Embed Size (px)
DESCRIPTION
child language acquisiton
Citation preview
BRAIN & LANGUAGE
Marzieh Hadei Koik Shuh Jie
Heng Wen ZhuoGoh Sue Yin
Anatomy of the brain
Marzieh Hadei
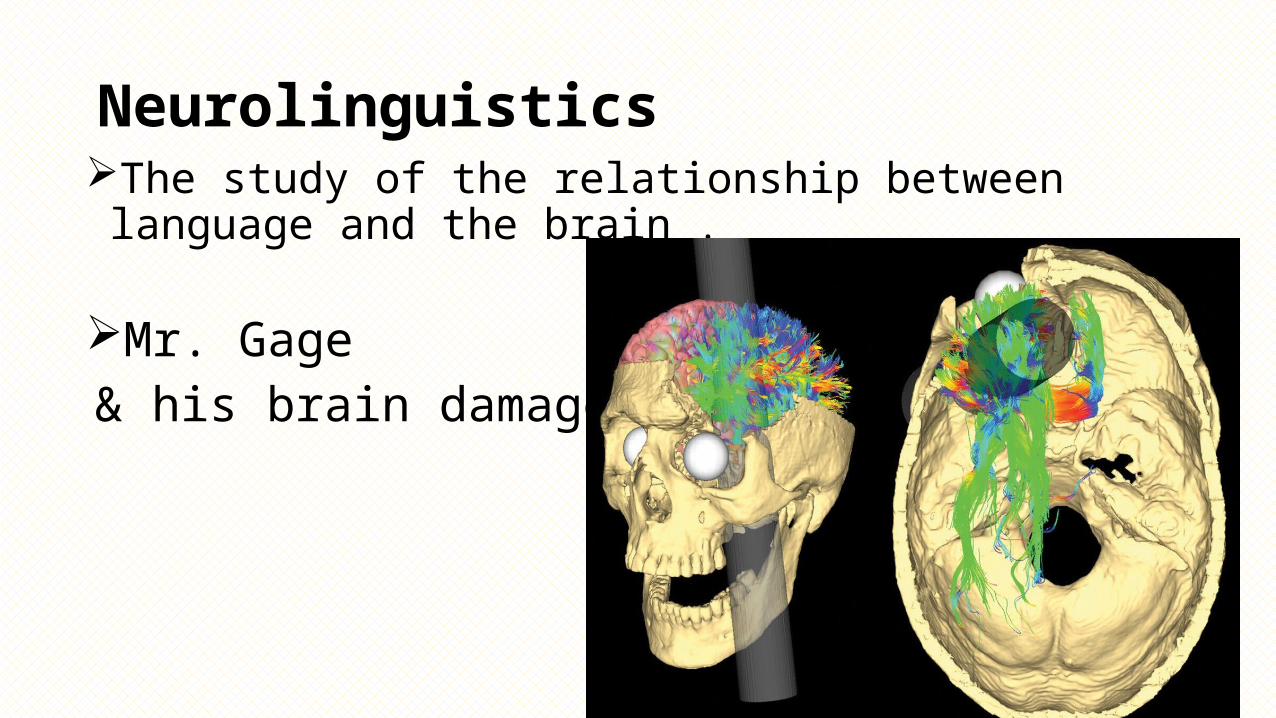
Neurolinguistics The study of the relationship between language and the brain .
Mr. Gage & his brain damage .
Cerebral cortex
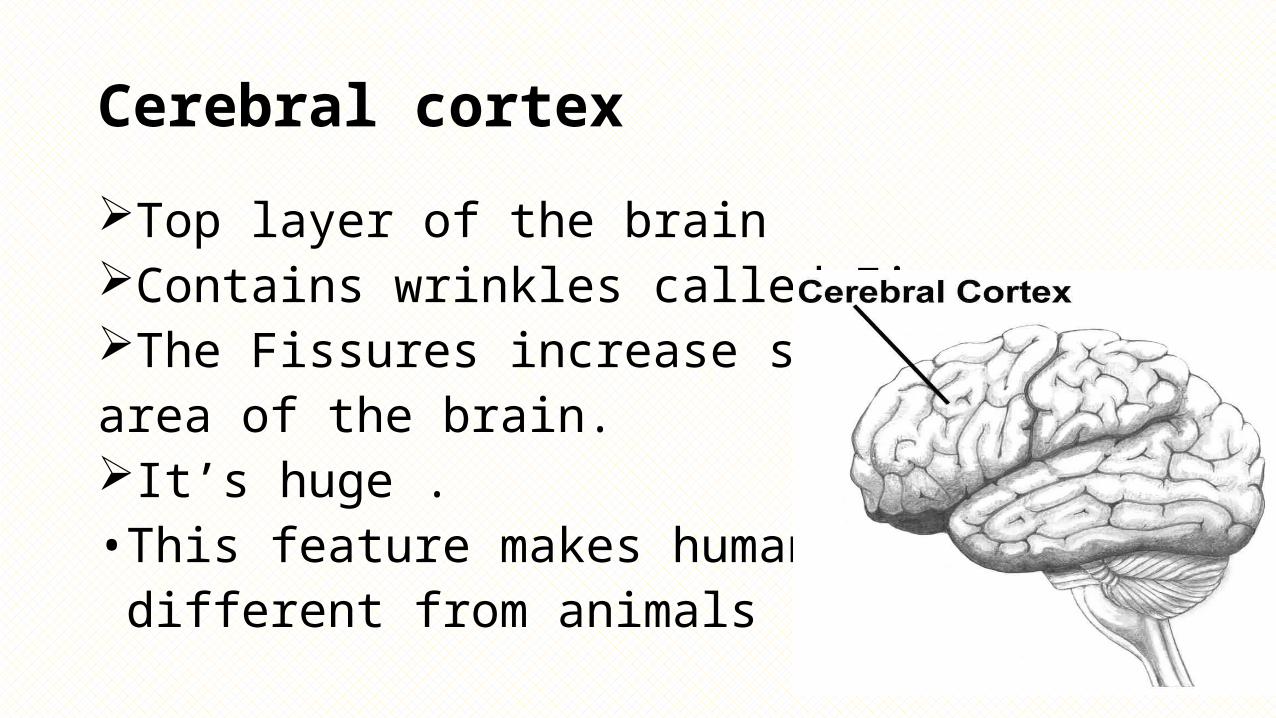
Top layer of the brainContains wrinkles called Fissures.The Fissures increase surfacearea of the brain.It’s huge .• This feature makes humans different from animals .
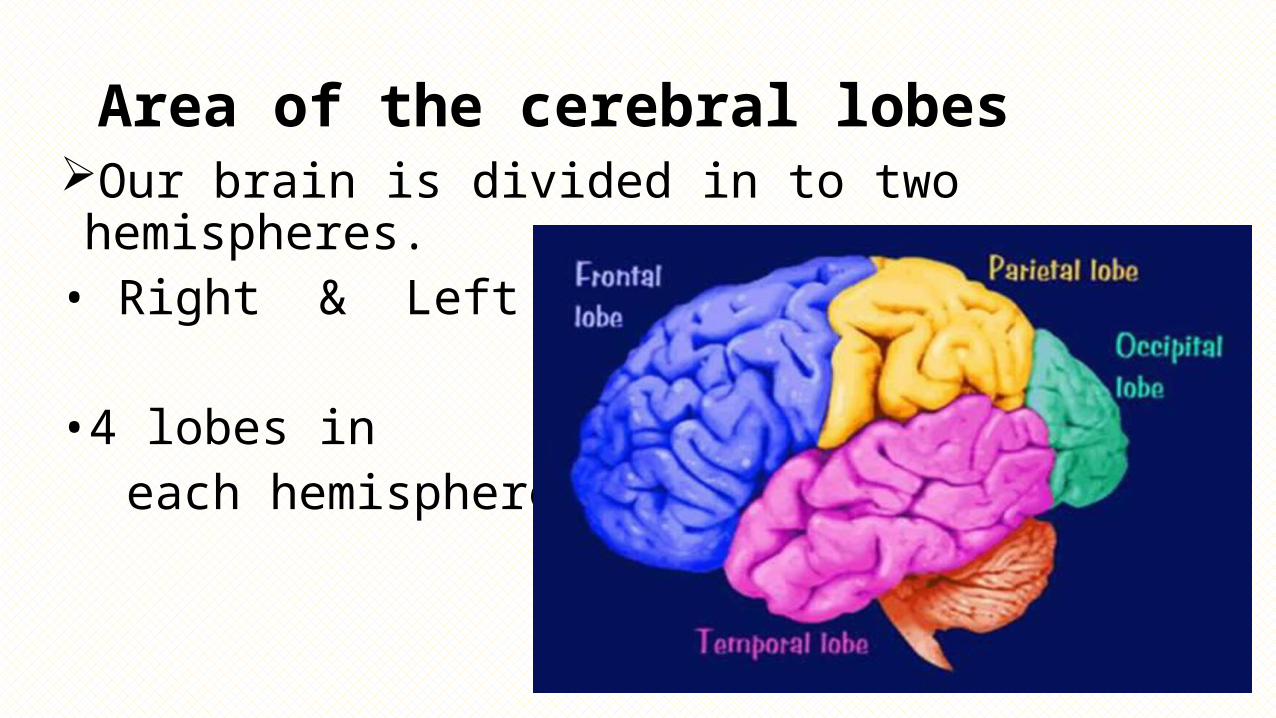
Area of the cerebral lobes Our brain is divided in to two hemispheres.• Right & Left
•4 lobes in each hemisphere.
