Embed Size (px)
Citation preview
Comprehensive Medication Assisted Treatment
Presented by: Michael Weaver, MD and Don Hall, LCDC
April 25, 2018

Thomas Durham, PhD
Director of Training
NAADAC, the Association for Addiction Professionals
www.naadac.org
Produced By
NAADAC, the Association for Addiction Professionalswww.naadac.org/webinars

www.naadac.org/webinars
www.naadac.org/comprehensive-MAT-webinar

Cost to Watch:
Free
CE Hours
Available:
1.5 CEs
CE Certificate for
NAADAC
Members:
Free
CE Certificate for
Non-members:
$20
To obtain a CE Certificate for the time you spent watching this
webinar:
1. Watch and listen to this entire webinar.
2. Pass the online CE quiz, which is posted at
www.naadac.org/comprehensive-MAT-webinar
3. If applicable, submit payment for CE certificate or join
NAADAC.
4. A CE certificate will be emailed to you within 21 days of
submitting the quiz.
CE Certificate
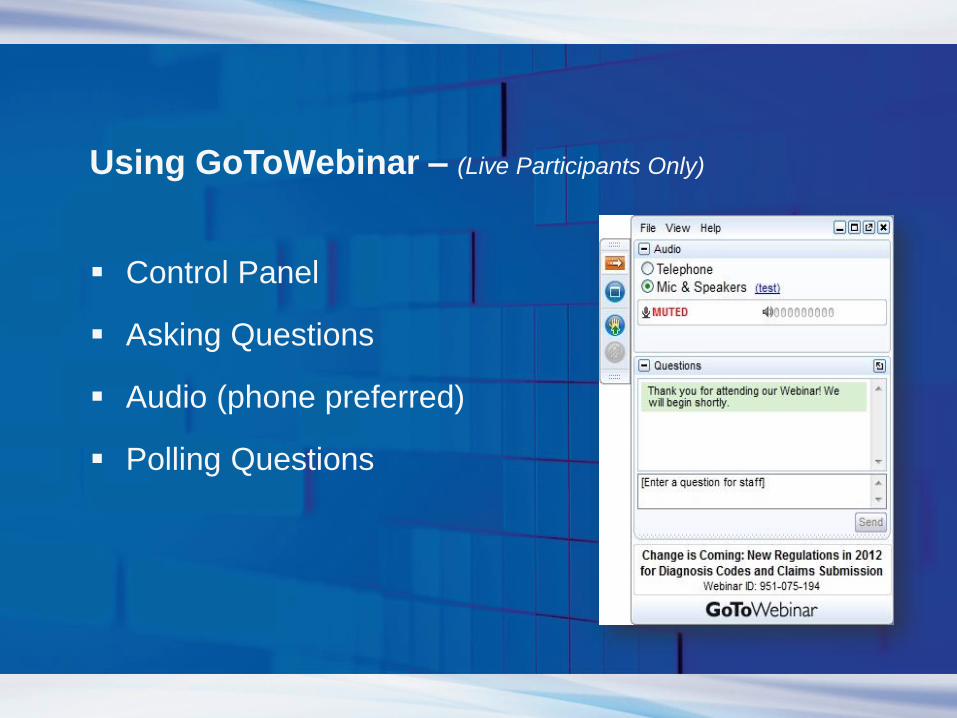
Using GoToWebinar – (Live Participants Only)
Control Panel
Asking Questions
Audio (phone preferred)
Polling Questions
Webinar PresentersYour
Michael Weaver, MD, DFASAM
Professor & Medical Director,
Center for Neurobehavioral Research on
Addiction
UTHealth McGovern Medical School
Don Hall LCDC, CPT
Adult Rehabilitation Services, SEARCH

