Embed Size (px)
Citation preview
Complex Topics in Arthroscopic Subacromial Spaceand Rotator Cuff Surgery
Richard K. N. Ryu, M.D., Stephen S. Burkhart, M.D., Peter M. Parten, M.D.,and R. Michael Gross, M.D.
APPROACH TO THE FAILEDARTHROSCOPIC SUBACROMIAL
DECOMPRESSION
Richard K. N. Ryu, M.D.
The purpose of this presentation is to accomplishthe three “Ds”: (1) Define failed arthroscopic
subacromial decompression (ASD), (2) Determine thecause, and (3) “Do the right thing.” The success ratewith arthroscopic subacromial decompression has his-torically ranged from 80%-90%.1-7 Therefore, a “fail-ure” rate of 10%-20% must be accounted for. In thosecircumstances where a failure has occurred, frustra-tion on the part of both patient and physician caninterfere with a systematic approach to surgical fail-ure. It is essential that the surgeon be meticulous andsystematic in the assessment of the failed ASD.
Although the time interval before deciding that anacromioplasty has failed is debatable, patients withpersistent symptomatology who are six months statuspost decompression should be considered potentialfailures. The definition of a failed arthroscopic sub-acromial decompression would be any or a combina-tion of the following: persistent pain, weakness, mo-tion loss, or an inability to return to sports, recreation,or the workplace.
Once a failed ASD has been determined, the fol-lowing questions need to be answered: (1) Was theinitial diagnosis correct? (2) Was the appropriate pro-cedure chosen? (3) Was the procedure performed cor-rectly? (4) Was associated pathology recognized andadequately treated? And (5) Was the rehabilitation
timely and appropriate? Once these questions havebeen answered, there are three possible explanations:(1) Incorrect diagnosis, (2) Technical or treatmenterror, (3) Complication of treatment.
Incorrect Diagnosis
Diagnostic error can account for failure followingarthroscopic subacromial decompression. Several in-vestigators have attributed nearly 50% of acromio-plasty failures to an incorrect or missed diagnosis.3,8,9
The most common possibilities include unrecognizedprimary shoulder instability with secondary rotatorcuff symptoms, internal rotation contracture, neuro-logic dysfunction such as a brachial plexus neuritis,thoracic outlet syndrome or cervical radiculopathy,glenohumeral arthritis, acromioclavicular arthritis,and symptomatic os acromiale. The following high-lights several of these diagnostic dilemmas.
Instability
Unrecognized shoulder instability can be found inthe younger overhand athletic population. Internal im-pingement as a possible source of pain should beconsidered,10-12 whereas primary external impinge-ment due to outlet impingement is uncommon. Ar-throscopic subacromial decompression under thesecircumstances serves only to destabilize an alreadycompromised shoulder, and in many cases, leads to aworsening of symptoms. Persistent posterior shoulderpain in the young overhead athlete should lead to ahigh index of suspicion for internal rather than exter-nal impingement in this patient population. An arthro-scopic subacromial decompression would only be ap-propriate in conjunction with primary treatment suchas capsular plication and/or SLAP repair, and if sec-ondary changes are present in the subacromial space.
Address correspondence to Richard K. N. Ryu, M.D., 533 E.Micheltorena St, Santa Barbara, CA 93103, U.S.A. E-mail:[email protected]
© 2002 by the Arthroscopy Association of North America0749-8063/02/1802-0105$35.00/0doi:10.1053/jars.2002.31798
51Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 18, No 2 (February, Suppl 1), 2002: pp 51-64

Os Acromiale
For those patients with a symptomatic os acromiale,a decompression alone may not be sufficient if themobile fragment is the source of pain.13 Oftentimesthe mobile fragment alone may be the source of on-going discomfort and may occur absent any impinge-ment phenomenon. Once the diagnosis of a symptom-atic os acromiale has been made with the use of acareful history and physical examination, bone scan,contralateral comparison x-rays, and motion at thenon-union site has been confirmed at arthroscopy,open reduction and internal fixation with parallel can-nulated screws supplemented with local bone graftfrom the greater tuberosity is the recommended treat-ment.14,15One exception would be the pre-acromion, asmall fragment which can be excised in its entiretywith minimal morbidity. For the meso-, meta-, orbasi-acromion, internal fixation would be recom-mended. Although others16,17have described success-ful arthroscopic excision or near total excision of themeso-acromion without residual sequelae, should asubsequent weakness or pain pattern develop due toloss of the deltoid fulcrum, no adequate solution ex-ists.
Posterior Capsular Contracture
Limitations in internal rotation, often noted in theoverhand athlete, can shift the center of humeral headrotation into a posterior-superior direction, effectivelycreating a secondary impingement as the humeralhead and rotator cuff are forced into the subacromialspace. In a reported series of nine isolated internalrotation contractures,18 three occurring after an arthro-scopic subacromial decompression, eight of nine pa-tients who underwent an isolated posterior capsularrelease were relieved of pain. Internal rotation in theabducted position increased an average of nearly 40degrees.
An awareness of this unusual source of impinge-ment type pain, and a careful examination evaluatinginternal rotation in the abducted position can helpprevent missing this diagnosis which will not respondto decompression alone.
Technical Error
Technical errors can and do occur and usually takethe form of variable bone resection. The most com-mon error is under-resection with a residual spur in anexternal impingement patient leading to persistentsymptoms. Under-resection has been cited as a cause
of failure2,3,19,20in up to 50% of failed cases. Over-resection can lead to intraoperative or delayed frac-ture,29 as well as possible deltoid detachment.1,22
Fractures following an acromioplasty have historicallybeen associated with a poor prognosis.
Obtaining quality, preoperative radiographs and inparticular, the outlet view, allows the surgeon to de-termine the amount of bone resection, as well as thesize and shape of the acromion. The cutting blocktechnique23 can be used for the actual bone resection,as well as for measuring the amount of bone excised.If a lateral portal technique for bone resection is used,a blunt trocar passed from the posterior portal can beused to assess acromial morphology and to determineif adequate bone has been resected. If the acromion isthin and curved, the cutting block technique must bemodified such that a “contoured” acromioplasty isperformed and thinning avoided.
Treatment FailuresRotator Cuff Insufficiency: There is a role for
arthroscopic subacromial decompression in the rotatorcuff deficient patient. In a limited goals operation, anarthroscopic subacromial decompression can yieldsignificant pain relief even though the rotator cuff isnot repaired. Careful selection of the proper candidatefor an isolated decompression in the face of a rotatorcuff which is not repairable, or in a patient who electsnot to undergo a formal repair, is imperative. Anyevidence of superior migration of the humeral head onthe AP radiographs is a contraindication to an isolateddecompression. As a guideline, patients with an intactsubscapularis and at least one-half of their infraspina-tus and teres minor intact, usually maintain satisfac-tory force couples allowing for a decompression with-out decompensating the shoulder.24,25 Individualswithout balanced force couples may require an intactcoracoacromial arch acting as a fulcrum in order toelevate their arm. In these instances, removing a por-tion of the acromion and releasing the CA ligamentputs these patients at risk for loss of superior contain-ment of the humeral head with subsequent loss of thearch, a predicament for which there is no good solu-tion.
Partial Rotator Cuff Tear: There has been con-siderable discussion regarding the appropriate treat-ment of high-grade partial rotator cuff tears. A recentstudy26 indicated that for partial rotator cuff tears ofless than 50% treated by decompression only, thelong-term success rate was equal to that of patientswith minimal rotator cuff pathology treated with ASDalone. Others have cited their experience with poor
52 R.K.N. RYU ET AL.

outcomes following isolated decompression in indi-viduals in whom a high-grade partial tear is present,high-grade being defined as 50% or greater.27-30In theyoung active population, especially in a dominantextremity, at the time of a proposed decompression, ifsignificant rotator cuff pathology is noted in the formof a high-grade partial tear, current recommendationsinclude not only a decompression but repair of thepartial rotator cuff tear. This could be achieved withan arthroscopic trans-tendon repair with anchorsplaced in the foot print of the rotator cuff or withcompletion of the tear from the bursal side of the cufffollowed by a routine arthroscopic rotator cuff repair.I believe it is critical for the surgeon to discuss thispossibility with all patients undergoing a routinearthroscopicsubacromial decompression. AlthoughMRI scans or other preoperative testing may yieldwhat appears to be sufficient information regardingthe status of the rotator cuff, there is enough uncer-tainty with diagnostic testing such that discussion ofall possible pathologies and the surgical algorithmmust be discussed in advance with the patient so thata complete solution can be accomplished at the time ofsurgery.