Right hemisphere controls the left side of the body and vice versa .
Any areas not dealing with our senses or muscles movements are called association area.
The main connection between the two hemispheres is a bundle of nerves fibers known as Corpus callosum .• Its primary function is to allow the two hemispheres to
communicate with one another.
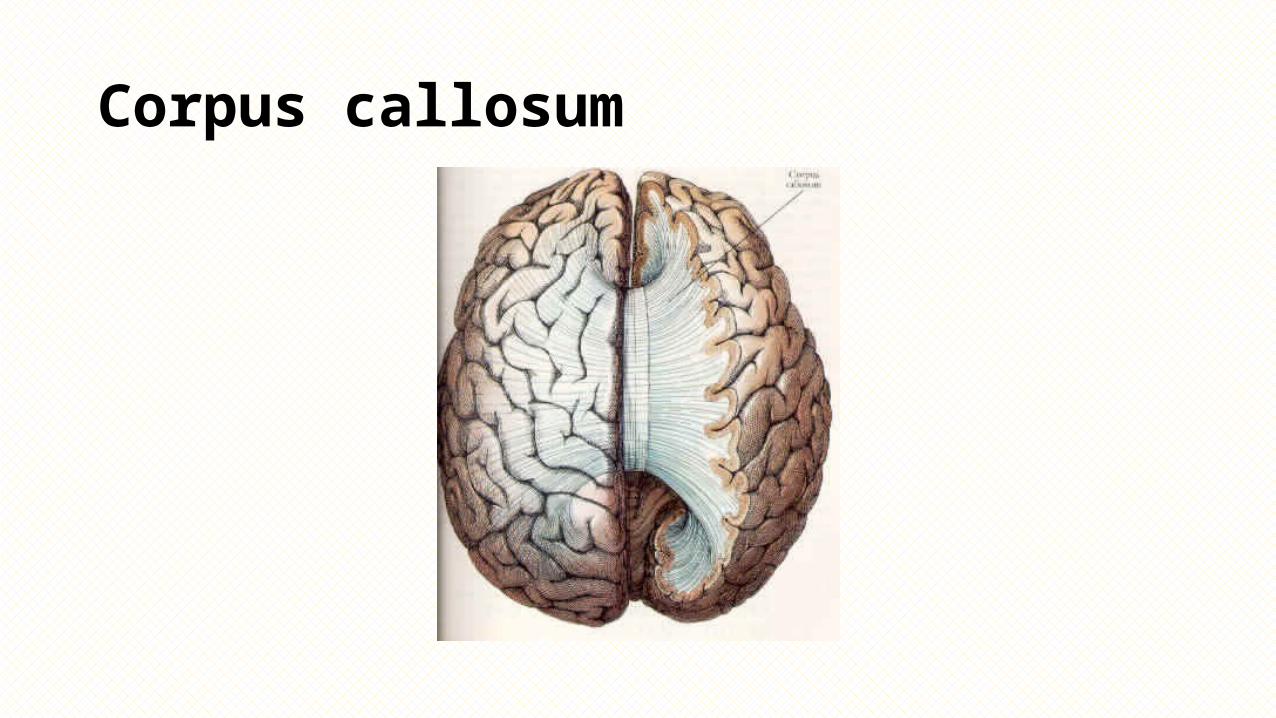
Corpus callosum
Split - brain
The corpus callosum make sure that there is a connection from the right side of the brain to the left side of the brain.
A procedure in which the two hemispheres of the brain are isolated
by cutting the connecting fibers ( corpus callosum ) .
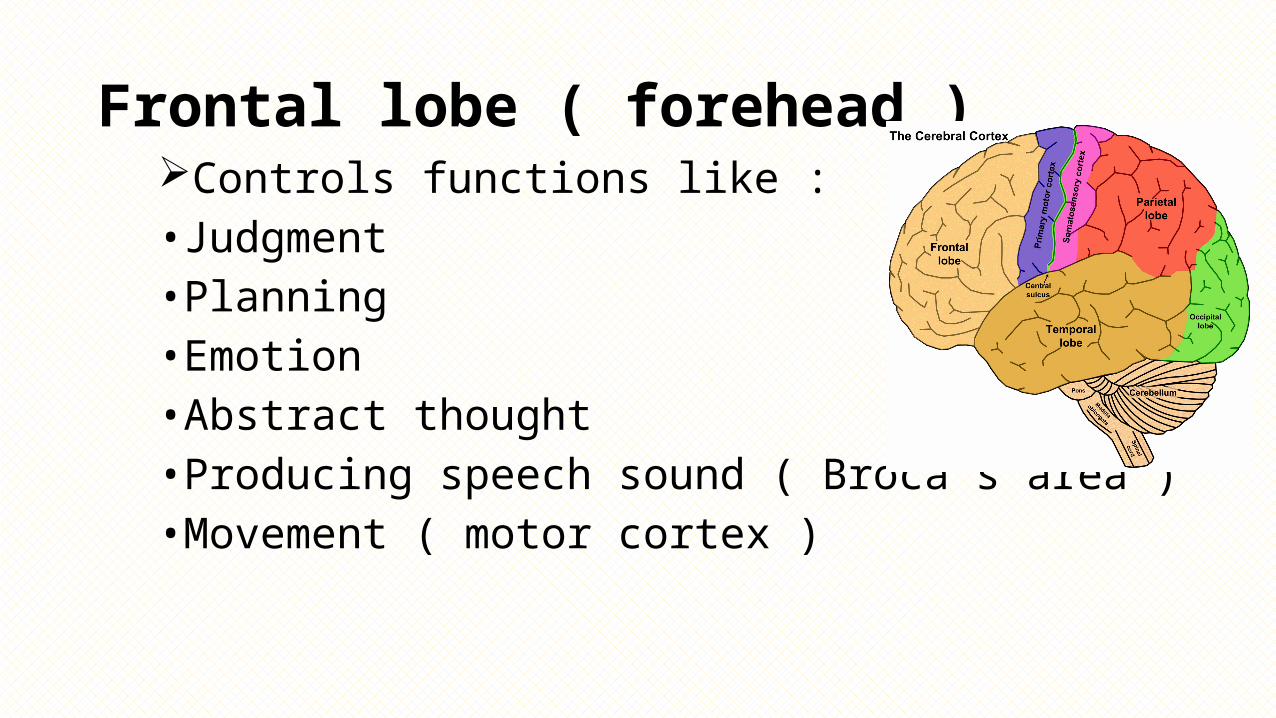
Frontal lobe ( forehead ) Controls functions like :• Judgment • Planning• Emotion• Abstract thought • Producing speech sound ( Broca’s area )•Movement ( motor cortex )
Motor cortex
The strip of brain issue at the rear of frontal lobesResponsible for the voluntary movement Different parts of cortex control different part of bodyThe motor cortex in the left hemisphere control the
right part of body and vise versa.
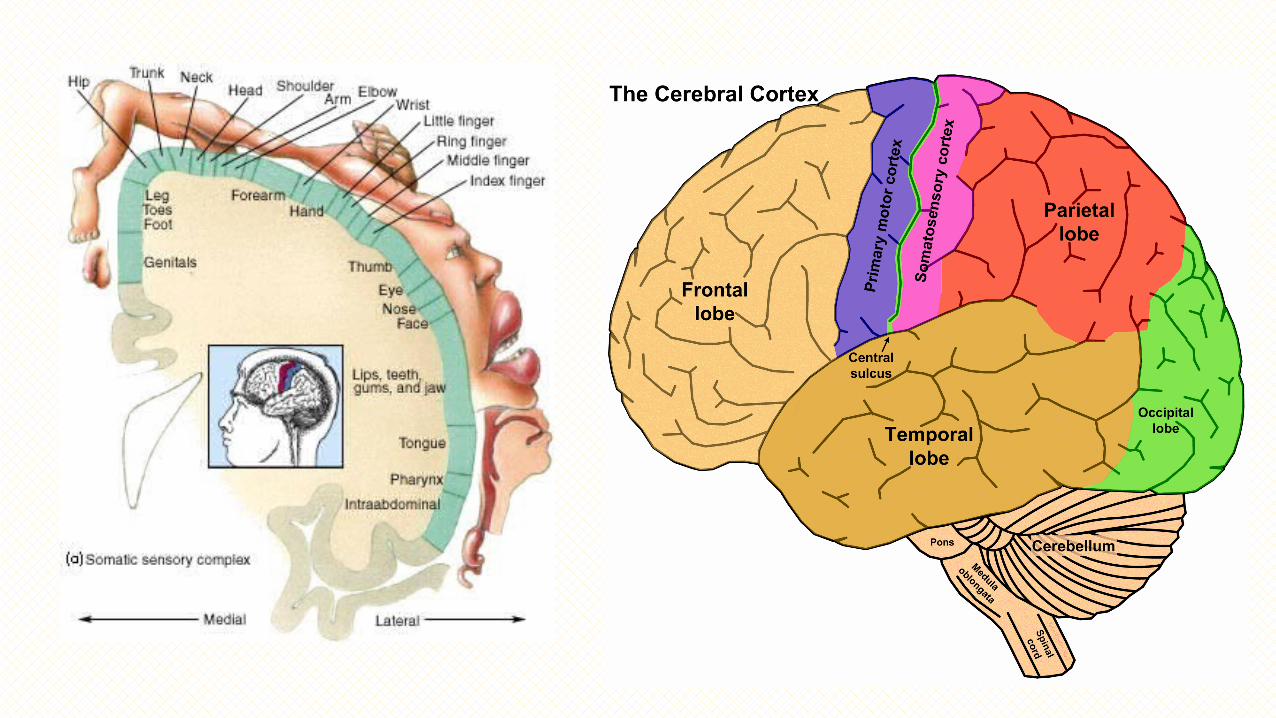
Parietal lobe ( top to rear head )
Control functions like:•Body position• Spatial reasoning likeTouchPressurePain• Somatosensory cortex
Occipital lobe ( back head )
Control functions like :•All aspects of vision•Right half of each retina goes to left occipital lobe and vise versa .
