Embed Size (px)
Citation preview
Complex Thoracoscopic Resections for Locally Advanced Lung Cancer
Thomas A. D’Amico MDGary Hock Professor of Surgery
Section Chief, Thoracic Surgery, Duke University Medical CenterChief Medical Officer, Duke Comprehensive Cancer Institute
Duke Thoracoscopic Lobectomy WorkshopMarch 21, 2018
Disclosure
• Consultant for Scanlan
• No conflicts related to this presentation
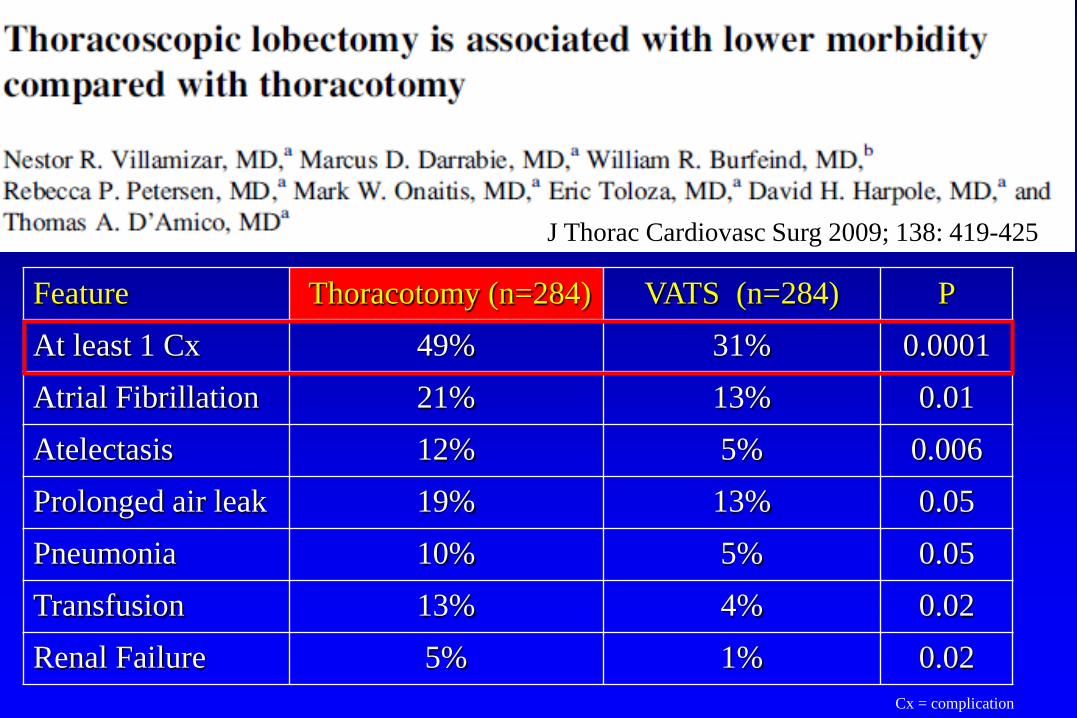
Thoracoscopic Lobectomy is Associated with Lower Morbidity Compared to ThoracotomyVillamizar N, et al. J Thorac Cardiovasc Surg
2009; 138: 419-425 J Thorac Cardiovasc Surg 2009; 138: 419-425
Feature Thoracotomy (n=284) VATS (n=284) PAt least 1 Cx 49% 31% 0.0001Atrial Fibrillation 21% 13% 0.01Atelectasis 12% 5% 0.006Prolonged air leak 19% 13% 0.05Pneumonia 10% 5% 0.05Transfusion 13% 4% 0.02Renal Failure 5% 1% 0.02
Cx = complication
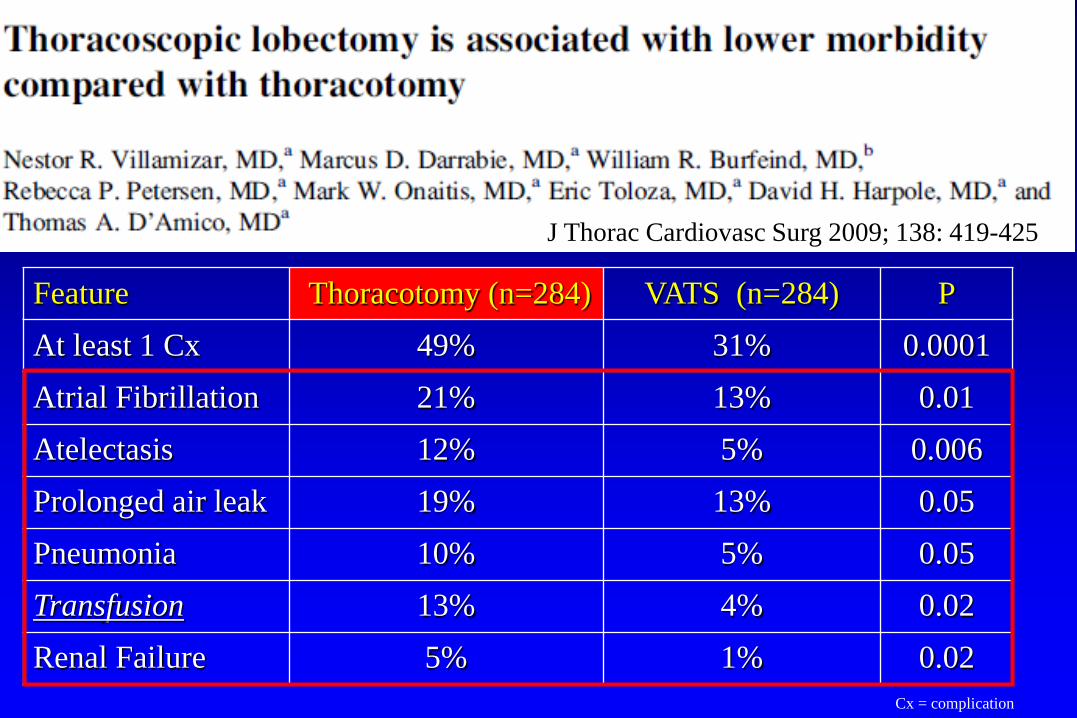
Thoracoscopic Lobectomy is Associated with Lower Morbidity Compared to ThoracotomyVillamizar N, et al. J Thorac Cardiovasc Surg
2009; 138: 419-425 J Thorac Cardiovasc Surg 2009; 138: 419-425
Feature Thoracotomy (n=284) VATS (n=284) PAt least 1 Cx 49% 31% 0.0001Atrial Fibrillation 21% 13% 0.01Atelectasis 12% 5% 0.006Prolonged air leak 19% 13% 0.05Pneumonia 10% 5% 0.05Transfusion 13% 4% 0.02Renal Failure 5% 1% 0.02
Cx = complication
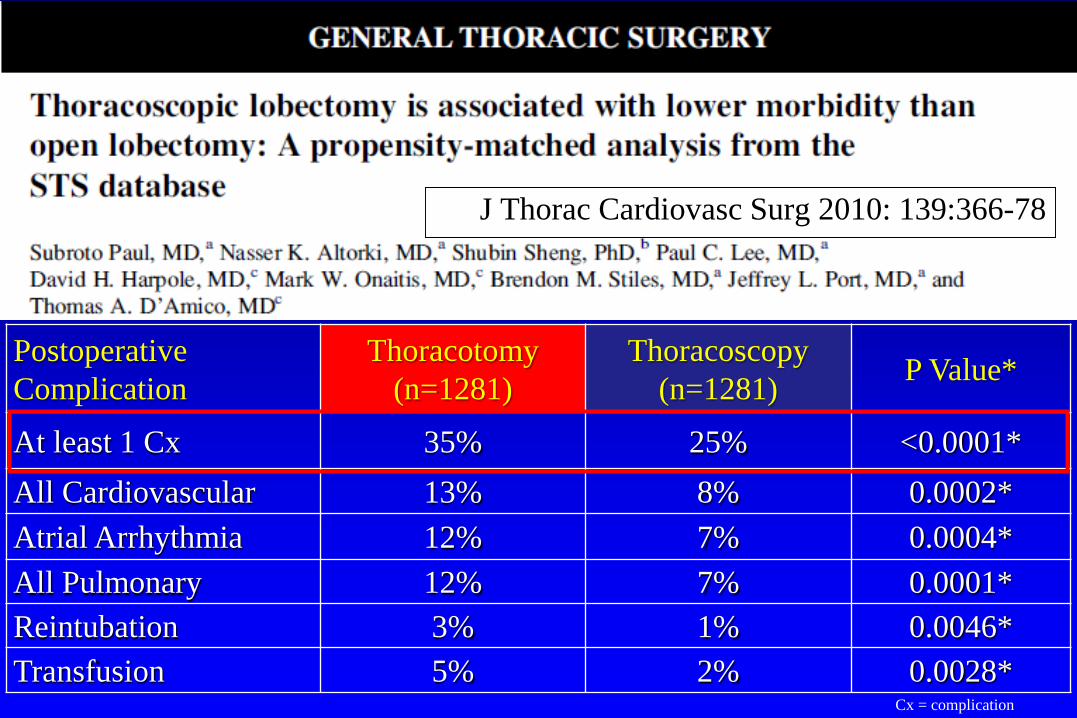
