Embed Size (px)
Citation preview
Progress in Cardiovascular Diseases 54 (2011) 2–13www.onlinepcd.com
Comprehensive Medical Management of Peripheral Arterial DiseaseSanjay Gandhi, Ido Weinberg, Ronan Margey, Michael R. Jaff⁎
Section of Vascular Medicine, Department of Cardiovascular Medicine, Massachusetts General Hospital, Boston, MA 02114
Abstract Peripheral arterial disease (PAD) is highly prevalent and is associated with high morbidity and
Statement of Conf⁎ Address reprint
FAHA, Medical DirBoston, MA 02114.
E-mail address: m
0033-0620/$ – see frodoi:10.1016/j.pcad.20
mortality. The medical management of PAD involves a comprehensive approach to the patientwith emphasis on cardiovascular risk factor modification in addition to therapies directed attreatment of limb symptoms. This manuscript will review the current status of medical therapyin management of patients with PAD. (Prog Cardiovasc Dis 2011;54:2-13)
© 2011 Elsevier Inc. All rights reserved.Keywords: Peripheral arterial disease; Medical therapy
Peripheral arterial disease (PAD) is highly prevalent yetunder diagnosed in the general population. Usingobjective measures for detection of PAD, such as theankle-brachial index (ABI), the prevalence of PAD ismaybe as high as 12% to 30% in people aged 70 or older.1
Atherosclerosis is the major cause of PAD. Conventionalrisk factors for atherosclerosis such as diabetes mellitus(DM), tobacco abuse, hyperlipidemia, and hypertension(HTN) increase the likelihood of developing PAD. Inparticular, tobacco use increases the risk of developingPAD by 2- to 6-fold, and DM increases the risk by 2- to 4-fold.2 In the PAD Awareness, Risk, and Treatment: NewResources for Survival (PARTNERS) study, in primarycare practices across the United States, PAD was detectedin 29% of patients older than 70 years or 50 to 70 yearswith history of DM or tobacco use.3 A large proportion ofpatients with PAD have either no symptoms (20%-50%)or atypical leg pain (40%-50%). Only 10% to 35% ofpatients with PAD present with typical claudication and1% to 2% progress to critical limb ischemia (CLI).2
Cardiovascular morbidity and mortality are increased inpatients with PAD whether they are symptomatic orasymptomatic.4 Within 1 year of presentation, one quarter
lict of Interest: see page 10.requests to Michael R. Jaff, DO, FACP, FACC,ector, Vascular Center, 55 Fruit St, GRB-800,
[email protected] (M.R. Jaff).
nt matter © 2011 Elsevier Inc. All rights reserved.11.02.004
of patients with CLI die of cardiovascular causes andanother 25% suffer major limb amputation. Even patientswith stable or no symptoms have a 20% incidence ofmyocardial infarction (MI) or stroke and 15% to 30%mortality in 5 years. It, therefore, follows that detection ofPAD mandates aggressive treatment of cardiovascular riskfactors.1,2 Notwithstanding, primary care physicians werefound to treat atherosclerotic risk factors less diligently inpatients with PAD than in patients with other manifesta-tions of atherosclerosis.3,5,6 The purpose of this review isto provide a current and comprehensive review of medicaltherapies available for the treatment of PAD. Thesetreatments can be seen as having 2 primary aims: (1) toreduce cardiovascular morbidity and mortality and (2) toimprove function, limb outcomes, and quality of life.
Medical treatments to reduce cardiovascularmorbidityand mortality
The current American College of Cardiology (ACC)/American Heart Association (AHA) guidelines recom-mend aggressive management of atherosclerotic riskfactors (Table 1) to reduce future cardiovascular eventsin all patients with PAD.
Diabetes mellitus management
The prevalence of PAD in patients with DM has beenestimated to be 20% to 30%, higher than in any other
2

Table 1ACC/AHA guidelines for cardiovascupatients with PAD
Recommenda
Smoking cessation Quit smokingWeight reduction Counseling toHyperlipidemia LDL b100 mg
if diabetes orHypertension BP b140/90 o
renal failureDiabetes Hemoglobin A
6% as possiblAntiplatelet therapy ASA for all p
Clopidogrel mto ASA
Abbreviation: LDL indicates low-densit
Abbreviations and Acronyms
ABI = ankle brachial index
ACC = American College ofCardiology
AHA = American HeartAssociation
CAD = coronary arterydisease
CLI = critical limb ischemia
DM = diabetes mellitus
FGF = fibroblast growthfactor
HTN = hypertension
IC = intermittant claudication
MI = myocardial infarction
PAD = peripheral arterialdisease
VEGF = vascular endothelialgrowth factor
3S. Gandhi et al. / Progress in Cardiovascular Diseases 54 (2011) 2–13
matched population.7,8
The risk of developingPAD correlates with theduration and severity ofDM.9 Patients with DMhave symptomatic PADmore often than nondia-betic patients. In the Fra-m i n g h a m c o h o r t ,presence of DM in-creased the risk of clau-dication by 3.5-fold inmen and 8.6-fold inwomen.10 Diabetes mel-litus also alters the distri-bution of the disease, andPAD in patients with DMmore often involves thearteries below the kneethan in nondiabet icpatients.11,12 Finally, dia-betic patients with PADare more likely to presentwith tissue loss and are athigher risk for amputa-
tion compared to patients without DM.13,14 These patientsalso demonstrate reduced primary patency after endovas-cular interventions likely due to advanced and morediffuse disease.15
The effect of DM in progression of atherosclerosis ismultifactorial. The metabolic abnormalities associatedwith hyperglycemia and insulin resistance alter endothe-lial function, smooth muscle vasomotor balance, andplatelet aggregation, thereby promoting atherosclerosisand thrombus formation.16 Although tight glycemiccontrol in diabetic patients reduces the risk of developingmicrovascular disease including retinopathy and neurop-athy, it has not been shown to reduce the risk ofmacrovascular complications.17-19 The Veterans Affairs
lar risk factor modifications in
tions
reduce weight if BMI N25/dL for all patients or b70 mg/dLother vascular diseaser b130/80 in patients with DM or
1c goal of b7.0% or as close toeatients with symptomatic PAD.ay be an effective alternative
y lipoprotein.
Diabetes Trial (VADT)20 was a prospective trial random-izing 1,791 people with known type 2 DM to standardand intensive treatment of DM. The primary end pointwas cardiovascular events defined by a composite ofdeath; MI; stroke; congestive heart failure; operativetreatment of coronary, cerebrovascular, or PAD; inoper-able coronary artery disease (CAD); and amputation fromPAD. New intermittent claudication (IC) and CLI weresome of the secondary outcomes in the study. The medianglycalated hemoglobin level was 8.4% in the standardtherapy arm and 6.9% in the intensive therapy arm.However, there was no significant difference in the rate ofprimary or secondary outcomes or microvascular com-plications at a median follow-up of 5.6 years. TheEpidemiology of Diabetes Interventions and Complica-tions (EDIC) trial was a long-term follow-up of thelandmark Diabetes Control and Complications Trial(DCCT) that showed cardiovascular benefit forearly intensive treatment for patients with type 1 DMeven after going back to standard treatment.21 In thesubanalysis of the EDIC trial, assessing the developmentof low ABI for a period of 12 years in 1,398 persons,intensive treatment of blood glucose did not halt thedevelopment of low ABI but did reduce the occurrence ofarterial calcifications (P = .02).22 In summary, tightglucose control has no significant effect on cardiovascularoutcomes in patients with PAD. Therefore, to reducemacrovascular complications, the focus of therapy indiabetic patients should be on aggressive and appropriatemanagement of their other cardiovascular risk factorsincluding hyperlipidemia, HTN, and antiplatelet therapy,as outlined below.
