Embed Size (px)
Citation preview

Complex DM foot cases discussion

• Diabetic foot ulcer (DFU): soft tissue or bone infection below the malleoli 1,2
• Diabetic foot infection (DFI): DM foot with evidence of inflammation or purulence 1,2
DM foot
1. Fassil W et al. Am Fam Physician 2013.2. Lipsky BA et al. Diabetes Metab Res Rev 2016.

DFI

Orrapin S et al. Applied Vascular Surgery Vol 4: Clinical practice in Vascular surgery 2017.

Orrapin S et al. Applied Vascular Surgery Vol 4: Clinical practice in Vascular surgery 2017.
Endocrine
PM & R
Orthopedist
Wound care nurse
Multidisciplinary team
Vascular Sx
Plastic & Reconstruction Sx
Surgery

Principle Management
1. Diagnosis of soft tissue infection VS osteomyelitis
2. Control blood sugar and co-morbid condition (esp. Cardiac disease)
3. Assessing severity and Eradicated infection• Antibiotic
• Limited debridement and amputation
4. Microbiologic consideration • tissue specimen culture
5. Evaluation vascular supply and revascularization as indicated
6. Off-loading technique• Total Contact Cast (TCC) or other instrument
• Surgery

Case presentation

Case No.1

6o years old male
• DM type: DM Type 2• Duration: 5 years
• No history of severe hypoglycemia
• Complication• Eye complication: mild NPDR RE• DM nephropathy: none (urine protein negative)
• Peripheral neuropathy: present
• Painful neuropathy: none
• Lastest Cr: 0.8

• Medication• Ciprofloxacin (250) 2*2 o pc Clindamycin (300) 2*3 o pc
• ASA (81) 1*1 o pc Plavix (75) 1*1 o pc
• Carvedilol (25) 1*2 o pc ISMN (20) 1*2 o ac
• Mixtard 20 – 0 - 10 u SC Lasix (40) 1*1 o pc
• Aldactone (25) 1*1 o pc Gabapentin (300) 1 * 1 o hs
• Last HbA1C: 7.70%
• FBS (28/1/2560): 148 mg%
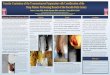
• Foot problem: Wet gangrene Rt foot with osteomyelitis 3rd -5th toe • Post 3,4,5th toe Rt amputation
• Thick callus as residual tissue
• Dry gangrene of 2nd toe

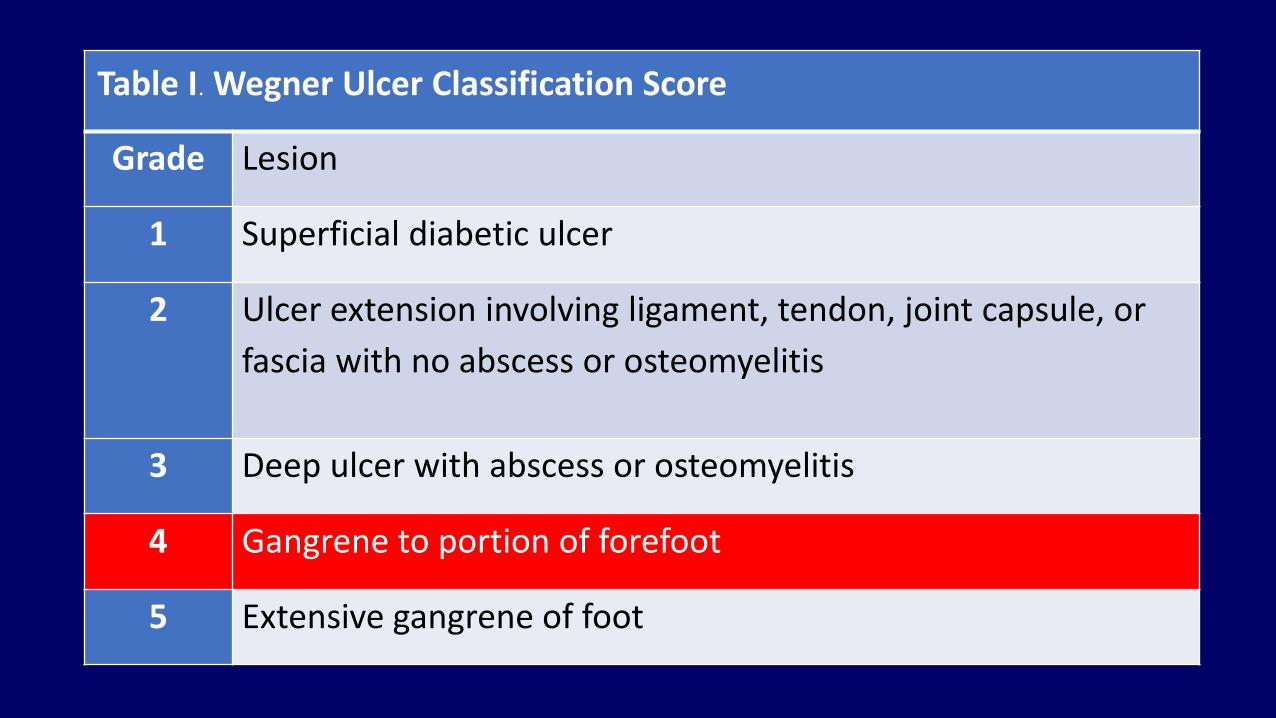
Table I. Wegner Ulcer Classification Score
Grade Lesion
1 Superficial diabetic ulcer
2 Ulcer extension involving ligament, tendon, joint capsule, or
fascia with no abscess or osteomyelitis
3 Deep ulcer with abscess or osteomyelitis
4 Gangrene to portion of forefoot
5 Extensive gangrene of foot

