Embed Size (px)
Citation preview
ORIG INAL ART ICLE
Compliance of Saudi dental students with infection controlguidelines
Ibrahim Ali Ahmad1, Elaf Ali Rehan1 and Sharat Chandra Pani2
1Restorative Dentistry Department, Riyadh Colleges of Dentistry and Pharmacy, Riyadh, Saudi Arabia; 2Preventive Dentistry Department,Riyadh Colleges of Dentistry and Pharmacy, Riyadh, Saudi Arabia.
The aim of this study was to investigate compliance of dental students in a Saudi dental school with recommended infec-tion control protocols. A pilot-tested questionnaire concerning various aspects of infection control practices was distrib-uted to 330 dental students. The response rate was 93.9% (n = 311). About 99% of students recorded the medicalhistory of their patients and 80% were vaccinated against hepatitis B. The highest compliance (100%) with recom-mended guidelines was reported for wearing gloves and use of a new saliva ejector for each patient. Over 90% of therespondents changed gloves between patients, wore face masks, changed hand instruments, burs and handpieces betweenpatients, used a rubber dam in restorative procedures and discarded sharp objects in special containers. A lower usagerate was reported for changing face masks between patients (81%), disinfecting impression materials (87%) and dentalprosthesis (74%) and wearing gowns (57%). Eye glasses and face shield were used by less than one-third of the sample.The majority of students were found to be in compliance with most of the investigated infection control measures. Nev-ertheless, further education is needed to improve some infection control measures including vaccination for Hepatitis Bvirus (HBV), wearing eye glasses, gowns and face shields and disinfecting impression materials and dental prostheses.
Key words: Compliance, dental students, hepatitis B, infection control, Kingdom of Saudi Arabia
INTRODUCTION
Infection control is today without doubt an integralpart of contemporary dental practice1. The repeatedexposure of dental health-care professionals (DHCPs)to pathogenic microorganisms causing diseases suchas the common cold, pneumonia, tuberculosis, hepati-tis B and acquired immune deficiency syndrome placesthem at a greater risk of acquiring and spreadinginfections2–4.A number of cross-infection guidelines have been
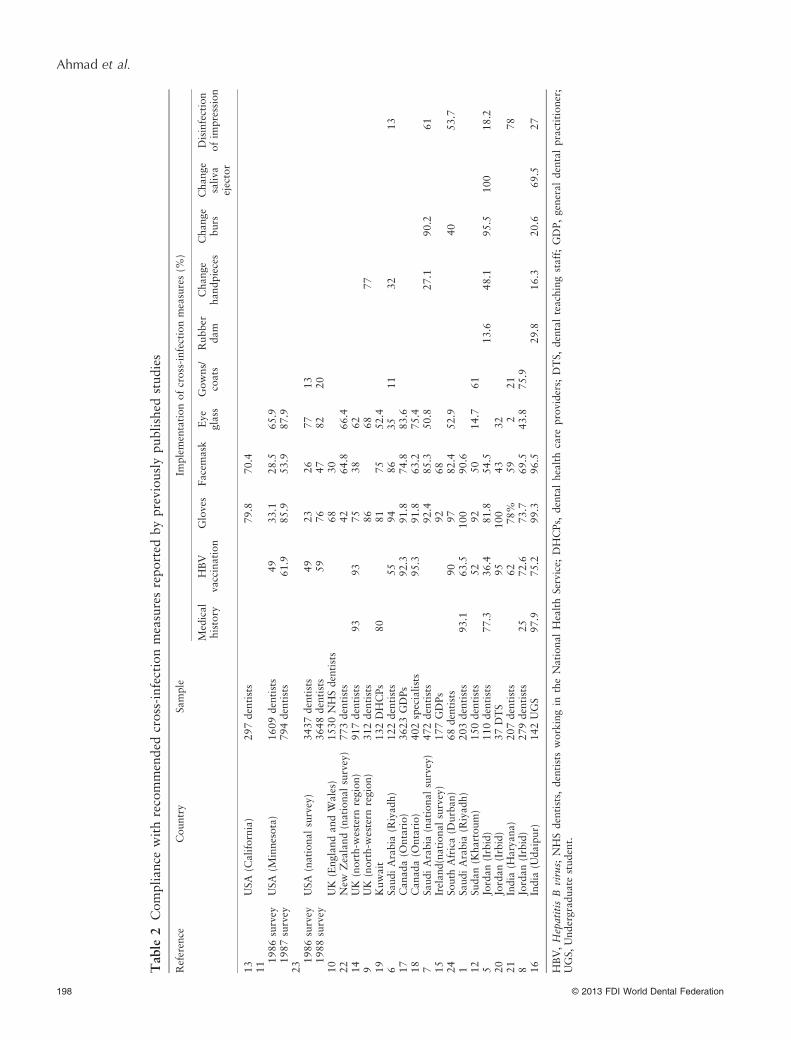
advocated by health and professional organisations toprevent or reduce the potential for disease transmis-sion between DHCPs and the patients and betweenthe patients themselves (Table 1)2–4. The complianceof DHCPs with these guidelines has been investigatedby a number of studies worldwide1,5–24. The results ofthese reports showed variations in implementation ofthe recommended guidelines and a need to improveadherence to some aspects of infection control prac-tices (Table 2).