Of note, the current American Diabetes Associationguidelines recommend targeting hemoglobin level A1c toless than 7% to reduce the incidence of microvascularevents. In addition to blood glucose control, proper footcare, including use of appropriate footwear, regularpodiatric foot and nail care, daily foot inspection, skincleansing, and use of topical moisturizing creams, shouldbe encouraged. Skin lesions and ulcerations should beaddressed urgently in all diabetic patients with PAD.23
The American Diabetes Association recommends that allpatients with DM older than the age of 50 years bescreened for PAD.23,24
Treatment of dyslipidemia
Treatment with 3-hydroxy-3-methylglutaryl coenzymeA reductase inhibitors (statins) has demonstrated areduction in the risk of nonfatal MI, stroke, andcardiovascular-related death in patients with prior strokeor established CAD. There are no randomized, controlledtrials of statin therapy in patients with PAD alone. TheHeart Protection Study25,26 randomized 20,536 high-riskpatients to 40 mg/d of simvastatin or placebo, including6,748 patients with PAD. In patients with PAD, there was

4 S. Gandhi et al. / Progress in Cardiovascular Diseases 54 (2011) 2–13
a 25% reduction in risk of cardiovascular events in patientsrandomized to simvastatin during the 5 years of follow-upregardless of their initial serum lipid levels and in additionto other treatments. In addition to the cholesterol-loweringeffect, statin use also correlates with improved 6-minutewalking distance and walking velocity.27 In a study of354 patients with an ABI 0.9 or less randomized toatorvastatin 10 mg/d, atorvastatin 80 mg/d, or placebo,there was improvement in pain-free walking time for65% of patients receiving 80 mg of atorvastatin at 12months. However, there was no significant differencebetween atorvastatin 10 mg/d and placebo groups. Therewere also fewer vascular events (defined as worseningsymptoms of claudication, development of ischemic restpain, peripheral revascularization procedures, or limbamputation) in the treatment group as compared withplacebo treated patients.28 Statin use has also beenshown to reduce the risk of new or worsening claudi-cation symptoms by 38% for 5.4 years in patients withhyperlipidemia and CAD in a retrospective analysis ofthe Scandinavian Simvastatin Survival Study (4S).29 Themechanism by which statins affect claudication walkingspeed, distance, and time is felt to be because of improvedendothelium-mediated vasodilatation and reducedplatelet aggregation along with modulation of plaquevulnerability.27,30
The current ACC/AHA PAD guidelines recommend atarget low-density lipoprotein in patients with PAD of lessthan 100 mg/dL1,31 and less than 70 mg/dL in patientswith evidence of other vascular bed involvement1 or thosedeemed to be at very high risk for ischemic events.2,31
Tobacco cessation
Cigarette smoking is one of the most importantpreventable risk factor for PAD in both men andwomen.2 Both current and former smokers have 2- to3-fold higher prevalence of symptomatic PAD com-pared with nonsmokers.32 In a systematic review of 17studies, overall odds ratio for prevalence of symptomaticPAD was 2.3 times in current smokers compared tononsmokers.32 The incidence of symptomatic PAD isdirectly proportional to the dose of exposure, with anincrease from 2.6% in never smokers to 9.8% in heavysmokers.33 Even passive tobacco exposure with secondhand smoke nearly doubles the risk of development ofPAD in nonsmokers.34 Although the prevalence ofsymptomatic PAD is decreased in former smokers, itstill remains higher than in never smokers.32 Smokingcessation not only decreases the rate of PAD progression,amputation, and CLI but also improves overall survivalwith lower rates of MI and stroke.35,36 Surprisingly, therole of smoking cessation in treating the symptoms ofclaudication is not as clear; studies have shown thatsmoking cessation is associated with improved walkingdistance in some, but not all, patients. However, these
benefits are not predictable and should not be presentedwith certainty of effect. Patients should therefore beencouraged to stop smoking primarily to reduce their riskof cardiovascular events as well as their risk of progressionto major limb amputation and progression of PAD.Unfortunately, smoking cessation is offered to only halfof patients with PAD in primary care.3
All patients with PAD should be asked strongly andrepeatedly to discontinue all tobacco products. All patientsshould be offered proven comprehensive tobacco cessa-tion interventions, including behavior modification ther-apy, nicotine replacement therapy, or bupropion. Smokingcessation counseling and treatment should be an integralpart of treatment of every patient with PAD.1,2
Hypertension control
Up to 55% of patients with PAD have HTN.37 Inaddition to reducing cardiovascular events, treatment ofHTN reduces the incidence of PAD-related amputation,particularly in patients with DM. In an analysis of theUK Prospective Diabetes Study (UKPDS) data, areduction of systolic blood pressure by 10 mm Hg con-ferred a 16% decrease in rate of limb amputation or deathfrom PAD.17
All pharmacologic agents that lower blood pressurereduce the risk of cardiovascular events.38 Therefore, thechoice of antihypertensive agent is less relevant thanactual control of blood pressure.39 However, angiotensin-converting enzyme inhibitors have shown benefit, speci-fically in PAD, potentially beyond their blood pressure–lowering effect. The Heart Outcomes Prevention Evalua-tion (HOPE) study evaluated the effect of ramipril inpatients with CAD, cerebrovascular disease, PAD, ordiabetes.40 The study included 4,051 patients with PAD.In this subgroup, the reduction in risk of MI, stroke, orvascular death in patients randomized to ramipril com-pared to placebo approached 22%, independent of theblood pressure–lowering effect. A similar reduction ofcardiovascular end points was seen in a subgroup of 883patients with PAD treated with perindopril in the Europeantrial on reduction of cardiac events with perindopril(EUROPA) trial.41 Therefore, angiotensin-convertingenzyme inhibitors are an attractive first-line agent formanagement of HTN in patients with PAD.
There had been concern in the past that the use ofβ-adrenergic antagonists in patients with PADmay worsenthe symptoms of claudication. However, in a meta-analysis of 11 trials, β-blockers were shown to be safe inpatients with PAD.42 Of note, the incidence of renal arterystenosis is increased in patients with PAD. This diagnosismust therefore be kept in mind when HTN resistant tomedical therapy is encountered in these patients.39
The current ACC/AHA PAD guidelines recommend agoal blood pressure less than 140/90 in patients with PADwithout DM and less than 130/80 in patients with DM orchronic kidney disease.

5S. Gandhi et al. / Progress in Cardiovascular Diseases 54 (2011) 2–13
Antiplatelet and antithrombotic therapy
AspirinAspirin use has been shown to reduce the risk of stroke,
MI, and vascular death by approximately 25% in patientswith established coronary and cerebrovascular disease.43
In the Antithrombotic Trialists' Collaboration meta-analysis, a subgroup of 9,214 patients with PAD hadbenefit similar to those of patients with coronary andcerebrovascular disease, with a 23% reduction in seriousvascular events.43 However, there remains uncertaintyabout the benefit of aspirin in patients with isolatedasymptomatic PAD without involvement of other vascularbeds. In a recent meta-analysis of 18 trials that included5,269 patients with PAD, aspirin therapy alone or incombination with dipyridamole led to a 12% reduction inthe primary end point of cardiovascular events; however,this did not reach statistical significance.44 Similarly, inpatients with diabetes and asymptomatic PAD, no benefitwith aspirin use was seen in the Japanese PrimaryPrevention of Atherosclerosis with aspirin in Diabetes(JPAD) trial and the prevention of progression of arterialdisease and diabetes (POPADAD).45,46 The Aspirin forAsymptomatic Atherosclerosis trial, one of the largestdouble-blind, placebo-controlled trial of 3,350 asymptom-atic subjects with ABI less than 0.95 without cardiovas-cular disease demonstrated no effect of aspirin inpreventing fatal or nonfatal coronary event or stroke orrevascularization. Although this study had a high rate ofnoncompliance (40%) and was underpowered, the benefitsof aspirin, if any, are likely to be very small.47
Aspirin use has been shown to have benefit in patientswith previous lower extremity surgical revascularization.Adjuvant aspirin therapy has also been recommended inserial Cochrane reviews to improve the patency rate afterlower extremity bypass grafts.48
ThienopyridinesThienopyridine class of agents inhibit platelet aggre-
gation via inhibition of the adenosine diphosphatepathway.49 They have been studied as an alternative toor in combination with aspirin. Ticlopidine, althoughshown to reduce the risk of MI, stroke, and vascular deathin patients with PAD, has limited role because of theserious adverse effects of neutropenia, thrombocytopenia,and thrombotic thrombocytopenic purpura.50 The Clopi-dogrel versus Aspirin in Patients at Risk of IschemicEvents (CAPRIE) trial compared the use of clopidogrel incomparison to aspirin in high-risk patients (recent MI,stroke, and PAD) and included 6,452 patients with PAD.In a post hoc analysis, patients with PAD treated withclopidogrel noted a 24% reduction in the incidence ofstroke, MI, or vascular death when compared to aspirin.51
The incremental benefit of clopidogrel in addition toaspirin was studied in the Clopidogrel for High Athero-thrombotic Risk and Ischemia Stabilization, Management,
and Avoidance (CHARISMA) study in a high-riskpopulation consisting of patients with established cardio-vascular disease (including PAD in 23% of enrolledpatients) and patients without a history of cardiovasculardisease but who had multiple atherosclerotic risk factors.52
This study demonstrated no benefit of dual antiplatelettherapy as compared to aspirin alone when studying theoutcome of MI, stroke, and vascular death. In a subgroupof patients with PAD, prior MI, or stroke, the compositeischemic event rate was significantly lower at 7.3% forclopidogrel plus aspirin compared to 8.8% for aspirinalone. Moderate bleeding complications, as described bythe Global Utilization of Streptokinase and TissuePlasminogen Activator for Occluded Coronary Arteries(GUSTO) definition of bleeding requiring blood transfu-sion but not including fatal bleeds, intracranial hemor-rhage, or hemorrhage culminating in hemodynamiccompromise requiring resuscitation, inotropes, or surgery,were more common with dual therapy.52 Based on currentdata, combination therapy cannot be recommended inpatients with stable PAD, and if clopidogrel is considered,it should be used as monotherapy.