J Thorac Cardiovasc Surg 2010: 139:366-78
Postoperative Complication
Thoracotomy (n=1281)
Thoracoscopy (n=1281) P Value*
At least 1 Cx 35% 25% <0.0001*All Cardiovascular 13% 8% 0.0002*Atrial Arrhythmia 12% 7% 0.0004*All Pulmonary 12% 7% 0.0001*Reintubation 3% 1% 0.0046*Transfusion 5% 2% 0.0028*
Cx = complication
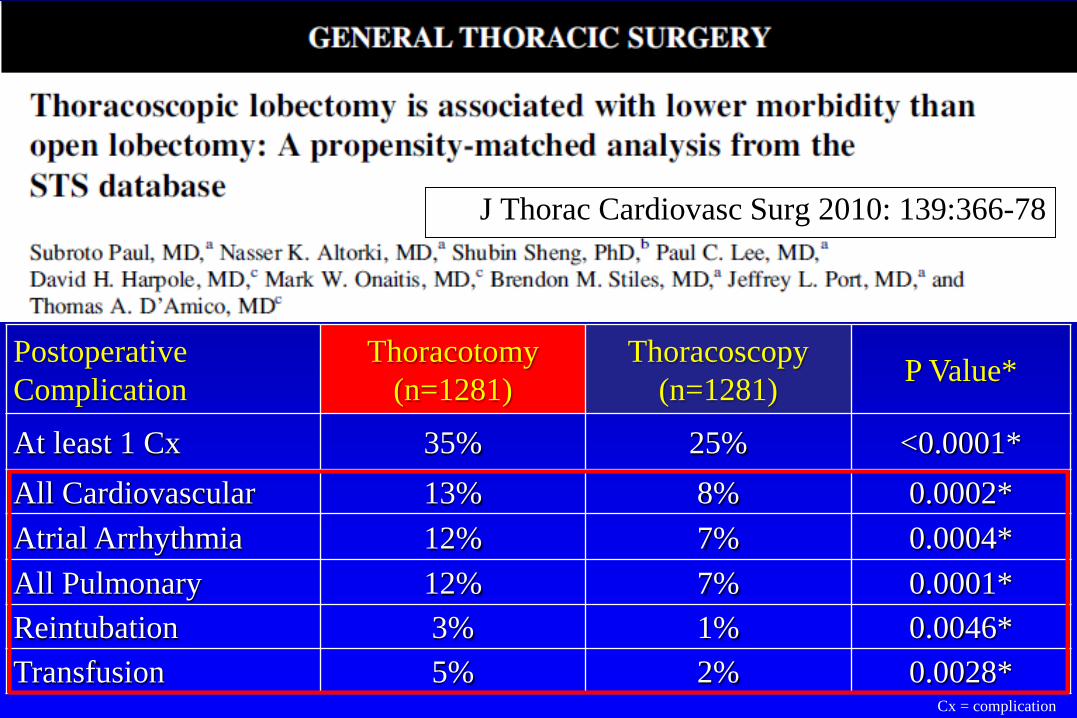
J Thorac Cardiovasc Surg 2010: 139:366-78
Postoperative Complication
Thoracotomy (n=1281)
Thoracoscopy (n=1281) P Value*
At least 1 Cx 35% 25% <0.0001*All Cardiovascular 13% 8% 0.0002*Atrial Arrhythmia 12% 7% 0.0004*All Pulmonary 12% 7% 0.0001*Reintubation 3% 1% 0.0046*Transfusion 5% 2% 0.0028*
Cx = complication
• Meta-analysis of 3 studies with propensity matching
• Villamizar N, et al. J Thorac Cardiovasc Surg 2009; 138: 419
• Paul S, et al et al. J Thorac Cardiovasc Surg: 2010; 139: 366
• Ilonen IK et al. Acta Oncologic 2011; 50: 1126
Ann Cardiothorac Surg 2012: 1: 16-23
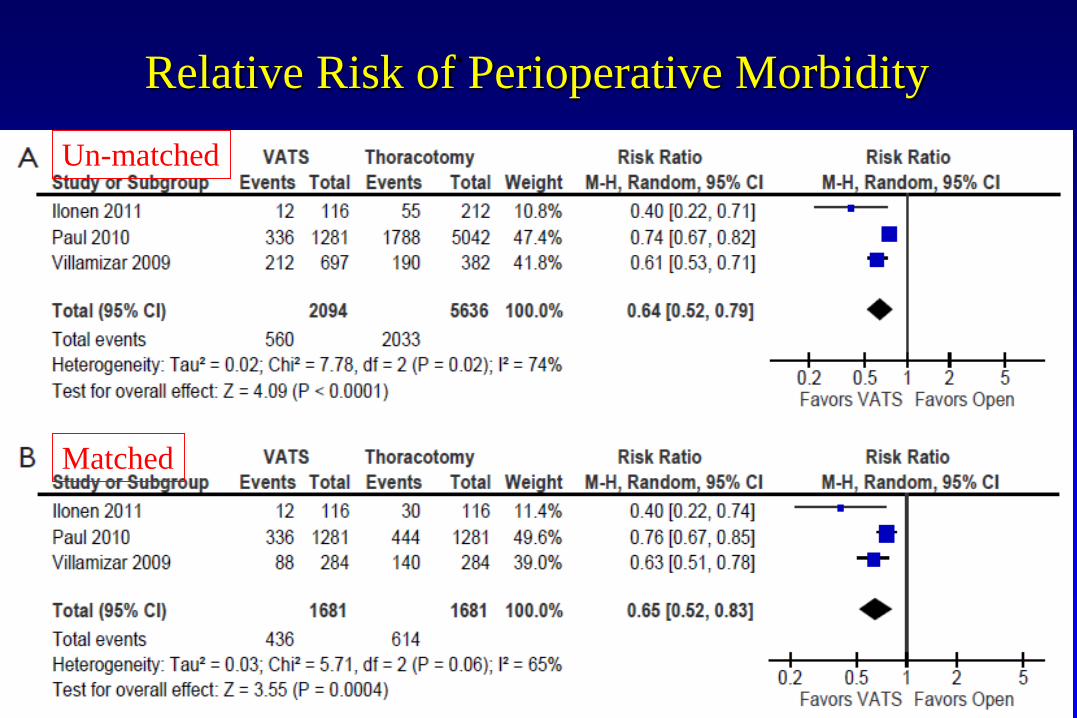
Relative Risk of Perioperative MorbidityUn-matched
Matched
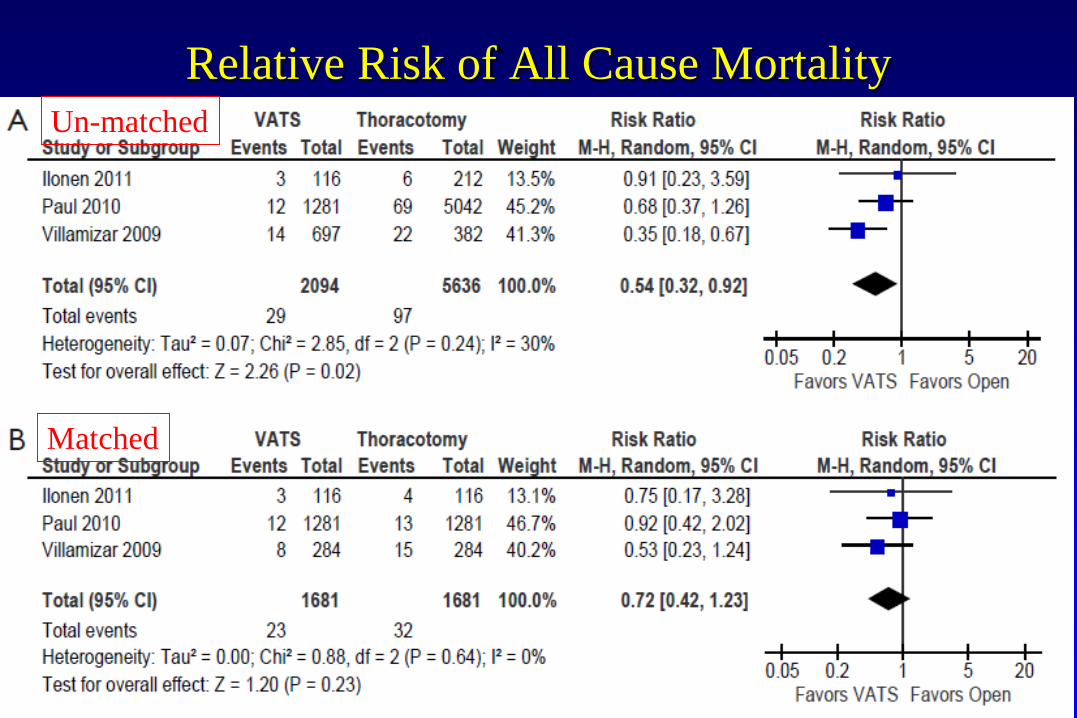
Relative Risk of All Cause MortalityUn-matched
Matched
A National Analysis of Long-term Survival Following Thoracoscopic vs Open Lobectomy for
Stage I Non-small Cell Lung Cancer
Chi-Fu Jeffrey Yang, Arvind Kumar, Jacob Klapper, Matthew Hartwig,Betty C. Tong, David Harpole, Mark Berry, Thomas A. D’Amico
