Embed Size (px)
Citation preview

Compliance with Standard Precautions Bnd Occupational Exposure Reporting
among Operating Room Nurses in Australia
Sonya Ranee Osborne
A thesis submitted in fulfillment of the requirements for the degree of
Master of Nursing by Researeh
Division of Science and Design
School ofNursing
University of Canberra
March 2002

Abstract
Compliance with standard precautions and occupational exposure reporting
among operating room nurses iD Australia.
Occupational exposures of hcalthcare workers tend to occur because of
inconsistent compliance with standard precautions. Also, incidence of occupational
exposure is underreportcd among operating room personnel. Thc purpose of this
project was to develop national estimates for compliance with standard precautions
and occupational exposure reporting praetiees among operating room nurses in
Australia. Data was obtained utilizing a 96-item self-report survey. The Standard
Precautions and Occupational Exposure Reporting survey was distributed
anonymously to 500 members of the Australian College of Operating Room Nurses.
The Health Belief Model was the theoretical framework used to guide thc analysis of
data. Data was analysed 10 examine relationships between specific construets of the
Health Belief Model to identify factors that might influence the operating room nurse
to undertake particular health behaviours to comply with standard preeautions and
occupational exposure reporting. Results of the study revealed complianee rates of
55.6% with double gloving, 59.1% with announcing sharps transfers, 71.9% with
using a hands-free sharps pass technique, 81.9% with no needle recapping and 92.0%
with adequate eye protection. Although 31.6% of respondents indicated receiving an
occupational exposure in the past 12 months, only 82.6% of them reported thcir
exposures. The results of this study provide national estimates of compliance with
standard precautions and occupational exposure reporting among operating room
nurses in Australia. These estimates can now be used as support for the development
and implementation of measures to improve practiees in order to reduce occupational
exposures and, ultimately, disease transmission rates among this high-risk group.
11

Certifieate of Authorship of Thesis
Except as specially indicated in footnotes, quotations and the bibliography, I
certify that I am the sole author of the thesis submitted today enlilled-
Compliance with standard precautions and occupational exposure
reporting among operating room nurses in Australia
in terms of the Statement of Requirements for a Thesis issued by the University
Higher Degrees and Scholarships Committee.
Date--------------
./-~y-£- {~Signature of Author_+,_if__v '-----1-.. {-I _I' /J
;)0/ 't- /~ z-
III

Unillt'rsity ofCallbrrra Pr>/icy r>n lIigher Degrees by Research
APPENDIX 18A-REQUlREMENrs FOR A THESIS
UNIVERSITY OF CANBERRA
FORMC
32
Retention and Use of Thesis
I, (name ofcandidate) SON YfI OSC>OAAI£nA--&12 &1= Ill" - 'Nt". t!J t. /fG".~B/{(,rl
being a candidate for the degree of f"fMI4'i·er6t6~)·idt~.:prttItr'teqnirel\le.mof theUniversity relating to the retention and use oftheses deposited in the Library.
I agree to abide by any general condilions eslilblished by the University for the care,
loan or reproduction of theses and any special conditions of usage in relation to this
thesis entitled- (title ofthesis). COlll rA..111NC~ eJJF lA.-.'lIH S'f/7/VDllteD r),{tE'L-JTl/I/ONS/f-tJO OL(/l1Pr7-rIO~.)ItL £.7<-iJo~utX.C A£f'OK.:(;l~(c H//10/liG 0/'£"/(11///\/6 1l0(.l/I/
lv' uJ\.SLEOS //\1 /f-U ::::,(I!.4'..<- lit.In tenns of these conditions, I agree that the original of my thesis deposited in the
Library should be accessible for purposes of study and research, in accordance with
the nonnal conditions established by the Librarian for the care, loan or reproduction
of theses.32
A <:andidale wishing 10 impose special condiljon~ limiting access to or usage of the thesis, should~eek (he agreement of the n:levant comrnil1ce.
154 Version: March /9, 1999

Acknowledgments
I gratefully acknowledge the assistance of my supervisor, Reverend Dr
Elizabeth MacKinlay, for her help, encouragement and support throughout this
cxereise and my eo-supervisor, Ms Jan Taylor, for seeing me through to the end.
To my husband, Roger, I offer my thanks for countless hours of support and
encouragement; and, to my little angels, Megan and Melissa, hugs and kisses for
breaking the monotony.
IV

Table of Contents
Abstract
Certificate of Authorship of Thesis
Acknowledgments
Table of Contents
Chapler 1. Introduction
1.1. Background to the Study
1.2. Statement of Problem
1.3. Purpose of Study
1.4. Aims of the Study
1.5. Overview of the Thesis
1.6 Conclusion
Chapter 2. Literature Review
2.1. Introduction
2.2. Hislory of Standard Precautions
2.3. Slandard Precautions in the Operating Room
2.3. l, Double Gloving
2.3.2. Eye Prolection
2.3.3. Safe Sharps Handling
2.3.3.41. Announcing Sharp Transfers
2.3,3,b. Hands-free sharp passage technique
2.3.3.c. No Needle Reeapping
2.4. Compliance with Standard Precautions
2.5. Occupational Exposure in the Operaling Room Environment
2.6. Occupational Exposure and Incidence of Disease Transmission
2.7. Under Reporting ofOceupational Exposures
ii
iii
iv
1
2
5
5
5
8
9
9
II
13
15
17
19
19
20
21
21
24
24
25
v

2.8. Benefits ofOccupational Exposw-c Reponing
2.9. Summary and Conclusion
Chapter 3. Methodology
3.1. Introduction
3.2. Design 0 f the Research Study
3.J. Theoretical Framework-Thc Health Belief Model
3.4. The Sample/Study Popnlation
3.4.1. Response Rale
3.4.2. Demographics of the Sample
3.5. Dala Collection Process
3.5.1. Ethical Considerations
3.5.2. Development of Instrument
3.5.3. Pilot Study
3.5.4. Revision of Instrument
~.6. Reliability and Validity of the Instrumcnt
~.6.1. Reliability
~.6.2. Validity
3.7. Data Analysis
3.8. Limilalions of the Study
3.9. Summary and Conclusion
Chllpcer 4. Reliultti
4.[ Introduction
4.2. Compliance with Standard Precautions
4.3. Compliance Rates with Occupational Exposw-e Reponing
4.4. The Health BeliefConstructs
4.4.1. Perception of Risk of Blood Borne Infeclion
4.4.2. Perception of Severity of Blood Borne Infection
4.4.3. Benefits ofCompJiance with Slandard Precautions
4.4.4. Barriers to Compliance with Standard Precautions
27
28
30
30
31
32
33
35
35
37
39
40
41
42
43
43
44
45
46
48
49
49
50
51
55
55
56
57
5R
VI

4.4.5. Benefits ofOccupatiDnal Exposure Reporting 60
4.4.6. Barriers to Compliance Wilh Occupational Exposure Reporting 61
4.5. Demographics .100 Compliana with Standard Precautions 62
4.6. Demographics and Compliance with Occupational Exposure Re-porting 66
4.7. Compliance with Standard Precautions and the Health Belief Constructs 66
4.7. t. Compliance with Standard Precautions and Perception of Risk 68
4.7.2. Compliance with Slandard Precautions and Perception of Severity 68
4.7.3. Compliance with Standard Precautions and Perception of Benefils 68
4.7.4. Compliance with Standard Precautions and Perception of Barriers 69
4.8. Occupational Exposure Reporting and Health BeliefConstructs 71
4.8.1. Occupational Exposure Reporting and Perception of Risk 71
4.8.2. Occupationa I Exposure Reporting and Perception of Severity 72
4.8.3. Occupational Exposure Reporting and Perception of Benefits 72
4.8.4. Occupational Exposure Reporting and Perce-ption or Barriers 73
4.9. Summary and Conelusion 74
Chapter S. DiscunioD 75
5.1 Introduction 75
5.2. Compliance Rates 75
53. The Health Belief Model 78
5.4. Summary and Conclusion 80
Chapter 6. Recommendatians 82
6.1. Introduclion 82
62. Prev~~on ~
6.3. Education 86
6.4. Policy 88
6.5. Summary and Conclusion 90
Chapter 7. Summary of Thesis 92
AppendiJ: I. Epidemiologically Significant Pothogens Requiring Additlonol Precautions 97
VII

Appendix 2. Conceprual Definitions 98
Appendix 3. Covel" letter aceompanying survey 99
Appendix 4. Information for Pal"ticipants 100
Appendix S. SUl"vey Instrument 101
Appendix 6. Items Evide ncing 'nternal Consistency Cor Risk, Severity and Benefi t Seal" 110
Appendix 7. Items Evidencing Inter-nal Consistency for Bar.-ier Scale 111
Appendix 8. Demographics of the So mple 112
Appendix 9. Demographic Variables and Standard Precautions Compliance 113
Appendix 10. Demographic Vui.ablcs and OCCD plltional Exposul"e Reporting lIS
Refel"enees 116
Vlll

Chapter 1. Introduction
1.1. Background to the Study
Statisties on occupational exposures10 f health eare workers to blood-borne
pathogens around the world are startling. The International Health Care Worker
Safety Center (lHCWSC) reports that 1996 EPINct2 data in the United States
estimated the total annual percutaneous and mucocutaneous exposures to blood or
other body substances was 786,885 exposures, at a rate of30 exposures per 100 daily
oceupied hospital beds (IHCWSC, 1998). Additionally, IHCWSC (1998) estimates
that 39% of incidents occurring in hospitals are not reported. Prospective studies
have estimated transmission rates after occupational exposure for Human
Immunodeficiency Virus (HIV), Hepatitis B Virus (HBV), and Hepatitis C Virus
(HCV) at 0.3%, 6-30%, and 1-10%, respectively (Centers for Disease Control
[CDCl. 1998R, 1998b
). These transmission rates are used to estimate thai between 18
and 35 new occupational HIV infections and belWeen 118 to 5,902 new occupational
HCV infections would occur from percutaneous exposures each year. The IHCWSC
(1998) also suggests from data on mucocutaneous exposures that between 2 and 4
HIV cases and between 39 to 1,967 HCV cases would occur from mucocutaneous
exposures.
I Occupational Exposure is an incident in which the heahhcare worker has been exposed to potentially infectious.blood or body fluids from a patient by percutaneous. mucocutaneous, or cUlall~aus exposure; or by anycombination of thc three.
1 EPI Net, the Exposure Prcvention In fonnatlon Nelwork. was sec up in the Uni ted Stales in Illn to provide astandardized, hospital-widc sUl1lciIlance system for traclo.ing adverse occupational exposures (Sauhrada. 199.5).Over 1000 institutions in the US, as well as hospital" In Canada, Australia, Italy and New Zealand have adoptedthe EPINet sUl1leillance system, whieh IS the only international standard for the collection of data on adverseoccupational exposnres (Souhrada, 1995). Through EPINet, institutions are able to direclly comparecircumstances ~nrround ing cxposun:s in My hospical and avert difficullics. EPINcl's inlonnation helpsinstitutions lraelo. and analyze injury frequency, identIfy Injuries that may be preventable, compare and shareillfonnaLlon. and idrllli(y ~uccessful prevenlion slralc:gic:~ ill order to reduce healthean: workers' occupationalexposure to blood and body fluids (Souhrada, 1995).

National monitoring of occupational exposure to HIV, HBV and HCV began
in Australia in 1995. Data collection in Australia resulted in a total of 1,718 reported
exposures in 1998 at a rate of25 cxposures per 100 daily occupied beds, with 83% of
these exposures being percutancous, and about 60% of the exposures reported by
nurses (MacDonald and Ryan, 1999). In Australia, the National Centre in HIV
Epidemiology and Clinical Research (1999) estimatcd thc risk of HIV transmission
following a single exposure to HIV to be 0.32%, from percutaneous exposure, and
0.03%, from mucoeutaneous exposure. In thc same report, the Centre also estimated
the risk of HCV following a single percutaneous five pcrccnt of worldwide cases
resulting in transmission of HIV infection among healtheare workers following a
specific occupational exposure to blood or body fluids occurrcd in Australia
(MacDonald and Ryan, 1999).
1.2. Statement of Problem
Limited research has been conducted on types of occupational exposures,
frequency of occupational exposures, health care professionals at greater risk of
occupational exposures, effectiveness of standard precautions) in reducing risk of
occupational exposures and rates of compliance with standard precautions. Although,
standard precautions were introduced in the 1980s. research continues to report less
than 100% compliance among health care professionals with measures that have
been demonstrated to decrease disease transmission by decreasing the risk of
exposure. (Gruber et al, 1989~ Hammond, Eckes, Gomez and Cunningham, 1990).
Several instruments were dcveloped around this time to try and accurately assess
J Standard Precautions are healthcare guidelines to prolect the hellithcare wor"er (rom occupatlonal exposure toblood-borne infections. Examples of standard precautions include use of barrier prorection (e.g. gloves, eyeprotection), safe sharps handling (e.g. no needle recapping, announcing sharps transfers, hands frce passage ofsharps) and hepatitis B vaccination.
2

knowledge of standard precautions, compliance with standard precautions and
comparisons between self-reported and observed compliance with standard
precautions (Gauthier, Turner, Langley, Neil and Rush, 1991).
Operating room nursing is considered a high-risk nursing specialty (Atkinson,
1992). There is an increased risk of blood exposure in the operating room because of
the prolonged exposure to open surgieal sites, the frequent manipulation of sharps,
the dosc environment, and the presence of relatively large quantities of blood
(Jagger and Perry, 2000). Blood exposure is associated with increased risk for
infection with blood borne pathogens (Denes et ai, 1978 cited in Lynch and White,
1993). In addition, surgical personnel were among those occupational categories with
increased risk for disease transmission during the eourse of a career because they arc
frequently exposed to blood and secretions from patients (McKinney and Young,
1990 eited in Lynch and White, 1993; Colbert and Sheehan, 1995). [nfonnation on
disease transmission is continually being challenged and updated and new diseases
are being "diseovered" at an alanning rate.
H is both important, and necessary, to assess not only reasons for non
complianee but also other factors, such as attitudes and beliefs, that may exert an
influence on compliance. Knowledge of these will assist in the development of
appropriate edueational as well as interventional measures to improve eompliance.
The consequences of an occupational exposure to blood borne pathogens
extend beyond transmission of infection. Consequences related to health can inelude
side effects from prophylactie agents, liver disease and subsequent transplant
complieations, ehronic disabilities and premature death (IHCWSC, 1998).
Consequenees related to employment can include punitive disciplinary action, job
discrimination, denial of worker's eompensation claims and loss of employment
3

potential (IHCWSC, 1998). Other personal consequences can include ehange in
sexual practices or postponement of child bearing (IHCWSC, 1998).
It is impossible to distinguish blood and body substances infected with
hannful organisms from those not infected unless the samples have been
serologically tested and, unfortunately, results from most serological tests are not
immediately available. There are documented cases of disease transmission of HIV,
HBY and HCY from occupationally acquired exposures (Sepkowitz, 1996). From
the analysis of these documented cases, statistics have estimated risk of transmission,
albeit small, of HIV, HBV and HCY from occupationally acquired exposures.
However, "small" risk does not equal "no" risk. In order to decrease the risk of
transmission of a blood-borne infection from an occupational exposure, health care
workers, especially those in designated high risk areas, such as the operating rooms,
must lake every precaution demonstrated and available to prevent and proteet
themselves from oecupational exposure in the first instanee. Standard precautions,
including barrier methods (e.g., double gloving and adequate eye protection) and safe
sharps handling (e.g., no needle recapping and immediate disposal of sharps) have
been found to be significant in the reduetion of occupational exposures in the
operating room. In addition, hepatitis B vaccination and prompt reporting and
prophylactic treatment following occupational exposure have been suecessful In
prevention of disease transmission following an occupational exposure.
No studies have been found that assess compliance with standard precautions
and occupational exposure reporting or explore intluenees on compliance among
operating room nurses in Australia.
4

1.3. Purpose of Study
The purpose of this study was to contribute to the body of nursing knowledge
by developing national estimates for compliance with standard preeautions and
occupational exposure reporting practices in a high risk category of nursing. This
will in tum provide a basis upon which to develop and implement measures to
improve these practices thus minimising occupational exposure and disease
transmission rates among this group. Additional projects can then be developed to
pilot protocols aimed at improving compliance with standard precautions and
reporting of occupational exposures as they oceur.
1.4. Aims of tbe Study
The aims ofthis study were:
1. To assess operating room nurses' attitudes and beliefs and level of compliance
with healthcare guidelines established to protect them from contracting infectious
diseases from patients (that is, standard precautions).
2. To identify influences on non-eompliance with Standard Precautions.
3. To assess operating room nurses' attitudes and beliefs and level of compliance
with reporting incidents in which they have been exposed to potentially
infectious diseases from patients (that is, occupational exposure)
4. To idenlify influences on non-compliance with occupational exposure reporting.
1.5. Overview of the Thesis
Chapter I laid a foundation leading to the problem statement under
investigation and the purpose and broad aims of the study, namely, ·what are the
5

compliance rates for standard precautions and occupational exposure reporting
among operating room nurses in Australia?' and 'what influences compliance?'
In order to understand where we are today. we must look back on the history
of standard precautions. Chapter 2 discusses this history, specifically the history in
Australia. This ehapter then progresses into a review of the literature on the use and
efficacy of specific standard preeaution behaviours (ie double gloving, eye protection
and safe sharps handling) in the reduction of occupational exposure and compliance
rates with standard precautions among health professionals. The chapter ends with a
discussion on various issues associated with occupational exposure and occupational
exposure reporting, namely, incidence of occupational exposure and disease
transmission. underreporting of occupational exposures and benefits of reporting
occupational exposures as evidenced by previous research.
Chapter 3 discusses the methodology chosen to undertake the study. In order
to meet the aims of this study a descriptive correlational design was used. In
addition, a theoretical framework, The Health Belief Model (HBM), was used to give
meaning to the variables under study. The HBM describes four variables (ie
perception of risk, perception of severity, perception of benefits, perception of
barriers) that influenee action to undertake self-protective behaviour (eg compliance
with standard precautions or compliance with occupational exposure reporting). This
chapter also describes other aspects of the research design, including the sample and
study population, the data collection procedures, and the development, piloting and
testing of the data collection instrument, the Standard Precautions and Occupational
Exposure Reporting survey. Also ineluded in this chapter is an outline of the data
analysis plan. The ehapter concludes with a discussion of limitations of the study.
6

Chapter 4 diseusses the results of the study. The demographics of the
respondents are discussed in tenns of age, level of nursing, type of training, and
years of experience. Other demographies include type of facility, size of hospital and
operating suite and state of employment. Results of this study demonstrate that
compliance with standard precautions and occupational exposure reporting among
operating room nurses in Australia is less than 100% and the variables of the HBM
are signifieant influences on compliance with some behaviours. In addition,
perception of barriers was found to have the most substantial relationship with
compliance.
Chapter 5 proceeds with a discussion of the previously mentioned results.
The results of this study are compared with results available from previous studies.
Each of the study behaviours and reporting practices are examined separately.
Results of this study are similar to results ofpreviously published studies in reporting
the less than 100% eomplianee rates with standard precautions and occupational
exposure reporting. Although previous studies deseribe barriers to compliance, this
study demonstrates the signifieanee of the influence of the perception 0 f barriers on
complianee.
Chapter 6 outlines reeommendations for improving compliance with standard
preeautions and occupational exposure reporting. Recommendations are categorised
under three headings: prevention, education and policy. Recommendations include
the responsibility to prevent occupational exposures in the first place, the need to
develop and implement effective operating theatre infection control education
programs that take into account the possible influences on levels of compliance, and
the need to develop policies that mandate compliance.
The thesis concludes with Chapter 7, a synopsis ofthe entire study.
7

1.6 Conclnsion
This thesis presents a perioperative issue arising from questions about clinical
practice, namely, 'how do we, as operating room nurses working in a high-risk
specialty, protcct ourselves from risk of disease transmission and what influcnces our
self-protective behaviours. It then describes the subsequent process of developing
and refining a plan to answer that qucstion. It is intended that the answers to the
questions will be used to inform praetice through the development of evidence-based
policics, a change in clinical practiee, and a push for further research on the topic.
8