Webinar Learning Objectives
LO #1 Recognize
how long-term
pharmacotherapy
fits into the context
of overall addiction
treatment.
LO #2 Describe types
of pharmacotherapy
for smoking cessation,
alcohol dependence,
and opioid addiction.
LO #3 Learn tasks
specific to working with
Medication Assisted
Treatment clients.
1 32
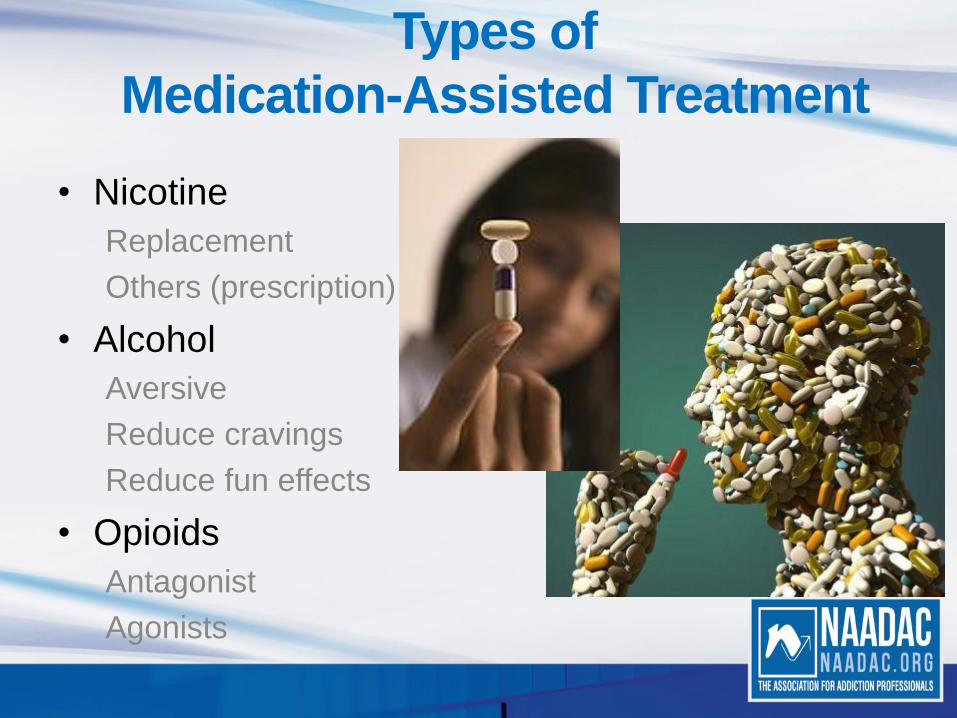
• Nicotine
Replacement
Others (prescription)
• Alcohol
Aversive
Reduce cravings
Reduce fun effects
• Opioids
Antagonist
Agonists
Types of
Medication-Assisted Treatment

• Always combine with a
behavioral therapy
program
• Most available OTC,
but all are expensive
• Reduces harmful
effects of tobacco
smoking
• Patients should not
smoke while using
Nicotine Replacement
Therapy

• There have been many studies
and several meta-analyses of all
products
• Nicotine replacement therapy quit
rates are similar with different
products
Doubles chance of successful
quitting
• Combinations are more effective
than a single product at a time
Efficacy of Tobacco
Cessation Products
• Varenicline
• Higher rate of continuous
tobacco abstinence compared
to bupropion & nicotine patch
• Bupropion
• Quit rates are comparable to
nicotine patch