Annals of Surgery (In Press)
A National Analysis of Long-term Survival Following Thoracoscopic vs Open Lobectomy for
Stage I Non-small Cell Lung Cancer• Outcomes of open vs VATS lobectomy for
clinical T1-2N0M0 NSCLC in the NCDB • 7,114: patients• Open; 5,566 (78%) VATS: 1,548 (22%) • Propensity-score matching resulted in 2 groups
of patients who were well-matched by 11 common prognostic co-variates
• 1,464 open and 1,464 VATS
A National Analysis of Long-term Survival Following Thoracoscopic vs Open Lobectomy for
Stage I Non-small Cell Lung Cancer• VATS approach was associated with a shorter
LOS (5 vs 6 d, p<0.001) and better 5-year survival (66.0% vs 62.5%, p=0.026)
• No differences in 30-day readmission rate or nodal upstaging
• Propensity-matched analysis: no significant differences in 5-year survival between the VATS and open groups (66.3% vs 65.8%, p=0.92)
Complex Thoracoscopic Resections
• Larger tumors, central tumors, N1• Lobectomy with chest wall resection• Sleeve resections
• Pneumonectomy• Lobectomy after induction therapy
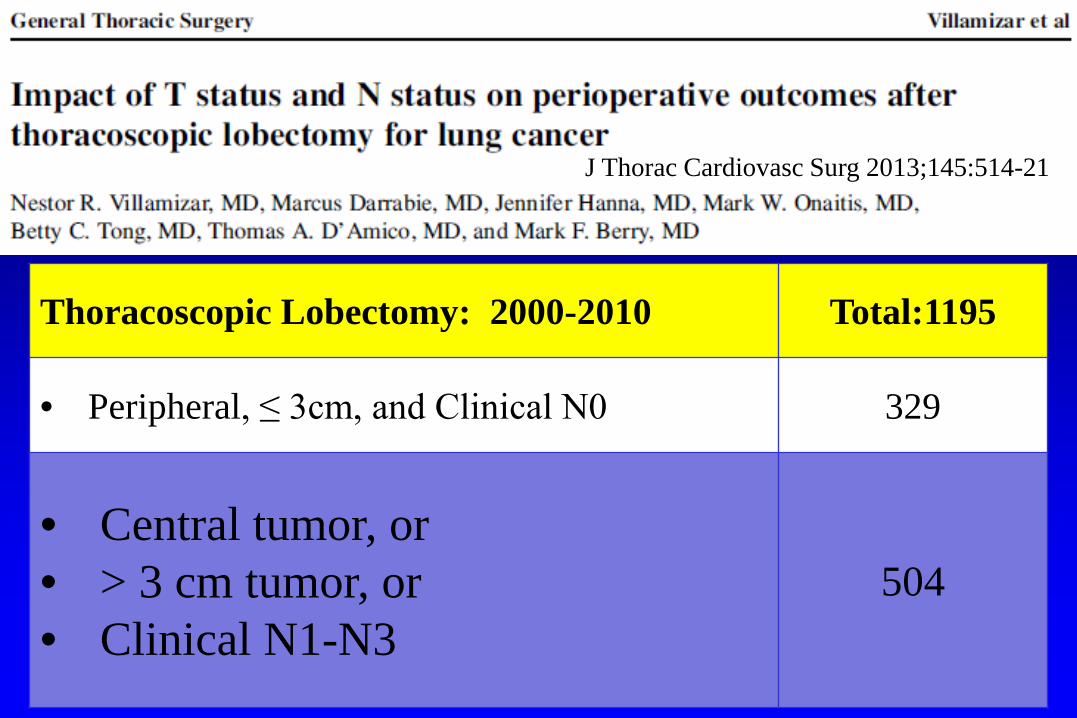
Impact of T Status and N Status on Outcomes after Thoracoscopic Lobectomy for Lung Cancer
J Thorac Cardiovasc Surg 2013;145:514-21
Thoracoscopic Lobectomy: 2000-2010 Total:1195
• Peripheral, ≤ 3cm, and Clinical N0 329
• Central tumor, or• > 3 cm tumor, or• Clinical N1-N3
504
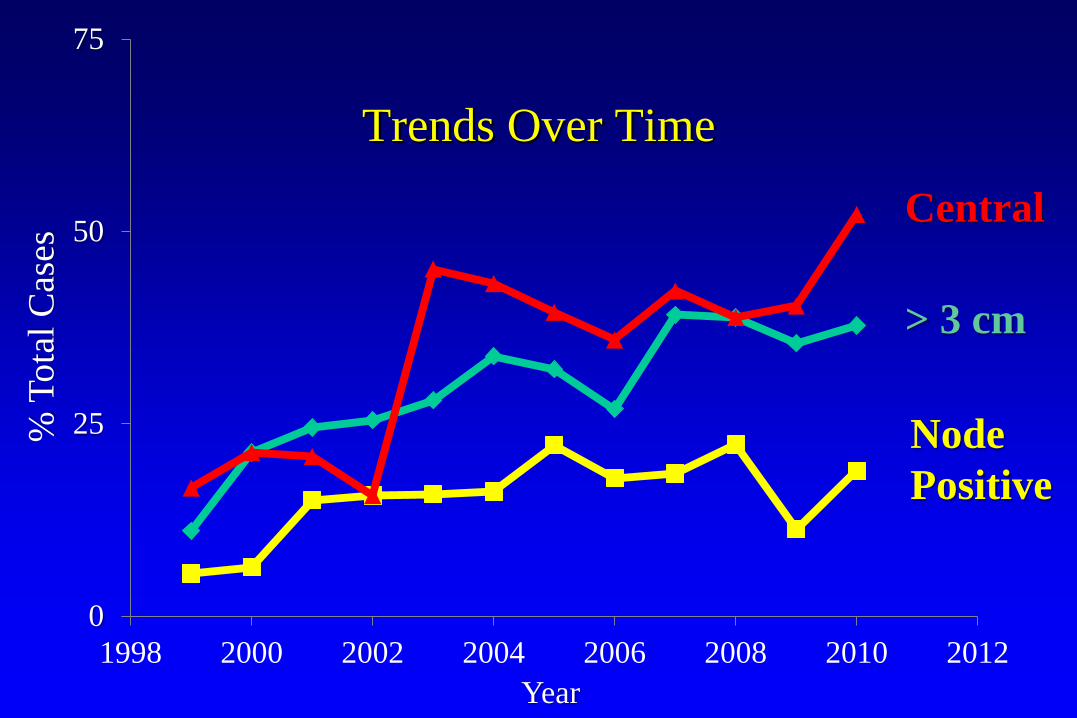