Temporal lobe ( side of head )Controls functions like:•Hearing • Storing long term memory• Speech and language Understanding ( Wernicke's area )
language areas in the brain
There are areas of the brain that appear dedicated to processing language. The original reason that we knew this is because people who had damage in these particular areas of the brain had very specific problems with their understanding or use of language.
Broca’s area Wernicke’s area
Broca’s area Broca’s area : in the left frontal lobe that directs musclemovements involved in speech .Language production areaactually deals with taking words ,forming structured
sentences. Basically, this area is your grammar center that puts the
words together in a coherent fashion.
Broca’s Area• Or “ Anterior speech cortex “
•Marc Dax, during the first years of the 19th century, concluded that the loss of language was more frequently associated with damages to the left half of the brain.
• After the 19th century physician Pual Broca , a French Surgeon , reported that damage to this specific part of the brain was related to extreme difficulty in producing speech.
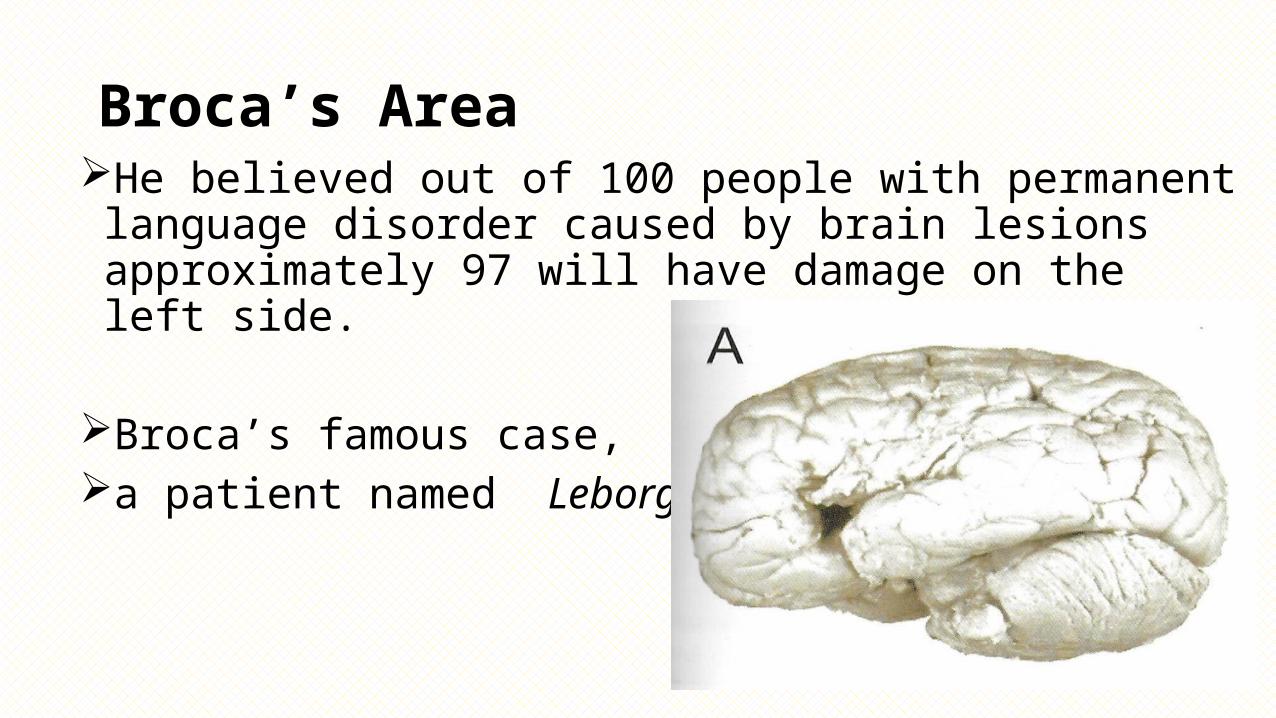
Broca’s AreaHe believed out of 100 people with permanent language
disorder caused by brain lesions approximately 97 will have damage on the left side.
Broca’s famous case, a patient named Leborgne,
Wernicke’s area
•Or Posterior speech cortex
•Carl Wernicke was a German doctor , in the 1870s, reported that damage to this part of the brain was found among patients who had speech comprehension difficulties.
Wernicke’s area in left Temporal lobe that is involved in language comprehension
and expression .
General rule - associated with language understanding… that is, the meaning of words in a sentence rather than the sentence structure.
Example: sometimes people with damage to this area ramble meaninglessly, but can sometimes speak their words fluently.
Lateralization and Localization of Function
Koik Shuh Jie
• Lateralization: The specialization of function between the left and right hemispheres of the brain.
• Lenneberg (1967) and others suggested that lateralization is a slow process that begins around the age of 2 and is completed around puberty.• It has been found that children up to the age of puberty who suffer
injury to the left hemisphere are able to relocalize linguistic functions to the right hemisphere, to ‘relearn’ their first language with relatively little impairment. – CPH.
• While language production is left-lateralized in up to 90% of right-handed subjects, it is more bilateral, or even right lateralized in approximately 50% of left-handers.• Thus, left handed people tend to be less lateralized than right-handed
people.
• In terms of muscle movement and sensation, each hemisphere is responsible for half the body, the opposite half. The left hemisphere controls the right side of the body and vice versa.• Stroke?
• Left hemisphere : analytic tasks such as arithmetic• Right hemisphere : recognition of familiar faces and melodies
• Language;• Left hemisphere : grammar, vocabulary and literal meaning • Right hemisphere : intonation and accentuation
• Perhaps to differing degrees, complex mental activities involve the coordinated functioning of both hemispheres in the normal human brain.• Example: The representation of language in the brain.• Not every aspects of language is represented in the left hemisphere.
• Adults who have had their left cerebral hemispheres surgically removed lose most, but not all, of their linguistic competence. They typically lose their ability to speak and process complex syntactic patterns but retain some language comprehension ability. Right hemisphere?
• Patients who suffer damage to the right cerebral hemisphere exhibit difficulty in understanding jokes and metaphors in everyday conversation.• ‘He was wearing a loud tie’.• Frequently misunderstand people: loudness and intonation as cues.• Thus, the right hemisphere has a distinct role to play in normal
language use.
• Although the left and right hemispheres have different abilities and different responsibilities, complex skills such as language do not always fall neatly into one hemisphere or the other.
Putting One Half of the Brain to Sleep:The Wada Test
• Juhn Wada (1949) developed a test for language dominance that involved injection of the drug sodium amytol.• The injection generally produces immediate contralateral hemiplegia
(paralysis of one side).• The forearm and leg of the side opposite to the injection fall.
• Example: Counting is momentarily interrupted, but with nondominant deactivation, it resumes within 5 to 20 seconds. Yet if the dominant hemisphere is involved, dysphasic responses may persist for as long as 1-3 minutes.