Chapter 2. Literature Review
2.1. Introduction
The early focus of infeetion control since the discovery 0 f the mechanism of
disease transmission by Lister and others in the 1800s has been on the prevention of
patient acquired infections (Greundemann and Fernsebner, 1995), especially
nosocomial infections, i.e. those occurring while thc patient is in hospital. Over the
years, healtheare workers have beeome increasingly aware of their risks of
contracting diseases from patients, most notably, blood-borne infections, such as
HBV, HCV and Acquired Immune Deficiency Syndrome (AIDS).
The focus of concern in the 1970s was HBV. HBV is an infection caused by
the hepatitis B virus, which is present in the blood, tissues and body fluids of infeeted
individuals. HBV causes an acute liver infeetion, from which most people reeover.
However, as many as 10% of those infected become chronic earriers of the virus for
an indefinite amount of time (National Health and Medical Researeh Council
[NHMRC], 1996). It is these ehronie carriers who present the greatest risk to
healthcare workers. Risk of transmission of HBV is 1-40%, depending on E antigen
status (Sepkowitz, 1996). Hepatitis B vaceination is available and recommended for
all healthcare workers, especially those who may be exposed to blood, tissue and
other body tluids.
Even though it was known in the 1970s that healthcare workers were at risk
of occupational exposure from HBV (Greundemann and Fernsebner, 1995), it was
the onset of the AIDSIHIV epidemic in the mid-1980s that spawned new concerns
about healthcare workers' risk of occupational exposure and infection from the
patient. HIV was first recognised in 1981 (NHMRC, 1996). It is transmitted through
9

blood and other body substances, through mucous membrane exposure and through
eontact with non-intact skin. HIV ean progress to AIDS. which is a severe,
debilitating and eventually fatal disease. Data from 1995 estimated 19,087 people in
Australia diagnosed with HIV, 6, 035 diagnosed with AIDS, and 4, 309 deaths
following AIDS (National Centre in HIV Epidemiology and Clinical Research,
1995). The risk of a healthcare worker acquiring HIV from an infected patient is low
(0.3%) (NHMRC, 1996). At present. there is no known cure for AIDS. However,
treatment with antiretroviral agents is successful in slowing the progression from
HN to AIDS. New drugs are being trialled as vaccinations against HIV.
In the 1990s the focus of concern changed to HCV. The HCV virus was
identified in 1989. Acute HCV is asymptomatic and infections are rare, however,
HCV causes chronic hepatitis which can lead to chronic liver disease, cirrhosis, and
hepatocellular carcinoma (NHMRC, 1996). It is estimated that there are over
100,000 HCV carriers in Australia (NHMRC, 1996). The risk of HCV transmission
to healthcare workers following needlestick injury is 2-10% (NHMRC, 1996).
Active immunisation is not available and there is no documented proof that passive
immunisation is useful, although infected individuals may benefit from new drugs
currently being tested.
Although, the success of the Hepatitis B vaccine is encouraging. a similar
vaccine for HIV or HCV has not yet been approved for general use anywhere in the
world. Thus, it is imperative to each healthcare worker to demonstrate behaviours
that will be the most beneficial in decreasing or preventing their exposure to these
10

and other blood-borne pathogens, thereby, deereasing their risk of transmission of
these morbid diseases4.
2.2. History of Standard Precautions
In the mid 1980s, in response to the increase in prevalence of HIV/AIDS and
the increased concern for the protection of the healthcare worker. CDC in the United
States proposed the concept of Universal Precautions. Universal Precautions
guidelines involved treating the blood and body fluids from all patients as potentially
infectious. However, certain body fluids (i.e. faeces, nasal secretions, sputum,
sweat, tears, urine, and vomitus. unless they visibly contained blood) were not
included in these guidelines (CDC, 1994). This definition of Universal Precautions
was adopted in Australia, albeit, in an expanded form.
Work practices in Australia assume that all blood and body substances,
without exception, were considered as a potential risk of disease transmission. In
Australia, the principle of "confine and contain" applies to all patients and all
procedures in the operating room and universal precautions is mandated by state
departments of health as the policy of infection control in public hospitals. Universal
Precautions is limited in that it focuses only on disease transmission through blood
and body fluids and does not incorporate precautions for transmission by other
means.
It was recognised in Australia that the term Universal Precautions was
ambiguous, caused confusion in its interpretation and led to a false sense of security
4 Survey questions for thIS srudy focus on heallhcare worker concern with acquinng HBV or HeV. Theseriousness of HIV/AIDS has Increased standanJ precautions compliance among heahhcan: workers since the1980s, Although, there is a higher transmission rate of HBV than HIV, healtheare workers are still nOl asconcerned about acqui ring Hepatitis B. The availabi lilY of an effeetive vaccine may ha~ e some in fluence on thiSbehaviour. Currently, there is not as much mfonnation on HCV as on HIV and HBV, ThIs may be due to thefaet that HCV was only first identified in 1989. Although, disease transmIssion rates for HCV follOWingoecupational exposure is greater than HIV bUI less (han HBV, acute Hey is asymptomatIc. ChrOniC HCY leads
11

(NHMRC, 1996). This was evident in reports of healtheare workers substituting
glove wearing for appropriate hand washing. It was at this time that the NHMRC and
the National Couneil on AIDS recommended a change in terminology. This change
in terminology renects a two·tiered approach to infection control and is in line with
the changes in terminology adopted by the CDC in 1996 (NHMRC, 1996).
Universal Precautions has been broken down to reflect a two-tiered approach.
The first tier, Standard Precautions, is the first line of defense in infection control and
assumes that all blood and body fluids are potentially infectious. Standard
Precautions includc diligent hygiene practices (e.g. hand washing and drying), use of
personal protective equipment (e.g. gloves, gowns, masks and eye protection), and
appropriate handling and disposal of sharps (e.g. safe transfer, no needle recapping,
immediate disposal after use). Standard Precautions are used when handling non-
inlact skin, mucous membranes and blood plus all other body fluids, even if dried,
except sweat (NHRMC, 1996).
In 1996, "the Infection Control Working Party in Australia recommended
adoption of thc term 'Standard Precautions' as the basic risk minimisation
strategy ... to prevent transmission of infection... " (NHMRC, 1996, p.ll)
The second tier, Additional Precautions, is the second line of defense in
infection control. It is used in addition to Standard Precautions in situations where
Standard Precautions may be insufficient to prevent transmission of infection in
cases where the patient has a known or suspected infection or colonisation with an
epidemiologically important or highly transmissible pathogen (NHMRC, 1996) (see
Appendix I). The modes of transmission of thesc signi fieant pathogens is usually by
10 chronic liver disease and liver cancer. At present, a vaccine for active or passive immunity to Hev has nolbeen proven In eli nical trials.
12

airborne transmission, droplet transmission or transmission via direct or indirect
contact with intact skin or contaminated surfaces (NHMRC, 1996).
By consistently incorporating this two tiered approach of Standard and
Additional Precautions into work practices, a high level of protection against
occupational exposure of diseases from the patient to the healthcare worker can be
obtained. Breaches in these guidelines, designed to protect the healthcare worker,
may result in an increased risk of occupational exposure and subsequent disease
transmission.
2.3. Standard Precautions in the Operating Room
The three vital components of Standard Precautions are proper hand washing,
use of protective barriers, and precautions in handling sharps (Greundemann and
Fernsebner, 1995). Standard precaution behaviours include handling the blood and
body substances of all patients as potentially infectious, washing hands before and
after all patient or specimen contact, wearing gloves when contact with blood or
body substances could occur; removing gloves after each individual task, washing
hands after removal of gloves, wearing a gown or disposable plastic apron when
splash of blood or body substanee eould occur, covering any break in skin integrity
with a waterproof covering, wearing protective eye wear and a mask if facial splatter
with blood or body substances could occur; wearing a mask for protection against
airborne transmitted diseases, placing used needles and syringes in nearby puncture
resistant containers, and not recapping or manipulating used needles in any way
(NSW Health Department, 1995; ACT Government, 1997).
In the operating room environment, the wearing of gloves, gowns, and masks
by operating room personnel are necessary requirements to establish and maintain an
aseptic environment for the patient, thus helping to decrease the chance of wound
13

infection for the patient. But more diligent use of these barriers. as well as other self
proteetive health behaviours, can be employed in the operating room to decrease the
operating room nurses' chance of occupational exposure and risk of aequiring
infections from patients. Several measures, some in excess of the minimal standard
precautions, have been demonstrated to be effective in decreasing occupational
exposure in the operating room. Some of these measures include double gloving
(Dodds, Barker, Donaldson and Thomas, 1990; Telford and Quebbemann, 1993;
Marin-Bertolin, Gonzales-Maninez, Giminez, Vila and AmOITortu-Velayos, 1996;
Jensen, Kristensen and Fabrin, 1997), wearing adequate protective eye wear
(Geberding, 1993; NHRMC, 1996), and diligent and safe handling of sharps
(Geberding, 1993; Telford and Quebbemann, 1993, Hersey and Martin, 1994;
NHMRC. 1996). Measures identified as decreasing the risk of acquiring an infection
following an occupational exposure include hepatitis B vaccination (Short and Bell,
1993, Hunter, 1998; Mujeeb, Khatri and Khanani, 1998) and prompt reporting and
appropriate follow up with prophylactics, if available. after the incident (Geberding,
1996; CDC, 1997). Paramount to all of these interventional type health behaviours
is a comprehensive education and training program on infection control.
This study focused on five standard precaution behaviours that can be
employed in the operating room environment to decrease the healthcare worker's risk
of occupational exposure. The first two behaviours are (1) double gloving (when
scrubbed for surgical procedures) and (2) use of appropriate protective eyewear. The
final three study behaviours, whieh can be grouped together as safe sharp handling,
are: (3) utilising a hands-free technique when passing sharps, (4) announcing sharps
transfers, and (5) no recapping of hypodernlic needles. An examination of each of
these standard precaution behaviours follows. Hepatitis B vaeeination and prompt
14

reporting and prophylactic treatment of occupational exposures has also been
reported as sueeessful interventions in preventing disease transmission following an
occupational exposure (CDC, 1998a; CDC, 1998b
). Oceupational exposure reporting
will be addressed laler in this chapter.
2.3.]. Double Gloving
Barrier precautions are one of the major principles of Standard Precautions.
The practice of wearing gloves when there is the possibility of contact with
potentially infectious blood or body fluids increased significantly with the
development of Universal Precautions in the 1980s. This practice is recommended in
national guidelines, specific state guidelines and individual professional healtheare
organisations' guidelines throughout Australia (NHMRC, 1996; ACT, 1997; New
South Wales Nurses Registration Board, 1995; ACORN, 2000; RACS, 1998).
Wearing gloves in the operating room not only protects the patient from
eontamination from the healthcare worker, thus decreasing the risk of post operative
wound infection, but also protects the healthcare worker from oecupational exposure
ofpotentially infectious material from the patient.
Double gloves are currently recommended for surgeon use by several policy
documents (NHRMC, 1996; Australasian College of Surgeons, 1998). The majority
of studies on the efficacy of wearing two pairs of gloves (i.e. double gloving) have
concluded that double gloving decreases the risk of oecupational exposure in the
event of glove perforation.
Dodds et al (t 990) studied the practiee of single and double gloving of
surgeons in 100 hernia operations and found that glove perforation occurred in 31 %
of single-gloved operations and 39% of double.gloved operations. Of these double
gloved eases, there was only an 8% perforation of the inner glove as well. Study
15

participants were unaware of these perforations in 42% of the single gloved cases
and 50% of the double-gloved cases (Dodds, Barker, Donaldson and Thomas, 1990).
This study, therefore, concluded that wearing double gloves significantly reduces the
healthcare workers' risk of skin contamination from 31% to 8% (Dodds, Barker,
Donaldson and Thomas, 1990).
In a randomised study of procedures (n=234) that were predicted to last
longer than two hours and incur more than 100 milliliters (mls) of blood loss, Telford
and Quebbemann (1993) found thai personnel who wore single gloves had a
contamination rate of 40-76%, and those who wore double gloves had a
contamination rate of 6~9%. The participants in this study included not only
surgeons, but also first surgical assistants.
Results of another randomised study of single and double-gloving among
surgeons and scrub nurses (n=8) in a plastic surgery unit demonstrated a perforation
rate for single gloves (7.31 %) that was significantly higher than the perforation rate
of the inner glove (2.95%) when double gloves were worn (Marin-Bcrtolin,
Gonzales-Martinez, Giminez, Vila and Amorrortu-Velayos, 1996). In this study, a
total of 1092 gloves were examined over a two-month period. Marin-Bertolin et al
(1996) also found that the rate of glove perforation was higher among the scrub
nurses in comparison to the surgeons, although this difference was not found to be
statistically significant. This study also recommends double-gloving to decrease risk
of skin contact with potentially infectious organisms.
In a recent randomised controlled study of single and double gloving (n=400
glove barriers) of surgeons during abdominal procedures, it was concluded that
double gloving reduces the rate of perforation of glove barriers and thus reduces the
16

episodes in which disease transmission can occur (Jensen, Kristensen and Fabrin,
1997).
All of the above mentioned studies examined different health care workers
(surgeons, first assistants, nurses) in different clinical situations (hernia surgery,
procedures lasting longer than 2 hours and losing greater than 100 mls of blood,
plastic surgery procedures, abdominal procedures). None of the studies purported
that wearing two pairs of gloves would prevent a sharps related injury but that there
would be a significant decrease in occupational exposure via cutaneous means. One
of the main concerns in glove perforation rate is awareness of the perforation. The
longer the glove wearer is unaware of the perforation. the longer the skin may be in
contact with potentially infectious pathogens and the greater the risk of disease
transmission. It has been found that hepatitis B and other blood-borne pathogens can
be transmitted through small breaks in the skin (Weiss, Goedert and Gartner, 1988).
Thus, double gloving is one way to decrease the risk of disease transmission from
skin contact with potentially infectious organisms.
2.3.2. Eye Protection
The wearing of protective eyewear is another barrier method of standard
precautions. According to the NHRMC guidelines, "protective eyewear or face
shields must be worn during procedures where splashing, splattering or spraying of
blood or other body substances may occur" and "protective eyewear... must be
optically clear, anti-fog and distortion free, close fitting and should be shielded at the
side" (NHRMC, 1996, pA7). According to the Australian College of Operating
Room Nurses (ACORN) "the multidisciplinary team shall wear protective apparel
and use equipment to minimise the potential for direct contact with body fluids" and
17

Criteria 3.1 states that the perioperatlve nurse shall "ensure that protective eyewear
and face masks are worn" (ACORN, 2000, Reference A26, p.2 of 4).
Hersey and Martin (1994), found that only one tenth of patient care staff,
physicians, and housekeeping staff (n=3094) surveyed via a self-report questionnaire
always used protective eye wear. Since then, several studies on preventing
intraoperative blood exposures have documented the significance of and
recommended the use of protective eye wear.
In a study of skin and mucous membrane contacts (n=1382 surgical
procedures observed), the rate of eye mueous membrane contacts was 1.3% of the
time in surgeons using no facial protection other than a surgical mask and
significantly lower among those using eyeglasscs (0.1 %), or face shield or goggles
(0%) (Tokars et ai, 1995).
Two years latcr, In a nationwide study (n=6005 surveys returned) of
compliance among Danish physieians, Nelsing, Nielsen and Nielsen (1997) found
that only 35% of physicians were compliant with standard precautions. Additionally,
in an analysis of 320 splash exposures, the exposure was potentially preventable in
98% of the cases if masks and proteetive cye wear were worn. Nelsing, Niclsen and
Nielsen (1997) also concludcd that blood splashes in the eyes wcre the most frequent
occupational exposure in the operating room.
Ovcr time, observed compliance of operating room personnel (n=597
healthcarc procedures observed) wearing protcctive eye wcar, specifically goggles,
has been markedly higher (39%), while use of face shields remains low (5%)
(Akduman, Kim, Parks ct ai, 1999).
18

2.3.3. Safe Shnps Handling
There is a high potential for percutaneous injuries to personnel from the use
of sharps in the operating room environment. ACORN Standard A26 recommends
"the multidiseiplinary learn shall take precautions to minimise injuries caused by
sharp instruments:' whieh includes use of a hands-free technique for passing sharps
and not recapping needles (ACORN, 2000, Reference A26: p.3). Sharps include
anything that has the potential to perforate the skin, for example, scalpel blades,
suture needles, scissors, wires and hypodermic needles. The likelihood of injuries
may be inereased for several reasons. such as the continuous passage of sharps
between co-workers, eonfined workspace, poor visibility of the surgical field by
some team members and, quite often, the need for speed (Davis, 1999). It is
estimated that percutaneous occupational exposures occur in 15% of surgical
procedures (Pugliese, 1993). In a recent study by Jagger and Perry (2000) the most
frequent cause of occupational injuries in the OR was sharps injuries. The practice
of safc sharps handling encompasses several specific self-protective behaviours in
thc operating room to reduce the incidence of percutaneous inj ury. These behaviours
include, but are not limited to announcing sharps transfers, using a hands-free
technique when transferring sharps, and not re-capping hypodcrmic needles. Each of
thcsc self-protcctive behaviours will be cxamined more closely.
2.3.3.a. Announcing Sharp Transfers
Sharps are frequently transferred or passed from one team mcmbcr to another
during thc course of a surgical procedure. Thc usual route of sharps transfer is
between the scrub nurse and the surgeon, and thc second most usual route is between
the scrub nurse and the first assistant surgeon. When the passage of sharps betwecn
19

members of the serub team is preceded by a verbal announcement of the transfer, the
team members become more aware of the inherent danger and proceed with caution
(Kovach, 1993). The scrub person should verbally alert the surgeon when passing a
sharp item to the neutral zones. After the sharp is used, the surgeon returns the item
to the neutral zone and verbally alerts the scrub person.
2.3.3.b. Hands-free sharp passage technique
Sharp injuries can oceur during the passage of sharps from one member of the
surgical team to another (Kovaeh, 1993). The safest method to prevent injuries from
sharps on the sterile field is the hands-free technique instead of hand-to-hand passing
of needles or sharps between the surgeon and the serub person (AORN, 2000).
Hand-to-hand passage of sharps can be eliminated in several ways, including using a
neutral zone for passing sharps or using a transfer dish. The neutral zone method
involves establishing an area among the team where sharps will be placed for
retrieval. This neutral zone may be on the may06 stand, on an instrument mat or any
other place that has been decided by the team and that all members of the team are
fully aware. The transfer dish method involves placing all sharps for passage into a
container or dish so that two hands are not attempting to handle one sharp at the
same time. The scrub nurse passes the sharp to the surgeon in a dish and the dish is
left in a convenient, safe place for thc surgeon to place the sharp when it is no longer
needed.
, A neutral zone is an area, agreed to by the surgical team, where sharps are placed for retrieval toavoid hand to hand passage ofsharps.
6 The mayo stand is a piece of furniture that is situated over the end of the operating table near thescrub nurse once the patient is prepped and draped to establish a sterile field. It is traditionally the"domain" ofthe scrub nurse and serves as a working table for easy retrieval of instruments that will befrequently used during a surgical procedure.
20

2.3.3.c. No Needle Recapping
One study in the early 1990s found that almost 50% of the nurses surveyed
still fe-capped needles using the two-handed tcehnique (Troya, Jackson, Lovrich and
McPherson, 1991). In a comparison of observed and self-reported behaviour among
emergency department staff (during 270 observations eneompassing 1,018 healthcare
worker observations), Henry, Campbell and Malei (1992) also reported a compliance
rate of 51 % with not recapping, and of these, 79% recapped using the two-handed
technique. Additionally, nurses were observed to recap more frequently than
physicians and the three top reasons for re-capping using the two handed technique
were time (71%), dexterity (61%) and perception of patient as low risk (50%)
(Henry, Campbell and Malei, 1992). Two years later, in another study comparing
observed behaviour (n=1822 observations) with self reported behaviour of
emergency department personnel Henry, Campbell, Collier and Williams (1994)
reported the compliance with not recapping needles had decreased to 34%, and of
these 78.1% used the two handed technique. Both of these studies also highlighted
that personnel are not fully aware of their own non-compliance as evidenced by the
difference between the observed behaviours and the self reported behaviours.
2.4. Compliance with Standard Precautions
In the previously available literature, complianee with standard precautions
has fluctuated over the years, increasing for some standard precaution behaviours
and decreasing for others.
Henry, Campbell, and Maki (1992) observed emergeney room physicians to
use gloves more frequently (81.8%, n= 194) than nursing assistants (71.6%, n=95) or
registered nurses (61.5%, n=192) and registered nurses were observed to reeap more
21

frequently (61.5%, n=200) than physicians (45.3%, n=75). In a follow up study of
emergency department personnel in two community hospitals (n=1822 procedures),
Henry, Campbell, Collier and Williams (1994) observed gloves used at the
appropriate time 67.2% of the time, goggles used at the appropriate time 50.7% of
the time and needles recapped 34.4% of the time. Both of these studies compared
observational data on compliance with self-reported compliance and both studies
concluded that healthcare workers have a tendency to significantly overestimate their
compliance.
In a more recent prospective observational cohort study of operating room
procedures (n=597 healtheare worker procedures), Akduman, Kim, Parks et al (1999)
obseIVed that 41 % wore goggles or face shields, 32% wore regular glasses, and 24%
used no eye protection. Scrub nurses and medical students were more likely to wear
goggles (60% of the time) than other healthcare workers (Akduman, Kim, Parks et
aI, 1999). These authors also found 28% of health care workers double gloved, and
use of double gloves was highest for house staff (43%) than for medical students
(26%) and scrub nurses (15%). Lastly, Akduman, Kim, Parks et al (1999) found that
sharp transfers were not announced in 91% of surgical proeedures.
Several self-report studies also found significant differences in compliance
between healthcare professional groups and different standard precaution behaviours.
In a U.S. national survey (n=3094 hospital workers), Hersey and Martin (1994)
found that only 56% of physicians and 55% of health care staff reported receiving at
least one of the injections recommended in the hepatitis B vaeeination series and
about 50% of health care staff reported that they reeapped used needles. In a
convenience sample of 84 nurses and 26 physicians, JetTe, Mutha, L'Ecuyer et al
(1997) found that 47% agreed that they always wore double gloves when performing
22

an invasive procedure, 84% disagreed that prescription glasses without side shields
were adequate protection, 79% disagreed that they would only report an occupational
exposure if the patient was known to be positive for HIV, AIDS, HBV or HeV, 89%
agreed that it was OK to dispose of sharps in appropriate receptacles without
recapping and 84% agreed that every hospital employee should receive the hepatitis
B vaccine. Also significant was that more surgeons (58%) than OR nurses (37%)
disagreed with the need to double glove for all invasive procedures. In a nation-wide
survey of Danish physicians (n=6005), Nelsing, Nielsen and Nielsen (1997) found
the following compliance rates among 'surgeons and pathologists' and 'other
physicians' are as follows: gloves, 63% and 23.4%, respectively; protective eyewear
11.5% and 4%. respectively. In a survey of surgeons (n=768), Patterson el al (1998)
fOWld that 92 of 768 surgeons reported thai they always use double gloves and only
83 surgeons reported that they usually use double gloves. In a survey of post
anaesthesia care nurses (n=26), Tait et al (2000) found that 81 % reported always
complying with standard precautions guidelines when caring for an HIV or HBV
infected patient, but only 31.1% complied if they thought the patient was low risk.
Michalsen, Delclos, Felknor et aI, 1997; and Nelsing, Nielsen, and Nielsen, 1997).
Previous research that focused on operating room personnel, and specifically,
operating room nurses, reported incidence of exposure but not necessarily incidence
of compliance with standard precautions to prevent exposure (Lynch and White,
] 993; White and Lynch, 1993; Tokars et. ai, 1995; White and Lyneh, 1997; Mujeeb,
Khatri and Khanani, 1998).
Improving compliance rates with standard preeautions is possible. Sahdev et
a1 (1994) reported "significant improvement in compI iance after a three phase
intervention of informational material in prominent places, seminars, and
23

administrative mandates threatening sanctions for noncompliance" (p.100). White
and Lynch (1997) also reported improved compliance with standard precautions after
involving operating room personnel in identifying high-risk behaviours and
situations and developing strategies for improving compliance.
2.5. Occupational Exposure in the Operating Room Environment
Oeeupational exposure is an incident in which the healthcare worker has been
exposed to potentially infectious blood or body fluids from a patient by
percutaneous, mucocutaneous, or cutaneous exposure; or by any combination of the
three7,
By nature of the work environment, operating room nurses are at high risk for
occupational exposure. The incidenee of mucocutaneous and cutaneous exposure far
exceeds that of pereutaneous exposures and may occur in 30-50% of surgical
procedures (Wright et aI, 1991; Pugliese, 1993). The incidence of occupational
exposure from a percutaneous injury occurs in up to 15% of surgical procedures
(Pugliese, 1993). The most common mechanism of injury of percutaneous exposures
in the operating theatres is by needlestick, more specifically, a solid suture needle,
which was imphcated in one study to cause 67% of sharp injuries observed (Wright
et ai, 1991).
2.6. Occupational Exposure and Incidence of Disease Transmission
The greatest risk for occupational transmission of blood-borne infections is
from occupational exposure by percutaneous injury from needles and other sharp
objects (Pugliese, 1993). Independent studies have shown that the risk of acquiring
hepatitis B after a single percutaneous exposure is 30%; Hepatitis C risk ranges from
24