Year
% T
otal
Cas
es
0
25
50
75
1998 2000 2002 2004 2006 2008 2010 2012
Central
> 3 cm
Node Positive
Trends Over Time
Risk Factors for MorbidityComplications: incidence is not related to• Central location• Tumor size >3cm• Clinical node status
Conversions• Not higher for central tumors or for tumors > 3cm• Higher for clinically node positive disease
cN0 3.3% cN1-N3 7.2% p=0.03
Hybrid Approach to Chest Wall Tumors
• Thoracoscopic hilar dissection and ligation• Small counter incision centered over lesion• Chest wall resection and specimen removal • Advantages
– Smaller incision overall– Precise dissection– No rib spreading – No scapular retraction/rotation
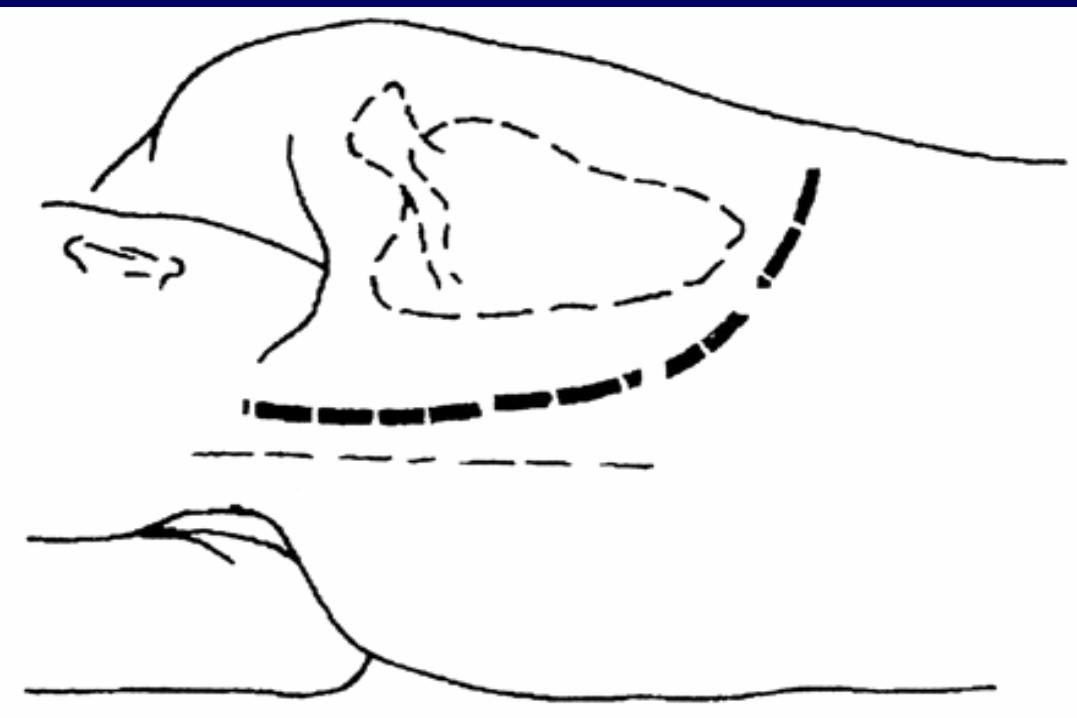
Posterior Approach
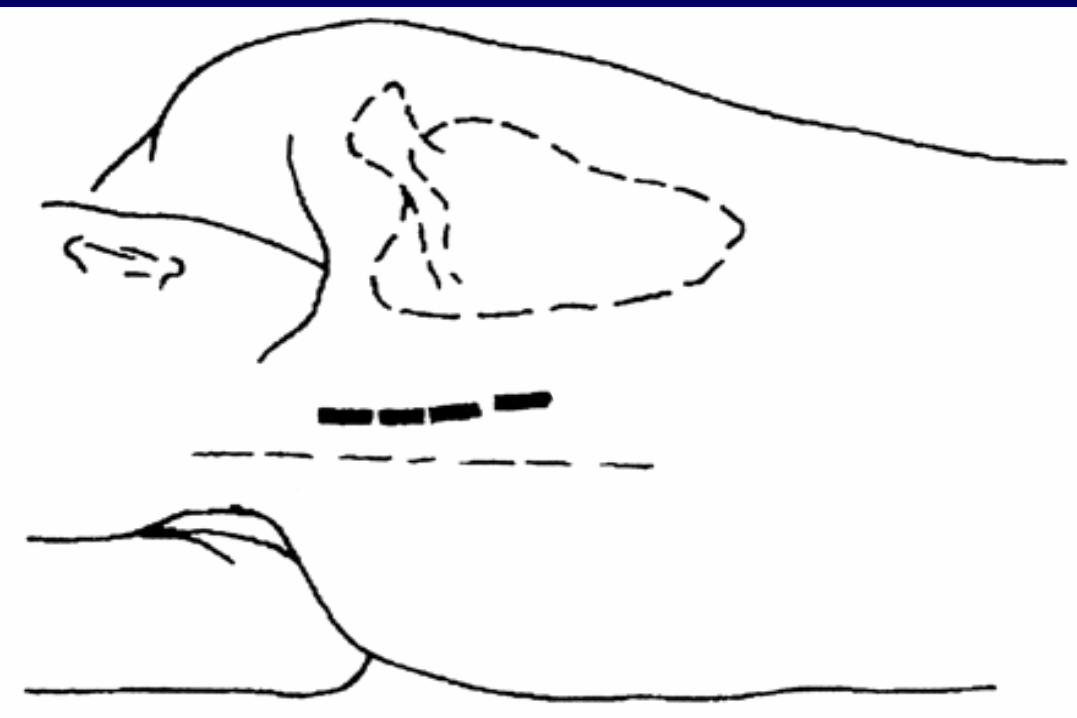
Posterior Approach
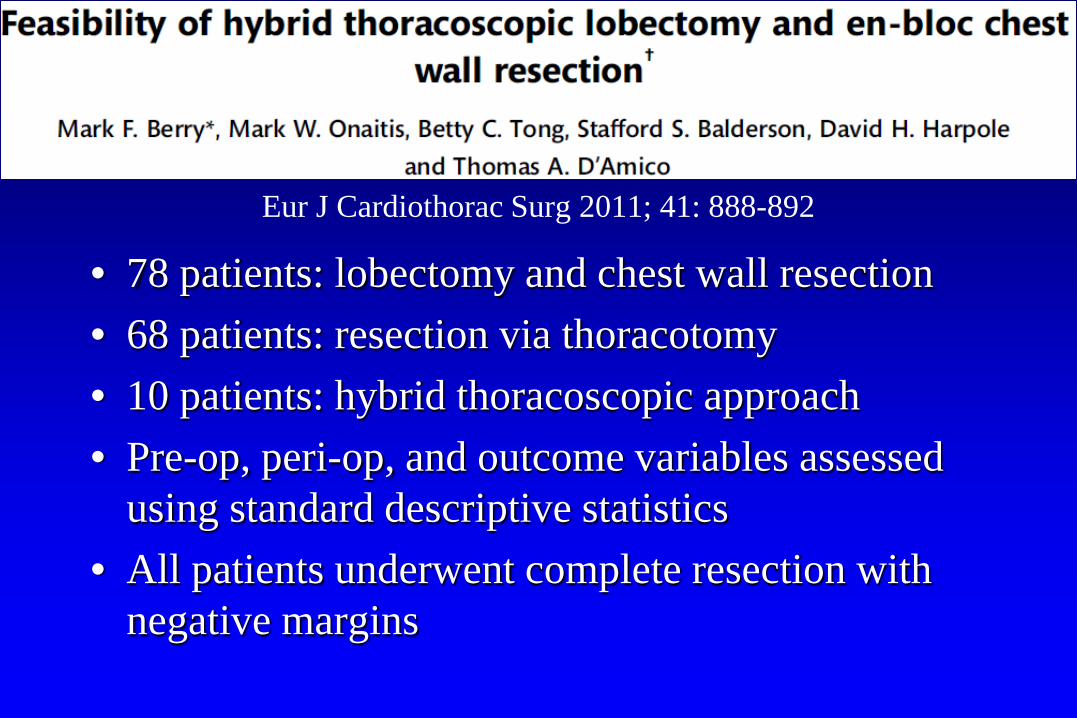
Feasibility Of Hybrid Thoracoscopic Lobectomy And En Bloc Chest Wall
ResectionEur J Cardiothorac Surg 2011; 41: 888-892
• 78 patients: lobectomy and chest wall resection• 68 patients: resection via thoracotomy• 10 patients: hybrid thoracoscopic approach• Pre-op, peri-op, and outcome variables assessed
using standard descriptive statistics• All patients underwent complete resection with
negative margins
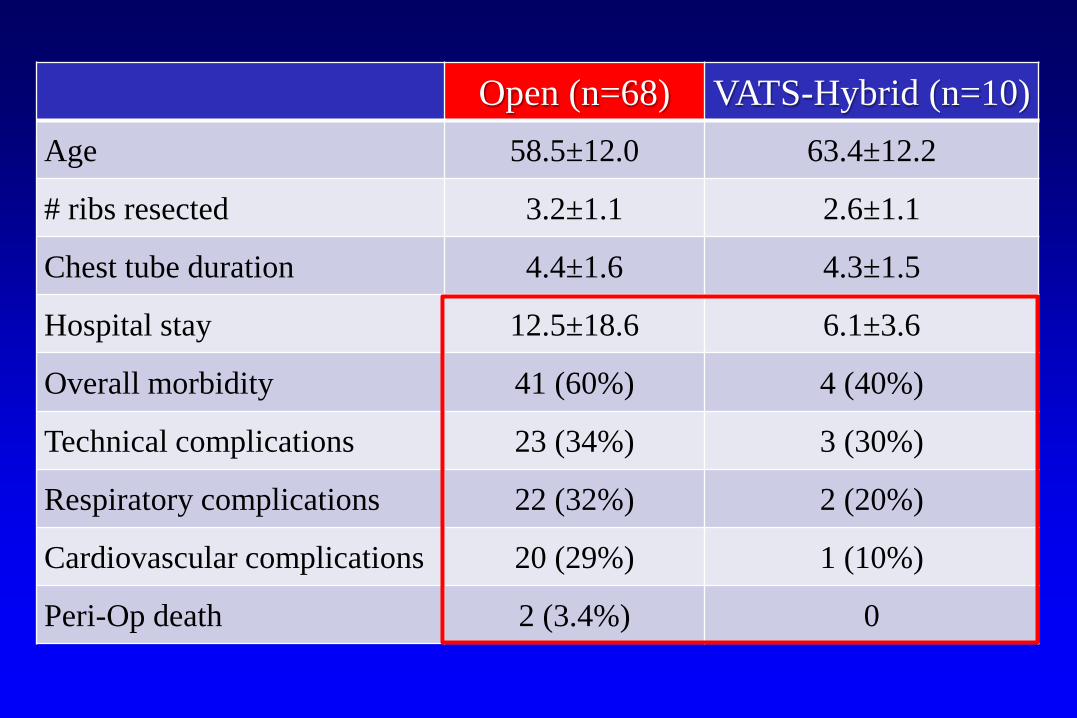
DataOpen (n=68) VATS-Hybrid (n=10)
Age 58.5±12.0 63.4±12.2
# ribs resected 3.2±1.1 2.6±1.1
Chest tube duration 4.4±1.6 4.3±1.5