There is little information regarding compliancewith universal control precautions in the Middle Eastin general and Saudi Arabia in particular. Therefore,the aim of this study was to investigate the compli-ance of dental students in a private school in SaudiArabia with recommended cross-infection protocols.
MATERIALS AND METHODS
The study was conducted in full accordance with theWorld Medical Association Declaration of Helsinkiand ethical clearance was obtained from the researchcentre of the institution. The study sample includedundergraduate students in their clinical years (fourthto sixth year) and dental interns. The students wereasked to complete a self-administered, anonymousquestionnaire. The questionnaire was developed afterconsulting with specialists from each dental specialtyat the teaching hospital and based on similarquestionnaires used in the past5,21. The initial question-naire was then tested for reliability and reproducibility
196 © 2013 FDI World Dental Federation
International Dental Journal 2013; 63: 196–201
doi: 10.1111/idj.12030

using Cronbach’s alpha. The initial questionnaire hada Cronbach’s alpha of 0.86, with scores for itemsranging from 0.79 to 0.91, suggesting good reliability.Further details of the validation of the questionnaireare beyond the scope of this paper.The questionnaire included 18 questions that evalu-
ated: (1) demographic data (gender and academiclevel); (2) Recording patient’s medical history and stu-dents’ hepatitis B virus (HBV) vaccination status; (3)use of personal protective equipment; (4) sterilisationand/or disinfection of patient-care items; (5) disposalof sharp medical objects. The data were tabulated andanalysed using the Statistical Package for Social Sci-ence (SPSS for Windows version 17.0; SPSS Inc, Chi-cago, IL, USA). Data analysis included descriptivestatistics and Pearson’s chi-square (v2) test was usedto assess differences in infection control practicesaccording to the gender and academic level of therespondents. A probability value of < 0.05 was con-sidered statistically significant.
RESULTS
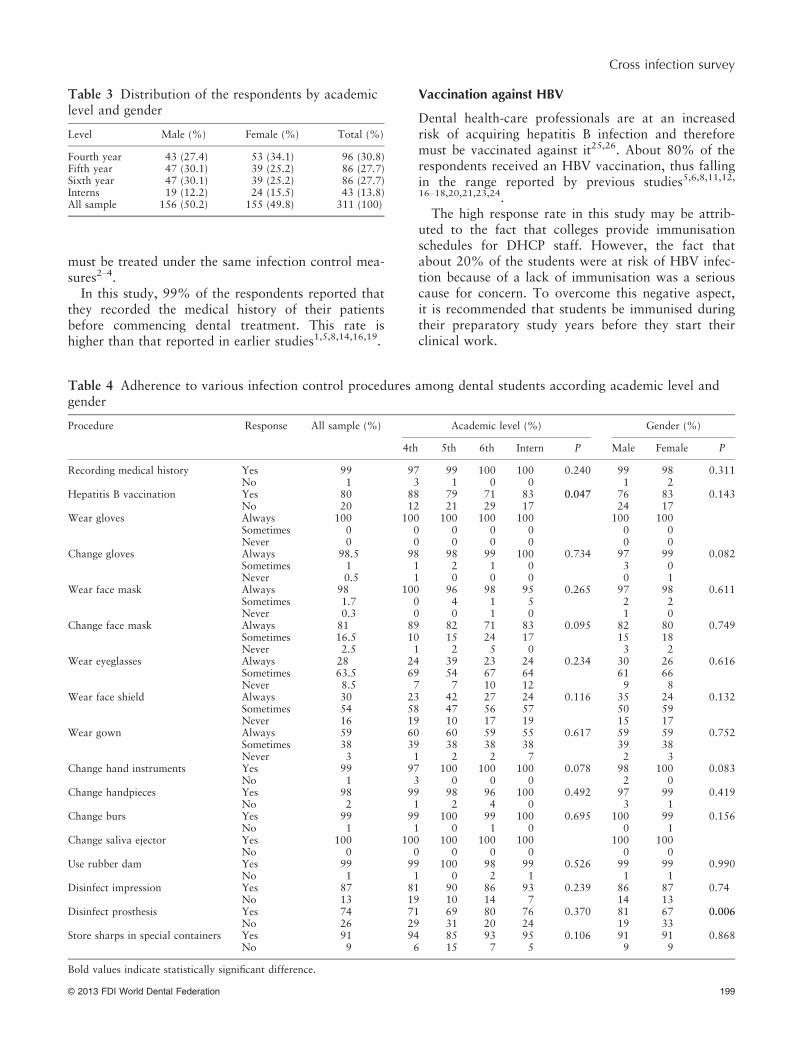
Overall, 311 students (93.9%) responded to the sur-vey. The distribution of respondents by academic leveland gender is shown is Table 3.About 99% reported that they usually review the
medical history of their patients before commencingdental treatment and 80% were vaccinated againsthepatitis B (Table 4).Among the personal protective equipment, the
highest compliance rates were reported for wearing(100%) and changing (98.5%) gloves betweenpatients. Face mask ranked second: 98% of studentsreported that they wore it routinely and about 80%changed it between patients. However, fewer subjectswore gowns (57%) while only one-third of the sam-ple used the face shield and eye glasses on a routinebasis.Almost all the students (99%) changed hand instru-
ments and burs between patients and all of themchanged saliva ejectors between patients. Approxi-mately 98% reported that they changed handpiecesbetween patients. Routine disinfection of impressions