2.70/0 to 10%; and HIV risk is 0.3% (Short and Belt, 1993). There has also been a
documented case of HIV transmission after mucocutaneous exposure (Short and
Bell, 1993).
Although we cannot detennine the risk of contracting a blood-borne infeetion
from occupational exposure simply by knowing the incidence of occupational
exposure, we can conclude that reducing exposure reduces the risk (Telford and
Quebbemann.1993).
2.7. UDder Reporting of Occupational Exposures
It is estimated that 40-90% of pereutaneous injuries by healthcare workers are
unreported (Short et ai, 1994). As far back as 1983, studies have reported the
underestimation of occupational exposures by healthcare workers. Hamory (1983)
surveyed 1429 university hospital employees and from data based on 726 responses,
showed that 40% of needlestiek injuries had not been reported in the past three
months and that 75% of needlestick injuries had not been reported in the previous
year.
In another study of internal medicine house staff, 19% recalled aceidental
exposure to HIV infected blood and 36% recalled exposure to blood of high-risk
patients in the past 12 months, and of these, only 30% were reported (Mangione,
Geberding and Cummings, 1991). The principle reasons for not reporting were time
constraints, perception that the injury was not a significant exposure, lack of
knowledge about the reporting mechanism, concern about eonfidentiality and
professional discrimination (Mangione, Geberding and Cummings, 1991).
1 The lerms "pereutaneous", "mucocutaneous" and "cutaneous" are defined in Appendix 2-ConceprualDefinitions.
2S

[n a study that same year, Tandburg (1991) found that 35% of occupational
exposures recalled by emergency department personnel were formally reported.
Furthermore, physieians recalled more exposures (mean=3.8 exposures recalled) than
emergency medieal technicians (mean--=2.8 exposures recalled) or nurses (mean=1.8
exposures recalled) and, of these, nurses formally reported (mean=1.25 exposures
reported) occupational exposures more frequently than physicians (mean=0.26
exposures reported) or emergency medical technicians (mean=0.85 exposures
reported). Tandburg (1991) eoneluded that perception of risk. oeeupation, years in
occupation, and concern about excessive paper work were the most common
predictors of low reporting rate.
The percentage of occupational exposure risk in the operating room IS
considered low in comparison to hospital wide risk probably because of inadequate
reporting of exposures in the operating room (Jagger, Hunt and Pearson, ]990). In
the early 1990s, several studies were conducted on risk of exposure, compliance with
infection control policies and procedures, and lack of reporting of oecupational
exposures in operating rooms in the United Slales (Telford and Quebbemann. 1993;
Pugliese, ]993; Short and Bell, 1993). Occupational exposures among operating
room personnel have been substantially underreported in incident reports by as much
as a factor of twenty five (Lynch and White, 1993).
Studies in the United States have shown reasons for not reporting
occupational exposures in the operating room include perceptions of lack of benefit
of reporting, inconvenience because of where staff must go to report, too much
paperwork, and embarrassment (Williams, Campbell, Henry and Collier, 1994).
Unfortunately, hospitals typically rely on incident reports on occupational exposures
26

to determine the frequency of exposures and the need for improving measures to
decrease and/or prevent them (Lynch and White, 1993).
2.8. Benefits of Occupational Exposure Reporting
There are several benefits of reporting occupational exposures and it is in the
best interest of the operating room nurse to report all oecupational exposures.
Studies have concluded that treatment with prophylactie agents within 24 hours of
exposure decreases the risk of some disease transmission (CDC, 1998a; CDC, 1998~).
In a retrospective case-controlled study of health care workers, after eontrolling for
other risk factors for HIV transmission, the risk for HIV infection among health care
workers who used a prophylactie anti retrovi ral agent (e.g. zidovudine) was redueed
by approximately 81 % (Cardo, Culver, Ciesielski et ai, 1997). In the case of HBV, a
positive test for hepatitis B surface antigen (HbsAg) indieates that the souree person
is actively infected and potentially infectious and a positive test for hepatitis B e
antigen (HbeAg) indicates that the source person is infectious (NHMRC, 1996).
Antibody to HbsAg is considered to be a protective antibody and is present in
persons who have recovered from acute HBV infection and in those who have been
vaccinated. Health care personnel who are persistent non-responders to hepatitis B
vaeeination should be offered hepatitis B immunoglobulin (HBIG) within 48 hours
of parenteral exposure to HBV (NHMRC, 1996). In the case of HCV, although
interferon has been approved in the US for the treatment of chronic HCV, no
assessments have been made of post exposure use of antiviral agents to prevent HCV
infection (CDC, 1998b).
Another benefit of reporting occupational exposures is that reporting the
ineident will ensure appropriate follow up with reminders for treatment and
subsequent follow up.
27

Still another benefit of reporting occupational exposures is the use of the
initial report in assisting the operating room nurse in future elaims of workers
eompensation for medical treatment or possible loss of income following an
exposure and subsequent disease transmission. The direct costs for one incidence of
occupational exposure have been estimated to be in access of $3500.00 ($USD) per
healthcare worker (Johnson and Johnson Medical, Inc, 1995). In addition, there are
indirect costs, which include filing of worker's compensation fonns, occupational
health and safety reports and other administrative paperwork. There is also the
potential increase in liability premiums and legal fees. By reporting an oceupational
exposure, the operating room nurse can better support his/her claims for
compensation and assistance with proof that disease transmission may be a direct
result of the occupational injury incurred.
2.9. Summary and Conclusion
Although the early focus of infection eontrol has been on the prevention of
nosocomial infection, the focus of concern has changed to prevention of the
healthcare worker acquiring a blood borne infection secondary to oecupational
exposure in the workplace. In response to this ehange in focus of eoneem, CDC
instituted universal precautions in the United States. This eoncept was adopted in
Australia, albeit in an expanded fonn, and ealled Standard Precautions. Standard
precautions is the first line of defense in infection control and diligent use of standard
precautions, such as double gloving, wearing adequate protective eye wear, and safe
sharps handling has been demonstrated to decrease the risk of disease transmission
following an occupational exposure.
The risk of pereutaneous oeeupational exposure in the operating room has
been estimated as high as 15% and almost 50% of surgical procedures result in
28

mucocutaneous or skin exposures. In addition, disease transmission following
occupational exposures has been documented previously in the literature. It is in the
bcst interest of operating room nurses to comply with standard precaution guidelines
in the first instance and to promptly report any exposures in order to obtain
appropriate treatment and follow up, thus decreasing the risk of disease transmission.
Now that the history of standard precautions and the efficacy of complianee
in reducing occupational exposure, as well as the benefits of reporting exposures and
the prevalence ofunderreporting has been presented, a problem becomes apparent. If
certain measures and self-protecti'IJe beha'IJiours ha'IJe been demonstrated in the
literature to reduce the risk ofoccupational exposure and disease transmission. why
is compliance with these behaviours less than 100%? A plan must now be devised to
address the problem. The plan or methodology chosen to address this problem will
be diseussed in Chapter 3.
29

Chapter 3. Methodology
3.1. Introduction
This ehapter will diseuss the methodology chosen to investigate the issues
surrounding complianee with standard precautions and occupational exposure
reporting. According to Bums and Grove (1997), quantitative research attempts to
"describe variables, examine relationships among variables and determine eause-and
effect interactions between variables" (Burns and Grove. 1997. p. 27). A quantitative
methodology was chosen for this study because the intent of this study was to
describe relationships that might exist between speeific variables (or influences) and
standard precautions and occupational exposure reponing behaviour of operating
room nurses in Australia.
The chapter begins with a description and rationale for ehoosing a
deseriptivc, correlational design to conduct the study. Following this, is a discussion
of the theoretical framework chosen to provide structure to the data collection
proeess. The theoretical framework utilised in this study was the Health Belief Model
(Becker, 1974).
This chapter then proceeds with a description of the sample population and a
detailed discussion of the data eolleetion process, ineluding ethieal considerations
impacting on the data collection procedure and the eonstruetion and testing of the
data colleetion instrument. The chapter concludes with a brief description of the data
analysis plan and a discussion on the limitations of the methodology.
30

3.2. Design of the Research Study
The research design chosen for this study is a descriptive correlational design.
"The purpose of a descriptive correlational design is to examine the relationships that
exist in a situation" (Burns and Grove, 1997, p. 259). By utilising this type of
research design, interrelationships that exist in a situation between variables can be
examined and identified in a short period of time. With a correlational descriptive
design, the researcher is not attempting to control or manipulate the situation nor to
establish any causality between the variables, but 10 predict relationships among
variables (Bums and Grove, 1997). Protection against bias is achieved through (1)
linkages between conceptual and operational definitions of variables, (2) sample
selection and size, (3) data collection procedures that achieve some environmental
control and (4) valid and reliable instruments (Bums and Grove, 1997).
Data obtained from this type of design can be used to identify problems with
current practice and provide knowledge about the variables and the population that
can be used in further research to develop specific interventions to alleviate the
current problem. Correlational studies are also used to develop hypotheses for future
studies.
In this study, an attempt is being made to establish a relationship between
variables that may influence the undertaking of self-protective behaviours, that is,
complianee with standard precautions and occupational exposure reporting. By
utilising a theoretical framework, these variables are given meaning and logical
conclusions can be then drawn about which variables have the greatest influence
over the health behaviour. As mentioned previously, the theoretical framework
utilised in this study is the Health Belief Model.
31

3.3. Theoretical Framework-The Health Belief Model
United States public health researehers began to develop models to identify
appropriate targets for health education programs in the 1950s and 60s (Davidhizar,
1983). Early research suggested that health beliefs were correlated with behaviour
and could be used to differentiate between those who did and did not undertake these
behaviours (Rosenstock, 1974). This theory was supported in the first instance by
the Hochbaum (1958, eited in Becker, 1974) studies on uptake of xray screening for
tuberculosis and later by Kegel's (1963. eited in Becker, 1974) study of the uptake of
preventative dental care to prevent the worst imagined dental problems. Several
other supportive studies followed. Haefner and Kirseht (1970, eited in Beeker, 1974)
later extended the model to postulate that educational interventions designed to
increase perceived susceptibility or perceived severity led to an increase in doctor's
visits merely for routine 'check up'. Becker (1972, eited in Becker, 1974) further
extended this model to include eompliancc with medical regimens.
The Health Belief Model (HBM) describes specific variables that influence
whether or not an individual will undertake particular health behaviours. These
variables include (1) perception of risk or susceptibility to the illness, (2) perception
of severity of the illness, (3) perception of benefits of undertaking a recommended
health behaviour, (4) perception of barriers or costs of undertaking a particular health
behaviour, and (5) cues to action that trigger the health behaviour (Davidhizar,
1983). The first four variables have been tested and demonstrated in subsequent
researeh, but the difficulty in testing eues to action was recognised, especially in
retrospeetive studies, beeause of the individuality of this variable (Rosenstoek,
1974). In later versions of the Health Belief Model the construct of health
32

motivation or the desire to undertake the partieular health behaviour was added
(Champion, 1984).
The HBM is a model based on the interaetion of the individual's readiness to
comply with the behaviour and the motivating and enabling factors that detennine
what the individual will do (Ross and Mico, 1980). Readiness depends on
pereeptions of risk and severity of acquiring a blood-borne infection, as well as
perceived benefits of undertaking the self-protective behaviours. Motivating and
enabling factors include the individual's personal eharacteristics, previous
experience, social pressure, and barriers to undertaking the behaviour. This
interaction detennines the likelihood of compliance with recommended self
protective behaviours. It is the interaction of these variables and other modifying
variables, such as demographics, that allow for the predietion ofhealth behaviours.
In order to provide the variables with theoretical meaning, a set of
conceptual definitions has been compiled for this study (see Appendix 2). In future
studies, interventions aimed at these variables can be developed to exert the greatest
impact on changing the health behaviour.
3.4. The Sample/Study Population
When utilising a eorrelational deseriptive researeh design a representative
sample that refleets the full range of scores possible on the variables being measured
needs to be seleeted for the study (Bums and Grove, 1997). The target population
being studied is operating room nurses in Australia. A sample population was
seleeted from the accessible population of eurrent members of ACORN, the
professional nursing organisation representing operating room nurses in Australia.
The total membership at the time of survey distribution was 1710 members. Based
on calculations using a 95% eonfidence level and confidence interval of 7, it was
33

detennined that at least 176 members must be surveyed in order for the study sample
to be representative of the total ACORN membership. Knowing this, and also that
the return rates for mail out questionnaires ranges from 25 to 30% (Bums and Grove,
1997), 500 questionnaires were distributed. To obtain a study sample that reflected
the state representation in ACORN, subjects were chosen from the sampling frame of
ACORN membership using a stratified random sampling method, based on the
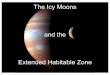
proportion of ACORN members per state in Australia (see Figure 1). The only
sampling criteria for inclusion in the study sample were current membership III
ACORN and a mailing address in Australia at the time of survey distribution.
50%
45%
40%CD 35%tJ)lIS- 30%c:CDUI- 25%CDa..g. 20%.s::.III 15%I-ell
.Q10%E
ell:::E 5% .
0% 2%I- ;: C c2: (J) (.) c2: I-(.)
(/) -I (/) <: S 3: z« z a I-
State
Figure 1. ACORN Membersbip Distribution by State
34

3.4.1. Response Rate
Two hundred and thirty of 500 questionnaires were returned (46%). Three
questionnaires were disearded beeause they were returned with no answers selected
for questions in Seetion I and/or II and/or III. Thus, 227 questionnaires were included
in the analysis. This 45% response rateS represents 13% of the total membership of
ACORN.
3.4.2. Demographics of the Sample
The majority of the respondents were female (96.5%) registered nurses
(96.9%), ranging in age from 23 years to 64 years old (mean ± S.0.9, 42.76 ± 8.44).
Most of the respondents were hospital-trained nurses (74.3%) with greater than ten
years post registration experience (83.8%) and greater than ten years of serub nurse
experience (67%) (see Appendix 8). Sixty pereent of the respondents reported
working full time. Of the questionnaires included in the analysis, 65% of the
respondents were employed in public hospitals and 31.4% reported working in
private and/or day only hospitals (3.6% either selected no answer or more than one
answer).
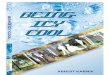
There was less variability in distribution of number of beds in the facility and
number of operating theatres. Facility size ranged from less than 100 beds to greater
than 600 beds, with most respondents working in medium sized facilities (see Figure
2). The number of theatres ranged from 1-2 theatres to greater than 8 theatres, with
most respondents working in operating suites with 3-5 theatres (see Figure 3).
8 This 45% return rate is higher than lhe 25-30% return rate for mail out que~tionnairesestimated byBums and Grove (1997). If anonymity of respondents were sacrificed, a seeond mail au t to oonresponders may have yielded a higher return rate.
9 S.D., Sumdard Deviation
35

Figure 2. Number of Beds in Facility
Figure 3. Number of Operating Theatres
[J < 100 beds1i:1101-300 beds11301-600 beds.> 600 beds
1!11-2 theatres
El3-5 theatres
115-8 theatres
II> 8 theatres
36

Most respondents worked in New South Wales and ACT (33.9%), and
Victoria (30.8%). State demographics were proportional with distribution of
ACORN members across states (see Figure 4).
Distribution of ACORNMembership by State
o Returned SUl'\eys byState
50%
45%
40%
35%
- 30%c:G)(,) 25%10-G)
20%c..15%
10%
5%
0%ACT NSW OLD SA TAS VIC WA NT
State
Figure 4. Percent of Surveys Returned Compared to ACORN MembershipDistribution by State
3.5. Data Collection Process
Data collection was via a self-report mail-out questionnaire. Five hundred
questionnaires were mailed to a stratified random sample of ACORN members. As
mentioned in the previous section, the only sampling criteria for inclusion in the
study sample were current membership in ACORN and a mailing address in
Australia at the time of questionnaire distribution.
Advantages of using a self-report mail out questionnaire in comparison with
face-ta-face interviews or telephone surveys are response rates, quality of answers,
and implementation of the survey.
37

Although response rates for mail out sUlVeys have been estimated at 25-30%
(Bums and Grove, 1997), a well administered mail out survey ean yield higher rates
at a mueh lower cost than face-lo-face or telephone sUlVeys (de Vaus, 1995).
Telephone and face-to-face interviews may yield higher results in general
populations, but mail out surveys ean yield response rates at least equal to those from
telephone or face-to-face interviews in specific, homogeneous populations (ie
professional groups) (Dillman, 1978, cited in De Vaus, 1995). A potential low
response rate was accommodated in this study by sending out a large number of
questionnaires (n=500) in comparison to the number needed to analyse (n=176). This
adjustment proved successful in the 46% return rate.
Another advantage of the mail out survey is the quality of answers. In faee
to-face interviews there is an increased ehanee for bias as respondents may be
inclined to answer controversial questions in a way that they perceive as socially
acceptable and "even the best-trained intelViewers can affect the way respondents
answer questions" (de Vaus, 1995. p. I 10). Mail out surveys have the ability of
avoiding distorted responses that may be due to interviewer characteristics and/or
opinions (de Vaus, 1995).
Another advantage of a mail out survey is in implementation of the survey.
Face-to-face interviews and telephone interviews are resource intensive, usually
requiring suitable staff and time. Additional costly expenditures include interviewer
training, travel and increased utility fees (eg long distance phone charges). National
face-to-face interviews could cost as much as five times more than telephone
interviews and up to twenty times more than mail out surveys (de Vaus, 1995). The
eost of mails out surveys are barely affeeted by distance and the costs of printing
usually decreases with sample size (de Vaus, 1995).
38

A disadvantage of mail out surveys is the bias introduced in trying to obtain a
representative sample. This bias may be due to the sampling frame and the inability
to obtain answers from non-responders. These disadvantages will be discussed in
more detail later in this ehapter in section 3.12, Limitations ofthe Study.
3.S.1. Ethical Considerations
Ethical considerations impacting on data collection were in the areas of
informed consent and confidentiality. The University of Canberra Human Ethics
Committee approved this project. In order to ensure that respondents were
adequately informed about the research study, a cover letter explaining the aims of
the research proposal accompanied each questionnaire distributed (see Appendix 3).
Contact details of the investigator and supervisor were given for queries about the
project. An information sheet for participants that contained information about data
collection also accompanied each questionnaire (see Appendix 4). This information
sheet included a statement that indicated informed consent would be implied by
returning the completed questionnaire.
In order to ensure that respondent information was treated anonymously
identifying only general demographic data was solicited on the questionnaire. No
other personal infonnation was required on the questionnaire. The questionnaires
were sent to a eouneil representative of ACORN who agreed to assist in the
distribution of the questionnaire. The ACORN councilor received the questionnaires
in sealed, stamped envelopes (which also included a pre paid return envelope). The
ACORN councilor generated mailing labels from ACORN's membership list based
on randomisation parameters set forth by the investigator. The ACORN eouneilor
affixed the mailing labels and posted the questionnaires. Although an organisational
mailing list was used to distribute the questionnaire, the researcher did not have
39

access to this mailing list. Completed questionnaires were returned directly to the
study investigator anonymously via the prepaid return envelopes enclosed with each
questionnaire. The questionnaires were distributed in this way to ensure the
anonymity of the sample population from the researcher and to ensure that the
personal information of the members was protected by ACORN.
In order to ensure eonfidentiality of the data returned questionnaires and other
paper data will be kept in a locked file cabinet at the University of Canberra for five
years. Computer data will only be aeeessible by password of the researcher.
3.5.2. Development of Instrument
This study attempts to establish relationships between variables (influences)
and compliance with standard precautions and occupational exposure reporting.
Therefore, an instrument was developed to test and explore these relationships. By
using an instrument that allows collection of data of speeific variables, relationships
between the variables can then be established.
The data collection instrument, The Standard Precautions and Oeeupational
Exposure Reporting (SPOER) Survey (see Appendix 5) was based on questions
adapted from a study by Champion (1984). Questions about perceived risk and
susceptibility of acquiring a blood-borne infection and perceived benefits and
barriers to undertaking standard precautions and occupational exposure reporting
were modified from questions developed by Champion (1984). Champion's
questions were previously tested for internal consistency and reliability in application
of the Health Belief Model in the prediction of undertaking health behaviours.
Additional questions were formulated to determine level of compliance with standard
precautions and occupational exposure reporting behaviour and to gather basic
demographic information.
40

