Embed Size (px)
Citation preview

Complications of Prematurity
Jenny Wilson MD Pediatric neurology
Developmental Evaluation Clinic (formally NICU follow-up clinic) at OHSU
wilsjenohsuedu
512014
Outline
bull Definitions
bull Overview of epidemiologyoutcomes
bull Common NICU complications by organ system
bull Common medical concerns after discharge
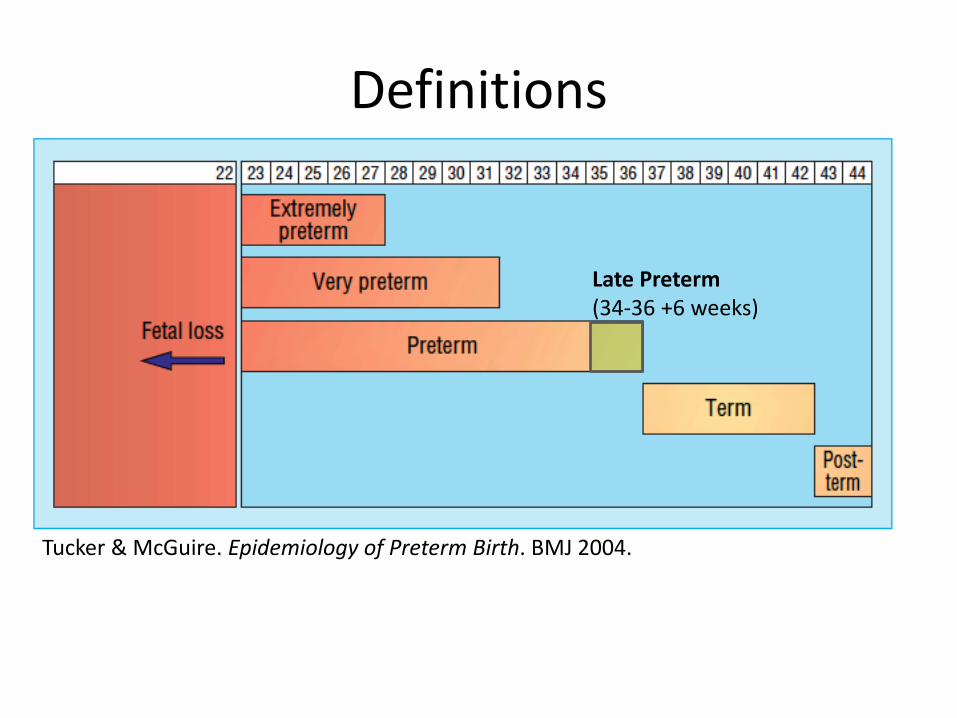
Definitions
Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
Late Preterm (34-36 +6 weeks)
Definitions
Classification Birthweight
Low Birthweight (LBW) lt 2500 grams
Very Low Birthweight (VLBW)
lt 1500 grams
Extremely Low Birthweight (ELBW)
lt 1000 grams
Epidemiology
bull Preterm delivery affects 115 of pregnancies in the United States
Survival
Mortality amp Morbidity
Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
Neonatal Intensive Care Unit (NICU) Complications By Organ System
The Lungs
Respiratory Distress Syndrome (RDS)
bull Gas exchange occurs in the alveoli
bull Surfactant a detergent keeps the alveoli open by decreasing surface tension
bull Surfactant deficiency results in collapse of the alveoli
bull Surfactant is not produced well before 30-32 weeks
bull Surfactant deficiency results in respiratory failure (RDS)
Respiratory Distress Syndrome (RDS)
ndash Occurs in 10 increasing with decreasing gestational age
ndash A leading cause of morbiditymortality in premature babies
ndash Treatment
bull Prenatal steroids
bull Postnatal
ndash Surfactant replacement therapy
ndash Respiratory support (mechanical ventilation)
Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118
Outline
bull Definitions
bull Overview of epidemiologyoutcomes
bull Common NICU complications by organ system
bull Common medical concerns after discharge
Definitions
Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
Late Preterm (34-36 +6 weeks)
Definitions
Classification Birthweight
Low Birthweight (LBW) lt 2500 grams
Very Low Birthweight (VLBW)
lt 1500 grams
Extremely Low Birthweight (ELBW)
lt 1000 grams
Epidemiology
bull Preterm delivery affects 115 of pregnancies in the United States
Survival
Mortality amp Morbidity
Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
Neonatal Intensive Care Unit (NICU) Complications By Organ System
The Lungs
Respiratory Distress Syndrome (RDS)
bull Gas exchange occurs in the alveoli
bull Surfactant a detergent keeps the alveoli open by decreasing surface tension
bull Surfactant deficiency results in collapse of the alveoli
bull Surfactant is not produced well before 30-32 weeks
bull Surfactant deficiency results in respiratory failure (RDS)
Respiratory Distress Syndrome (RDS)
ndash Occurs in 10 increasing with decreasing gestational age
ndash A leading cause of morbiditymortality in premature babies
ndash Treatment
bull Prenatal steroids
bull Postnatal
ndash Surfactant replacement therapy
ndash Respiratory support (mechanical ventilation)
Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118
Definitions
Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
Late Preterm (34-36 +6 weeks)
Definitions
Classification Birthweight
Low Birthweight (LBW) lt 2500 grams
Very Low Birthweight (VLBW)
lt 1500 grams
Extremely Low Birthweight (ELBW)
lt 1000 grams
Epidemiology
bull Preterm delivery affects 115 of pregnancies in the United States
Survival
Mortality amp Morbidity
Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
Neonatal Intensive Care Unit (NICU) Complications By Organ System
The Lungs
Respiratory Distress Syndrome (RDS)
bull Gas exchange occurs in the alveoli
bull Surfactant a detergent keeps the alveoli open by decreasing surface tension
