
Number of cases 59
CPR fraction 0.71
Compression depth (cm) 5.03
Compression rate (per min) 104.57 1ROSC 62.7%
Survival to hospital discharge 25.4%
DC = compressions during charging; CPR = cardiopulmonary resuscitation; ROSC = return
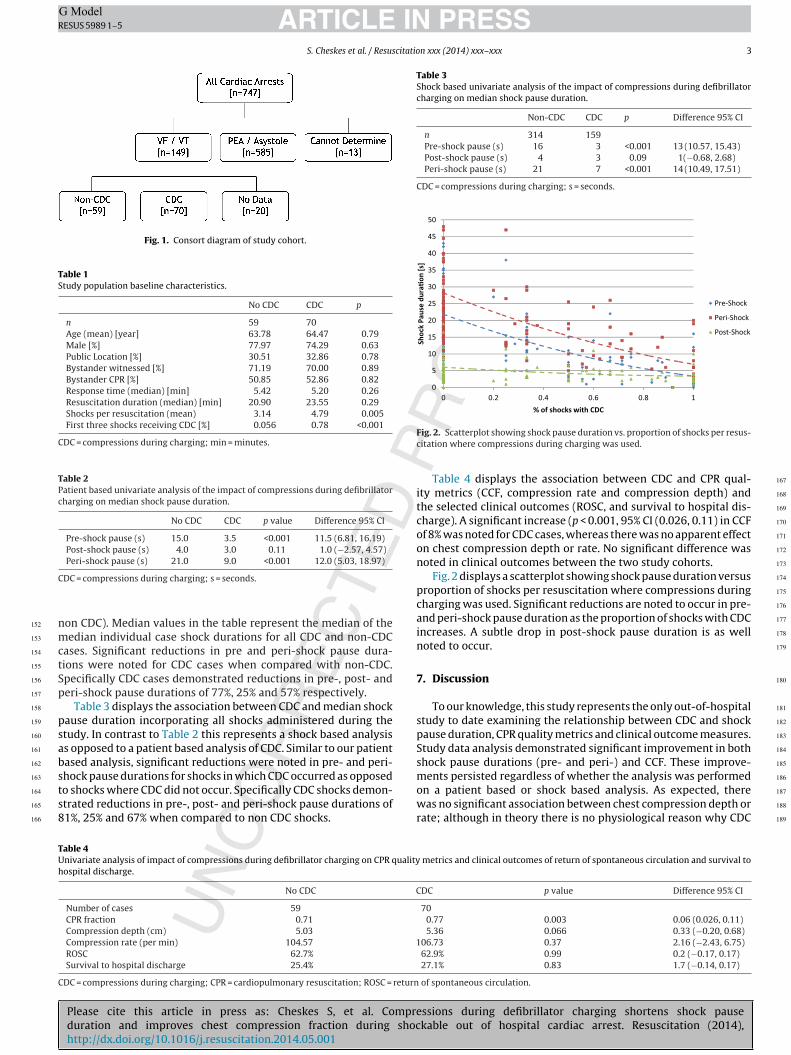
Fig. 2. Scatterplot showing shock pause duration vs. proportion of shocks per resus-citation where compressions during charging was used.
Table 4 displays the association between CDC and CPR qual-ity metrics (CCF, compression rate and compression depth) andthe selected clinical outcomes (ROSC, and survival to hospital dis-charge). A significant increase (p < 0.001, 95% CI (0.026, 0.11) in CCFof 8% was noted for CDC cases, whereas there was no apparent effecton chest compression depth or rate. No significant difference wasnoted in clinical outcomes between the two study cohorts.
Fig. 2 displays a scatterplot showing shock pause duration versusproportion of shocks per resuscitation where compressions duringcharging was used. Significant reductions are noted to occur in pre-and peri-shock pause duration as the proportion of shocks with CDCincreases. A subtle drop in post-shock pause duration is as wellnoted to occur.