The purpose of questions In Section I of the SPOER was to collect
demographic infonnation about the respondents. The purpose of the questions in
Section II was to gather infonnation about the respondents' attitudes, beliefs and
compliance with standard precautions. Questions in Section III were included to
gather information about the respondent's attitudes, beliefs, and compliance with
occupational exposure reporting. Respondents were asked to mark the questions in
Sections 2 and 3 using a Likert type scale. The usual response set was a choice of
five responses (i.e. "strongly agree", "agree", "neutral", "disagree", and "strongly
disagree"). Three questions requiring either a "yes" or "no" answer were included in
Section II regarding hepatitis 8 vaccination status and monitoring of HBV and HIV
slatus.
The SPOER survey was checked for eontent validity by review from four
operating room nurses with at least five years of operating room experienee who
were currently employed at the Clinical Nurse Speeialist level or above. Comments
and suggestions were taken into aecount and appropriate changes were made. The
Cronbach Alpha statistic was used to test the questionnaire items for internal
consistency. The Survey Resource Group at a public teaching hospital, the Operating
Room Nurse Manager at the same public teaching hospital, and the Operating Room
Nurse Manager at a private hospital approved the SPOER Survey for distribution.
The University of Canberra Ethics Committee on Human Research also granted
approval for the study. The SPOER survey was then piloted on a small sample of
operating room nurses in the ACT.
3.5.3. Pilot Study
The SPOER Survey was piloted among operating room nurses at two
hospitals In the ACT. Respondents were asked to write comments about the
4\

questionnaire. Fifty questionnaires were distributed, twenty-five to a public hospital
and twenty-five to a private hospital. Twenty-six questionnaires were returned for a
response rate of 52%1. The SPOER Survey was aecompanied by a participant
infonnation sheet outlining the purpose of the study, contact details of the researcher
and eontact details to make complaints about the study. Based on the type and
quality of data and infonnation obtained from this pilot study, the data collection
instrument was revised.
3.5.4. Revision of Instrument
The validity of the questionnaire can be threatened if respondents fail to
answer all the questions. This may occur because they do not agree with available
choices and write comments in the side that cannot be coded or included in the
analysis. For this reason, the format of questions was revised in the following
manner. Questions pointed out as ambiguous by either reviewers or pilot
questionnaire respondents were omitted or reworded. Questions left blank by more
than 90% of the subjects were omitted. Questions with several ehoiees were
converted to closed ended questions with Likert scaled choices. Open-ended
questions were omitted because of the difficulty in coding answers and the ambiguity
of some answers. The question regarding area of practice was omitted and the
question regarding previous operating room experience was reworded to reflect
Scrub experience only. This was done because of the number of incomplete
questionnaires returned from nurses who reported themselves to be Anaesthetic
Nurses or Recovery Room Nurses. The majority of questions were changed to Likert
response questions with the same five responses (i.e. strongly agree, agree, neutral,
disagree, strongly disagree) for ease of response. Questions about reasons why you
would not undertake certain behaviours were changed from open ended to Likert
42

type responses to facilitate coding. Questions on frequeneies were changed so that
"none" was a category on its own. This was done because of the difficulty in
separating 'no' exposures from a small number of exposures (i.e. "'lor 2") when
analysing the pilot survey data. Although the exelusion of open ended questions may
be considered a limitation in the quality of data collected (ie qualitative), for the
purposes of this study (ie to gain baseline data), closed endcd questions were
considered suitable by the researcher for this study.
The revised survey (see Appendix 5) was distributed 10 a sampling frame of
500 financial members ACORN. These subjects were selected using a stratified
random selection process in order to obtain a sample population proportional to the
distribution of the total ACORN membership (n= 1710) in each state/territory in
Australia.
3.6. Reliability and Validity of tbe Instrument
3.6.1. Reliability
Reliability is the consistency of measure. It is the amount of random error in
the measurement technique. For well-developed instruments the lowest acceptable
reliability coefficient is usually 0.80, although for a new instrument, 0.70 is
considered acceptable (Polit and Hungler, 1995). Reliability testing using Cronbach's
alpha coeffieient was utilised to test each item of the instrument for internal
reliability within the construct scales of the Health Belief Model. Items yielding low
eorrelations with their respective seales were deleted, and internal consistency was
re-calculated (see Appendix 6 and 7). "When further deletion... [begins] to decrease
the alpha coeffieient, seales... [are] considered to be at maximum reliability"
(Champion, 1984, p. 80). The construct seales of risk and severity had consistency
43

coefficients of 0.71 and 0.70, respectively. The scales for benefits of standard
precautions and occupational reporting had consistency coefficients of 0.51 and 0.34.
respectively. Scales for barriers to standard precautions were sub grouped inlo
double gloving, eye protection and hepatitis B vaccination. These three barrier
scales yielded consistency coeffleients of scales 0.78, 0.76 and 0.93, respectively.
The scale for barriers to mueocutaneous occupational exposure reporting produced
consistency coefficients of 0.87 and for barriers to percutaneous occupational
exposure reporting Cronbach's alpha was .86. Seales with a Cronbach's alpha
coefficient less than 0.70 were not included in the analysis, unless otherwise
indieated.
3.6.2. Validity
Validity is the extent to which the instrument actually measures the concepts
being studied (Burns and Grove, 1997). Content validity evidence examines the
extent to which the instrument covers all major aspects relevant to the construct
being measured. This comes from the literature, the representativeness of the
sample, and content experts. Four perioperative nurses, each with greater than five
years experience, reviewed the SPOER survey. There were a total of 43 years of
perioperative nursing experience between the reviewers. Two of the reviewers were
working as clinical nurse specialists. The third reviewer was a clinical nurse
consultant and the fourth reviewer was a perioperative nurse educator. hems marked
as questionable by at least 2 of the 4 reviewers were either reworded or omitted from
the questionnaire. The SPOER was reviewed prior to distribution for the pilot study
and then again before nationwide distribution.
44

3.7. Data Analysis
Descriptive statistics were applied to characterise the frequency of
distribution of variables. Demographic data and frequency tables were compiled
from the returned questionnaires. Relationships between demographic data and self
reported compliance with standard precautions and self reported occupational
exposure reporting were analysed using contingency tables and Chi square analysis.
The dependent variables were compliance with standard precautions (double
gloving, adequate eye protection, announcing sharps transfers, hands-free sharps
passage and no needle recapping) and complianee with occupational exposure
reporting. The independent variables were pereeived risk of infection, perceived
severity of consequences of infection, perceived benefits of compliance, and
perceived barriers to complianee with standard precautions and oceupational
exposure reporting. The five response categories for questions relating to compliance
were collapsed and re-coded into three categories. This was done for two reasons.
First, the more categories, the larger the table produced when performing eross
tabulations and the harder it is for the table to be read and understood (deVaus,
1995). Also, some response categories yielded very low frequencies in some
questions and low frequencies can produce misleading tables and distort some
statistics (deVaus, 1995). Therefore, ··Strongly agree" and "Agree" were coded as
"compliant." "Neutrar· was coded as "neutral." "Disagree" and "Strongly disagree"
were coded as "noncompliant."
The type of regression model employed depended on the dependent variables
analysed. The model ineluded univariate correlation regression. Univariate
correlation analysis, using Kendall's tau b was applied to describe any association
between compliance with standard precautions and occupational exposure reporting
45

and eaeh single independent variable. Strength of association was measured by the
eorrelation eoefficient. Statistieal significance (P) was assumed at the .05 level. The
analysis was performed using SPSS Version 9.1.
Analysis of data from this study will serve to provide a basis upon which to
develop and implement measures to improve standard preeautions and occupational
exposure reporting praetiees thus, minimizing occupational exposure and disease
transmission rates among this group.
3.8. Limitations of the Study
One of the limitations of the study is the sampling frame used. The sampling
frame was operating theatre nurses with membership in the professional organisation.
ACORN. Aeeording to the Australian Institute of Heallh and Welfare (1998), there
were 11,222 registered nurses working in operating theatres in Australia in 1996,
which is 7.3% of the registered nurse workforee. The number of these nurses
belonging to ACORN (n= 1710) represents 12.7% of operating theatre nurses.
Therefore, the generalisability of findings of this study should be limited to members
of ACORN. Future studies will need to also include nurses who are not members of
the professional body to obtain a more representative sample of all operating theatre
nurses in Australia.
Another limitation is the inability to eompare compliance rates of responders
with non-responders and this affect on bias of the sample. Although there are
statistical tests for minimising the affect of bias, the difficulty lies in not being able
to work out what the bias is and to what extent it oecurs (deVaus, 1995). One way to
make adjustments for this bias is to eompare charaeteristies of the sample with those
of the sampling frame. Since the researcher did not have direct access to
46

characteristics of the sampling frame, it was not possible to determine how closely
the eharaeteristics of the sample reflected the sampling frame.
A third limitation of the design of the study is the tendency for overestimation
of compliance via self-report: method. Previous studies utilising observation and self
reporting mechanisms found that "by comparing self-reported with observed
eompliance of standard precautions, healtheare work.ers tend to overestimate their
eompliance with proteetive barriers (Henry K, Campbell S, Collier P, Williams CO,
1994). Future studies may need to use a combination of self-reporting instruments
with prospective observation to improve estimates as well as to collect valuable
qualitative as well as quantitative data.
A fourth possible limitation of the study was the potential for a low response
rate, reported to be typical of a mail out questionnaire. This potential limitation was
pre-empted by first determining the minimum sample size required for the sample to
be representative of the sampling frame. Then, keeping in mind that the average
return rate for mail out questionnaires ranges from 25 to 30% (Bums and Grove,
1997), a sufficient number of questionnaires were distributed to ensure an adequate
return rate. The effectiveness of this technique was evident in the 46% return rate.
The response rate in future studies could be improved by including provisions for a
second mail-out to non-responders.
A final issue that may introduce bias into the results of this study is that
nurses in the ACT who participated in the pilot study were not excluded from
participating in the main study. Of the total respondents, eight (4%) were from the
ACT. Because of thc anonymity of the study it would be difficult to determine
whether any of the eight ACT respondents partieipated in the pilot study.
47

3.9. Summary and Concludon
The purpose of this study was to examine relationships between variables. In
order to do this, a descriptive, eorrelational design was employed. A theoretieal
framework, the Health Belief Model, was used to give the variables meaning and
allow logical conclusions to be drawn about which variables have the greatest
influenee over the health behaviour. Ethical considerations, in the areas of informed
consent and confidentiality, were eonsidered in the data eollection process. The data
colleetion instrument, the self~report SPOER survey, was approved and piloted
among operating room nurses in the ACT. The survey was revised based on pilot
study results and rc-testcd for content validity and internal reliability. The
questionnaire was then distributed anonymously to 500 members ACORN.
This chapter described and justified the plan, ineluding the methodology,
research design, data collection proeess and analysis plan, chosen to address the
questions of what is the compliance rate with standard preeautions and occupational
exposure reporting and what variables influenee decisions to comply or not eomply.
In addition. steps taken to ensure that the data collection would adequately address
the problem, as well as limitations of the methodology were outlined. The next step
in the research process is to implement the plan (ie methodology) through the
collection and analysis of data in order to obtain results that will provide answers to
the question. The data analysis plan includes a variety of statistical tests on
dependent and independent variables, including frequency tables, chi-square,
univariate eorrelation regression, and multivariate regression analysis. The results of
data analysis will be diseussed in Chapter 4.
48

Chapter 4. Results
4.1 Introduction
A data analysis plan including a variety of statistical tcsts on dependent and
independent variables, including frequency tables, chi-square, univariate correlation
regression, and multivariate regression analysis was utilised to obtain answcrs to the
research questions.
The results of this study revealed a less than 100% compliance with standard
precautions, with a range from 55.6% (for double gloving) to 92% (for wearing
adequate proteetive eyewear). The results of this study also revealed underreporting
of occupational exposures by a range of 8% to 58% for percutaneous and
mucoeutaneous exposures, respectivcly.
1n analysis of variables using the HBM, significant eorrelations were found 10
exist between perceptions of risk, severity, benefits and barriers with compliance of
both standard precautions and occupational exposure reporting. These correlations
varied depending on the specifie standard preeaution examined and the specific
question asked. One of the unique findings of Ihis study is that perception of barriers
demonstrated the most substantial relationship with compliance for double gloving,
wearing protective eyewear and reporting occupational exposures.
This chapter will present the answers to the research questions through
deseriptions of statistical outcomes paralleled with tables and graphs.
49

4.2. Compliance with Standard Precautions
Operating theatre nurses' mean compliance rate with the five standard
precautions behaviours that are the foeus of this study was high (72.1 %), but varied
considerably across individual standard precaution behaviours. (see Table 1).
Compliance was highest with adequate eye protection (92%, neutral 3.6%).
Compliance was lowest with double gloving, which yielded a response rate of 55.6%
(13.3% neutral).
In the subeategories of safe sharps handling, compliance was highest with no
recapping of needles (81.9%, neutral 5.2%). Approximately 59% of the respondents
reported always announcing sharps transfers (neutral 18.2%) and 71.9% of the
respondents reported using a hands free sharps passage technique (neutral 10.7%).
In the subcategories of technique of needle recapping, 21.4% of these
reported reeapping using the one handed teehnique (9.41)/1) neutral) and 4.9% reported
recapping using the two handed technique (5.8% neutral).
Most of the respondents (96.1 %) reported that they had been vaccinated
against HBV and 58.0% reported "yes" to having their hepatitis B titre check.ed
within the past 12 months. Incidentally, 42.7% of the respondents reported "yes" to
having their HIV status checked in the past 12 months.
50

TABLE I. COMPLIANCE RATES WITH STANDARD PRECAUTION BEHAVIOURSAMONG OPERATING ROOM NURSES IN AUSTRALIA
IStandard Precautions Behaviours c/o* 0/.
Q33 I always wear protective eyewear when scrubbed 206/224 92.0
Q34 I always double glove while scrubbed for surgical procedures 125/225 55.6
Q35 I always recap hypodermic needles after use. I861227t 81.9
Q36& I always announce sharps transfe~ when passing sharps 133/225 59.1
Q37 /l I always pass sharps using hands-free technique 161/224 71.9
Average Coq>liance for the five study behaviours 1841230 72.1(033. 34. 35. 36 and 37)
Q388 I have been vaccinated against hepatitis B 219/228 96.1
I 046 I have had my hepatitis B titre checked for immunity in the past 131/226 58.0I
12 months II
I'047 I have had my HIV status checked in the past 12 months ~ 97/227 42.7
IQ79 If! sustained a percutaneous sharps injury I would report it. 1208/227 91.6
Q86 IfI sustained a mucous membrane exposure I would report it. 198/228 86.8
teln, number of self-reported compltant respondents per number of respondents answering questIon.~Q3.5 was a negatively worded question. therefore min = non-compliant responders, which indicates compliancewith not recapping.°Q36, Q37 and Q38 are subcategories ofthe study behaviour "safe sharps handling."
4.3. Compliance Rates with Occupational Exposure Reporting
Self reported incidence of occupational exposures in the past twelve months
is relatively low with respondents reporting more percutaneous exposures than
mucocutaneous exposures. Approximately 71 % of the respondents indicated they
received no percutaneous exposures and 94% of the respondents indicated they
received no mucocutaneous exposures (see Figure 5).
51

93.90%• Percutaneous
exposures
mMucocutaneousexposures
30% 1.70% 0.40~.
. "0% 0%
25.20%
100%90%
80%70%60%
50%40%
30%20%10%0%+----,..-------,.-----,.-----,
none 1-2 3-5 7-10exposures eXOOSW'9S ...8xoosures
Number or I:xposureS' In past TW81veMonths
Figure S. Incidence of Occupational Exposures in Past Twelve Months
Most respondents (91.6%) indicated that they would report percutaneous
exposUl'Ies (3.1% were neutral) and 86.8% of respondents indicated they would report
mucocutaneous exposures (7.0% were neutral). By adding conditions to this
statement, a small number of respondents were teased out who would only report a
percutaneous exposure if the patient was considered "high risk" (7.5%) or if they
thought the exposure was "serious" (7.0%). The same scenario occurred for
mucocutaneous exposures, where 11.0% would only report if the patient was "high
risk" and 8.4% would report only if they perceived the exposure to be "serious" (see
Figures 6 and 7). Results also revealed that not all occupational exposures were
reported (see Figure 8).
52

100%90%80%70%60%50%40%30%20%10% I
0%
91.6% rJagree
Cn6ufral
Only If PatientHigh Risk
Only IfExposureSerious
Conditions of Reporting
Always
Figure 6. Attitudes toward Reporting Percutaneous Exposures
86.80%agree
l!Ineutral
8.40%
90%
80%
70%
'60%....i 50%eCII 40%Q.
30%
20%
10%
O%-t-----.-------.-------,Always Only If Only If
Patient ExposureHigh Risk Serious
Conditions of Exposure
Figure 7. Attitudes toward Reporting Mucocutaneous Exposures
53

100%
90%
80%W)
i'tJIS 70%Q.:: 60%
~ 50%o• 40%JIi 30%
~ 20%a.
10%
0% +'-----1_.....
97%
III PercutaneousExposures Reported
mMucocutaneousExposures Reported
none 1-2 exposures 3-5 exposures
Number of Occupational Exposures
Figure 1. Occupational Exposures Reported in Past Twelve Months
Analysis of occupational exposure reporting yielded contradictory results
when intention to report and actual reporting were compared among respondents in
different age groups. Although intention to report an occupational exposure was
fairly high, compliance rates with actually reporting percutaneous occupational
exposures (see Table 2) and mucocutaneous occupational exposures (see Table 3)
was lower.
TABLE 2. COMPARISON OF INTENTION TO REPORT AND ACTUALREPORTING OF PERCUTANEOUS EXPOSURES IN PAST 12 MONTHS.
AGE GROUP (IN INTENTION TO PERCUTANEOUS PERCUTANEOUSYEARS) REPORT EXPOSURES EXPOSURES
IRECEIVED REPORTED20-29 92.3% 46.2% 83%
30-39 97.1% 24.6% 94%
40-49 88.2% I 21.8% 94%I
50-59 90.6I
34% 77%Ii
60+ 50% 50% 0%
54

TABLE 3. COMPARISON OF INTENTION TO REPORT AND ACTUALREPORTING OF MUCOCUTANEOUS EXPOSURES IN PAST 12
MONTHS.AGE GROUP (IN INTENTION TO MUCOCUTANEOUS MUCOCUTANEOUS
YEARS)I
REPORT EXPOSURES EXPOSURESRECEIVED REPORTED
2()"29 84.6% 15.4% 50%I
30-39 89.9% 5.7% 25%
40-49 87.2% 6.8% 50%
50-59 83.0% 1.9% 100%
60+ 50%~
0% 0%
4.4. The Health Belief Constructs
4.4.1. Perception of Risk of Blood Borne Infection
Perception of susceptibility or risk is the degree to which a person perceives
him/herselfto be at risk of acquiring a blood-borne infection. Several questions were
included in the questionnaire to gather infonnation about respondents' perceived
risks of acquiring blood-borne infections. Approximately 52% of respondents agreed
that there was a possibility that they might contract a blood-borne infection, while
only 43% agreed that the possibility was high. The number of respondents who
agreed that their work activities put them at risk was high (80.2%), although, a
smaller percentage agreed that they came into a lot of contact with patients with
blood-borne infections (32.7%). Forty three percent of respondents agreed that the
thought of acquiring a blood-borne infection scared them, but only 10% agreed that
they were worried about contracting a blood-borne infection. There was little
difference between the percentage of respondents who agreed that if they had a
mucocutaneous exposure they would contract a blood borne infection (36%) and
55

those who agreed that if they had a percutaneous occupational exposure they would
contract a blood-borne infection (39%). Only a small percentage (4.8%) of the
respondents agreed that their physical health put them at risk (see Figure 9).
Perception of Risk of Acquiring Blood·borne Infection (BBI)
my physical health puts
me at risk ••••!E.,·-···~···~:!l······-E..::·~$·:···:·!l~·~··.. ·E.. ·~·····!i·.. ·!l:JS····:·:!:·"·:E-:·:·'S:·:·:··ai'·,.···Il~",Ew.•..!E..:;~,:
my wor1< activities putmeat risk
mucocutaneous injurywill lead to BBI
percutaneous injury will I
lead to B81 . ~
large amount of contact "r;lilii~with people with B81 '~
worry a lot about '1
getting BBI
thought of getting B81scares me _.mm.lm$J
ctIanceof getting B81 ,II=:=~:high l! <;w·
possibility that I wi,11 geta BBI
I
20 lie
agree
• neutral
mldisagree I
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Percengg8ofRespond&n~
Figure 8. Perception of Risk of Acquiring Blood-borne Infection (BBI)
4.4.2. Perception of Severity of Blood Borne Infection
Perception of severity is the degree of consequence that a person perceives
will result from acquiring a blood-borne infection, i.e., the degree to which his/her
life will be affected. Approximately 40% of the respondents agreed that a significant
relationship would be in danger, 50% agreed that their financial security would be in
danger, and nearly 69% agreed that their career would be in danger. A high
percentage of respondents agreed that a blood-borne infection was a serious illness
(97%) and 87% agreed that problems would last a long time (see Figure 10).
56

98.90%100%
90%
80%70%
60%
50%40%30%
20%
10%
0%career
would be indanger
Fmncial Serioussecurity it disease
danger
Areas Affected
Pl"obIerr6would last a
long lime
Figure 9. Perception of Severity of Acquiring A Blood-Borne Infection
4.4.3. Benefits of Compliance with Standard Precautions
Perception of benefits is the perception of the efficacy of the standard
precaution behaviour in preventing or reducing the risk of acquiring a blood-borne
infection. Most respondents agreed that specific standard precautions behaviours
were beneficial in preventing or reducing the risk of acquiring a blood-borne
infection, but to differing degrees. Most respondents agreed in the benefits of barrier
precautions, but only 78% of respondents agreed that double gloving was a benefit,
whereas, almost 98% agreed that wearing protective eye wear was beneficial.
Percentage of agreement was more similar in regards to safe sharp handling. Ninety
percent of respondents agreed in the efficacy of announcing sharps transfers, yet,
94% agreed in benefits of using a no hands transfer technique, and 92% agreed that
no recapping of hypodermic needles was beneficial (see Figure 11).
57

100%
III 90%...Iii 80%'t'E:
70%0
i 60%CD0::::
50%...0CD 40%C)
J:!I 30%c:CD
20%~CD
10%0..
0%doublegloving
decreasesrisk
wearingprotectiveeyewear
decreasesrisk
announcing hands free not recappingsharps pass decreases
decreases decreases riskrisk risk
Perceived Benefits
hep Bvaccine
decreasesrisk
Figure 10. Perception of Benefits of Staoda'rd Precautions
4.4.4. Barriers to Compliance with Standard Precautions
Perception ofharriers is what a person perceives to be interfering with hislher
undertaking or continuing the self-protective behaviour. Perception of barriers can
be internal, (e.g. causes hand tingling or poor fit) or external (e.g., limited supply or
expensive to use). Some barriers to double gloving include the following: double
gloves are a poor fit (9.0% agreed), cause hand tingling (23.1% agreed), interfere
with duties (14.3%), are in limited supply (1.3% agreed), and are too expensive
(4.0%). Some barriers to wearing protective eye wear include: protective eye wear
lIDpmrs vision (17.8%), interferes with duties (7.9%), is expensive (5.8%), is
uncomfortable (24.2%), and is not provided by the employer (3.1 %). Barriers for
r:espondents not receiving the Hepatitis B Vaccine inetude the following:
noncQnversion after unsuccessful attempts at vaccination, employer does not provide
58

the vaccine, vaccination is inconvenient, and perception that the vaccination won't
protect against injury (see Figures 12-14).
1000'"
90%l!c 80%4J~c 70%0a-lii 60%4J
ID'50%-0
CD 40%C)
S 30%i
• 20%
D.10%
0%limited supply poor fit hand tingling too expensive interleres with
duties
Barriers to Double Gloving
Figure 11. Perception of Barriers to Double Gloving
100%
90%J!i 80%~c 70%0i 60%CD
ID'50%-0
4J 40%Q
B 30%cCD
• 20%D.
10%
0%uncomfortable not provided
by employer
Barriers
interferes withmy duties
Figure 12. Barriers to Wearing Protective Eye wear
59