Workers’ Compensation
Results in the Workers’ Compensation categorysuggest a glaring difference in the success rate be-tween patients treated with a decompression and thoseinjured on an industrial basis treated with a decom-pression.1,3,20,24Although there may be a mechanicalreason for failure, the issue of “secondary gain” canplace the Workers’ Compensation group into the treat-ment failure category. At least one author has cited afailure rate of 18% despite a correct diagnosis andcorrect treatment being rendered.3 Despite this poten-tial selection bias, it is important for the surgeon todiscuss in advance with the patient and possibly thecase manager, the expected course which usually in-volves more postoperative pain, a slower rehabilita-tion, and a slower return to duties. Despite the docu-mented poor outcomes in the Workers’ Compensationgroup, it is important for the surgeon to carefullyevaluate each of these patients for a potential causeother than their worker’s status.
Complications of Treatment
Following surgery in the subacromial space, com-plications can occur, including infection, neurovascu-lar injury, arthrofibrosis, reflex sympathetic dystro-phy, heterotropic ossification, late acromioclavicular
joint pain, as well as recurrent spur formation. Themost common reported complication following arthro-scopic subacromial decompression is scarring.35
The Captured Shoulder
The captured shoulder was described in 1996 andattributed to subdeltoid adhesions following subacro-mial space surgery. This in turn led to compensatorymechanics and asynchronous shoulder girdle motion.Although the arthroscopic subacromial decompressionis usually performed with little concern for scarring,the possibility of scarring and “capture” of the sub-acromial space secondary to bleeding and raw sur-faces must be considered. A well-conceived, super-vised rehabilitation program can help minimize thisrisk. In particular, posterior capsular stretching to pre-vent the possibility of an internal rotation contracturepostoperatively can help minimize the risk of continu-ing impingement forces. Furthermore, a full functionalrange of motion should be achieved before strengthwork is initiated, and particular attention should bepaid to the scapula as it is often overlooked. For acomplete recovery, scapular strengthening and normalscapulothoracic and glenohumeral synchrony must bereestablished safely.
Coplaning and Late Pain
Several authors have reported late acromioclavicu-lar (A-C) pain following arthroscopic subacromial de-compression combined with co-planing of the distalclavicle.32,33Interruption of the inferior capsule desta-bilizes the A-C joint, which may in turn cause prema-ture acromioclavicular joint degeneration. Despiteearly reports of late A-C pain and the destabilizingeffect of co-planing, several recent clinical reviewshave failed to identify an increase in late A-C jointdisease following co-planing.34,35Current recommen-dations emphasize a thorough preoperative evaluationof the A-C joint, and a complete resection in conjunc-tion with an ASD if true A-C pathology is diagnosed.Unless there is evidence that distal clavicular spurringis a source of symptoms, the A-C joint should bespared.
Conclusions
When confronted with a failed ASD, the treatingphysician must consider the following: diagnostic er-ror, technical or treatment failures, and complicationsof treatment. The treating physician must methodi-cally identify the reason for failure and then proceedwith corrective action if indicated. It is imperative to
53SUBACROMIAL SPACE AND ROTATOR CUFF

remember that up to 15 percent of failures may nothave a discernible cause with the correct diagnosis andcorrect operation having been performed. One must bepatient and meticulous and should remember that anyproblem can be made worse with an indiscriminateintervention.
REFERENCES
1. Ryu RK. Arthroscopic subacromial decompression: A clinicalreview.Arthroscopy1992;8:141-147.
2. Stephens SR, Warren RF, Payne LZ, et al. Arthroscopic acro-mioplasty: A 6-10 year follow-up.Arthroscopy1998;14:382-388.
3. Ogilvie-Harris DJ, Wiley AM, Sattarian J. Failed acromio-plasty for impingement syndrome.J Bone Joint Surg Br1990;72:1070-1072.
4. Ellman H. Arthroscopic subacromial decompression: analysisof one to three year results.Arthroscopy1987;3:173-181.
5. Esch JC, Ozerkis LR, Helgager JA, et al. Arthroscopic sub-acromial decompression: results according to the degree ofrotator cuff tear.Arthroscopy1988;4:241-249.
6. Tibone J, Jobe F, Kerlan R. Shoulder impingement syndromein athletes treated by an anterior acromioplasty.Clin OrthopRel Res1985;198:134-140.
7. Altcheck D, Warren R, Wickiewicz T. Arthroscopic acromio-plasty: Techniques and results.J Bone Joint Surg Am1990;72:1198-1207.
8. Hawkins RJ, Chris T, Bokor D. Failed anterior acromioplasty:a review of 51 cases.Clin Orthop 1989;243:106-111.
9. Rockwood CA, Lyons FR. Shoulder impingement syndrome:diagnosis, radiographic evaluation and treatment with a mod-ified Neer acromioplasty.J Bone Joint Surg Am1993;74:409-424.
10. Walch G, Boileau P, Renaud E, et al. Impingement of the deepsurface of the supraspinatus tendon on the posterosuperiorglenoid rim: An orthopaedic study.J Shoulder Elbow Surg1992;1:238-245.
11. Ryu RK. Internal impingement: an overview. Presented at 18th
annual meeting San Diego Shoulder Arthroscopy, Arthroplastyand Fractures, San Diego, CA. June 20-23, 2001.
12. Paley K, Jobe FW, Pink MM, et al. Arthroscopic findings inthe overhand throwing athlete: Evidence for posterior internalimpingement of the rotator cuff.Arthroscopy2000;16:35-40.
13. Hutchinson MR, Veenstra MA. Arthroscopic decompressionof shoulder impingement secondary to os acromiale.Arthros-copy1993;9:28-32.
14. Ryu RK, Fan RS, Dunbar WH. The treatment of symptomaticos acromiale.Orthopaedics1999;22:3:325-328.
15. Warner JP, Beim GM, Higgins L. The treatment of symptom-atic os acromiale.J Bone Joint Surg Am1998;80:1320-1326.
16. Wolf E. Os acromiale: Always excise/My experience. Pre-sented at Shoulder Surgery Controversies 2000, Laguna Hills,CA, October 2000.
17. Wright RW, Heller MA, Quick DC, et al. Arthroscopic de-compression for impingement syndrome secondary to an un-stable os acromiale.Arthroscopy2000;16:595-599.
18. Ticker JB, Beim GM, Warner JP. Recognition and treatmentof refractory posterior capsule contracture of the shoulder.Arthroscopy2000;16:27-34.
19. Flugstad D, Matsen FA, Larry I, Jackins SE. Failed acromio-plasty etiology and prevention.Orthop Trans1986;10:299(abstr).
20. Hawkins RJ, Saddemi SR, Mor JT. Analysis of failed arthro-scopic subacromial decompression.Arthroscopy1991;7:315-316 (abstr).
21. Matthews LS, Burkhead WZ, Gordon S, et al. Acromial frac-ture: a complication of arthroscopic subacromial decompres-sion.J Shoulder Elbow Surg1994;3:256-261.
22. Bonell S. Detached deltoid during arthroscopic subacromialdecompression.Arthroscopy2000;16:745-748.
23. Sampson TD, Nisbet JK, Glick JM. Precision acromioplastyin arthroscopic subacromial decompression of the shoulder.Arthroscopy1991;7:301-307.
24. Burkhart SS. A stepwise approach to arthroscopic rotator cuffrepair based on biomechanical principles.Arthroscopy2000;16:82-90.
25. Ryu RK. Arthroscopic management of massive rotator cufftears.Arthroscopy1994;10:334 (abstr).
26. Backer M, Cordasco FA, Craig EV, et al. Arthroscopic sub-acromial decompression and debridement for partial thicknessrotator cuff tears: A clinical outcome study. Presented at 20th
Annual Meeting, Arthroscopy Association of North America,Seattle, Washington, April 2001.
