Embed Size (px)
Citation preview

Complications of Cirrhosis
Alan Bonder, MDAssistant Professor of Medicine
Harvard Medical SchoolBeth Israel Deaconess Medical CenterCOPYRIG
HT

Disclosures
• NO conflict of interests to disclose
COPYRIG
HT

Objectives
• Recognize and manage complications from cirrhosis
• Diagnostic tests for patients with cirrhosis
• Screening tests for patients with cirrhosis
COPYRIG
HT

Cirrhosis
• The prevalence of cirrhosis, both worldwide and in the US, is unknown1
– Cirrhosis is an outcome of a variety of causes, and the underlying cause is commonly used for surveillance purposes 2
– Compensated cirrhosis often goes undetected for prolonged periods of time1
• Experts estimate that 5.5 million people in the United States have cirrhosis1. Schuppan D, Afdhal NH. Lancet 2008;371(9615):838-851.2. Available at http://pubs.niaaa.nih.gov/publications/surveillance83/Cirr05.htm. Accessed 01/15/12. 3. Khungar V, Poordad F. Clin Liver Dis 2012;16:73-89
COPYRIG
HT

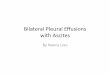
Decrease in local vasodilators withincrease of local vasoconstrictors
Decreased systemic vascular resistance
CIRRHOSISPortal hypertension
Splanchnic arterial vasodilation
Arterial underfilling
Stimulation of systemic vasoconstrictors
Renal vasoconstriction
Increased systemic andlocal vasodilators
Preserved renalperfusionHepatorenal Syndrome
Early Stages of CirrhosisLate Stages of Cirrhosis
RAAS SNS AVP
Cardenas et al, Schiff�s disease of the liver ,2002
Varices
AscitesCOPYRIG
HT

Complications of Cirrhosis• Primary complications of cirrhosis include
– Ascites– Jaundice– Variceal hemorrhage– Hepatic encephalopathy
• Other complications that can occur include– Hepatocellular carcinoma – Spontaneous bacterial peritonitis– Hepatic hydrothorax– Hepatorenal syndrome – Portopulmonary hypertension– Portal vein thrombosis – Hepatopulmonary syndrome
Lefton HB et al. Med Clin N Am 2009;93:787-799.
COPYRIG
HT

Outcome of complications(survival)
Complication Survival at 1 year Survival at 3 yearsNon bleeding varices w/o ascites 1
97% ND
Ascites � varices 1, 2 80%� 50%
Bleeding varices � ascites 1 43% ND
Hepatic encephalopathy 3 42% 23%
1. Adapted from D’Amico G et al. J Hepatol 2006;44:217-231. 2. Arroyo V, Colmenero J. J Hepatol. 2003;38:S69-S89.3. Adapted from Bustamante et al. J Hepatol. 1999;30:890-895.
COPYRIG
HT

Assessment of severity/prognosis
• CPT score– Ascites (none = 1, present = 2, tense =3)– Encephalopathy (none = 1, I-II = 2, III-IV = 3)– INR (< 1.7 = 1, 1.71-2.2 = 2, > 2.2 = 3)– Bili (< 2 = 1, 2-3 = 2, > 3 = 3) – Alb (> 3.5 = 1, 2.8-3.5 = 2, < 2.8 = 3)
• MELD score– 0.957 X log (serum creatinine) + 0.378 X log (serum bilirubin) + 1.120 X log
(INR)
COPYRIG
HT

EVALUATION OF CIRRHOSISassessing prognosis
Child�s (Pugh) Turcotte score
• Empirically developed• Modified in 1972• Predicts survival (1 & 2yr)
– A (5-6) 100%, 85%– B (7-9) 80%, 60%– C (10-15) 45%, 35%
• Limitations– Subjective assessment– Not a continuous severity
score
MELD• 231 patients undergoing
TIPS at 4 US centers• Predicts death within 3
months• Adopted for liver allocation
in Feb 27 2002COPYRIG
HT

Severity of liver cirrhosis• Prognosis is dependent Compensated verses Decompensated
– Dependent on development of ascites, variceal bleeding, jaundice or encephalopathy
• New classification (to improve prognostication)
Stage Description 1 year mortality1 Compensated cirrhosis with no esophageal
varices1%
2 Compensated cirrhosis with esophageal varices
3.4%
3 Cirrhosis with ascites 20%
4 Cirrhosis with gastrointestinal bleeding 57%
5 Cirrhosis with infection and renal failure 67%
D�Amico et al. J Hepatol 2006; 44: 217-231Arvaniti et al. Gastro 2010; 139; 1246-1256
COPYRIG
HT

