Embed Size (px)
Citation preview

Complications during Hemodialysis
Hassan El Hajj, F1Nephrology Department
HHUMC

Common Complications Hypotension (20% - 30%) Cramps (5% - 20%) Nausea and Vomiting (5% - 15%) Headache (5%) Chest pain (2% - 5%) Back pain (2% - 5%), Itching (5%) Fever and Chills (<1%)

Hypotension It’s the most common acute complication of HD.
Incidence : 20 – 50% .
older patients and women more frequent.
Increased morbidity and mortality especially when episodes occur frequently.

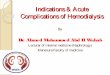
ETIOLOGY — Many factors may contribute to dialysis hypotension.These include:
A rapid reduction in plasma osmolality Inaccurate determination of true "dry weight“. Rapid fluid removal in an attempt to attain "dry weight“. Autonomic neuropathy. Diminished cardiac reserve. Use of acetate rather than bicarbonate as a dialysate buffer. Intake of antihypertensive medications that can impair cardiovascular
stability. Use of a lower [Na] in the dialysate. Sudden release of adenosine during organ ischemia. Ingestion of a meal immediately before or during dialysis. Arrhythmias or pericardial effusion with tamponade, which are volume-
unresponsive causes of hypotension. Reactions to the dialyzer membrane, which may cause wheezing and
dyspnea as well as hypotension. Increased synthesis of endogenous vasodilators, such as nitric oxide.



UltrafiltrationUltrafiltration
Osmolality Osmolality FallFall
Warm Warm DialysateDialysate
Bio-incom-Bio-incom-patibilitypatibility
EndotoxinEndotoxin
AcetateAcetateInfusionInfusion
VolumeVolume
VasopressorsVasopressors
VasodilatatorVasodilatator
Cell Cell DysfunctionDysfunction
ComplementComplementActivation, Activation, Cytokine releaseCytokine release
HypoxemiaHypoxemia
Heart DiseaseHeart Disease
Vascular Vascular DiseaseDisease
Autonomic Autonomic DysfunctionDysfunction
Hormonal Hormonal DysfunctionDysfunction
MedicationsMedications
SepsisSepsisInfectionInfection
Vasovagal stim.Vasovagal stim.HYPOTENSiONHYPOTENSiON
CARDIACCARDIACOUTPUTOUTPUT
PERIPHERAL PERIPHERAL RESISTANCERESISTANCE
PATHOGENESIS MEDIATORSPATHOPHYSIOLOGY PATIENT

DIAGNOSIS AND TREATMENT : Patients with hypotension may suffer from light-
headedness, muscle cramps, nausea, vomiting, and dyspnea.
The acute management of low blood pressure associated with hemodialysis includes the following: UF should either be stopped or the rate decreased The patient should be placed in the Trendelenburg position The blood flow rate should be reduced Intravascular volume may be replaced with mannitol or saline.
Further treatment is based upon the etiology of the hypotension. Particular concerns should include: Occult sepsis Previously unrecognized cardiac and/or pericardial disease GI bleeding

Prevention: Accurate setting of the "dry weight" Steady, constant UF Increased dialysate [Na+] and Na modeling Sequential UF and isovolemic dialysis Bicarbonate dialysate buffer Temperature control Improvement in CV performance Midodrine Avoidance of food Adenosine release

Recommendations for Prevention
Among patients with resistant cases of intradialytic hypotension, the 2005 K/DOQI guidelines suggest the use of the following combinations of modalities:
Midodrine and dialysate temperature profiling Dialysate temperature profiling plus 3 meq/L dialysate calcium
level Dialysate temperature and sodium modeling
Isolated UF and other approaches may also provide benefit.

Muscle cramps Etiology: The 4 most important predisposing factors are :
Hypotension Hypovolemia High UFR Use of low-sodium dialysis solution.
These factors all tend to favor vasoconstriction.
Muscle cramps most commonly occur in association with hypotension, although cramps often persist after seemingly adequate BP has been restored.
Contributing factors: Elevations in CPK levels. Hypomagnesemia. Hypocalcemia Predialysis hypokalemia

Muscle cramps Management :
Hypotension + muscle cramps 0.9% saline.
Hypertonic solutions (saline, glucose, mannitol) may be more effective in dilating muscle-bed blood vessels.
Hypertonic glucose administration is preferred for treatment of cramps in nondiabetic patients .
Nifedipine (10 mg) has also been found to reverse cramping (should be reserved for cramping in hemodynamically stable patients).
Forced stretching of the muscle involved may provide relief.