• PAD evaluation:• ABI Rt 0.47 Lt 0.45
• AP Rt 56 Lt 54• CAVI Rt 5.9 Lt 7.2
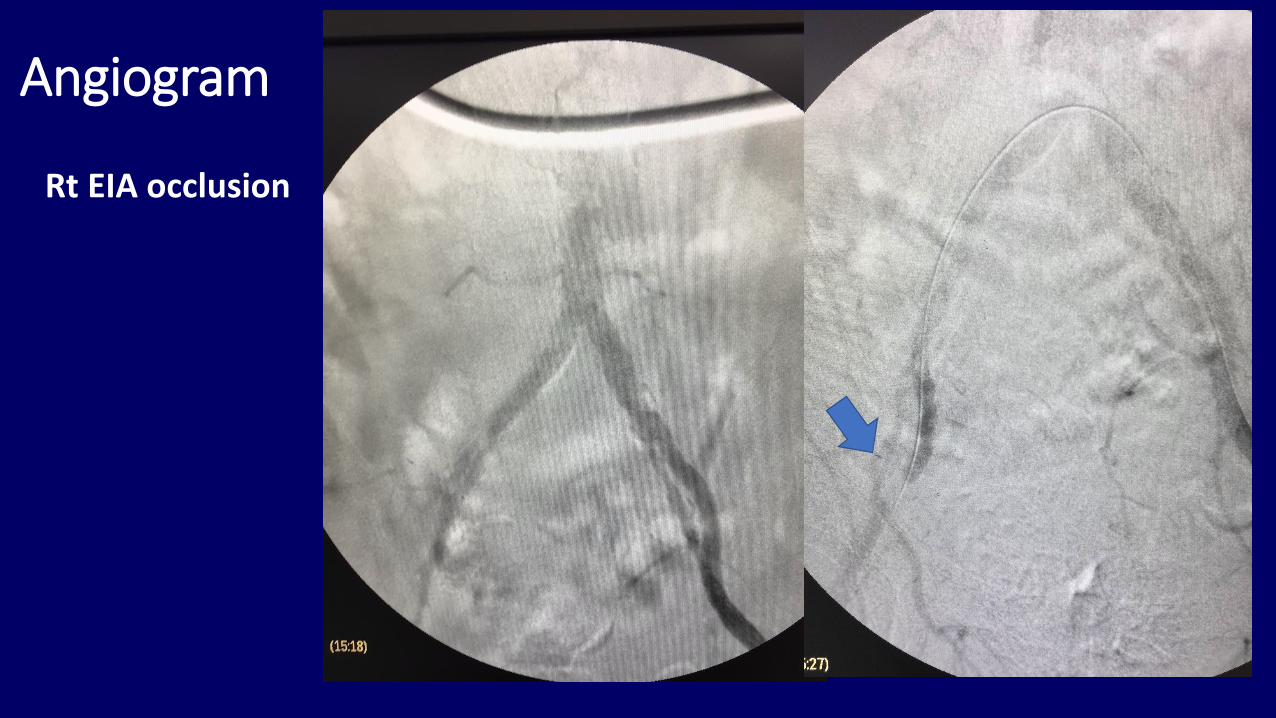
Angiogram
Rt EIA occlusion

Angiogram
Rt CFA and SFA stenosis

Angiogram
Rt proximal tibioperonealtrunk stenosis
Rt anterior tibial artery occlusion

Revascularization
• Percutaneous balloon angioplasty of • Rt external iliac artery,
• Rt superficial femoral artery (SFA),
• Rt tibioperoneal artery,
• Rt plantar artery
• with stenting at distal and proximal SFA


• Post-angioplasty PAD evaluation:• ABI Rt 0.80 Lt 0.46
• AP Rt 96 Lt 55• CAVI Rt 5.9 Lt 7.2

Right foot (Post revascularization and debridement)

Right foot (Post revascularization and debridement)

Right foot (Post revascularization and debridement)