27. Weber SC. Arthroscopic debridement and acromioplasty ver-sus mini-open repair in the management of significant partialthickness tears of the rotator cuff.Orthop Clin North Am1997;28:79-82.
28. Ogilvie-Harris DJ, Wiley AM. Arthroscopic surgery of theshoulder.J Bone Joint Surg Br1986;68:201-207.
29. Ellman H. Diagnosis and treatment of incomplete rotator cufftears.Clin Orthop Rel Res1990;254:64-74.
30. Yamaguchi K, Connor PM, Pollock RG, et al. Surgical treat-ment for failed anterior acromioplasties: A comparison ofarthroscopic and open revision decompression.Arthroscopy1996;12;355 (abstr).
31. Mormino MA, Gross RM, McCarthy JA. Captured shoulder: acomplication of rotator cuff surgery.Arthroscopy1996;12:457-461.
32. Rodosky MW, Kennick JA, Vangura A, et al. Effect of acro-mioplasty and distal clavicle resection in acromioclavicularjoint mechanics.Arthroscopy2000;16:435 (abstr).
33. Kharrazi D, Glousman R, Tibone J, et al. Re-operation on theacromioclavicular joint following arthroscopic subacromialdecompression.Arthroscopy2000;16:435 (abstr).
34. Barber FA. To co-plane or not to co-plane: how does theremaining A-C joint respond?Arthroscopy 2000;16:436(abstr).
35. Hazel M, Tosto JP, Klassen J. Arthroscopic subacromial de-compression: A 9 year follow-up.Arthroscopy1999: Vol 15ISAKOS Supplement 1;58 (abstr).
CORACOACROMIAL ARCHINSUFFICIENCY
Stephen S. Burkhart, M.D.,and Peter M. Parten, M.D.
Coracoacromial arch insufficiency can cause a tre-mendous amount of dysfunction in the shoulder,
and is extremely difficult to treat surgically. Unfortu-nately, it is not well understood and this lack ofunderstanding has caused treatment options to developin several disparate directions. In exploring this prob-lem, we will attempt to define the problem by definingthe underlying cause, the anatomic deficit, the me-chanical problem, and the dysfunction. Then we willlook at the various means of treatment, as well assome of the unanswered questions.
54 R.K.N. RYU ET AL.
Defining the Problem
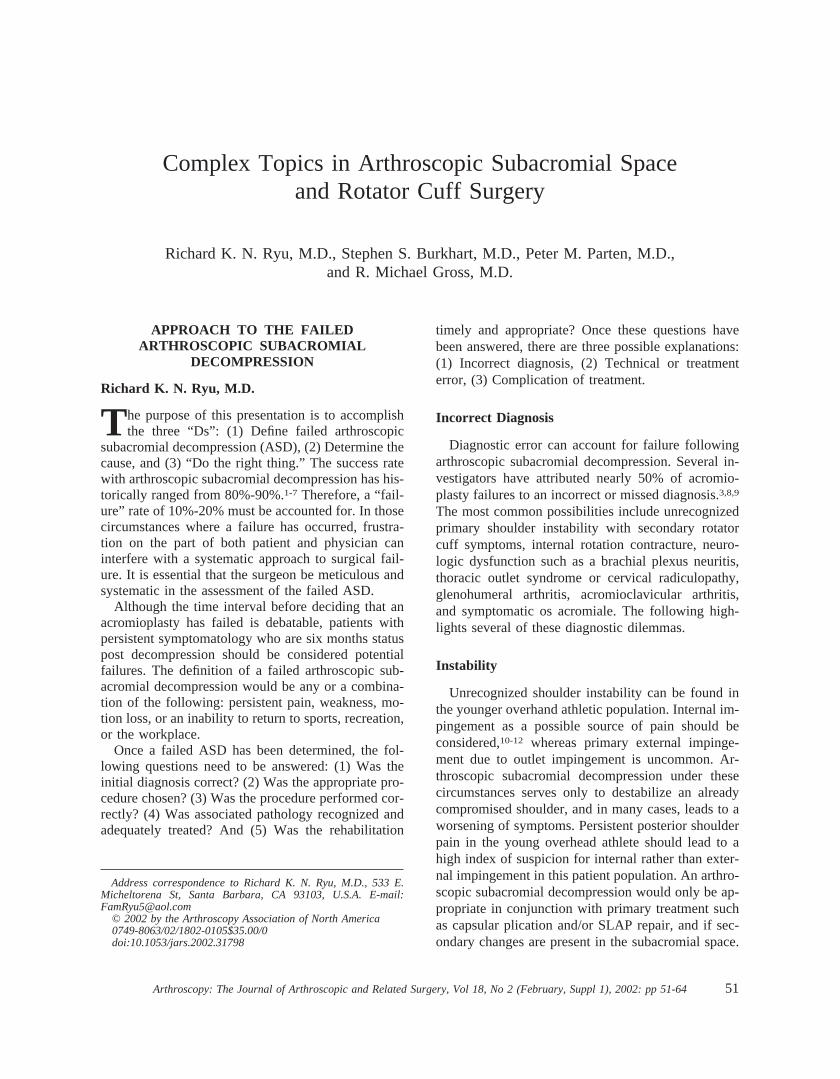
Patients with coracoacromial arch insufficiencyhave generally had previous shoulder surgery in whichan acromioplasty has been done along with excision ofthe coracoacromial ligament, in the face of proximalmigration of the humerus. This allows the humerus tomigrate beneath the anterior deltoid, the last remain-ing constraint of the coracoacromial arch. Frequently,in patients that have deltoid detachment, or in patientswith very small muscle mass, the humeral head willappear to be directly under the skin (Fig 1).
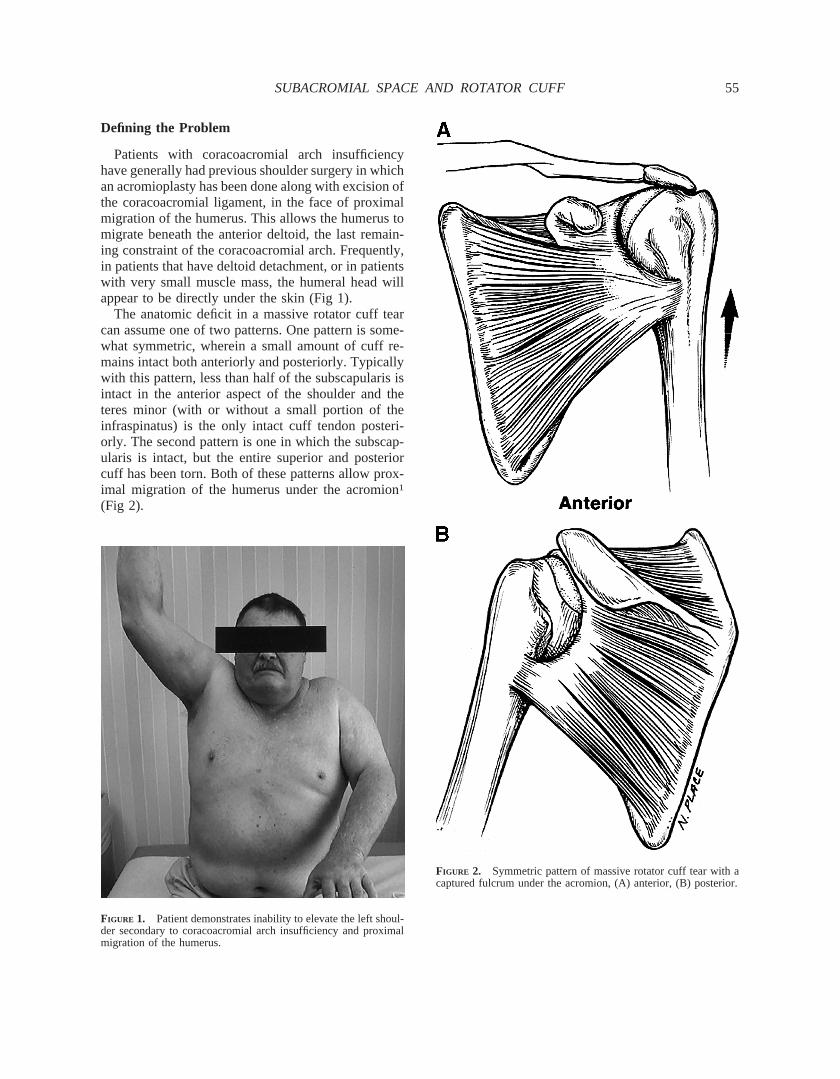
The anatomic deficit in a massive rotator cuff tearcan assume one of two patterns. One pattern is some-what symmetric, wherein a small amount of cuff re-mains intact both anteriorly and posteriorly. Typicallywith this pattern, less than half of the subscapularis isintact in the anterior aspect of the shoulder and theteres minor (with or without a small portion of theinfraspinatus) is the only intact cuff tendon posteri-orly. The second pattern is one in which the subscap-ularis is intact, but the entire superior and posteriorcuff has been torn. Both of these patterns allow prox-imal migration of the humerus under the acromion1
(Fig 2).