and prostheses was undertaken by 87% and 74% ofthe respondents, respectively. Finally, 99% of thestudy sample used a rubber dam and 91% discardedsharp objects in special containers.Pearson’s chi-square test showed that HBV vaccina-
tion status was the only infection control procedurethat differed significantly between the academic levels:more of the fourth year students and the dentalinterns received the vaccine compared with the finalundergraduate years students (fifth and sixth years).When evaluating the effect of gender, male respon-dents reported significantly more disinfection of dentalprostheses.
DISCUSSION
There are many possible routes for the transmissionof infection within dental procedures, including directcontact with blood, oral fluids and other secretions orindirect contact with contaminated instruments, oper-atory equipment and environmental surfaces. Infectionmay even occur as a result of contact with droplets,splatter, airborne contaminants and aerosols2–4.Adherence to various aspects of universally recom-mended guidelines is therefore critical to preventcross-infection between the health providers andpatients, and indeed the patients themselves.
Medical history
A thorough medical history must be recorded andreviewed before starting the dental treatment andupdated at subsequent visits3. It may help in detectionof infectious diseases and provides clues about whatprecautions are necessary for patients having medicalproblems that require pre-medications or modifica-tions of treatment applied5.Given that the identification of infectious diseases
through medical history, physical examination or lab-oratory tests may not always be possible, the Centreof Disease Control and Prevention (Atlanta, GA,USA) introduced the concept of ‘universal precau-tions’. The concept states that each patient must beconsidered as ‘potentially infectious’ and all patients
Table 1 Cross-infection control guidelines
Immunisation against infectious diseases (i.e. hepatitis B virus)Use of personal protective equipment (PPE) including gloves, masks, protective eyewear, face shields and protective clothing such as gowns andjacketsSterilisation and/or disinfection of patient-care itemsCritical items are those that penetrate soft tissue, contact bone, enter into or contact the bloodstream or other normally sterile tissue.Examples include: surgical instruments, periodontal scalers, scalpel blades and surgical dental bursSemi-critical items are those that contact mucous membranes or non-intact skin; they will not penetrate soft tissue, contact bone, enter into orcontact the bloodstream or other normally sterile tissue. Examples include: dental mouth mirror, amalgam condenser, reusable dentalimpression trays and dental handpiecesNon-critical items are those that contact intact skin. Examples include: radiograph head/cone, blood pressure cuff, facebow and pulse oximeterEnvironmental infection control of operating surfaces such as light handles, unit switches and drawer knobsSafe disposal of waste materials