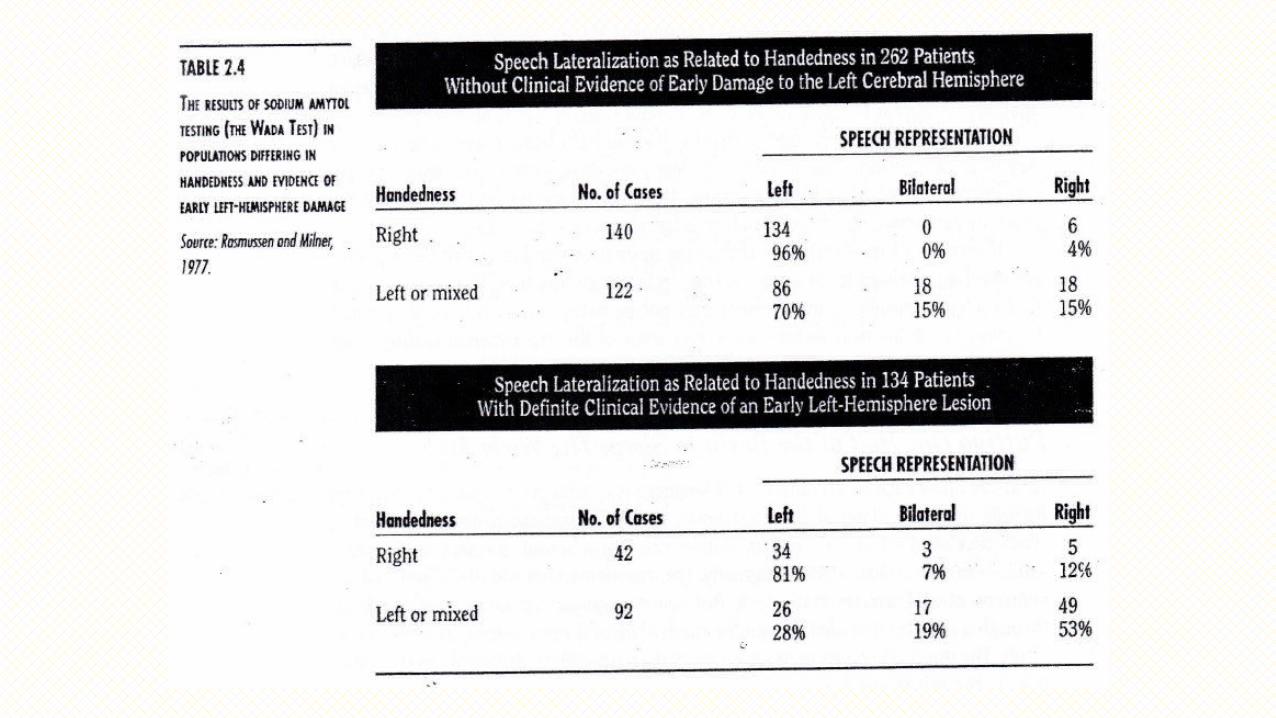
• Right/ left-handed/ ambidextrous left/ right/ tri lateralization for language? Early brain damage?
• Shifting of lateralization: Broca’s view that the right hemisphere can assume any language functions if damage occurs early enough. Rasmussen and Milner (1977) found that damage after five years of age rarely results in shift of laterality. – CPH
Splitting Apart the Hemispheres: Commissurotomy
• Introduced in 1940 by Van Wagenen as a treatment to prevent the spread of electrical discharges associated with epilepsy from one hemisphere to another.
• The aim of this surgery was to disconnect the two cerebral hemispheres.• After examining the first series of patients, no major effects involving
language was found (Akelaitis, 1964).
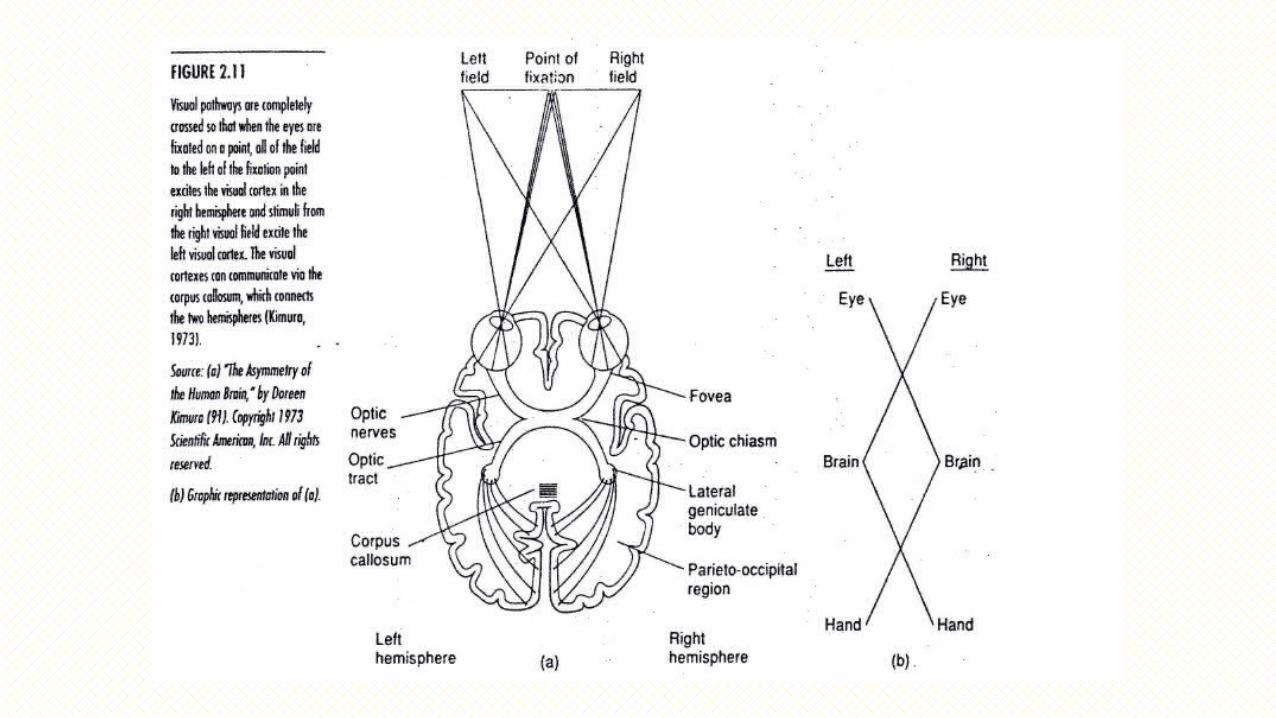
• All information presented to the right visual field is projected to the left (generally language dominant) hemisphere and vice versa.
• Myers (1955) sectioned both the corpus callosum and the optic chiasm in a group of laboratory animals. Corpus callosum’s function not only to hold both hemispheres together.• Experiment example: Monkeys.• Learning in one hemisphere totally fails to transfer to the other
hemisphere.
• In vast majority, only the dominant hemisphere can produce verbal output, but the nondominant hemisphere is not without language abilities.• Right hemisphere does have some language understanding, but it is
mute.
• Experiment example: Key.
• The left and right hemispheres operate together as a ‘team’.• Through the corpus callosum, messages are sent back and forth so
that both hemispheres are involved in much of the neurological activity of the human brain.
• Most problem solving involves the capacities of both hemispheres, and often the best solutions to problems are those in which each hemisphere has participated optimally (Danesi, 1988).
Taking Out Half the Brain:Hemispherectomy• In 1927, Walter Dandy introduced a procedure involving the total
removal of an entire hemisphere for the treatment of intractable epilepsy.
• In all cases of dominant hemispherectomy in adults, verbal and written output, while not totally obliterated, was severely affected. Comprehension appeared much less involved.
• Removal of the dominant hemisphere, no matter how early, does exact a toll; because the right hemisphere is incapable of acquiring all aspects of language even when the left hemisphere is removed at an early age.
Listening With Both Ears:The Dichotic Listening Technique• Evidence from normal individuals.
• The basic paradigm for this approach was created by Donald Broadbent (1954).• Presented subjects with a sequence of three digits to one ear, while
simultaneously presenting another sequence to the opposite ear.
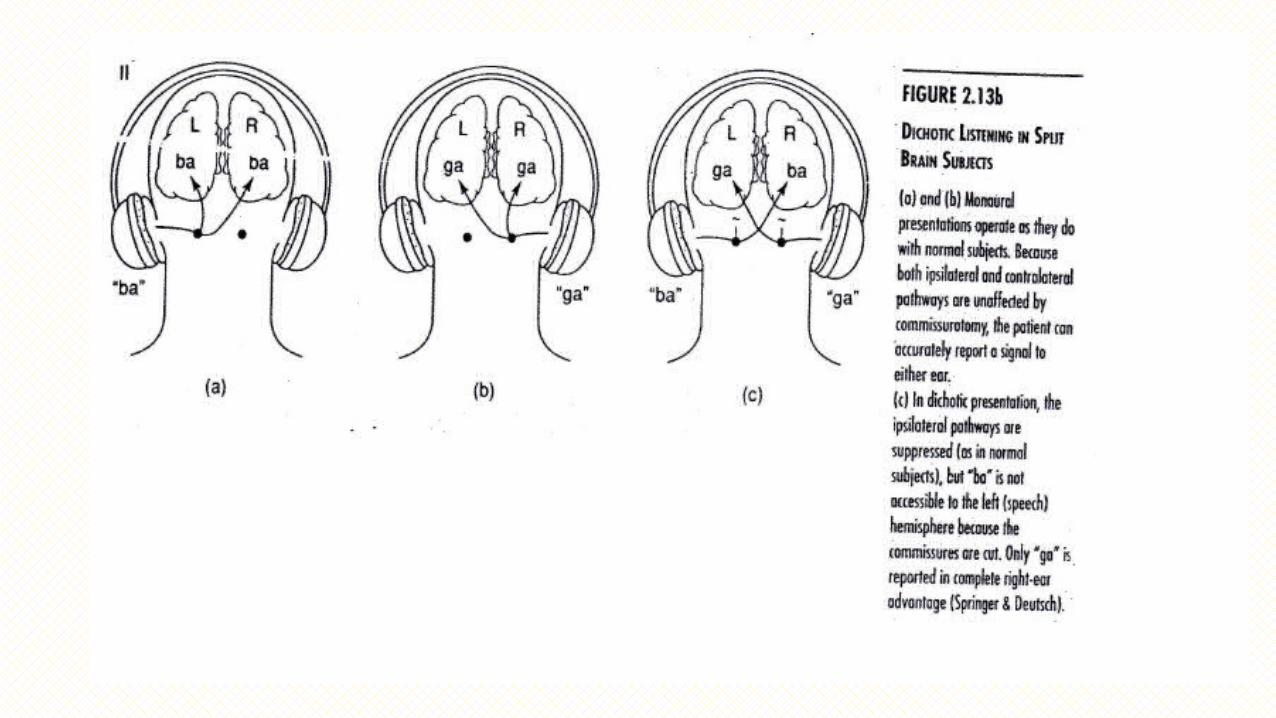
• In administering this test, Kimura (1961) discovered that digits presented to the ear contralateral to the dominant hemisphere were reported more accurately.
