Embed Size (px)
Citation preview

Competence, competency and pharmaceutical care:
The why, what and how of competence assessment
Competence, competency and pharmaceutical care:
The why, what and how of competence assessment
Graham Davies,Professor of Clinical Pharmacy & Therapeutics,King’s College, London
Graham Davies,Professor of Clinical Pharmacy & Therapeutics,King’s College, London

David Webb Ian BatesDenise Farmer Duncan McRobbieLizzie Mills Sotiris AntoniouLaura Obiols Naomi Meadows Roger Fernandes
FundingNWL WDC, NSC WDD and Department of Health (scoping higher level practice)
ObjectivesObjectives
Scene setting - why is competence important?Definitions:
- competence, competences, competencies- performance
Putting competence at the heart of care - the pharmacist development strategyMeasuring competence - the General Level Competency Framework
Scene setting - why is competence important?Definitions:
- competence, competences, competencies- performance
Putting competence at the heart of care - the pharmacist development strategyMeasuring competence - the General Level Competency Framework

Bristol Inquiry into Paediatric cardiac surgery -Kennedy Report (2000)Clinical governance & professional regulationAnti–professional attitude – professions are driven by self-interest and promotion.Public involvement (‘Informed consent’, Information and Choice)
Bristol Inquiry into Paediatric cardiac surgery -Kennedy Report (2000)Clinical governance & professional regulationAnti–professional attitude – professions are driven by self-interest and promotion.Public involvement (‘Informed consent’, Information and Choice)
Why is competence so important?Why is competence so important?

Why is competence so important?Why is competence so important?
‘A patient is entitled to be cared for and by healthcare professionals with relevant and up-to-date skills and expertise.’
Kennedy Report (p14)

Attaining Competence - Problems for PharmacistsAttaining Competence - Problems for Pharmacists
The service providedLack of clear career strategy with appropriate milestonesNo agreement on higher levels of practice – within and between pharmacy disciplinesVariability in quality of practice at junior and senior levelsNo succession planning
Education and trainingInequality of workforce access to structured, accredited learning experiencesDriven by academic attainment – divorced from service need and practitioner development
The service providedLack of clear career strategy with appropriate milestonesNo agreement on higher levels of practice – within and between pharmacy disciplinesVariability in quality of practice at junior and senior levelsNo succession planning
Education and trainingInequality of workforce access to structured, accredited learning experiencesDriven by academic attainment – divorced from service need and practitioner development

Outcome……………..for staff?Outcome……………..for staff?
Poor staff morale Poor job satisfactionPoor staff retentionPoor staff recruitment
Poor staff morale Poor job satisfactionPoor staff retentionPoor staff recruitment

Outcome……………..for service?Outcome……………..for service?
Increase pressure on existing staff Fire-fighting cultureLittle opportunity for service review or improvementInadequate risk management cultureIncrease in medication error
Increase pressure on existing staff Fire-fighting cultureLittle opportunity for service review or improvementInadequate risk management cultureIncrease in medication error

Why a competency approach?Why a competency approach?
PolicyFitness-for-purpose in the post Kennedy eraCommon NHS pay spine - Agenda for Changeand the Knowledge & Skills Framework
Research EvidenceResults of Clinical Skills Assessment
PolicyFitness-for-purpose in the post Kennedy eraCommon NHS pay spine - Agenda for Changeand the Knowledge & Skills Framework
Research EvidenceResults of Clinical Skills Assessment
Testing competence of pre-registration pharmacists
Objective Structured Clinical Examination (OSCE) of pre-registration pharmacists,Workstations to test required skills,Students rotate through stations,Set time in each station,Assessed against predetermined checklist.