FIGURE 1. Patient demonstrates inability to elevate the left shoul-der secondary to coracoacromial arch insufficiency and proximalmigration of the humerus.
FIGURE 2. Symmetric pattern of massive rotator cuff tear with acaptured fulcrum under the acromion, (A) anterior, (B) posterior.
55SUBACROMIAL SPACE AND ROTATOR CUFF
The mechanical deficit relates to a loss of balancedforce couples in the shoulder. The force couple in thetransverse plane is lost (Fig 3). In the coronal plane,the inferior portion of the cuff is not adequate tocounterbalance the deltoid so that proximal migrationoccurs1-4 (Fig 4).
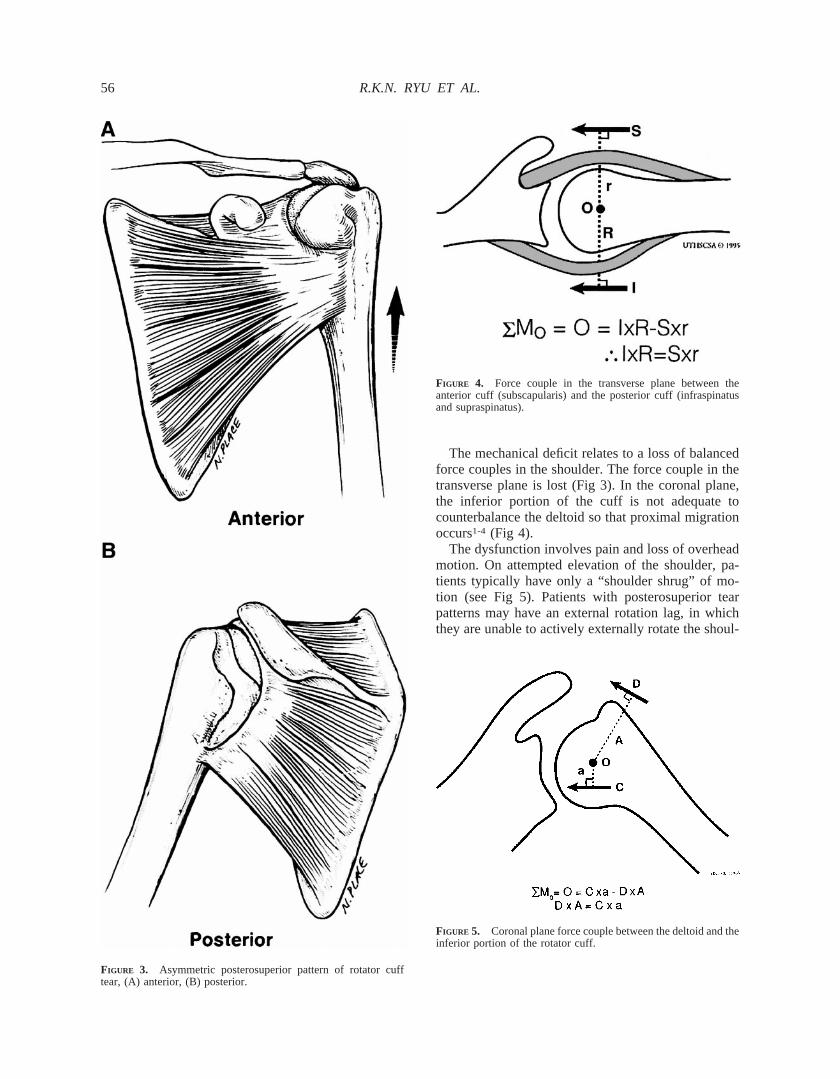
The dysfunction involves pain and loss of overheadmotion. On attempted elevation of the shoulder, pa-tients typically have only a “shoulder shrug” of mo-tion (see Fig 5). Patients with posterosuperior tearpatterns may have an external rotation lag, in whichthey are unable to actively externally rotate the shoul-
FIGURE 3. Asymmetric posterosuperior pattern of rotator cufftear, (A) anterior, (B) posterior.
FIGURE 4. Force couple in the transverse plane between theanterior cuff (subscapularis) and the posterior cuff (infraspinatusand supraspinatus).
FIGURE 5. Coronal plane force couple between the deltoid and theinferior portion of the rotator cuff.
56 R.K.N. RYU ET AL.
der to neutral (Fig 6). Those that have loss of sub-scapularis function will exhibit a positive Napoleontest5 (Fig 7).
Radiographically, the AP x-rays show proximal hu-meral migration (Fig 8). The MRI scan shows a mas-sive rotator cuff tear (Fig 9). Since we have found theMRI to be less reliable for subscapularis tears than forthe rest of the rotator cuff,5 the subscapularis may ormay not appear to be intact on MRI.
The Awning Effect
The senior author (S.S.B.) did a kinematic studyseveral years ago in which he observed an awning
FIGURE 6. External rotation lag sign of the left shoulder withattempted active external rotation.
FIGURE 7. Positive Napoleon sign indicates a nonfunctional sub-scapularis on the right shoulder. The patient can press on belly onlyby flexing the wrist 90 degrees, using the posterior deltoid ratherthan the subscapularis for this function.
FIGURE 8. AP radiograph shows proximal humeral migrationwith decreased acromiohumeral distance and incongruity of infe-rior articular margin of humerus and glenoid.
FIGURE 9. Coronal plane MRI of massive rotator cuff tear.
57SUBACROMIAL SPACE AND ROTATOR CUFF
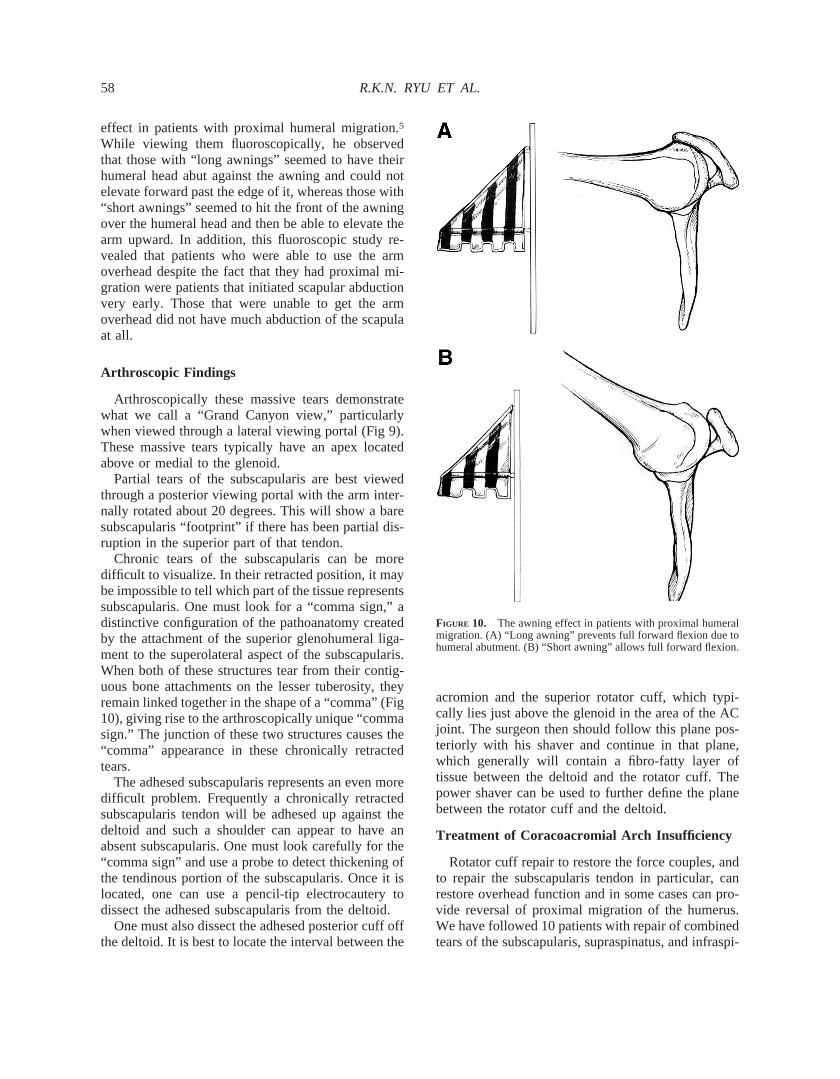
effect in patients with proximal humeral migration.5
While viewing them fluoroscopically, he observedthat those with “long awnings” seemed to have theirhumeral head abut against the awning and could notelevate forward past the edge of it, whereas those with“short awnings” seemed to hit the front of the awningover the humeral head and then be able to elevate thearm upward. In addition, this fluoroscopic study re-vealed that patients who were able to use the armoverhead despite the fact that they had proximal mi-gration were patients that initiated scapular abductionvery early. Those that were unable to get the armoverhead did not have much abduction of the scapulaat all.