bull Surfactant deficiency results in collapse of the alveoli
bull Surfactant is not produced well before 30-32 weeks
bull Surfactant deficiency results in respiratory failure (RDS)
Respiratory Distress Syndrome (RDS)
ndash Occurs in 10 increasing with decreasing gestational age
ndash A leading cause of morbiditymortality in premature babies
ndash Treatment
bull Prenatal steroids
bull Postnatal
ndash Surfactant replacement therapy
ndash Respiratory support (mechanical ventilation)
Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Definitions
Classification Birthweight
Low Birthweight (LBW) lt 2500 grams
Very Low Birthweight (VLBW)
lt 1500 grams
Extremely Low Birthweight (ELBW)
lt 1000 grams
Epidemiology
bull Preterm delivery affects 115 of pregnancies in the United States
Survival
Mortality amp Morbidity
Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
Neonatal Intensive Care Unit (NICU) Complications By Organ System
The Lungs
Respiratory Distress Syndrome (RDS)
bull Gas exchange occurs in the alveoli
bull Surfactant a detergent keeps the alveoli open by decreasing surface tension
bull Surfactant deficiency results in collapse of the alveoli
bull Surfactant is not produced well before 30-32 weeks
bull Surfactant deficiency results in respiratory failure (RDS)
Respiratory Distress Syndrome (RDS)
ndash Occurs in 10 increasing with decreasing gestational age
ndash A leading cause of morbiditymortality in premature babies
ndash Treatment
bull Prenatal steroids
bull Postnatal
ndash Surfactant replacement therapy
ndash Respiratory support (mechanical ventilation)
Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Epidemiology
bull Preterm delivery affects 115 of pregnancies in the United States
Survival
Mortality amp Morbidity
Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
Neonatal Intensive Care Unit (NICU) Complications By Organ System
The Lungs
Respiratory Distress Syndrome (RDS)
bull Gas exchange occurs in the alveoli
bull Surfactant a detergent keeps the alveoli open by decreasing surface tension
bull Surfactant deficiency results in collapse of the alveoli
bull Surfactant is not produced well before 30-32 weeks
bull Surfactant deficiency results in respiratory failure (RDS)
Respiratory Distress Syndrome (RDS)
ndash Occurs in 10 increasing with decreasing gestational age
ndash A leading cause of morbiditymortality in premature babies
ndash Treatment
bull Prenatal steroids
bull Postnatal
ndash Surfactant replacement therapy
ndash Respiratory support (mechanical ventilation)
Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Survival
Mortality amp Morbidity
Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
Neonatal Intensive Care Unit (NICU) Complications By Organ System
The Lungs
Respiratory Distress Syndrome (RDS)
bull Gas exchange occurs in the alveoli
bull Surfactant a detergent keeps the alveoli open by decreasing surface tension
bull Surfactant deficiency results in collapse of the alveoli
bull Surfactant is not produced well before 30-32 weeks
bull Surfactant deficiency results in respiratory failure (RDS)
Respiratory Distress Syndrome (RDS)
ndash Occurs in 10 increasing with decreasing gestational age
ndash A leading cause of morbiditymortality in premature babies
ndash Treatment
bull Prenatal steroids
bull Postnatal
ndash Surfactant replacement therapy
ndash Respiratory support (mechanical ventilation)
Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118
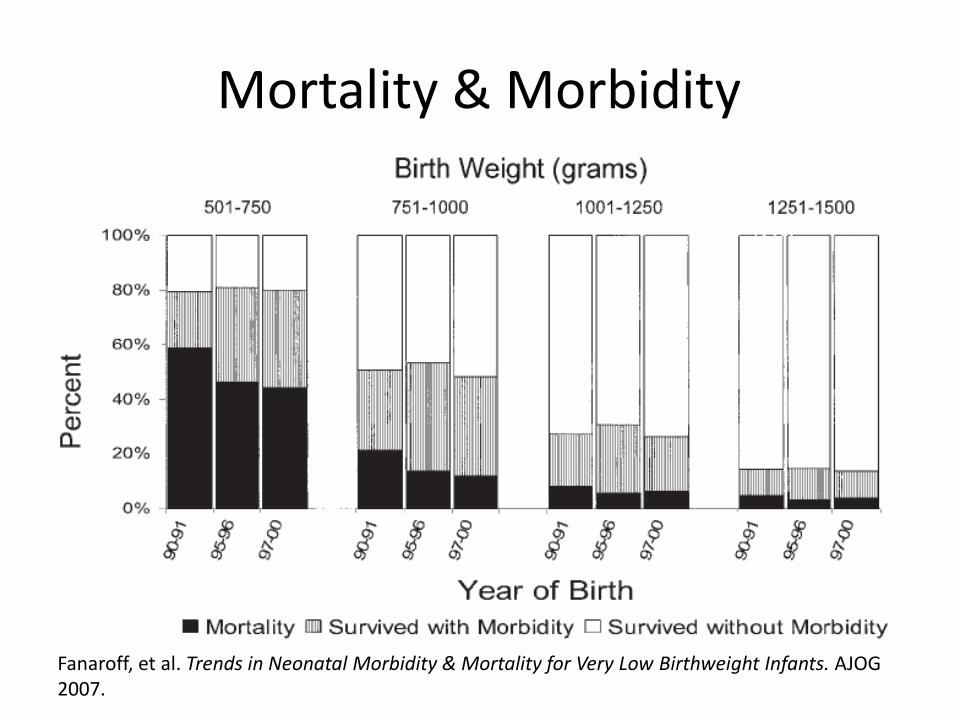
Mortality amp Morbidity
Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