Endocrine Evaluation
• Fair glycemic control
• DM with DR VA?? and peripheral neuropathy
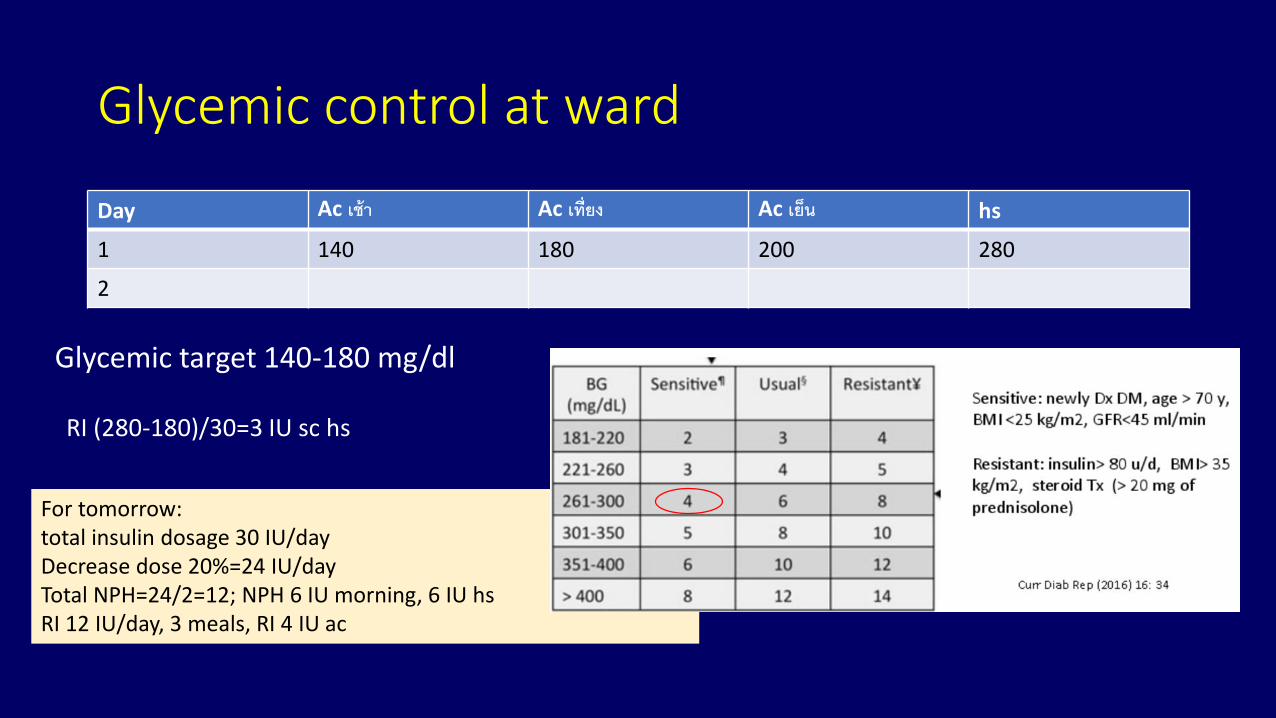
Glycemic control at ward
Day Ac เช้า Ac เที่ยง Ac เยน็ hs
1 140 180 200 280
2
Glycemic target 140-180 mg/dl
RI (280-180)/30=3 IU sc hs
For tomorrow: total insulin dosage 30 IU/day Decrease dose 20%=24 IU/dayTotal NPH=24/2=12; NPH 6 IU morning, 6 IU hsRI 12 IU/day, 3 meals, RI 4 IU ac

Glycemic control at ward
Day Ac เช้า Ac เที่ยง Ac เยน็ hs
1 140 180 200 280
2 152 (R4, N6) 254 (R4+4) 80 (R4) 145 (N6)
Glycemic target 140-180 mg/dl

Pitfalls
• ใช้ NPH เป็น correction insulin
• รอให้น ำ้ตำลสงูก่อนจงึฉีดยำเช่น

Glycemic control at ward
Day Ac เช้า Ac เที่ยง Ac เยน็ hs
1 140 180 200 280 (R4)
2 241 (R8) 140 324 (R10) 180
3 342 (R10) 174 246 (R6) 259 (R8)
4 327
Glycemic target 140-180 mg/dl