Arthroscopic Findings
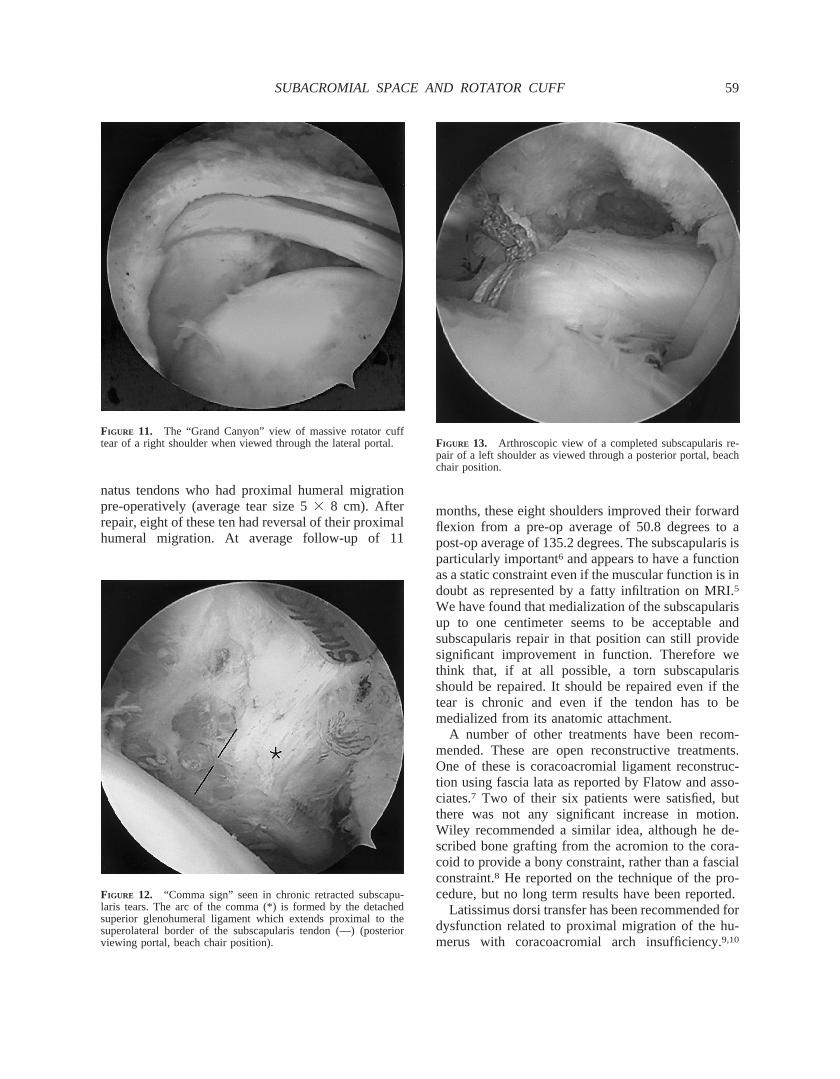
Arthroscopically these massive tears demonstratewhat we call a “Grand Canyon view,” particularlywhen viewed through a lateral viewing portal (Fig 9).These massive tears typically have an apex locatedabove or medial to the glenoid.
Partial tears of the subscapularis are best viewedthrough a posterior viewing portal with the arm inter-nally rotated about 20 degrees. This will show a baresubscapularis “footprint” if there has been partial dis-ruption in the superior part of that tendon.
Chronic tears of the subscapularis can be moredifficult to visualize. In their retracted position, it maybe impossible to tell which part of the tissue representssubscapularis. One must look for a “comma sign,” adistinctive configuration of the pathoanatomy createdby the attachment of the superior glenohumeral liga-ment to the superolateral aspect of the subscapularis.When both of these structures tear from their contig-uous bone attachments on the lesser tuberosity, theyremain linked together in the shape of a “comma” (Fig10), giving rise to the arthroscopically unique “commasign.” The junction of these two structures causes the“comma” appearance in these chronically retractedtears.
The adhesed subscapularis represents an even moredifficult problem. Frequently a chronically retractedsubscapularis tendon will be adhesed up against thedeltoid and such a shoulder can appear to have anabsent subscapularis. One must look carefully for the“comma sign” and use a probe to detect thickening ofthe tendinous portion of the subscapularis. Once it islocated, one can use a pencil-tip electrocautery todissect the adhesed subscapularis from the deltoid.
One must also dissect the adhesed posterior cuff offthe deltoid. It is best to locate the interval between the
acromion and the superior rotator cuff, which typi-cally lies just above the glenoid in the area of the ACjoint. The surgeon then should follow this plane pos-teriorly with his shaver and continue in that plane,which generally will contain a fibro-fatty layer oftissue between the deltoid and the rotator cuff. Thepower shaver can be used to further define the planebetween the rotator cuff and the deltoid.
Treatment of Coracoacromial Arch Insufficiency
Rotator cuff repair to restore the force couples, andto repair the subscapularis tendon in particular, canrestore overhead function and in some cases can pro-vide reversal of proximal migration of the humerus.We have followed 10 patients with repair of combinedtears of the subscapularis, supraspinatus, and infraspi-
FIGURE 10. The awning effect in patients with proximal humeralmigration. (A) “Long awning” prevents full forward flexion due tohumeral abutment. (B) “Short awning” allows full forward flexion.
58 R.K.N. RYU ET AL.
natus tendons who had proximal humeral migrationpre-operatively (average tear size 53 8 cm). Afterrepair, eight of these ten had reversal of their proximalhumeral migration. At average follow-up of 11
months, these eight shoulders improved their forwardflexion from a pre-op average of 50.8 degrees to apost-op average of 135.2 degrees. The subscapularis isparticularly important6 and appears to have a functionas a static constraint even if the muscular function is indoubt as represented by a fatty infiltration on MRI.5
We have found that medialization of the subscapularisup to one centimeter seems to be acceptable andsubscapularis repair in that position can still providesignificant improvement in function. Therefore wethink that, if at all possible, a torn subscapularisshould be repaired. It should be repaired even if thetear is chronic and even if the tendon has to bemedialized from its anatomic attachment.
A number of other treatments have been recom-mended. These are open reconstructive treatments.One of these is coracoacromial ligament reconstruc-tion using fascia lata as reported by Flatow and asso-ciates.7 Two of their six patients were satisfied, butthere was not any significant increase in motion.Wiley recommended a similar idea, although he de-scribed bone grafting from the acromion to the cora-coid to provide a bony constraint, rather than a fascialconstraint.8 He reported on the technique of the pro-cedure, but no long term results have been reported.