© 2013 FDI World Dental Federation 197
Cross infection survey
Table
2Compliance
withrecommended
cross-infectionmeasuresreported
bypreviouslypublished
studies
Reference
Country
Sample
Implementationofcross-infectionmeasures(%
)
Medical
history
HBV
vaccination
Gloves
Facemask
Eye
glass
Gowns/
coats
Rubber
dam
Change
handpieces
Change
burs
Change
saliva
ejector
Disinfection
ofim
pression
13
USA
(California)
297dentists
79.8
70.4
11 1986survey
USA
(Minnesota)
1609dentists
49
33.1
28.5
65.9
1987survey
794dentists
61.9
85.9
53.9
87.9
23 1986survey
USA
(nationalsurvey)
3437dentists
49
23
26
77
13
1988survey
3648dentists
59
76
47
82
20
10
UK
(EnglandandW
ales)
1530NHSdentists
68
30
22
New
Zealand(nationalsurvey)
773dentists
42
64.8
66.4
14
UK
(north-w
estern
region)
917dentists
93
93
75
38
62
9UK
(north-w
estern
region)
312dentists
86
68
77
19
Kuwait
132DHCPs
80
81
75
52.4
6SaudiArabia
(Riyad
h)
122dentists
55
94
86
35
11
32
13
17
Canad
a(O
ntario)
3623GDPs
92.3
91.8
74.8
83.6
18
Canad
a(O
ntario)
402specialists
95.3
91.8
63.2
75.4
7SaudiArabia
(nationalsurvey)
472dentists
92.4
85.3
50.8
27.1
90.2
61
15
Ireland(nationalsurvey)
177GDPs
92
68
24
South
Africa(D
urban)
68dentists
90
97
82.4
52.9
40
53.7
1SaudiArabia
(Riyad
h)
203dentists
93.1
63.5
100
90.6
12
Sudan(K
hartoum)
150dentists
52
92
50
14.7
61
5Jordan(Irbid)
110dentists
77.3
36.4
81.8
54.5
13.6
48.1
95.5
100
18.2
20
Jordan(Irbid)
37DTS
95
100
43
32
21
India
(Haryana)
207dentists
62
78%
59
221
78
8Jordan(Irbid)
279dentists
25
72.6
73.7
69.5
43.8
75.9
16
India
(Udaipur)
142UGS
97.9
75.2
99.3
96.5
29.8
16.3
20.6
69.5
27
HBV,Hepatitis
Bvirus;
NHSdentists,
dentistsworkingin
theNational
HealthService;
DHCPs,
dentalhealthcare
providers;
DTS,dentalteachingstaff;GDP,generaldentalpractitioner;
UGS,
Undergraduate
student.
198 © 2013 FDI World Dental Federation
Ahmad et al.
must be treated under the same infection control mea-sures2–4.In this study, 99% of the respondents reported that
they recorded the medical history of their patientsbefore commencing dental treatment. This rate ishigher than that reported in earlier studies1,5,8,14,16,19.
Vaccination against HBV
Dental health-care professionals are at an increasedrisk of acquiring hepatitis B infection and thereforemust be vaccinated against it25,26. About 80% of therespondents received an HBV vaccination, thus fallingin the range reported by previous studies5,6,8,11,12,16–18,20,21,23,24.The high response rate in this study may be attrib-
uted to the fact that colleges provide immunisationschedules for DHCP staff. However, the fact thatabout 20% of the students were at risk of HBV infec-tion because of a lack of immunisation was a seriouscause for concern. To overcome this negative aspect,it is recommended that students be immunised duringtheir preparatory study years before they start theirclinical work.