Ascites
• Most common complications of cirrhosis– 60% of patients with compensated
cirrhosis develop ascites within 10 years
• 50% mortality within 3 years• Liver Transplant should be consideredCOPYRIG
HT

Prognosis of Patients with Cirrhosis at Onset of Ascites
Arroyo V, Colmenero J. J Hepatol. 2003;38:S69-S89.
COPYRIG
HT

Tests for patients with new ascites
COPYRIG
HT

Management of AscitesFirst-Line TherapyTense ascites
Paracentesis
Sodium restriction(<2 Gm/24 Hrs)and diuretics*
Non-tense ascites
*Diuretics: Spironolactone 100 mg/day,furosemide 40 mg/day or bumetanide1 mg/day; uptitrate stepwise to spironolactone 400 mg/day, furosemide160 mg/day or bumetanide 4 mg/day astolerated
RefractoryAscites 10 %
Second-Line Therapy• Repeated large volume paracentesis (LVP)�
• TIPS
• Liver Transplantation�Albumin infusion of 6-8 gm/liter of fluid removed is a consideration for repeated LVP; post-paracentesis albumin infusionmay not be necessary for < 5 liters removed
Adapted from Runyon BA. Hepatology. 2009; 49:2087-2107.
COPYRIG
HT

Refractory ascites
COPYRIG
HT

Management of AscitesProbability of survival without transplantation in patients assigned to TIPS
and in those assigned to paracentesis plus albumin.
Hepatology 2004;40;629 NEJM 2000;342:1701-1707
COPYRIG
HT

Norfloxacin prevents SBP & HRS and improves survival
Probability of developing SBP Probability of developing HRS
Fernandez et al. Gastroenterology 2007; 133: 818
COPYRIG
HT

Treatment of SBP• 1.5 gr/kg at diagnosis and 1gr/kg 48 hours later
30
RENAL IMPAIRMENT (%)
20
0CEFOTAXIME CEFOTAXIME
+ALBUMIN
10
HOSPITAL MORTALITY (%)
30
20
0CEFOTAXIME
10
CEFOTAXIME+
ALBUMIN
COPYRIG
HT

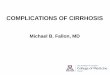
International Ascites Club�s Diagnostic Criteria of Hepatorenal Syndrome.
NEW DIAGNOSTIC CRITERIA FOR HEPATORENAL SYNDROME
1. Cirrhosis with Ascites
2. Serum creatinine > 1.5mg/dl (>133umol/l)
3. No improvement in serum creatinine (decrease to < 1.5mg/dl) after at least 2 days with diuretic withdrawl and volume expansion with albumin 1g/Kg of body weight per day to a maximum of 100g/day
4. Absence of shock
5. No current or recent treatment with nephrotoxic drugs
6. Absence of parenchymal kidney disease as indicated by proteinuria > 500mg/d, microhematuria (> 50 rbc/hpf) and/or abnormal ultrasonography
Salerno et al. Gut 2007;56: 1310-1318
COPYRIG
HT

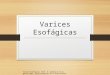
12
Type-2
Type-1
0.0
0.2
0.4
0.6
0.8
1.0
0 8 106
Months42
Pro
babi
lity
p=0.001
Ginès et al, Gastroenterology 1993
Type 1Rapidly progressive reduction of renal function:>100% increase in serum creatinine to > 2.5 mg/dL in lessthan 2 weeks.
Type 2Stable or less progressive reduction of renal function associated with diuretic resistant ascites to a serum creatinine of > 1.5.
COPYRIG
HT

COPYRIG
HT

COPYRIG
HT

COPYRIG
HT

COPYRIG
HT

Hepatic encephalopathy• Covert hepatic encephalopathy (CHE) affects
approximately 20% to 60% of patients with liver disease– Has been called subclinical encephalopathy or minimal
encephalopathy (MHE) in the past– International Society for Hepatic Encephalopathy and
Nitrogen Metabolism has recently endorsed using the term covert encephalopathy
• Overt hepatic encephalopathy (OHE) occurs in– 30% to 45% of cirrhotic patients
– 10% to 50% of patients with TIPS . Mullen KD, et al. Semin Liver Dis. 2007;27(Suppl 2):32-47. Mullen KD, Prakash RK. Clin Liver Dis 2012;16:91-93, Poordad FF. Aliment Pharmacol Ther. 2006;25(Suppl 1):3-9.
COPYRIG
HT