In the recently published clopidogrel and acetylsa-licylic acid in bypass surgery for peripheral arterialdisease (CASPAR) trial, the combination of clopidogrelplus aspirin did not improve limb or systemic outcomesin the overall population of patients with PAD requiringbelow-knee surgical bypass grafting. Subgroup analysissuggests that clopidogrel plus aspirin confers benefit inpatients receiving prosthetic grafts without significantlyincreasing major bleeding risk.53
Finally, newer generation thienopyridine antiplateletagents such as prasugrel have recently been approved foruse in patients with CAD and acute coronary syndromes asan alternative to clopidogrel.54,55
Although these agents have more rapid and effectiveantiplatelet efficacy than aspirin, they are associated withhigher bleeding complication rates. No evidence currentlyexists describing a therapeutic role or safety for theseagents in patients with PAD only, and they do not have anFood and Drug Administration–approved indication foruse in this population.49,54,55
Warfarin
The Warfarin Anti-platelet Vascular Evaluation(WAVE) trial has confirmed that vitamin K antagonistshave no role in the prevention of cardiovascular events inpatients with PAD. In this trial, patients randomized to acombination of antiplatelet and anticoagulant therapy hadan increase in life-threatening bleeding.56 However, ifpatients have an alternative indication for anticoagulationwith vitamin K antagonists, such as atrial fibrillation,venous thromboembolic disease, or prosthetic heartvalves, then combination of warfarin and antiplatelettherapy can be prescribed, although the patients should bemonitored closely for bleeding complications.
6 S. Gandhi et al. / Progress in Cardiovascular Diseases 54 (2011) 2–13
In conclusion, the current ACC/AHA PAD guidelinesrecommend antiplatelet therapy for all symptomaticpatients with PAD with or without cardiovascular diseaseto reduce the risk of cardiovascular morbidity andmortality. Aspirin is effective in patients with PAD inwhom there is evidence of other forms of cardiovasculardisease. The use of aspirin in patients with PAD withoutovert cardiovascular disease can be considered, but theevidence is controversial. Clopidogrel, as an alternative toaspirin, is effective in decreasing cardiovascular events insymptomatic patients with PAD with or without othercardiovascular disease. Finally, oral anticoagulation ther-apy with warfarin is not indicated to reduce the risk ofadverse cardiovascular ischemic events in individuals withatherosclerotic PAD.
Medical therapy to treat limb symptoms
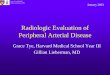
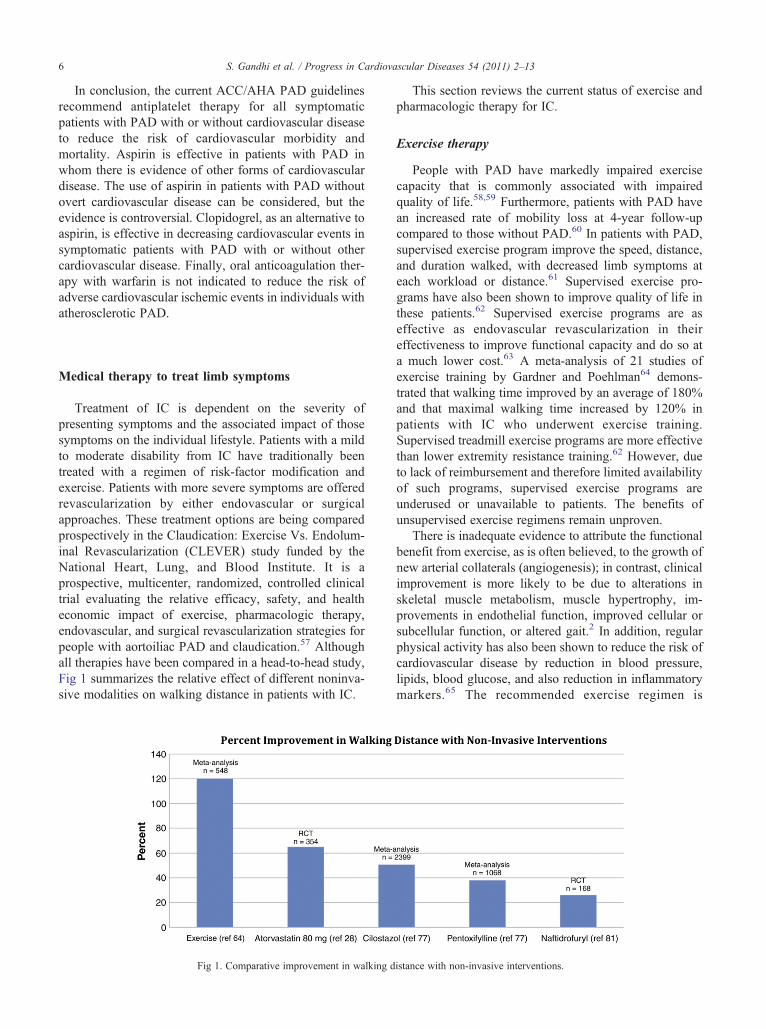
Treatment of IC is dependent on the severity ofpresenting symptoms and the associated impact of thosesymptoms on the individual lifestyle. Patients with a mildto moderate disability from IC have traditionally beentreated with a regimen of risk-factor modification andexercise. Patients with more severe symptoms are offeredrevascularization by either endovascular or surgicalapproaches. These treatment options are being comparedprospectively in the Claudication: Exercise Vs. Endolum-inal Revascularization (CLEVER) study funded by theNational Heart, Lung, and Blood Institute. It is aprospective, multicenter, randomized, controlled clinicaltrial evaluating the relative efficacy, safety, and healtheconomic impact of exercise, pharmacologic therapy,endovascular, and surgical revascularization strategies forpeople with aortoiliac PAD and claudication.57 Althoughall therapies have been compared in a head-to-head study,Fig 1 summarizes the relative effect of different noninva-sive modalities on walking distance in patients with IC.
Fig 1. Comparative improvement in walking d
This section reviews the current status of exercise andpharmacologic therapy for IC.
Exercise therapy
People with PAD have markedly impaired exercisecapacity that is commonly associated with impairedquality of life.58,59 Furthermore, patients with PAD havean increased rate of mobility loss at 4-year follow-upcompared to those without PAD.60 In patients with PAD,supervised exercise program improve the speed, distance,and duration walked, with decreased limb symptoms ateach workload or distance.61 Supervised exercise pro-grams have also been shown to improve quality of life inthese patients.62 Supervised exercise programs are aseffective as endovascular revascularization in theireffectiveness to improve functional capacity and do so ata much lower cost.63 A meta-analysis of 21 studies ofexercise training by Gardner and Poehlman64 demons-trated that walking time improved by an average of 180%and that maximal walking time increased by 120% inpatients with IC who underwent exercise training.Supervised treadmill exercise programs are more effectivethan lower extremity resistance training.62 However, dueto lack of reimbursement and therefore limited availabilityof such programs, supervised exercise programs areunderused or unavailable to patients. The benefits ofunsupervised exercise regimens remain unproven.
There is inadequate evidence to attribute the functionalbenefit from exercise, as is often believed, to the growth ofnew arterial collaterals (angiogenesis); in contrast, clinicalimprovement is more likely to be due to alterations inskeletal muscle metabolism, muscle hypertrophy, im-provements in endothelial function, improved cellular orsubcellular function, or altered gait.2 In addition, regularphysical activity has also been shown to reduce the risk ofcardiovascular disease by reduction in blood pressure,lipids, blood glucose, and also reduction in inflammatorymarkers.65 The recommended exercise regimen is
istance with non-invasive interventions.

7S. Gandhi et al. / Progress in Cardiovascular Diseases 54 (2011) 2–13
supervised exercise for 30 minutes 3 times a week for atleast 12 weeks, with further increase of exercise time to anhour each session. Intensity should be submaximal in sucha way that induces pain within 3 to 5 minutes.1,66 TheAHA and American College of Sports Medicine alsorecommend 30 minutes or more of moderate intensityphysical activity, preferably daily, for reduction incardiovascular risk.66
Weight loss
Obesity and metabolic syndrome are highly prevalentamong patients with PAD. In the subgroup of patients withPAD in the Reduction of Atherothrombosis for ContinuedHealth (REACH) registry, nearly half of the patients withPAD had abdominal obesity.5 Similarly, in another study,metabolic syndrome as defined by adenosine triphosphateIII report was present in 41% of patients with PAD.67 Bothobesity and metabolic syndrome are independent pre-dictors of adverse cardiovascular events in thesepatients.67,68 Obesity also correlates with reduced abilityto walk and shorter time to onset of IC symptoms. A 6-year, ongoing longitudinal study examined the prevalenceof self-reported effort-related calf pain in 4,047 obeseSwedish people and a reference group of 1,135 subjects.Obese people experienced more calf symptoms thannonobese (odds ratio for symptoms was 4.4 and 6.8 formen and women, respectively) counterparts. Calf symp-toms improved as patients lost weight in a dose-responsefashion. The most prominent recovery occurred in personswho had lost the most weight secondary to bariatricsurgery.69 Obese patients also experience a higher rate ofpostoperative surgical site infections after lower extremitybypass surgery.70 Therefore, all overweight or obesepatients with PAD should be encouraged to lose weight.