Neonatal Intensive Care Unit (NICU) Complications By Organ System
The Lungs
Respiratory Distress Syndrome (RDS)
bull Gas exchange occurs in the alveoli
bull Surfactant a detergent keeps the alveoli open by decreasing surface tension
bull Surfactant deficiency results in collapse of the alveoli
bull Surfactant is not produced well before 30-32 weeks
bull Surfactant deficiency results in respiratory failure (RDS)
Respiratory Distress Syndrome (RDS)
ndash Occurs in 10 increasing with decreasing gestational age
ndash A leading cause of morbiditymortality in premature babies
ndash Treatment
bull Prenatal steroids
bull Postnatal
ndash Surfactant replacement therapy
ndash Respiratory support (mechanical ventilation)
Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118
Neonatal Intensive Care Unit (NICU) Complications By Organ System
The Lungs
Respiratory Distress Syndrome (RDS)
bull Gas exchange occurs in the alveoli
bull Surfactant a detergent keeps the alveoli open by decreasing surface tension
bull Surfactant deficiency results in collapse of the alveoli
bull Surfactant is not produced well before 30-32 weeks
bull Surfactant deficiency results in respiratory failure (RDS)
Respiratory Distress Syndrome (RDS)
ndash Occurs in 10 increasing with decreasing gestational age
ndash A leading cause of morbiditymortality in premature babies
ndash Treatment
bull Prenatal steroids
bull Postnatal
ndash Surfactant replacement therapy
ndash Respiratory support (mechanical ventilation)
Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

The Lungs
Respiratory Distress Syndrome (RDS)
bull Gas exchange occurs in the alveoli
bull Surfactant a detergent keeps the alveoli open by decreasing surface tension
bull Surfactant deficiency results in collapse of the alveoli
bull Surfactant is not produced well before 30-32 weeks
bull Surfactant deficiency results in respiratory failure (RDS)
Respiratory Distress Syndrome (RDS)
ndash Occurs in 10 increasing with decreasing gestational age
ndash A leading cause of morbiditymortality in premature babies
ndash Treatment
bull Prenatal steroids
bull Postnatal
ndash Surfactant replacement therapy
ndash Respiratory support (mechanical ventilation)
Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Respiratory Distress Syndrome (RDS)
bull Gas exchange occurs in the alveoli
bull Surfactant a detergent keeps the alveoli open by decreasing surface tension
bull Surfactant deficiency results in collapse of the alveoli
bull Surfactant is not produced well before 30-32 weeks
bull Surfactant deficiency results in respiratory failure (RDS)
Respiratory Distress Syndrome (RDS)
ndash Occurs in 10 increasing with decreasing gestational age
ndash A leading cause of morbiditymortality in premature babies
ndash Treatment
bull Prenatal steroids
bull Postnatal
ndash Surfactant replacement therapy
ndash Respiratory support (mechanical ventilation)
Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Respiratory Distress Syndrome (RDS)
ndash Occurs in 10 increasing with decreasing gestational age
ndash A leading cause of morbiditymortality in premature babies
ndash Treatment
bull Prenatal steroids
bull Postnatal
ndash Surfactant replacement therapy
ndash Respiratory support (mechanical ventilation)
Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Bronchopulmonary Dysplasia (BPD) also known as Chronic Lung Disease (CLD)
bull Abnormal alveolar formationinjury in premies who had RDS from mechanical ventilationhigh oxygen concentration
bull Defined as requiring oxygen at 36 weeks post-conceptual age
Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Symptoms ndash Increased work of breathing ndash Oxygen requirement ndash Growth failure ndash Can result in pulmonary hypertension and heart
failure Treatment - Respiratory support - Diuretics - Bronchodilators (albuterol) inhaled steroids - Systemic steroids (though worsens
neurodevelopmental outcomes) - Maximize nutrition (often have high caloric needs)
BPD
Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Apnea of Prematurity
bull Premature infants may stop breathing for 20 seconds or more may be followed by drop in heart rate and oxygen saturation
bull May be treated with caffeine
bull Typically but not always resolves by term
The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

The Heart
Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Patent Ductus Arteriosus (PDA)
ndash In fetal life the ductus shunts blood away from the lungs and to the body (placenta does the job of the lungs)
ndash The ductus closes within 48 hours of birth
- Premature babies are at high risk of the ductus not closing (PDA)- occurs in 30 of VLBW infants - This can result in worsening of pulmonary function higher rates of BPD IVH and NEC heart failure - Treatment conservative indomethacin or surgical ligation
Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Gastrointestinal
Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Necrotizing enterocolitis (NEC)
bull Bacterial infection of intestines leading to inflammation amp necrosis
bull Occurs in 6-7 of VLBW infants bull Presents with feeding intolerance blood in stools
apnea and other nonspecific signs bull Can result in bowel perforation septic shock bull Management
ndash Medical antibiotics supportive ndash Surgical resection with ostomy placement or placement of
peritoneal drain
bull Complications death (20-30) stricture formation short gut syndrome (9) frequentloose stools impaired growth worse neurodevelopmental outcome
The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

The Eyes
Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Retinopathy of Prematurity (ROP)
ndash Retinal blood vessels are sensitive to stress which can cause them to stop growing
ndash When they start growing again it is abnormal excessive growth called ROP
ndash Eyes need to be examined until retina are completely vascularized
ndash Abnormal vessels may regress or can progress to retinal detachment vision loss
ndash Treated with laser ablation if severe
The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

The Brain
24 weeks
Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Intraventricular Hemorrhage (IVH)
ndash Bleeding in the periventricular germinal matrix (a layer of neuronal precursor cells)
ndash Classification (Grades)
bull I germinal matrix hemorrhage
bull II IVH without ventricular dilation
bull III IVH with ventricular dilation
bull IV IVH with parenchymal involvement
ndash Treatment
bull Supportive
bull Shunting for hydrocephalus
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118
IVH and Neurodevelopmental Outcomes
bull Grades I-II
ndash Developmental delay 8
ndash Cerebral palsy 105
bull Grades III-IV
ndash Developmental delay 175
ndash Cerebral palsy 30
bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

bull Necrosis of periventricular white matter resulting from cerebral hypoperfusion and oligodendrocyte vulnerability
bull Ocurs in 6 of VLBW babies on ultrasound
bull More than half of patients with cystic PVL develop cerebral palsy classically spastic diplegia (affecting the lower extremities)
Periventricular Leukomalacia (PVL)
Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Discharge