• Disulfiram (Antabuse) Alcohol antagonist, person will get ill if they drink while it is in their system. Often used as aversion therapy.
• Acamprosate (Campral) prescribed with counseling and therapy. Mechanism is not fully understood.
• Naltrexone (ReVia, Vivitrol) as used in the Sinclair method was shown to reduce levels of abusive drinking by 70 – 80% over time.
Pharmacotherapy for
Alcohol Dependence
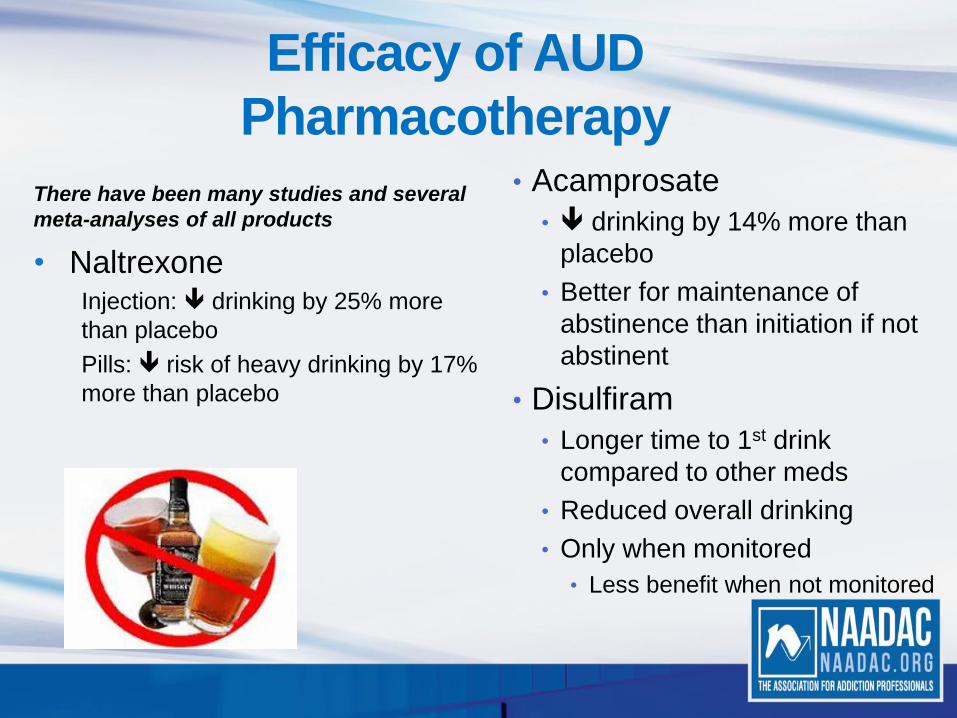
There have been many studies and several
meta-analyses of all products
• NaltrexoneInjection: drinking by 25% more
than placebo
Pills: risk of heavy drinking by 17%
more than placebo
Efficacy of AUD
Pharmacotherapy• Acamprosate
• drinking by 14% more than
placebo
• Better for maintenance of
abstinence than initiation if not
abstinent
• Disulfiram
• Longer time to 1st drink
compared to other meds
• Reduced overall drinking
• Only when monitored
• Less benefit when not monitored

Depo-Naltrexone
and Alcohol Use Disorder

Antagonist
maintenance◦Naltrexone
Opioid maintenance◦Methadone
◦Buprenorphine
Opioid Addiction Treatments

Part of comprehensive
plan that addresses
psychological, social, &
spiritual needs
Do not use in place of
counseling
Works best in combination
with psychosocial support
Clinical Use of
Pharmacotherapy
• Medication must be taken
consistently to be effective
• Challenging with long-term
pharmacotherapy for
addiction
Many are not immediately
rewarding
• Requires sustained
motivation
Counselors and advocates help
with this
Adherence
• Enhanced recovery
• Reduced mortality70% reduction
Overdose
Trauma
Homicide
Medical illnesses
• Improved healthMedical
Psychiatric
• Improved psychosocial functioningEmployment
Criminal activity
Family responsibilities
Beneficial Effects
If heroin had a warning label…

• Duration of most long-
term pharmacotherapy is
not indefinite
Months to years
• Goal is stabilization
Flexibility
Individualized
Allow for relapse
What is the Endpoint?
• Opioid substitution therapy• Long-acting medication in controlled
settingCounselingSocial services
• Avoid withdrawal & craving
• Harm reductionIndividualSociety
• Single daily dose of the long-acting opioid in a controlled setting
• Highly regulatedNarcotic treatment programs must be licensed
Methadone
Efficacy of Methadone
• There have been many
studies and several meta-
analyses
• Maintenance superior to
detox
• Higher doses (80-100
mg/day) superior to lower
doses (50 mg/d)
• illicit opioid use
• retention in treatment