Design of OSCE
6 baseline stations in at start of pre-registration year
15 stations at end of pre-registration year
7 minutes per station
Students assessed using checklists by experienced practitioners

Baseline workstations
Drug history takingInformation retrieval - medical notesResponding to symptomsTherapeutic Drug MonitoringDevice counsellingMedication counsellingHealth promotion

0
10%
20%
30%
40%
50%
60%
70%
1996/97 1997/98 1998/99 2001/02
Clinical Competence(OSCE)
Graduation
One year later
60%
30%
McRobbie et al
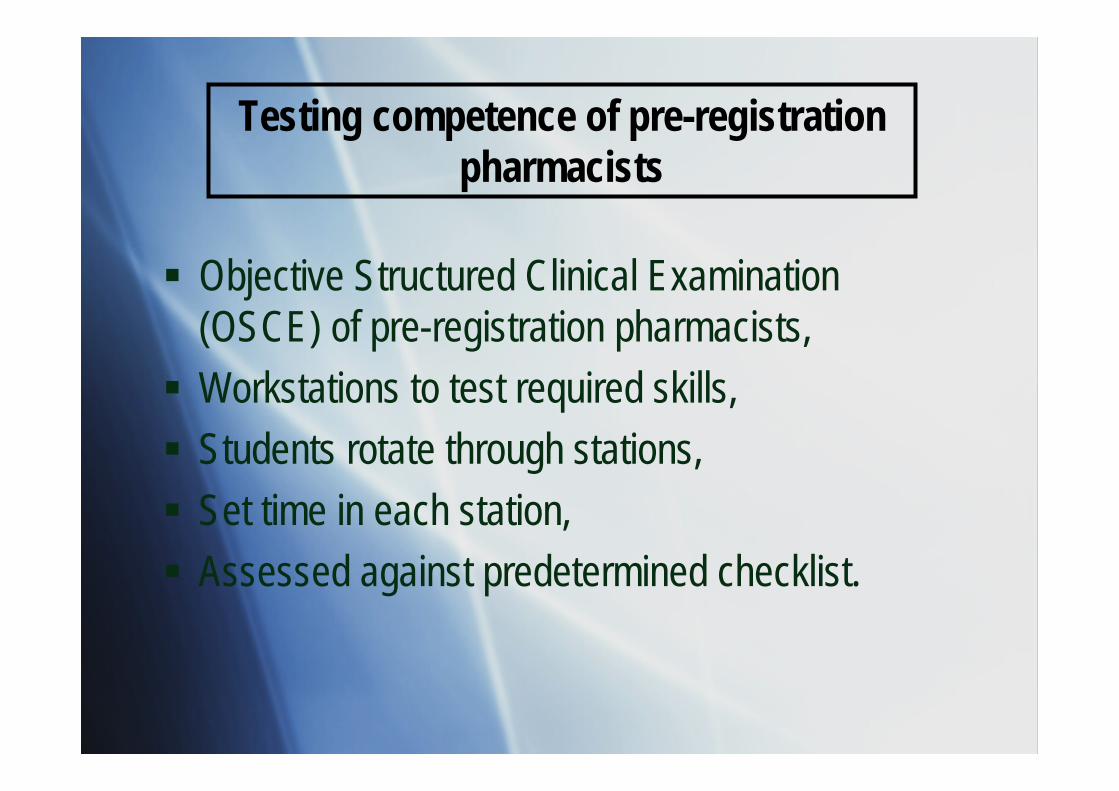
Registration
Total Comp Not Comp
Registered 136 93 43
Not Registered
20 9 11

Why a competency approach?Why a competency approach?
PolicyFitness-for-purpose in the post Kennedy eraCommon NHS pay spine - Agenda for Change and the Knowledge & Skills Framework
Research EvidenceResults of Clinical Skills AssessmentThe General Level Competency Framework
Accelerated and sustained performance(Antoniou et al. Pharmacy Education 2005)defines and makes explicit development needsachieves dynamic between workforce flexibility and competence
PolicyFitness-for-purpose in the post Kennedy eraCommon NHS pay spine - Agenda for Change and the Knowledge & Skills Framework
Research EvidenceResults of Clinical Skills AssessmentThe General Level Competency Framework
Accelerated and sustained performance(Antoniou et al. Pharmacy Education 2005)defines and makes explicit development needsachieves dynamic between workforce flexibility and competence