Pitfalls
• ใช้ NPH เป็น correction insulin
• รอให้น ำ้ตำลสงูก่อนจงึฉีดยำเช่น
• ไมป่รับยำฉีดดงัตวัอยำ่ง
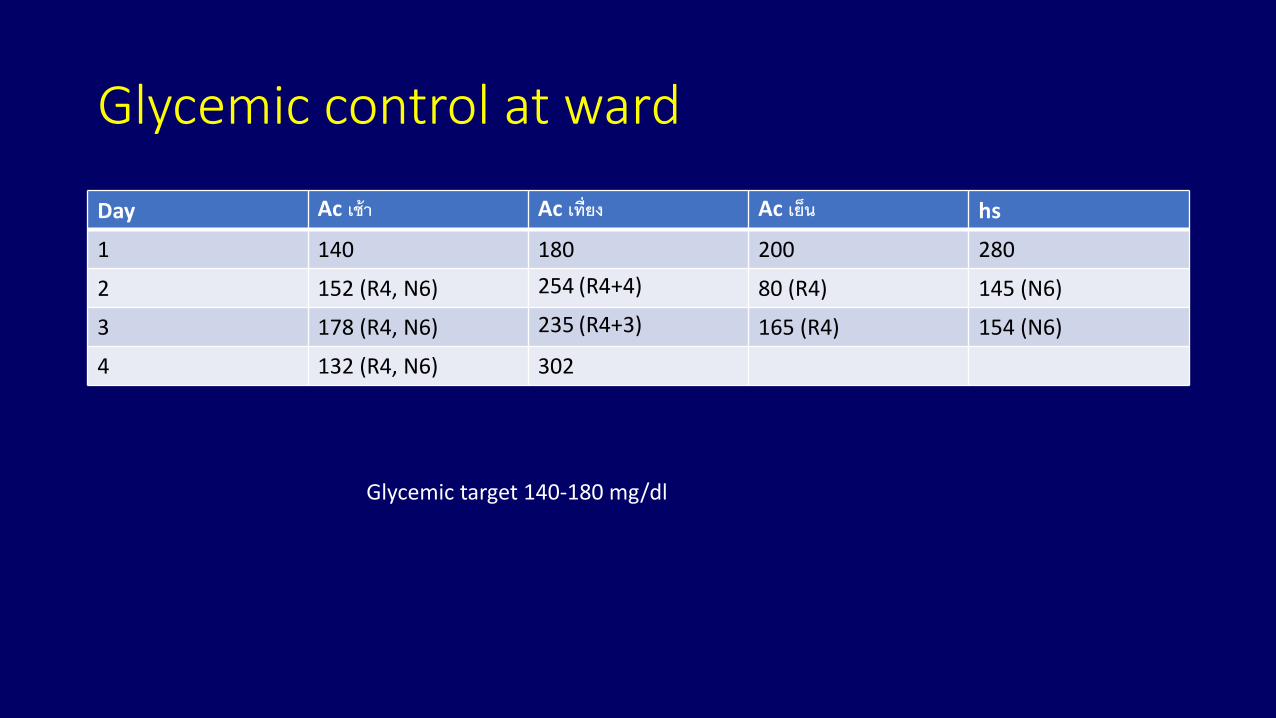
Glycemic control at ward
Day Ac เช้า Ac เที่ยง Ac เยน็ hs
1 140 180 200 280
2 152 (R4, N6) 254 (R4+4) 80 (R4) 145 (N6)
3 178 (R4, N6) 235 (R4+3) 165 (R4) 154 (N6)
4 132 (R4, N6) 302
Glycemic target 140-180 mg/dl

Pitfalls
• ใช้ NPH เป็น correction insulin
• รอให้น ำ้ตำลสงูก่อนจงึฉีดยำ• ไมป่รับยำฉีดแม้วำ่น ำ้ตำลจะสงู• Glucose alert level (<70)
• ไม่มีกำรแก้ไข ฉีดยำเท่ำเดิม • ให้กินน ำ้หวำนแล้วไม่เจำะน ำ้ตำลซ ำ้ท่ี 15 นำที• ไม่ฉีดยำหลงัน ำ้ตำลขึน้• Over sugar correction
• ขำดกำรวำงแผนตอน discharge
• ไมมี่ monitor CBG

Patient age
Disease duration
Comorbidities
Hypoglycaemia risk
Behavioral – social – economicHigher motivation, knowledge
Greater self-care capacity, insight, supportLess motivated, non-adherent,
Limited self-care capacity, insight support
Established ComplicationsNone Early Microvascular Advanced MicrovascularCV
Ismael-Beigi F. Ann Intern Med. 2011;154(8):554-559.
8.0%7.0%6.0%
Individualising Glycaemic Targets
HbA1ctarget

TARGET OF GLYCEMIC CONTROL
การควบคุมเบาหวาน เป้าหมายควบคุมเขม้งวดมาก ควบคุม
เขม้งวดควบคุมไม่เขม้งวด
ระดบัน ้าตาลในเลือดขณะอดอาหาร >70-110 mg/dl 80-<130 mg/dl <150 mg/dl
ระดบัน ้าตาลในเลือดหลงัอาหาร 2ชัว่โมง
<140 mg/dl
ระดบัน ้าตาลในเลือดสูงสุดหลงัอาหาร - <180 mg/dl
%HbA1c <6.5% <7.0% 7.0-8.0%
Thai DM guideline 2014

end



Right foot (Post revascularization and debridement)

Right foot (Post revascularization and debridement)
Case No.2
1410822

65 years old male
• DM type: DM Type 2
• Duration: diagnosis 10 years
• Chronic pancreatitis
• Complication• Eye complication: pending• DM nephropathy: Usugar 3+,Uprotein
• Peripheral neuropathy: present• Painful neuropathy: none• Lastest Cr: 1.01 (eGFR 50) (CKD stage 3)