Buprenorphine
• Alternative to methadone for opioid addiction treatment
• Long-acting opioid agonist-antagonist
• Multiple forms available• Combined with naloxone
(Suboxone, Zubsolv, Bunavail)
• Buprenorphine only (Subutex)
• Detox or maintenance

Efficacy of Buprenorphine• Multiple studies and meta-analyses
• Higher doses (12-16 mg/day) superior to lower doses (6-8 mg/d) to illicit opioid use
• Longer duration of treatment always has superior outcomes to shorter duration
• Few serious adverse events
Methadone or Buprenorphine?
• Treatment efficacy equivalent
• Similar opioid side effects
• Abuse potential• Slightly higher for buprenorphine in opioid non-dependent persons
• Buprenorphine has fewer drug interactions
• Methadone has no ceiling effect
• Buprenorphine more convenient (less restricted)
• Methadone less expensive• Higher cost of buprenorphine, counseling separate cost
• Buprenorphine not age-restricted (can use in teens)
• Individual decision
Methadone or Buprenorphine?
• How “hardcore” a user was the person?
• What is the person’s history with either medication?
• Financial resources
• Time resources
• Buprenorphine is not FDA approved for pregnant women
at this time.
• Person’s attitude toward MAT.
• Family support for MAT.
• Other medical provider’s support for MAT.

MAT Medication Options
For more information, see SAMHSA’s online Decisions in Recovery tool available here:
http://archive.samhsa.gov/MAT-Decisions-in-Recovery/section/whether.aspx
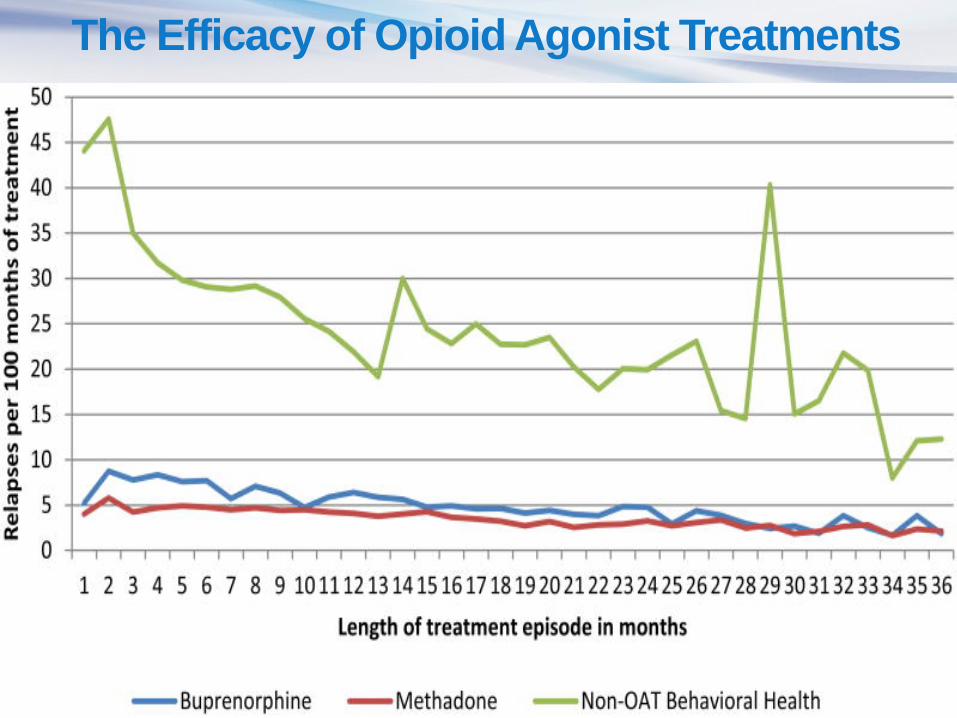
The Efficacy of Opioid Agonist Treatments

Recovery: A process of change through which
individuals improve their health and wellness, live a self-directed life, and strive to reach their full potential.
Health: Overcoming or managing one’s disease(s)
as well as living in a physically and emotionally healthy way.
Home: A stable and safe place to live.
Purpose: Meaningful daily activities, such as a job,
school, volunteerism, family care taking, or creative endeavors, and the independence, income, and resources to participate in society.
Community: Relationships and social
networks that provide support, friendship, love, and hope.