Hospital stay 12.5±18.6 6.1±3.6
Overall morbidity 41 (60%) 4 (40%)
Technical complications 23 (34%) 3 (30%)
Respiratory complications 22 (32%) 2 (20%)
Cardiovascular complications 20 (29%) 1 (10%)
Peri-Op death 2 (3.4%) 0
Bronchoplastic Thoracoscopic Resections
• Safe, feasible, practiced by many surgeons • Reasonable to conclude that it is oncologically
equivalent to thoracotomy• Is likely associated with the same outcome
advantages as with thoracoscopic lobectomy, as compared to thoracotomy (not yet studied)
Performing Sleeve Lobectomy Instead of Pneumonectomy for Non-Small Lung Cancer with N1 Nodal Disease Does Not Compromise Long-
Term Survival
Mark F. Berry MD, Mathias Worni MD MHS, Xiaofei Wang PhD, David H. Harpole MD, Thomas A. D’Amico
MD, Mark W. Onaitis MD
Ann Thorac Surg 2013; 97: 230-235
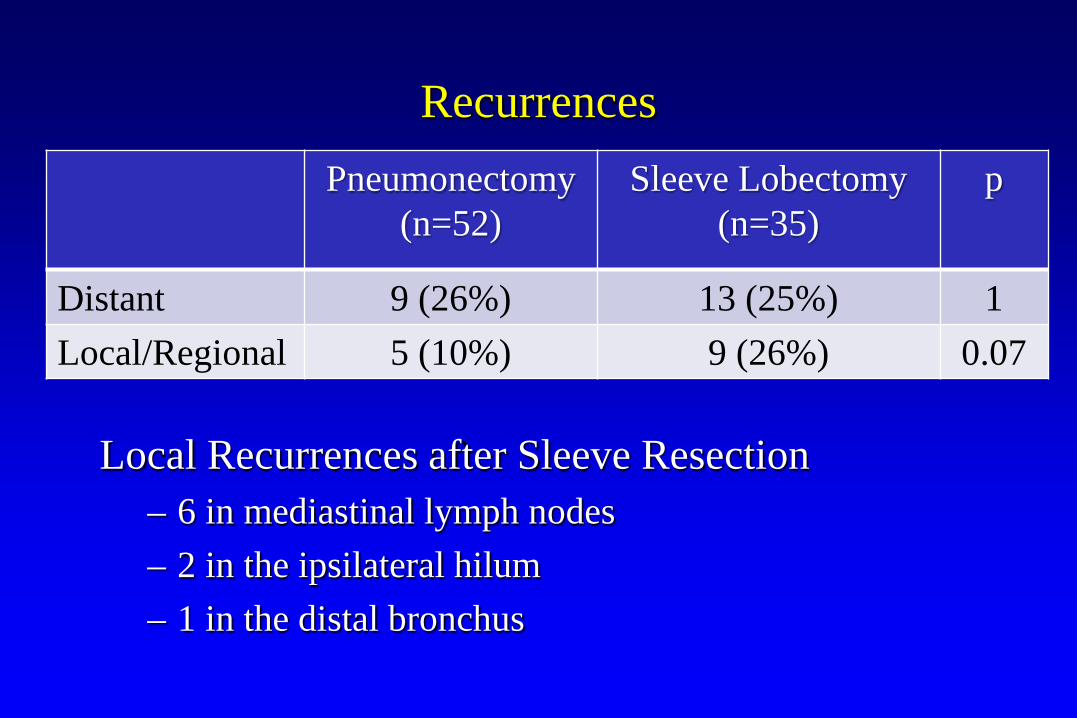
Recurrences
Local Recurrences after Sleeve Resection– 6 in mediastinal lymph nodes– 2 in the ipsilateral hilum– 1 in the distal bronchus
Pneumonectomy (n=52)
Sleeve Lobectomy (n=35)
p
Distant 9 (26%) 13 (25%) 1Local/Regional 5 (10%) 9 (26%) 0.07
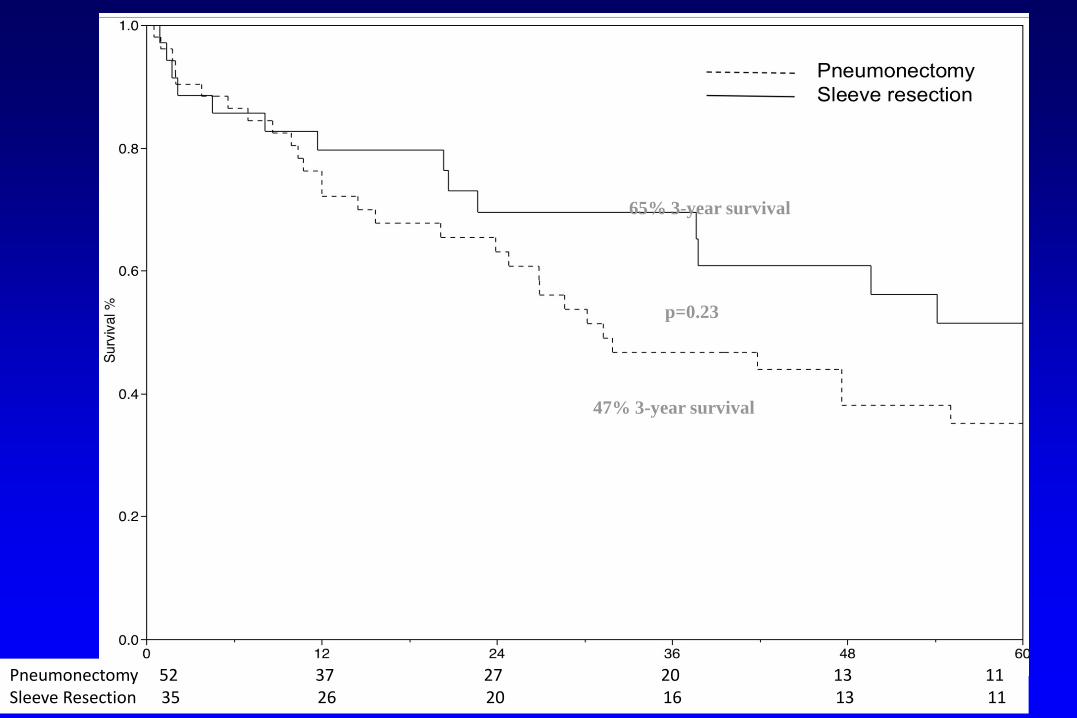
Pneumonectomy 52 37 27 20 13 11Sleeve Resection 35 26 20 16 13 11
65% 3-year survival
47% 3-year survival
p=0.23
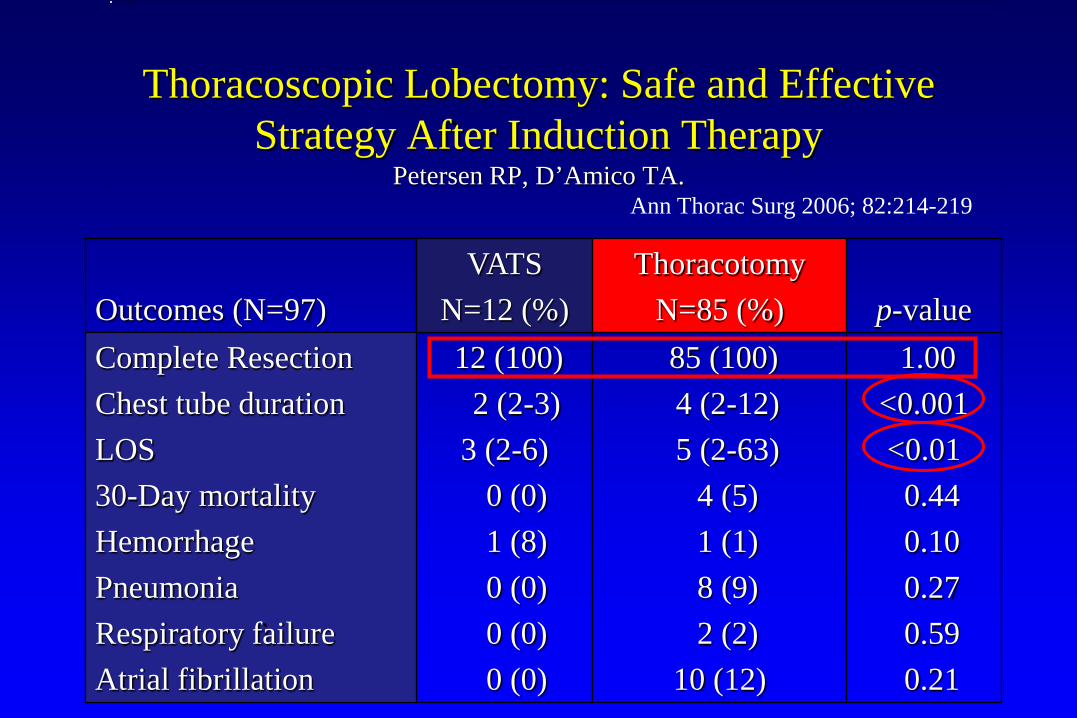
Thoracoscopic Lobectomy: Safe and Effective Strategy After Induction Therapy
Petersen RP, D’Amico TA.