• Medication
• ASA (81) 1x1 po pc Atrovastatin(40) 1x1 po hs
• Atenolol(50) ½ x1 op pc
• NPH 14-0-0-4 RI 14-8-8-0
• Gabapentin(300) 1x1 op pc Ativan(0.5) 1x1 op hs
• Last HbA1C: 7.7 %
• Fasting Blood Sugar: 142 mg%

• PAD evaluation:• ABI Rt 0.36 Lt 0.78
• Ankle pressure Rt 50 mmHg Lt 110 mmHg

Foot problem:
• Chronic ulcer with open wound with tissue loss at Lateral plantar site of Rt 5rd toe to fore foot and midfoot deep to muscle with necrotic tissue and frank pus with extension to Rt 4th-5th metatarsal (bone exposed to bone) at dorsum part
• Probe to bone test positive

Film foot
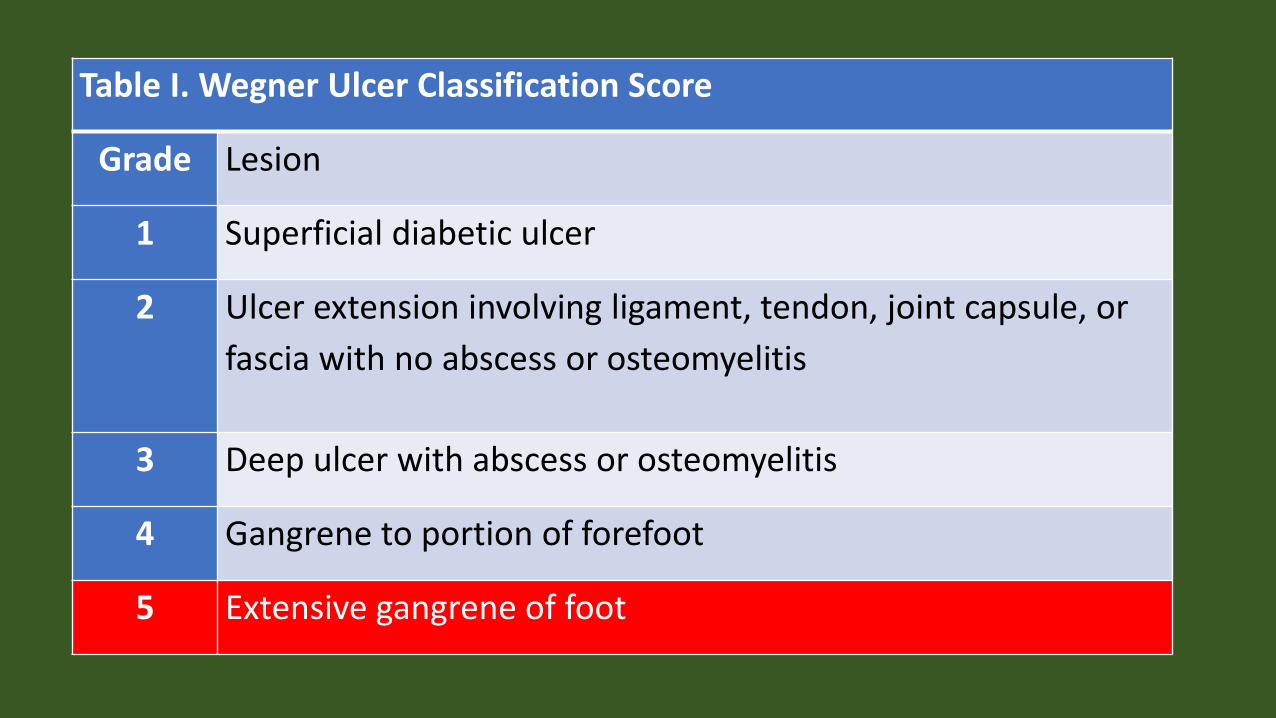
Table I. Wegner Ulcer Classification Score
Grade Lesion
1 Superficial diabetic ulcer
2 Ulcer extension involving ligament, tendon, joint capsule, or
fascia with no abscess or osteomyelitis
3 Deep ulcer with abscess or osteomyelitis
4 Gangrene to portion of forefoot
5 Extensive gangrene of foot

Preoperative
• Autonomic neuropathy?
• EKG
• Random PG=350 mg/dl (T1DM)
• Goal??
• Insulin drip
• DTX q 1 hr
• DKA??