100%
90%
80%
70%
60%
50%
40%
30%20%1 .3
10%
0%employer jncon· positivedoes nol venient antigensJprovide non-
converter
painful afraid of offersneedles limited
protectionfrom HBV
woo'tprotectfrom
sharpsinjury
Barriers to Hepatitis B Vaccination
Figure 13. Perception of Barriers to Hepatitis B Vaccination of Respondents NotVaccinated
4.4.5. Benefits of Occupational Exposure Reporting
Perception of benefits is the perception of the efficacy of the self-protective
behaviour (i.e. occupational exposure reporting) in preventing or reducing the risk of
acquiring a blood-borne infection. A majority of respondents agreed in the
perception of benefits to reporting. Almost 90% agreed that reporting benefits them
and their family. Approximately 85% agreed that reporting would be beneficial in
early discovery of disease transmission. There was less agreement on whether
reporting prevented future problems (72.7%). Only 23% agreed that reporting was
beneficial in reducing their anxiety about acquiring a blood-borne infection (see
Figure 15).
60

Benefits of Occupational Exposure Reporting
100% WI.
~ 90%i'0 80%g 70%,
:- 60%~'0 50%CII 40%
E 30%
~ 20%
:. 10%0%
reporting benefits me helps dis<:over decreases myand my family disease I1ansmissionanxiety about Hep b
eany and c
Benefits of Reporting
• agree
• neutral
IiJdisagree
prevents futureproblems
Figure 14. Benefits of Occupational Exposure Reporting
4.4.6. Barriers to Compliance with Occupational Exposure Reporting
Perception of barriers is what a person perceives to be interfering with hislher
undertaking or continuing the self-protective behaviour. The barrier to reporting
agreed upon by most of the respondents (71.9%) was that reporting was time
conswning. Almost 40% of respondents agreed that reporting was unpleasant and
just under 25% of respondents agreed that reporting interfered with duties (see
Figure 16).
61

100%
J1 90%c
80%G)"tJc 70%0
a- 60%G)
0::50%-0
G) 40%Q.1'! 30%cB 20%...G)D. 10%
0%01
CJI .ljj
~~i~... ~
OlC Q) ... l::: oS !'§.E Cl ~-;i~lJl "".£ Ol·~ :8~ C7lE (11.>0:- .c <Il "" - Q)
.e-<II~ ~Q);:J ~gg.a. ,si ,!lEi i~~... c ~ §;:J 5i:2': -~~
... _ E~fd... i- .E[ .- n! Q)
~..a
Barriers to Reporting
Figure 15. Barriers to Occupational Exposure Reporting
4.5. Demographics and Compliance with Standard Precautions
Contingency tables and chi square analysis was conducted to detennine
whether there was an association between demographic variables and compliance
with standard precautions (see Appendix 9). There was no significant relationship
found between nursing status, nurse training, or type of facility and compliance with
any standard precautions. However, significant relationsbips were present in other
demographic categories for specific standard precautions behaviours.
62

Age and compliance with standard precautions was first analysed by recoding
the respondents into age groUpS.lO Nurses 50-59 years old were significantly less
compliant with wearing protective eyewear (11 = 35.77, df = 8, p < .05) and
announcing sharps transfers ('l = 15.842, df= 8, P < .05). Compliance rates of nurses
aged 30-39 and those aged 40-49 were significantly lower for not recapping needles
than nurses in other age groups ('l = 18.802, df= 8, p < .05) although more nurses
aged 20-29 were neutral on the subject of not recapping than any other age group
(12 = 15.842, df= 8, P < .05). Compliance rates for always reporting a percutaneous
injury were significantly lower for nurscs aged 40-49 ('l= 20.875, df= 8, P < .05).
The analysis was then recomputed using analysis of variance with age means
(see Table 4) in order to tease out possible masked significance. Non compliant
responders tended to be older than compliant responders for all standard precaution
behaviours except for not recapping needles. This is consistent with the contingency
table analysis for this variable.
A significant relationship was present between double gloving and several
demographic variables. Compliance rates were significantly higher for nurses with
less than two years of scrub experience ('l = 16.415, df = 3, p < .05). Compliance
rates for double gloving when scrubbed were significantly lower for nurses working
in small facilities ('l = 15.761, df = 6, p < .05) with few operating theatres
(12 = 14.025, df= 6, P < .05). Differences in compliance rates across states is also
significant ('l = 57.69, df = 10, P < .05) with great variation reported between states
(see Table 5).
10 Since only two respondents were 60 years old or older, analysis for this age group would be limitedin interpretations of representativeness. Therefore, analytieal data from tbis age group will not beundertaken in tbis section.
63

Table 4. Mean Age in Compliant and Non Compliant Responders
Standard Precaution Behaviour Mean Age± P dfS.D.~
Q33 I always wear protective eyewear when scrubbedCompliant 42.31 ± 8.24 .155 2Non Compliant 47.50 ± 8.49
Q34 I always double glove while scrubbed for surgicalproceduresCompliant 41.8 ± 8.64 .048- 2Non compliant 44.8 ± 8.23
Q35 I always recap hypodermic needles after use.tCompliant with not recapping 43.0 ± 6.82 .836 2Non compliant with not recapping 42.78 ± 8.54
Q36 I always announce sharps transfers when passing sharpsCompliant 41.95 ± 8.03 .162 2Non compliant 44.63 ± 8.78
Q37 I always pass sharps using a "hands-free" techniqueCompliant 42.37 ± 8.56 .018- INon compliant 43.62 ± 8.66
Q38 I have been vaccinated against hepatitis BCompliant 42.5 ± 8,43 .046· 1Non Compliant 48.22 ± 7.41
Q79 If I sustained a percutaneous injury I would report itCompliant 42,42 ± 8.47 .604 2Non compliant 43.08 ± 6.83
Q86 If I sustained a mucous membrane exposure I would report itCompliant 42.53 ± 8.29 .024· 2Non compliant 44.71 ± 7.31
tS.D., standard deviation.tQ35 was a negatively worded question, therefore min = non-compliant responders, which indicates
compliance with not recapping.·P<.05.
64

Table s. State of employment and compliance with always double gloving whenscrubbed.
Percent of respondents from state
State compliant neutral noncompliantII
NSW/ACf 81.8% 6.5% 11.7%
NTIWA 42.9% 21.4% 35.7%
SA 30.8% 7.7% 61.5% I
TAS 37.5% 50.0% I 12.5%I
I
VIC:1
30.4% 20.3% 49.3%
QLD I 65.1% 7.0% 27.9%
Totalofan 55.8% 13.4% 30.8%respondents
-
A significant relationship was present between announcing sharp transfers
and certain demographic variables. Compliance rates for announcing sharps
transfers was significantly lower for males ('l = 6.641. df= 1, P < .05). Compliance
rates were also lower for nurses working in large facilities (t = 12.544, df = 6,
p < .05). Nurses employed in South Australia and Tasmania reported significantly
lower compliance rates than nurses working in other states (:l = 24.178, df = 10,
p < .05). But, compliance rates were significantly higher for nurses with only two to
five years post registration experience (Xl = 16.415. df= 6, p < .05).
A significant relationship was present between wearing protective eyewear
and state of employment (t= 40.47, df= 10, P < .05). The compliance rate (69.2%)
for nurses employed in South Australia was significantly lower than compliance rates
65

for nurses in other states. In addition, 30.8% of the South Australian nurses were
neutral on the subject.
4.6. Demograpbics and Compliance with Occupational Exposure Reporting
Contingency tables and chi square analysis were conducted to determine
whether there was an association between demographic variables and compliance
with occupational exposure reporting (see Appendix 10). There was no significant
relationship for occupational exposure reporting and gender, nurse status, education,
years of post registration experience, years of scrub nurse experience or state of
employment. However, eompliance with mucocutaneous exposure reporting was
significantly lower for nurses working in smaller (l= 13.153, df= 6, p < .05), private
faeilities (l = 10.021, df = 6, P < .05. and few operating theatres (11 = 14.700, df = 4,
P < .05). Compliance was also significantly lower for nurses 20-29 years old
(l= 122.118,df= 16,p<.05).
4.7. Compliance with Standard Precautions and the Health Belief Constructs
The dependent variables were compliance with standard precautions (double
gloving, wearing protective eyewear, safe sharps handling, and hepatitis b
vaeeination). The independent variables were the health belief constructs (perceived
risk of infection, perceived severity of the eonsequences of infeetion, perceived
benefits of compliance with standard precautions, and perceived barriers to
eompliance with standard precautions). Univariate correlation analysis, using
Kendall's tau b, was applied Lo describe any association between eompliance with
standard precautions and each single independent variable. Degree of association
was indicated by the size of the correlation coefficient. The correlation coefficient
indicates both thc strength and direction of relationship betwccn two variables. The
66

strength is indicated by the value of the coefficient and the direction is indicated by
the sign (+ or -) of the coefficient. The closer the correlation coefficient is to 1 the
stronger is the relationship between the two variables. With this in mind we can
grade the degree of correlation and association by knowing the correlation coefficient
(see Table 6). This rough guide will be used to label relationships between the health
belief constructs and compliance with standard precautions.
Table 6. Rough Guide to Degree of Association II
Range of Correlation Assotiation
Correlation Coefficient
0.90-1.00 Very High Correlation Very Strong Association
0.70-0.90 High Correlation Marked Association
0.40-0.70 Moderate Correlation Sllb~lantjal A~sociation
0.20-0.40 Low Correlation Wealc: Association
Less than 0.20 Slight Correlation Association se small as Ie bene~[igible
Reliability testing using Cronbach's alpha coeffieient was utilised to test and
develop reliable scales for each construct of the Health Belief Model. Scales with a
Cronbach's alpha coefficient less than 0.70 were not included in the analysis, unless
otherwise indicated. Only significant results will be discussed in the following
seetions.
II Table adapted from BLlms (2000), IntrooLlcllon to Research Methods (41h edition), Longman: Frenchs Forest.NSW, p.235.
67

4.7.1. Compliance with Standard Precautions and Perception of Risk
Double Gloving.
There is only a slight correlation between perception of risk if a percutaneous
exposure occurs and double gloving when scrubbed, the relationship is negligible
(r= .132, df = 2, p< . 05). Respondents who pereeived they were al risk of
contracting a blood-borne infection from a percutaneous exposure were more likely
to double glove.
4.7.2. Compliance witb Standard Precautions and Perception of Severity
No correlation was found between perception of severity of consequences of
acquiring a blood-borne infection and any of the standard precaution behaviours.
4.7.3. Compliance witb Standard Precautions and Perception of Benefits
Although questionnaire statements assessmg perception of benefits of
compliance with standard precautions (scc Appendix 7) were found to have limited
reliability (Cronbach's alpha < .70), univariate correlations analysis was pcrformed
to identify any eorrclations or relationships belween compliance with standard
preeautions and perception of benefits.
Double Gloving.
There is a moderate correlation between perception of double gloving as a
benefit (beeause it decreases the risk of acquiring a blood-borne infection) and
double gloving when scrubbed (r= - A03, df=2, p< .05). This indicates a substantial
relationship belween these variables. Of the 78% of respondents who agreed with
this statement, 62% of them always double gloved when scrubbed.
68

Protective Eyewear.
There is only a slight correlation between perception of the benefit of wearing
protective eyewear (beeause it decreases the risk of acquiring a blood-borne
infection) and wearing protective eyewear (r= -.163, df=2, p< .05). This indicates a
negligible relationship between the variables. Of the 98% of respondents, who
agreed that wearing appropriate eye protection decreases their risk of getting
hepatitis B or C, 86% of them always wear appropriate eye protection.
Sale Sharps Handling.
There is a low correlation between the perception of safe sharps handling as a
benefit to decreasing risk of acquiring blood-borne infection with announcing sharps
transfers (r= .374, df=2, p< .05), using a hands-free sharps pass technique
(r= .323, df=2, p< .05) and not reeapping needles (r= - .292, df=2, p< .05). This
indieates a weak relationship between these standard precautions behaviours and the
perception of their benefit. Of the large percentage (average 98%) of respondents
who agreed that safe sharps handling decreased the risk of aequiring a blood-borne
infection, there was much less reported compliance with announcing sharps transfers
(66%), using a hands-free sharp pass technique (75%) or not recapping needles
(69%).
4.7.4. Compliance with Standard Precautions and Perception of Barriers
Double Gloving.
There are several moderate correlations between pereeption of such barriers
to double gloving as interfering with duties (r= - .483, df = 2, p< .05) and causing
hand tingling and numbness (r= - .513, df= 2, p< .050), which indicated a substantial
relationship between these variables. Of the 14% of respondents, who agreed that
69

double gloving interferes with their duties, 6% of them always double glove when
scrubbed. Of the 23% of respondents who agreed that double gloving causes hand
tingling or numbness, 8% of them always double glove when scrubbed.
There are several low correlations, between perception of such barriers to
double gloving as being 100 expensive (r= - .244, df=2, p< .05) and being a poor fit
(r= -.343, df=2, p< .05). These low correlations indicate a weak. relationship
between the variables. Only 4% of respondents agreed that double gloving is
expensive, yet 33% of them always double glove when scrubbed. Of the 9% of
respondents who agreed that double gloves are a poor fil, 15% of them always
double glove when scrubbed.
There is only a sligh I correlation between perception that gloves are in
limited supply as a barrier to double gloving (r= ~.156, df=2, p<.05), the relationship
is negligible. Of the 1% of respondents who agreed that double gloves were in
limited supply, 33% of them always double gloved.
Protective Eyewear.
There is one moderate correlation between wearing proteetive eyewear and
pereeption of the barrier that wearing protective eyewear interferes with duties
(r= -.431, df=2, p< .05). This indieates a substantial relationship between the
variables. Of the 8% of respondents, who agreed that wearing appropriate eye
proteetion interferes with their duties, 50% of them always wear appropriate eye
protection.
There is a low eorrelation between wearing proteetive eyewear and barriers to
wearing protective eyewear, such as eyewear being uneomfortable (r= -.246, df=2,
p<.OS), and impairing vision (r= -.357, df=2, p<.05). This indieates a weak.
relationship between the variables. Of the 24% of respondents who agreed that
70

wearing appropriate eye proteetion is uncomfortable, 73% of them always wear
appropriate eye protection. Of the 18% of respondents who agreed that wearing
appropriate eye protection impairs their vision, 63% of them always wear appropriate
eye proteetion.
There is only a slight correlation between wcaring protective eyewear and
barriers to wearing protective eyewear, such as being expensive (r= ·.187, df=2,
p< .05). This indieates a negligible relationship between the variablcs. Of the 6% of
respondents, who agreed that wearing appropriate eye protection is expcnsive, 77%
of them always wear appropriate eye protection.
4.8. Occupationa) Exposure Reporting and Health Belief Constructs
The dependent variable was compliance with occupational exposure
reporting. The independent variables were the health belief constructs (perceived
risk of infection, perceived severity of the consequences of infection, perceived
benefits of compliance with standard precautions, and perceived barriers to
compliance with standard precautions). Univariate correlation analysis, using
Kendall's tau b, was applied to describe any association between compliance with
occupational exposure reporting and each single independent variable. As in the
previous section, degree of association was indicated by the size of the cocfficient
(Refer back to Table 6, pg. 57).
4.8.1. Occnpational Exposure Reporting and Perception of Risk
No correlation was found between perception of risk of consequences of
acquiring a blood-borne infection and compliance with occupational exposure
reporting.
71

4.8.2. Occupational Exposure Reponing and Perception of Severity
There is only a slight eorrelation between reporting oeeupational exposures
and the pereeption of severity of an endangered eareer as a result of the exposure
(r=.153, df=2, p< .05). This indieates a negligible relationship between the variables.
Of the 58% of respondents, who agreed that if they get hepatitis B or C, their eareer
would be endangered, 93% of them would report a percutaneous exposure and 92%
of them would report a mueocutaneous exposure.
4.8.3. Occupational Exposure Reporting and Perception of Benefits
Although questionnaire statements assessmg benefits of oecupational
exposure reporting (see Appendix 7) were found to have limited reliability
(Cronbach's alpha < .70), univariate correlations analysis was performed to compare
occupational exposure reporting with perception of these benefits.
Mucocutaneous Occupational Exposures (MOExp).
No correlation was found between reporting a MOExp and pereeption of
benefits of reporting a MOExp.
Percutaneous Occupational Exposures (POExp).
There was a low correlation between reporting POExp and perceptions that
reporting benefited the respondent and the respondent's family (r=.202, df=2,
p< .05). This indicates a weak relationship between these two variables. Of the 89%
of respondents who agreed that reporting benefits them and their family, 94% of
them would report pereutaneous exposures. There was only a slight correlation
between reporting POExp and perceptions that reporting was of benefit because it
allowed the discovery of disease transmission sooner than later (r=.180, df=2,
p< .OS). This indicates a negligible relationship between the variables. Of the 90% of
72

respondents who agreed that reporting and follow up may discover disease
transmission sooner than later, 93% of them would report percutaneous exposures.
4.8.4. Occupational Exposure Reportinl! and Perception of Barriers
Mucocutaneous Occupational Exposures (MOExp).
There was a moderate correlation between reporting MOExp and perception
of barriers to reporting, such as being time consuming (r= .463, df=2. p< .05),
inconvenient (r= .479, df=2, p< .05) and requiring too much paperwork (r= .450,
df=2, p< .05). This indicates a substantial relationship between the variables. Of the
72% of respondents who agreed that reporting occupational exposures is time
consuming, 87% would report a mucocutaneous exposure.
There was a low correlation between reporting MOExp and perception of the
barrier that reporting was embarrassing (r= .259, df=2, p< .05). This indicates a weak
relationship between the variables. Of the 14% of respondents who agreed that
reporting oceupational exposures is embarrassing, 81% would report a
mucocutaneous exposure.
Percutaneous Occupational Exposures (POExp).
There was a moderate correlation between reporting POExp and perception
of barriers to reporting, such as being time consuming (r= .464, df=2, p< .05),
inconvenient (r= .467, df=2, p< .05) and requiring too much paperwork (r= .410,
df=2, p< .05). This indicates a substantial relationship between the variables. Of the
72% of respondents who agreed that reporting occupational exposures is time
consuming, 92% would report a percutaneous.
There was a low correlation between reporting POExp and perception of the
barrier that reporting was embarrassing (r= .388, df=2, p< .05). This indicates a weak

relationship between the variables. Of the 14% of respondents who agreed that
reporting occupational exposures is embarrassing, 87% would report a pereutaneous
occupational exposure.
4.9. Summary and Conclusion
The results of this study revealed a less than 100% eompliance with standard
preeautions, with a mean compliance rate for the five study behaviours (double
gloving, adequate eye protection, announeing sharps transfers, hands-free sharp
passage technique and no needle recapping) of 72.1 %. The lowest compliance rate
was with double gloving (55.6%) and the highest with adequate eye protection
(89.6%). Certain demographie characteristics demonstrated significance with speeifie
standard preeaution behaviours and occupational exposure reporting. These included
age, years of experienee, size of facility and state of employment. The results of this
study also revealed underreporting of occupational exposures by a range of 8% to
58% for percutaneous and mucocutaneous exposures, respeetively.
In analysis of variables using the HBM, signifieant eorrelations were found to
exist between pereeptions of risk, severity, benefits and barriers with complianee of
both standard precautions and occupational exposure reporting. These eorrelations
varied depending on the specific standard preeaution examined and the specific
question asked. One of the unique findings of this study is that perception ofbarriers
demonstrated the most substantial relationship with compliance for double gloving,
wearing protective cyewear and reporting occupational exposures.
Chapter 5 will diseuss the results of this study in comparison with previously
reported results.
74

Chapter S. Discussion
S.l Introduction
To better assess the level of compliance with standard preeautions and
occupational exposure reporting among operating room nurses in Australia, the
results of this study must be viewed in context with other published results in order
to first determine where on the continuum the compliance rates of operating room
nurses in Australia lie. The results presented in Chapter 4 support the findings of
previous studies in reporting a less than 100% compliance rate with standard
precautions and an underreporting of occupational exposures among operating room
nurses in Australia. An assumption can be made at this time that conditions and risks
faced by Australian operating theatre nurses are similar to those faced in other
countries. Chapter 5 will discuss comparisons between the findings of this study and
the findings of previous studies. First, each standard precaution behaviour will be
discussed individually. Next the results of occupational exposure reporting from this
study will be compared with those of previous findings. Finally, this chapter will
discuss the appropriateness of using the constructs of the HBM to define the
variables that have influence on complianee and a comparison of previous studies
reporting specifically on perception of barriers to compliance.
S.l. Compliance Rates
Double gloving. This study revealed a mean complianee rate of 55.6%
among operating room nurses for double gloving during surgical procedures. This
compliance rate is considerably higher than that previously reported. Akduman,
Kim, Parks et al (1999) reported that 28% of surgical team members double gloved,
75

and that the use of double gloves was higher for surgeons and registrars (43%) than
for medical students (26%) and scrub nurses (15%). This study found an increase in
the use ofdouble gloves by operating room nurses.
Adequate eye proteetion. This study revealed a mean compliance rate of
92% among operating room nurses for wearing adequate eye protection during
surgical procedures. Akduman, Kim, Parks et al (1999) observed that 41% of
surgical team members wore goggles or face shields, 32% wore regular glasses, and
24% used no eye protection. Scrub nurses and medical students were more likely to
wear goggles (60% of the time) than other healtheare workers (Akduman, Kim,
Parks et ai, 1999). This study found an increase in the reported use of adequate eye
protection among operating room nurses in Australia.
Hands-free sharps passage. This study revealed a mean compliance rate of
71.9% among operating room nurses for using a hands-free sharps passage technique
during surgical proeedures. There is not much data in the literature to detennine if
there has been an increase in compliance with this behaviour.
Announcing sharps transfers. This study revealed a mean compliance rate
of 59.1 % among operating room nurses for announcing sharps transfers during a
surgical procedure. Akduman, Kim, Parks et al (1999) found that sharp transfers
were not announced in 91% of surgical procedures. There is limited literature
available on complianee rates of announcing sharps transfers specifically among
operating room nurses and thus, no basis for comparison.
Not recapping needles. This study revealed a mean 81.9% compliance rate
among operating room nurses for not recapping needles. Henry, Campbell, and Maki
(1992) observed registered nurses to recap more frequently (61.5%, n=200) than
physicians (45.3%, n=75). Complianee rate among operating room nurses in
76

