Embed Size (px)
Citation preview

Competences, education and support for new roles in cancergenetics services: outcomes from the cancer genetics pilot projects
Catherine Bennett Æ Hilary Burton Æ Peter Farndon
Published online: 23 May 2007
� Springer Science+Business Media B.V. 2007
Abstract In 2004 the Department of Health in collabo-
ration with Macmillan Cancer Support set up service
development projects to pilot the integration of genetics in
mainstream medicine in the area of cancer genetics.
In developing these services, new roles and responsi-
bilities were devised that required supporting programmes
of education and training. The NHS National Genetics
Education and Development Centre has worked with the
projects to draw together their experience in these aspects.
New roles include the Cancer Family Nurse Specialist, in
which a nurse working in a cancer setting was trained to
identify and manage genetic or family history concerns,
and the Genetic Risk Assessment Practitioner—a small
team of practitioners working within a secondary care
setting to deliver a standardised risk assessment pathway.
Existing roles were also adapted for a different setting, in
particular the use of genetic counsellors working in a
community ethnic minority setting. These practitioners
undertook a range of clinical activities that can be mapped
directly to the ‘UK National Workforce Competences for
Genetics in Clinical Practice for Non-genetics Healthcare
Staff’ framework developed by Skills for Health and the
NHS National Genetics Education and Development
Centre (2007; draft competence framework). The main
differences between the various roles were in the ordering
of genetic tests and the provision of advice on invasive
preventive options such as mastectomy. Those involved in
service development also needed to develop competences
in project management, business skills, audit and evalua-
tion, working with users, general management (personnel,
multi-agency work and marketing), educational supervi-
sion, IT, public and professional outreach, and research.
Important resources to support the development of new
roles and competences included pathways and guidelines, a
formal statement of competences, a recognised syllabus,
appropriate and timely courses, the availability of a mentor,
supervision and opportunities to discuss cases, a formal
assessment of learning and continuing support from
specialist genetics services. This represents a current
resource gap that will be of concern to cancer networks
and a challenge to providers of educational resources and
regional genetics services.
Keywords Cancer genetics � Competences � Education �Genetics education � Roles � Service development
Abbreviations
GRAP Genetic risk assessment practitioner
GPwSI General practitioner with a special interest
NICE National Institute for Health and Clinical
Excellence
NHS National Health Service
PCT Primary Care Trust
C. Bennett (&)
NHS National Genetics Education and Development Centre,
Morris House, c/o Birmingham Women’s Hospital, Edgbaston,
Birmingham B15 2TG, UK
e-mail: [email protected]
H. Burton
Foundation for Genomics and Population Health, Cambridge,
UK
P. Farndon
West Midlands Regional Clinical Genetics Service, Birmingham
Women’s Hospital, Birmingham, UK
123
Familial Cancer (2007) 6:171–180
DOI 10.1007/s10689-007-9127-y

Introduction
The development of genetics in mainstream medicine is
one of the main themes of the Department of Health’s (DH)
2003 White Paper on genetics [2]. It recognised the
importance of genetic subsets of disease within most areas
of clinical medicine and funded service development pro-
jects which would pioneer new services and generate
valuable clinical experience of genetics in mainstream
medicine. Seven service development projects jointly
funded with Macmillan Cancer Support formed an impor-
tant subset in which the development of services for risk
assessment and cancer prevention based on family history
risk could be piloted.
Developing services for cancer genetics is important
because of the increased risk of disease in relation to family
history in breast, ovarian, colorectal cancer and other rarer
cancers with possibilities for preventive action. Methods to
stratify individuals with family history into high, moderate
and population risk have been devised. This allows iden-
tification of those with single gene mutations such as
BRCA1/2 or HNPCC for whom substantial preventive
action such as mastectomy or regular colonoscopy might
be appropriate; those for whom enhanced surveillance
options would be advised; and others who need general
prevention advice and reassurance. As a result of the high
absolute numbers of people in the population with a family
history of common cancers, practitioners who are not
specialists in genetics will need to be involved in initial
assessment and advice for those with concerns. This
represents a new set of activities in the community and the
cancer genetics pilots looked at ways of setting up appro-
priate models of service delivery.
At a workshop in November 2006, facilitated by the
NHS National Genetics Education and Development
Centre, representatives from the cancer genetics pilots met
to discuss their experiences in developing new roles and
their main needs for educational support and resources.
They identified the types of activities undertaken (e.g.
clinical, administrative etc.); the main clinical and
non-clinical activities required for new roles in cancer
genetics—including competences developed or needed;
the resources required for staff to achieve the competences
and fulfil their new roles (including, but not limited to,
education); and barriers and challenges to implementing
new roles. For completeness the workshop was followed
by a two-part questionnaire designed to collect compara-
ble summary information from all projects (part 1) and
all individuals undertaking new roles (part 2). The
latter part collected information on role title, education
and professional background; clinical and non-clinical
activities/competences including information on how the
competences were achieved; whether formal statements of
competences were developed for the role; important
educational development factors and resources used or
developed in fulfilling the role; and any other comments.
Experience was contributed by six of the seven projects
and by 11 individuals working in new cancer genetics roles
in mainstream medicine, 10 of whom were practitioners
who did not have specialist genetics expertise.
New roles in cancer genetics
The cancer genetics pilots involved the development of a
variety of new roles, reflecting the different aims and
emphases of the projects. Table 1 summarises the
responses received from six of the seven pilot projects and
the main substantive new roles that they described.
All projects involved the development and testing of
new models for delivering cancer genetics services which
were centrally funded for 3 years, with the hope and
expectation that the services would subsequently be inte-
grated into local funding. They were primarily delivered
locally in a primary care or community setting with the
joint aims of increasing uptake and enhancing efficiency
through reduction of hospital visits and demand on the
specialist department. One project used telephone consul-
tations. All projects required non-genetics practitioners to
undertake risk assessment activities within agreed proto-
cols and with close supervision. Although new job roles
were given different names, the commonest pattern was
for nurses with experience in primary care, community
nursing, or, more often, cancer nursing to gain the nec-
essary cancer genetics competences. In two projects where
there was a particular emphasis on increasing uptake in
lower socio-economic groups and ethnic minorities, nurses
with substantial experience in community development
and in working with ethnic minority communities were
recruited.