Pharmacologic therapy for IC
CilostazolCilostazol is a type 3 phosphodiestherase inhibitor that
increases cyclic adenosine monophosphate. The precisemechanism whereby cilostazol improves walking distancein patients with IC is unclear. The putative mechanismsinclude a favorable effect on platelet aggregation,vasodilation, and modification of the lipid profile (raisinghigh-density lipoprotein, lowering triglyceride levels).71,72
Besides effect on claudication, cilostazol reducesvascular smooth muscle cell proliferation73 and maydecrease chronic inflammation and atherogeniccytokines.74 In a small randomized trial of 78 patientsundergoing femoropopliteal intervention, patientsassigned to cilostazol plus aspirin (n = 39) had lowerrate of restenosis (46.3% vs 70.3%) and repeat revascu-larization (18% vs 43.6%) at 2 years compared to patientsrandomized to aspirin alone.75
Several trials have demonstrated the efficacy ofcilostazol in improving walking distance and quality of
life in patients with IC compared with placebo or pento-xifylline. In a pooled analysis of data from 9 randomized,controlled trials of cilostazol at 100 mg BID, cilostazolwas associated with a 50.7% improvement from baselinein maximal walking distance compared to placebo (24.3%)for a mean follow-up period of 20.4 weeks. These benefitswere sustained during the 24-week treatment period.76
These findings are similar to those of a previous meta-analysis by Thompson et al77 and Cochrane review in2008,78 both of which showed significant benefit ofcilostazol at a dose of 100 mg BID. A 50-mg twice dailydosing of cilostazol led to a lower (44%) improvement inmean walking distance from baseline.77 Patients treatedwith cilostazol improved far better than patients random-ized to either pentoxifylline (38%) or placebo (21%).
The most common adverse effects noted by patientstreated with cilostazol were related to the vasodilatoryproperties of the agent, notably headaches, diarrhea,dizziness, and palpitations.71,78
Because cilostazol is structurally similar to milrinone,which has been shown to increase mortality in patientswith congestive heart failure, cilostazol's use is contra-indicated in patients with congestive heart failure and/orleft ventricular ejection fraction less than 40%. However,there is little direct evidence of increased mortality withcilostazol. The Cilostazol: A Study in Long-term Effects(CASTLE) study79 was a randomized multicenter place-bo-controlled post market study to evaluate the safety ofcilostazol for a period of 3 years. It randomized assigned718 patients to cilostazol and 717 patients to placebo.However, the study was discontinued prematurelybecause of a low event rate and a high rate of drugdiscontinuation (N60%) at 3 years. Notwithstanding theselimitations, the study showed that the all-cause (1.72events per person-year of follow-up) and cardiovascularmortality (1.34 events per person-year) rates were lowand similar to that of the placebo arm. There was noincrease in bleeding in patients treated with cilostazol.
The current ACC/AHA PAD guidelines recommendcilostazol 100 mg orally twice daily to improve ICsymptoms in the absence of heart failure.
PentoxifyllinePentoxifylline is a methylxanthine derivative that is
believed to exert hemorrheologic effects by decreasingblood viscosity, increasing red blood cell deformability,inhibiting neutrophil adhesion and activation, and lower-ing plasma fibrinogen concentrations in some studies butnot in others.2
The clinical data regarding benefits of pentoxifyllineare inconsistent. Pentoxifylline does not improve ABIat rest or after exercise. A 3-arm comparison of cilos-tazol, pentoxifylline, or placebo in 698 patients did notprove a statistically significant advantage for pentoxifyl-line over placebo.80
8 S. Gandhi et al. / Progress in Cardiovascular Diseases 54 (2011) 2–13
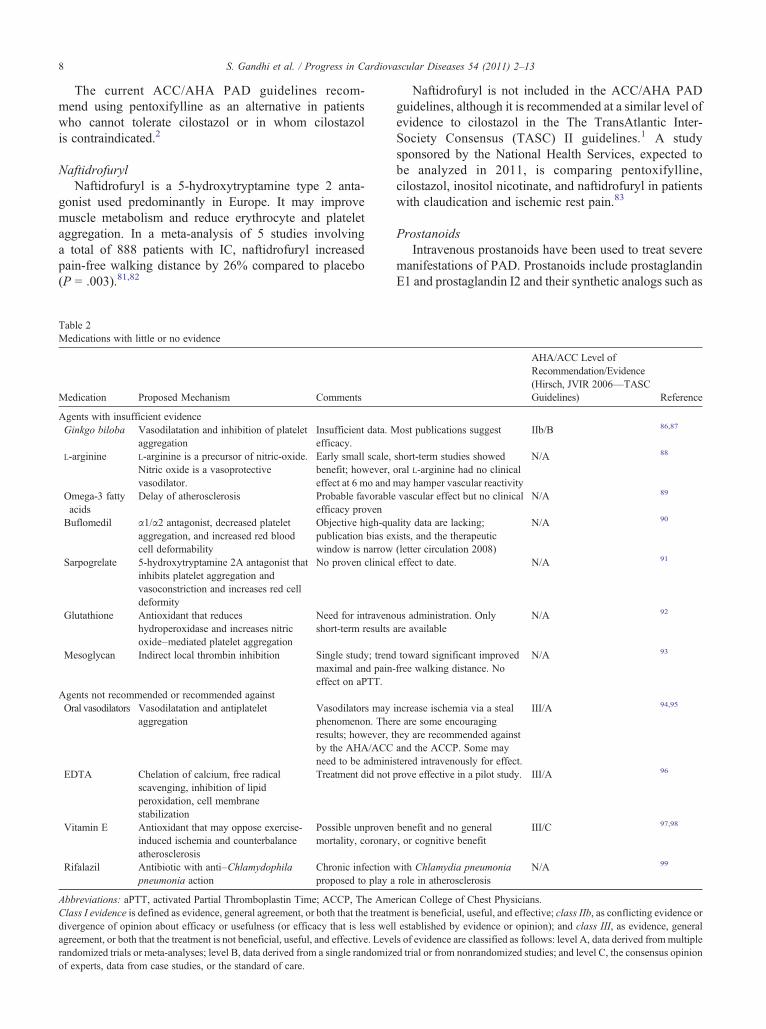
The current ACC/AHA PAD guidelines recom-mend using pentoxifylline as an alternative in patientswho cannot tolerate cilostazol or in whom cilostazolis contraindicated.2
NaftidrofurylNaftidrofuryl is a 5-hydroxytryptamine type 2 anta-
gonist used predominantly in Europe. It may improvemuscle metabolism and reduce erythrocyte and plateletaggregation. In a meta-analysis of 5 studies involvinga total of 888 patients with IC, naftidrofuryl increasedpain-free walking distance by 26% compared to placebo(P = .003).81,82
Table 2Medications with little or no evidence
Medication Proposed Mechanism Comments
Agents with insufficient evidenceGinkgo biloba Vasodilatation and inhibition of platelet
aggregationInsufficient data. Mefficacy.
L-arginine L-arginine is a precursor of nitric-oxide.Nitric oxide is a vasoprotectivevasodilator.
Early small scale,benefit; however,effect at 6 mo and
Omega-3 fattyacids
Delay of atherosclerosis Probable favorableefficacy proven
Buflomedil α1/α2 antagonist, decreased plateletaggregation, and increased red bloodcell deformability
Objective high-qupublication bias exwindow is narrow
Sarpogrelate 5-hydroxytryptamine 2A antagonist thatinhibits platelet aggregation andvasoconstriction and increases red celldeformity
No proven clinical
Glutathione Antioxidant that reduceshydroperoxidase and increases nitricoxide–mediated platelet aggregation
Need for intravenoshort-term results
Mesoglycan Indirect local thrombin inhibition Single study; trendmaximal and pain-effect on aPTT.