Limited debridement procedure
• Right Chopart’s amputation • Finding: Navicular, Cuboid, Cuneiforms and Metatarsal bone fragile and pus
involvement
• No bleeding from raw surface tissue
• Heavy calcification of Dorsalis pedis artery

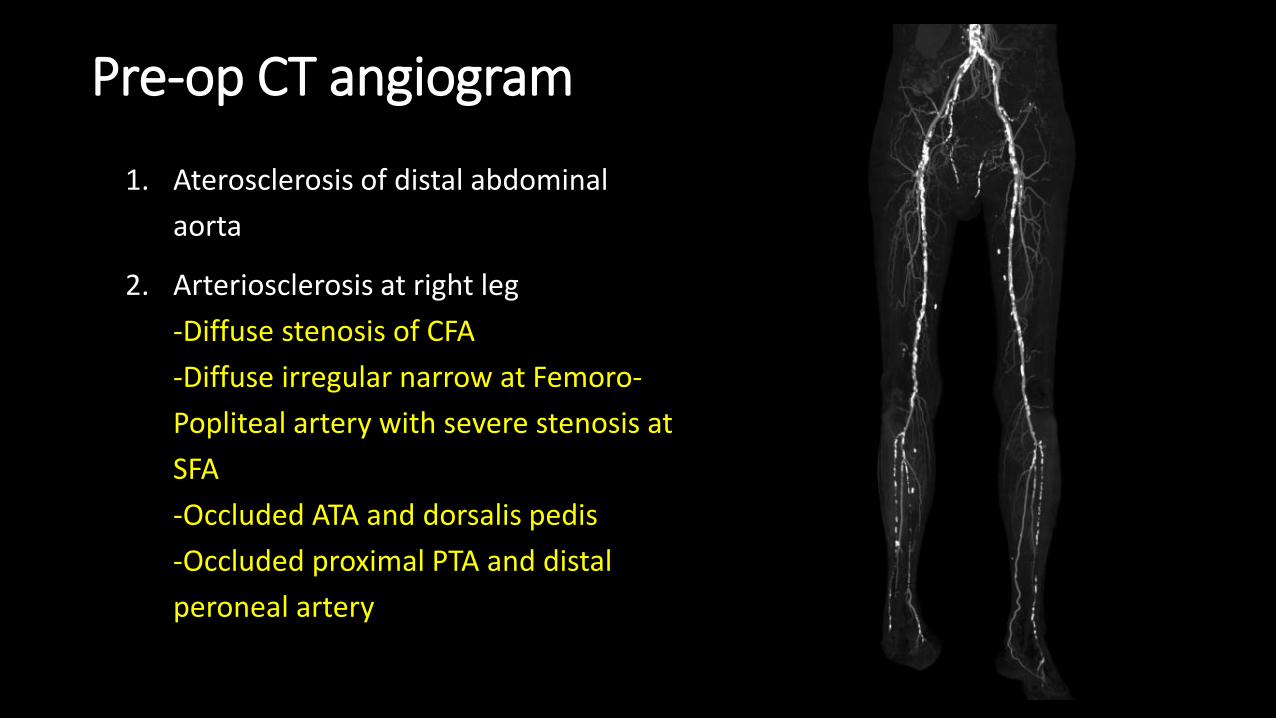
Pre-op CT angiogram
1. Aterosclerosis of distal abdominal
aorta
2. Arteriosclerosis at right leg
-Diffuse stenosis of CFA
-Diffuse irregular narrow at Femoro-
Popliteal artery with severe stenosis at
SFA
-Occluded ATA and dorsalis pedis
-Occluded proximal PTA and distal
peroneal artery
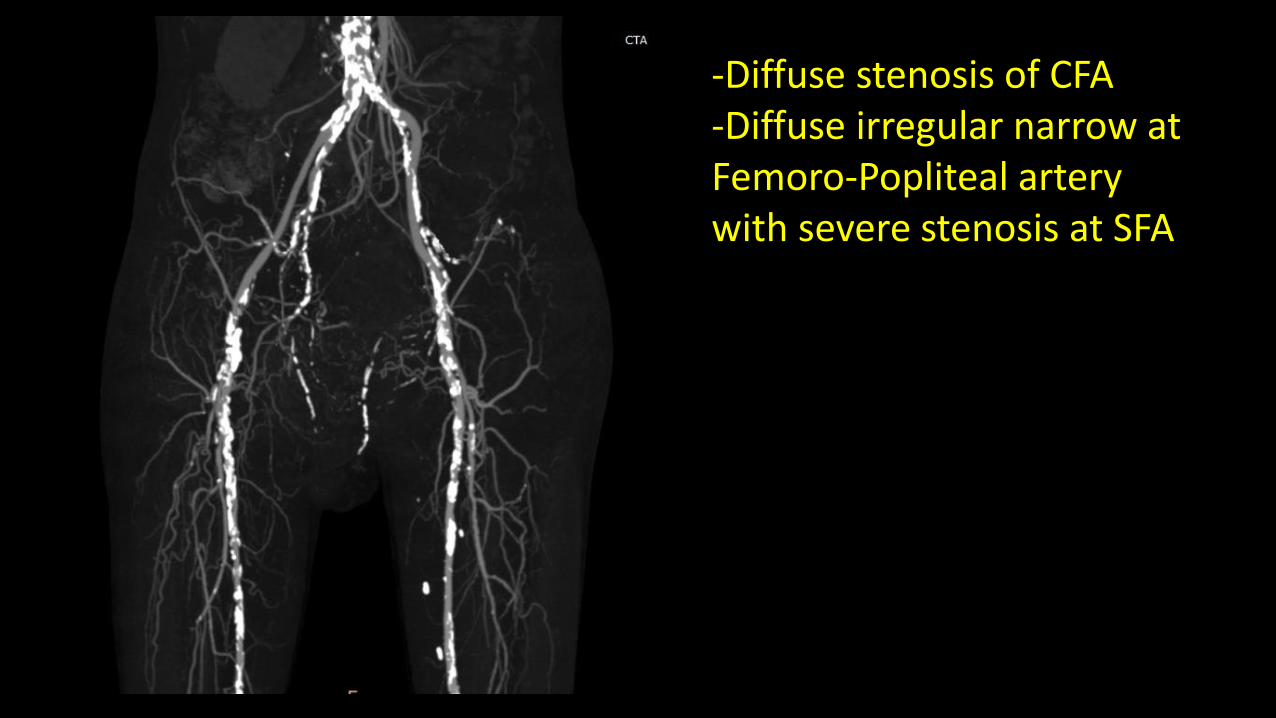
-Diffuse stenosis of CFA -Diffuse irregular narrow at Femoro-Popliteal artery with severe stenosis at SFA