Hospital discharges associated with HE
21% growth
HE = hepatic encephalopathy; ICD = International Classification of Diseases.*Data calculated using ICD-9-CM codes 291.2 (alcoholic dementia, not elsewhere classified), 348.30 (encephalopathy, not otherwise specified), and 572.2 (hepatic coma). †Includes all listed discharge diagnoses.HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville, MD. http://hcupnet.ahrq.gov. Accessed January 2013.
COPYRIG
HT

HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville, MD. http://www.ahrq.gov/HCUPnet/.
$5.9 billion
*Includes codes 348.3 and 572.2
Tota
l Cha
rges
1993-2003$0
$200,000,000
$400,000,000
$600,000,000
$800,000,000
$1,000,000,000
$1,200,000,000
1994 1996 1998 2000 2002 2003
$1,300,000,000
Healthcare costs for HE
COPYRIG
HT

Current Therapy Options for HEDrug Name Drug Class Indication
Lactulose Poorly absorbed disaccharide
• Decrease blood ammoniaconcentration
• Prevention and treatment of portal-systemic encephalopathy
RifaximinNon-aminoglycoside semi-synthetic, nonsystemic antibiotic
Reduction in risk of overt hepatic encephalopathy (HE) recurrence in patients ≥ 18 years of age.
Neomycin Aminoglycoside antibiotic
Not to be used, renal and ototoxic risk
Metronidazole Synthetic antiprotozoal and antibacterial agent Not approved for HE
Vancomycin Aminoglycoside antibiotic Not approved for HE
Adapted from http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/GastrointestinalDrugsAdvisoryCommittee/UCM203247.pdf, accessed 02/17/11 andhttp://www.accessdata.fda.gov/drugsatfda_docs/label/2010/022554lbl.pdf, accessed 02/17/11.
COPYRIG
HT

Rifaximin Trial
COPYRIG
HT

Rifaximin Trial: Time to First Breakthrough HE Episode Primary End
Point
Prop
ortio
n of
Pat
ient
s W
ithou
tB
reak
thro
ugh
HE
(%)
Rifaximin*(77.9%)
Placebo*(54.1%)
*Rifaximin 550 mg or placebo twice daily
Hazard ratio with rifaximin, 0.42 (95% Cl, 0.28–0.64)P<0.001
Days Since RandomizationBass NM et al. N Engl J Med. 2010;362:1071-1081.
COPYRIG
HT

Driving performance with Covert Encephalopathy
COPYRIG
HT

• Varices decompress the hypertensive portal vein
• Threshold pressure of 10-12 mmHg
• Prevalence of EV ranges from 24-81%
• De novo -8% / year -30% @ 6 years
• Progression -25% with small varices
Varices as a consequence of portal hypertension
COPYRIG
HT

0
20
40
60
80
100
RW Absent Moderate SevereCPT score A B C
s m l s m ls m l
% b
leed
NIEC. N. Engl.J. Med. 1988; 319: 983
Predicting risk of variceal hemorrhage
COPYRIG
HT

Varices-surveillance and management
COPYRIG
HT

b-Blockers -9 randomised trials-4 significant reduction in bleeding-5 reduced mortality, 1 significant
Meta-analysis -significant reduction in bleeding (45%)-lower rates of fatal bleeding (50%)-trend ¯ overall mortality (D’Amico et al. Hepatology. 1995; 22: 332)
Therapeutic response should be assessed by HVPG(Conn et al. Hepatology 1991; 13: 902)
Primary prophylaxis - Drug therapy
COPYRIG
HT

Management of Acute Hemorrhage
• Patients with suspected acute variceal hemorrhage require intensive-care unit setting for resuscitation and management
• Acute GI hemorrhage requires:– Intravascular volume support– Blood transfusions – Maintaining hemoglobin of ~8 g/dL
• Institute short-term (7-day) antibiotic prophylaxis• Initiate therapy with somatostatin (or its analogs)• Perform esophagogastroduodenoscopy within 12 hours;
treat with endoscopic band ligation or sclerotherapy
Garcia-Tsao G et al. Hepatology. 2007;46:922-938.
COPYRIG
HT