• Kimura attributed this effect to cerebral dominance, coupled with the greater strength of the contralateral pathways over ipsilateral (on the same side) ones.
• When stimuli were presented monaurally, the right ear advantage was not observed.
• The left hemisphere more quickly and accurately processes words (aural & written), identify letters and has an advantage when processing nonsense syllables and backward speech.
• The right hemisphere appears to do better when asked to process musical stimuli, human nonspeech stimuli (cough) and has an advantage during visual-spatial processing tasks.
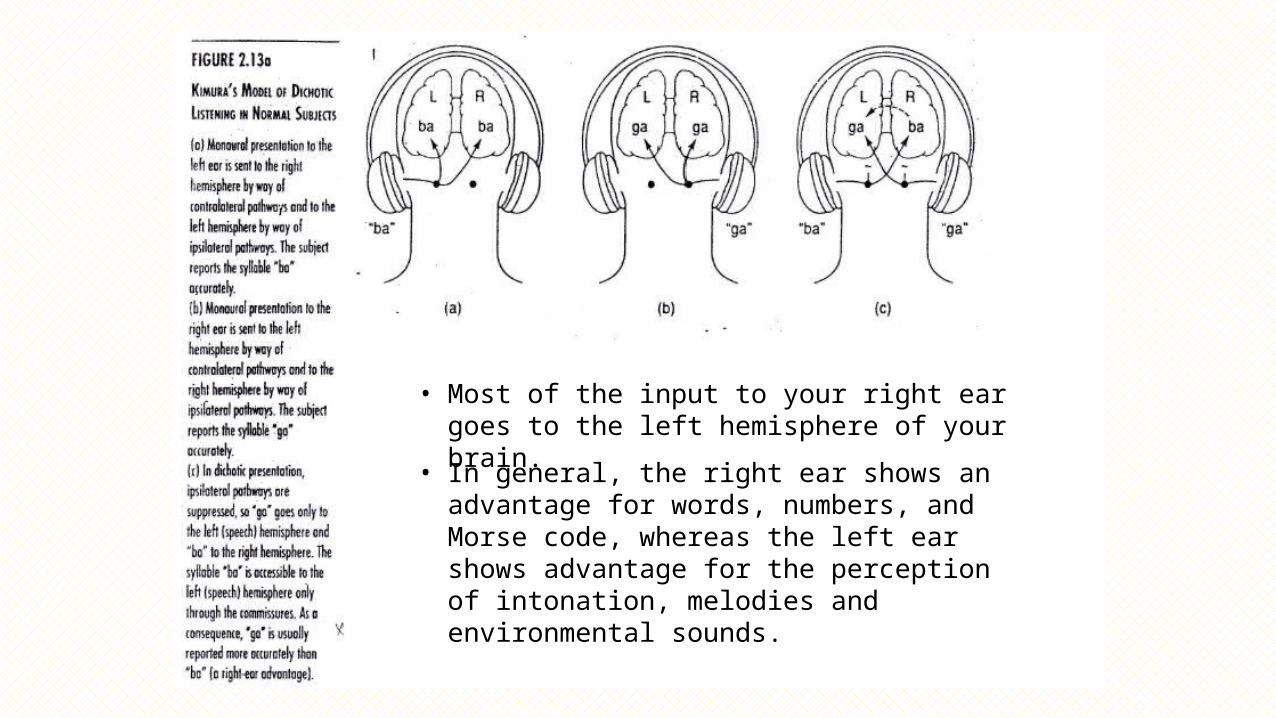
• Most of the input to your right ear goes to the left hemisphere of your brain.
• In general, the right ear shows an advantage for words, numbers, and Morse code, whereas the left ear shows advantage for the perception of intonation, melodies and environmental sounds.
Intrahemispheric Localization of Function
• It is clear that linguistic processing is not entirely confined to the dominant hemisphere. Both hemispheres are active during linguistic processing. Thus, laterality appears to be continuous rather than dichotomous (entirely different).
• Measuring Electrical Activity in the Brain• electrodes, radioactive isotopes
• Measuring Blood Flow in the Brain
Measuring Blood Flow in the Brain
• Neuroimaging methods: functional magnetic resonance imaging (fMRI) and magnetoencephalography (MEG) show involvement of both hemispheres in many aspects of language processing.• The "dominance" of one hemisphere just refers to more brain
activation relative to the other hemisphere (or better performance by that hemisphere on psycholinguistic tasks: dichotic listening); it is not the case that language is "localized" in any one hemisphere.
• Modern brain-imaging techniques such as fMRI and MEG have greatly increased our knowledge of where language processing takes place in the brain.
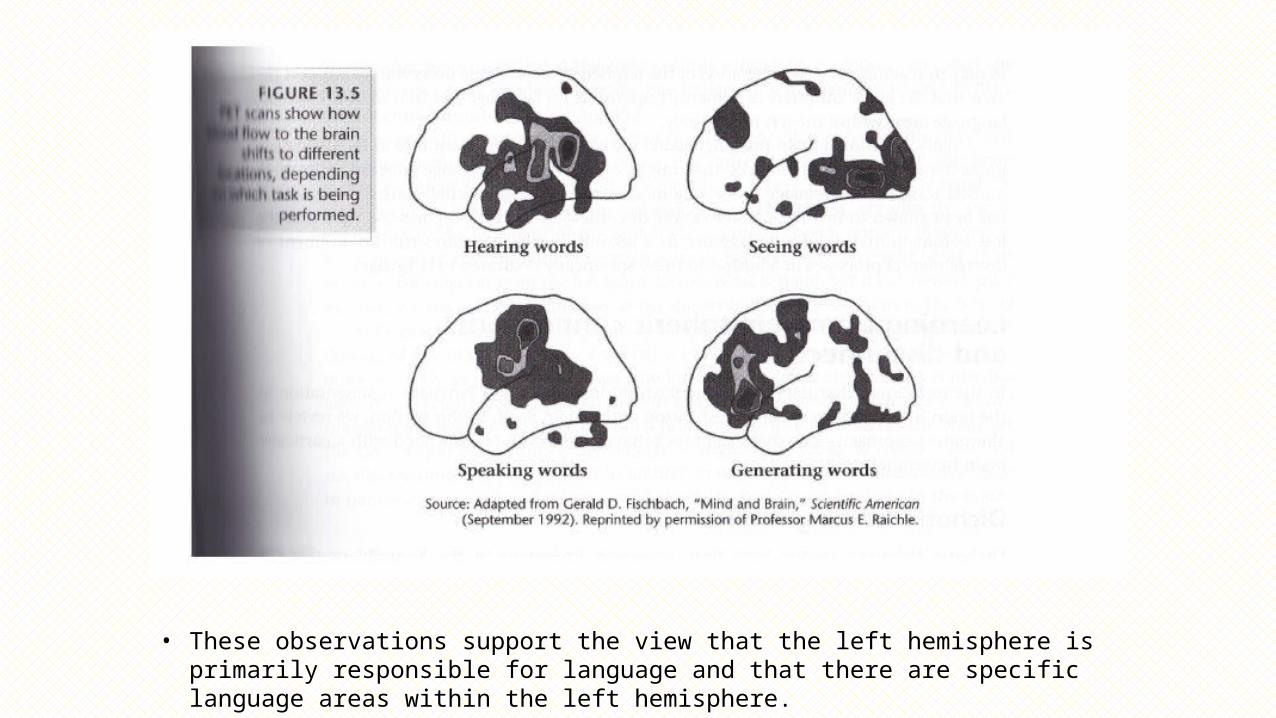
• These observations support the view that the left hemisphere is primarily responsible for language and that there are specific language areas within the left hemisphere.