bull Most premies are discharged when they reach term
bull Parents typically asked to stay 1-2 nights with their baby in the hospital
bull Many have significant ongoing medical needs after discharge
bull First clinic visit within one week of discharge
bull Need a pediatrician able to care for the complicated needs of a premie
Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Monitoring
bull Growth
bull Vaccinations ndash Palivizumab (Synagis) in high-risk infants
bull Hearing
bull Vision
bull Development
bull Respiratory
bull Parentalsocial concerns
bull Safety higher rates of SIDS in premature babies
Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Which baby is safest
A B
C D E
LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

LungsRespiratory
BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

BPD after discharge
bull Infants with BPD - 50 higher rates of rehospitalization in the first year after
bull Higher rates of respiratory infections
bull Higher rates of asthma
bull Higher caloric needs
ndash 30 to 65 of infants with BPD experience growth failure soon after initial hospital discharge
bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

bull May be on oxygen diuretics albuterol
bull Will often need follow-up with pulmonology
bull Monitor ndash Respiratory status
ndash Growthnutrition (may need 25 more calories)
ndash Electrolytes if on diuretics
ndash Sometimes cardiac monitoring
bull Typically becomes less problematic after the first two years
BPD Management
The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

The Heart after discharge
ndash Infants with BPD at risk for pulmonary hypertension and right heart failure
ndash At higher risk for later
bull Hypertension
ndash already at school age BP higher in premature children
ndash Extreme prematurity (23ndash27 weeks) associated with a 25-fold increased rate of BP medication in young adulthood compared with full-term birth
bull Cardiovascular disease
bull Type 2 diabetes
Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Anemia
bull Term babies have a dip in hemoglobin (physiologic anemia) at 8-12 weeks
bull Premature babies have more severe anemia
bull The AAP recommendation is to treat premature and LBW infants with iron if breastfed
Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Gastroesophageal Reflux
bull Reflux is common in premature infants
bull If ldquocauses morbidityrdquo called GERD
(D=disease) ndash Discomfort duringafter feeds
ndash Respiratory difficulties
ndash Failure to thrive
bull If the above symptoms are present treat ndash Change feeding frequencypositioning
ndash Medication H2 blockers (raniditine) or PPI (omeprazole)
ndash Rarely jejunal feeding or surgery (nissen fundoplication)
ndash Often resolves by one year
Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Vision
bull Preterm infants at higher risk for vision problems ndash Decreased acuity 27
ndash Strabismus 13-25
ndash Astigmatism 11 (at 5 years of age)
bull Severe visual impairment or blindness 1ndash2 (26ndash27 weeks) 4ndash8 (lt 25 weeks)
bull 36 of ELBW adolescents wear glasses
bull Premature babies need regular eye exams after discharge
Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Hydrocephalus
ndash Build-up of fluid in the ventricles causing increased pressure
ndash 25 of babies with IVH develop hydrocephalus
ndash May require ongoing monitoring after discharge
ndash Monitor head circumference
ndash Signs of increased ICP bull Bulging fontanelle
bull Vomiting
bull Lethargy
ndash May require ventriculoperitoneal shunt (VPS) placement
Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Neurodevelopment Case
bull 4 year-old boy who was born at 25 weeks twin pregnancy PDA RDS ROP
bull At 4 years
ndash Expressive language disorder (childhood apraxia of speech) requiring 3 xwk speech therapy
ndash Developmental coordination disorder
ndash Strabismus sp two eye surgeries wears glasses and has some difficulties with judging distances
ndash Mild cognitive disability
ndash Some inattentionhyperactivity
Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Who is at risk for abnormal neurodevelopmental outcomes
bull Higher risk with increasing prematurity decreasing BW
bull IVH particularly grades III-IV
bull Shunted hydrocephalus
bull PVL or other brain injury
bull BPD ROP
Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Who is at risk for abnormal neurodevelopmental outcomes
bull Environment ndash One study found that 45 of
medicaid-insured premies had language delay compared with 8 of privately insured at ~2 yrs (Wild et al Early Hum Dev 2013)
ndash Another study found that preterm infants spoken to more in the NICU had better cognitivelanguage outcomes at 7 and 18 months (Caskey et al
Pediatrics 2014)
Hart and Risley Education Review 2004
Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Developmental Delays
ndash More than 15 SD below the mean or 25 below chronologic age in one or more of the following areas physical cognitive communication social or emotional or adaptive development
ndash Correct for prematurity until around 2 years of age
ndash httpswwwvtoxfordorgresearchelbwcalcreadmeaspx (google ldquoelbw calculatorrdquo)
Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Ages and Stages Questionnaire
Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Approach for the delayed child
bull Environmental enrichment
ndash Teach families to talk to their babies use lots of language singmusic
ndash Tummy time opportunities to be mobile
ndash Age-appropriate toys
bull Referral to early intervention
bull Have hearing and vision been checked
bull Refer to developmental specialist
Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Cerebral Palsy
bull While all premature babies are at risk those with PVL and higher grade IVH (III-IV) are at highest risk
bull Early in infancy they may be hypotonic
bull Delayed motor milestones
bull May have asymmetric reaching at 4-6 months
bull Posturing spasticity clonus develops
bull Diagnosis often reached between 1-2 years sometimes later
Disorder of movement or posture as a result of non-progressive injury in the developing brain
Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Cerebral Palsy
bull Treatment
ndash Manage symptoms of increased muscle tone (medications botox orthopedic surgery)
ndash Provide services PT OT
bull Services for children with disabilities mandated for children under 21 years
bull Children 0-3 years eligible for early intervention
ndash Provide equipment AFOs walkers wheelchairs wrist splints assistive technology etc
ndash Provide supportresources
Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Other Deficits
bull Developmental coordination disorder
ndash Mild gross motor delays and difficulties with coordination
bull Fine motor deficits
bull Language disorders
bull Cognitive deficits
Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Hearing
ndash 6 of 6-year-olds born before 26 weeksrsquo gestation were wearing hearing aids and another 4 had mild hearing loss
Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Behavioral etc
bull ADHD bull Academic issues learning disabilities
