Embed Size (px)
Citation preview

CA
SE
RE
PO
RT
Case Report
Compression of Trachea due to Double Aortic Arch:Demonstration by Multi-slice CT Scan (MSCT)
Charanjeet Singh, MD ∗, Mamta Gupta, DMRD and Sanjiv Sharma, MDDepartment of Cardiac and Interventional Radiology, Cardio-Thoracic and Neuro-Sciences Centre,
All India Institute of Medical Sciences, New Delhi, India
Double aortic arch (DAA) is a form of vascular ring, completely encircling trachea and esophagus by its connectingsegments, and thus can lead to clinical picture of aero-digestive tract obstruction. MRI and CECT in addition to the locationand extent of aero-digestive tract obstruction can also delineate adjacent cardio-vascular anatomy. 3D reconstruction ofaorta and airway can be useful tool for pre-operative planning.
(Heart, Lung and Circulation 2006;15:332–333)© 2006 Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society of Australia and
New Zealand. Published by Elsevier Inc. All rights reserved.
Keywords. Double aortic arch; Tracheal compression; Vascular ring and multi-slice CT scan
D
ouble aortic arch (DAA) is a form of vascular rings,completely encircling trachea and esophagus by itsconnecting segments. DAA was first described by Hom-mel in 1737.1 Right or left arch may be larger or similar
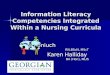
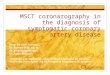
Figure 1. Multi-planer reconstruction (coronal view) of contrastenhanced multi-slice CT scan revealed separate right and left aortic
in size, or one arch can be atretic. In more than 75% ofcases, right arch is dominant. During embryogenesis apatterned regression and persistence of various vascularstructures occurs ultimately resulting in normal, mature
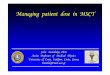
arches (Arrows). The trachea and esophagus are surrounded by thevascular ring made by DAA. The trachea is slightly compressed by thevascular ring (*), from right side. ASC.AO indicates the ascending Figure 2. 3D-volume rendered image of the contrast enhanced
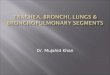
aortic arch. Volume rendered airway tract (trachea and both principalbronchi, marked as (*)) superimposed, to show their relationship withmediastinal sturctures. Small arrows indicate right and left arches. DAindicates descending aorta.
ons and the Cardiac Society ofl rights reserved.
1443-9506/04/$30.00doi:10.1016/j.hlc.2006.02.006
aorta; RA indicates right atrium and LV indicates left ventricle.
Received 1 September 2005; received in revised form 19 December2005; accepted 5 February 2006; available online 17 April 2006
∗ Corresponding author. Fax: +91 11 26588122.E-mail addresses: [email protected], [email protected](C. Singh).
© 2006 Australasian Society of Cardiac and Thoracic SurgeAustralia and New Zealand. Published by Elsevier Inc. Al
multi-slice CT scan from the top view. The right subclavian artery(RSCA) and right common carotid artery (RCCA) originatedseparately from the right aortic arch, and the left subclavian artery(LSCA) and left common carotid artery (LCCA) originated from the left

CA
SE
RE
PO
RT
Heart, Lung and Circulation Singh et al. 3332006;15:332–333 Compression of trachea due to double aortic arch: Demonstration by multi-slice CT scan (MSCT)
configuration of the aorta and its branches. Both fourtharches and both dorsal aortas remain present, to formDAA. On chest X-ray, lateral indentation of tracheal aircolumn may be revealed in AP or PA view, usually in both.MRI and CECT in addition to location and extent of air-way obstruction, also delineate cardiac anatomy. Threedimensional (3D) reconstruction of aorta and airway canbe useful tool for pre-operative planning.2
A 5-year-old girl, a known case of isolated VSD pre-sented with recurrent respiratory tract infections and fea-tures of air trapment. She underwent contrast enhancedmulti-slice computed tomography (MSCT) (Sensation 16,Siemens, Germany), 2 ml/kg body weight iodinated non-ionic contrast was injected, using pressure injector. Axialsource images, multi-planner reconstruction in coronalplane and volume rendered images revealed separate
right and left aortic arches, surrounding trachea andesophagus. Right sided arch was causing slight compres-sion over trachea. Right subclavian and right commoncarotid arteries originated separately from right aortic archand left subclavian and left common carotid arteries orig-inated from left aortic arch (Figs. 1 and 2).
References
1. Moes CAF. Vascular rings and anomalies of the aortic arch. In:Keith JD, Rowe RD, Vlad P, editors. Heart disease in infancy andchildhood. New York: Macmillan; 1978. p. 856–81.
2. Colin J, McMohan, Louis I, Bezold, Giles W, Vick III. Doubleaortic arch in D-transposition of the great arteries, confirmationof double aortic arch by magnetic resonance imaging. Tex HeartInst J 2000;27:398–400.