AphasiaHeng Wen Zhuo
What is Aphasia?•OED: from Greek, from aphatos 'speechless', from a- 'not'
+ phanai 'speak‘
• Some semantic purist dislike the term aphasia, pointing our that some aphasic patients actually produce more speech than normal people do. (Freemon, F.R, 1981)
Classical model of Aphasia from Wernicke’s work
•Aphasia are the consequence of lesions of the language centres and/or connections, input and output pathways.
•Aphasias are not disorders of intelligence
• They occur in symptom groupings; essential syndromes are identified (motor, sensory, conduction aphasia)
Classical model of Aphasia from Wernicke’s work
•The syndromes depend on the localisation of the lesion
•Aphasias are the disorders of the normal flow of speech/ language processing
(Tesak & Code, 2008, p83)
What is Aphasia?• Acquired disorder of symbolic communication (Freemon, F.R, 1981)
• Difficulty in producing and understanding speech, reading , and writing
•What about those who are deaf ? Americal Sign Language(Goodglass and Kaplan , 1963)
• Specific disorder of higher cerebral function • Not applicable to everyone who does not speak (Freemon, F.R, 1981)
What is Aphasia?
•A disorder of linguistic processing. •Not a disorder of perception•Not a disorder of movement •Not a result of disordered thought processes.
(Mesulam, 2000)
What is Aphasia?•Aphasia not only disrupts communication but any ability
whose final performance depends on the use of internal speech.
- Decision making- Creativity - Ability to perform calculations
•often compromised because of a primary language defect (-Marsel Mesulam, 2000)
What is affected in Aphasia?
•Listening/ Speaking/ Reading/ Writing•Sign Languages•Gesture• Internal Speech ( Decision making, creativity and the ability to perform calculations) (Mesulam, 2000)
•Anxiety (if aware of their own condition)
What causes Aphasia?
Aphasia is the result of damage to the parts of brain related to Language. • Stroke (30 % suffer from aphasia)
• Severe Head injury• Cerebral Tumor• Degenerative Dementia • Health conditions that causes aphasia progressively : Alzheimer’s disease • Hydrocephalus - Anomia (most frequent aphasia)
Why study Aphasia?
•Aphasia caused by circumscribed brain dysfunction, •a valuable diagnostic tool in the localization of lesions and as a natural window on the functions of the human neurophysiology
•Promised to tell us about how the brain works and the role it plays in language function (Tesak & Code, 2008)
Types of Aphasia
• Fluent Aphasia VS Non-Fluent Aphasia
•mid of the 20th century, Goodglass and colleagues a major division between two types of aphasia : ‘phrase length’.
Fluent Aphasia
• Fluent - the defining characteristic• normal rate •without the effort and hesitation association with
non-fluent aphasia
• 4 types of Fluent Aphasia : Wernicke’s aphasia Transcortical sensory aphasiaConduction aphasia Anomia.
Non- Fluent Aphasia
• Speech: laborious & Halting
• Types of Non-Fluent AphasiaBroca’s Aphasia Transcortical motor aphasiaGlobal Aphasia
Broca Aphasia – Which area of the
brain ?•Becoming increasingly clear that the anterior language area is larger than previously supposed
•the area implicated in Broca’s aphasia was now taken “to encompass most of operculum, insula, and subjacent white matter, exceeding Broca’s area (Mohr 1976, p202) cited in (Grodzinsky, 2000).
Broca Aphasia - Which area of the
brain ?•Many researchers now consider that syntactic processing
takes place in Broca’s area and neighbouring regions
• ( operculum, insula, and subjacent white matter in which connections with other brain regions occur) (Grodzinsky & Amunts, 2006, p10)
• Basso, Lecours, Moraschini and Vanier (1985) and de Bleser (1988) Demonstrated that there is, at best, a weak association between site of lesion and syndrome.
Characteristics of Broca’s Aphasics• Speech: Laborious & Slow
• Lack melodic modulation
• Selection of words is often correct, especially for nouns, and less so for verbs and conjunctions.
•Physical weakness : right arm & right side of the face.
Characteristics of Broca’s Aphasics•Agrammatism• inability to organize words into grammatical sentences and
improper use or lack of use of grammatical morphemes and omit inflectional affixes
•Arnold Pick noted that word order is often retained correctly in agrammatic speakers, an indication that the sentence schema may be intact (Tesak & Code, 2008)
Characteristics of Broca’s Aphasics
Reason for Agrammatism: Economy of effort or Adaptation
ExampleDoctor: Could you tell me what you have been doing in the hospital?
Patient: Yes, sure, Me go, er, uh, P.T (physical theraphy) non o’cot, speech…two times… read…r.. ripe. .rike..uh write… practice…get… ting..better(Fromkin et al, 2007)
Characteristics of Broca’s Aphasics
•phonetic disintegration’ - distort the production of speech sounds (phonemes) and omit or add phonetic features that do not belong in the proper articulation of a given phoneme (eg: misproduction of /b/ for /p/)
•Difficulty discriminating closely related phonemes (such as /b/ for /p/)
Characteristics of Broca’s Aphasics
• In comprehension, Broca’s aphasics can construct basic syntactic trees (phrase structure) like active sentences,
•Difficulty recognizing the meaning of ‘reversible’ passive sentences such as ‘the girl was kissed by the boy’
•Patients seem to have no impairment in their lexicon in comprehension
Damage to Broca’s area alone?
•does NOT produce long-lasting severe aphasia; the surrounding areas and underlying white matter must be damaged as well.
• mild and transcient - ‘Broca’s area aphasia’. • Even more restricted damage - ‘aphemia’
Wernicke’s Area• no universally accepted boundary
• Usually defines as ‘the region which causes Wernicke’s aphasia when damaged.’• One of the very few lesion sites that elicits two-way naming
deficit
•May give impression of word representation storage, but unlikely
(Mesulam, 2000)
Wernicke’s Area
•Wernicke’s area coordinates reciprocal interactions between the sensory representation of word forms & arbitrary (second-order or symbolic) associations that give them meaning)
•NOT center for word selection.
(Mesulam, 2000)
Characteristics of Wernicke’s Aphasics• Speech : Fluent, produced at normal or faster than normal
rate , BUT does not make sense.•Melodic• Adhere to rules of syntax• Semantically incoherent
• Frequent errors in phoneme choice and word choice : Phonemic paraphasia & Semantic paraphasia
Characteristics of Wernicke’s Aphasics•Writing is formally very good• Good spelling and handwriting. • Their written production, however, like speaking, makes
little sense.
• Reading comprehension is severely impaired.• Auditory comprehension severely impairedWhy?
Characteristics of Wernicke’s Aphasics
linguistic deficits observed in Wernicke’s aphasics tend to be more lexical- semantic than those found in Broca’s Aphasia
Rarely have any motor impairment.
Conduction Aphasia
•Unable to repeat sentences verbatim •Phonemic paraphasia•Defective naming
•Able to produce and comprehend simple sentences
•Right facial weakness
Conduction Aphasia
•According to Geschwin (1965) , Lesion located in the arcuate fasciculus, the fibre tract that connects Broca’s and Wernicke’s areas
•Arcuate fasciculus is part of the system required to assemble phonemes into morphemes, necessary for vocalization of word perceived auditorily or generated internally, in the mind’s ear
Global Aphasia
•Almost complete loss of ability to comprehend language or formulate speech,
•Deliberate speech is reduced to a few words and sentences.
•May use the same word repeatedly in a vain attempt to communicate an idea.
Global Aphasia
• Some non-deliberate ‘automatic’ speech is preserved
• stock expletives, eg: ‘Goddamn it’- are used appropriately and with normal phonemic, phonetic and inflectional structures.
(Mesulam, 2000)
Global Aphasia
•Other ‘automatic’ speech routines , such as counting or reciting the days of the week, are often intact• the ability to sing parts of previously learned melodies
and their lyrics.
• right facial weakness and right hemiplegia (paralysis of one side of body)
(Mesulam, 2000)
Global Aphasia
• Presence or absence of hemiplegia is an important clue to the chance of recovery
•When hemiplegia is present, there is large degree of damage, patients severely aphasics from outset and show little or no improvement
•With transcient hemiplegia or no weakness, the patients tend to recover (Mesulam, 2000)
How about Right Hemisphere damage?
• Impairs a language ability known as discourse - tell or appreciate stories, jokes or write letters
Marked changes in Prosody , an ability which refers to inflections, stresses, and melody of speech
Aphasia Management
• No standard approach , each require customized program .• Following damage, the brain and its impaired
functions tend to show some degree of spontaneous recovery, assuming the cause of damage is removed.
• The fact that therapeutic intervention is beneficial is generally accepted.
Aphasia Management
Techniques• Melodic intonation therapy• Syntax training programmes• Visual Action Therapy• Sentence Level Auditory Comprehension Treatment programme• Visual Communication Therapy
(Mesulam, 2000)
Aphasia Management• In aphasia caused by stroke and head injury, the maximal
recovery seems to occur in the first 3 months following onset.