Competence approaches have their critics…..………Competence approaches have their critics…..………
Critical accountCritical accountCompetence approaches
ReductiveShopping listsJob specificCentral controlAdequacy
Competence approaches
ReductiveShopping listsJob specificCentral controlAdequacy

The problem with competency frameworks………….The problem with competency frameworks………….
Robust developmentValidity and Reliability
Duplication of effort –“Not invented here syndrome”Lack of testing and use of evidence – “Do they do what it says on the tin?”Lack of integration – silo mentality
Robust developmentValidity and Reliability
Duplication of effort –“Not invented here syndrome”Lack of testing and use of evidence – “Do they do what it says on the tin?”Lack of integration – silo mentality

Alternative departuresAlternative departures
Novice-to-expertDreyfus & Dreyfus 1986
5 stage progressionFrom adherence to intuitive graspReliable metric to identify expert?
Novice-to-expertDreyfus & Dreyfus 1986
5 stage progressionFrom adherence to intuitive graspReliable metric to identify expert?
Reflective practiceSchön 1983
Learning from experienceNecessary and sufficient?Cause or effect?
Reflective practiceSchön 1983
Learning from experienceNecessary and sufficient?Cause or effect?

Competency icebergCompetency iceberg
Effective and persistent behaviour
Knowledge
Skills
Abilities
Values, attitudes and beliefs

Competency…a complex constructCompetency…a complex construct
Skills
Behaviours
Knowledge
Valuesattitudes
Competency
Skills
Behaviours
Knowledge
Valuesattitudes
Competency
Skills
Behaviours
Knowledge
Valuesattitudes
Competency
Skills
Behaviours
Knowledge
Valuesattitudes
Competency

In search of the holy grailIn search of the holy grail
…………….assessing performance…………….assessing performance

Characteristics and Traits
Knowledge, Skills and Abilities
Competencies
Performance
Education and training
Integration
Experience
Innate
Developed
Bundled
Deployed
Competence and performanceCompetence and performance

Fuzzy conceptsFuzzy concepts
CompetenceOverarching capacity
CompetencesFunctional, the what
CompetenciesQualities, the how
CompetenceOverarching capacity
CompetencesFunctional, the what
CompetenciesQualities, the how

Professional competenceProfessional competence
Habitual and judicious use of communication, knowledge, technical skills, clinical reasoning, emotions, values, and reflection in daily practice for the benefit of the individual and community being served
Epstein and Hundert, 2002
Habitual and judicious use of communication, knowledge, technical skills, clinical reasoning, emotions, values, and reflection in daily practice for the benefit of the individual and community being served
Epstein and Hundert, 2002

Pharmacist Development StrategyPharmacist Development Strategy
……don’t consider competence in isolation……don’t consider competence in isolation

Key Ingredients of a StrategyKey Ingredients of a StrategyDescribe the key areas of practice & their associated outputs or competencies,Tool to measure competence of practitioners, Describe the curriculum to support development,Reform education system to deliver curriculum,Overarching body to award statements of completion of training.Workforce Planning Data – how many?
Describe the key areas of practice & their associated outputs or competencies,Tool to measure competence of practitioners, Describe the curriculum to support development,Reform education system to deliver curriculum,Overarching body to award statements of completion of training.Workforce Planning Data – how many?

Higher Level Development Phase
Practice development strategy
General Level Development
PhaseUndergraduate & Pre-registration Phases
General Level Practitioner
Advanced Practitioner
Higher Level Development Phase 2
1Consultant Practitioner
General Level Framework
Higher Level Framework: Advanced & Consultant

The General Level FrameworkThe General Level Framework
Design and EvaluationDesign and Evaluation

Framework StructureFramework StructureCompetency models
OutcomeEducationalPersonal
General Level FrameworkHybridDerived by recognised process
Agenda for Change - NHS common pay spine.Adopts a generic evaluation framework (the Knowledge and Skills Framework {KSF}) – with gateways GLF consistent with requirements of KSFGLF enables KSF – provides evidence of care made.
Competency modelsOutcomeEducationalPersonal
General Level FrameworkHybridDerived by recognised process
Agenda for Change - NHS common pay spine.Adopts a generic evaluation framework (the Knowledge and Skills Framework {KSF}) – with gateways GLF consistent with requirements of KSFGLF enables KSF – provides evidence of care made.