Latissimus dorsi transfer has been recommended fordysfunction related to proximal migration of the hu-merus with coracoacromial arch insufficiency.9,10
FIGURE 11. The “Grand Canyon” view of massive rotator cufftear of a right shoulder when viewed through the lateral portal.
FIGURE 12. “Comma sign” seen in chronic retracted subscapu-laris tears. The arc of the comma (*) is formed by the detachedsuperior glenohumeral ligament which extends proximal to thesuperolateral border of the subscapularis tendon (—) (posteriorviewing portal, beach chair position).
FIGURE 13. Arthroscopic view of a completed subscapularis re-pair of a left shoulder as viewed through a posterior portal, beachchair position.
59SUBACROMIAL SPACE AND ROTATOR CUFF

Miniaci and associates reported on 17 patients.9 Theystated that their patients’ average flexion improvedfrom 42 degrees to 101 degrees and that their UCLAscores improved from 6.8 to 16.4. Hennigan et al.reported on 14 patients in which the ASES scoreimproved from 39.5 to 65.9.10 They postulated a te-nodesis affect.
Wirth and Rockwood described a pectoralis majortransfer that was superficial to the conjoined tendon.11
Concerns about the direction of pull of the transferredtendon resulted in subcoracoid placement of the pec-toralis major transfer as described by Resch and as-sociates.12 Galatz et al. also have reported using thistransfer.13 They favor it because they feel that thedirection of pull helps to limit proximal migration andthat the coracoid base acts as a pulley, optimizing thedirection of muscle contraction. In their 17 patients,flexion improved from 37 degrees to 72 degrees. Wil-liams and Iannotti described iliotibial band graft re-construction in the front of the shoulder for subscap-ularis insufficiency.14 They felt that there was abeneficial tenodesis effect, even though they did notrestore any muscular function. Forward flexion im-proved from 42 degrees to 105 degrees. Hemiarthro-plasty has been recommended for treatment of a pain-ful shoulder with proximal humeral migration andcoracoacromial arch insufficiency. Cofield et al. re-ported pain relief in 75 percent, but stated that motionwas not improved in these patients.15
Finally, as a last resort, one might consider gleno-humeral arthrodesis as a solution to this very difficultproblem.
Conclusions
1. Coracoacromial arch insufficiency is a very dif-ficult problem to treat, and prevention is the bestmeans of treatment. This requires meticulousrotator cuff repair in patients that do not haveproximal humeral migration.
2. In patients with proximal humeral migration,repair of chronic subscapularis tears in associa-tion with repair of the rest of the cuff can some-times result in reversal proximal humeral migra-tion.
3. Static tenodesis (for example with ITB graft)has reported results with better function thanpectoralis major transfer, and approximatelyequivalent to latissimus dorsi transfer.
4. Hemi-arthroplasty should be done for pain reliefonly.
5. Arthrodesis should be considered as a last re-sort.
6. The tenodesis effect in place of subscapularismuscle function may be a mechanism of im-proving function, by restoring the force couplein the transverse plane. The big unknown is therole of the awning effect in enhancing or dimin-ishing overhead function.
REFERENCES
1. Burkhart SS. Fluoroscopic comparisons of kinematic patternsin massive rotator cuff tears: A suspension bridge model.ClinOrthop 1992;284:144-152.
2. Burkhart SS. Arthroscopic debridement and decompression forselected rotator cuff tears. Clinical results, pathomechanics,and patient selection based on biomechanical parameters.Or-thop Clin North Am1993;24:111-123.
3. Burkhart SS. Arthroscopic treatment of massive rotator cufftears. Clinical results and biomechanical rationale.Clin Or-thop 1991;267:45-46.
4. Burkhart SS. Reconciling the paradox of rotator cuff repair vs.debridement: A unified biomechanical rationale for the treat-ment of rotator cuff tears.Arthroscopy1994;10:1-16.
5. Burkhart SS, Tehrany AM. Arthroscopic subscapularis tendonrepair: Technique and preliminary results.Arthroscopy (inpress).
6. Warner JJP, Higgins L, Parsons IM IV, et al. Diagnosis andtreatment of anterosuperior rotator cuff tears.J Shoulder andElbow Surg2001;10:37-46.
7. Flatow EL, Connor PM, Levine WM, et al. Coracoacromialarch reconstruction for anterosuperior subluxation after failedrotator cuff surgery: A preliminary report (abstract).J Shoul-der and Elbow Surg6:228.
8. Wiley AM. Superior humeral dislocation: A complication fol-lowing decompression and debridement for rotator cuff tears.Clin Orthop 1991;263:135-141.
9. Miniaci A, MacLeod M. Transfer of the latissimus dorsi mus-cle after failed repair of a massive tear of the rotator cuff.J Bone Joint Surg1999;81A:1120-1127.
10. Hennigan SP, Ramsey ML, Herzog R, et al. Latissimus dorsitransfer for irreparable rotator cuff tears: Clinical, anatomicand electromyographic results. Presented at the 17th AnnualMeeting of the American Shoulder and Elbow Surgeons. SanFrancisco, CA. March 3, 2001.
11. Wirth MA, Rockwood CA. Operative treatment of irreparablerupture of the subscapularis.J Bone Joint Surg Am1997;79(5):722-731.
12. Resch H, Povacz P, Ritter E, Matschi W. Transfer of thepectoralis major muscle for the treatment of irreparable ruptureof the subscapularis tendon.J Bone Joint Surg Am2000;82(3):372-382.
13. Galatz LM, Connor PM, Calfee R, et al. Results of subcora-coid pectoralis major transfer for the treatment of anterosupe-rior shoulder instability. Presented at the 17th Annual Meetingof the American Shoulder and Elbow Surgeons. San Francisco,CA. March 3, 2001.
14. Ianotti JP, Antoniou J, Williams GR, et al. Iliotibial band graftreconstruction for treatment of glenohumeral instability asso-ciated with irreparable subscapularis tears and capsular defi-ciency. Presented at the 17th Annual Meeting of the AmericanShoulder and Elbow Surgeons. San Francisco, CA. March 3,2001.
15. Sanchez-Sotelo J, Cofield RH, Rowland CS. Shoulder hemi-arthroplasty for rotator cuff tear arthropathy. Presented at the17th Annual Meeting of the American Shoulder and ElbowSurgeons. San Francisco, CA. March 3, 2001.
60 R.K.N. RYU ET AL.

GLENOHUMERAL INSTABILITY ANDROTATOR CUFF DYSFUNCTION
R. Michael Gross, M.D.
Glenohumeral instability and rotator cuff tears ap-pear to be unrelated, but that is often not the case
to joint destruction. In fact, instability and rotator cuffdisorders are acutely interrelated with one frequentlydirectly contributing to and/or causing the other todevelop. It is important to understand the mechanicsof the normal anatomy and how damage of either theligaments and/or the rotator cuff can lead to pathologywithin related structures.
The Vacuum Phenomena
Peter Helmi et al. demonstrated the loss of shoulderstability in the unloaded state simply by puncturingthe capsule thus releasing the vacuum. This studynoted that with the loss of the vacuum, the humerusexhibited marked increased laxity on both the AP aswell as the superior inferior plane. Habermeyer et al.noted that traction on a normal shoulder leads to anincreased negative pressure while this increase wasnot noted in a shoulder with a Bankart lesion. One canonly assume that the same effect would be seen witha full thickness rotator cuff tear.
Conformity Compression Principle
Stephen Lippitt et al. have introduced the confor-mity compression principle. It states that the confor-mity of the G/H joint coupled with the compressiveload from the rotator cuff stabilizes the shoulder. Withthe labrum intact, the humeral head resists a tangentialforce of up to 60 percent of the compression loadacross the joint. Resection of the glenoid labrum (aswith a Bankart injury) drops the resistance force by 40percent.