Australia is higher than that previously reported among nurses in other high-risk
areas.
Hepatitis B vaccination. Although hepatitis B vaccination was not one of
the standard precautions behaviours that were the focus of this study, compliance
rates will be mentioned here. This study revealed a mean eompliance rate of 96.1 %
among operating room nurses for hepatitis B vaceination. In a U.S. national survey
(n=3094 workers in hospitals), Hersey and Martin (1994) found that only 56% of
physicians and 55% of healthcare staff (ineluding nurses) reported receiving at least
one of the injections recommended in the hepatitis B vaccination series although it
was offered in most cases. Currently, hepatitis B vaccination is the one standard
preeaution behaviour that is most frequently mandated by infection control
guidelines and facility policies. This may indicate that mandated policies yield
higher compliance rates.
OccupatiODsl Exposure Reporting. Although this study revealed high mean
compliance rates with intention to report percutaneous exposures (91.6%) and
mucocutaneous exposures (86.8%), the mean compliance rates on the SPOER self
report survey for actual reporting of percutaneous and mueocutaneous exposures was
considerably lower (22.20% and 1.70%, respectively, for those incurring 1-2
exposures in the past 12 months, and 0.9% and 1.3%, respeetively, for those
incurring 3-5 exposures in the past 12 months). This low rate of aetual reporting is
eause for concern. Without accurate data on the ineidence of occupational
exposures, the incidence of exposures may be inaeeurately considered low and thus
not treated as a priority in the development of strategic infection eontrol plans. It
must also be reiterated here that previous research eomparing self-report data and
77

observed data questioned the true reliability of self-report surveys, and demonstratcd
that sclfreported data may be an underestimatc of actual reporting in practicc.
5.3. The Health Belief Model
The ideas for the development of the Health Belief Model (HBM) came about
In the 1950s and 60s in an attempt to predict when people would undertake
protective health behaviours to decrease risk or prevent illness or disease stales.
After a thorough critique of the HBM, Davidhizar (1983) concluded that although the
HBM did offer an approach to understanding health behaviour, the model needed
development and testing. Champion (1984) developed an instrument to measure the
constructs of the HBM with valid and reliable scales. Internal reliability for
perception of risk, perception of severity and pereeption of barriers (Cronbach alphas
0.77, 0.78 and 0.76, respeetively) was greater than that for perception of benefits
(Cronbach alpha 0.61). When tested for construct validity, pereeption of barriers
accounted for the greatest variance and those people who saw fewer barriers were
more likely to report undertaking of the health behaviour studied. Champion's
instrument was adapted for use in this study.
Similar results to those obtained by Champion (1984) were found when
scales of the SPOER were tested for internal reliability. The internal reliability for
the scales of perception of risk and severity (Cronbach alpha 0.71 and 0.70,
respectively) was high. Internal reliability for behaviour-specific barrier scales for
double gloving, adequate eye protection, and hepatitis B vaccination were also high
(Cronbach alpha 0.78, 0.76, 0.93). Internal reliability for behavior-specific barrier
scales for reporting percutaneous exposures and reporting mucocutaneous exposures
were also high (Cronbaeh alpha 0.87 and 0.86, respeetively). Internal reliability for
the perception of benefit to standard precautions and benefit to occupational
78

exposure reporting were lower (Cronbach alpha 0.51 and 0.34, respectively). This
latter finding is consistent with the internal reliabili ty of the benefit scale reported by
Champion (1984). Scales for measuring perception of benefits wi II have to be
further refined and tested to yield more confident reliability in measuring this
construct of the HBM.
This study partially supports the findings of earlier studies that demonstrated
that constructs of the HBM are appropriate to identify attitudes of nurses regarding
standard precautions and occupational exposures (Champion, 1984; Grady,
Shortridge, Davis and Klinger, 1993). Although this study revealed substantial
relationships between compliance with standard precautions and perception of
barriers to these behaviours, as welt as between compliance with occupational
exposure reporting and perception of barriers to these behaviours (i.e. there was
higher compliance where perception of barriers was low), there were only weak or
negligible relationships between compliance with standard precautions or
occupational exposure reporting and perception of risks. severity and most benefits.
Barriers to compliance with standard precautions and occupational exposure
reporting are noted extensively in the literature. Some of these include lack of time
(71-74%), patient low risk (50-57%), personal protective equipment (PPE)
interfering with care (55%), and PPE equipment not available (19.3-41 %) (Henry,
Campbell and Maki, 1992; Williams, Campbell, Henry and Collier. 1994: Nelsing,
Nielsen and Nielsen, 1997). Williams, Campbell, Henry and Collier (1994)
concluded that a eorrelation exists between perceived barriers and compliance. This
study analysed barriers previously cited in the literature as reasons for non
complianee. For double gloving, the most significant barriers revealed in this study
were interference with duties, hand numbness and tingling. For wearing protective
79

eyewear, the most significant barrier in this study was interferenee with duties. For
occupational exposure reporting, the mosl signifieant barricrs in this study were
inconvenience, time consuming and too much paperwork (for reporting either
mucocutaneous or percutaneous exposures). The importance of this study is its
further support of previous studies in finding barriers to slandard prccautions as a
significant influcnce on compliance to standard precautions. Unique to this study is
the conclusion that barriers to occupational exposure reporting arc a significant
influence on compliance with reporting occupational exposurcs among operating
room nurses.
S.4. Summary and Contlusion
Studies in the past have utilised varying methodologies in analysing data on
compliance with standard precautions and occupational exposure. Consequently,
sludies have not agreed on actual compliancc rates. In addition, compliancc rates
have varied over the years. One fact that pCJVades throughout all previous studics,
and is supported by this study, is the facl thai compliance rates with guidelines
developed to protect the health care worker are less than 100%. This study has
dcmonstratcd that compliancc rates with standard precautions and occupational
exposure reponing among operating room nurses in Australia are less than 100%.
Although the assumption has been madc that conditions and risks faced by
Australian operating room nurscs is similar to those in other countries, further
rescarch may revcal that differcnces between countries' hcalthcare systems. disease
prcvalence and technologies may impact on the general level of compliance with
standard prccautions and occupational exposure rcponing within individual
countrics. This study also supports previous rescarch findings that perception of
barriers to standard precaulions is a significant influcnce on compliance with
80

standard precautions. An additional finding of this study is that perception of
barriers demonstrated the most substantial association with compliance with
occupational exposure reporting.
81

Cbapter 6. Recommendations
6.1. Introduction
It is clear from the data analysis and discussion that measures must be
implemented to not only increase operating room nurses' eompliance with standard
precautions, but also to increase occupational exposure reporting among this high
risk nursing group. Thcse measures fall under three main subheadings: prevention,
education and policy.
6.2. Prevention
The most logical way to prevent occupational transmission of blood borne
infections in the operating room is by prevention of occupational exposure in the first
instance. Standard precautions are guidelines developed to protect the healtheare
worker from occupational exposure. Two major components of standard precautions
are the use ofprotective barriers and safe sharps handling.
Results of this study demonstrate that perception of barriers to the use of
protective barriers, such as double gloving and adequate eye protection, had a
significant influence on compliance with these standard precautions. Statistically
significant barriers to double gloving included interference with duties, hand tingling
or numbness, and, to a lesser extent, expense, poor fit and limited supply. This study
found that compliance rates wcre significantly lower for double gloving for nurses
working in small facilities with fewer operating rooms. Further investigation may
find that cost and supply could be a major factor for smaller faeilities with
understandably smaller budgets in the provision of a wide enough range of glove
sizes as well an adequate supply available for double gloving.
82

Statistically signi fleant barriers to wearing adequate proteetive eyewear
included interferenee with duties. comfort, and expense. This study found that
nurses aged 50-59 were less likely to wear adequate protective eyewear. Further
analysis also found that 70.6-75.5% of 40-59 year olds disagreed that preseription
eyewear was adequate protection in eomparison to olds 82.4-92.3% of 20-39 year
olds who disagreed with this statement. Dependence on prescription glasses
inereases in direet proportion to the status of aging and perhaps further investigation
may find some links between age and habitual behaviour in regards to prescription
glasses wearing.
It has already been demonstrated in the literature that double gloving and
wearing adequate eye proteetion significantly decrease the ineidenee of oceupational
exposure. It would be in the best interest of the employer to enaet measures to
eliminate or at least attempt to decrease barriers to the use of personal protective
equipment. Employers must make personal proteetive equipment available and
aceessible to all employees. A cost benefit analysis of double gloving vs treatment of
oeeupational exposures can justify the use of two pairs of gloves by serub staff.
Adequate eye protection, in the form of face shields, masks with faee shields and/or
goggles with side shields must be made available to operating room staff. Staff
members who wear prescription glasses must be provided with side shield
attachments or goggles with side shields that fit comfortably over their glasses or
goggles that incorporate their prescription. The costs of these modifications to
prescription glasses may be covered by the hospital or through private insurance. If
these modifieations are required in the workplaee, the cost may also be recoverable
through personal ineome tax deductions. This is an area that needs to be investigated
and eosted further and available options offered to employees.
83

Safe sharps handling has also been demonstrated in the literature to
significantly decrease the risk of occupational exposure in the operating room. This
study reported mean eompliance rates of 59.1 % with announcing sharps transfers,
71.0% of using a hands-free sharps pass technique and 81.9% with not recapping
needles. Employers must provide point of use needle disposal units and encourage
the practices of announcing sharps transfers, using a hands-free technique for passing
sharps and not recapping needles during surgical procedures.
The significance of the hepatitis B vaccination In decreasing disease
transmission after occupational exposure has also been previously reported in the
literature (NHMRC, 1996). A hepatitis B vaccination program must be available for
all staff and employees' immune status must be diligently monitored.
Statistically significant barriers to reporting occupational exposures included
time constraints, inconvenience, too much paperwork, and embarrassment.
Occupational exposure reporting mechanisms should be user-friendly.
"Inconvenience", "'too time consuming" and "too much paperwork" were the most
significant barriers to occupational exposure reporting in this study. Occupational
exposure reporting impinges on the operating room nurses' time as well as the other
team members' time. During working hours. staff members may have to report to an
occupational medicine unit. which mayor may not be located within the theatre
complex. After hours, staff may be required to report to the emergency department if
the occupational medicine service is not available as an on-call service. Anecdotal
evidenee from area health care facilities uncovered reports of staff members waitjng
up to two hours for treatment and follow up after an occupational exposure. This
lack of access to prompt post exposure management has been previously reported in
the literature (Mangione, Geberding and Cummings, 1991; Williams, Campbell,
84

Henry and Collier, 1994). One measure to streamline this process is to allow staff
members' priority proeessing in the emergeney department after hours. This, of
eourse, would depend on the eondition of other patients waiting for emergency room
admission.
Another measure that may streamline the reporting proeess for operating
room nurses, as well as other team members is to establish a liaison infection control
nurse program in the operating rooms. Several operating room nurses eould be
trained in infection eontrol. oeeupational exposures and eounseling, reporting
proeedures and speeimen eolleelion and proeessing. These liaison nurses would be
available on eaeh shift, within the theatre eomplex, to assist and support staff
members with post exposure management. This would save time ehanging in and
out of operating room attire, time in leaving the unit to go to the oeeupational
medieine unit, time waiting in the emergency department and lost time while the
theatre eloses. It may also alleviate anxiety of the injured staff member during the
time waiting for possible treatment or counseling. It may be easier and more cost
effieient to relieve the injured nurse and the liaison nurse from theatre duties for 15
20 minutes than to delay a theatre for an hour or more.
Operating room nurses must be proaetive in their approaeh to oceupational
exposures. Maintaining a eurrent knowledge base about disease transmission and
treatment is paramount. Proaetive measures must take on a community approaeh.
Each nurse must be aware of their own behaviour as well as that of other team
members. The organisation also has a major role in being proactive in their approaeh
to oeeupational exposures. Adequate barrier preeautions, in the form of personal
proteetive equipment, must be provided for all employees who may eome in eontaet
with potentially infectious materials. Personal proteetive equipment must be readily
BS

available and located in convenient areas for use by staff. Policies must also be put
in place that mandate the usc of standard precautions, including hepatitis B
vaccination. There must also be policies in place that ensure that employees are
monitoring their blood borne infection status regularly. Routine monitoring of
employee status is not only beneficial for statTmembers but also for the protection of
the patients.
6.3. Education
Another component of a successful infection control program is education.
The program must incorporate initial, as well as on-going training and education.
When developing the education component, the core principles of adult learning
must be utilised in order to ensure learning takes place (see Table 7).
Table taken ITom Knowles. M S (l998). The Adult Leamer (5 edition), Gulf Pubhshing Company:Houslon, p4
Table 7. PRINCIPLES OF ADULT LEARNING
1. Learners Need to Know - Why- What- How
2. Self-Concept of the Leamer - Autonomous- Self-directing
3. Prior Experience of the Learner - Resource- Mental models
4. Readiness to Learn - Life related- Developmental task
5. Orientation to Learning - Problem centered- Contextual
6. Motivation to Learn - Intrinsic value- Personal payoff
-m ..
In addition to Knowles (1998) core principles of adult learning, demographics
of the group must also be taken into consideration so that the program addresses the
needs of all learners. Motivation and readiness to learn varies according to life span
86

development (Knowles, 1998). This study found that the mean age for non
compliance was higher than the mean age for eomplianee with standard precautions
(Table 4, p. 59). An edueation program must take into account the age of the
participants and incorporate concepts that appeal to all age groups.
The education program must tailor the material to focus on the constructs of
the Health Belief Model, espeeially perception of barriers to compliance, to present
material in a way that will reach all participants, no matter which construct they
identify with most. This study found that perception of barriers was a signifieantly
influential factor in complianee, especially for double gloving, wearing adequate
protective eyewear and reporting oecupational exposures. For these staff, the
perception of barriers must be dispelled. They must be made aware of the
availability and loeation of personal protective equipment and how to obtain more if
the stock supply is depleted. They must be made aware of the protocols for reporting
occupational exposure and how to minimise and/or avoid the barriers. Some
strategies to eliminating barriers to reporting may include maintaining a stock of the
required paperwork in the theatre eomplex, arranging for the oeeupational medicine
staff to come to the operating theatre when an oceupational exposure occurs or by
establishing an operating theatre infeetion control liaison to handle incidents in the
theatre complex. Even with all of these strategies in place, staff must be aware of the
existence of these strategies to comply with standard precautions and occupational
exposure reporting.
Although, the other constructs of the health belief model (i.e. perception of
risk, perception of severity and perception of benefits), were not found to be
significant factors (exeept perception of benefits and double gloving), they were,
nonetheless, noted as reasons for non-eompliance. This study found that just over
87

80% of respondents felt their work activitics put them at risk for acquiring a blood
borne infection. Educational programs, for those staff members, must present
information on risk of occupational exposure for compliance and non-compliance as
well as information on disease transmission rates.
This study also found that almost 97% of respondents agreed that HBV and
HeV are serious diseases and approximately 86% agreed that problems encountered
from acquiring one of theses disease would last a long time. Tn addition to other
infOImation, education programs, for these staff members, must provide information
on the debilitating after affects of acquiring a blood borne infection, ineluding its
affcct on career, significant relationships and financial situation.
This study found that 77-97% of respondents agreed that compliance with
standard precautions was beneficial in decreasing their risk of aequiring blood borne
infeetions. Education programs, for these staff must present information on the
effieaey of compliance with standard precautions and occupational exposure In
preventing occupational exposure and decreasing risk of disease transmission.
In order to capturc all staff, regardless of which health belief construet is
most influential for them individually, the edueation program must incorporate
aspects focusing on each of the constructs. By using the principles of adult learning,
the education program foeuses on what each staff member needs to know and can be
adjusted according 10 staff members' readiness to learn, orientation to learning and
motivation to learn.
6.4. Policy
Another component of an effective infection control program is the
development and enforcement of polieies mandating the use of standard precautions
and occupational exposure reporting. Risk of exposurcs can be decreased by
88

implementing stringent policies on mandatory compliance with such measures as
hepatitis B vaccination, wearing adequate protective eye and face wear, handling
sharps in a safe and responsible manner. Mandated, enforceable policies may yield
higher compliance rates. Most healthcare facilities in Australia follow the
recommendations of the NHMRC guidelines on providing hepatitis B vaccination to
employees, and offer the scrics of vaccination to all new employees or require proof
of immunisation. The Royal Australasian College of Surgeons' policy on infection
eontrol also advocates this recommendation. The high mean compliance rate of
hepatitis B vaccination (96.1 %) found in this study may reflect the influence of
mandatory vaccination or proof of immunity_ The difference in levels of complianee
between states found in this study, specifically with double gloving, is noteworthy.
The slate demonstrating the highest compliance rate with double gloving, ie NSW, is
the only state with mandated infection control guidelines for health professionals that
link compliance to professional registration. In somc eases non-compliance can lead
to de-registration (NSW Health Departmcnt, 1995).
Policies can be general at thc organisational level but can bc more specific at
the unit level. For example, operating room units ean develop and implement
specific policies on using a neutral zone for sharps passage or eliminating hand-to
hand passage of sharps. Although using safe sharps handling techniques was not
found to be significant in the incidence ofoccupational exposure in this study (except
in the case of wearing adequatc eye protection (p< .05)), this study did find that of
the rcspondents incurring 1-2 or 3-5 occupational exposures in the past 12 months
there were varying degrees of non·compliance (e.g. for using a hands free sharps
passage technique (22.8-25%), for announcing sharps transfers (24.1-25%), for not
recapping needles (10.3-500/0». Speeifie policies on the use of goggles or masks
89

with side shields ean also be implemented on the unit level. As mentioned earlier,
wearing adequate protective eyewear was significant with the number of
occupational exposures ineurred and, of those, IO~25% were non-compliant with that
standard preeaution.
The best way to help the staff to comply with written policies is to let the
staff develop the policy. The more input that the staff has into policies on the unit
the more lik.ely they are to eomply. This is supported by White and Lyneh (1997)
who reported improved eompliance with standard precautions after involving
operating room personnel in identifying high-risk behaviours and situations and
developing strategies for improving compliance. Each operating theatre unit ean
establish working parties for the review of standard precautions and occupational
exposure reporting policies within their unit. Working parties from facilities in
geographically close areas ean network and share infonnation on current available
literature.
We aJl need reminders at some time m our lives. Organisational
implementation of an annual reminder to all staff regarding the monitoring of their
hepatitis and HIV status is another measure that can be utilised to increase
compliance rates with this NHMRC guideline. These reminders ean be sent out on
each anniversary date of all employees working in patient care areas, including the
operating rooms.
6.S. Summary and Conclusion
It is imperative that intervention strategies are developed and implemented to
improve the less than optimal compliance rates. These strategies can be categorised
under three main sub headings: prevenlion, education and policy. Prevention
strategies must include the provision of personal protective equipment, hepatitis B
90

vaccination and user-friendly and convenient reporting protocols. Effective
infection control programs must incorporate issues around risk and severity of blood
borne diseases, as well as issues around decreasing barriers to compliance with
standard precautions and occupational exposure reporting the behaviour.
Enforceable mandates and policies must be developed and implemented to ensure
complianee with standard precautions and occupational exposure reporting. All of
these strategies can be immediately implemented within individual operating theatre
units.
Data obtained from this study can be used to justify a larger scale study of the
standard precautions and occupational exposure reporting behaviour among all
operating room nurses, including members and non members of professional
organisations, so that the results are better generaliseable to the entire population of
operating room nurses in Australia. Once these results are known, national strategies
can be developed and implemented to decrease the risk of disease transmission in
this high risk category of health professionals.
91

Chapter 7. Summary of Thesis
National monitoring of occupational exposure to HIV, HBV and HCV began
in Australia in 1995. In 1998, data collection in Australia resultcd in a total of 1,718
reported exposures, at a rate of exposure of 25 cxposures per 100 daily occupied
beds, with 83% of thcsc exposures being percutaneous and about 60% of the
exposures reported by nurses (MacDonald and Ryan, 1999).
Although, standard precautions were introduced in thc 19805, research
continues to rcport less than 100% compliance among health care profcssionals with
measures that have been demonstrated to decrease disease transmission by
decreasing the risk of exposure. Cases of disease transmission of HIV, HBV and
HCV from occupationally acquired exposures have bccn documented in the
literature. It is impossible to distinguish blood and body substances infected with
harmful organisms from those not infccted without serological testing. This is the
underpinning premise of standard precautions, which stresses Ihe importancc of
treating all blood and body substances as if they were infected.
Operating room nursing is considered a high-risk nursing specialty because of
the increased likelihood of contact with blood and body substances. In order to
decrease the risk of transmission of a blood-borne infection from an occupational
exposure, health care workers, especially thosc in designated high risk areas, such as
the operating rooms, must take every precaution, demonstrated 10 be effective, to
prevent and protect themselves from occupational exposure, in the first instance.
Standard precautions, including bamer methods (e.g., double gloving and adcquatc
eye protection) and safc sharps handling (e.g., no-hands transfer technique,
immediate disposal of sharps, not recapping needles) have bccn found to be
significant in the reduction of oecupational exposures in the opcrating room. In
92

addition, prophylactic hepatitis B vaccination and prompt reporting and prophylactic
treatment following occupational exposure has been successful in prevention of
disease transmission following an occupational exposure.
A quantitative methodology (using a descriptive correlational design) was
chosen for this study because the intent of this study was to describe relationships
that may e.xlst between specific variables (or influenees) and standard precautions
and occupational exposure reporting behaviour of operating room nurses in
Australia. These relationships were examined utilising an instrument developed and
tested to explore them. A theoretical framework, the Health Belief Model, was
utilised to give the variables meaning and to be able to draw logieal conclusions
about which variables have the greatest influence over the health behaviour. In
future studies. interventions aimed at these variables can be developed in order to
exert the greatest impact on ehanging the health behaviour. Four of the five
constructs of the Health Belief Model were studied to detennine if these variables
have any influenee on whether an individual will undertake partieular health
behaviours. The four constructs studied were: (1) perception 0 f susceptibility or risk
to the illness, (2) perception of severity of the illness, (3) perception of benefits of
undertaking a recommended health behaviour, and (4) perception of barriers or costs
of undertaking a particular health behaviour (Davidhizar, 1983).
One of the most significant findings of this study is the less than 100%
compliance of operating room nurses in Australia with the five standard precaution
behaviours studied (i.e. double gloving, adequate eye protection, announcing sharps
transfers, using a hands-free sha'1's passage technique and no needle recapping).
Selfreported compliance with double gloving was 55.6%. Self reported compliance
with wearing adequate eye protection was 92.0%. Self reported compliance was
93