Mortality from gastroesophageal variceal bleeding
• Meta-analysis of 1475 patients included in 28 trials of primary prophylaxis between 1960-2000
• Bleed related mortality was reduced from 65% to 40% (p=0.024)
McCormick PA et al Gut 2001;49: 607-608
COPYRIG
HT

Antibiotic Prophylaxis During/After Acute Variceal Bleeding
• Prophylatic ofloxacin vs antibiotics only at diagnosis of infection
• ¯ infections (2/59 vs 16/61)
• Less rebleeding within 7 days
• ¯ blood transfusions for rebleeding
• Prophylactic antibiotics recommended in management of acute variceal hemorrhage
Prob
abili
ty o
f Reb
leed
ing
Follow-up (Months)
0.01 2 3 12 18
1.0
0.8
0.6
0.4
0.2
0 24 30
On-demand antibiotics (n=61)
Prophylactic antibiotics (n=59)
Hou M-C et al. Hepatology. 2004;39:746-753.
Patients at riskProphylactic: 59 48 42 38 17 8 2On demand: 51 36 34 30 19 9 2
COPYRIG
HT

Rising Incidence of Hepatocellular Carcinoma
0
1
2
3
4
5
6
7
1976-
1980
1991-
1995
White Men
91-95
Black Men
91-95
Per 100,000
Represents a 41%
increase in
mortality rate and
a 46% increase in
hospitalization
El-Serag et al. N Engl J Med. 1999;340(10):745-750.
1.4
2.42.8
6.1
COPYRIG
HT

Screening for HCC
• Most studies in HCV are retrospective• 360 patients (167 had HCV)• US q 6 months for mean of 56 months• Compare with 2170 patients not
screened• 75% of those screened had unifocal
disease < 3cm as compared to 15% of those not screened
Solmi et al, Am J Gastroenterol 1996; 91: 1189-1194
COPYRIG
HT

HCC Surveillance-AASLD Guidelines
Non-hepatitis B cirrhosis• Hepatitis C• Alcoholic cirrhosis• Genetic hemochromatosis• Primary biliary cirrhosis
Although the following groups have an increased risk of HCC no recommendations for or against surveillance can be made because a lack of data precludes an assessment of whether surveillance would be beneficial.
• Alpha1-antitrypsin deficiency• Non-alcoholic steatohepatitis• Autoimmune hepatitis
Hepatitis B carriers• Asian males 40 years• Asian females 50 years• All cirrhotic hepatitis B carriers• Family history of HCC• Africans over age 20• For non-cirrhotic hepatitis B carriers
not listed above the risk of HCC varies depending on the severity of the underlying liver disease, and current and past hepatic inflammatory activity. Patients with high HBV DNA concentrations and those with ongoing hepatic inflammatory activity remain at risk for HCC.
Bruix and Sherman Hepatology Nov 2005
COPYRIG
HT

Non-disease-specific minimal listing criteriaAmerican Society for Transplant physicians and AASLD
(Liver Transplant Surg 1997; 3: 628-637)
• Immediate need for transplant• Estimated 1-year survival of < 90%• Child Pugh score > 7• Portal hypertensive bleeding • Single episode of SBP irrespective of CPTCOPYRIG
HT

Comparison of mortality for wait list patients versus transplanted patients
HR 3.64 2.35 1.21 0.62 0.38 0.22 0.18 0.07 0.04
P-values <0.001 <0.001 0.41 <0.01 <0.001 <0.001 <0.001 <0.001 <0.001
Merion et al. AJT 2005;5:307-313
COPYRIG
HT

Other potential pharmacotherapy• NSBB reduces bacterial translocation• Rifaximin reduces minimal HE• Rifaximin reduces HVPG• Statins reduce HVPG• Statins reduce the risk of HCC in Diabetics• Anticoagulation decreases risk of PVTCOPYRIG
HT

Summary• Complications of cirrhosis substantially
reduce overall survival• Advice to patients with cirrhosis
– Avoid alcohol– Advise weight reduction for compensated
cirrhosis– Vaccinate non immune patients
• Inform patients of benefits of smoking cessation, avoid cannabis use, drinking coffee
COPYRIG
HT

Summary
• Medical management has some impact on survival
• Liver transplantation prolongs survivalCOPYRIG
HT

Website for references
• aasld.org (practice guidelines)
COPYRIG
HT