Nausea and Vomiting Incidence : 10 % The cause is multifactorial :
Most episodes in stable patients are probably related to hypotension. Disequilibrium Syndrome Dialyzer Reactions. Gastroparesis Contaminated or incorrectly formulated dialysis solution (high sodium,
calcium) Management :
The first step is to treat any associated hypotension. Vomiting may be particularly problematic when associated with a
hypotension-induced reduction in the level of consciousness due to the risk of aspiration.
Antiemetics can be administered for other causes of vomiting as needed.
Prevention : Avoidance of hypotension during dialysis is of prime importance. Persistent symptoms unrelated to hemodynamics may benefit from
metoclopramide. Sometimes a single predialysis dose of 5 -10 mg is sufficient.

Headache Etiology :
Cause is largely unknown. May be a subtle manifestation of the disequilibrium syndrome. Caffeine Withdrawal. With atypical or particularly severe headache, a neurologic cause
(particularly a bleeding event precipitated by anticoagulation) should be considered.
Mg deficient
Management : Acetaminophen can be given during dialysis.
Prevention : Decreasing dialysis solution sodium also may be helpful in patients being
treated with high sodium levels. A cup of strong coffee may help prevent (or treat) caffeine withdrawal
symptoms. A cautious trial of magnesium supplementation may be indicated

Chest pain and Back pain Incidence : 1% to 4%.
The cause is unknown.
There is no specific management or prevention strategy, though switching to a different variety of dialyzer membrane may be of benefit.
The occurrence of Angina during dialysis is common and must be considered in the differential diagnosis, along with numerous other potential causes of chest pain (e.g., hemolysis, air embolism, pericarditis).
If dialysis is continued, the administration of O2, reduction of the desired UF and/or blood pump speed, and administration of nitrates or MO should be considered on an individual basis.

Itching It’s a common problem in dialysis patients.
Etiology : ? May be a manifestation of low-grade hypersensitivity to dialyzer or
blood circuit components. Itching may simply be present chronically. Viral (or drug-induced) hepatitis should not be overlooked as a potential
cause of such itching.
Management : Standard symptomatic treatment using antihistamines is useful. Chronically, general moisturizing and lubrication of the skin using
emollients is recommended. Ultraviolet light therapy may be of help Recent small, randomized studies have suggested beneficial effects for gabapentin
Pruritus often is found in patients with elevated serum calcium - phosphorus product and/or substantially elevated parathyroid hormone (PTH) level.

Dialysis disequilibrium syndrome The dialysis disequilibrium syndrome (DDS) is a central nervous
system disorder described in dialysis patients.
It is characterized by neurologic symptoms of varying severity that are thought to be due primarily to cerebral edema.
New patients just being started on hemodialysis are at greatest risk, particularly if the BUN is markedly elevated (above 175 mg/dl)
Other predisposing factors include : Severe metabolic acidosis Older age Pediatric patients The presence of other CNS disease such as a preexisting seizure
disorder.

Dialysis disequilibrium syndrome Pathogenesis :
The symptoms of DDS are caused by water movement into the brain, leading to cerebral edema.
Two theories have been proposed to explain why this occurs: a reverse osmotic shift induced by urea removal; and a fall in cerebral intracellular pH.
Clinical Manifestations: Early : headache, nausea, disorientation, restlessness,
blurred vision, and asterixis. More severely affected patients progress to confusion,
seizures, coma, and even death.

Dialysis disequilibrium syndrome Management: In an acute dialysis setting:
One should not prescribe an overly aggressive treatment session. The target reduction in the BUN should initially be limited to about 40%. Use of a low-sodium dialysis solution dialysis solution (more than 2 - 3
mM less than the plasma sodium level) may exacerbate cerebral edema and should be avoided.
In hypernatremic patients, one should not attempt to correct the plasma sodium concentration and the uremia at the same time.
It is safest to dialyze a hypernatremic patient initially with a dialysis solution sodium value close to the plasma level and then to correct the hypernatremia slowly postdialysis by administering 5% dextrose.
Daily dialysis for 3 to 4 days with gradual increases in dialysis time and blood flow often prevents symptoms and signs of disequilibrium.
For severe headache, seizures, or obtundation, the dialysis procedure should be immediately terminated. Intravenous administration of mannitol or diazepam is useful in treating seizures caused by disequilibrium.