Agents not recommended or recommended againstOral vasodilators Vasodilatation and antiplatelet
aggregationVasodilators mayphenomenon. Theresults; however, tby the AHA/ACCneed to be admini
EDTA Chelation of calcium, free radicalscavenging, inhibition of lipidperoxidation, cell membranestabilization
Treatment did not
Vitamin E Antioxidant that may oppose exercise-induced ischemia and counterbalanceatherosclerosis
Possible unprovenmortality, coronary
Rifalazil Antibiotic with anti–Chlamydophilapneumonia action
Chronic infectionproposed to play a
Abbreviations: aPTT, activated Partial Thromboplastin Time; ACCP, The AmeClass I evidence is defined as evidence, general agreement, or both that the treatmdivergence of opinion about efficacy or usefulness (or efficacy that is less welagreement, or both that the treatment is not beneficial, useful, and effective. Leverandomized trials or meta-analyses; level B, data derived from a single randomizof experts, data from case studies, or the standard of care.
Naftidrofuryl is not included in the ACC/AHA PADguidelines, although it is recommended at a similar level ofevidence to cilostazol in the The TransAtlantic Inter-Society Consensus (TASC) II guidelines.1 A studysponsored by the National Health Services, expected tobe analyzed in 2011, is comparing pentoxifylline,cilostazol, inositol nicotinate, and naftidrofuryl in patientswith claudication and ischemic rest pain.83
ProstanoidsIntravenous prostanoids have been used to treat severe
manifestations of PAD. Prostanoids include prostaglandinE1 and prostaglandin I2 and their synthetic analogs such as
AHA/ACC Level ofRecommendation/Evidence(Hirsch, JVIR 2006—TASCGuidelines) Reference
ost publications suggest IIb/B 86,87
short-term studies showedoral L-arginine had no clinicalmay hamper vascular reactivity
N/A 88
vascular effect but no clinical N/A 89
ality data are lacking;ists, and the therapeutic(letter circulation 2008)
N/A 90
effect to date. N/A 91
us administration. Onlyare available
N/A 92
toward significant improvedfree walking distance. No
N/A 93
increase ischemia via a stealre are some encouraginghey are recommended againstand the ACCP. Some maystered intravenously for effect.
III/A 94,95
prove effective in a pilot study. III/A 96
benefit and no general, or cognitive benefit
III/C 97,98
with Chlamydia pneumoniarole in atherosclerosis
N/A 99
rican College of Chest Physicians.ent is beneficial, useful, and effective; class IIb, as conflicting evidence orl established by evidence or opinion); and class III, as evidence, generalls of evidence are classified as follows: level A, data derived from multipleed trial or from nonrandomized studies; and level C, the consensus opinion
9S. Gandhi et al. / Progress in Cardiovascular Diseases 54 (2011) 2–13
iloprost. They are proposed to cause vasodilatation andinhibit platelet activation, adhesion, and aggregation andmay have antithrombotic and profibrinolytic actions. Theymay also improve endothelial function.84 The resultsconcerning their efficacy are contradictory. A recentCochrane database review of 20 trials with a total of2,724 patients concluded that despite positive resultsregarding pain relief, ulcer healing, and amputation ratereduction, there was not enough data to recommend the useof prostanoids for CLI.85 The AHA/ACC guidelines2 forthe management of patients with PAD recommendedagainst the use of prostanoids for claudication (level ofevidence III/A) or for reducing the risk of amputation inpatients with CLI (level of evidence III/B). Parenteralprostanoids may be considered to facilitate the healing ofulcers or reduction of rest pain (level of evidence IIb/A).
Other agents
There have been many other pharmacologic agentsstudied to improve physical functioning in patients withIC, all demonstrating limited or no benefit. These aresummarized in Table 2.
Regenerative therapies
Several trials are evaluating the role of protein and genetransfer therapies for patients with PAD. Despite the vast
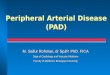
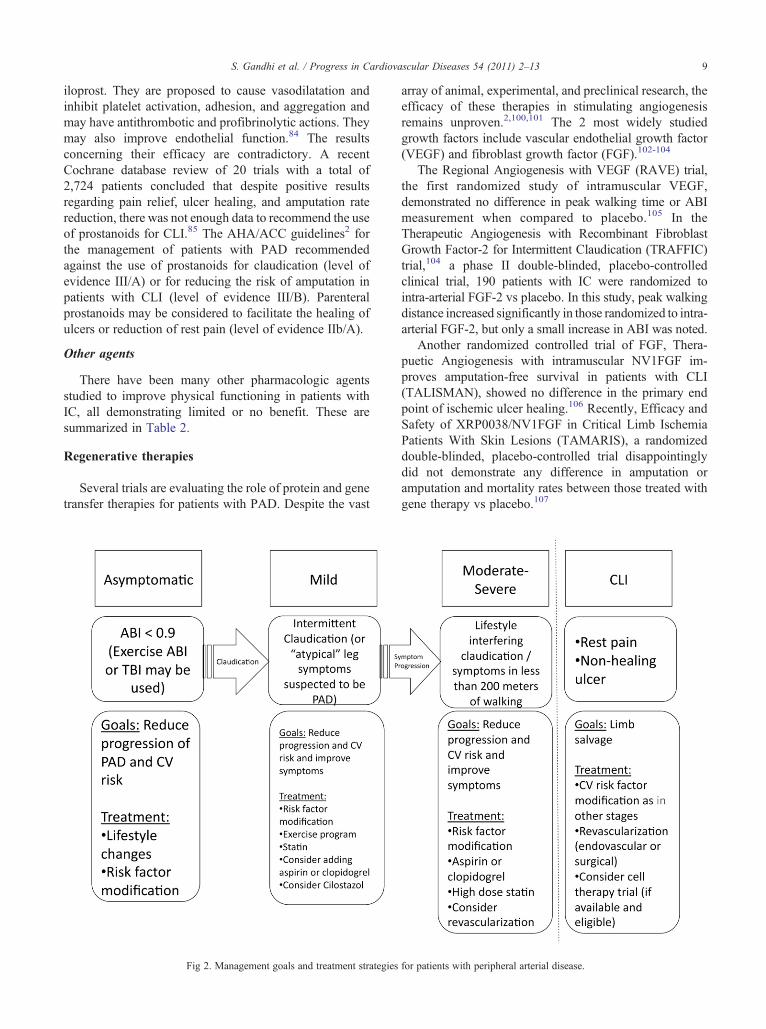
Fig 2. Management goals and treatment strategies
array of animal, experimental, and preclinical research, theefficacy of these therapies in stimulating angiogenesisremains unproven.2,100,101 The 2 most widely studiedgrowth factors include vascular endothelial growth factor(VEGF) and fibroblast growth factor (FGF).102-104
The Regional Angiogenesis with VEGF (RAVE) trial,the first randomized study of intramuscular VEGF,demonstrated no difference in peak walking time or ABImeasurement when compared to placebo.105 In theTherapeutic Angiogenesis with Recombinant FibroblastGrowth Factor-2 for Intermittent Claudication (TRAFFIC)trial,104 a phase II double-blinded, placebo-controlledclinical trial, 190 patients with IC were randomized tointra-arterial FGF-2 vs placebo. In this study, peak walkingdistance increased significantly in those randomized to intra-arterial FGF-2, but only a small increase in ABI was noted.
Another randomized controlled trial of FGF, Thera-puetic Angiogenesis with intramuscular NV1FGF im-proves amputation-free survival in patients with CLI(TALISMAN), showed no difference in the primary endpoint of ischemic ulcer healing.106 Recently, Efficacy andSafety of XRP0038/NV1FGF in Critical Limb IschemiaPatients With Skin Lesions (TAMARIS), a randomizeddouble-blinded, placebo-controlled trial disappointinglydid not demonstrate any difference in amputation oramputation and mortality rates between those treated withgene therapy vs placebo.107
for patients with peripheral arterial disease.

10 S. Gandhi et al. / Progress in Cardiovascular Diseases 54 (2011) 2–13
There are also several studies looking at the role ofbone marrow progenitor or peripheral blood progenitorcells in patients with PAD. The Therapeutic Angiogenesisusing Cell Transplantation (TACT) trial initially studied25 patients with unilateral limb ischemia. In this study,patients were administered autologous bone marrow–derived mononuclear cells injected intramuscularly.108 At25 weeks, there were markedly improved transcutaneousoxygen pressure gradients, pain-free walking time, andreduction in ischemic rest pain. From this pilot study, afurther 22 patients were randomized to bone marrow–derived cells in 1 leg and peripheral blood derived cells inthe other. The same clinical improvements were noted inthis segment of the study, and safety has been reported outto 3 years of follow-up.
Multiple clinical series have reported similar positivefindings in contrast to the largely disappointing resultsfrom gene therapy. Huang et al109,110 have published smallseries demonstrating the clinical efficacy of peripherallyharvested mononuclear progenitor cells for angiogenesistherapy in diabetic patients with PAD without surgical orendovascular options. Although promising, these therapiesneed to be evaluated in rigorous well-controlled random-ized trials before considered for clinical use.