Factors affecting success of therapeutic intervention:• Premorbid characteristics of patient• Types and severity of language / non-language defect• Emotional status• Human support
80
When language goes wrong
Disorders of speaking, comprehension & reading
Acquired Dyslexia & Developmental Dyslexia
Goh Sue Yin
81
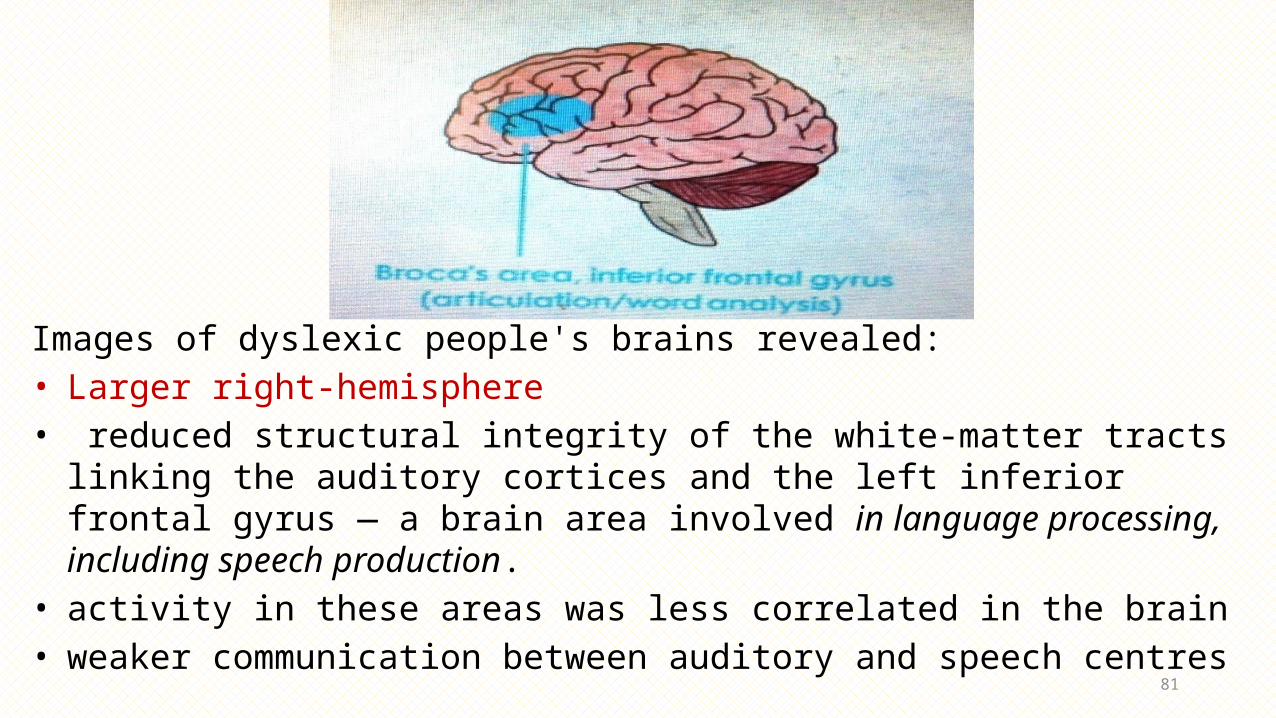
Images of dyslexic people's brains revealed:• Larger right-hemisphere • reduced structural integrity of the white-matter tracts linking the auditory cortices
and the left inferior frontal gyrus — a brain area involved in language processing, including speech production.
• activity in these areas was less correlated in the brain • weaker communication between auditory and speech centres
82
What isDYSLEXIA?• from dys - 'difficult' + Greek lexis 'speech' (apparently by confusion of Greek legein 'to speak' and Latin legere 'to read')• A learning difficulty that is neurological in origin• Affects the way people* read, write & spell*• A processing problem• A different way of thinking (visual)• A most widely known Learning Disability (LD)
NOTE!• No physical manifestation - Not linked to intelligence• Not a disease - Not the result of poor instruction
83
Type 1: Acquired dyslexia/Alexia
What causes? Few cases: injuries, stroke or some other type of traumaResult? A disorder where reading skills are lost
Type 2: Developmental Dyslexia
What causes? Common cases: Inherited, dyslexia often runs in families
- Wide range of people, producing different symptoms and varying degrees of severity
- 5 to 10% of the world’s populationResult? A disorder where the reading skills are not gained/reading difficulties
BothCanBe
DealtThe
SameWay
84
TypesACQUIRED DYSLEXIA
1. Phonological dyslexia: can read familiar words, lost ability to use spelling-to-sound rules
→ can only read familiar wordsExample: new word = blug (x)
2. Surface dyslexia: cannot recognise words as wholes→ can read regularly spelt wordsExample: regularly spelt word = bat /bǽt(√) irregularly spelt word = yacht /jɒt/(x)
→ understand the word produced, not what they seeExample: worm = /warm/ = opposite of cold
(O’Grady et al, 1996)
85
Reading New Word
•How do you know how to pronounce them?•A set of spelling-to-sound rules (LAD: language
acquisition device) •we hear it as a wholeExample: New word: blogFamiliar word: blue + log = /blɒg/
86
Reading Non visual words
•When people learn to read, their brains make connections between written symbols and components of spoken words.
•But people with dyslexia seem to have difficulty identifying and manipulating the speech sounds to be linked to written symbols
87
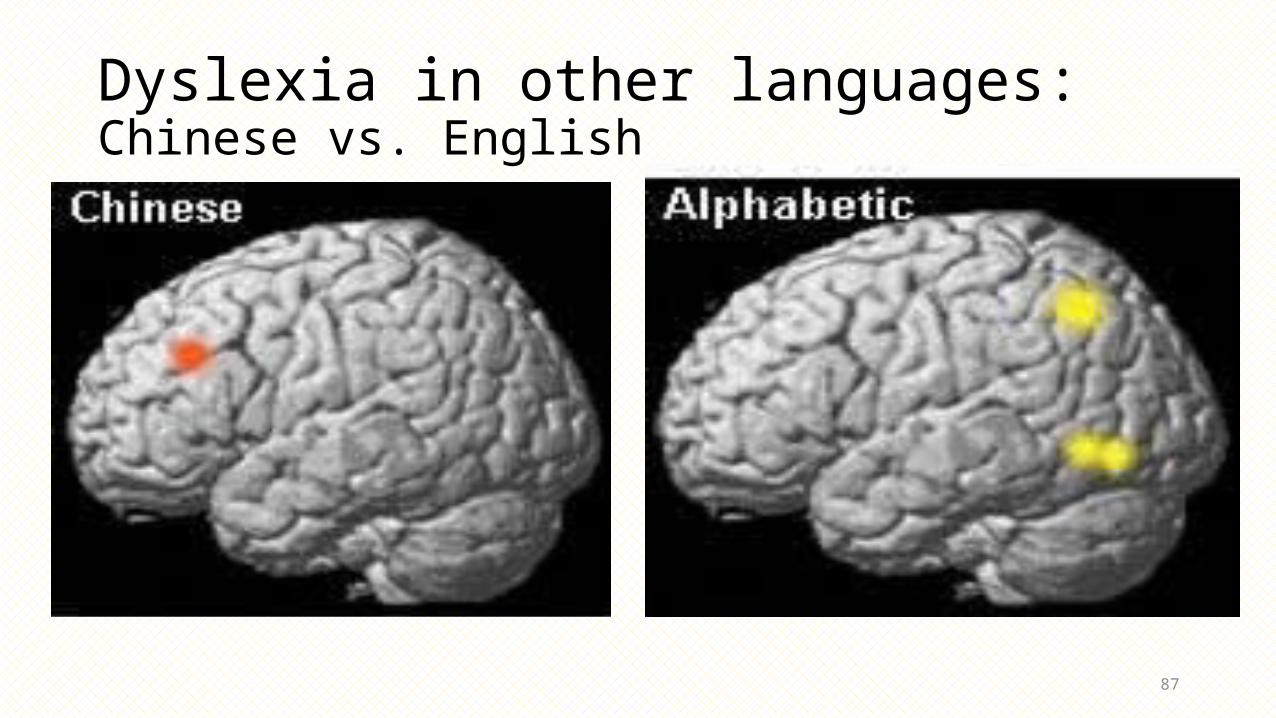
Dyslexia in other languages: Chinese vs. English
88
Chinese & English: A case study 2004, Tan L.H., University of Hong Kong
• examined patterns of activity in the brain of English and Chinese speakers
• the brain areas involved in dyslexia vary between languages
• English: reading involves translating letters into sounds and putting them together. • Chinese: reading involves memorizing a huge number of characters
• The differences between the two languages suggests that dyslexia could be two separate disorders.
89
Japanese vs. English : A case study Wydell T. N. & Butterworth B. B. Cognition, 70. 273 - 305(1999).