Some projects undertook further development of spe-
cialist genetic roles in order to support the new practitio-
ners who had more limited genetics expertise. For example,
in one project a genetic counsellor was involved in the
setting up and support of the primary care clinic. In an-
other, a special part-time role was created for an individual
with substantial experience in cancer care and in the setting
up and running of a cancer family history clinic to take
responsibility for the education and supervision of non-
genetics specialist practitioners. In other projects support
roles were undertaken by consultant geneticists and genetic
counsellors from the genetics service as part of their
commitment to the project.
172 C. Bennett et al.
123
Competences in clinical cancer genetics for
practitioners in new roles
Table 1 shows that the majority of the new roles were
developed, as anticipated, in mainstream services. In the
following analysis we concentrate on the new roles
undertaken by practitioners who were not genetic special-
ists (i.e. those who did not have professional specialist
accreditation in genetics, whether as clinical consultants or
genetic counsellors).
The NHS National Genetics Education and Develop-
ment Centre and Skills for Health have been collaborating
to develop a competence framework for genetics in clinical
practice for non-genetics healthcare staff [1]. Each
competence describes how an activity relating to genetics
should be carried out (‘performance criteria’) and the
underpinning knowledge and understanding required to
undertake the activity.
Although the competences cover the whole of the
pathway for a patient with, or at risk of, a genetic disorder,
for any individual health professional only those genetic
competences relevant to their professional role will be re-
quired. Some competences will be widely applicable and
others will be relevant only to a small number of specialist
healthcare professionals.
The genetics competence framework was in its final
consultation stage as the workshop was being planned with
the pilot projects. Discussions with the projects showed
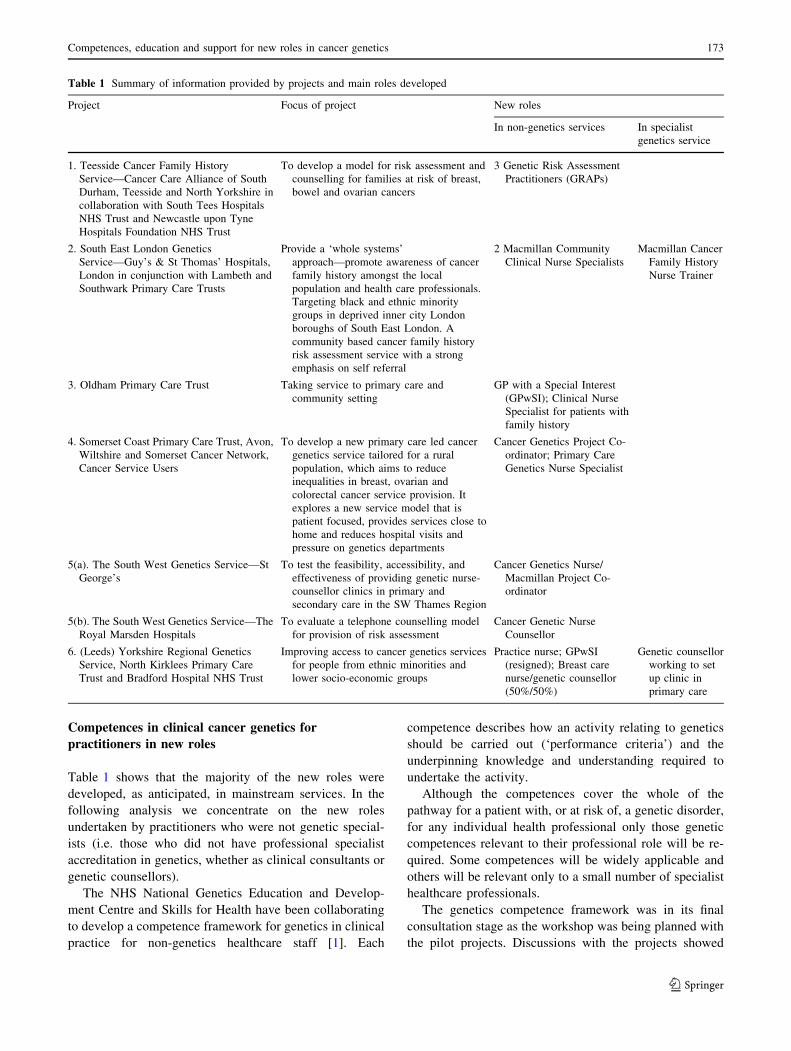
Table 1 Summary of information provided by projects and main roles developed
Project Focus of project New roles
In non-genetics services In specialist
genetics service
1. Teesside Cancer Family History
Service—Cancer Care Alliance of South
Durham, Teesside and North Yorkshire in
collaboration with South Tees Hospitals
NHS Trust and Newcastle upon Tyne
Hospitals Foundation NHS Trust
To develop a model for risk assessment and
counselling for families at risk of breast,
bowel and ovarian cancers
3 Genetic Risk Assessment
Practitioners (GRAPs)
2. South East London Genetics
Service—Guy’s & St Thomas’ Hospitals,
London in conjunction with Lambeth and
Southwark Primary Care Trusts
Provide a ‘whole systems’
approach—promote awareness of cancer
family history amongst the local
population and health care professionals.