Outcomes (N=97)VATS
N=12 (%)Thoracotomy
N=85 (%) p-valueComplete ResectionChest tube durationLOS30-Day mortalityHemorrhagePneumoniaRespiratory failureAtrial fibrillation
12 (100)2 (2-3)
3 (2-6)0 (0)1 (8)0 (0)0 (0)0 (0)
85 (100)4 (2-12)5 (2-63)
4 (5)1 (1)8 (9)2 (2)
10 (12)
1.00<0.001<0.01
0.440.100.270.590.21
The picture can't be displayed.
Ann Thorac Surg 2006; 82:214-219
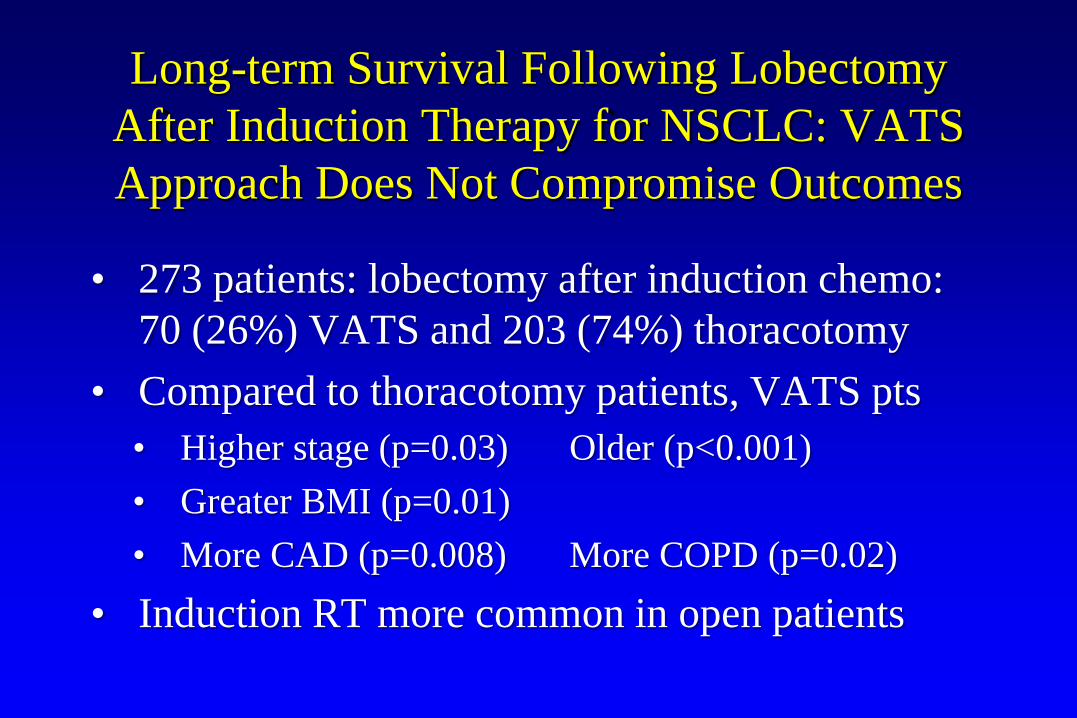
Long-term Survival Following Lobectomy After Induction Therapy for NSCLC: VATS Approach Does Not Compromise Outcomes
• 273 patients: lobectomy after induction chemo: 70 (26%) VATS and 203 (74%) thoracotomy
• Compared to thoracotomy patients, VATS pts• Higher stage (p=0.03) Older (p<0.001) • Greater BMI (p=0.01)• More CAD (p=0.008) More COPD (p=0.02)
• Induction RT more common in open patients
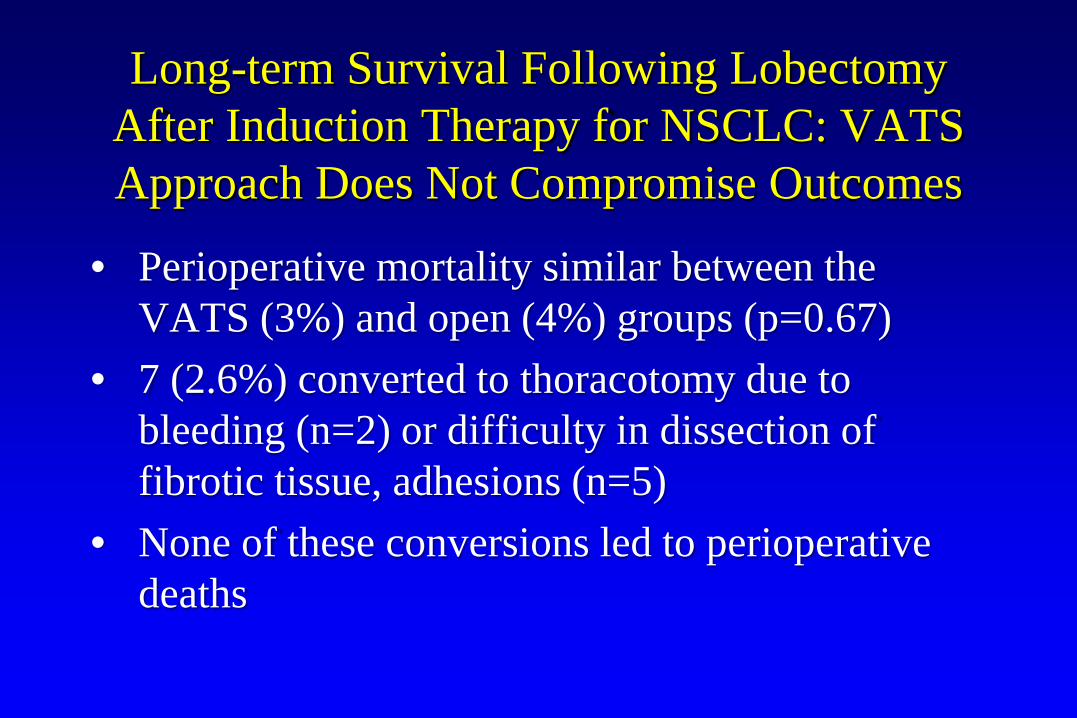
Long-term Survival Following Lobectomy After Induction Therapy for NSCLC: VATS Approach Does Not Compromise Outcomes
• Perioperative mortality similar between the VATS (3%) and open (4%) groups (p=0.67)
• 7 (2.6%) converted to thoracotomy due to bleeding (n=2) or difficulty in dissection of fibrotic tissue, adhesions (n=5)
• None of these conversions led to perioperative deaths
Lobectomy After Induction Therapy: VATS Approach Does Not Compromise Outcomes
• Univariate analysis: VATS patients had improved 3-year survival compared with thoracotomy (61% vs 43%; p=0.008)
• Multivariable analysis: VATS approach was associated with improved overall survival (p=0.04)
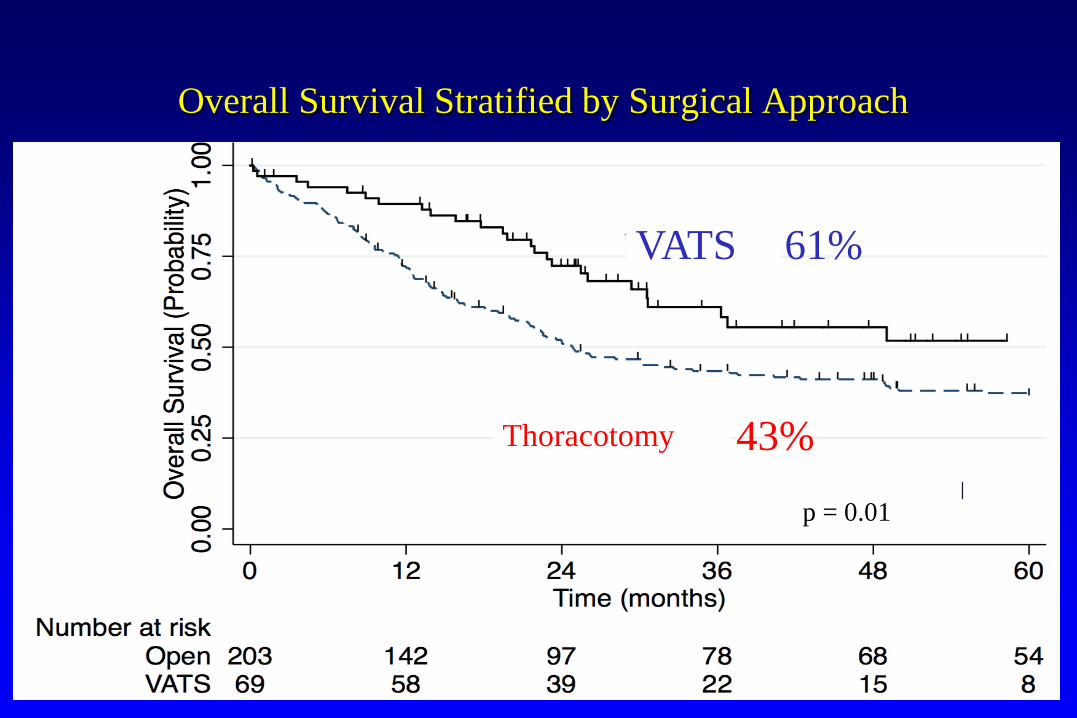
Overall Survival Stratified by Surgical Approach
Thoracotomy
VATS 61%
43%
p = 0.01
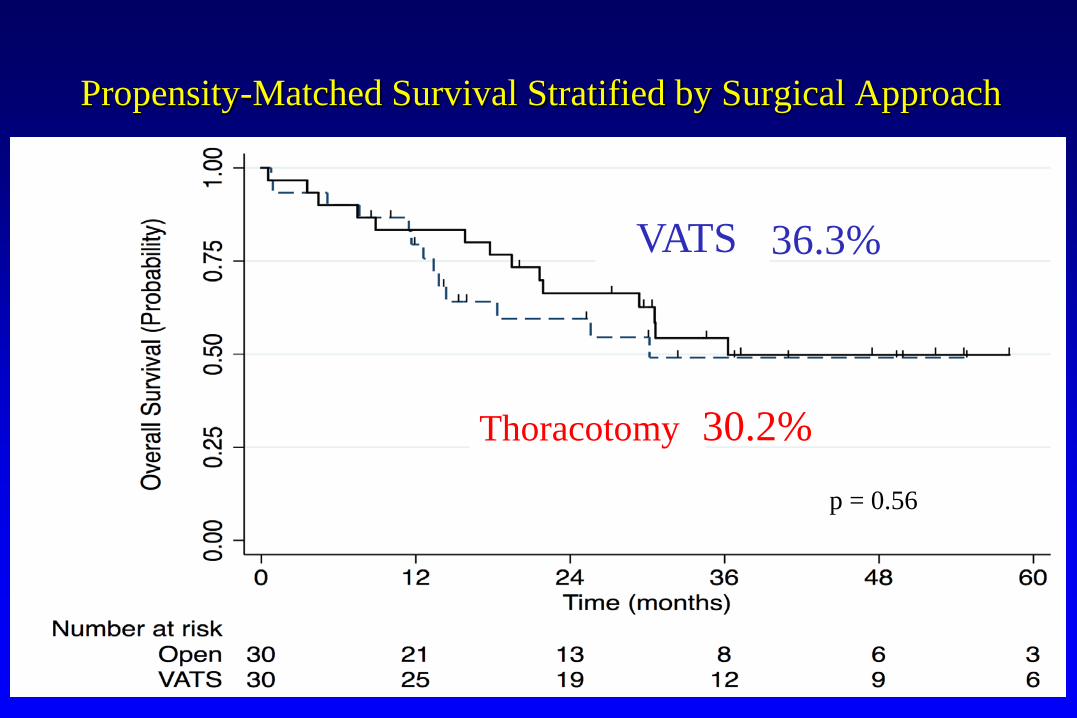
Propensity-Matched Survival Stratified by Surgical Approach