Structure of the GLFStructure of the GLF

Competency Framework: General Level
PERSONAL PROBLEM MANAGEMENT
DELIVERYOF
PATIENTCARE
Organisation, Team working,Communication,Professionalism
Drug use
process
Gathers informationKnow ledge
Analyses InformationProvides information
Follows up and reflects
PunctualityInitiative
Confidentiality
Drug history takingInteraction identification
Patient counselling
Assesses informationAccurate providesRelevant, Timely
McRobbie, Webb, Bates, Davies, Wright 2001


GLF structureGLF structure
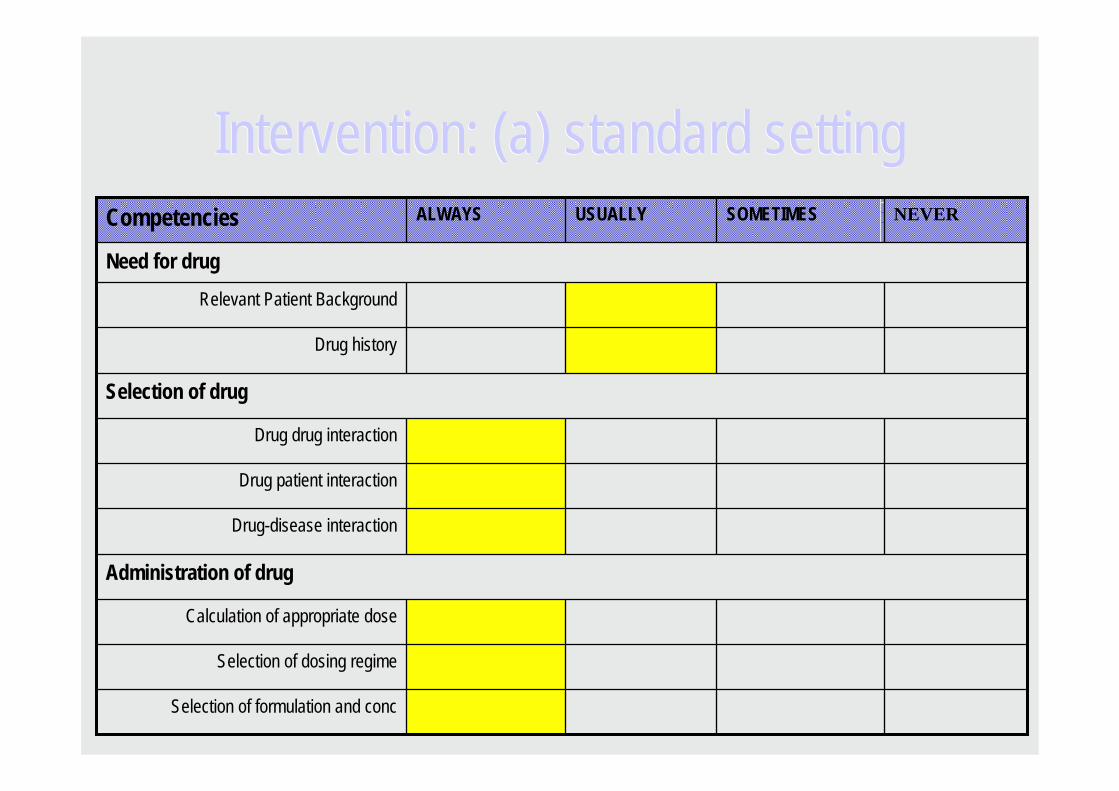
Selection of formulation and conc
Selection of dosing regime
Calculation of appropriate dose
Administration of drug
Drug-disease interaction
Drug patient interaction
Drug drug interaction
Selection of drug
Drug history
Relevant Patient Background
Need for drug
NEVERSOMETIMESUSUALLYALWAYSCompetencies
Intervention: (a) standard settingIntervention: (a) standard setting