Medication Assisted Treatment
Medication-assisted treatment is the use of medications,
in combination with
counseling and behavioral
therapies, to provide a whole-patient approach to the treatment of
substance use disorders.

Medication-assisted
treatment for opiate
addiction reflects many
elements of the chronic
care treatment model.
How MAT Fits in
Person in Recovery
An individual can be considered a person in
recovery (PIR) if free from other drugs and non-prescribed medications while participating in MAT (now often referred to as
Medication-Assisted Recovery (MAR).
Recovery Management
• First, recovery management will intensify pre-treatment recovery support services to strengthen the engagement process, enhance motivation for change, and remove environmental obstacles
• Second, recovery management will intensify in-treatment recovery support services to enhance treatment retention and effects.
• Third, recovery management will shift the focus of treatment from acute stabilization to support for long-term recovery maintenance.

Recovery Capital
• Granfield and Cloud (1999) defined recovery capital as “.... the breadth and depth of internal and external resources that can help initiate and sustain recovery from substance use problems”.
• Cloud and Granfield(2009) recently revisited their initial concept and have argued that there are four components to recovery capital:
1 Social capital is defined as the sum of resources that each person has as a result of
their relationships, and includes both support from and obligations to groups to which they belong; thus,
family membership provides supports but will also entail commitments and obligations to the other
family members.
2 Physical capital is defined in terms of tangible assets such as property and money
that may increase recovery options (e.g. being able to move away from existing friends/networks or to
afford an expensive detox service).
3 Human capital includes skills, positive health, aspirations and hopes, and personal
resources that will enable the individual to prosper. Traditionally, high educational attainment and high
intelligence have been regarded as key aspects of human capital, and will help with some of the
problem solving that is required on a recovery journey.
4 Cultural capital includes the values, beliefs and attitudes that link to social
conformity and the ability to fit into dominant social behaviors.
Types of Recovery Capital

Recovery Planning
PIR should be supported in the development of a recovery plan attending to
the four dimensions of wellness and recovery:
- Health: Overcoming or managing one’s disease(s) as well as living
in a physically and emotionally healthy way.
- Home: A stable and safe place to live.
- Purpose: Meaningful daily activities, such as a job, school,
volunteerism, family care taking, or creative endeavors, and the
independence, income, and resources to participate in society.
- Community: Relationships and social networks that provide
support, friendship, love, and hope.

Monitoring for Relapse
• Patient report
• Clinical observation
• Collateral information
• Family
• Other counselors
• Probation officer
• Urine drug screening

• Methadone and to a lesser extent, Buprenorphine
are often stigmatized in many circles.Family
Medical
Police
Work
Support groups
Self
• Methadone and Buprenorphine are protected under
the American with Disabilities Act, and can not be
used as the sole reason for a firing.
• Travel can be a problem. http://www.indro-online.de/travel.htm
Discussion of Stigma and Laws
Summary
• Long-term pharmacotherapy is available and
effective for several Substance Use Disorders
• Medication + counseling = recovery
• Smoking cessation: Replacement Therapy,
Bupropion, Varenicline
• Alcohol Dependence: Disulfiram, Acamprosate,
Naltrexone
• Opiate Dependence: Methadone,
Buprenorphine,Naltrexone

Summary
Medication Assisted Recovery is a practical,
accurate, and non-stigmatizing way to describe a pathway
to recovery made possible by physician-prescribed and
monitored medications, along with other recovery supports,
e.g., counseling and peer support.