Thoracotomy
VATS
30.2%
36.3%
p = 0.56
Thoracoscopic Pneumonectomy
• Introduced with the demonstration of feasibility without the demonstration of advantages (unlike thoracoscopic lobectomy)
• Outcome advantages—QOL, complications, compliance with adjuvant chemo—are inferred
• Experience thus far is not as convincing as for VATS lobectomy regarding safety and efficacy
Thoracoscopic Pneumonectomy
Potential Criticisms1. Safety: inability to manage bleeding2. Efficacy: inability to determine is sleeve
lobectomy is feasible
Does Thoracoscopic Pneumonectomy for Lung Cancer Affect Survival?
Nwogu CE, et al. Ann Thorac Surg 2010;89:2102-2106
• Pneumonectomy for malignancy (2002-08)• 70 patients: VATS 24, Open 35, Conversions 8• Complication rates similar among all 3 groups• VATS: shorter LOS and less blood loss vs Open• Conversion pts: longer LOS and more blood loss• 30-day mortality: 1 death in VATS and open
groups
Thoracoscopic Pneumonectomy: Duke
• 23 patients underwent attempted VATS pneumonectomy; 17 (73.9%) were completed VATS and 6 required conversion to thoracotomy
• There were no peri-operative mortalities• Conversions were more likely to have CAD, DM,
CHF, poorer pulmonary function and to have received induction chemotherapy or previous thoracic surgery
Thoracoscopic Pneumonectomy
Reasons for Conversion (n=6)• Anatomical hilar dissection not amenable to
VATS (n=4)• Pulmonary artery bleeding (n=1)• Adhesions (n=1)
Thoracoscopic Pneumonectomy
Outcome of Conversion:
Higher blood loss (p = 0.001)VATS Open Conversions
EBL (ml) 200 250 1275
Thoracoscopic Pneumonectomy
Compared to 44 matched thoracotomy patients:• VATS patients had shorter hospital stay (median
LOS = 4 vs. 5 days, p < 0.01)• Operative time, morbidity, and mortality were