Targeting black and ethnic minority
groups in deprived inner city London
boroughs of South East London. A
community based cancer family history
risk assessment service with a strong
emphasis on self referral
2 Macmillan Community
Clinical Nurse Specialists
Macmillan Cancer
Family History
Nurse Trainer
3. Oldham Primary Care Trust Taking service to primary care and
community setting
GP with a Special Interest
(GPwSI); Clinical Nurse
Specialist for patients with
family history
4. Somerset Coast Primary Care Trust, Avon,
Wiltshire and Somerset Cancer Network,
Cancer Service Users
To develop a new primary care led cancer
genetics service tailored for a rural
population, which aims to reduce
inequalities in breast, ovarian and
colorectal cancer service provision. It
explores a new service model that is
patient focused, provides services close to
home and reduces hospital visits and
pressure on genetics departments
Cancer Genetics Project Co-
ordinator; Primary Care
Genetics Nurse Specialist
5(a). The South West Genetics Service—St
George’s
To test the feasibility, accessibility, and
effectiveness of providing genetic nurse-
counsellor clinics in primary and
secondary care in the SW Thames Region
Cancer Genetics Nurse/
Macmillan Project Co-
ordinator
5(b). The South West Genetics Service—The
Royal Marsden Hospitals
To evaluate a telephone counselling model
for provision of risk assessment
Cancer Genetic Nurse
Counsellor
6. (Leeds) Yorkshire Regional Genetics
Service, North Kirklees Primary Care
Trust and Bradford Hospital NHS Trust
Improving access to cancer genetics services
for people from ethnic minorities and
lower socio-economic groups
Practice nurse; GPwSI
(resigned); Breast care
nurse/genetic counsellor
(50%/50%)
Genetic counsellor
working to set
up clinic in
primary care
Competences, education and support for new roles in cancer genetics 173
123
that the competence framework was equally applicable to
the work of the pilot projects and that their experiences
could be mapped directly to the competence statements in
the framework.
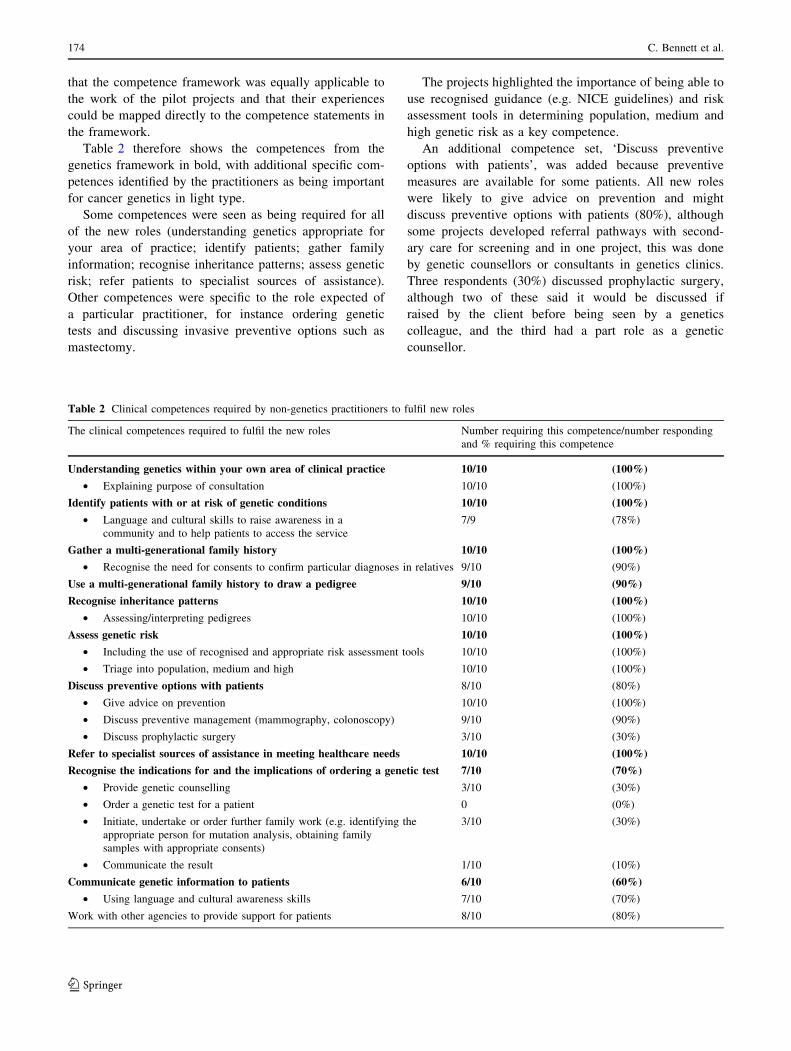
Table 2 therefore shows the competences from the
genetics framework in bold, with additional specific com-
petences identified by the practitioners as being important
for cancer genetics in light type.
Some competences were seen as being required for all
of the new roles (understanding genetics appropriate for
your area of practice; identify patients; gather family
information; recognise inheritance patterns; assess genetic
risk; refer patients to specialist sources of assistance).
Other competences were specific to the role expected of
a particular practitioner, for instance ordering genetic
tests and discussing invasive preventive options such as
mastectomy.
The projects highlighted the importance of being able to
use recognised guidance (e.g. NICE guidelines) and risk
assessment tools in determining population, medium and
high genetic risk as a key competence.
An additional competence set, ‘Discuss preventive
options with patients’, was added because preventive
measures are available for some patients. All new roles
were likely to give advice on prevention and might
discuss preventive options with patients (80%), although
some projects developed referral pathways with second-
ary care for screening and in one project, this was done
by genetic counsellors or consultants in genetics clinics.
Three respondents (30%) discussed prophylactic surgery,
although two of these said it would be discussed if
raised by the client before being seen by a genetics
colleague, and the third had a part role as a genetic
counsellor.