Capsular Structures
The capsular structures are the main passive stabi-lizers of the glenohumeral joint. The superior gleno-humeral ligament stabilizes the shoulder from inferiorsubluxation while the arm is at 0 degrees of abduction,and from posterior subluxation while it is flex 90degrees and internally rotated. O’Brien et al. studiedthe inferior glenohumeral ligament and described athree-part structure: an anterior and posterior bandwith the axillary pouch being supported between thesetwo bands. In abduction and external rotation, theanterior band prevents anterior translation of the hu-
meral head while the posterior band rotates inferior tothe humeral head, and supports the abducted arm frominferior glide. The opposite happens while the shoul-der is in abduction and internal rotation.
Stephen Howell et al. studied humeral motion onthe transverse plane. Howell’s group found a consis-tent 4-mm posterior translation of the abducted hu-meral head as it reached full external rotation. Thisphenomenon is lost in an unstable shoulder. Usingselective nerve blocks Howell isolated the cause ofthis “roll back” phenomenon to the capsular struc-tures.
The Rotator Cuff
Hsu et al. at the Mayo Clinic studied the effect ofdamage to the rotator cuff on the stability of theglenohumeral joint. Hsu et al. found that tears in thecritical zone had a greater effect on the inferior sta-bility of the joint, while those located in the rotatorinterval had a greater affect on the anterior stability ofthe joint. The size of the tear had a greater effect whenit was located in the rotator interval than in the criticalzone.
From this understanding of the static and dynamicstabilizers of the joint, one can separate 4 pathologicalconditions or groups that occur when the static, thedynamic, or both components are deficient: Groups Iand II, external and internal impingement in the over-head athlete; group III, Primary anterior dislocation inthe older patient is frequently; and group IV, Rotatorcuff tear arthropathy.
EXTERNAL IMPINGEMENT AND THEOVERHEAD ATHLETE
In the mid-’80s, Tibone and Jobe discussed thefrustration of treating impingement pain in the youngoverhead athlete with a decompression. While Tiboneand Jobe reported excellent pain relief in this popula-tion, unfortunately only 46 percent were able to returnto their pre-entry-level of activity, and only 25 percentwith capsular laxity or labral pathology did so. Tiboneand Jobe’s work identified the concept of mild insta-bility leading to and presenting as an impingementproblem.
Clinical Presentation
Pain is the presenting complaint with all of thesepatients. Few if any have a sense of instability. Theclassic impingement sign of Neer and Hawkins isalmost always positive. The apprehension sign is pain-
61SUBACROMIAL SPACE AND ROTATOR CUFF

ful but not apprehensive. The Jobe relocation test isoften positive and an asymmetrical positivesulcussign is occasionally present.
Treatment
Treatment always begins with rest, anti-inflamma-tory medications, and oftentimes a cortical steroidinjection into the subacromial bursa. The goal of thisinitial treatment is to break the cycle of pain/inflam-mation with the bursa and rotator cuff tendons toallow the patient an opportunity to rehabilitate effec-tively. The entire shoulder musculature, including thescapula stabilizers, must be rehabilitated. Tight poste-rior capsular structures need to be stretched. If surgeryis necessary, it begins with an examination underanesthesia and arthroscopy. Evidence of instabilitycan be subtle. The arthroscopic examination mustinclude the bursa. If the bursal tissue is hypertrophied,it must be cleaned out. The bursal side of the rotatorcuff and the coricoacromio ligament must be evalu-ated. If no damage is found, decompression is notjustified. Partial tears of the rotator cuff, bursal orarticular, in a young individual usually require repair.The instability problem needs to be dealt with in afashion that will return the athlete to full strength, fullmotion, and normal function. As Tibone and his as-sociates discovered, pain relief and mobility alone arenot adequate measures of recovery. Bankart lesionsmust be repaired, and stretched ligaments should beplicated. Jobe has emphasized that the plane of plica-tion should be superior to inferior without disruptionof the subscapularis muscle. His results were excel-lent: 92% good or excellent. Jobe’s goal was fullmotion by 3 months and full sporting activities at 6months. The temptation is to try to reproduce theseresults arthroscopically with a Bankart repair to re-store the anatomy and plication of the capsule or morecommonly thermal energy to achieve the same goal.Although this is possible, failure rates with this ap-proach are worrisome.
INTERNAL IMPINGEMENT
This syndrome presents as a painful shoulder inan overhead athlete. Initially the symptoms arevague and present only during sports, but as theproblem progresses pain can become constant andeven disturb sleep. The clinical examination wasspelled out clearly in a paper by Kevin Paley et al.Fifteen percent A/C joint pain, 26 percent positiveNeer or Hawkins sign, 62 percent evidence of subtle
glenohumeral instability as indicated by a positiverelocation test, and 63 percent a painful apprehensiontest. Morgan and Burkhart specifically noted an aver-age of 25 degrees decrease in internal rotation on theaffected side.
Anatomy
Both arthroscopic findings as well as laboratorydissections have indicated that contact between theposterior superior labrum and the rotator cuff is bothcommon and physiological. Helbrecht used a gadolin-ium enhanced MRI in a study comparing throwing andnon-throwing shoulders. He noted that abnormalitiesof rotator cuff and superior labrum could be seen incompletely asymptomatic throwing shoulders. His re-sults led him to caution against treating the youngoverhead athlete on MRI findings alone.
Arthroscopic Findings
The arthroscopic findings in internal impingementcan include any of the following: 1) damage to theposterior superior labrum, 2) damage to the rotatorcuff, 3) damage to the posterior humeral head in thearea of the insertion of the supraspinatus tendon, and4) damage to the anterior glenoid labrum and/or infe-rior glenohumeral ligament. In addition, Jobe wouldadd a normal or near normal subacromial bursa.
Pathology
The difficulty in dealing with internal impingementcomes in the strong differences of opinion as to thepathomechanics of the problem. Morgan and Burkhartare adamant that the problem starts and ends posteri-orly. They described the pathology as starting with atight posterior capsule leading to a posterior superiorshift of the G/H rotation point, which results in a“peeling off ” of the posterior superior glenoid labrumwhich results in what they term as “pseudo-laxity.” Ifconservative measures fail, their logical treatment isfirst a course of posterior capsular stretching followedby arthroscopy and repair of the posterior type IISLAP. Many physicians, notably Walch, have notfound instability (pseudo or otherwise) to be associ-ated with this disorder and often find damage but notavulsion or peeling off of the posterior labrum.
C. Jobe described the problem of internal impinge-ment as an excess of external rotation leading toposterior impingement and overload of the posteriorlabrum and rotator cuff. Jobe recommended that phys-ical therapy should include exercises that strengthenthe rotator cuff muscles and the scapula stabilizers as
62 R.K.N. RYU ET AL.

well as coordination exercises. He also suggested thatif conservative measures fail, surgery should consistof an examination of anesthesia, an arthroscopic ex-amination, debridement or repair of the rotator cuff asindicated, and anterior capsular labral stabilization ifnecessary.
Conclusion
This topic was featured inArthroscopy “PointCounterpoint.” The discussion was presented as ifthere were one answer for this disorder. That may notbe the case. There may be different pathological prob-lems, which present with similar symptoms and ar-throscopic findings. It seems as if the most predictableapproach is for the surgeon to understand that thesymptoms that present as internal impingement canhave any of a number of disorders, including a type IISLAP, anterior capsular labral abnormalities, and ro-tator cuff damage, as the major disorders. Each mustbe dealt with as the situation presents.
PRIMARY ANTERIOR SHOULDERDISLOCATION IN THE OLDER PATIENT
The third circumstance that emphasizes the relation-ship between glenohumeral instability and the rotatorcuff is found in the patient who is.40 years of agewhen he/she suffers a primary anterior shoulder dis-location. In their review of 500 primary anteriorshoulder dislocations, Rowe and Sakellarider pointedout that the frequency of a primary dislocation is ascommon for those over the age of 45 years as it is forindividuals under 45. In this study, they said that whilethe recurrent rate was much greater in the youngerpatient, complications were both more frequent andmore severe in the older patient. The 3 complicationsthat seemed to increase with age are: 1) fracture of thegreater tuberosity or glenoid, 2) axillary nerve injury,and 3) rotator cuff tear. The third complication is themost pertinent to this discussion. Many have recog-nized the association of rotator cuff tear with a pri-mary dislocation in an older patient. Frequency of30-90% has been reported in this age group.