Table 3 Distribution of the respondents by academiclevel and gender
Level Male (%) Female (%) Total (%)
Fourth year 43 (27.4) 53 (34.1) 96 (30.8)Fifth year 47 (30.1) 39 (25.2) 86 (27.7)Sixth year 47 (30.1) 39 (25.2) 86 (27.7)Interns 19 (12.2) 24 (15.5) 43 (13.8)All sample 156 (50.2) 155 (49.8) 311 (100)
Table 4 Adherence to various infection control procedures among dental students according academic level andgender
Procedure Response All sample (%) Academic level (%) Gender (%)
4th 5th 6th Intern P Male Female P
Recording medical history Yes 99 97 99 100 100 0.240 99 98 0.311No 1 3 1 0 0 1 2
Hepatitis B vaccination Yes 80 88 79 71 83 0.047 76 83 0.143No 20 12 21 29 17 24 17
Wear gloves Always 100 100 100 100 100 100 100Sometimes 0 0 0 0 0 0 0Never 0 0 0 0 0 0 0
Change gloves Always 98.5 98 98 99 100 0.734 97 99 0.082Sometimes 1 1 2 1 0 3 0Never 0.5 1 0 0 0 0 1
Wear face mask Always 98 100 96 98 95 0.265 97 98 0.611Sometimes 1.7 0 4 1 5 2 2Never 0.3 0 0 1 0 1 0
Change face mask Always 81 89 82 71 83 0.095 82 80 0.749Sometimes 16.5 10 15 24 17 15 18Never 2.5 1 2 5 0 3 2
Wear eyeglasses Always 28 24 39 23 24 0.234 30 26 0.616Sometimes 63.5 69 54 67 64 61 66Never 8.5 7 7 10 12 9 8
Wear face shield Always 30 23 42 27 24 0.116 35 24 0.132Sometimes 54 58 47 56 57 50 59Never 16 19 10 17 19 15 17
Wear gown Always 59 60 60 59 55 0.617 59 59 0.752Sometimes 38 39 38 38 38 39 38Never 3 1 2 2 7 2 3
Change hand instruments Yes 99 97 100 100 100 0.078 98 100 0.083No 1 3 0 0 0 2 0
Change handpieces Yes 98 99 98 96 100 0.492 97 99 0.419No 2 1 2 4 0 3 1
Change burs Yes 99 99 100 99 100 0.695 100 99 0.156No 1 1 0 1 0 0 1
Change saliva ejector Yes 100 100 100 100 100 100 100No 0 0 0 0 0 0 0
Use rubber dam Yes 99 99 100 98 99 0.526 99 99 0.990No 1 1 0 2 1 1 1
Disinfect impression Yes 87 81 90 86 93 0.239 86 87 0.74No 13 19 10 14 7 14 13
Disinfect prosthesis Yes 74 71 69 80 76 0.370 81 67 0.006No 26 29 31 20 24 19 33
Store sharps in special containers Yes 91 94 85 93 95 0.106 91 91 0.868No 9 6 15 7 5 9 9
Bold values indicate statistically significant difference.
© 2013 FDI World Dental Federation 199
Cross infection survey

Personal protective equipment
The purpose of personal protective equipment (PPE) isto protect the skin and mucous membrane of the eyes,nose and mouth of the DHCP from exposure topatients’ blood or fluids and in an oral health settingthese would include gloves, mouth masks, faceshields, protective eyewear and protective clothingsuch as gowns or jackets4.Gloves are perhaps the most commonly used PPE,
preventing contamination of the DHCP’s hands whiletouching mucous membranes blood or saliva and atthe same time preventing transmission of microorgan-isms from the hands of the DHCP to the patient. Anew pair of gloves must be worn for each patient andchanged when punctured or torn. AS exposure to dis-infectants can cause defects in gloves, diminishing theirvalue as an effective barrier, repeated use of glovesafter disinfection between patients should beavoided3,4. All the study sample wore gloves and98.5% changed them between patients. This compli-ance with routine glove-wearing and -changing com-pares favourably with previously published studieswhich showed that the routine use of gloves increasedfrom as low as 23% in late 1980s to 100% now1,20,23.The second highest level of compliance was
reported for wearing (98%) and changing (81%) facemasks. The current usage rate reported in the dentalliterature is in the range of 26–96.5% (Table 2). Incontrast, fewer applicants wore face shields (30%)and protective eye glasses (28%). Indeed, the routineuse of the latter barriers is low among the dentists allover the world (Table 2). Efforts must be made toencourage the routine use of these measures amongstudents, especially when air aerosols are expected toform (i.e. during scaling or cavity preparation). In thiscontext, additional protection may be achieved by theregular use of a rubber dam, as this was shown to sig-nificantly reduce bacterial contamination of the atmo-sphere during restorative procedures27. Fortunately,99% of the students in this study used a rubber damfor all restorative procedures, in comparison with40% of the dentists in South Africa24 and 13.6% ofJordanian dentists5 and 29.8% of undergraduateIndian students16.