-Diffuse stenosis of CFA -Diffuse irregular narrow at Femoro-Popliteal artery with severe stenosis at SFA

- Occluded ATA and dorsalis pedis- Occluded proximal PTA and distal peroneal artery

Pre-op CT angiogram
1. Aterosclerosis of distal abdominal
aorta
2. Arteriosclerosis at right leg
-Diffuse stenosis of CFA
-Diffuse irregular narrow at Femoro-
Popliteal artery with severe stenosis at
SFA
-Occluded ATA and dorsalis pedis
-Occluded proximal PTA and distal
peroneal artery
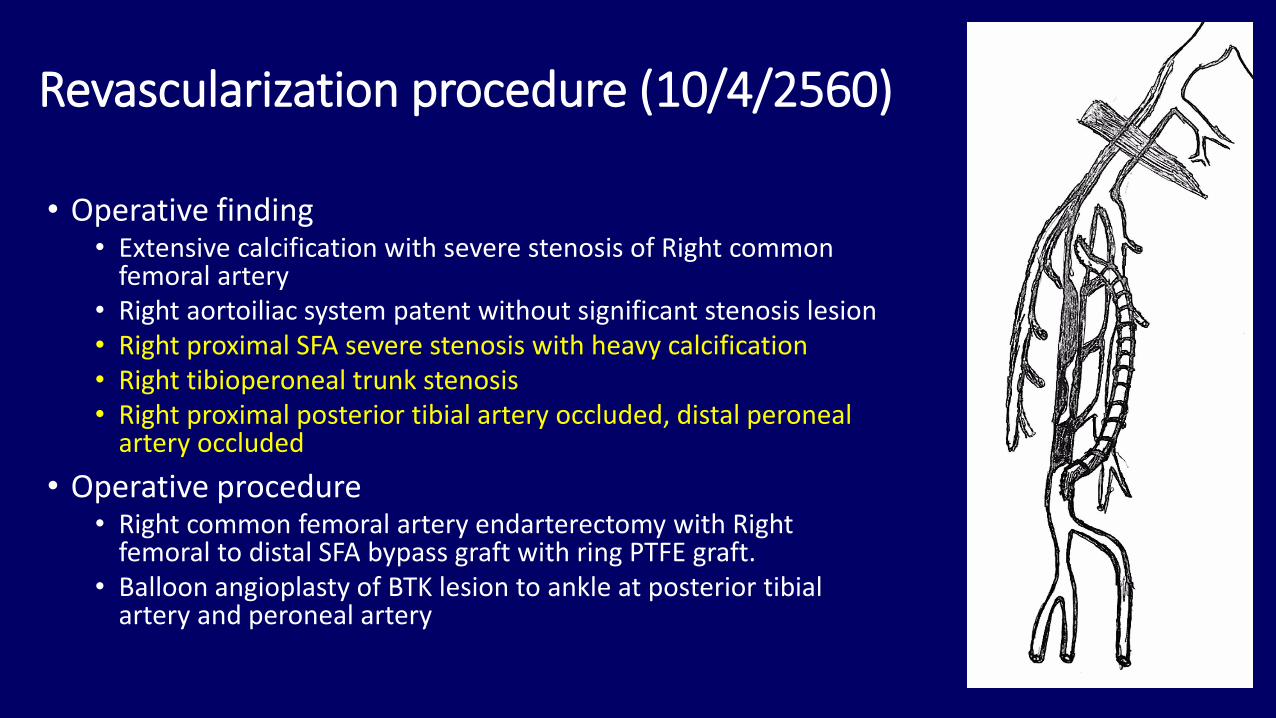
Revascularization procedure (10/4/2560)
• Operative finding• Extensive calcification with severe stenosis of Right common
femoral artery• Right aortoiliac system patent without significant stenosis lesion• Right proximal SFA severe stenosis with heavy calcification• Right tibioperoneal trunk stenosis• Right proximal posterior tibial artery occluded, distal peroneal
artery occluded
• Operative procedure• Right common femoral artery endarterectomy with Right
femoral to distal SFA bypass graft with ring PTFE graft.• Balloon angioplasty of BTK lesion to ankle at posterior tibial
artery and peroneal artery

Right common femoral artery endarterectomy with Right femoral
to distal SFA bypass graft with ring PTFE graft.