ndash 72 of adolescents with a BW lt750 grams had school difficulties)
bull Psychological anxiety and depression bull Autism spectrum disorder
ndash Higher rates among preterm children ndash Consider if lack of expressive language decreased eye
contact no pointing no ldquojoint attentionrdquo ndash Autism screening questionnaires M-CHAT is free online ndash Formal diagnosis done in Autism Clinic or by a trained
psychologist using Autism Diagnostic Observation Schedule (ADOS)
ndash Treatment Applied Behavior Analysis (ABA)
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118
httpswwwm-chatorg_referencesmchatDOTorgpdf
Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Psychosocial bull Psychosocial distress highest for parents of VLBW infants
during the first month of life persisting during the first two years of life
bull Higher effect with low income families with less education and more severely disabled children
bull Vulnerable child syndrome ndash Parents
bull Overprotective separation anxiety are unable to set limits have excessive concerns about their childrsquos health overuse medical services
ndash Children bull Sleep disorders school problems behavior problems
ndash Treatment bull uncovering the source of the parentsrsquo anxiety and re-educating them
about their childrsquos health regular visits with PMD may need therapy
Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118

Summary
bull Prematurity is common and has high morbidity and mortality
bull All organ systems are vulnerable to complications of prematurity
bull Premature babies often need closer monitoring after discharge and have higher health care needsutilization
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118
References bull Ritu Chitkara MD
bull Tucker amp McGuire Epidemiology of Preterm Birth BMJ 2004
bull Saigal et al An overview of mortality and sequelae of preterm birth from infancy to adulthood Vol 371 January 19 2008
bull Fanaroff et al Trends in Neonatal Morbidity amp Mortality for Very Low Birthweight Infants AJOG 2007
bull William Engle Surfactant-Replacement Therapy for Respiratory Distress in the Preterm and Term Neonate Pediatrics Vol 121 No 2 February 1 2008 pp 419 -432
bull Kair et al Bronchopulmonary Dysplasia Pediatrics in Review 201233255
bull UpToDate
bull Bolisetty et al Intraventricular hemorrhage and Neurodevelopmental Outcomes in Extremely Preterm Infants Pediatrics 201413355
bull Carter et al Infants in a neonatal intensive care unit parental response Arch Dis Child Fetal Neonatal Ed 200590
bull Howell and Graham Parentsrsquo Experiences of Neonatal Care Nov 2011 Picker Institute Europe
bull Doyle LW Faber B Callanan C Morley R Blood pressure in late adolescence and very low birth weight Pediatrics 2003 111 252ndash57
bull Hack M Schluchter M Cartar L Rahman M Blood pressure among very low birth weight (lt1middot5 kg) young adults Pediatr Res 2005 58 677ndash84 Keijzer-Veen MG Finken MJJ Nauta J Group obotDP-CS
bull Risk of Hypertension Among Young Adults Who Were Born Preterm A Swedish National Study of 636000 Births Am J Epidemiol (2011) 173 (7) 797-803
bull Early Hum Dev 2013 Sep89(9)743-6 doi 101016jearlhumdev201305008 Epub 2013 Jun 23 The effect of socioeconomic status on the language outcome of preterm infants at toddler age Wild KT1 Betancourt LM Brodsky NL Hurt H Pediatrics
bull 2014 Mar133(3)e578-84 doi 101542peds2013-0104 Epub 2014 Feb 10 Adult talk in the NICU with preterm infants and developmental outcomes Caskey M1 Stephens B Tucker R Vohr B
bull Hart B amp Risley TR ldquoThe Early Catastropherdquo (2004) Education Review 77 (1) 100-118