Conclusion
Peripheral arterial disease is the most underrecognizedand undertreated atherosclerotic syndrome in the generalpopulation. Clinicians should actively seek out patients atrisk for PAD because they are at very high risk for futurecardiovascular events and mortality. Once the diagnosis ofPAD is established, all patients must receive a compre-hensive program to lower their risk for future cardiovas-cular events. Our approach to manage these patients issummarized in Fig 2. This includes aggressive atheroscle-rotic risk factor modification including tobacco cessation,weight loss, antiplatelet therapy, lipid-lowering therapy,control of DM, and high blood pressure. For patients whoare symptomatic, participation in a supervised exerciseprogram and pharmacologic therapy should be advised toimprove quality of life.
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest.
References
1. Norgren L, Hiatt WR, Dormandy JA, et al: Inter-Society Consensusfor the Management of Peripheral Arterial Disease (TASC II).J Vasc Surg 2007;45(Suppl S):S5-S67.
2. Hirsch AT, Haskal ZJ, Hertzer NR, et al: ACC/AHA 2005 Practiceguidelines for the management of patients with peripheral arterial
disease (lower extremity, renal, mesenteric, and abdominal aortic): acollaborative report from the American Association for VascularSurgery/Society for Vascular Surgery, Society for CardiovascularAngiography and Interventions, Society for Vascular Medicine andBiology, Society of Interventional Radiology, and the ACC/AHATask Force on Practice Guidelines (Writing Committee to DevelopGuidelines for the Management of Patients With Peripheral ArterialDisease): endorsed by the American Association of Cardiovascularand Pulmonary Rehabilitation; National Heart, Lung, and BloodInstitute; Society for Vascular Nursing; TransAtlantic Inter-SocietyConsensus; and Vascular Disease Foundation. Circulation 2006;113:e463-e654.
3. Hirsch AT, Criqui MH, Treat-Jacobson D, et al: Peripheral arterialdisease detection, awareness, and treatment in primary care. JAMA2001;286:1317-1324.
4. Diehm C, Allenberg JR, Pittrow D, et al: Mortality and vascularmorbidity in older adults with asymptomatic versus symptomaticperipheral artery disease. Circulation 2009;120:2053-2061.
5. Zeymer U, Parhofer KG, Pittrow D, et al: Risk factor profile,management and prognosis of patients with peripheral arterialdisease with or without coronary artery disease: results of theprospective German REACH registry cohort. Clin Res Cardiol2009;98:249-256.
6. Welten GM, Schouten O, Hoeks SE, et al: Long-term prognosis ofpatients with peripheral arterial disease: a comparison in patientswith coronary artery disease. J Am Coll Cardiol 2008;51:1588-1596.
7. Marso SP, Hiatt WR: Peripheral arterial disease in patients withdiabetes. J Am Coll Cardiol 2006;47:921-929.
8. Selvin E, Erlinger TP: Prevalence of and risk factors for peripheralarterial disease in the United States: results from the National Healthand Nutrition Examination Survey, 1999-2000. Circulation 2004;110:738-743.
9. Wattanakit K, Folsom AR, Selvin E, et al: Risk factors forperipheral arterial disease incidence in persons with diabetes: theAtherosclerosis Risk in Communities (ARIC) Study. Atheroscle-rosis 2005;180:389-397.
10. Kannel WB, McGee DL: Update on some epidemiologic features ofintermittent claudication: the Framingham Study. J Am Geriatr Soc1985;33:13-18.
11. Mackaay AJ, Beks PJ, Dur AH, et al: The distribution of peripheralvascular disease in a Dutch Caucasian population: comparison oftype II diabetic and non-diabetic subjects. Eur J Vasc EndovascSurg 1995;9:170-175.
12. Dosluoglu HH, Lall P, Nader ND, et al: Insulin use is associatedwith poor limb salvage and survival in diabetic patients withchronic limb ischemia. J Vasc Surg 2010;51:1178-1189 [discussion1188-1189].
13. Jude EB, Oyibo SO, Chalmers N, et al: Peripheral arterial disease indiabetic and nondiabetic patients: a comparison of severity andoutcome. Diabetes Care 2001;24:1433-1437.
14. Bild DE, Selby JV, Sinnock P, et al: Lower-extremity amputation inpeople with diabetes. Epidemiology and prevention. Diabetes Care1989;12:24-31.
15. DeRubertis BG, Pierce M, Ryer EJ, et al: Reduced primary patencyrate in diabetic patients after percutaneous intervention results frommore frequent presentation with limb-threatening ischemia. J VascSurg 2008;47:101-108.
16. Beckman JA, Creager MA, Libby P: Diabetes and atherosclerosis:epidemiology, pathophysiology, and management. JAMA 2002;287:2570-2581.
17. Adler AI, Stratton IM, Neil HA, et al: Association of systolic bloodpressure with macrovascular and microvascular complicationsof type 2 diabetes (UKPDS 36): prospective observational study.BMJ 2000;321:412-419.
18. UK Prospective Diabetes Study (UKPDS) Group: Intensive blood-glucose control with sulphonylureas or insulin compared with
11S. Gandhi et al. / Progress in Cardiovascular Diseases 54 (2011) 2–13
conventional treatment and risk of complications in patients withtype 2 diabetes (UKPDS 33). Lancet 1998;352:837-853.
19. Patel A, MacMahon S, et al, ADVANCE Collaborative Group:Intensive blood glucose control and vascular outcomes in patientswith type 2 diabetes. N Engl J Med 2008;358:2560-2572.
20. Duckworth W, Abraira C, Moritz T, et al: Glucose control andvascular complications in veterans with type 2 diabetes. N Engl JMed 2009;360:129-139.
21. Nathan DM, Cleary PA, Backlund JY, et al: Intensive diabetestreatment and cardiovascular disease in patients with type 1diabetes. N Engl J Med 2005;353:2643-2653.
22. Carter RE, Lackland DT, Cleary PA, et al: Intensive treatment ofdiabetes is associated with a reduced rate of peripheral arterialcalcification in the diabetes control and complications trial.Diabetes Care 2007;30:2646-2648.
23. American Diabetes Association: Standards of medical care indiabetes—2010. Diabetes Care 2010;33(Suppl 1):S11-S61.
24. Olin JW, Allie DE, Belkin M, et al: ACCF/AHA/ACR/SCAI/SIR/SVM/SVN/SVS 2010 Performance measures for adults withperipheral artery disease: a report of the American College ofCardiology Foundation/American Heart Association Task Force onPerformance Measures, the American College of Radiology, theSociety for Cardiac Angiography and Interventions, the Society forInterventional Radiology, the Society for Vascular Medicine, theSociety for Vascular Nursing, and the Society for Vascular Surgery(Writing Committee to Develop Clinical Performance Measures forPeripheral Artery Disease). Circulation 2010;122:2583-2618.
25. Heart Protection Study Collaborative Group: Randomized trial ofthe effects of cholesterol-lowering with simvastatin on peripheralvascular and other major vascular outcomes in 20,536 people withperipheral arterial disease and other high-risk conditions. J VascSurg 2007;45:645-654 [discussion 653-654].
26. Heart Protection Study Collaborative Group: MRC/BHF HeartProtection Study of cholesterol lowering with simvastatin in 20,536high-risk individuals: a randomised placebo-controlled trial. Lancet2002;360:7-22.
27. McDermott MM, Guralnik JM, Greenland P, et al: Statin use andleg functioning in patients with and without lower-extremityperipheral arterial disease. Circulation 2003;107:757-761.
28. Mohler III ER, Hiatt WR, Creager MA: Cholesterol reduction withatorvastatin improves walking distance in patients with peripheralarterial disease. Circulation 2003;108:1481-1486.
29. Pedersen TR, Kjekshus J, Pyorala K, et al: Effect of simvastatin onischemic signs and symptoms in the Scandinavian SimvastatinSurvival Study (4S). Am J Cardiol 1998;81:333-335.
30. Beckman JA, Creager MA: The nonlipid effects of statins onendothelial function. Trends Cardiovasc Med 2006;16:156-162.
31. Grundy SM, Cleeman JI, Merz CN, et al: Implications of recentclinical trials for the National Cholesterol Education ProgramAdult Treatment Panel III guidelines. Circulation 2004;110:227-239.
32. Willigendael EM, Teijink JA, Bartelink ML, et al: Influence ofsmoking on incidence and prevalence of peripheral arterial disease.J Vasc Surg 2004;40:1158-1165.
33. Price JF, Mowbray PI, Lee AJ, et al: Relationship between smokingand cardiovascular risk factors in the development of peripheralarterial disease and coronary artery disease: Edinburgh ArteryStudy. Eur Heart J 1999;20:344-353.