Table 2 Clinical competences required by non-genetics practitioners to fulfil new roles
The clinical competences required to fulfil the new roles Number requiring this competence/number responding
and % requiring this competence
Understanding genetics within your own area of clinical practice 10/10 (100%)
• Explaining purpose of consultation 10/10 (100%)
Identify patients with or at risk of genetic conditions 10/10 (100%)
• Language and cultural skills to raise awareness in a
community and to help patients to access the service
7/9 (78%)
Gather a multi-generational family history 10/10 (100%)
• Recognise the need for consents to confirm particular diagnoses in relatives 9/10 (90%)
Use a multi-generational family history to draw a pedigree 9/10 (90%)
Recognise inheritance patterns 10/10 (100%)
• Assessing/interpreting pedigrees 10/10 (100%)
Assess genetic risk 10/10 (100%)
• Including the use of recognised and appropriate risk assessment tools 10/10 (100%)
• Triage into population, medium and high 10/10 (100%)
Discuss preventive options with patients 8/10 (80%)
• Give advice on prevention 10/10 (100%)
• Discuss preventive management (mammography, colonoscopy) 9/10 (90%)
• Discuss prophylactic surgery 3/10 (30%)
Refer to specialist sources of assistance in meeting healthcare needs 10/10 (100%)
Recognise the indications for and the implications of ordering a genetic test 7/10 (70%)
• Provide genetic counselling 3/10 (30%)
• Order a genetic test for a patient 0 (0%)
• Initiate, undertake or order further family work (e.g. identifying the
appropriate person for mutation analysis, obtaining family
samples with appropriate consents)
3/10 (30%)
• Communicate the result 1/10 (10%)
Communicate genetic information to patients 6/10 (60%)
• Using language and cultural awareness skills 7/10 (70%)
Work with other agencies to provide support for patients 8/10 (80%)
174 C. Bennett et al.
123

Seven (70%) respondents agreed that recognising the
indications for and the implications of ordering a genetic
test was required for their role although two of these said
the patient would be referred on to specialist genetics
services. In this context of genetic testing, only three
respondents (30%) said they would provide genetic coun-
selling, and two of these specified that this would be at a
basic level (i.e. it was expected that patients would sub-
sequently be seen by colleagues within specialist genetics
services for further information, exploration of the issues
surrounding testing and for any genetic testing). Only three
respondents would initiate, undertake or order further
family work, and this might involve arranging blood stor-
age or discussing the most appropriate relative to test. In
most cases, these activities were carried out by specialist
genetics staff.
Six (60%) indicated the need for competence in com-
municating genetic information to patients. The fact that
this number was not 100% might indicate different
understandings of ‘genetic information’ in practitioners
from different professional backgrounds. A similar number
reported using language and cultural skills to raise aware-
ness in a community and to help patients to access the
service. Three quarters described the need to work with
other agencies in supporting patients. A good example of
this is the work with agencies involved in community
development to improve access for ethnic minority groups.
Supporting the gaining of competences for new
clinical roles
A number of important forms of resources for personal
development of competences were identified at the work-
shop. Through the questionnaire we aimed to assess the
importance of these across the range of projects, to identify
resources that were currently available and any that had
been developed by the projects. Table 3 gives a list of the
supporting resources with average scores (maximum 5) for
their importance and an indication of whether these were
available to new practitioners.
Support from genetics departments was considered the
most important factor for educational development and
most respondents said this was available to them. Two
projects said they developed consultation guidelines or
clinic proforma to steer and focus the consultation and
provide consistency across different project staff. Ongoing
support and mentorship included one-to-one sessions
with a genetics consultant or genetic counsellor. Projects
reported that clinical supervision or observation were
important either initially or throughout the project. The
opportunity to discuss cases was highly valued.
An example of a programme for training and support
developed by the Guy’s and St Thomas’ Project is given in
Box 1.
Box 1: Example of a programme for training and support
Initial training with attendance at an 8-day cancer genetics for health
care professionals course, attendance at genetics clinics and family
history clinics and the development and agreement of a learning
contract. Following a period of training, support and close
supervision in the clinics, the practitioner was assessed as being
competent to undertake the clinic alone through a formal process of
clinic observation and review of cancer risk in breast, ovarian and
colorectal cancer cases. A process of ongoing support and
supervision was then provided by review of risk assessments,
attendance at clinics, attendance at lectures and study days, and
ongoing provision of advice from genetic counsellors and
consultant clinical geneticists.
The availability of timely courses was seen as an
important priority. However, most respondents had not
been able to access nationally available (external) courses
and had to rely on training programmes organised locally.
Accessing the right course, at the appropriate level and at
the best time was an issue. This has implications for
resources for providing formal core genetics courses at a
national level:
‘‘I participated in a three day course in Cancer
Genetics but the educational level was very high and
that course was not of much help to me because I
took it at the start of my job when I didn’t know
anything about Genetics.’’
For most practitioners a mixed learning experience was
used and thought to be appropriate:
‘‘Competences were achieved by attending a course
in cancer genetics, reading articles and books, dis-
cussing issues with genetic counsellors and consul-
tants, attending cancer genetics clinic and doing
observations, mock sessions, conducting clinic under
supervision.’’
Respondents considered that understanding the scope of the
role and having a clear ‘syllabus’ for learning were
important for their educational development in the new
roles.
As job competences can be used to identify education
and training required for a particular role, those working in
new roles were asked whether formal statements of com-
petences had been developed for their role (Table 4).