S9.1 % for announcing sharps transfers and 71.9% for using a hands free sharps
transfer technique. Self reported compliance with no needle recapping was 81.9%.
The highest compliance rate was with hepatitis B vaccination, with a compliance rate
of96.1%.
Although, there were no significant differences found among demographie
groups in their compliance rates with standard precautions or occupational exposure
reporting, the mean age for non compliance with standard preeautions and
occupational exposure reporting was greater than the mean age for compliance,
except for the specific behaviour of not recapping needles. Further studies on age
and compliance may assist in strategy development aimed at older nurses who may
be quite set in their ways.
Although some studies in the past have examined reasons given for non
complianee with standard precautions and occupational exposures, few studies have
attempted to examine influences on behaviour within a thcoretieal framework in
order to predict which reasons have greater a greater influence.
With respect to the constructs of the Health Belief Model, this study found
no significant differences among demographic groups in their perceptions of benefits
of and barriers to standard precautions and occupational exposure reporting. There
were, however, significant differences among demographic groups in their
perceptions of risk and severity of acquiring blood borne infections and compliance
with occupational exposure reporting.
The findings of this study partially support previous findings that the HBM is
appropriate in predieting eompliance with standard precautions and occupational
exposure reporting. One of the other significant findings of this study was the
influenee of perceptions of barriers on eomplianee with particular standard
94

precautions and with oeeupational exposure reporting. The hindrance to compliance
with standard preeautions and oecupational exposure reporting caused by pereeption
of barriers may be overeome through a structured multi-faceted intervention
program.
Intervention programs to improve compliance with standard preeautions and
oecupational exposure reporting must focus on prevention, education and poliey.
Prevention strategies that inelude provision and aceessibility of adequate supplies of
personal protective equipment, hepatitis B vaceination and eonvenient reporting
mechanisms are necessary. Education strategies must include programs aimed at
risk and severity issues, as well as concern about barriers in order to appeal to all
operating room nurses in one way or another. Policies must be in place to enforce
compliance with standard preeautions and occupational exposure reporting.
It is evident from this study that compliance among operating room nurses in
Australia with standard preeautions and occupational exposure reporting is less than
100%. Prevention of oceupational exposure through the diligent use of standard
precautions can decrease disease transmission. Prompt reporting and post exposure
management in the event of an exposure can also decrease the risk of disease
transmission. Operating room nurses need a reporting mechanism that is convenient,
Icss time consuming and involves less paperwork to make reporting as uscr.friendly
as possible. Reporting will also be useful in generating better data on the actual
occupational exposure rate among operating room nurses, which can then be
incorporated into a national strategic plan for the reduction of disease transmission
among this risk group in Australia.
The purpose of this study was to contribute to the body of nursing knowledge
by developing national estimates for compliance with standard precautions and
95

occupational exposure reporting practices in a high risk category of nursing. Data
from this study can provide a basis to develop and implement measures to improve
these practices, thus minimising occupational exposure and disease transmission
rates among this group. Additional projects can be developed to improve compliance
with slandard precautions and improve reporting of occupational exposure incidents
as they occur.
96

Appendix 1. Epidemiologically Significant Pathogens Requiring AdditionalPrecautions
Pathogen Mode of Transmission Additional PrecautionsRecommended**
Creutzfeld- Contact with infected central High temperature sterilisation (134°C)Jakob nelVOUS system (CNS) or of neurological instruments for aDisease neurological tissue minimum of 18 minutes single cyele or(CJO) six separate 3 minute cycles.GI pathogens Contact (oral faecal route) Single room with ensuite toilet IS
desirableHepatitis A Contact (oral faecal route) Additional precautions may be required(HAV) for incontinent patientsRBV*** Blood-borne pathogen; direct Standard Precautions
contact with blood or bodysubstances
ReV*** Blood-borne pathogen; direct Standard Precautionscontact with blood or bodysubstance.'>
HIV*** Blood-bome pathogen; direct Standard PrecautionscontaL't with blood or bodysubstances
Influenza Respiratory--airborne and Single room or cohort placement indroplet spread cases of outbreaks, particularly for
children and elderly patientsMeasles Airborne and droplet spread, Single room for infected patients during
direct contact with infected infectious period; infected staft" shouldthroat or nasal secretions- not be in contact with patientshighly communicable
Meningo- Respiratory via droplet from Standard precautions once treatmentcoccus nose or throat initiatedMumps Airborne-droplet spread and Single room for 9 days after onset of
direct contact with saliva of swellinglparoti tisinfected person
Pertussis Respiratory-airborne or droplet Single room for known cases for at least(whooping spread 5 days after start of antibiotic treatment.cough) Exclude suspected cases from the
presence of young children and infants,especially those not immunized
Rubella Droplet spread or direct contact Single roomStaphylo- Contact Additional precautions for MRSA -coccus single roomTuberculosi s Air borne Single room-see state and territory
tuberculosis guidelinesVaricella Airbome/Contact Single room; preclude non-lmmuneZoster exposed staff from working in areas(chicken with susceptible patientspox)
...Additional Precautions recommended in addition to Standard PrecautIons***Standard precautions only recommended for these blood-borne pathogens (the focus ofthis study)
97

Appendix 2. Conceptual Definitions
Sel(protective behaviour is defined as "activity undertaken by a person who
believes himself to be healthy for the purpose of preventing disease or detecting
disease in an asymptomatie state." (Kasl and Cobb, ]966)
Blood-borne infection is an infection that is transmitted via eontaminated
blood or other body fluids (e.g., HIV, HBV, HCY)
Standard Precautions are healthcare guidelines to protect the healtheare
worker from occupational exposure to blood·bome infections.
Occupational Exposure is an incident in whieh the healtheare worker has
been exposed to potentially infeetious blood or body fluids from a patient by
pereutaneous, mucocutaneous, or eutaneous exposure; or by any eombination of the
three.
Occupational Etposure Reporting is reporting an ineident of occupational
exposure in aeeordanee with established protocols (e.g. reporting the ineident to the
nurse manager and/or oeeupational health and safety unit) in order to ensure
treatment and follow up.
Percutaneous e.tposure is exposure to blood and/or body fluids through a
penetration in the skin (e.g. needle stick or other sharp injury).
Mucocutaneous exposure is an exposure to blood and/or body fluids through
mueous membranes in the eye, nose or mouth (e.g. splash injury).
Cutaneous exposure is an exposure to blood and/or body fluids through
eontamination of the epidennis of the skin (e.g. eontact exposure).
Perception o(Susceptibility or Risk is the degree to which a person perceives
him/herself to be at risk of acquiring a blood-borne infection.
Perception of Severity is the degree of consequence that a person pereeives
will result from acquiring a blood-borne infection, i.e., the degree to which hislher
life will be affected.
Perception ofBenefits is the perception of the efficacy of the self-protective
behaviour (either standard precautions or oeeupational exposure reporting) in
preventing or redueing the risk of acquiring a blood-borne infection.
Perception of Barriers is what a person perceives to be interfering with
his/her undertaking or eontinuing the self.protective behaviour.
98

Appendix 3. Cover letter accompanying ~urvey
Practice of Standard Precautions and Occupational Exposure Reporting
You are invited to participate in a research study. The title of the project is ~Operating room
nurses' knowledge. beliefs, and compliance with standard precautions and occupational
exposure reporting practices in Australian.
The purpose of this research study is twofold: (1) to assess operating room (OR) nurses'
knowledge, beliefs and practice of standard precautions. and (2) to evaluate their occupational
exposure reporting practices. Expected benefits of the project are an increased understanding
of beliefs and intentions of OR nurses to comply with standard precautions and occupational
exposure reporting. This has implications for further research by providing background and
support for future projects on development and implementation of measures 10 increase levels
of compliance.
As a participant in Ihe research study you will be provided with information about the research
project. If you have any questions that are not answered by the information provided, you
should consult the Research Study Investigator or the Research Supervisor. Requests for
reports of the Sludy may be addressed to the Research Study Investigator.
Research Study Investigator
Sonya Osborne, Masters Student
School of Nursing. Division of Science
ScienceDesign, University of Canberra
Canberra, ACT 2601
telephone: (02) 6201 5129
facsimile: (02) 6201 5128
Research Supervisor
Rev. Dr. Elizabeth MacKinlay
School of Nursing, Division of
and Design, University of Canberra
Canberra. ACT 2601
telephone: (02) 6201-2930
facsimile: (02) 6201 5128
If you wish to discuss with an independent person a complaint relating to (1) conduct
of the project. (2) your rights as a participant, or (3) university policy on research
involving human participants, you should contact the Secretary of the Uni'Jersity
Research Committee at telephone (02) 6201 2466 or by mail at Room 1085.
Secretariat, Uni'Jersity of Canberra. ACT 2601.
99

Appendix 4. Information for Participants
Practice of Standard Precautions and Occupational Exposure Reporting
Information for Participants
The University of Canberra Committee for Ethics in Human Research approved this research
study. Participation in this study is volunteer.
A 96·item survey was mailed out to randomly selected members of the Australian
Confederation of Operating Room Nurses (ACORN) who are currently employed in the
perioperative setting in Australia. The distribution of the surveys was undertaken by
ACORN. The Research Investigator did not and will not have access to your personal
information. Data will be collected anonymously. Returning the completed questionnaire to
the Research Study Investigator implies consent.
Completed surveys will be stored in locked filing cabinets at The University of Canberra and
computer data will be available only by password to the Research Study Investigator and the
Research Supervisor. Research participants will not be identified in any presentation or
publication resulting from this study.
Directions: You are requested to follow the directions preceding each section and answer all
questions based on your current beliefs and practice. You may avoid answering questions
that you do not wish to answer. Do not add your name to this form. Completion of lhe
survey should lake approximately 15 minutes of your time. Upon completion of the
questionnaire. please return it in the envelope provided by 1 Mar 2001.
Your cooperation in this study Is greatly appreciated.
100

Appendix 5. Survey Instrument
Section I
Directions for this section (items 1-11): Unleaa otherwise indicated, for each item
please tick the one box that most closely reflects your usual situation.
1. Age: (number in years)
2. Sex: 10Male 20Female
3. Nursing status: 10RN 20EN
4. Nursing education: 10 hospital 20 universitytrained trained
5. Years of post registration nursing experience:10<2 yrs 202-5 yrs 305-10 yrs 40>10 yr.
6. Years of Scrub nursing experience:~<2 yrs 202-5 yrs 305-10 yrs 40>10 yrs
7. Number of hospital beds in your facility:10<100 20101-300 30301-60 40>601
8. Number of operating theatres in your facility:101-2 203-5 306-8 40>8
9. Work category: 1Ofull time 20part time 30casual
10. Type of facility in which you work:1Oprivate hospital
30day surgery hospital
20public hospital
400ther
11. State or territory in which you work:10ACT 20NSW
SOTAS SOWA
30NT
70VlC
40SA
eOQLD
101

Section II
Directions for this section (Items 12-68): For each item, please circle the one answer
that best reflects your beliefs, altitudes and usual practice regarding standard
precautions.
Strongly Agree Neutral Disagree Stronglyagree Disagree
12. My chance of getting hepatitis B 2 3 4 5or C is high.
13. I have a large amount of 2 3 4 5contact with patients withhepatitis B or C.
14. My physical health makes it 2 3 4 5more likely that I will gethepatitis B or C.
15. There is a possibility that I will 2 3 4 5get hepatitis 8 or C.
16. I worry a lot about getting 1 2 3 4 5hepatitis B or C.
17. The thought of hepatitis B or C 1 2 3 4 5scares me.
18. If I get hepatitis B or C my 2 3 4 5career would be endangered.
19. Hepatitis 8 or C would 1 2 3 4 5endanger a significantrelationship.
20. My financial security would be 2 3 4 5endangered if I got hepatitis 8 orC.
21. Problems I would experience 2 3 4 5from hepatitis B or C would lasta long time.
22. Hepatitis Band C are serious 2 3 4 5diseases.
23. My work related activities put 1 2 3 4 5me at risk of contractinghepatitis B or C.
102

Strongly Agree Neutral Disagree Stronglyagree Disagree
24. If I sustain a percutaneous 2 3 4 5occupational exposure (i.e.contaminated needlestick/sharps injury), it is likelythat I would contract hepatitis Bor C.
25. If I sustain a mucous 2 3 4 5membrane occupationalexposure (i.e. splash withcontaminated blood or bodyfluids in eye, nose or mouth), itis likely that I would contracthepatitis Bar C.
26. Wearing protective eyewear 2 3 4 5(i.e. eyewear with side shields,a face shield, or a mask withshield) decreases my risk ofacquiring hepatitis B or C.
27. Double gloving when scrubbed 2 3 4 5for surgical proceduresdecreases my risk of acquiringhepatitis Bar C.
28. Not recapping needles 2 3 4 5decreases my risk of acquiringhepatitis B or C.
29. Announcing sharps transfers 1 2 3 4 5decreases my risk of acquiringhepatitis B or C.
30. Using a hands-free sharps 1 2 3 4 5passage technique decreasesmy risk of acquiring hepatitis Bor C.
31. The hepatitis B vaccine 1 2 3 4 5decreases my risk of acquiringhepatitis B.
32. I have a greater chance of 1 2 3 4 5getting hepatitis B or C as theresult of a sharps injury with asuture needle than with ahypodermic needle.
33. I always wear protective 2 3 4 5eyewear while scrubbed forsurgical procedures.
103

Strongly Agree Neutral Disagree Stronglyagree Disagree
34.1 always double glove while 1 2 3 4 5scrubbed for surgicalprocedures.
35.1 always recap hypodermic 1 2 3 4 5needles after use.
36. I always announce sharps 1 2 3 4 5transfers when passing sharps.
37. I always pass sharps using a 1 2 3 4 5"hands free" technique.
38. I have been vaccinated againsthepatitis B.
1DVes (PLEASE SKIP TOqUESTION 46)
2DNo (PLEASE GO TOQUESTION 39)
39. I have not obtained the hepatitis 2 3 4 5B vaccine because it won'tprotect me from getting aneedleslickJ sharps injury.
40. I have not obtained the hepatitis 2 3 4 5B vaccine because it offerslimited protection from acquiringhepatitis B after occupationalexposure.
41. I have not obtained the hepatitis 2 3 4 5B vaccine because I am afraidof needles.
42. I have not obtained the hepatitis 2 3 4 5B vaccine because it is painful.
43. I have not obtained the hepatitis 2 3 4 5B vaccine because I havepositive surface antigensalready.
44. I have not obtained the hepatitis 1 2 3 4 5B vaccine because theprocedure is inconvenienl.
45. I have not obtained the hepatitis 1 2 3 4 5B vaccine because myemployer does not provide it.
104

Strongly Agree Neutral Disagree Stronglyagree Disagree
46.1 have had my hepatitis 8 titrelevel checked for immunity in thepast 12 months?
1DVes
2DNo
47. I have had my HIV statuschecked in the past 12 months?
1DVes
2DNo
48. I always wear protective 1 2 3 4 5eyewear for every procedure.
49. Prescription glasses provide 1 2 3 4 5adequate protection from splashexposures.
50. Protective eyewear is not 1 2 3 4 5required for proceduresexpected to be less than twohours in duration.
51. Protective eyewear is not 1 2 3 4 5required for cases in whichblood loss is expected to beless than 100 millilitres.
52. Protective eyewear interferes 1 2 3 4 5with my duties.
53. Protective eyf1Near is 2 3 4 5uncomforfable.
54. Protective eyewear i5 2 3 4 5expensive.
55. Protective eyewear impairs my 2 3 4 5vision.
56. My employer does not provide 2 3 4 5protective eyewear.
57. I always double glove when 1 2 3 4 5scrubbing for surgicalprocedures.
58. There is no need to double 1 2 3 4 5glove for surgical proceduresless than two hours in duration.
lOS

Strongly Agree Neutral Disagree Stronglyagree Disagree
59.There is!lQ need to double glolle 2 3 4 5for surgical procedures whenblood loss is expected to be lessthan 100 millilitres.
60. I do not always double glolle 2 3 4 5because it produces handtingling and/or numbness.
61. I do not always double glolle 2 3 4 5because it interferes with myduties.
62. I do not always double glolle 1 2 3 4 5because it is too expensille.
63. I do not always double glolle 2 3 4 5because the glolles are a poorfit.
64. I do not always double glolle 1 2 3 4 5because there are limitedsupplies at my facility.
65. It is safer to dispose of 1 2 3 4 5hypodermic needles byrecapping.
66. I recap hypodermic needles by 1 2 3 4 5using the one-handedtechnique.
6? I recap hypodermic needles by 2 3 4 5using the two-handedtechnique.
68. I neller recap hypodermic 1 2 3 4 5needles.
106

Section III
Directions tor this section (items 69·96): For each item, please circle the one answer
that most closely reflects your beliefs. attitudes and usual practice regarding
occupational exposure reporting.
Strongly Agree Neutral Disagree Stronglyagree Disagree
69.Reporting and following up on 2 3 4 5occupational exposuresprevents future problems forme.
70. Reporting and following up on 1 2 3 4 5occupational exposures wouldbenefit my family and me.
71. It is embarrassing for me to 2 3 4 5report an occupationalexposure.
72. Reporting and following up on 2 3 4 5occupational exposures can bean unpleasant experience.
73. Reporting and following up on 1 2 3 4 5occupational exposures is timeconsuming.
74. If I report and follow up on 1 2 3 4 5occupational exposures I maydiscover disease transmissionbefore it is discovered by aroutine health exam.
75. I would not be so anxious 2 3 4 5about hepatitis B or C it Ireported occupationalexpOsures.
76. My partner/parent would make 1 2 3 4 5tun ot me for reporting anoccupational exposure.
107

Strongly Agree Neutral Disagree Stronglyagree Disagree
77.The practice of reporting and 2 3 4 5following up on an occupationalexposure interferes with myduties.
78. I am afraid I would not be able 1 2 3 4 5to report an occupationalexposure.
79. If I sustained a percutaneous 1 2 4 5sharps injury I would report it.
80. I would report a percutaneous 1 2 3 4 5sharps injury only if the patientwas in a high risk category.
81. I would not report a 2 3 4 5percutaneous sharps injury if Idid not think it was a seriousinjury.
82. I would not report a 1 2 3 4 5percutaneous sharps injurybecause the procedure islengthy and time consuming.
83. I would not report a 1 2 3 4 5percutaneous sharps injurybecause it would beembarrassing.
84. I would not report a 2 3 4 5percutaneous sharps injurybecause there is too muchpaperwork involved.
85. I would not report a 1 2 3 4 5percutaneous sharps injurybecause the procedure isinconvenient.
86. If 1sustained a mucous 1 2 3 4 5membrane exposure I wouldreport it.
87. I would report a mucous 2 3 4 5membrane injury only if thepalient was in a high riskcategory.
88. I would not report a mucous 1 2 3 4 5membrane injury if I did notthink it was a serious injury.
t08

Strongly Agree Neutral Disagree Stronglyagree Disagree
89.1 would not report a mucous 2 3 4 5membrane injury because theprocedure is lengthy and timeconsuming.
90. I would not report a mucous 2 3 4 5membrane injury because itwould be embarrassing.
91.1 would not report a mucous 1 3 4 5membrane injury because ofthe paperwork involved.
92. 1would not report a mucous 1 2 3 4 5membrane injury because theprocedure is inconvenient
93.How many perculaneous sharps injuries have you sustained in the last twelve months?
10none 201-2 303-5 407-10 50>10
94. How many of these percutaneous sharps injuries did you report?
10none 201-2 303-5 407-10 50>10
95. How many mucous membrane exposures have you sustained in the last twelve months?
10none 201-2 407-10 50>10
96. How many of these mucous membrane exposures did you report?
10none 201-2 303-5
End of Survey
407-10 50>10
Thank you for taking the timeto complete and return
this survey_
109

Appendix 6. Items Evidencing Internal Consisteney for Risk, Severity andBenefit Scales
Item
RisksQI2 HIGH CHANCEQ15 POSSIBILITYQl6 WORRY A LOTQ23 DUTIES PUT ME AT RISKQ24 LIKELY IF POEX OCCURS
Cronbach Alpha =
SeverityQ18 CAREER ENDANGEREDQ19 RELATIONSHIPS ENDANGEREDQ20 FINANCIAL SECURITY ENDANGERED
Cronbach Alpha =
Corrected Item-Total Correlation
.39
.34
.36
.35
.59
.71
.49
.47
.59
.70
BenefitsStandard PreeautionsQ26 EYE PROTECTION: .{). RISK .2 J
Q27 DOUBLE GLOVES: .{).RISK .27Q28 NOT RECAPPING:.{).RISK .30Q29 ANNOUNCING SHARPS TRANSFERS: .{).RISK .57Q30 HANDS FREE TECHNIQUE: D-RISK .30Q31 HEPB VACCINATION:.{). RISK .00
Cronbach Alpha = .51
Occupational Exposure ReportingQ690ER: PREVENTS FUTURE PROBLEMS .19Q700ER: BENEFITS ME ANO FAMILY .28Q74 OER: DJSCOVER DISEASE TRANSMISSION EARLY .08Q7) OER : .{). ANXIETY .25
Cronbach Alpha = .34
110