not significantly different • Adjuvant chemotherapy was started sooner in
VATS patients• No differences in short or long term survival
• 107 consecutive pneumonectomies 2002 to 2012• Open 40 VATS 50 Conversions 17• VATS cohort had more pre-op comorbidities and
were older (65 years vs 63 years, P =0.07)• C-stage lower for VATS (26% vs 50% stage III,
P= 0.035)• P-stage was similar (25% vs 38%, P = 0.77)
CHEST 2014; 146(5): 1300 - 1309
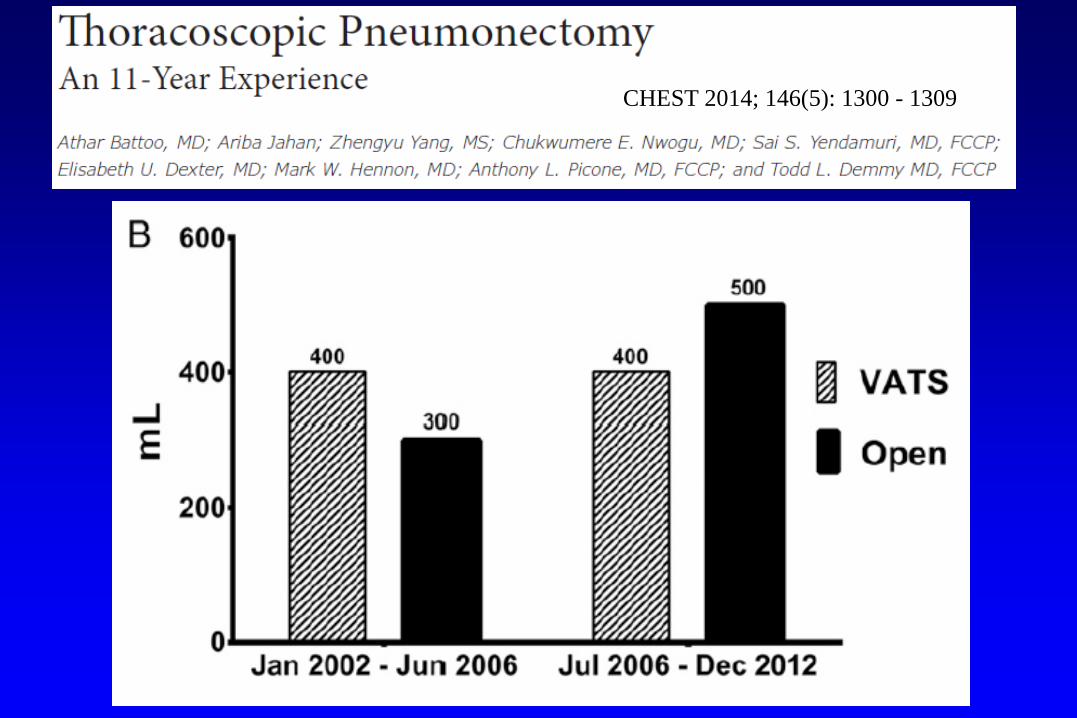
• VATS approach yielded similar complications with no catastrophic intraoperative bleeding
• Successful VATS rates rose from 50%-82% by the 2nd half of the series (P =0.001)
• Completion pneumonectomy cases (13.4% VATS, 7.5% open) had similar outcomes
CHEST 2014; 146(5): 1300 - 1309
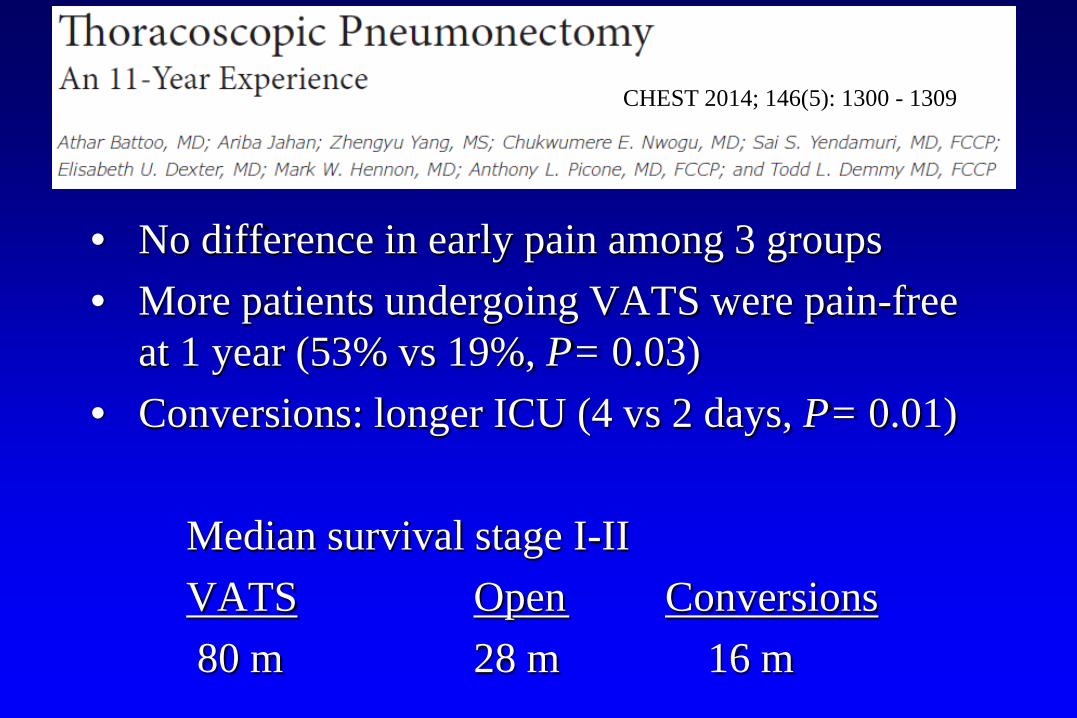
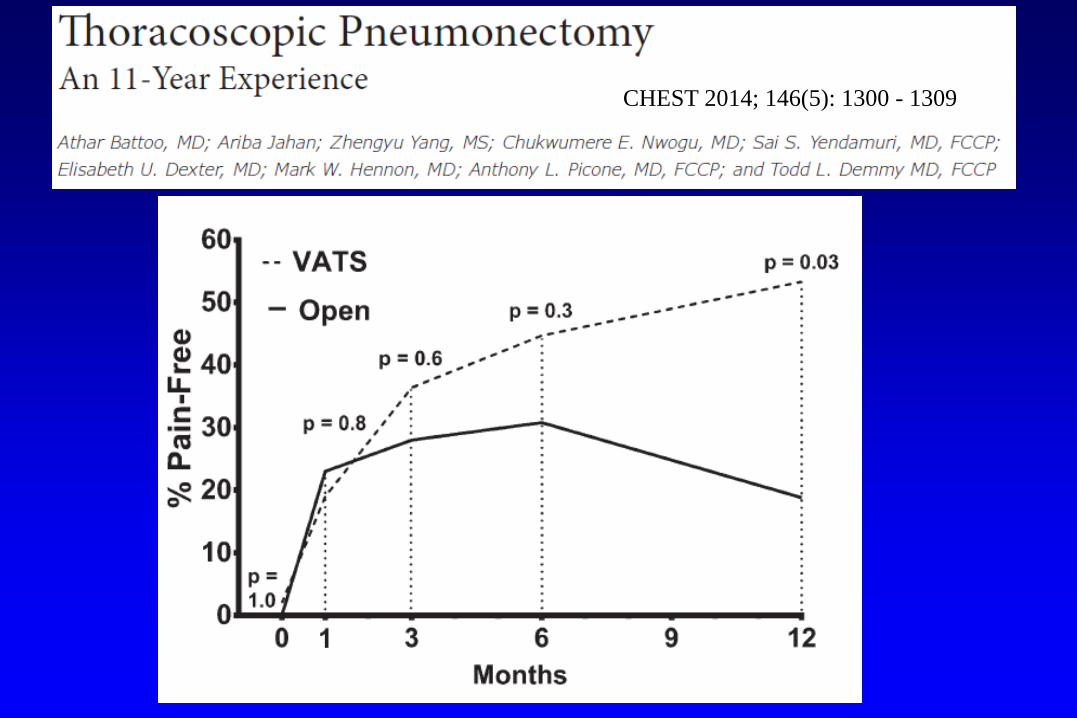
• No difference in early pain among 3 groups• More patients undergoing VATS were pain-free
at 1 year (53% vs 19%, P= 0.03)• Conversions: longer ICU (4 vs 2 days, P= 0.01)
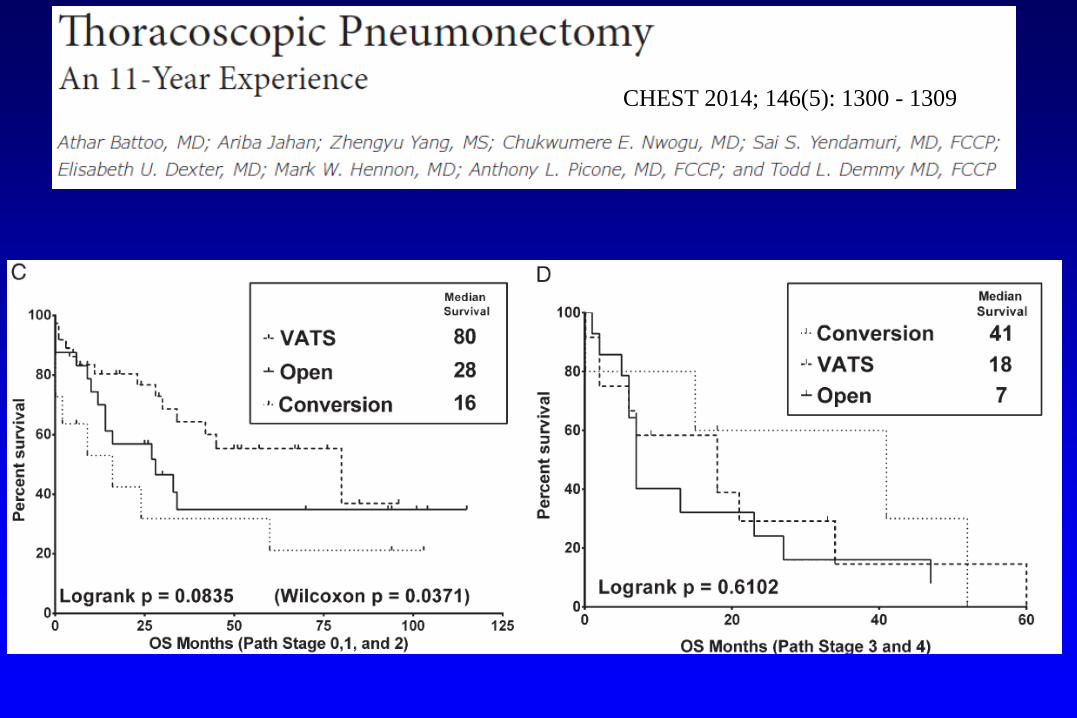
Median survival stage I-II VATS Open Conversions80 m 28 m 16 m
CHEST 2014; 146(5): 1300 - 1309
CHEST 2014; 146(5): 1300 - 1309
CHEST 2014; 146(5): 1300 - 1309
CHEST 2014; 146(5): 1300 - 1309
Multicenter Study of Open vs VATS Pneumonectomy for Lung Cancer
• 3 Institutions • 401 patients
VATS 155 (39%)Open 246 (61%)
Thoracoscopic Extended Resections
• Feasible• Safe• Adhere to the principle of conversion whenever
patient safety or oncologic standards would be compromised

11th Annual Masters in Minimally Invasive Thoracic Surgery
September 21-22, 2018Waldorf AstoriaOrlando, Florida
endo.surgery.duke.edu/courses





