Two projects did develop competence frameworks (see
Boxes 2 and 3) whilst others used the job description or
Competences, education and support for new roles in cancer genetics 175
123
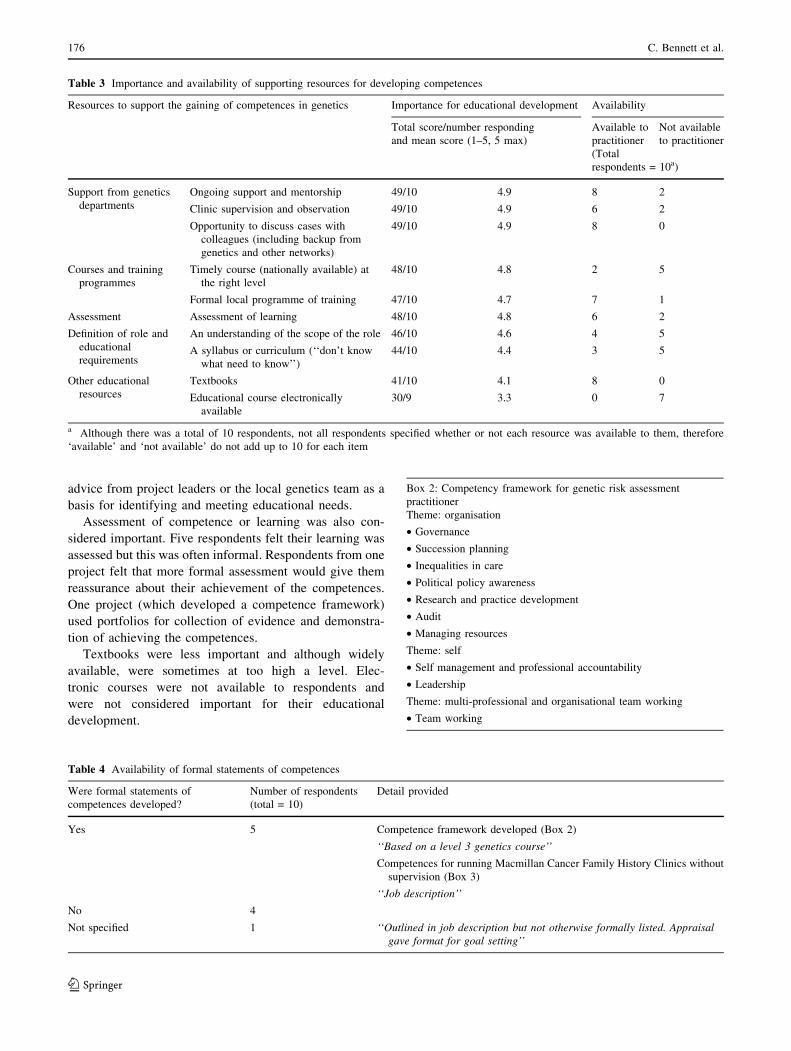
advice from project leaders or the local genetics team as a
basis for identifying and meeting educational needs.
Assessment of competence or learning was also con-
sidered important. Five respondents felt their learning was
assessed but this was often informal. Respondents from one
project felt that more formal assessment would give them
reassurance about their achievement of the competences.
One project (which developed a competence framework)
used portfolios for collection of evidence and demonstra-
tion of achieving the competences.
Textbooks were less important and although widely
available, were sometimes at too high a level. Elec-
tronic courses were not available to respondents and
were not considered important for their educational
development.
Table 3 Importance and availability of supporting resources for developing competences
Resources to support the gaining of competences in genetics Importance for educational development Availability
Total score/number responding
and mean score (1–5, 5 max)
Available to
practitioner
Not available
to practitioner
(Total
respondents = 10a)
Support from genetics
departments
Ongoing support and mentorship 49/10 4.9 8 2
Clinic supervision and observation 49/10 4.9 6 2
Opportunity to discuss cases with
colleagues (including backup from
genetics and other networks)
49/10 4.9 8 0
Courses and training
programmes
Timely course (nationally available) at
the right level
48/10 4.8 2 5
Formal local programme of training 47/10 4.7 7 1
Assessment Assessment of learning 48/10 4.8 6 2
Definition of role and
educational
requirements
An understanding of the scope of the role 46/10 4.6 4 5
A syllabus or curriculum (‘‘don’t know
what need to know’’)
44/10 4.4 3 5
Other educational
resources
Textbooks 41/10 4.1 8 0
Educational course electronically
available
30/9 3.3 0 7
a Although there was a total of 10 respondents, not all respondents specified whether or not each resource was available to them, therefore
‘available’ and ‘not available’ do not add up to 10 for each item
Table 4 Availability of formal statements of competences
Were formal statements of
competences developed?
Number of respondents
(total = 10)
Detail provided
Yes 5 Competence framework developed (Box 2)
‘‘Based on a level 3 genetics course’’
Competences for running Macmillan Cancer Family History Clinics without
supervision (Box 3)
‘‘Job description’’
No 4
Not specified 1 ‘‘Outlined in job description but not otherwise formally listed. Appraisalgave format for goal setting’’
Box 2: Competency framework for genetic risk assessment
practitioner
Theme: organisation
• Governance
• Succession planning
• Inequalities in care
• Political policy awareness
• Research and practice development
• Audit
• Managing resources
Theme: self
• Self management and professional accountability
• Leadership
Theme: multi-professional and organisational team working
• Team working
176 C. Bennett et al.
123
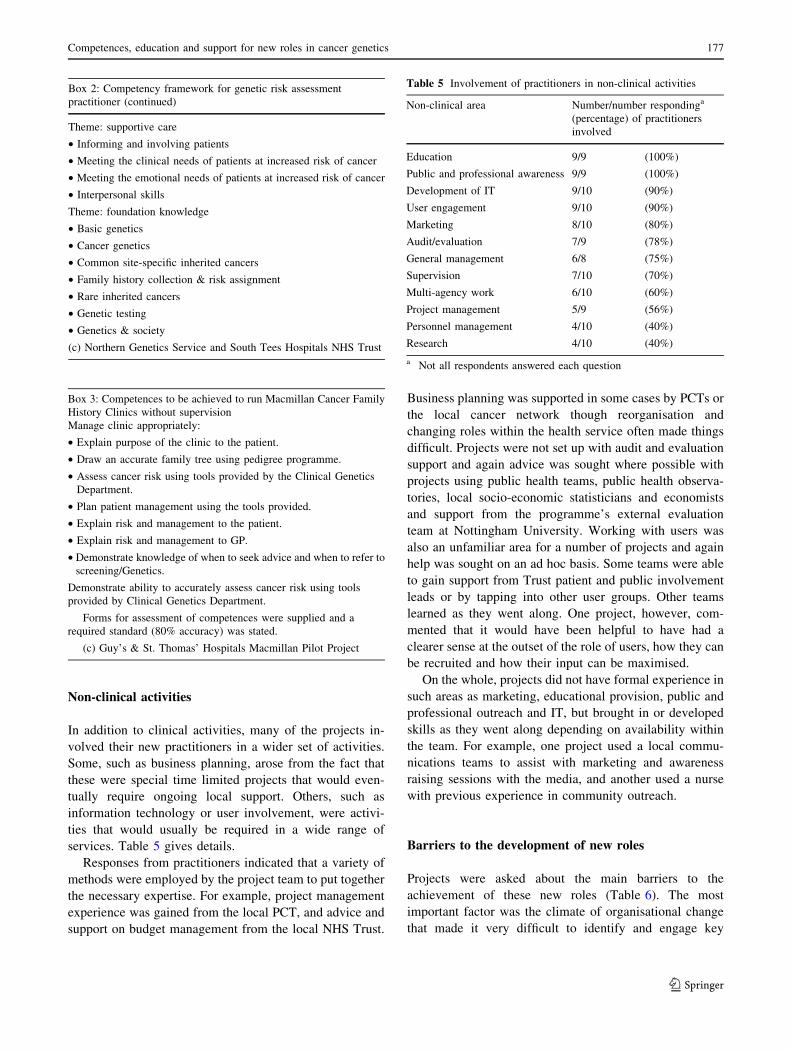
Non-clinical activities
In addition to clinical activities, many of the projects in-
volved their new practitioners in a wider set of activities.