Selection of formulation and conc
Selection of dosing regime
Calculation of appropriate dose
Administration of drug
Drug-disease interaction
Drug patient interaction
Drug drug interaction
Selection of drug
Drug history
Relevant Patient Background
Need for drug
NEVERSOMETIMESUSUALLYALWAYSCompetencies
(b) performance measurement(b) performance measurement

Selection of formulation and conc
Selection of dosing regime
Calculation of appropriate dose
Administration of drug
Drug-disease interaction
Drug patient interaction
Drug drug interaction
Selection of drug
Drug history
Relevant Patient Background
Need for drug
NEVERSOMETIMESUSUALLYALWAYSCompetencies
(c) performance improvement(c) performance improvement

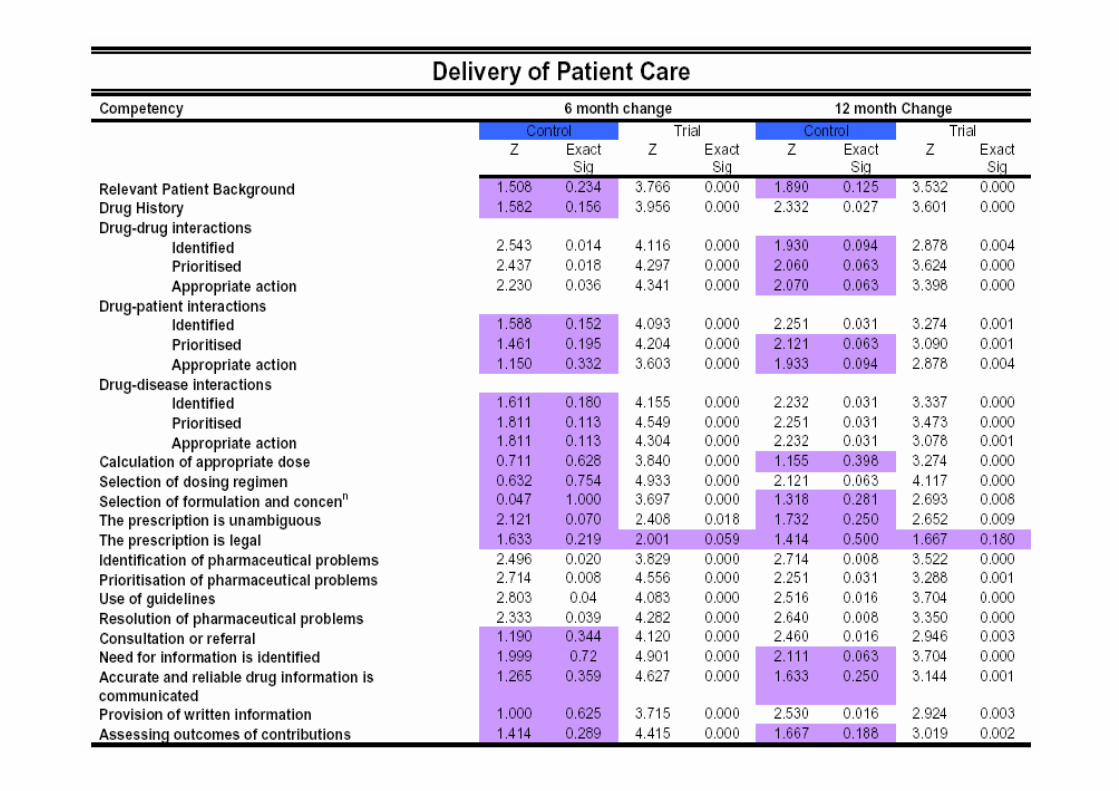
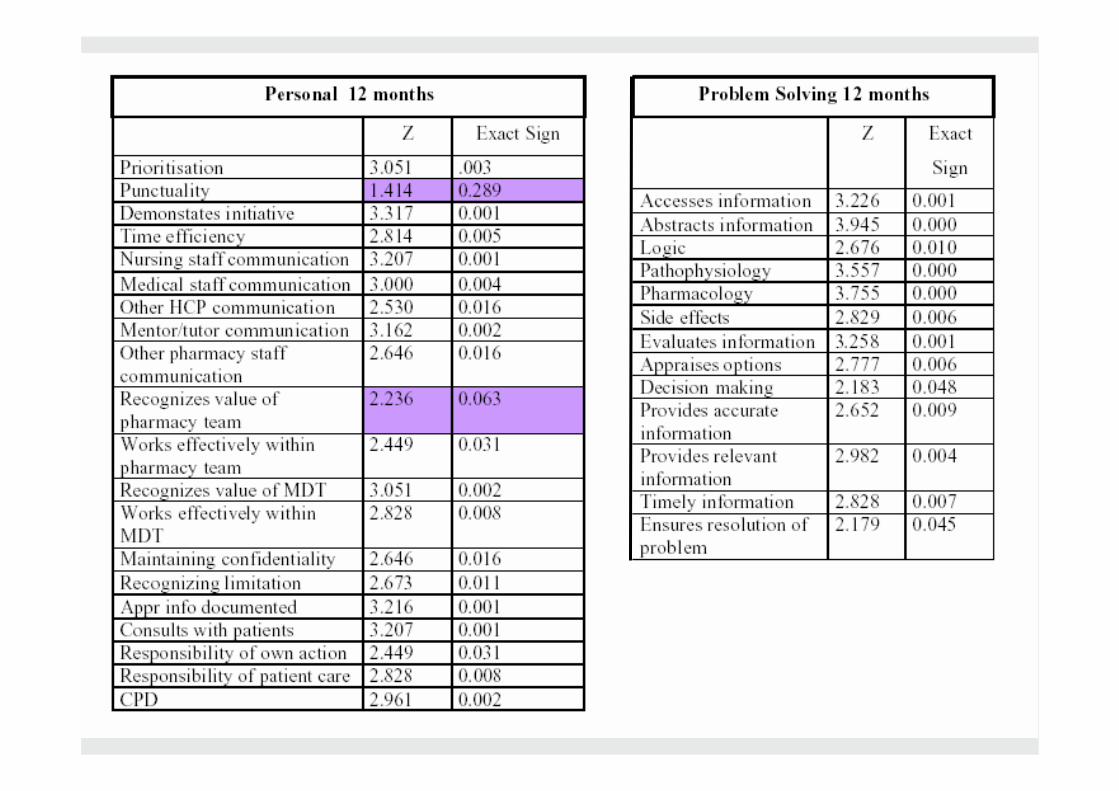
Month-12 findingsBPC 2004
Month-12 findingsBPC 2004

RecruitmentRecruitmentEducational research
Difficulty with controlled study designs3-part recruitment
Election for intervention groupElection for non-intervention groupNo preference
Final allocationIntervention group: 13 NHS trustsNon-intervention group: 9 NHS trusts
Educational researchDifficulty with controlled study designs
3-part recruitmentElection for intervention groupElection for non-intervention groupNo preference
Final allocationIntervention group: 13 NHS trustsNon-intervention group: 9 NHS trusts

Intervention Group n= 74 NHS Trusts = 13
Junior grade pharmacists
All use competency framework, supervised and assessed by clinical managers
Non-intervention Group n= 30 NHS Trusts = 9
Junior grade pharmacists
All undertake orthodox training supervised by clinical managersAssessment made using framework by independent assessor (no feedback)
Design