Robert and Tom Neviaser reported on 12 patientswith recurrent instability following a dislocation thatoccurred after the age of 40. In the 11 patients whowere suffering from anterior recurrent instability, thesurgical findings revealed an isolated subscapularstear associated with an avulsion of the capsular liga-ments from humerus (HAGL). In a separate study,Robert, Tom, and Jules Neviaser reported on 31 older
patients who were unable to abduct the involved armafter a primary dislocation. All were found to have arotator cuff tear. In each case, the patient was pre-sumed to have an axillary nerve injury, yet only 4 ofthe 20 EMGs done to document the injury confirmedthat the axillary nerve was injured. Berbig et al. offerthe same caution: “if the patient is unable to elevatethe affected arm. 90 degrees in plane of the scapulatwo weeks after a dislocation there should be a highsuspicion of rotator cuff tear.”
The conclusions that one can draw from these are:
1. The combination of a rotator cuff tear with aprimary dislocation in a patient over 40 is com-mon.
2. Patients who do not recover quickly (within 3weeks), especially in terms of active abduction,should be evaluated for a rotator cuff tear.
3. Subscapularis tears and capsular avulsion fromthe lesser tuberosity seem to be disproportion-ately common in terms of surgical findings.
4. In a patient suffering from the combination ofrecurrent instability along with a torn rotatorcuff, satisfactory surgical results can only beobtained if both problems are dealt with.
ROTATOR CUFF TEARARTHROPATHY (RCTA)
This disorder was described 140 years ago by Smithand Adams. It wasn’t mentioned again until Codmandescribed it in his 1934 monograph on shoulder dis-orders. He looked at the problem as the end result ofuntreated rotator cuff disease. RCTA was not men-tioned again until the 1960s. Then over the next 20years it was rediscovered and renamed on severaloccasions. Finally in 1983 Dr. Neer et al. gave it thename that has stuck: rotator cuff tear arthropathy.
Pathology
While the index injury for this disorder seems to bea rotator cuff tear, only a small percent (4%) of agroup of patients whom Dr. Neer followed over an8-year period developed rotator cuff arthropathy. Thecommon denominator does not seem to be the size ofthe tear so much as the loss of balance in the trans-verse and coronal plane of the force couples, gener-ated by the rotator cuff. Dr Neer postulated that onlythe tears that progressed to the loss of the primary andsecondary stabilizers of the shoulder joint would de-velop RCTA.
This is an odd disorder that progresses in an oppo-
63SUBACROMIAL SPACE AND ROTATOR CUFF

site fashion as rheumatoid arthritis. It begins as adegenerative arthritis and ends as an inflammatoryarthritis. The inflammation is the result of a reaction tocalcium phosphate crystals in the synovium and sy-novial fluid. These crystals cause a low grade inflam-matory reaction by the synovial tissue, which inducesthe synovium to synthesize proteolytic enzymes thatare responsible for the degradation of collagen mate-rial, causing damage to both the articular cartilage andthe rotator cuff.
Treatment
Although the discussion of rotator cuff arthropathyis beyond the scope of this presentation, it is importantto recognize the shoulder in which the force coupleshave been “unlinked,” or as Dr. Burkhart refers to it“biomechanically unstable.” If the shoulder is biome-chanically unstable, poor treatment decisions will onlyaccelerate the process. Decompression without restor-ing biomechanical stability to the rotator cuff fre-quently makes matters worse. Repair or replacementwithout decompression are far safer routes to take.The key to successful treatment is the recognition thatthe primary and secondary stabilizers of the shoulderjoint along with the rotator cuff need attention.
ANNOTATED REFERENCES
1. Tibone JE, Jobe FW, Kerlan RK, et al. Shoulder impingementsyndrome in athletes treated by an anterior acromioplasty.ClinOrthop 1985;198:134-140.
This is one of the first papers to identify that impingementpain in an overhead athlete may be a more complex problemthan in an older nonathletic individual. They report an 89percent improvement in the symptoms of pain but only 43percent of their patients were able to return to their preoper-ative athletic level. Within that group of athletes, no swim-mers recovered to their pre-injury level and only 22 percent ofthe baseball pitchers and throwers recovered.
2. Rubenstein DL, Jobe FW, Glousman RE, et al. Anterior capsu-lolabral reconstruction of the shoulder in athletes.J ShoulderElbow Surg1992;1:229-237.
Jobe et al. relate that most instability operations are morepredictable in terms of restoring stability than in terms ofmaintaining full external rotation. This becomes pertinentwith the overhead athlete. The goal of the capsular labralreconstruction is to offer a safe, predictable, reproduciblesurgical procedure that offers stability as well as maintains afull range of motion. His surgical procedure does not violatethe subscapularis insertion and tightens the capsular structures
primarily on a superior to inferior direction. The results of 76patients at an average of 39 months postoperative were: 96percent satisfied with procedure, 93 percent return to preop-erative athletic level. The average loss of external rotation at90 degrees of abduction was 2 degrees while the loss ofabduction was 1 degree.
3. Barber FA, Morgan CD, Burkhart SS, et al. Labrum-biceps-cuffdysfunction in the throwing athlete.Arthroscopy1999;15:852-857.
This article focuses on the pathomechanics of internal im-pingement. Two differing views are featured. Chris and FrankJobe both favor anterior laxity or increased external rotationas the primary abnormality that leads to internal impingement.Burkhart and Morgan favor a tight posterior capsule whichprevents normal external rotation and shifts the fulcrum ofrotation superioposterior to the insertion of the biceps tendoncausing a “peel back” injury of the biceps insertion into theposterior labrum. They indicate that the instability is “pseudo-laxity” and will disappear with repair of the SLAP injury.Since both authors have been successful in treating this prob-lem, yet with differing approaches, it leaves room for thepossibility that the single problem may have more than onepathomechanical pathway.
4. Neviaser RJ, Neviaser TJ. Recurrent instability of the shoulderafter age 40.J Shoulder Elbow Surg1995;4:416-418.
This is a report of 12 patients with recurrent instability fol-lowing their index dislocation, which occurred after the age of40 years. Eleven of the patients with anterior instability allhad a rupture of the subscapularis muscle as well as a humeralavulsion of the glenohumeral ligaments. The main messagefrom this article is that the pathology for recurrent dislocationsin this age group is frequently not the routine Bankart injuryas seen with younger individuals.
5. Jensen KL, Williams GR, Rockwood CA. Current conceptsreview—Rotator cuff tear arthropathy.J Bone Joint Surg Am1999;81a:1312-1324.
The authors describe a condition of the shoulder in which atear of the rotator cuff progresses in size and in location to thepoint where the force couples are disrupted and secondaryinstability ensues. The degenerative process, which resultsfrom this situation, creates basic calcium phosphate crystals,which cause an inflammatory condition that frequently resultsin severe bony deformity. This is a thorough overview ofrotator cuff tear arthropathy and would be an excellent articlefor any individual interested in a deeper understanding of thisdisorder.
6. Burkhart SS. Arthroscopic treatment of massive rotator cufftears. Clinical results and biomechanical rationale.Clin Orthop1991;267:45-56.
Burkhart emphasizes the importance of looking at the rotatorcuff as a three-dimensional structure. He emphasizes that thelength of a tear is not nearly as important as is its effect on“force couples.” The loss or the maintenance of force coupleson the frontal (deltoid balanced by the intact portion of therotator cuff), and the transverse plane (the subscapularis bal-anced by the infraspinatus and teres minor), will allow thesurgeon a better biomechanical view of the effect of a tear onthe shoulder. This paper offers a logical approach to assessand plan treatment for a rotator cuff tear.
64 R.K.N. RYU ET AL.
![Arthroscopic Subacromial Decompression for Small and ...nosis of the subacromial impingement is usually clinical and based on the provocative clinical tests [8] -[10] , but occasionally](https://img.pdfslide.us/doc/110x75/60c199bcd9b91479387e740d/arthroscopic-subacromial-decompression-for-small-and-nosis-of-the-subacromial.jpg)




