34. He Y, Lam TH, Jiang B, et al: Passive smoking and risk ofperipheral arterial disease and ischemic stroke in Chinese womenwho never smoked. Circulation 2008;118:1535-1540.
35. Faulkner KW, House AK, Castleden WM: The effect of cessationof smoking on the accumulative survival rates of patients withsymptomatic peripheral vascular disease. Med J Aust 1983;1:217-219.
36. Jonason T, Bergstrom R: Cessation of smoking in patients withintermittent claudication. Effects on the risk of peripheral vascular
complications, myocardial infarction and mortality. Acta MedScand 1987;221:253-260.
37. Lip GY, Makin AJ: Treatment of hypertension in peripheral arterialdisease. Cochrane Database Syst Rev 2003:CD003075.
38. Chobanian AV, Bakris GL, Black HR, et al: The seventh report ofthe Joint National Committee on Prevention, Detection, Evaluation,and Treatment of High Blood Pressure: the JNC 7 report. JAMA2003;289:2560-2572.
39. Singer DR, Kite A: Management of hypertension in peripheralarterial disease: does the choice of drugs matter? Eur J VascEndovasc Surg 2008;35:701-708.
40. Yusuf S, Sleight P, Pogue J, et al: Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events inhigh-risk patients. The Heart Outcomes Prevention EvaluationStudy Investigators. N Engl J Med 2000;342:145-153.
41. Fox KM, EURopean trial On reduction of cardiac events withPerindopril in stable coronary Artery disease Investigators: Efficacyof perindopril in reduction of cardiovascular events among patientswith stable coronary artery disease: randomised, double-blind,placebo-controlled, multicentre trial (the EUROPA study). Lancet2003;362:782-788.
42. Radack K, Deck C: Beta-adrenergic blocker therapy does notworsen intermittent claudication in subjects with peripheral arterialdisease. A meta-analysis of randomized controlled trials. ArchIntern Med 1991;151:1769-1776.
43. Antithrombotic Trialists' Collaboration: Collaborative meta-analy-sis of randomised trials of antiplatelet therapy for prevention ofdeath, myocardial infarction, and stroke in high risk patients. BMJ2002;324:71-86.
44. Berger JS, Krantz MJ, Kittelson JM, et al: Aspirin for theprevention of cardiovascular events in patients with peripheralartery disease: a meta-analysis of randomized trials. JAMA 2009;301:1909-1919.
45. Belch J, MacCuish A, Campbell I, et al: The prevention ofprogression of arterial disease and diabetes (POPADAD) trial:factorial randomised placebo controlled trial of aspirin andantioxidants in patients with diabetes and asymptomatic peripheralarterial disease. BMJ 2008;337:a1840.
46. Ogawa H, Nakayama M, Morimoto T, et al: Low-dose aspirinfor primary prevention of atherosclerotic events in patients withtype 2 diabetes: a randomized controlled trial. JAMA 2008;300:2134-2141.
47. Fowkes FG, Price JF, Stewart MC, et al: Aspirin for prevention ofcardiovascular events in a general population screened for a lowankle brachial index: a randomized controlled trial. JAMA 2010;303:841-848.
48. Dorffler-Melly J, Koopman MM, Adam DJ, et al: Antiplateletagents for preventing thrombosis after peripheral arterial bypasssurgery. Cochrane Database Syst Rev 2003:CD000535.
49. Vivas D, Angiolillo DJ: Platelet P2Y receptor inhibition: an updateon clinical drug development. Am J Cardiovasc Drugs 2010;10:217-226.
50. Zakarija A, Kwaan HC, Moake JL, et al: Ticlopidine- andclopidogrel-associated thrombotic thrombocytopenic purpura(TTP): review of clinical, laboratory, epidemiological, andpharmacovigilance findings (1989-2008). Kidney Int Suppl 2009:S20-S24.
51. A randomised, blinded, trial of clopidogrel versus aspirin in patientsat risk of ischaemic events (CAPRIE). CAPRIE Steering Commit-tee. Lancet 1996;348:1329-1339.
52. Bhatt DL, Fox KA, Hacke W, et al: Clopidogrel and aspirin versusaspirin alone for the prevention of atherothrombotic events. N EnglJ Med 2006;354:1706-1717.
53. Belch JJ, Dormandy J, CASPAR Writing Committee, et al. Resultsof the randomized, placebo-controlled clopidogrel and acetylsa-licylic acid in bypass surgery for peripheral arterial disease(CASPAR) trial. J Vasc Surg 2010;52:825,33, 833.e1-e2.

12 S. Gandhi et al. / Progress in Cardiovascular Diseases 54 (2011) 2–13
54. Montalescot G, Wiviott SD, Braunwald E, et al: Prasugrelcompared with clopidogrel in patients undergoing percutaneouscoronary intervention for ST-elevation myocardial infarction(TRITON-TIMI 38): double-blind, randomised controlled trial.Lancet 2009;373:723-731.
55. Morrow DA, Wiviott SD, White HD, et al: Effect of the novelthienopyridine prasugrel compared with clopidogrel on spontane-ous and procedural myocardial infarction in the Trial to AssessImprovement in Therapeutic Outcomes by Optimizing PlateletInhibition with Prasugrel-Thrombolysis in Myocardial Infarction38: an application of the classification system from the universaldefinition of myocardial infarction. Circulation 2009;119:2758-2764.
56. Anand S, Yusuf S, et al, Warfarin Antiplatelet VascularEvaluation Trial Investigators: Oral anticoagulant and antiplatelettherapy and peripheral arterial disease. N Engl J Med 2007;357:217-227.
57. Murphy TP, Hirsch AT, Ricotta JJ, et al: The Claudication: ExerciseVs. Endoluminal Revascularization (CLEVER) study: rationale andmethods. J Vasc Surg 2008;47:1356-1363.
58. McDermott MM, Greenland P, Liu K, et al: The ankle brachialindex is associated with leg function and physical activity: theWalking and Leg Circulation Study. Ann Intern Med 2002;136:873-883.
59. McDermott MM, Liu K, Greenland P, et al: Functional decline inperipheral arterial disease: associations with the ankle brachialindex and leg symptoms. JAMA 2004;292:453-461.
60. McDermott MM, Guralnik JM, Tian L, et al: Baseline functionalperformance predicts the rate of mobility loss in persons withperipheral arterial disease. J Am Coll Cardiol 2007;50:974-982.
61. Bendermacher BL, Willigendael EM, Nicolai SP, et al: Supervisedexercise therapy for intermittent claudication in a community-basedsetting is as effective as clinic-based. J Vasc Surg 2007;45:1192-1196.
62. McDermott MM, Ades P, Guralnik JM, et al: Treadmill exerciseand resistance training in patients with peripheral arterial diseasewith and without intermittent claudication: a randomized controlledtrial. JAMA 2009;301:165-174.
63. Spronk S, Bosch JL, den Hoed PT, et al: Cost-effectiveness ofendovascular revascularization compared to supervised hospital-based exercise training in patients with intermittent claudication: arandomized controlled trial. J Vasc Surg 2008;48:1472-1480.
64. Gardner AW, Poehlman ET: Exercise rehabilitation programs forthe treatment of claudication pain. A meta-analysis. JAMA 1995;274:975-980.
65. Mora S, Cook N, Buring JE, et al: Physical activity and reduced riskof cardiovascular events: potential mediating mechanisms. Circu-lation 2007;116:2110-2118.
66. Thompson PD, Franklin BA, Balady GJ, et al: Exercise and acutecardiovascular events placing the risks into perspective: a scientificstatement from the American Heart Association Council onNutrition, Physical Activity, and Metabolism and the Council onClinical Cardiology. Circulation 2007;115:2358-2368.
67. van Kuijk JP, Flu WJ, Chonchol M, et al: Metabolic syndrome is anindependent predictor of cardiovascular events in high-risk patientswith occlusive and aneurysmatic peripheral arterial disease.Atherosclerosis 2010;210:596-601.
68. Giugliano G, Brevetti G, Laurenzano E, et al: The prognosticimpact of general and abdominal obesity in peripheral arterialdisease. Int J Obes (Lond) 2010;34:280-286.
69. Karason K, Peltonen M, Lindroos AK, et al: Effort-related calf painin the obese and long-term changes after surgical obesity treatment.Obes Res 2005;13:137-145.
70. Giles KA, Hamdan AD, Pomposelli FB, et al: Body mass index:surgical site infections and mortality after lower extremity bypassfrom the National Surgical Quality Improvement Program 2005-2007. Ann Vasc Surg 2010;24:48-56.
71. Chapman TM, Goa KL: Cilostazol: a review of its use inintermittent claudication. Am J Cardiovasc Drugs 2003;3:117-138.
72. ElamMB,Heckman J, Crouse JR, et al: Effect of the novel antiplateletagent cilostazol on plasma lipoproteins in patients with intermittentclaudication. Arterioscler Thromb Vasc Biol 1998;18:1942-1947.