DemographicsDemographics
2626weeks (median)41.7542.9weeks (mean)
Time with trust 1 (1.35)0 Diploma completed24 (32.4)11 (36.7)Certificate completed
Academia9 (12.2)2 (6.7)Split39 (52.7)17 (56.7)Hospital26 (35.14)11 (36.7)Community
Place of Pre-reg8473Gender (% F)26.87 (+/- 4.17)27.2 (+/- 5.02)Mean age (yrs) +/- stdIntervention (n=74)Non-intervention (n=30)

One Minus Survival Functions
TSURVIVE
14121086420-2
One
Min
us C
um S
urvi
val
.7
.6
.5
.4
.3
.2
.1
0.0
-.1
group
active
active-censored
control
control-censored
(log rank, p=0.0048)

Adapting the General Level Competency Framework for Primary Care and Community Pharmacy
Adapting the General Level Competency Framework for Primary Care and Community Pharmacy

General Level Framework 2nd EditionGeneral Level Framework 2nd Edition

Testing the 2nd Edition General Level Competency Framework in Primary Care and Community Pharmacy
Testing the 2nd Edition General Level Competency Framework in Primary Care and Community Pharmacy

Evaluation
AimsTo evaluate the framework as a measurable mechanism to support the continuing professional development of pharmacists
To validate self assessment as a measure of competence
To explore the use of facilitators to support pharmacists using the framework.

Performance improvementPerformance improvement
12 months8 months4 monthsBaseline
4.0
3.5
3.0
2.5Self-
asse
ssed
per
form
ance
in th
e d
eliv
ery
ofpa
tient
car
ecl
uste
r (m
ean
+ 95
% C
I) Non-intervention (n=31)Intervention (n=69)


Community pharmacyCommunity pharmacyI would like to thank you all for
your help with this project. Without it I still wouldn’t have
started my CPD ..identified areas for CPD. Helps to have competencies as a prompt...you need to know
what you need to be able to doI think I was doing lots of the
skills but never put them together into a sequence step by step to actually realise that
was how I was working
Mills PhD thesis 2007
Competency Framework: General LevelCompetency Framework: General Level
Describes the competencies• Patient care• Problem solving• Personal• Management & organisation
Sector independent• Evidence supporting it’s use in
the acute and community sectors
Valid, evaluated tool• No disagreement on content• Sensitive to change• Improves and sustains
performance
Describes the competencies• Patient care• Problem solving• Personal• Management & organisation
Sector independent• Evidence supporting it’s use in
the acute and community sectors
Valid, evaluated tool• No disagreement on content• Sensitive to change• Improves and sustains
performance
Benefits to clinical pharmacy service
‘These grids, allow me to give structured feedback and target the response to agree an action plan’‘The framework is now an integral part of my training armoury. A development programme for each junior pharmacist has been drawn up based on their competency assessment’
Benefits to clinical pharmacy service
‘These grids, allow me to give structured feedback and target the response to agree an action plan’‘The framework is now an integral part of my training armoury. A development programme for each junior pharmacist has been drawn up based on their competency assessment’

ImplementationImplementation
East and South East EnglandSouth West of EnglandParts of North of England
Piloting in Ireland and Wales
Adapted and adopted in Queensland, Australia
Discussions with Spain
East and South East EnglandSouth West of EnglandParts of North of England
Piloting in Ireland and Wales
Adapted and adopted in Queensland, Australia
Discussions with Spain

Competence, like truth, beauty and contact lenses, is in the eye of the beholder
Laurence J Peter
Competence, like truth, beauty and contact lenses, is in the eye of the beholder
Laurence J Peter

Copy of slides and 2nd Edition of GLF available on: www.codeg.orgCopy of slides and 2nd Edition of GLF available on: www.codeg.org

Competence, competency and pharmaceutical care:
The why, what and how to competence assessment
Competence, competency and pharmaceutical care:
The why, what and how to competence assessment
Graham Davies,Professor of Clinical Pharmacy & Therapeutics,King’s College, London
Graham Davies,Professor of Clinical Pharmacy & Therapeutics,King’s College, London
Questions?