Some, such as business planning, arose from the fact that
these were special time limited projects that would even-
tually require ongoing local support. Others, such as
information technology or user involvement, were activi-
ties that would usually be required in a wide range of
services. Table 5 gives details.
Responses from practitioners indicated that a variety of
methods were employed by the project team to put together
the necessary expertise. For example, project management
experience was gained from the local PCT, and advice and
support on budget management from the local NHS Trust.
Business planning was supported in some cases by PCTs or
the local cancer network though reorganisation and
changing roles within the health service often made things
difficult. Projects were not set up with audit and evaluation
support and again advice was sought where possible with
projects using public health teams, public health observa-
tories, local socio-economic statisticians and economists
and support from the programme’s external evaluation
team at Nottingham University. Working with users was
also an unfamiliar area for a number of projects and again
help was sought on an ad hoc basis. Some teams were able
to gain support from Trust patient and public involvement
leads or by tapping into other user groups. Other teams
learned as they went along. One project, however, com-
mented that it would have been helpful to have had a
clearer sense at the outset of the role of users, how they can
be recruited and how their input can be maximised.
On the whole, projects did not have formal experience in
such areas as marketing, educational provision, public and
professional outreach and IT, but brought in or developed
skills as they went along depending on availability within
the team. For example, one project used a local commu-
nications teams to assist with marketing and awareness
raising sessions with the media, and another used a nurse
with previous experience in community outreach.
Barriers to the development of new roles
Projects were asked about the main barriers to the
achievement of these new roles (Table 6). The most
important factor was the climate of organisational change
that made it very difficult to identify and engage key
Box 2: Competency framework for genetic risk assessment
practitioner (continued)
Theme: supportive care
• Informing and involving patients
• Meeting the clinical needs of patients at increased risk of cancer
• Meeting the emotional needs of patients at increased risk of cancer
• Interpersonal skills
Theme: foundation knowledge
• Basic genetics
• Cancer genetics
• Common site-specific inherited cancers
• Family history collection & risk assignment
• Rare inherited cancers
• Genetic testing
• Genetics & society
(c) Northern Genetics Service and South Tees Hospitals NHS Trust
Box 3: Competences to be achieved to run Macmillan Cancer Family
History Clinics without supervision
Manage clinic appropriately:
• Explain purpose of the clinic to the patient.
• Draw an accurate family tree using pedigree programme.
• Assess cancer risk using tools provided by the Clinical Genetics
Department.
• Plan patient management using the tools provided.
• Explain risk and management to the patient.
• Explain risk and management to GP.
• Demonstrate knowledge of when to seek advice and when to refer to
screening/Genetics.
Demonstrate ability to accurately assess cancer risk using tools
provided by Clinical Genetics Department.
Forms for assessment of competences were supplied and a
required standard (80% accuracy) was stated.
(c) Guy’s & St. Thomas’ Hospitals Macmillan Pilot Project
Table 5 Involvement of practitioners in non-clinical activities
Non-clinical area Number/number respondinga
(percentage) of practitioners
involved
Education 9/9 (100%)
Public and professional awareness 9/9 (100%)
Development of IT 9/10 (90%)
User engagement 9/10 (90%)
Marketing 8/10 (80%)
Audit/evaluation 7/9 (78%)
General management 6/8 (75%)
Supervision 7/10 (70%)
Multi-agency work 6/10 (60%)
Project management 5/9 (56%)
Personnel management 4/10 (40%)
Research 4/10 (40%)
a Not all respondents answered each question
Competences, education and support for new roles in cancer genetics 177
123
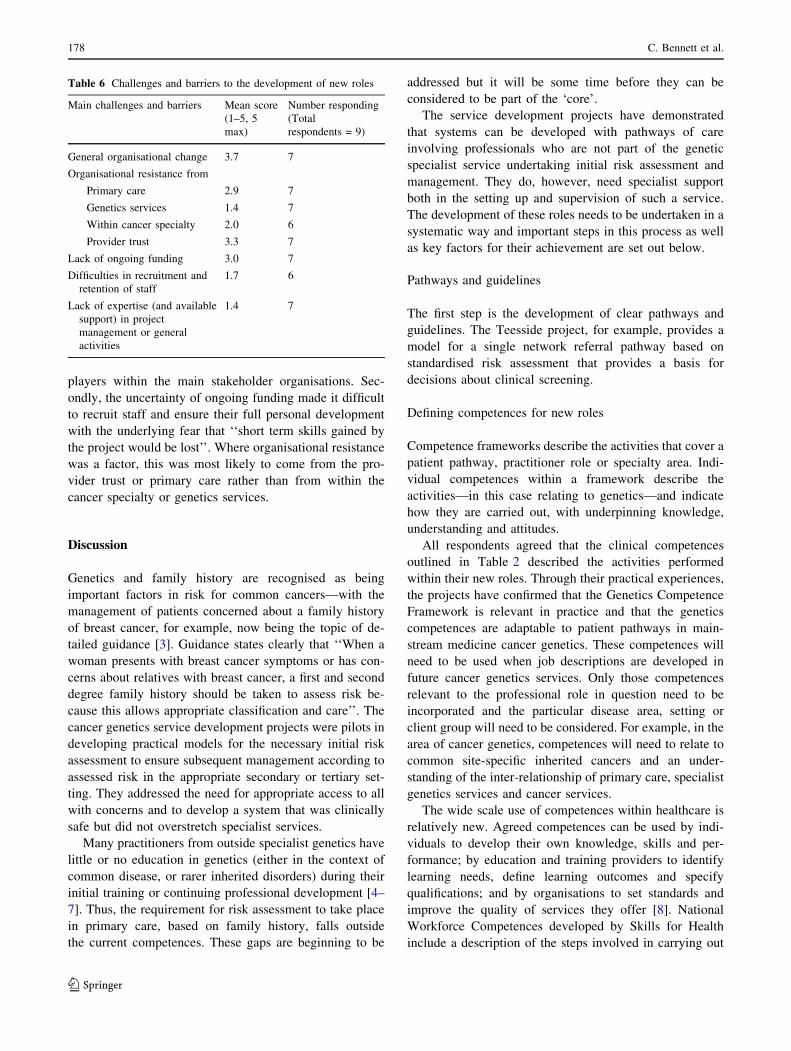
players within the main stakeholder organisations. Sec-
ondly, the uncertainty of ongoing funding made it difficult
to recruit staff and ensure their full personal development
with the underlying fear that ‘‘short term skills gained by
the project would be lost’’. Where organisational resistance
was a factor, this was most likely to come from the pro-
vider trust or primary care rather than from within the
cancer specialty or genetics services.