• one bilingual boy has reading problems in English, but none in Japanese• Japanese is a halfway house between alphabetic languages and
Chinese• Readers often have to match shapes to syllables, a different
task that is likely to involve a third, as yet unidentified brain region • The boy’s left temporoparietal cortex was probably under
active, whilst the unknown Japanese language-related area was fine
90
Languages: A comparison
91
Children with dyslexia have trouble learning to read, but the cause of their difficulties depends on what language they are attempting to
learn:
• “…you could be fine in one language and struggling in the other," (Gabrieli, 2008)
• "Previous genetic studies suggest that malformations of the brain are associated with different genes” (Tan L.H., 2004)
• “…neural basis of reading is complex and differs depending on the nature of the writing system,” (Wydell T. N. & Butterworth B. B.,1999)
92
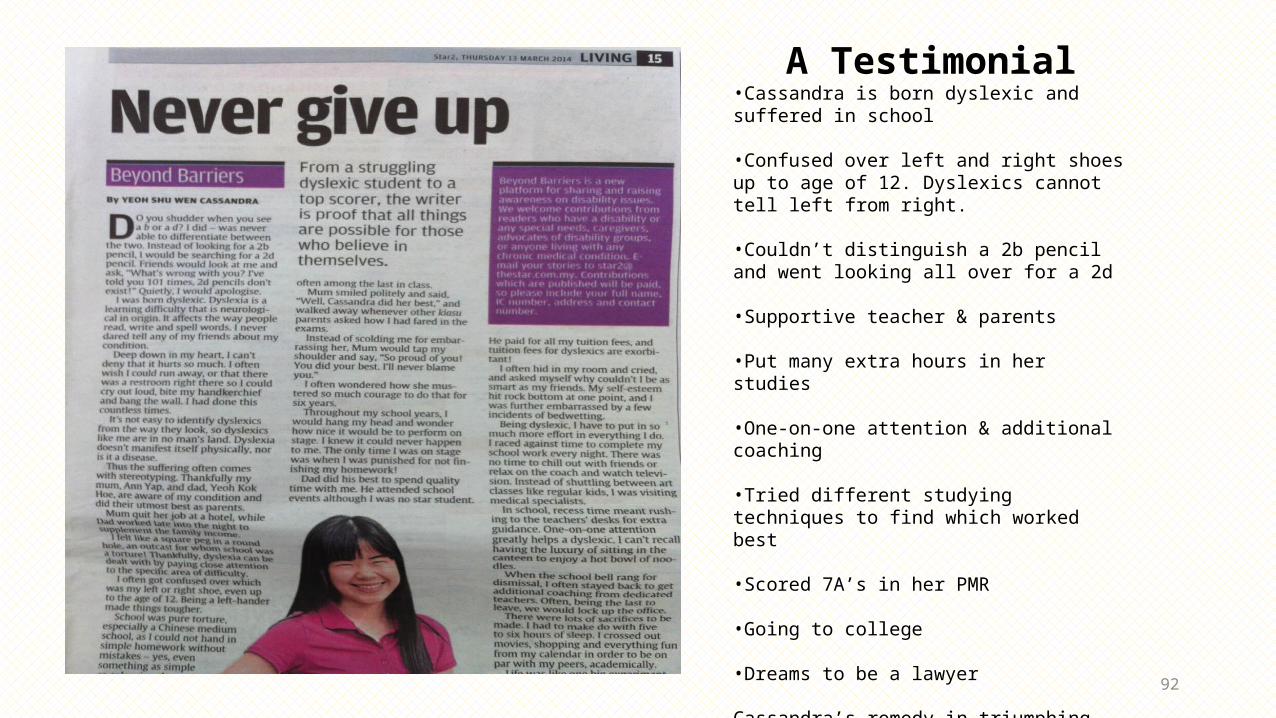
A Testimonial•Cassandra is born dyslexic and suffered in school
•Confused over left and right shoes up to age of 12. Dyslexics cannot tell left from right.
•Couldn’t distinguish a 2b pencil and went looking all over for a 2d
•Supportive teacher & parents
•Put many extra hours in her studies
•One-on-one attention & additional coaching
•Tried different studying techniques to find which worked best
•Scored 7A’s in her PMR
•Going to college
•Dreams to be a lawyer
Cassandra’s remedy in triumphing despite dyslexia: DETERMINATION!
93
Ways to overcome reading difficulties1. Visual wordsa) Add a pictureExample: - Blue cat- Lightning speedb) Use Sign LanguageExample:- Put this very beautiful flower in my house.
94
Ways to overcome reading difficulties2. Read fast! Example: - The blue teapot is next to the cups.-Use a 2B pencil for the exam.
* Reading by guessing through exposure. For adults.
95
People with dyslexia can be BRILLIANT!!
• Alexander Graham Bell - inventor of the telephone. • Lewis Carroll - author of Alice's Adventures in Wonderland. • Albert Einstein - physicist who developed the general theory of relativity. • Leonardo da Vinci - painter, scientist and mathematician. • Tom Cruise - actor. • Steve Jobs - co-founder of Apple Inc. • John Lennon - musician, one of The Beatles. • Jamie Oliver - celebrity chef. • Kanu Reeves - actor. • Steven Spielberg - film director.• Whoopi Goldberg - actress, film director.• Cher- singer, musician.• Muhammad Ali - boxer.• Walt Disney - creator
96
video
• http://www.youtube.com/watch?v=TxA_rvSNpx8• http://www.youtube.com/watch?v=UyyjU8fzEYU Important part : 11.17 mins & 12.40 mins
References
• Griggs, Richard A. Psychology: A Concise Introduction. p. 69.• Boeree, C.G. (2004). "Speech and the Brain". Retrieved February 17, 2012.• Taylor, I. & Taylor, M. M. (1990). Psycholinguistics: Learning and using Language. Pearson.• Beaumont, J.G. (2008). Introduction to Neuropsychology, Second Edition. The Guilford Press.• Ross ED, Monnot M (January 2008). "Neurology of affective prosody and its functional-anatomic organization in right
hemisphere". Brain Lang. 104 (1): 51–74.• George MS, Parekh PI, Rosinsky N, Ketter TA, Kimbrell TA, Heilman KM, Herscovitch P, Post RM (July 1996). "Understanding
Emotional Prosody Activates Right Hemisphere Regions". Arch Neurol. 53 (7): 665–670.• Brown, H.D. (2007). Principles of Language Learning and Teaching. New York: Pearson.• Berko-Gleason, J. & Bernstein-Ratner, N. (1998). Psycholinguistics. Orlando: Harcourt Brace.• O’Grady, W. & Dobrovolsky, M. (2011). Contemporary Linguistics. Toronto: Pearson.• Fromkin, V., Rodman, R., & Hyams, N. (2011, 2007, 2003). An introduction to language (9th Ed.): Wadworth cengage Learning.• O'Grady, W., & Archibald, J. (2012). Contemporary Linguistic Analysis (7th ed.). Toronto: Pearson Canada.• Yule, G. (2006). The study of language (3rd ed.). New york: Cambridge University press.• Fadiga, L., Craighero, L., & D’Ausilioa, A. (2009). Broca’s Area in Language, Action, and Music. THE NEUROSCIENCES AND
MUSIC III—DISORDERS AND PLASTICITY.
Reference
Siegel, L.S., Paediatr. Child Health. 11(9), 581–587 (2006). Siok, W. T. et al. Proc. Natl Acad. Sci. USA 105, 5561-5566 (2008). Siok, W. T., Perfetti, C. A., Jin, Z. & Tan, L. H. Nature 431, 71-76 (2004). Wydell T. N. & Butterworth B. B. Cognition, 70. 273 - 305(1999). Mesulam, M.M (2000) Principles of Behavioral and Cognitive Neurology, second edition.
Oxford University Press http://www.ncld.org/types-learning-disabilities/dyslexia/what-is-dyslexia
Questions1. Please explain about the strip of brain issue at the rear of frontal lobe( name and functions ).
2. What was the main point of Mr. Gage story?
3. Is language lateralized only to a specific part of the brain? Please justify your answer.
4. Explain the Dichotic Listening Test with example
Questions
5. Based on the parts of the video clips shown from (Jill’s Stroke of insight), explain what was happening to her, by relating the phenomenon to what has been mentioned about Aphasia.
6. Perform a dialogue between a non-aphasic individual, and an aphasic individual (either Broca’s aphasics or Wernicke’s aphasic).
Questions•7. In this fast moving technology era, do you think
dyslexics find life easier or more challenging? Support your answer with 2 justifications.
•8. If a child cannot tell his left shoe from his right shoe by the age of 7 or 8, he is most likely dyslexic.
a) What can be done to help him put on his shoes correctly?b) Why will your suggestions be successful?
The End
Thank You
Stress ???
@ .@
Gambateh Yo!!
![Comparing Risky Prospects - Lecture Slides › ... › lecture-slides › MIT14_121F15_7S.pdf · Complete Dominance Orderings [Optional] FOSD and SOSD are partial orders on lotteries:](https://img.pdfslide.us/doc/110x75/5f1cabf61eef2c169556386d/comparing-risky-prospects-lecture-slides-a-a-lecture-slides-a-mit14121f157spdf.jpg)