7. Discussion
To our knowledge, this study represents the only out-of-hospitalstudy to date examining the relationship between CDC and shockpause duration, CPR quality metrics and clinical outcome measures.Study data analysis demonstrated significant improvement in bothshock pause durations (pre- and peri-) and CCF. These improve-ments persisted regardless of whether the analysis was performed
ssions during defibrillator charging shortens shock pausekable out of hospital cardiac arrest. Resuscitation (2014),
was no significant association between chest compression depth orrate; although in theory there is no physiological reason why CDC
metrics and clinical outcomes of return of spontaneous circulation and survival to
DC p value Difference 95% CI
700.77 0.003 0.06 (0.026, 0.11)5.36 0.066 0.33 (−0.20, 0.68)
06.73 0.37 2.16 (−2.43, 6.75)62.9% 0.99 0.2 (−0.17, 0.17)27.1% 0.83 1.7 (−0.14, 0.17)
of spontaneous circulation.
188
189

ING ModelR
4 citatio
siaopliitdpRpqtwespeitr
wcc2ttbpppRpp
inatbrloa
ucCoaiFmpdod
hsbnd
Q2
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
ARTICLEESUS 5989 1–5
S. Cheskes et al. / Resus
hould impact these two variables. CDC, when performed properlyntuitively would decrease pre-shock and peri-shock interval yetn improvement in post-shock pause duration was also noted. It isur belief that paramedics who are focused on improving shockause duration and CPR quality by implementing interventions
ike CDC may be more focused on the importance of minimizingnterruptions during CPR, which may account for the benefit seenn post-shock pause duration in the cohort receiving CDC. Givenhe previously demonstrated associations between shock pauseuration, CCF and survival to hospital discharge8,10 it would seemlausible that CDC may impact critical clinical outcomes such asOSC and survival to hospital discharge. Unfortunately the sam-le size of our study was insufficient to adequately address thisuestion. Assuming an absolute improvement in survival of 5% inhe CDC cohort, a sample size of 2500 cases (alpha 5%, power 80%)ould be required to adequately power the study to detect differ-
nces in clinical outcomes. Due to the magnitude of the proposedample size, a large multi-center trial would be required. Based onrevious research demonstrating a reduction in survival of 7% forach 5 increase in pre-shock pause10, our findings of a 13 s decreasen median pre-shock pause by employing CDC has the potentialo improve survival by 18%. Few interventions in cardiac arrestesuscitation have the potential to improve survival by this degree.
Our findings are consistent with the findings of Edelson et al.13
ho were able to demonstrate that rescuer performance of chestompressions during the defibrillator “charging phase” signifi-antly lowered pre-shock pause intervals to less than 3 s (median.6 s; IQR: 1.9, 3.8). The improvement in pre-shock pause noted inhe Edelson study of 80% (13.3–2.6 s) was somewhat greater thanhe 64% improvement noted in our study and may be explainedy the lack of “run in” period after training for our paramedicroviders. Sell et al.16 discovered a significant relationship betweenre- and post-shock pause durations and the likelihood of ROSC inatients presenting in VF in a small study of OHCA resuscitations.eceiver–operator curves demonstrated an optimal pre-shockause duration of 2.3 s, which was only achievable by providerserforming CDC.
Defibrillator mode has long been noted to have a significantmpact on shock pause duration particularly automated exter-al defibrillators (AED). The mandatory time required for rhythmnalysis and defibrillator charging have been known to have a dele-erious impact on pre-shock pause duration.9–11,17 While CDC haseen shown to decrease pre-shock pause in AED mode, similaresults can be obtained by pre-charging the manual mode defibril-ator (pressing the defibrillator charge button prior to completionf the CPR cycle) thereby eliminating the defibrillator charge timefter rhythm assessment.12,13
Technological advances in defibrillator software which allowsnderlying rhythm analysis during CPR as well as defibrillatorharging and delivery of a shock immediately at the end of thePR interval could significantly decrease pre-shock pause intervalsbviating the need for CDC.18,19 Similarly, improved algorithmsllowing for earlier detection of shockable rhythms while work-ng in automated mode could also decrease pre-shock pause time.inally a new paradigm in defibrillator software voice promptsay exist particularly when providers work in AED mode. Voice
rompts have classically been programmed to state “Stop CPR”uring automatic defibrillator analysis and charging phase. Givenur study findings voice prompts stating “Continue CPR” duringefibrillator charging may be appropriate.