73. Otsuki M, Saito H, Xu X, et al: Cilostazol represses vascular celladhesion molecule-1 gene transcription via inhibiting NF-kappaBbinding to its recognition sequence. Atherosclerosis 2001;158:121-128.
74. Hsieh CJ, Wang PW: Effect of cilostazol treatment on adiponectinand soluble CD40 ligand levels in diabetic patients with peripheralarterial occlusion disease. Circ J 2009;73:948-954.
75. Soga Y, Yokoi H, Kawasaki T, et al: Efficacy of cilostazol afterendovascular therapy for femoropopliteal artery disease in patientswith intermittent claudication. J Am Coll Cardiol 2009;53:48-53.
76. Pande RL, Hiatt WR, Zhang P, et al: A pooled analysis of thedurability and predictors of treatment response of cilostazol inpatients with intermittent claudication. Vasc Med 2010;15:181-188.
77. Thompson PD, Zimet R, Forbes WP, et al: Meta-analysis of resultsfrom eight randomized, placebo-controlled trials on the effect ofcilostazol on patients with intermittent claudication. Am J Cardiol2002;90:1314-1319.
78. Robless P, Mikhailidis DP, Stansby GP: Cilostazol for peripheralarterial disease. Cochrane Database Syst Rev 2008:CD003748.
79. Hiatt WR, Money SR, Brass EP: Long-term safety of cilostazol inpatients with peripheral artery disease: the CASTLE study (Cilostazol:A Study in Long-term Effects). J Vasc Surg 2008;47:330-336.
80. Dawson DL, Cutler BS, Hiatt WR, et al: A comparison of cilostazoland pentoxifylline for treating intermittent claudication. Am J Med2000;109:523-530.
81. Boccalon H, Lehert P, Mosnier M: Effect of naftidrofuryl onphysiological walking distance in patients with intermittentclaudication. Ann Cardiol Angeiol (Paris) 2001;50:175-182.
82. Kieffer E, Bahnini A, Mouren X, et al: A new study demonstratesthe efficacy of naftidrofuryl in the treatment of intermittentclaudication. Findings of the Naftidrofuryl Clinical IschemiaStudy (NCIS). Int Angiol 2001;20:58-65.
83. Leng G: Cilostazol, naftidrofuryl oxalate, pentoxifylline andinositol nicotinate for the treatment of intermittent claudication inpatients with peripheral arterial disease. http://guidance.nice.org.uk/TA/Wave22/8.
84. Marchesi S, Pasqualini L, Lombardini R, et al: ProstaglandinE1 improves endothelial function in critical limb ischemia. JCardiovasc Pharmacol 2003;41:249-253.
85. Ruffolo AJ, Romano M, Ciapponi A: Prostanoids for critical limbischaemia. Cochrane Database Syst Rev 2010:CD006544.
86. Pittler MH, Ernst E: Ginkgo biloba extract for the treatment ofintermittent claudication: a meta-analysis of randomized trials. AmJ Med 2000;108:276-281.
87. Nicolai SP, Kruidenier LM, Bendermacher BL, et al: Ginkgo bilobafor intermittent claudication. Cochrane Database Syst Rev 2009:CD006888.
88. Wilson AM, Harada R, Nair N, et al: L-arginine supplementation inperipheral arterial disease: no benefit and possible harm. Circulation2007;116:188-195.
89. Sommerfield T, Price J, Hiatt WR: Omega-3 fatty acids for inter-mittent claudication. Cochrane Database Syst Rev 2007:CD003833.
90. de Backer TL, Bogaert M, Vander Stichele R: Buflomedil forintermittent claudication. Cochrane Database Syst Rev 2008:CD000988.
91. Norgren L, Jawien A, Matyas L, et al: Sarpogrelate, a 5-hT2Areceptor antagonist in intermittent claudication. A phase IIEuropean study. Vasc Med 2006;11:75-83.
92. Arosio E, De Marchi S, Zannoni M, et al: Effect of gluta-thione infusion on leg arterial circulation, cutaneous micro-circulation, and pain-free walking distance in patients withperipheral obstructive arterial disease: a randomized, double-
13S. Gandhi et al. / Progress in Cardiovascular Diseases 54 (2011) 2–13
blind, placebo-controlled trial. Mayo Clin Proc 2002;77:754-759.
93. Nenci GG, Gresele P, Ferrari G, et al: Treatment of intermittentclaudication with mesoglycan–a placebo-controlled, double-blindstudy. Thromb Haemost 2001;86:1181-1187.
94. Reiter M, Bucek RA, Stumpflen A, et al: Prostanoids forintermittent claudication. Cochrane Database Syst Rev 2004:CD000986.
95. Mohler III ER, Hiatt WR, Olin JW, et al: Treatment of intermittentclaudication with beraprost sodium, an orally active prostaglandinI2 analogue: a double-blinded, randomized, controlled trial. J AmColl Cardiol 2003;41:1679-1686.
96. van Rij AM, Solomon C, Packer SG, et al: Chelation therapy forintermittent claudication. A double-blind, randomized, controlledtrial. Circulation 1994;90:1194-1199.
97. Kleijnen J, Mackerras D: Vitamin E for intermittent claudication.Cochrane Database Syst Rev 2000:CD000987.
98. Sesso HD, Buring JE, Christen WG, et al: Vitamins E and C inthe prevention of cardiovascular disease in men: the Physicians'Health Study II randomized controlled trial. JAMA 2008;300:2123-2133.
99. Jaff MR, Dale RA, Creager MA, et al: Anti-chlamydial antibiotictherapy for symptom improvement in peripheral artery disease:prospective evaluation of rifalazil effect on vascular symptoms ofintermittent claudication and other endpoints in Chlamydiapneumoniae seropositive patients (PROVIDENCE-1). Circulation2009;119:452-458.
100. Sneider EB, Nowicki PT, Messina LM: Regenerative medicinein the treatment of peripheral arterial disease. J Cell Biochem 2009;108:753-761.
101. Gupta R, Tongers J, Losordo DW: Human studies of angiogenicgene therapy. Circ Res 2009;105:724-736.
102. Isner JM, Pieczek A, Schainfeld R, et al: Clinical evidence ofangiogenesis after arterial gene transfer of phVEGF165 in patientwith ischaemic limb. Lancet 1996;348:370-374.
103. Baumgartner I, Pieczek A, Manor O, et al: Constitutive expressionof phVEGF165 after intramuscular gene transfer promotescollateral vessel development in patients with critical limb ischemia.Circulation 1998;97:1114-1123.
104. Lederman RJ, Mendelsohn FO, Anderson RD, et al: Therapeuticangiogenesis with recombinant fibroblast growth factor-2 forintermittent claudication (the TRAFFIC study): a randomisedtrial. Lancet 2002;359:2053-2058.
105. Rajagopalan S, Mohler III ER, Lederman RJ, et al: Regionalangiogenesis with vascular endothelial growth factor in peripheralarterial disease: a phase II randomized, double-blind, controlled studyof adenoviral delivery of vascular endothelial growth factor 121 inpatients with disabling intermittent claudication. Circulation 2003;108:1933-1938.
106. Nikol S, Baumgartner I, Van Belle E, et al: Therapeuticangiogenesis with intramuscular NV1FGF improves amputation-free survival in patients with critical limb ischemia. Mol Ther 2008;16:972-978.
107. Hiatt WR: TAMARIS phase III NV 1 FGF gene therapy onamputation-free survival in critical limb ischemia-phase IIIrandomized double-blind placebo controlled trial. Clinical trialpresented at Scientific Sessions of the American Heart AssociationNov 14-17, 2010, in Chicago.
108. Tateishi-Yuyama E, Matsubara H, Murohara T, et al: Therapeuticangiogenesis for patients with limb ischaemia by autologoustransplantation of bone-marrow cells: a pilot study and arandomised controlled trial. Lancet 2002;360:427-435.
109. Huang PP, Li SZ, Han MZ, et al: Autologous transplantation ofperipheral blood stem cells as an effective therapeutic approach forsevere arteriosclerosis obliterans of lower extremities. ThrombHaemost 2004;91:606-609.
110. Huang P, Li S, Han M, et al: Autologous transplantation ofgranulocyte colony-stimulating factor-mobilized peripheral bloodmononuclear cells improves critical limb ischemia in diabetes.Diabetes Care 2005;28:2155-2160.



![ARTERIAL PERIPHERAL VASCULAR DISEASES.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000113-cardiovascular-system/… · arterial peripheral vascular diseases acute arterial occlusion](https://img.pdfslide.us/doc/110x75/604e83caf1418f71db611c5a/arterial-peripheral-vascular-read-onlyocwusuacidcoursedownload1110000113-cardiovascular-system.jpg)