Arrhythmia: Risk factors include: CAD, advanced age, myocardial dysfunction, and
LVH During hemodialysis, the incidence of arrhythmias may be enhanced
because of rapid fluctuations in hemodynamics and electrolyte concentrations, as well as the induction of hypoxemia in patients with a high incidence of myocardial disease.
Cardiac Tamponade: Unexpected or recurrent hypotension during dialysis can be a sign of
pericardial effusion or impending cardiac tamponade.
Intracranial Bleeding: Underlying vascular disease and hypertension combined with heparin
administration can sometimes result in the occurrence of intracranial, subarachnoid, or subdural bleeding during the dialysis session.
Seizures: Children, patients with high predialysis plasma urea nitrogen levels, and
patients with severe hypertension are the most susceptible to seizures during dialysis.
Seizure activity can be one manifestation of the disequilibrium syndrome

Hemolysis Presentation : chest pain, chest tightness, or back pain. If hemolysis is not recognized early, severe hyperkalemia may ensue and lead to
death.
Findings highly suggestive of substantial hemolysis include : A port wine appearance of the blood in the venous line Complaints of chest pain, shortness of breath, and/or back pain A falling hematocrit A pink color of the plasma in centrifuged specimens.
The etiology of hemolysis in hemodialysis patients is usually related to problems with the dialysis solution . These include: Blood line obstruction/narrowing Overheating Hypotonicity due to an insufficient concentrate-to-water ratio Contamination with formaldehyde, bleach, chloramine, or nitrates from the water
supply, and copper from copper tubing or piping.
RBC trauma due to improperly functioning roller clamps on dialysis machines, kinking of the blood lines, and poorly constructed blood tubing can also occur.

Hemolysis Treatment:
The initial treatment of suspected hemolysis in a patient on HD is to : Stop dialysis immediately. Clamp the blood lines (do not return the blood to avoid increasing the
risk of hyperkalemia), Prepare to treat hyperkalemia and the potentially severe anemia. Investigate the cause.
Patients require hospitalization for observation since life-threatening hyperkalemia may develop after dialysis has been terminated.

Air embolism Air embolism during dialysis is another cause of chest pain as well as other
symptoms, particularly dyspnea.
It can lead to death.
Symptoms : the seated patient with an air embolism may lose consciousness and seize while the recumbent patient may initially develop dyspnea, cough, and
perhaps chest tightness.
Treatment of suspected air embolism includes: clamping the venous line and stopping the blood pump. The patient should be positioned on the left side in a supine position with the
chest and head tilted downward. Cardiorespiratory support, the administration of 100 % O2 by either mask or
ET tube, and attempted percutaneous aspiration of air from the ventricle may be required.

Visual and Hearing Loss The osmolar gradients that develop in dialysis between the
blood and the intraocular fluid and vestibular system may alter sensory function.
Transient blindness in patients with glaucoma and hearing loss due to endolymphatic hydrops have been reported to occur during dialysis.
Complications of heparin administration (inner ear, vitreous or retinal hemorrhage) may result in similar clinical findings.
Intradialytic hypotension or unrelated vascular events can also alter visual and auditory function.

Dialysis associated hypoxemia
Etiology :There are several possible reasons for the drop in PO2 during dialysis:
Hypoventilation. 2 mechanisms may contribute to hypoventilation during dialysis:
Acetate-containing dialysis solution. Bicarbonate-containing dialysis solution
Intrapulmonary diffusion block. dialysis using unsubstituted cellulose membranes causes sequestration of neutrophils in the lung. Some studies have suggested that the alveolar-to-arterial oxygen gradient is increased very early during dialysis, presumably due to neutrophil embolization into the pulmonary capillaries.

Dialysis associated hypoxemia Management:
Intervention is usually not required. With active cardiac ischemia or severe COPD, nasal oxygen
administration may be beneficial. In patients with CO2 retention, delivery of oxygen by Venturi
mask may be more appropriate.
Prevention: Oxygen administration will prevent (as well as treat) hypoxemia. In high-risk patients, one might consider avoiding dialyzer
membranes made of unsubstituted cellulose and using a bicarbonate-containing dialysis solution with a
bicarbonate concentration low enough to avoid alkalemia.

Thank You