CDC and the quest for the shortest possible pre-shock pauseave raised concerns surrounding provider safety (inadvertent
Please cite this article in press as: Cheskes S, et al. Comprduration and improves chest compression fraction during shochttp://dx.doi.org/10.1016/j.resuscitation.2014.05.001
hock of provider performing compressions). A systematic reviewy Hoke et al.20 failed to substantiate these concerns. A very smallumber (15) of adverse events involving unintentional shockselivered to rescuers have been reported in this review since the
PRESSn xxx (2014) xxx–xxx
advent of widespread defibrillator use by medical personnel. Symp-toms consisting of tingling sensations, discomfort, and minor burnswere most common; in no case were any long term effects reported.Similarly Edelson et al.13 only noted one case of inadvertent shockadministration with no untoward effects. Our providers wore latexgloves during resuscitations and we are unaware of any incidentsof unintentional shock of providers during the study period.
Recent animal models and human feasibility models havedemonstrated the potential benefit and safety of completely elim-inating shock pauses via “hands on defibrillation”.21,22 Given thesurvival benefit to shortening pre-shock pause, further studyappears warranted to determine whether any survival benefitexists between a short pre-shock pause strategy using CDC and ano shock pause or “hands on defibrillation” strategy.
Our study has several limitations. After training in the techniqueof CDC only 54 percent of paramedics performed CDC during thestudy period. As the study period progressed, the proportion of CDCcases increased, indicating that providers were either becomingmore comfortable using the technique, or becoming more effectivein its application. We believe this trend may have been eliminatedby allowing a “run in” period for providers to get used to the tech-nique and maximize its use. Additionally, despite our training ofCDC to minimize pre-shock pause, some providers may have bal-anced the need to perform CDC to eliminate pre-shock pause witha concomitant concern of provider safety. Our decision to minimizedownstream resuscitation confounding (intubation, antiarrythmicuse, epinephrine use, in hospital care) by limiting our analysis toonly the first three shocks may have impacted the total numberof cases available by excluding shock pause intervals in prolongedresuscitations. The findings of our secondary shock based analy-sis employing all shocks provided during the study suggests thatour findings are in fact not confounded by limiting shock num-ber. Our study sample size was impacted by the relatively low rate(20%) of VF/VT in our study population. Our data is abstracted froman observational registry and as such we can only demonstrate anassociation between CDC performance and shock pause durationrather than a causal relationship. Lastly, the study took place inregions with high performing and heavily monitored EMS systemswith rapid response times and overall high CPR quality. The applica-bility of our findings to other EMS systems without similar systemresponse optimization and CPR quality characteristics is uncertain.
8. Conclusion
Compressions during defibrillator charging may shorten shockpause duration and improves chest compression fraction in shock-able OHCA. Further study with a larger sample size is required todetermine the impact of this technique on clinical outcomes fromshockable OHCA.
Conflict of interest statement
Dr. Cheskes has received speaking honorarium from Zoll Med-ical. Dr. Cheskes has received grant funding as Co PI, Toronto site,Resuscitation Outcomes Consortium. Dr. Morrison has receivedgrant funding as PI, Toronto site, Resuscitation Outcomes Consor-tium. No other grant disclosures.
Acknowledgements
essions during defibrillator charging shortens shock pausekable out of hospital cardiac arrest. Resuscitation (2014),
We would like to acknowledge the hard work and dedicationof all paramedics of both the Region of Peel Paramedic Serviceand Halton EMS. Research in the pre-hospital setting would notbe possible without the tireless efforts of their paramedics.
310
311
312
313
ING ModelR
citatio
R
1
1
1
1
1
1
1
1
1
1
2
2
resuscitation and is safe for rescuers – a preclinical study. J Am Heart Assoc2012;1:e001313.
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
ARTICLEESUS 5989 1–5
S. Cheskes et al. / Resus
eferences
1. Sans S, Kesteloot H, Kromhout D. Task force of the European Society of Cardiologyon Cardiovascular Morbidity and Mortality Statistics in Europe. The burden ofcardiovascular diseases mortality in Europe. Eur Heart J 1997;18:1231–48.
2. Becker LB, Ostrander MP, Barret J, Kondos GT. Outcome of CPR in a largemetropolitan area: where are the survivors? Ann Emerg Med 1991;20:355–61.
3. Nichol G, Thomas E, Callaway CW, et al. Resuscitation outcomes consortiuminvestigators regional variation in out-of-hospital cardiac arrest incidence andoutcome. JAMA 2008;300:1423–31.