Appendix 7. Items Evidencing Internal Consistency for Barrier Scale
Item Corrected Item-Total Correlation
Bllrriers
GlovesBA60 PRODUCES HAND NUMBNESS
AND TINGLING .62BA61 lNTERFERES WITH DUTIES ,71BA62 TOO EXPENSIVE .46BA63 POOR FIT .64BA64 LIMITED SUPPLY .44Cronbacb Alpha = .78
Eye ProtectionBA52 INTERFERES WITH DUTIES .52BA53 UNCOMFORTABLE .68BA54 EXPENSIVE .39BA55 IMPAlRS V1SON .70Croobach Alpha = .76
Hepatitis B VaccinationBA39VAC .94BA40VAC .61BA44VAC .94BA45VAC .94Croobach Alpha = .93
Occupational Exposure Reporting (Mucocutaneous Exposures)BA89 TIME CONSUMING .66BA90 EMBARRASSING .51BA9l TOO MUCH PAPERWORK .70BA92 INCONVENIENT .65Cronbaeh Alpba .87
Occupational Exposure Reporting (Percutaoeous Exposures)
BA82 TIME CONSUMINGBA83 EMBARRASSINGBA84 TOO MUCH PAPERWORKBA85 INCONVENIENTCronbach Alpba
.63
.47
.70
.63
.86
til

Appendix 8. Demographies of the Sample
Nursing Educationhospital traineduniv and/or hospital trainedno answer
Years Post RegistrationNuning Experienceless than 2 years 0.9%2 to 5 years 4.4%5 to 10 years 11.0%greater than 10 years 83.8%
74.3%24.3%1.3%
Aee Range of Partieipants20-29 years 5.8%30-39 years 30.8%40-49 years 75.4%50-59 years 23.7%greater than 60 years 0.9%
Years Scrub Nurse Experienceless than 2 years 7.9%2 to 5 years 10.1 %5 to 10 years 15.0%greater than 10 years 67.0%
Type of FacilityPrivate/day hospitalpublic hospitalNo or both answers
31.4%65.0%3.6%
Employment Statusfull timepart time/casualno answer
59.7%38.93.6%
Number of Bedsless than I 00101 to 300301 to 600greater than 600
22.8%37.1%30.4%9.8%
Number ofOperatio2 Rooms1 to 2 16.4%3 to 5 37.6%6 to 8 23.5%greater than 8 22.6%
112

Appendix 9. Demographic Variables and Standard Precantions Compliance
Demographic: Variable Chi S~uare P('ll
Age Group033 I always wear protective eyewear when scrubbed 35.777 .000*034 1always double glove while scrubbed for sur~ical procedures 5.695 .681035 I always recap hypodermic needles after use.t 18.802 .016·036 [ alwayS announce sharps transfers when passing sharps 15.842 .045·Q37 I always pass sharps using a "hands-tree" technique 3.396 .907Q38 I have been vaccinated against hepatitis B 5,877 .209
02 Gender (male or female)Q33 I always wear protective eyewear when scrubbed 2.214 .331034 I always double £love while scrubbed for surgical procedures 1.441 .486035 I always recap hypodermic needles after use.t 1.026 .5990361 always announce sharps transfers when passin~ shams 6.641 .036*037 I always pass sh8Jl)s usine a "hands-free" techniQue 2.378 .305038 I have been vaccinated against hepatitis B .346 .557
03 Nurse Status (RN or EN)Q33 I always wear protective eyewear when scrubbed .635 .72&034 I always double glove while scrubbed for surgical procedures .562 .755Q35 I always recap hypodemlic needles after use.t 1.601 .449
Q36 I alwavs announce shams transfe~ when passing sharps .484 .785
037 I always pass sharps using a "hands-free" techniQue 3.394 .183Q38 [have been vaccinated against hepatitis B .298 .585
Q4 Highest Nursing Education (hospital or university)Q33 I always wear protective eyewear when ~crubbed .304 .990Q34 I always double glove while scrubbed for surgical procedures 6.856 .144035 I always recap hypodermic needles after use.t 5.179 .221<)36 I always announce sharps transfers when passing sharps 2.604 .626<)37 I always pass sharps using a "hands-free" technique 3.326 .505038 I have been vaccinated against hepatitis B 3.197 .202
Q5 Years of Post-registration Nursing ExperienceQ33 I always wear protective eyewear when scrubbed 2.585 .859034 J always double glove while scrubbed for surgical procedures lO.307 .112( 35 I always recap hypodermic needles after use.t 4.931 .553( 36 I always announce sharps transfers when passing sharps 16.415 .012*037 I always pass sharps using a "hands-tree" technique 5.491 .483038 I have been vaccinated against hepatitis B 1.825 .6lO
Q6 Years Scrub Nurse ExperienceQ33 I always wear protective eyewear when scrubbed 7.23 .300034 1alwavs double glove while scrubbed for sur~ical procedures 12.38 .054Q36 I alwavs announce sharps transfers when passing sharps 5.269 .510037 I always pass sharps using a "hands-tree" technique 11.263 .081035 I always recap hypodermic needles after use.t 6.10 .409038 I have been vaccinated against hepatitis B 1.32 .723
.p < .05.
113

Demognphit Vniable1i and Standard Precautions Compliance (continued)
Demographic Variable Chi S~uare P(oil
Q7 Size of facilityQ33 I always wear protective evewear when scrubbed 6.890 .331034 I alwavs double ~Iove while scrubbed for sur~ical procedures 15.761 .015·035 I always recap hypodermic needles after use.t 10.251 .114036 I always announce sharps transfers when passing sharps 12.544 .051-Q37 I always pass sharps using a "hands-free" techniaue 10.269 .114Q38 1have been vaccinated a~ainst hepatitis B .715 .870
08 Number ofoperating theatres033 I alwayS wear protective eyewear when scrubbed 3.003 .809034 I always double glove while scrubbed for sur~ical Drocedures 14.025 .029·035 I always recap hypodermic needles after use.t 5.856 .4390361 alwavs announce shams transfers when passing shams 4.473 .613037 I always pass shams using a "hands-free" techniaue 1.748 .941038 J have been vaccinated against hepatitis B .992 .820
09 Type ofemployment (fulltime, part-time or casual)033 I always wear protective eyewear when scrubbed 1.702 .790Q34 I always double glove while scrubbed for surgical nrocedures 9.370 .052·Q35 I always recap hypodermic needles after use.t 5.137 .274Q36 I always announce shams transfers when passing shams 10.905 .028-037 I always pass sharps using a "hands-free" technique 3.446 .486038 I have been vaccinated against hepatitis B 3.069 .216
010 Type of Facility (public or private/day only hospital)Q33 I always wear protective evewear when scrubbed 2.810 .590034 I always double glove while scrubbed for surgical procedures 2.816 .589035 I always recap hvoodennic needles after u~e. t 1.712 .789036 I always announce sharps transfers when passing sharps 4.741 .3[5
Q37 I always pass sharps usin~ a "hands-free" techniQue 1.980 .739Q38 I have been vaccinated a~ainst henatitis B .818 .664
Q 11 State of El11J)lovmentQ33 I always wear protective eyewear when scrubbed 40.47 .000·Q34 I always double glove while scrubbed for sureical nrocedures 57.69 .000·035 I always recap hypodermic needles after use.t 8.47 .583036 I always announce sharps transfers when passing shams 24.781 .006·OJ7 I always pass sharps usine a "hands~free" techniaue 14.239 .162038 I have been vaccinated against hepatitis B 1.31 .934
.p < ,os.
114

Appendix to. Demographic Variables and Occupational Exposure Reporting
Demographic VariAble Chi S~uare P(11
)
Age Group( 79 If I sustained a percutaneous sharps injury I would report it. 20.825 .007*( 86 If I sustained a mucous membrane exposure I would report it. 12.553 .129
02 Gender (male or female)079 If I sustained a percutaneous sharps injury I would report it. .725 .696Q86 If I sustained a mucous membrane exposure I would report it. .940 .625
Q3 Nurse Status (RN or EN)079 IfI sustained a percutaneous sharps injury I would report it. .663 .718086 IfI sustained a mucous membrane exposure I would report it. 1.282 .527
Q4 Highest Nursing Education (hospital or university)Q79 IfI sustained a percutaneous sharps iniurv I would report it. 2.998 .558Q86 1fT sustained a mucous membrane eXpOsure I would report it. 1.859 .762
Q5 Years of Post-registration Nursin.g Experience079 If I sustained a percutaneous sharps injury I would report it. 2.449 .874086 IfI sustained a mucous membrane exposure I would repon it. 3.187 .785
Q6 Years Scrub Nurse ExperienceQ79 If I sustained a percutaneous sharps iniurv I would report it. 4.377 .629Q86 If I sustained a mucous membrane exposure I would report it. 8.627 .196
07 Size of facility079 If I sustained a percutaneous sharps injury I would report it. 4.072 .667086 1ft sustained a mucous membrane exposure I would report it. 13. t 53 .041·
Q8 Number of operating theatresQ79 If I sustained a percutaneous shams rni urv I would report it. 7.498 .277086 Ifl sustained a mucous membrane exposure I would report it. 14.700 .023*
Q9 Type of employment (fulltime, part-time or casual)Q79 If I sustained a percutaneous sharps iniury I would report it. 2.536 .638Q86 IfI sustained a mucous membrane exposure I would report it. 3.689 .450
QlO Type of Facility (public or private/day onlv hospital)079 If I sustained a percutaneous sharps injury I would report it. 3.083 .544086 If I sustained a mucous membrane exposure I would report it. 10.021 .040*
011 State of EmploymentQ79 If I sustained a percutaneous sharps rniurv I would report it. 11.470 .322Q86 If I sustained a mucous membrane exposure I would report it. 14.522 .150
.p < .05.
lI5

References
ACT Government (1997). Occupational Risk Exposure Management. Australian
Capital Territory: Canberra.
Akduman D, Kim LE, Parks RL, L'Ecuyer PB, Mutha S, Jeffe DB, Evanoff BA,
Fraser V1 (1998). Usc of personal protective equipment and operating room
behaviors in four surgical subspecialties: personal protective equipment and
behaviors in surgery, Infection Control & Hospital Epidemiology, 20(2): 110
114.
Association of PeriOperative Registered Nurses, Inc (2000). Recommended
practices for standard and transmission-based precautions in the perioperative
practice setting. Standards, Recommended Practiees and Guidelines, AORN:
Denver, 336.
Atkinson, LJ (1992). Occupational hazards and safety in Berry & Kohn's Operating
Room Technique, Mosby Year Book: St. Louis, 244-264.
Australian College of Operating Room Nurses (2000). Standards, guidelines and
policy statements, ACORN: Adelaide.
Australian Institute of Health and Welfare (1999). Nursing Labour Force 1998 (cat
no. HWL 14), Australian Institute ofHealth and Welfare: Canberra.
Becker MH (ed.) (1974). The health belief model and personal health behaviour.
Charles B. Slack: Thorofare, New Jersey.
Bums N & Grove SK (1997). The practice of nursing researeh: Conduct, critique, &
utilization (3Td ed). WB Saunders Company: Philadephia.
Bums RB (2000). Introduction to research methods. Longman: Frenehs Forest,
NSW.
Cardo DM, Culver DH, Ciesielski CA, Srivastava PU, Marcus R, Abiteboul D,
Heptonstall J, Ippolito G, Lot F, McKibben PS & Bell DM (1997). A case
control study of HIV seroconversion in health eare workers after
percutaneous exposure. Centers for Disease Control and Prevention
Needlestick Surveillance Group, New England Journal of Medicine, 337(21):
1485-90.
Centers for Disease Control (1994). Draft guidelines for isolation precautions in
hospitals. Federal Register, 59:214.
116

Centers for Disease Control (1997). Recommendations for follow-up of HCW after
occupational exposure to HCV. MMWR, 46: 603-606.
Centers for Disease Control (1998t. Public health service guidelines for the
management of health care worker exposures to HIV and recommendations
for postexposure prophylaxis. MMWR 47 (RR-7): 1~33.
Centers for Disease Control (1 998)b. Recommendations for prevention and control
of Hepatitis C Virus (HCV) infection and HCV-related chronic disease.
MMWR, 47 (RR-19): 1-39.
Champion VL (1984). Instrument development for health belief model constructs.
Advances in Nursing Science, 2..-(3): 73-85.
Colbert S and Sheehan GJ (1995). Human immunodeficiency virus and hepatitis
implications for operating room personnel. Irish Journal of Medieal Science,
164: 12-19.
Davidhizar R (1983). Critique of the health-belief model. Journal of Advanced
Nursing, ~(6): 467-472.
Davis, MS (1999). Advaneed Precautions for Today's O.R., Sweinbinder
Publieations LLC: Atlanta.
deVaus, DA (1995). Surveys in soeial research .. Allen & Unwin: St Leonards, NSW.
Dodds RnA, Barker SGE, Donaldson DR & Thomas MH (1990). Selfproteetion in
surgery: the use of double gloves. British Journal of Surgery, 77: 219-220.
Gauthier OK, Turner JG, Langley LG, Neil CJ & Rush PL (1991). Monitoring
universal precautions: a new assessment tool. Infection Control & Hospital
Epidemiology, 11 (10); 597-601.
Gebcrding JL (1993). Procedure-specific infection control for preventing
intraoperative blood ex:posures. Arneriean Journal of Infection Control, ll:
364-367.
Geberding JL (1996). Prophylaxis for occupational exposure to HTV. Annals of
Internal Medieine, 125: 497-501.
Grady MM, Shortridge LA, Davis LS & Klinger CS. (1993). Occupational exposure
to blood-borne diseases and universal precautions: measurement of health
care workers' self-reported attitudes. AAOHN Journal, 41: 533-540.
Greundcmann BJ & Fernsebner B (1995). Comprehensive Perioperative Nursing:
Volume I Principles. Jones and Bartlett Publishers: Boston, 352-353.
[17

Gruber M, Beavers FE, Johnson B, Brackett M, Lopez T Feldman MJ & Ventura M
(1989). The relationship between knowledge about acquired
immunodeficiency syndrome and the implementation of universal precautions
by registered nurses. Clinieal Nurse Specialist, J.(4): 182-185.
Hammond JS, Eckes JM, Gomez GA & Cunningham DN (1990). HIV, trauma. and
infection control: universal precautions are universally ignored. Journal of
Trauma-Injury Infection & Critical Care, 30 (5): 555-558.
Hamory BH (1983). Underreporting of needlestick injuries in a university hospital.
Amcrican Journal of Infection Control. 11(5): 174-177.
Henry K, Campbell S & Maki MA (1992). Comparison of observed and self
reported compliance with universal precautions among emergency
department personnel at a Minnesota Public Teaching Hospital: Implications
for assessing infeetion control programs. Annals of Emergency Mcdicine,
21(8): 940-946.
Henry, K Campbell S, Collier P & Williams C (1994). Complianec with universal
precautions and needle handling and disposal practices among emergency
department staff at two community hospitals. American Journal of Infection
Control, 22 (3): 129-137.
Hersey Je & Martin LS (1994). Use of infection control guidelines by workers in
healtheare facilities to prevcnt occupational transmission of HBV and HIV:
Results from a national survey. Infection Control and Hospital Epidemiology,
U (4): 243-252.
Hunter, S (1998). Your infection control program. Occupational Health & Safety,
August: 76-80.
International Health Care Worker Safety Center [rHCWSC], University of Virginia
Health Scienees Center (1998). Estimated annual number of U.S.
occupational percutaneous injuries and mucocutaneous exposures to blood or
at-risk biological substances. Advances in Exposure Prevention, 1:(1): 3.
Jagger J & Perry J (2000). Safety in the OR. Nursing, 30 (8): 77.
Jaggcr J, Hunt EH & Pearson R (1990). Sharp object injuries in the hospital: causes
and strategies for prevention. American Journal of Infection Control, ~:
227-231.
Jeffe DB, Mutha S, L'Ecuyer PB, Kim LE. Singal RB, Evanoff BA & Fraser VJ
(1997). Healthcare workers' attitudes and compliance with universal
118

precautions: Gender, occupation, and specialty differences, Infection Control
and Hospital Epidemiology, .li: 71 0-712.
Jensen SL, Kristensen B & Fabrin K (1997). Double gloving as self protection in
abdominal surgery. European Journal of Surgery, 163: 163-166.
Johnson & Johnson Medical Inc. (1995). Occupational exposure to blood: Clinical
implications and the financial impact of accidental occupational exposure to
blood, 11M, Inc.: Texas, 5.
Kas] SV & Cobb S (1966). Health behaviour, illness behaviour and the sick-role
behaviour. Archives of Environmental Health, 11: 246-266.
Kovach T (1993). Controlling infection potentials when passing surgical instruments.
Today's OR Nurse, U. (November/December): 36-37.
Knowles, MS (1998). The Adult Leamer (5 1h edition), Gulf Publishing Company:
Houston, 4.
Lynch P & White MC (1993). Perioperative blood contact and exposures: A
comparison of incident reports and focused studies. American Journal of
Infection Control, 21 (6): 357-363.
MacDonald M and Ryan G (1999). Monitoring occupational exposure 10 blood
borne viruses in health care workers in Australia. Australian HIV
Surveillance Report, U. (2): 1-6.
Mangione CM, Gerberding JL & Cummings SR (1991). Occupational exposure to
HIV: frequency and rates of underreporting of percutaneous and
mucocutaneous exposures by medical houscstaff. American Journal of
Medicine, 90( 1):85-90.
Marin-Bertolin S, Gonzales-Martinez MD, Gimenez CN, Vila PM & AmOITortu
Velayos J (1996). Does double gloving protect surgical staff from skin
contamination during plastic surgery. Plastic and Reconstructive Surgery, 99:
956-960.
Michalsen A, Delclos GL, Felknor SA, Davidson AL, Johnson PC, Vcsley D,
Murphy LR, Kelen GD & Gershon RR (1997). Compliance with universal
precautions among physicians. Journal of Occupational & Environmental
Medicine. 39(2):130-137.
Mujeeb SA, Khatri Y & Khanani R (1998). Frequency of parenteral exposure and
seroprevalence of HBV, HCV, and HIV among operation room personnel.
Journal of Hospital Infection, 38: 133-137.
119

National Centre in HIV Epidemiology and Clinical Research (19991 Australian
health surveillance report, U(2).
National Centre in HIV Epidemiology and Clinical Research (1995). Australian
health surveillanee report, IH4).
National Health and Medical Research Council [NHMRC)(l996). Infection Control
in the Health Care Setting. Commonwealth of Australia: Canberra.
Nelsing S, Nielsen TL, & Nielsen JO (1997). Noncompliance with universal
precautions and the associated risk of mucocutaneous blood exposure among
Danish physicians. Infection Control and Hospital Epidemiology, ll.
(10):692-698.
New South Wales Nurses Registration Board (1995). Infection Control Regulations,
Nurses ACT 1991 ~Regulation (relating to infeetion control standards), 1995
No. 221.
NSW Health Department (1995). Infection Control Policy, Circular 95/13.
Patterson JM, Novak CB, Mackinnon SE & Patterson GA (1998). Surgeons' concern
and practices of protection against bloodbome pathogens. Annals of Surgery,
228(2):266-272.
Polit DF and Hungler BP (1995). Nursing Research Principles and Praetiee. JB
Lippincott Company: Philadelphia.
Pugliese G (1993). Should blood exposure in the operating room be considered part
of the job? American Journal of Infection Control, £1 (6): 337-342.
Rosenstock 1M (1974). Historical origins of the health belief model. Health
Education Monographs, ~(2): 328-335.
Ross HS and Mico PRo (1980). Theory and Practice in Health Education. Mayfield
Publishing Co.:PaloAlto, California, p58.
Royal Australasian College of Surgeons (1998). Policy document: Infection Control
in Surgery, R.A.C.S.: Melbourne.
Sahdev P, Lacqua MJ, Harrigan N, Evans JT & Vaish AK (1994). Barrier
precautions in trauma resuscitations: multivaried analysis of factors affecting
use. Annals of Emergency Medicine, 23:823-827.
Sepkowitz KA (1996). Oeeupationally acquired infections in health care workers.
Annals of Internal Medicine, 125 (11): 917-928.
Short L, Chamberland M, Culver D, Henry K, Geberding J, Mendelson M, et al.
(1994). Underrcporting of needle stick injuries among healthcare workers.
120

The Needlestick Study Group, Infection Control and Hospital Epidemiology,
II (suppl): P20 (Abstract)
Short U & Bell DM (1993). Risk 0 f oeeupational infection with blood-borne
pathogens in operating and delivery room settings. Ameriean Journal of
Infection Control, 21 (6): 343-350.
Souhrada, L (1995). The blunt truth about sharps injuries in the OR. Materials
Management in Healtheare, 1: 1.
Tait AR, Voepel-Lewis T, Tuttle B & Malviya S (2000). Complianee with standard
guidelines for the prevention of oecupational transmission of bloodborne and
airborne pathogens: A survey of post anaesthesia nursing practice. The
Journal of Continuing Edueation in Nursing, 1.1 (I): 38-44.
Tandberg D, Stewart KK & Doezema D (1991). Under-reporting of contaminated
needlestick injuries in emergeney health eare workers. Annals of Emergency
Medicine, 20(1 ):66-70.
Telford GL & Quebbeman EJ (1993). Assessing the risk of blood exposure in the
operating room. American Journal ofInfection Control, li (6): 351-356.
Tokars JL, Culver DH, Mendelson MH, Sloan EP, Farber BF, Fligner DJ,
Chamberland ME, Marcus R, McKibben PS, & Bell DM (1995). Skin and
mucous membrane contacts with blood during surgical procedures: risk and
prevention. Infection Control and Hospital Epidemiology, 16 (12), 703-7 t 1.
Troya SH, Jackson MM, Lovrich KM, McPherson DC (1991). A survey of nurses'
knowledge, opinions, and reported uses of the Body Substance Isolation
System. Ameriean Journal ofInfection Control, l2.:268-276.
Weiss SH, Goedert 11, Gartner S, et al. (1988). Risk of human immunodeficieney
virus (HIV-1) infection among laboratory workers. Science, 239: 68.
White MC & Lynch P (1993). Blood contact and exposures among operating room
personnel: a multicenter study. American Journal of Infeetion Control,
li(5):243-248.
White MC & Lynch P (1997). Blood contacts in the operating room after hospital
specific data analysis and action. American Journal of Infection Control.
25(3):209-214.
Williams CO, Campbell S, Henry K & Collier P (1994). Variables influencing
worker compliance with universal precautions in the emergency department.
Ameriean Journal of Infection Control, 22: 138-148.
121

WrighllG. McGeer Al, Chyattc D & RansohoffDF. (1991). Mechanisms of glove
lears and sharp inj uries among surgical personnel. lAMA, 266 (12): 1668
1671.
122