Discussion
Genetics and family history are recognised as being
important factors in risk for common cancers—with the
management of patients concerned about a family history
of breast cancer, for example, now being the topic of de-
tailed guidance [3]. Guidance states clearly that ‘‘When a
woman presents with breast cancer symptoms or has con-
cerns about relatives with breast cancer, a first and second
degree family history should be taken to assess risk be-
cause this allows appropriate classification and care’’. The
cancer genetics service development projects were pilots in
developing practical models for the necessary initial risk
assessment to ensure subsequent management according to
assessed risk in the appropriate secondary or tertiary set-
ting. They addressed the need for appropriate access to all
with concerns and to develop a system that was clinically
safe but did not overstretch specialist services.
Many practitioners from outside specialist genetics have
little or no education in genetics (either in the context of
common disease, or rarer inherited disorders) during their
initial training or continuing professional development [4–
7]. Thus, the requirement for risk assessment to take place
in primary care, based on family history, falls outside
the current competences. These gaps are beginning to be
addressed but it will be some time before they can be
considered to be part of the ‘core’.
The service development projects have demonstrated
that systems can be developed with pathways of care
involving professionals who are not part of the genetic
specialist service undertaking initial risk assessment and
management. They do, however, need specialist support
both in the setting up and supervision of such a service.
The development of these roles needs to be undertaken in a
systematic way and important steps in this process as well
as key factors for their achievement are set out below.
Pathways and guidelines
The first step is the development of clear pathways and
guidelines. The Teesside project, for example, provides a
model for a single network referral pathway based on
standardised risk assessment that provides a basis for
decisions about clinical screening.
Defining competences for new roles
Competence frameworks describe the activities that cover a
patient pathway, practitioner role or specialty area. Indi-
vidual competences within a framework describe the
activities—in this case relating to genetics—and indicate
how they are carried out, with underpinning knowledge,
understanding and attitudes.
All respondents agreed that the clinical competences
outlined in Table 2 described the activities performed
within their new roles. Through their practical experiences,
the projects have confirmed that the Genetics Competence
Framework is relevant in practice and that the genetics
competences are adaptable to patient pathways in main-
stream medicine cancer genetics. These competences will
need to be used when job descriptions are developed in
future cancer genetics services. Only those competences
relevant to the professional role in question need to be
incorporated and the particular disease area, setting or
client group will need to be considered. For example, in the
area of cancer genetics, competences will need to relate to
common site-specific inherited cancers and an under-
standing of the inter-relationship of primary care, specialist
genetics services and cancer services.
The wide scale use of competences within healthcare is
relatively new. Agreed competences can be used by indi-
viduals to develop their own knowledge, skills and per-
formance; by education and training providers to identify
learning needs, define learning outcomes and specify
qualifications; and by organisations to set standards and
improve the quality of services they offer [8]. National
Workforce Competences developed by Skills for Health
include a description of the steps involved in carrying out
Table 6 Challenges and barriers to the development of new roles
Main challenges and barriers Mean score
(1–5, 5
max)
Number responding
(Total
respondents = 9)
General organisational change 3.7 7
Organisational resistance from
Primary care 2.9 7
Genetics services 1.4 7
Within cancer specialty 2.0 6
Provider trust 3.3 7
Lack of ongoing funding 3.0 7
Difficulties in recruitment and
retention of staff
1.7 6
Lack of expertise (and available
support) in project
management or general
activities
1.4 7
178 C. Bennett et al.
123

each activity (‘performance criteria’) as well as the
underpinning knowledge and understanding required. This
level of detail has not usually been included at the role
level for individual practitioners. Although five practitio-
ners responded that formal statements of competences had
been defined for their new roles (Table 4), in many cases
job descriptions or less formal discussions with project
staff were being used and only two competence frame-
works were provided. Explicit statements of what is in-
volved in new roles (activities along the patient pathway)
and how these should be achieved will be vital to helping
new practitioners understand their role and to plan a
programme of personal development to achieve these
competences. As examples of cancer genetics competences
are specified for particular roles, the opportunity should be
taken to publicise and share them.
Resources to achieve competences
Building on an understanding of the competences, the next
step will be to develop an outline of the key points of the
course of study and personal development. It would be
helpful to achieve this at a national level, again by con-
sensus. Resources to meet these competences and course
outlines should then be identified and developed where
necessary.