Cases for Group Discussion
Case 1
• 45 y/o Black male
• Injecting $200 of heroin daily for 18 mo.
• Began snorting at age 22, injecting for past 20 years
• Multiple detox, residential 5 yrs ago
• Longest clean time was 3 years in prison, relapsed weeks after release
• Occasional cocaine and Vicodin pills bought on the street
Case 2
• 29 y/o White male
• On MM for 4 years, clean for over 3.5 yrs, on take-out
doses for over 2 years
• Off probation, has steady job in landscaping, supporting
wife & son
• Stable on medication for depression, followed by local
psychiatrist
• Wants to come off methadone
Case 3
• 36 y/o Hispanic woman
• Smokes tobacco cigarettes since age 16
• Currently smokes 1½ packs per day
• Tried light cigarettes, just smoked more of them each day
• Occasional use of an electronic cigarette
• Wants help to quit smoking now
Case 4
• 56 y/o White male
• Binges with beer and more mixed drinks on weekends
• Went through detox 3 years ago, but relapsed after a
month
• Occasionally goes to an Alcoholics Anonymous meeting
• Has cravings for alcohol during the week
• Wants to quit drinking because he is worried about liver
damage

Case Resolutions
• 1. Long-term user: suitable for maintenance
• 2. Doing well, wants to come off: taper slowly
• 3. Mult tx approp: NRT, pills; can use nic gum or
lozenge for cravings PRN; e-cig is not for
cessation
• 4. Binge drinker: acamprosate (esp. w/ liver
damage) or NTX appropriate
Questions?
Thank You!
YourMichael Weaver, MD, DFASAM
Professor & Medical Director,
Center for Neurobehavioral Research on
Addiction
UTHealth McGovern Medical School
Don Hall LCDC, CPT
Adult Rehabilitation Services, SEARCH

www.naadac.org/comprehensive-MAT-webinar
Cost to Watch:
Free
CE Hours Available:
1.5 CEs
CE Certificate for
NAADAC Members:
Free
CE Certificate for Non-
members:
$20
To obtain a CE Certificate for the time you spent watching this
webinar:
1. Watch and listen to this entire webinar.
2. Pass the online CE quiz, which is posted at
www.naadac.org/comprehensive-MAT-webinar
3. If applicable, submit payment for CE certificate or join
NAADAC.
4. A CE certificate will be emailed to you within 21 days of
submitting the quiz.
CE Certificate
May 8, 2018 June 13, 2018
May 23, 2018June 27, 2018
Upcoming Webinars
www.naadac.org/webinars
Intergenerational Trauma and the Healing Forest
Model
By J. Carlos Rivera, CADCIII
Ensuring Fidelity to Motivational Interviewing
among Frontline Service Providers
By Ben Callaway, LMSW and Nicole Chisolm,
MPH
Therapeutic Considerations of
Psychopharmacology for Opioid Use
Disorders
By Linda Shaffer, MA, ED.S, LCAS
Picking up the Pieces for Wholeness and
Recovery
By Dana DeDolf, MA, LPC, CADCIII, MAC

www.naadac.org/webinars
Over 145 CEs of free educational
webinars are available. Education
credits are FREE for NAADAC
members.
WEBINAR SERIES
In each issue of Advances in
Addiction & Recovery, NAADAC's
magazine, one article is eligible for
CEs.
MAGAZINE ARTICLES
NAADAC offers face-to-face
seminars of varying lengths in the
U.S. and abroad.
FACE-TO-FACE SEMINARS
Earn CEs at home and at your own
pace (includes study guide and
online examination).
INDEPENDENT STUDY COURSES
NAADAC Annual Conference, October 6-8
2018, Houston, TX
www.naadac.org/2018annualconference
CONFERENCES
Demonstrate advanced education in diverse
topics with the NAADAC Certificate Programs:
• Recovery to Practice
• Conflict Resolution in Recovery
• National Certificate in Tobacco Treatment
Practice
CERTIFICATE PROGRAMS
www.naadac.org/education

Thank you for joining!
NAADAC
44 Canal Center Plaza, Suite 301
Alexandria, VA 22314
phone: 703.741.7686 / 800.548.0497
fax: 703.741.7698 / 800.377.1136
www.naadac.org
NAADACorg
Naadac
NAADAC