Sterilisation and disinfection of patient-care items
Patient-care items are generally categorised into criti-cal, semi-critical or non-critical items (Table 1). Criti-cal items must be sterilised while disinfection and/orsurface protection is generally adequate for semi-critical and non-critical items. Of particular concern aredental handpieces which should be heat-sterilisedbetween patients despite the fact that they are classifiedas semi-critical items3,4.
In the current study, almost all the respondents(99%) used sterilised kits of hand instruments anddental burs for each patient and 98% changed thehandpieces after each patient. In contrast to a numberof published studies, 100% of respondents changedsaliva ejectors between patients, reflecting a high levelof compliance with recommended guidelines.A risk of infection of laboratory technicians by sal-
iva or blood-borne infections such as HBV has beendocumented6,28. Therefore, items such as impressions,casts, jaw relation records, prosthetic restorations anddevices that have been in the patient’s mouth must bedisinfected before they are sent to a dental labora-tory4. In the current study, 87% of the respondentsdisinfected impressions before sending them to dentallaboratories compared with the 53.7% reported byYengopal et al.24, and 18.1% by Al-Omari &Al-Dwairi5. However, only 74% of the study sampledisinfected dental prostheses before insertion into theirpatients’ mouths. Additional education is required topromote routine disinfection of impressions and pros-theses.
Disposal of waste materials
Waste materials must be handled carefully and dis-carded to minimise human contact. Disposable mate-rials such as gloves, masks, wipes, paper drapes andsurface covers that are contaminated with blood orbody fluids should be discarded in sturdy, imperviousplastic bags. Sharp items, such as needles and scalpelblades, should be placed into puncture-resistant con-tainers before disposal in plastic bags3. In previousstudies, 8–75% of dentists used puncture-resistantcontainers compared with 91% of the respondents inthis study1,5,8,14,16,21.It has been previously noted that students tend to
be more meticulous in following infection control pro-tocols than practising dentists and the results of thisstudy confirm that finding. Why do more dental stu-dents than practising dentists comply with infectioncontrol protocols? Three reasons may account for thedifference. First, during their study the students arewilling to learn and practise the different aspects oftheir future career. Second, cost/fee considerations,which have been shown to be a barrier for routineimplementation of cross-infection protocols, are usu-ally not applicable in a dental school setting. Third,implementation of these measures is mandatory in thisacademic institution and forms part of the student’sevaluation. This cohort of students may be surveyedagain in their future practices to see if their compli-ance rate has been maintained.The findings of this study must be seen as the prac-
tices in a single school and cannot be considered asbeing representative of students across Saudi Arabia.
200 © 2013 FDI World Dental Federation
Ahmad et al.
However, the findings could serve as a template forthe planning and implementation of future interven-tions, including a national survey of schools and prac-titioners across the country. Further research wouldbe needed to correlate observational data and corre-late those findings with the responses on the question-naires.
CONCLUSIONS
Dental students have an increased awareness of theimplementation of effective cross-infection controlmeasures. However, further improvement is needed ina number of areas such as vaccination against HBV,the wearing of eye glasses, face shields and gowns,and disinfection of dental prostheses before insertioninto the patients’ mouths. These areas may beaddressed by short-term courses and continuing edu-cation programmes, particularly those involving prac-tical component.
Acknowledgements
The authors are grateful to the students who partici-pated in this study.
Conflict of interest
None declared.
REFERENCES
1. Al-Rabeah A, Mohamed AG. Infection control in the privatedental sector in Riyadh. Ann Saudi Med 2002 22: 13–17.
2. The control of cross-infection in dentistry. Br Dent J 1988 165:353–354.
3. Infection control recommendations for the dental office and thedental laboratory. ADA Council on Scientific Affairs and ADACouncil on Dental Practice. J Am Dent Assoc 1996 127: 672–680.
4. Kohn WG, Collins AS, Cleveland JL et al. Guidelines for infec-tion control in dental health-care settings –2003. MMWRRecomm Rep 2003 52: 1–61.
5. Al-Omari MA, Al-Dwairi ZN. Compliance with infection con-trol programs in private dental clinics in Jordan. J Dent Educ2005 69: 693–698.
6. Al Bagieh NH. Cross-infection control practice of staff in a den-tal school. Odontostomatol Trop 1997 20: 25–28.
7. Al Shammary AR. Infection control measures among dentistspracticing in Saudi Arabia. Saudi Dent J 2000 12: 77–82.
8. AlNegrish A, Al Momani AS, Al Sharafat F. Compliance of Jor-danian dentists with infection control strategies. Int Dent J2008 58: 231–236.