4. Nadkami VM, Nolan JP, Billi JE, et al. Part 2: international collaboration in resusci-tation science: 2010 international consensus on cardiopulmonary resuscitationand emergency cardiovascular care science with treatment recommendations.Circulation 2010;122:S276–82.
5. Ornato JP, Peberdy MA. Measuring progress in resusciation: it’s time for a bettertool. Circulation 2006;114:2754–6.
6. Stiell IG, Brown SP, Christenson J, Cheskes S, et al. What is the role of chestcompression depth during out-of-hospital cardiac arrest resuscitation? Crit CareMed 2012;40:1192–8.
7. Idris AH, Guffey D, Aufderheide TP, et al. Relationship between chest compres-sion rates and outcomes from cardiac arrest/clinical perspective. Circulation2012;125:3004–12.
8. Christenson J, Andrusiek D, Everson-Stewart S, et al. Chest compression frac-tion determines survival in patients with out-of-hospital ventricular fibrillation.Circulation 2009;120:1241–7.
9. Cheskes S, Schmicker RH, Christenson J, et al. Peri-shock pause: an independentpredictor of survival from out-of-hospital shockable cardiac arrest. Circulation2011;124:58–66.
0. Cheskes S, Schmiker RH, Verbeek PR, et al. The impact of peri-shock pause onsurvival from out-of-hospital shockable cardiac arrest during the ROC PRIMED
Please cite this article in press as: Cheskes S, et al. Compreduration and improves chest compression fraction during shochttp://dx.doi.org/10.1016/j.resuscitation.2014.05.001
trial. Resuscitation http://dx.doi.org/10.1016/j.resuscitation.2013.10.0141. Snyder D, Morgan C. Wide variation in cardiopulmonary resuscitation
interruption intervals among commercially available automated external defib-rillators may affect survival despite high defibrillation efficacy. Crit Care Med2004;32:S421–4.
2
PRESSn xxx (2014) xxx–xxx 5
2. Thim T, Grove EL, Lofgren B. Charging the defibrillator before rhythm checkreduces hands-off time during CPR: a randomised simulation study. Resuscita-tion 2012;83:e210–1.
3. Edelson DP, Robertson-Dick BJ, Yuen TC, et al. Safety and efficacy of defibrillatorcharging during ongoing chest compressions: a multi-center study. Resuscita-tion 2010;81:1521–6.
4. Davis DP, Garberson LA, Andrusiek DL, et al. A descriptive analysis of emergencymedical services participating in the resuscitation outcomes consortium (ROC)network. Prehosp Emerg care 2007;11:369–82.
5. Morrison LJ, Nichol G, Rea TD, et al. Rationale, development and implementationof the resuscitation outcomes consortium epistry-cardiac arrest. Resuscitation2008;78:161–9.
6. Sell RE, Sarno R, Lawrence B, et al. Minimizing pre- and post-defibrillation pausesincreases the likelihood of return of spontaneous circulation (ROSC). Resuscita-tion 2010;81:822–5.
7. Tomkins WG, Swain AH, Bailey M, Larsen PD. Beyond the pre-shock pause:the effect of prehospital defibrillation mode on CPR interruptions and returnof spontaneous circulation. Resuscitation 2013;81:343–7.
8. Barash DM, Raymond RP, Tang Q, Silver AE. A new defibrillator mode to reducechest compression interruptions for health care professionals and lay rescuers:a pilot study in manikins. Prehosp Emerg Care 2011;15:88–97.
9. Silver A, Partridge R. Length of chest compression pauses is reduced with cardiacrhythm analysis and charging during chest compressions. Prehosp Emerg Care2014;18:123 [abstract].
0. Hoke RS, Heinroth K, Trappe HJ, Werdan K. Is external defibrillation an electricthreat for bystanders? Resuscitation 2009;80:395–401.
1. Neumann T, Gruenewald M, Lauenstein C, Drews T, Iden T, Meybohm P. Hands-on defibrillation has the potential to improve the quality of cardiopulmonary
ssions during defibrillator charging shortens shock pausekable out of hospital cardiac arrest. Resuscitation (2014),
2. Lloyd MS, Heeke B, Walter PF, Langberg JJ. Hands-on defibrillation: an analysisof electrical current flow through rescuers in direct contact with patients duringbiphasic external defibrillation. Circulation 2008;117:2510–4.
377
378
379