How is this educational challenge to be met? Timely
courses (nationally available) at the right level were seen as
very important to the educational development of practi-
tioners working in new roles, but were not avail-
able—either at the right time or the right level—to most
respondents. The development of additional suitable
courses is one solution, but funding to develop and run
such courses would need to be provided, as well as funding
to support practitioners to attend. This might be difficult at
present when education budgets are increasingly threatened
in the NHS. Electronic courses are sometimes suggested as
a potential solution to the need to provide courses on-
demand, more regularly or to distant participants [9, 10].
None of our respondents had used an electronic course and
they did not perceive this to be a relevant solution to their
educational development. This perhaps reinforces the point
that use of electronic courses must be in the context of
available time for study and backed up by expert tuition
and educational support.
Support from specialist genetics services
For all projects, the most important element in individual
learning was the support of the genetics department,
including ongoing direction and mentorship, clinical
supervision and observation and continuing opportunities
to discuss cases with colleagues and with experts at the
genetics centre. Two projects did appoint genetic coun-
sellors to undertake and supervise the development of
nurse practitioners and in other services this was under-
taken as part of the role of consultant geneticists or genetic
counsellors associated with the project. For all projects, it
was important that the relationship of practitioners with the
specialist genetics department was formalised.
Such processes are clearly very demanding for specialist
genetics services, which already experience many requests
for education from primary care and a wide range of sec-
ondary care specialties in addition to their contribution to
pre- and post-registration training of medical, nursing and
other health professionals. Similar models requiring service
support are emerging in other clinical areas such as oph-
thalmology, renal and cardiac services. An initial conclu-
sion is that widespread development of mainstream
genetics services will need to be supported by increased
staffing levels in the specialist genetics services. This will
undoubtedly be part of the solution. However, the high
level of support provided by specialist services for these
projects might not be necessary for all in the longer term. It
will be important that specialist services provide education
and clinical support where they, alone, have the expertise
and that they work in conjunction with more general sup-
port at primary or secondary care level. For example, if
national competences, course outlines and appropriate
resources were available, an educational supervisor could
provide guidance on the general range of resources to be
accessed, leaving specialist services to concentrate on
ensuring clinical supervision and providing support for
complex cases.
For cancer genetics services it will be important for
cancer networks to work with specialist genetics services
and the NHS National Genetics Education and Develop-
ment Centre to develop a strategy for further developing
practitioners in mainstream services that makes best use of
available expertise on a national basis.
Conclusions and practice points
The pilot projects have highlighted the educational and
support needs of staff working in new roles in cancer
genetics. The NHS National Genetics Education and
Development Centre will work to disseminate information
from such projects, including job descriptions and com-
petence frameworks for different roles. It will also support
the Skills for Health competences and promote the devel-
opment of national resources. We hope that future cancer
genetics service developments will be able to build on
these resources to continue to provide high quality patient
care where activities involving genetics are integrated into
services.
Competences, education and support for new roles in cancer genetics 179
123

Acknowledgements The authors would like to acknowledge the
financial support of the Department of Health in funding the NHS
National Genetics Education and Development Centre and to thank
the cancer genetics pilot projects for sharing their experiences within
the workshop, completing the questionnaires, and for sharing
resources.
References
1. NHS National Genetics Education and Development Centre and
Skills for Health (2007) UK national workforce competences for
genetics in clinical practice for non-genetics healthcare staff.
Draft competence framework. http://www.geneticseduca-
tion.nhs.uk/develop/index.asp?id=44. Cited 20 Mar 2007
2. Department of Health (2003) Our inheritance, our future—real-
ising the potential of genetics in the NHS. Government white
paper. http://www.dh.gov.uk/en/Publicationsandstatistics/Publi-
cations/PublicationsPolicyAndGuidance/DH_4006538. Cited 20
Mar 2007
3. McIntosh A, Shaw C, Evans G et al (2004; updated 2006)
Clinical guidelines and evidence review for the classification and
care of women at risk of familial breast cancer, London, National
Collaborating Centre for Primary Care/University of Sheffield.
NICE guideline CG014. www.nice.org.uk. Cited 20 Mar 2007
4. Kirk M (1999) Preparing for the future: the status of genetics
education in diploma-level training courses for nurses in the
United Kingdom. Nurse Educ Today 19(2):107–115
5. Burton H (2002) Education in genetics for health professionals.
Report to the Wellcome Trust. Public Health Genetics Unit.
http://www.testsite.phgu.org.uk/resources/educ_project/educa-
tion-report.pdf. Cited 20 Mar 2007
6. Metcalfe A, Burton H (2003) Post-registration genetics education
provision for nurses, midwives and health visitors in the UK. J
Adv Nurs 44(4):350–359
7. Burke S, Stone A, Bedward J, Thomas H, Farndon P (2006) A
‘‘neglected part of the curriculum’’ or ‘‘of limited use’’? Views
on genetics training by non-genetics medical trainees and
implications for delivery. Genet Med 8(2):109–115
8. Skills for Health (2007) Completed frameworks. National occu-
pational standards and national workforce competences. http://
www.skillsforhealth.org.uk/frameworks.php. Cited 20 Mar 2007
9. Dames D, Handscomb A (2002) A pilot study to assess the case
for e-learning in the NHS. J Res Nurs 7(6):428–443
10. Childs S, Blenkinsopp E, Hall A, Walton G (2005) Effective e-
learning for health professionals and students—barriers and their
solutions. A systematic review of the literature—findings from
the HeXL project. Health Info Libr J 22(s2):20–32
Practice points
• Identify the patient pathways for your service and develop
consultation guidelines.
• Identify existing competences or develop competences appropriate
for job role.
• Use the agreed competences for the role to identify an individual
practitioner’s education and training requirements.
• Appoint a trainer for supervision of the educational development
plan.
• Identify resources to achieve and assess competences and ensure
these can be accessed.
• Ensure that specialist genetic support is available for supervision,
including opportunities to discuss cases.
180 C. Bennett et al.
123