Finding:
• Right tibioperoneal trunk stenosis• Right proximal posterior tibial artery
occluded, distal peroneal artery occluded

Procedure:
• Balloon angioplasty of BTK lesion to ankle at posterior tibial artery and peroneal artery


How to management the ankle stump ?
• Wound management
• Stump closure method
• Blood sugar control (HbA1c 7.7%, FBS 142 mg%)
• Role of Plastic surgeon






Case No.3
545119

62 years old male
• DM type: DM Type 2• Duration: 20 years
• ESRD
• Complication• Eye complication: none• DM nephropathy: ESRD
• Peripheral neuropathy: present• Painful neuropathy: none• Lastest Cr: 8.55 (eGFR 4.52)
• On long-term HD via Left Brachio-Cephalic AVF

• Medication
• Alfacalcidol (0.25 mcg) Methyldopa(250) 2 x 2 o pc• Amlopine(10) 1 x 2 o pc Vitamin Bcomplex 1 x 2 o pc• Aspirin (81) 1 x 1 o pc Eprex 4000 U / week• Atrovastatin (40) 1 x 1 o pc Ferrous fumarate (200) 1 x 2 o pc• Caltab (1500) 1 x 3 o pc Losartan(50) 1 x 2 o pc • Glargine 14 unit SC ac morning
• Last HbA1C:
• 8.2 (8/3/2017)
• 10.2 (16/11/2016)
• Fasting Blood Sugar (8/3/2017): 169 mg%

• PAD evaluation:• ABI Rt 0.92 Lt 0.84
• Ankle pressure Rt 119 Lt 109
• Palpable pulse both pedal artery

• Foot problem: • Dry gangrene at tip of Left 1st and 2nd toe with callus formation at
tip of Left 3rd and 4th toe with deformities
• No sign and symptom of DFI



• Management:
• No role of revascularization
• No infection



Case No.4

2o years old male
• DM type: DM Type I• Duration: 20 years
• Last 1 year history of severe hypoglycemia
• Complication• Eye complication: PDR BE s/p Laser Rx
• DM nephropathy: UPCI 1.55 (Diabetic nephropathy (CKD stage 2))
• Peripheral neuropathy: present
• Painful neuropathy: none
• Lastest Cr: 1.17 (eGFR 71)

• Medication
• Clindamycin (300) 1 x 3 o pc Cefdinir (100) 3 x 2 o pc• Atrovastatin (40) 1 x 1 o pc • Ferrous fumarate (200) 1 x 2 o pc Folic acid 1 x 1 o pc• NPH insulin Gabapentin (300) 1 * 1 o hs
• Last HbA1C:• 16.9 (26/9/2011) - 18.5 (16/1/2012)• 15.5 (14/2/2012) - 19.8 (9/5/2012)• 16.6 (6/6/2012)• 8.2 (29/9/2016) - 10.9% (26/1/2017)
• Fasting Blood Sugar (25/1/2017): 154.28 mg%

• Foot problem: • Mottling at Right 3rd toe
• Open wound at Plantar site of Rt 3rd toe with callus and necrotic tissue
• Probe to bone test positive



Table I. Wegner Ulcer Classification Score
Grade Lesion
1 Superficial diabetic ulcer
2 Ulcer extension involving ligament, tendon, joint capsule, or
fascia with no abscess or osteomyelitis
3 Deep ulcer with abscess or osteomyelitis
4 Gangrene to portion of forefoot
5 Extensive gangrene of foot

• PAD evaluation:• ABI Rt 1.12 Lt 1.16
• CAVI Rt 6.6 Lt 6.0
• Palpable pulse both pedal artery

• Management:
• No role of revascularization
• Eradicated infection by Ray amputation Rt 3rd toe

Preoperative
• Autonomic neuropathy?
• EKG
• Random PG=350 mg/dl (T1DM)
• Goal??
• Insulin drip
• DTX q 1 hr
• DKA??



• รายละเอียดของการใช้รองเท้า• เดินเองได้ ไมใ่ช้ gait aid• เดินนอกบ้ำน 80% ใสร่องเท้ำแตะ• เดินในบ้ำนใสร่องเท้ำไมใ่สร่องเท้ำ

Thank you for your attention