9. Bentley EM, Sarll DW. Improvements in cross-infection controlin general dental practice. Br Dent J 1995 179: 19–21.
10. Burke FJ, Wilson NH, Wastell DG et al. Glove use in clinicalpractice: a survey of 2000 dentists in England and Wales. BrDent J 1991 171: 128–132.
11. DiAngelis AJ, Martens LV, Little JW et al. Infection controlpractices of Minnesota dentists: changes during 1 year. J AmDent Assoc 1989 118: 299–303.
12. Elkarim IA, Abdulla ZA, Yahia NA et al. Basic infection con-trol procedures in dental practice in Khartoum–Sudan. Int DentJ 2004 54: 413–417.
13. Gerbert B. AIDS and infection control in dental practice: den-tists’ attitudes, knowledge, and behavior. J Am Dent Assoc1987 114: 311–314.
14. Hudson-Davies SC, Jones JH, Sarll DW. Cross-infection controlin general dental practice: dentists’ behaviour compared withtheir knowledge and opinions. Br Dent J 1995 178: 365–369.
15. Kearns HP, Burke FJ, Cheung SW. Cross-infection control indental practice in the Republic of Ireland. Int Dent J 2001 51:17–22.
16. Kumar S, Sharma J, Duraiswamy P et al. Infection control prac-tices among undergraduate students from a private dentalschool in India. Rev Odonto Cienc 2009 24: 124–128.
17. McCarthy GM, MacDonald JK. The infection control practicesof general dental practitioners. Infect Control Hosp Epidemiol1997 18: 699–703.
18. McCarthy GM, MacDonald JK. A comparison of infection con-trol practices of different groups of oral specialists and generaldental practitioners. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1998 85: 47–54.
19. Morris E, Hassan FS, Al Nafisi A et al. Infection controlKnowledge and Practices in Kuwait: a survey on oral healthcare workers. Saudi Dent J 1996 8: 19–26.
20. Qudeimat MA, Farrah RY, Owais AI. Infection control knowl-edge and practices among dentists and dental nurses at a Jorda-nian University Teaching Center. Am J Infect Control 2006 34:218–222.
21. Rai B, Anand S, Jain R. Infection control procedures employedduring dental practice in Haryana (India). Int J Epidemiol 20063. Available from: http://www.ispub.com/journal/the-internet-journal-of-epidemiology/volume-3-number-2/infection-control-procedures-employed-during-dental-practice-in-haryana-india.html#sthash.ELwkpudi.dpbs. Accessed 07 July 2012.
22. Treasure P, Treasure ET. Survey of infection control proceduresin New Zealand dental practices. Int Dent J 1994 44: 342–348.
23. Verrusio AC, Neidle EA, Nash KD et al. The dentist and infec-tious diseases: a national survey of attitudes and behavior. JAm Dent Assoc 1989 118: 553–562.
24. Yengopal V, Naidoo S, Chikte UM. Infection control amongdentists in private practice in Durban. SADJ 2001 56: 580–584.
25. Cottone JA. Hepatitis B virus infection in the dental profession.J Am Dent Assoc 1985 110: 617–621.
26. Mosley JW, White E. Viral hepatitis as an occupational hazardof dentists. J Am Dent Assoc 1975 90: 992–997.
27. Cochran MA, Miller CH, Sheldrake MA. The efficacy of therubber dam as a barrier to the spread of microorganisms duringdental treatment. J Am Dent Assoc 1989 119: 141–144.
28. Georgescu CE, Skaug NF, Patrascu I. Cross infection in den-tistry. Roum Biotechnol Lett 2002 7: 861–868.
Correspondence to:Dr. Ibrahim Ali Ahmad,
Postal box 84891 Riyadh 11681,Restorative Dentistry Department,
Riyadh Colleges of Dentistry and Pharmacy,Saudi Arabia.
Email: [email protected]
© 2013 FDI World Dental Federation 201
Cross infection survey















![Infection Control Guidelines for Dental Clinics [compatibility mode]](https://img.pdfslide.us/doc/110x75/545c9b04af7959be098b4896/infection-control-guidelines-for-dental-clinics-compatibility-mode.jpg)













